Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
From Preconception to Postnatal: Parental Risk Factors for Fetal-Infant Growth Faltering in LMICs—a Scoping Review (2020–2025)
Authors Koeryaman MT ![]() , Rahayuwati L
, Rahayuwati L ![]() , Sari SP
, Sari SP ![]() , Mutyara K
, Mutyara K ![]() , Trisanto A
, Trisanto A
Received 11 October 2025
Accepted for publication 10 January 2026
Published 2 February 2026 Volume 2026:19 573036
DOI https://doi.org/10.2147/JMDH.S573036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Mira Trisyani Koeryaman,1 Laili Rahayuwati,2 Sheizi Prista Sari,2 Kuswandewi Mutyara,3 Agus Trisanto4
1Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia; 2Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia; 3Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, 45363, Indonesia; 4Department of Electrical Engineering, Faculty of Mathematics and Natural Sciences, Universitas Padjadjaran, Bandung, 45363, Indonesia
Correspondence: Mira Trisyani Koeryaman, Department of Maternity Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, 45363, Indonesia, Tel +44 7516 568119, Email [email protected]
Purpose: This review aimed to map the association between parental (both maternal and paternal) risk factors, from preconception through the postnatal period, and fetal-infant growth faltering.
Patients and Methods: This scoping review followed the PRISMA-ScR frameworks to systematically gather and analyze evidence from major databases (PubMed, Scopus and Web of Science). The inclusion criteria encompassed studies involving pregnant women, fetuses, or infants aged 0– 24 months, including those diagnosed with fetal or infant growth faltering that examined maternal and/or paternal risk factors, conducted in Low- and Middle-Income Countries (LMICs), using study designs such as observational, cross-sectional, cohort, case-control, or randomized controlled trials, and published in English between 2020 and 2025. Data were analysed through thematic synthesis.
Results: From 4235 initial records, we identified 17 eligible studies for this review. The findings showed that the determinants of fetal and infant growth disorders are multifaceted, falling into four key areas. These included individual factors including maternal age, education, nutritional status, health condition, reproductive history, mental health and psychological, marital and socioeconomic,occupation, substance use, and infant factors; environmental concerns including household sanitation and hygiene, water, fuel source, house conditions. Community factors including poverty, deprivation, ethnicity, social inequality, and geographical characteristics. Policy factors, including coverage and quality Antenatal care (ANC), and access to maternal and child health services. These factors represent secondary conditions shaped by broader social and structural determinants of health, rather than direct causal factors. The key determinants shown to influence fetal and infant growth are individual, environmental, community, and policy factors.
Conclusion: Fetal and infant growth are influenced by a combination of behavioural, socioeconomic, and environmental factors. These factors contribute considerably to the increased risk of growth disorders in fetal and infant.
Keywords: couple, growth disorder, health behaviour, infant, reproductive ages
Introduction
Infant growth faltering is a widely documented global health problem and a significant obstacle to efforts the overall health status of children.1 The World Health Organization (WHO) also recognizes this issue as part of the global challenge to achieve sustainable development targets in child health. Infant growth faltering, including conditions like Intrauterine Growth Restriction (IUGR) and stunting, is defined as when a fetus or child’s growth fails to reach its optimal potential. This can be due to various biological and environmental factors, even when the child has access to health and nutrition services.2,3 Furthermore, growth disorders in infants can have significant impacts on cognitive, physical, and economic development from childhood to adulthood, leading to lower productivity and increased vulnerability to chronic diseases later in life.4
This problem reflects the complexity of the various determinants of health environment, heredity, lifestyles, and health care services.5 Environmental factors include traditional practices during pregnancy and childrearing and cultural beliefs, which in some communities significantly impact infant health and growth. For example, in Papua, Indonesia, traditional care practices for low birth weight (LBW) infants are deeply rooted in cultural beliefs, which can sometimes hinder effective caregiving.6 Similarly, in South Africa, cultural beliefs and social aspects, including the lack of income and dependence on food purchasing, drive mothers’ eating habits, breastfeeding behavior, and infant and young child feeding (IYCF) practices.7 Heredity factors relate to biological predispositions, including maternal and infant characteristics, that affect fetal and infant growth.8 Maternal Lifestyle factors encompass infant health.9 Health care services refer to the availability and quality of maternal and child health services, affordability of nutritious food, access to health education, and effective prenatal and postnatal care, which are essential for supporting optimal child growth. Limited access to quality prenatal and postnatal care is associated with higher rates of growth faltering in infants.10,11
Based on these determinants, the approach to the infant growth disorder determinant model can be analysed through three main domains that influence each other: (1) contextual factors—including the influence of genetics, local culture, social, economic, and geographical systems that influence parenting practices and eating patterns; (2) individual and group influences—including personal and social beliefs about maternal and child nutrition practices and perceptions of normal growth; and (3) specific issues related to health and nutrition services—for example, the quality of antenatal nutrition interventions, nutrition education, and the ability of health workers to identify risks early.2,3
Despite numerous studies examining individual risk factors, the current evidence remains fragmented and largely focused on isolated periods, such as pregnancy or early infancy, without a full integration of parental and environmental influences across the continuum of reproductive and early life stages. Previous scoping review have mapped risk factors for undernutrition and poor growth, but have been limited to 0–6 months and a specific region, leaving gaps in understanding the full spectrum of parental and environmental influences on growth faltering in low- and middle-income countries (LMICs).12 Addressing this knowledge gap, the present scoping review aimed to map the association between parental (both maternal and paternal) risk factors, from preconception through the postnatal period, and fetal-infant growth faltering in LMICs.
Material and Methods
Study Design
This scoping review aimed to understand the determinants of infant growth and development influenced by couple reproductive age behaviour factors, and to identify updated information on risk factors that may cause infant faltering, as discussed and represented in the literature. We conducted this scoping according to PRISMA guidelines and the quality of included studies was assessed using the Joanna Briggs Institute (JBI) critical appraisal tools to ensure methodological rigor and relevance (Table S1).13,14 The scoping review was conducted following the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines (Table S2). This scoping review is registered with the Open Science Framework (OSF) (Registration DOI: [10.17605/OSF.IO/RSVX7]).
Search Strategy and Criteria
The literature was obtained from three databases searched: PubMed, Scopus and web of science using Medical Subject Headings (MeSH, word terms, or database-specific thesaurus equivalent) to retrieve the studies (Tables S3 and S4). The database search strategy was developed using two main concepts: infant growth faltering and its associated risk factors, within the context of pregnant people and infants. MeSH terms for infant growth faltering included “Infant, Small for Gestational Age” (MeSH), “Infant, Low Birth Weight” (MeSH), “Fetal Growth Retardation” (MeSH), and “Infant, Premature” (MeSH), while free-text terms included “fetal growth restriction”, “intrauterine growth restriction”, “IUGR”, “small for gestational age”, “SGA”, “growth faltering”, “postnatal growth faltering”, “infant growth faltering”, “low birth weight”, and “LBW”. Risk factor-related MeSH terms included Risk Factors (MeSH), and free-text terms included “risk factor*”, “population at risk”, “maternal risk factor*”, “paternal risk factor*”, “maternal factor*”, “paternal factor*”, “maternal characteristic*”, “paternal characteristic*”, “maternal exposure*”, “paternal exposure*”, “maternal determinant*”, and “paternal determinant*”. Contextual MeSH terms included Pregnancy (MeSH), Pregnant People (MeSH), Fetus (MeSH), and Infant (MeSH), while free-text terms included “pregnant wom*n”, “antenatal wom*n”, “prenatal wom*n”, “infant”, “newborn*”, “neonate*”, and “young infant*”. Geographic and socioeconomic context terms included Developing Countries (MeSH) and free-text terms such as “low- and middle-income countr*”, “low income countr*”, “middle income countr*”, “LMIC*”, “resource-limited setting*”, “resource-poor setting*”, “developing nation*”, and “developing region*”. The main search was published between 2020 and 2025. Additionally, free search articles were selected through Google Scholar. We also included articles written in English. Table 1 presents the detailed inclusion and exclusion criteria considered in the present review work.
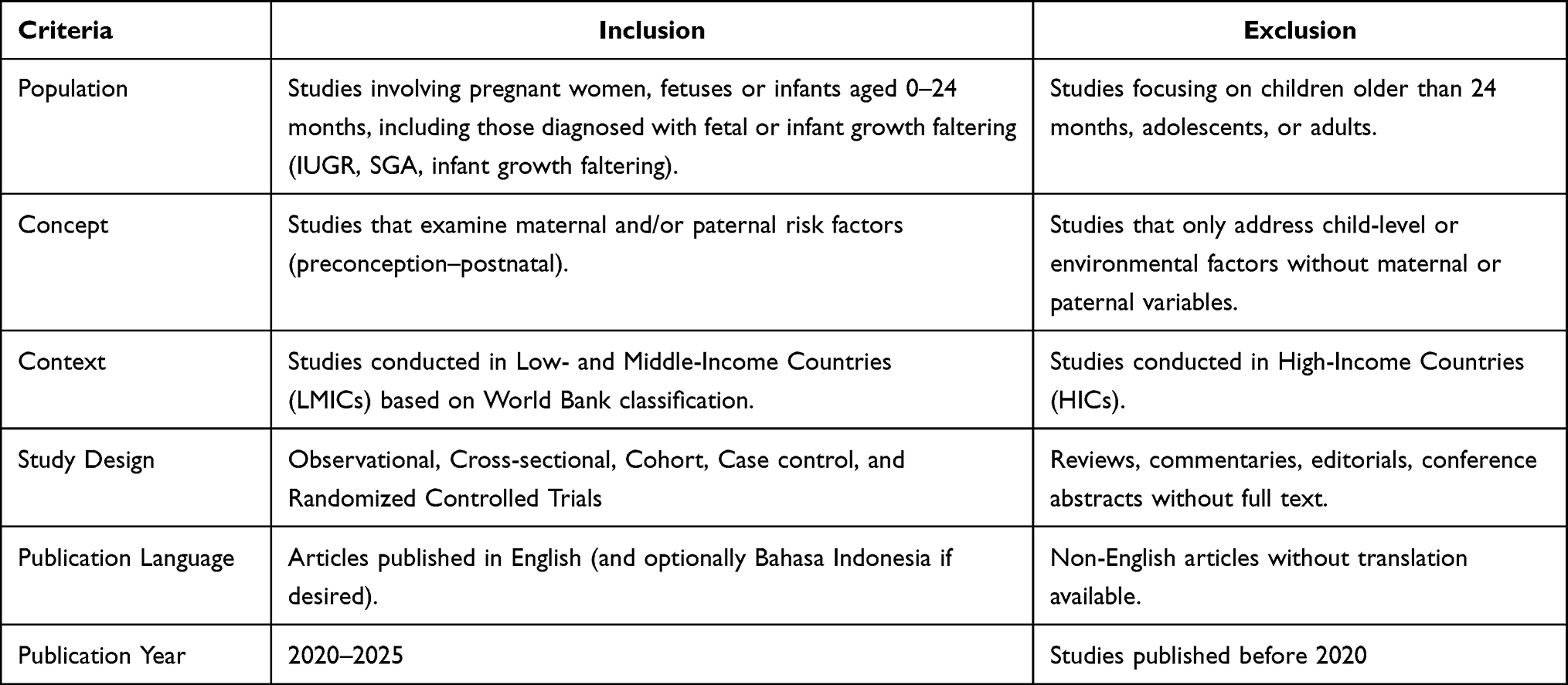 |
Table 1 Inclusion and Exclusion Criteria |
Article Screening and Selection
All publications that addressed the keywords based on inclusion and exclusion criteria. An authorship team independently fast-screened the articles through a three-step process: removing duplicate articles, screening by title and abstract, and making full-text reading eligible. Then, the selection was made by inclusion criteria. The identified articles were compiled and processed in open-source programs, such as EndNote and Microsoft Excel. Once the relevant publications were identified, key information was systematically extracted to align with the objectives of this scoping review. All extracted data include the characteristics of the study, such as author, year, country, methodology, and results. Then, the authors synthesised the extracted data retrospectively using a narrative approach.
Data Extraction
The process of data extraction consists of three phases. Firstly, the authorship team (MTK, LR and SP) conducted the data extraction process to ensure consistency across all articles using manual tables. The extracted data included the study location, population characteristics (particularly couples of reproductive age), specific risk factors, methodological approach, study focus, and a synthesis of principal findings. Secondly, the authorship team uses a thematic framework to extract meaningfully and group specific determinants factors related to fetal-infant growth disorders (Table 2). In Phase 3, the authorship team identified and categorised the findings of the included articles and mapped them into a chart of four domains that contribute to infant growth disorders. Data were highlighted and grouped as dominant risk factors, including individual, environmental, community-level, and policy factors (see Figure 1). The data extraction process was conducted on the most comprehensive report of a given study.
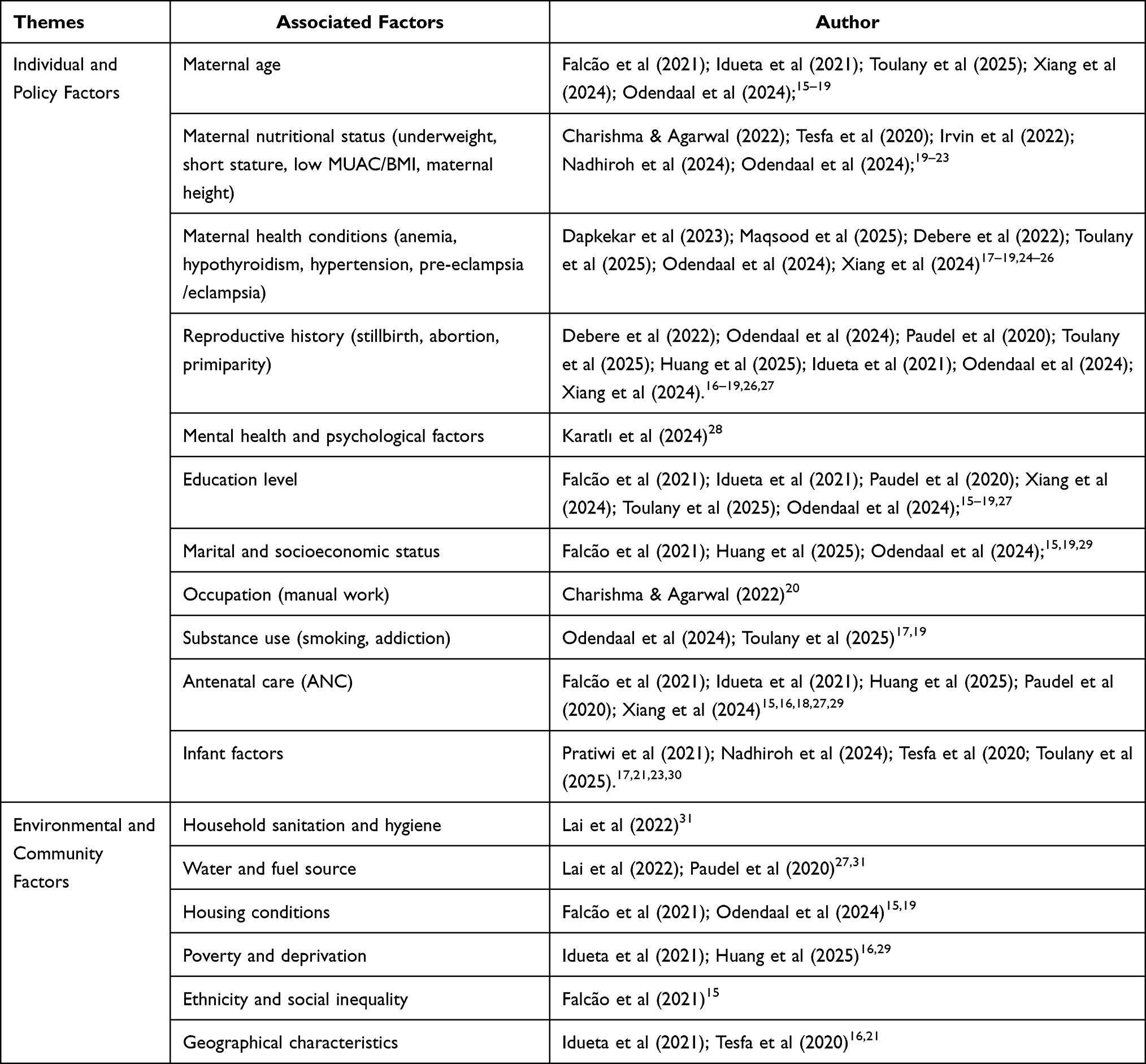 |
Table 2 Modified Themes Identified |
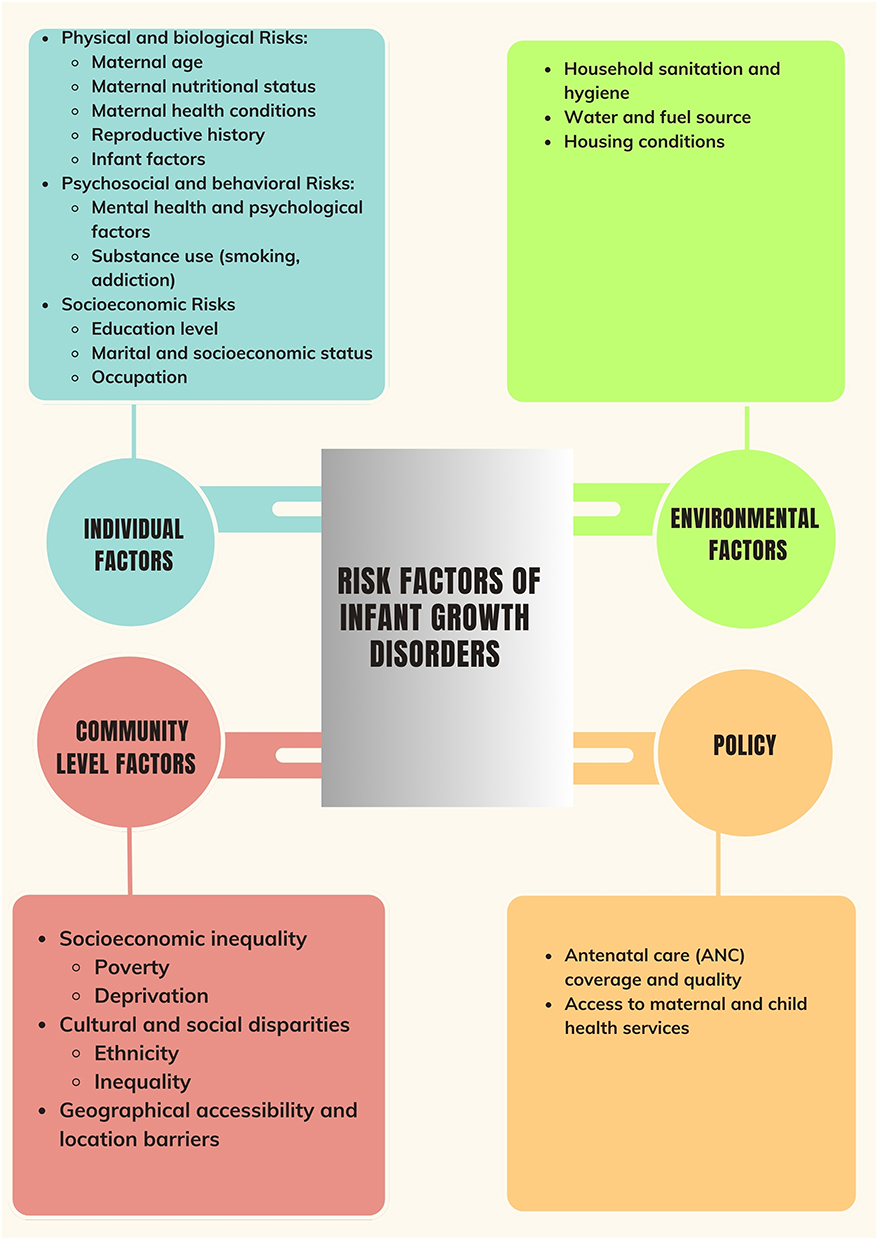 |
Figure 1 Risk Factors of Infant Growth Disorder. |
Data Synthesis and Analysis
In this updated scoping review, the included studies were organized into categories based on the identified risk factors associated with fetal-infant faltering. The categories were generated retrospectively by the author team and were not predefined or directly referenced in the original studies themselves. For each study, a summary was compiled that incorporated the extracted variables and the classification of determinants, which were then compiled and grouped to construct a descriptive analysis. This process allowed for the identification of consistent patterns, emerging themes, and gaps in the existing literature related to risk factors that may contribute to impaired infant growth and development.
Results
Search Results
A total of 4,235 articles were identified through searches conducted across three electronic databases. Following the removal of duplicate records, 2,267 articles remained for title and abstract screening. From these, 17 articles met the eligibility criteria for full-text assessment. Records excluded at this stage were removed due to irrelevance to the study objectives, incompatibility with the target study population, or unavailability of the full text. Figure 2 illustrates the PRISMA-ScR flow diagram detailing the screening process and reasons for exclusion. Figure 2 presents the PRISMA-ScR flow diagram, which outlines the study selection process from initial identification to final inclusion. The diagram details the number of records retrieved from each of the three databases, the removal of duplicates, and the subsequent stages of title/abstract screening and full-text assessment. Reasons for exclusion at the full-text stage included irrelevance to the study focus, mismatch with the target population, and lack of access to the full text.
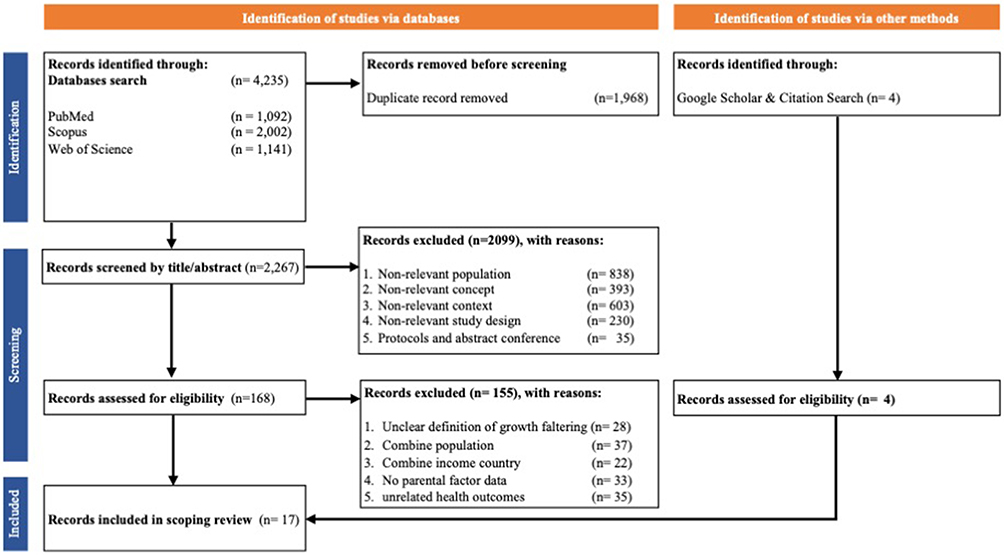 |
Figure 2 PRISMA Flow Diagram. |
Study Characteristics
A total of 17 studies published between 2020 and 2025 were included in this review, encompassing diverse geographical regions including Turkey, India, Ethiopia, Brazil, 32 low- and middle-income countries, Mexico, Indonesia, Cambodia, Pakistan, Iran, Nepal, South Africa, and China. The study designs varied, consisting of prospective observational studies, cross-sectional studies, case-control studies, and cohort studies. Sample sizes ranged widely from 54 participants in a small case-control study to over 12 million live births in national cohort studies. The populations investigated included pregnant women, postpartum mothers, infants, and children aged 0–24 months, with specific focus on those at risk of small-for-gestational-age (SGA), intrauterine growth restriction (IUGR), low birth weight (LBW), and childhood growth faltering (Table 3).
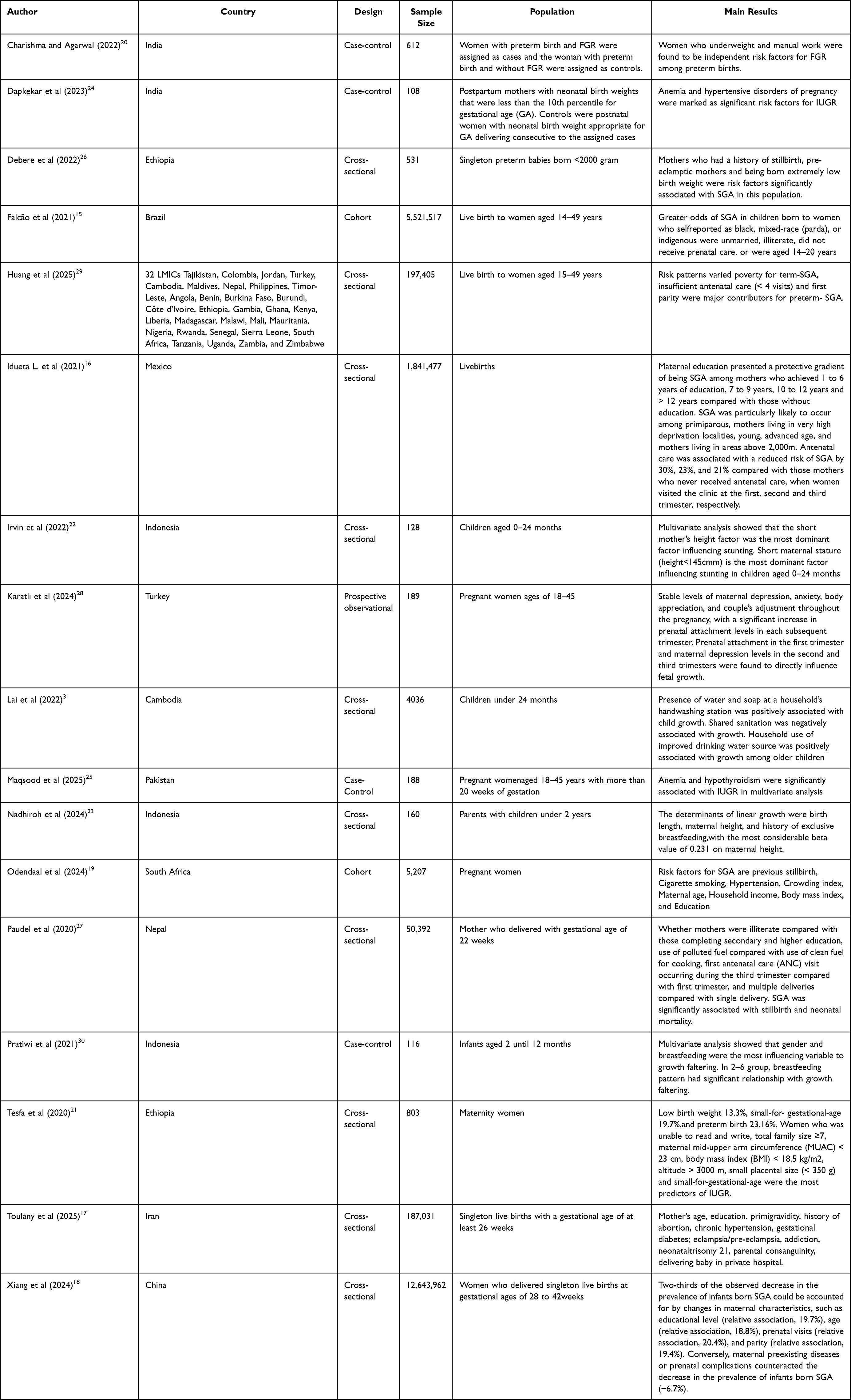 |
Table 3 Characteristic of the Study |
Risk Factors Contextual
The determinant risk factors for fetal-infant growth disorders can be categorized into behavioural, environmental and predictive indicators. Furthermore, the thematic mapping of the 17 included studies is illustrated in Figure 1, which organizes the findings into four main domains: individual factors – encompassing physical and psychological risks; environmental factors; community-level factors and policy factors.
Individual Factors and Policy Factors
Various individual conditions were identified as major risk factors for fetal–infant growth faltering. These include physical, psychosocial, and socioeconomic determinants that interact to influence growth outcomes. Physical risks involve maternal age, undernutrition, short stature, and pregnancy-related health conditions such as anemia, hypothyroidism, hypertension, and pre-eclampsia.15–26 These conditions affect placental function and fetal nutrient supply. Reproductive history factors such as stillbirth, abortion, and primiparity were also associated with an increased risk of fetal–infant growth faltering.16–19,26,27 Psychosocial factors, including maternal stress and depression, were found to disrupt the mother–infant bond and early stimulation, leading to poorer growth outcomes.28 Socioeconomic factors—such as low education, single marital status, and engagement in manual or physically demanding work—further increased the risk of restricted growth.15–20,27,29 Substance use, such as smoking and addiction, also showed negative associations.17,19 Limited and late antenatal care (ANC) was consistently linked with higher rates of fetal and infant growth faltering, reflecting structural and policy-level gaps in maternal health services.15,16,18,27,29 Overall, these findings highlight that maternal health, psychosocial well-being, and socioeconomic support are interdependent factors that require an integrated approach to prevent fetal–infant growth faltering in LMICs (Table 2).
Environmental Factors and Community Factors
Environmental and community-level conditions play an important role in influencing fetal–infant growth faltering. Poor household sanitation and hygiene were identified as key risk factors, as inadequate waste management and exposure to pathogens can increase infection risks and impair nutrient absorption.31 Limited access to clean water and safe fuel sources was also associated with higher risks of growth restriction, reflecting household environmental deprivation in many LMIC settings.27,31 Unfavorable housing conditions, such as overcrowded or poorly ventilated homes, were found to negatively affect maternal and infant health, increasing vulnerability to infection and undernutrition.15,19 Broader community and structural factors, including poverty, social inequality, and ethnic disparities, were recurrent determinants of growth faltering.15,16,29 Furthermore, geographical characteristics, such as living in remote or high-altitude areas, were linked to limited healthcare access and nutritional deficiencies.16,21 Ranging from sanitation and housing to broader socioeconomic and geographic disparities—shape the overall risk landscape for fetal–infant growth faltering in LMICs (Table 2).
Discussion
The findings of this updated scoping review indicate that infant growth disorders arise from a multifaceted network of risk factors operating at the individual, environmental, community, and policy levels. These determinants interact dynamically, meaning that vulnerabilities in one domain can amplify risks in another, ultimately influencing a child’s ability to achieve optimal growth and development.
At the individual level, physical, biological, psychosocial, behavioral, and socioeconomic vulnerabilities significantly influence infant growth outcomes. Maternal health conditions—such as anemia, hypothyroidism, hypertension, pre-eclampsia or eclampsia—can compromise placental nutrient and oxygen delivery, thereby increasing the risk of intrauterine growth restriction (IUGR) and low birth weight (birthweight reductions particularly notable in cases of inadequate gestational weight gain).32,33 Equally impactful are psychosocial factors such as postpartum depression has been consistently associated with poorer infant growth trajectories, likely mediated through disrupted breastfeeding practices and reduced maternal-infant interaction.34 According to previous longitudinal study from Nigeria, infants of mothers with postpartum depression exhibited significantly lower weight and length trajectories at three and six months postpartum.35
Similar findings have been reported across diverse low- and middle-income settings.36 The role of paternal health, though less emphasized, is also crucial. For instance, paternal pre-conception diabetes has been linked to lower infant birth weight and gestational age, while paternal education and nutrition status further predict adverse perinatal outcomes, including preterm birth and small for gestational age.37 Taken together, these findings underscore the need to adopt a holistic approach that integrates parental health—both physical and mental—to effectively address risks of infant growth disorders.
Based on previous research results, especially in low- and middle-income countries, the determinants of growth failure can be attributed to socioeconomic conditions, including extreme poverty, inadequate access to health services, food insecurity, and malnutrition.38,39 Additionally, environmental conditions, family planning programs, maternal education, and parenting patterns, can influence breastfeeding practices and feeding, potentially leading to the failure of anthropometric assessments in children.34,40 Other studies revealed that residential areas have an influence on growth developmental status, and children in urban areas tend to have better developmental outcomes than those in rural areas.40–42 As well as in Uganda, 30.22% of children are stunted, and 3.63% are wasted, with the highest prevalence in the northeastern and southwestern regions.43
Furthermore, there is a significant correlation between environmental factors and fetal-infant growth outcomes, such household sanitation and hygiene, water, fuel source, and housing condition. Even though it does not confirm a direct causal link between environmental conditions and child growth. Generally, a common growth issue in newborns is having a birth weight and length smaller than the normal size for their gestational age. This growth delay can originate from the fetal stage while still in the womb, a condition known as Intrauterine Growth Retardation (IUGR).44 This condition can be caused by various factors, such as inadequate prenatal care or smoking during pregnancy.45 Many of these conditions are challenging to detect early, which puts the infant at risk of experiencing growth problems throughout their life. Therefore, screening, early detection, and diagnosis are essential in reducing neonatal morbidity and mortality rates. As well as, predictive models can be applied to prevention, rehabilitation, clinical and physiological laboratory testing, medical care, and even in monitoring generic drug use.46 These models can help identify high-risk populations, detect early warning signs of growth impairment, and optimize resource allocation, thus complementing public health interventions aimed at mitigating the impact of adverse environmental exposures. For example, evidence-based algorithms integrate data on maternal nutrition, household sanitation, air quality, and socioeconomic indicators to predict the risk of stunting in children under five. By recognizing patterns that may not be readily apparent through conventional statistical approaches, these predictive models enable healthcare providers to implement targeted nutritional support, environmental interventions, and early rehabilitation strategies. Similarly, predictive analytics can help identify pregnant women at higher risk of complications from environmental exposures, enabling timely clinical monitoring and preventive care.
Conclusion
This scoping review highlights the multifactorial nature of infant faltering, emphasizing that risks extend beyond biological determinants to encompass psychosocial, environmental, community, and policy-level influences. At the individual level, maternal and paternal health— physical, biological, psychosocial, behavioral, and socioeconomic —play a pivotal role in shaping fetal and early childhood growth trajectories. Environmental factors such as household sanitation and hygiene, water, fuel source, and housing conditions. Community factors related to fetal-infant faltering are poverty, deprivation, ethnicity, social inequality, and geographic characteristics. Policy-related determinants, such as coverage and quality of ANC, and access to maternal and child health services, are critical levers for prevention but remain inconsistently implemented. Addressing fetal-infant faltering in LMCIs therefore requires an integrated, multisectoral approach—one that bridges healthcare, social protection, education, and environmental policy—to mitigate risks and promote optimal growth from conception through early childhood. This review provides an updated synthesis of evidence, highlighting the interconnection between parental health, environmental conditions, and policy-level interventions in influencing fetal-infant growth outcomes. Addressing these complex and interrelated factors requires an integrated, multisectoral approach that bridges healthcare, social protection, education, and environmental policy to promote optimal growth from conception through early childhood.
Acknowledgments
The authors gratefully acknowledge Universitas Padjadjaran for institutional support. This publication charge is funded by Unpad through the Grant for Article Review Universitas Padjadjaran (Contract No. 1974/UN6.L/PT.00/2025 and 403).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This scoping review was funded by the Academic Leadership Grant (ALG) of Universitas Padjadjaran as well as the open access article processing charge funded by Universitas Padjadjaran.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kang Y, Aguayo VM, Campbell RK, West KP. Association between stunting and early childhood development among children aged 36–59 months in South Asia. Matern Child Nutr. 2018;14(S4):12684. doi:10.1111/mcn.12684
2. González-Fernández D, Muralidharan O, Neves P, Bhutta Z. Associations of Maternal Nutritional Status and Supplementation with Fetal, Newborn, and Infant Outcomes in Low-Income and Middle-Income Settings: an Overview of Reviews. Nutrients. 2024;16(21):3725. doi:10.3390/nu16213725
3. Haymond M, Kappelgaard AM, Czernichow P, Biller BM, Takano K, Kiess W. Early recognition of growth abnormalities permitting early intervention. Acta Paediatr. 2013;102(8):787–13. doi:10.1111/apa.12266
4. Abidanovanty FM, Suryawan A, Hendarto H. Growth and Development Aged 0–24 Months with a History of Low Birth Weight (LBW) in Dr. Soetomo General Hospital Surabaya. Indonesian J Public Health. 2023;18(2):230–241. doi:10.20473/ijph.v18i2.2023.230-241
5. Blum HL. Planning for Health: Generics for the Eighties. Human Sciences Press; 1981.
6. Situmorang HE, Rustina Y, Novieastari E Understanding cultural barriers to the care of low-birth-weight infants in Papua, Indonesia: a qualitative descriptive study. Belitung Nurs J. 2025;11(5):579–588. doi:10.33546/bnj.3953
7. Chakona G Social circumstances and cultural beliefs influence maternal nutrition, breastfeeding and child feeding practices in South Africa. Nutr J. 2020;19(1):47. doi:10.1186/s12937-020-00566-4
8. Hambidge KM, Bann CM, McClure EM, et al. Maternal characteristics affect fetal growth response in the women first preconception nutrition trial. Nutrients. 2019;11(10):2534. doi:10.3390/nu11102534
9. Favara G, Maugeri A, Barchitta M, Lanza E, Magnano San Lio R, Agodi A Maternal lifestyle factors affecting breast milk composition and infant health: a systematic review. Nutrients. 2024;17(1):62. doi:10.3390/nu17010062
10. Memon Z, Zaidi S, Riaz A Residual barriers for utilization of maternal and Child health services: community perceptions from rural Pakistan. Glob J Health Sci. 2015;8(7):47. doi:10.5539/gjhs.v8n7p47
11. Parkhurst JO, Ssengooba F Assessing access barriers to maternal health care: measuring bypassing to identify health centre needs in rural Uganda. Health Policy Plan. 2009;24(5):377–384. doi:10.1093/heapol/czp023
12. Hjertholm KG, Iversen PO, Holmboe-Ottesen G, Jepsen R Risk factors for undernutrition and poor growth during the first 6 months of life in sub-saharan Africa: a scoping review. Clin Nutr ESPEN. 2025;68:309–318. doi:10.1016/j.clnesp.2025.05.019
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
14. Joanna Briggs Institute. The Joanna Briggs institute critical appraisal tools. 2017-07-15)[2022-09-18]. https://jbi global/critical-appraisal-tools. Preprint posted online 2017.
15. Falcão IR, Ribeiro-Silva R, de C, de Almeida MF. Factors associated with small- and large-for-gestational-age in socioeconomically vulnerable individuals in the 100 Million Brazilian Cohort. Am J Clin Nutr. 2021;114(1):109–116. doi:10.1093/ajcn/nqab033
16. SI L, H B, Eo O, CB M. Maternal Risk Factors for Small-for-Gestational-Age Newborns in Mexico: Analysis of a Nationwide Representative Cohort. Front Public Health. 2021;9:101125. doi:10.3389/fpubh.2021.707078
17. Toulany M, Khalili N, Heidarzadeh M, Habibelahi A, Haj-sheykholeslami A. Intrauterine growth restriction and its associated factors in Tehran, comparing 3 common standards. PLoS One. 2023;20(7):e0326348. doi:10.1371/journal.pone.0326348
18. Xiang L, Li X, Mu Y, et al. Maternal Characteristics and Prevalence of Infants Born Small for Gestational Age. JAMA Netw Open. 2024;7(8):e2429434. doi:10.1001/jamanetworkopen.2024.29434
19. Odendaal H, Brink L, Lachmanb A, Nel D. Risk factors for small for gestational age as defined by a birthweight z-score below minus one: A prospective observational study. Med Res Arch. 2024;12(8). doi:10.18103/mra.v12i8.5731
20. Charishma CS, Agarwal K. Risk factors for fetal growth restriction in preterm births: a retrospective case control study. Int J Reprod Contracept Obstet Gynecol. 2022;11(10): 2734. doi:10.18203/2320-1770.ijrcog20222470
21. Tadege M, Digssie A, Abebaw S. Intrauterine growth restriction and its associated factors in South Gondar zone hospitals, Northwest Ethiopia, 2019. Archives of Public Health. 2020;78(1):89. doi:10.1186/s13690-020-00475-2
22. Irving S, Rezkita BE, Putri IS, Nugroho HW, Usman NA. Risk factors for short stature among children aged 0-24 months in Surakarta. 2023;4(1):40–46. doi:10.24123/kesdok.V4i1.5313. Keluwih: Jurnal Kesehatan dan Kedokteran.
23. Nadhiroh SR, Ayuningtyas H, Salsabil IS. Linear growth determinants of under two years old children in Surabaya, Indonesia. Clin Epidemiol Glob Health. 2024;27:101605. doi:10.1016/j.cegh.2024.101605
24. Dapkekar P, Bhalerao A, Kawathalkar A, Vijay N. Risk Factors Associated With Intrauterine Growth Restriction: A Case-Control Study. Cureus. 2023;15(6):e40178. doi:10.7759/cureus.40178
25. Maqsood M, Ahad M, Irshad S. Risk Factors Associated with Intrauterine Growth Restriction: A Case-Control Study. Pakistan Journal of Health Sciences. 2025;110–114. doi:10.54393/pjhs.v6i9.3209
26. Debere MK, Haile Mariam D, Ali A, Mekasha A, Chan GJ. Factors associated with small-for-gestational-age births among preterm babies born <2000 g: a multifacility cross-sectional study in Ethiopia. BMJ Open. 2022;12(11):e064936. doi:10.1136/bmjopen-2022-064936
27. Gautam Paudel P, Sunny AK, Gurung R, et al. Prevalence, risk factors and consequences of newborns born small for gestational age: a multisite study in Nepal. BMJ Paediatr Open. 2020;4(1):e000607. doi:10.1136/bmjpo-2019-000607
28. Çetindağ Karatlı SK, Uğurlu M, Keskin A, Dağcıoğlu BF, Karakaş Uğurlu G, Karatlı S. A comprehensive and longitudinal view of pregnancy from the perspective of the couple, maternal mental health and fetal growth. Matern Child Health J. 2024;28(9):1592–1603. doi:10.1007/s10995-024-03953-z
29. Huang Y, Zhang H, Xiong Z, et al. Mortality and risk factors of small vulnerable newborns in 32 low- and middle-income countries. BMC Med. 2025;23(1):558. doi:10.1186/s12916-025-04406-2
30. Pratiwi R, Pramono A, Hardaningsih G. Risk factor of growth faltering in infants aged 2-12 months. Jurnal Gizi Indonesia. 2021;10(1):72–79. doi:10.14710/jgi.10.1.72-79
31. Lai A, Velez I, Ambikapathi R, Seng K, Cumming O, Brown J. Risk factors for early childhood growth faltering in rural Cambodia: a cross-sectional study. BMJ Open. 2022;12(4):e058092. doi:10.1136/bmjopen-2021-058092
32. Fasoulakis Z, Koutras A, Antsaklis P, et al. Intrauterine growth restriction due to gestational diabetes: From pathophysiology to diagnosis and management. Medicina. 2023;59(6):1139. doi:10.3390/medicina59061139
33. Tsikouras P, Antsaklis P, Nikolettos K, et al. Diagnosis, prevention, and management of fetal growth restriction (FGR). J Pers Med. 2024;14(7):698. doi:10.3390/jpm14070698
34. Deshpande M, Miriam D, Shah N, et al. Influence of parental anthropometry and gestational weight gain on intrauterine growth and neonatal outcomes: Findings from the MAI cohort study in rural India. PLOS Global Public Health. 2023;3(8):e0001858. doi:10.1371/journal.pgph.0001858
35. Salako J, Bakare D, Colbourn T, et al. Maternal mental well-being and recent child illnesses–A cross-sectional survey analysis from Jigawa State, Nigeria. PLOS Global Public Health. 2023;3(3):e0001462. doi:10.1371/journal.pgph.0001462
36. Fekadu Dadi A, Miller ER, Mwanri L. Antenatal depression and its association with adverse birth outcomes in low and middle-income countries: A systematic review and meta-analysis. PLoS One. 2020;15(1):e0227323. doi:10.1371/journal.pone.0227323
37. Murugappan G, Li S, Leonard SA, Winn VD, Druzin ML, Eisenberg ML. Association of preconception paternal health and adverse maternal outcomes among healthy mothers. Am J Obstet Gynecol MFM. 2021;3(5):100384. doi:10.1016/j.ajogmf.2021.100384
38. Retnakaran R, Wen SW, Tan H, et al. Paternal weight prior to conception and infant birthweight: a prospective cohort study. Nutr Diabetes. 2021;11(1):28. doi:10.1038/s41387-021-00172-1
39. Siddiqui F, Salam RA, Lassi ZS, Das JK. The intertwined relationship between malnutrition and poverty. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00453
40. Rahman MDA, Halder HR, Rahman MDS, Parvez M. Poverty and childhood malnutrition: Evidence-based on a nationally representative survey of Bangladesh. PLoS One. 2021;16(8):e0256235. doi:10.1371/journal.pone.0256235
41. Liang D, Jiang Z, Liu X, et al. Factors associated with anthropometry Z-scores in exclusively breastfed infants aged 0–6 months in 10 cities of China. Nutrients. 2025;17(13):2163. doi:10.3390/nu17132163
42. Andriyani R, Fadlyana E, Tarigan R. Factors affecting the developmental status of children aged 6 months to 2 years in urban and rural areas. Children. 2023;10(7):1214. doi:10.3390/children10071214
43. Ssentongo P, Fronterre C, Ericson JE, et al. Preconception and prenatal environment and growth faltering among children in Uganda. JAMA Netw Open. 2025;8(3):e251122. doi:10.1001/jamanetworkopen.2025.1122
44. Sharma D, Shastri S, Sharma P. Intrauterine growth restriction: antenatal and postnatal aspects. Clin Med Insights Pediatr. 2016;10. doi:10.4137/CMPed.S40070
45. Eftekhar H, Aghamolaei T, Abedini S. Risk factors associated with intrauterine growth retardation (IUGR) in Bandar Abbas, Iran. Payesh. 2007;6(3).
46. Takura T, Hirano Goto K, Honda A. Development of a predictive model for integrated medical and long-term care resource consumption based on health behaviour: application of healthcare big data of patients with circulatory diseases. BMC Med. 2021;19(1):15. doi:10.1186/s12916-020-01874-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.