Back to Journals » Infection and Drug Resistance » Volume 19
From Evidence to Implementation: A SIMPIOS Multimodal, Continuous Improvement Approach to Prevent Surgical Site Infections
Authors Sartelli M, Labricciosa FM, Moro ML, Pan A, Ripabelli G ![]()
Received 14 November 2025
Accepted for publication 20 January 2026
Published 22 January 2026 Volume 2026:19 565233
DOI https://doi.org/10.2147/IDR.S565233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Massimo Sartelli,1 Francesco M Labricciosa,2 Maria Luisa Moro,3 Angelo Pan,4 Giancarlo Ripabelli5
1Department of General Surgery, Macerata Hospital, Macerata, 62100, Italy; 2Global Alliance for Infections in Surgery, Macerata, 62100, Italy; 3Italian Multidisciplinary Society for the Prevention of Healthcare-Associated Infections. Scientific Committee, Milano, 20161, Italy; 4Unit of Infectious Diseases, ASST Cremona, Cremona, 26100, Italy; 5Department of Medicine and Health Sciences “vincenzo Tiberio”, University of Molise, Campobasso, 86100, Italy
Correspondence: Massimo Sartelli, Macerata Hospital, Macerata, 62100, Italy, Email [email protected]
Abstract: Surgical site infections (SSIs) represent the most prevalent healthcare-associated infections among surgical patients and are a major contributor to postoperative morbidity and mortality, prolonged hospitalization, and increased healthcare costs worldwide. Despite the availability of robust evidence-based guidelines for SSI prevention, adherence to these recommendations in routine clinical practice remains limited. To address this implementation gap, the Italian Multidisciplinary Society for the Prevention of Healthcare-Associated Infections (SIMPIOS) established a dedicated working group to identify, synthesize, and disseminate the most effective strategies for translating evidence-based SSI prevention measures into practice. The initiative was grounded in the recognition that the infection prevention and control (IPC) approach requires not only a solid scientific foundation but also a multidisciplinary, systems-based approach that integrates clinical evidence with a culture of collaboration and safety. The resulting article seeks to provide a structured framework for continuous quality improvement in IPC. The SIMPIOS framework provides an evidence-based approach to SSI prevention, focusing on the practical implementation of guidelines in everyday clinical practice. Grounded in implementation science, this framework promotes multimodal strategies, multidisciplinary collaboration, and continuous evaluation to support sustainable improvements in patient safety across the perioperative pathway.
Keywords: behavioral change, bundle, healthcare-associated infections, infection prevention and control, patient safety
Introduction
Healthcare-associated infections (HAIs) represent a serious threat to public health in Italy and worldwide. The phenomenon of HAIs is closely linked to that of antimicrobial resistance (AMR) and constitutes a priority for healthcare systems at all levels of care. One of the most important interventions for HAI control is the implementation of best practices within an integrated program that should be tailored to each care setting. Infection Prevention and Control (IPC) is a practical, evidence-based approach aimed at preventing both patients and healthcare workers from acquiring HAIs.
IPC is a highly complex field that requires a broad and integrated vision. It involves multiple factors—cultural, organizational, environmental, and patient-related—that interact synergistically to ensure the overall safety of care (Figure 1).
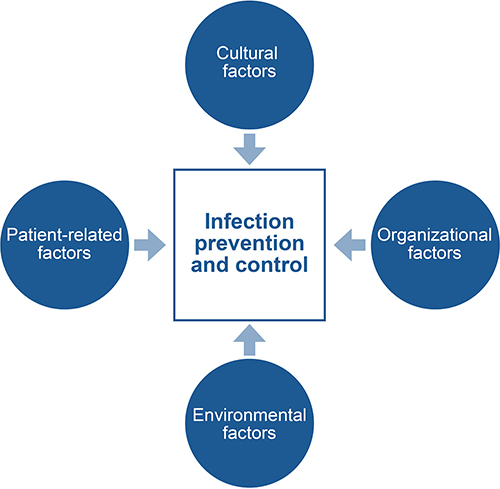 |
Figure 1 The dynamic interaction of multiple factors in infection prevention and control. |
Cultural factors play a central role in IPC and encompass three interrelated dimensions: knowledge, awareness, and attitude. Knowledge refers to the technical and scientific competencies that enable healthcare workers (HCWs) to understand and correctly apply preventive measures. Awareness involves recognizing the importance of HCW engagement in patient safety and understanding that even simple actions, such as proper hand hygiene, can have a significant impact on infection prevention. Attitude encompasses the values, motivations, and behaviors that guide HCWs in translating their knowledge of best practices into consistent, proactive, and collective actions.
Promoting knowledge, awareness, and attitude among HCWs thus reinforces the concept of IPC not only as a professional obligation but also as a shared ethical value fundamental to delivering safe and high-quality care.
Organizational factors represent the framework within which an integrated IPC system functions. Adequate resources, appropriate staffing levels, effective leadership, and continuous education and training are critical to the successful implementation of IPC measures. Healthcare organizations that foster a robust safety culture are better equipped to facilitate open communication, engage HCWs, and enhance preparedness for improving implementation and minimizing errors.
Environmental factors include all physical and infrastructural elements that influence the survival, transmission, and control of microorganisms within healthcare settings. These factors encompass environmental cleanliness, ventilation systems, water quality and supply, waste management, construction materials and design, and adherence to environmental hygiene practices. Effective control of these determinants is essential to reducing the risk of HAIs and ensuring patient protection.
Patient-related factors are equally significant. Aging, comorbidities, immunosuppression, and the use of invasive devices increase susceptibility to HAIs. However, patients should not be regarded merely as passive recipients of care, but rather as active participants in the IPC process. Patient education, engagement, and empowerment strengthen the overall safety of the care continuum. The prevention of HAIs results from the dynamic interaction of multiple factors; no single element can independently ensure success. Only an integrated and multidisciplinary approach can yield a truly effective IPC system.
Surgical site infections (SSIs) are the most prevalent HAIs among surgical patients and constitute a major cause of postoperative morbidity and mortality, prolonged hospital stays, and increased healthcare costs globally. SSIs arise from a combination of predisposing factors. Although bacterial contamination of surgical wounds is common, only a small proportion of cases progress to clinically significant infection.1. Colonization occurs when bacteria adhere to and proliferate at the surgical site. If the host immune response fails to control this process, infection ensues. Although host defenses typically prevent bacterial colonization, these mechanisms can be compromised in certain patients. Surgical trauma initiates an inflammatory cascade, and postoperative immunosuppressive responses may further weaken host immunity, fostering conditions favorable for SSI development.
The prevention of SSIs is a cornerstone of patient safety and surgical quality. SSIs impose substantial clinical and economic burdens, including prolonged hospitalisation, patient distress, disability, and increased mortality. IPC programmes may mitigate these impacts; however, evidence regarding their cost-effectiveness remains limited. Using patient-level data from the Evaluation of Cost of Nosocomial Infection (ECONI) study,2. a Monte Carlo microsimulation model was used to compare enhanced SSI IPC strategies with current practice in coronary artery bypass graft surgery, hip arthroplasty, and caesarean section over 1-month and 1-year time horizons. Overall, enhanced IPC strategies were associated with cost savings and gains in quality-adjusted life years, although their effectiveness varied by surgical procedure and timepoints and was influenced by multiple factors.
Effective IPC measures must be implemented consistently throughout the entire surgical pathway. Over the past decade, several organizations have published comprehensive, evidence-based guidelines for SSI prevention. The World Health Organization (WHO) released its Global Guidelines for the Prevention of Surgical Site Infection in 2016;3,4 in 2017, the Centers for Disease Control and Prevention (CDC) updated their guidelines.5. In the same year, the American College of Surgeons (ACS) and the Surgical Infection Society (SIS) jointly revised their SSI prevention recommendations.6. In 2019, the National Institute for Health and Care Excellence (NICE) published updated online guidance on SSI management,7 and in 2023, a multi-societal collaboration led by the Society for Healthcare Epidemiology of America (SHEA) released new guidelines for SSI prevention.8.
The WHO guidelines, updated in 2018,9. are based on systematic reviews and provide 29 evidence-based recommendations, 13 addressing the preoperative phase and 16 focusing on intraoperative and postoperative care. These recommendations emphasize simple, essential interventions whose adherence is mandatory for all HCWs involved in surgical care. Despite the strong evidence supporting these practices, consistent implementation in daily clinical routines remains a persistent challenge. This is particularly evident in the context of antibiotic prophylaxis.
A recent national Italian study,10. assessing quality indicators of appropriate inpatient antibiotic use through standardized point prevalence surveys conducted in 2016 and 2022, reported that 52.15% of surgical antibiotic prophylaxis courses lasted more than one day, highlighting persistent issues with prolonged prophylaxis despite evidence-based recommendations.
This article proposes a structured framework for continuous quality improvement in IPC. The SIMPIOS framework is an evidence-based, implementation-oriented model for SSI prevention. It translates international guidelines into routine practice through multimodal strategies, multidisciplinary engagement, and a continuous improvement cycle, promoting sustainable behavioral, organizational, and cultural change across the perioperative pathway.
Materials and Methods
A dedicated working group was established by the Italian Multidisciplinary Society for the Prevention of Healthcare-Associated Infections (SIMPIOS) to identify and disseminate the most effective implementation strategies for the prevention of SSIs. To achieve this objective, a narrative review of the relevant literature was conducted using the PubMed, MEDLINE, and Google Scholar databases, limited to English-language publications.
An initial draft document was prepared and circulated among members of the SIMPIOS working group for expert review and consensus development. The project was grounded in the understanding that IPC, although rooted in scientific evidence, requires a multidisciplinary approach that integrates clinical knowledge with a collaborative, safety-oriented culture.
Adopting a narrative review approach, the working group developed a cyclical improvement model.
Developed under the auspices of an Italian scientific society, this document is intended for international adaptation with minimal contextual modifications, taking into account variations in available resources and infrastructure. Although focused on the prevention of SSIs, the conceptual framework and implementation strategies described herein can be readily applied to other HAIs.
Implementing SSI Prevention
The implementation of SSI prevention measures exemplifies the broader challenge of translating evidence-based guidelines into consistent clinical practice. Despite the availability of robust scientific evidence on the determinants of SSIs and the effectiveness of preventive interventions, implementation remains suboptimal.11.
A systematic review by Tomsic et al made a significant contribution to implementation science within IPC, focusing specifically on SSI prevention in abdominal surgery.12. The authors identified 40 eligible studies published up to 2018. The review revealed that a relatively narrow range of implementation interventions dominated the literature. The most frequently reported strategies included: audit and feedback (80% of studies), enhancement of organizational culture (70%), performance monitoring of healthcare delivery (65%), reminders (53%), and educational meetings (45%). Notably, 29 studies (72.5%) adopted a multimodal approach involving three or more concurrent interventions, underscoring the complexity and interdependence of successful implementation efforts.
Similarly, in 2019, Ariyo et al identified a critical gap between evidence and practice, emphasizing that the effective adoption of SSI prevention measures necessitates a deliberate, structured process of change.13. Their systematic review categorized implementation strategies into four domains, collectively referred to as the “Four E’s Model”: (1) engaging the entire team in patient safety; (2) educating staff on evidence-based practices; (3) executing those practices through standardized protocols; and (4) evaluating performance through data collection and feedback mechanisms.
“Engaging” entails the early involvement of all relevant stakeholders – including IPC specialists, surgeons, anesthesiologists, nurses, administrators, and patients – to foster shared ownership and accountability. The identification of local “champions” within surgical teams can further enhance commitment and motivation.
“Educating” refers to the continuous process of equipping HCWs with the necessary knowledge, skills, and attitudes to apply best practices effectively. Educational initiatives should extend beyond traditional didactic teaching to include interactive learning methods, reinforced over time and adapted to evolving evidence and workflows.
“Executing” encompasses the operational dimension of implementation, involving the systematic application of preventive measures across the preoperative, intraoperative, and postoperative phases. Effective execution depends on both individual compliance and system-level reliability, ensuring that preventive measures are embedded into routine clinical practice.
“Evaluating” highlights the cyclical nature of the implementation process. Evaluation involves systematic surveillance of adherence to local protocols, monitoring SSI rates, and providing structured feedback to HCWs and institutional leadership. Audit and feedback mechanisms are essential for identifying performance gaps, recognizing progress, and adjusting strategies in real time. Evaluation transforms implementation from a static intervention into a dynamic process of continuous quality improvement.
Together, these four domains underscore that implementation is not a linear transfer of knowledge but a complex adaptive process influenced by context, behavior, and organizational culture. This approach aligns closely with the principles of implementation science, emphasizing that sustainable change arises from the integration of evidence into local systems through participatory and iterative methods.
The importance of process-oriented implementation is also underscored in the 2018 WHO Implementation Manual, which operationalizes the Global Guidelines for SSI Prevention into a practical roadmap for healthcare teams.14. The manual emphasizes that global recommendations are effective only when adapted to local contexts and embedded within strategies that address human behavior, communication, and organizational dynamics. The WHO advocates a five-step improvement cycle to conceptualize IPC implementation as a continuous and iterative process: (1) preparing for action; (2) assessing the baseline; (3) developing and executing an action plan; (4) evaluating impact; and (5) sustaining change.
These steps are inherently iterative, encouraging healthcare institutions to view IPC not as a one-time initiative but as a process of ongoing refinement and learning. Building on this foundation, the SIMPIOS working group proposes a gradual, cyclical approach to the implementation of SSI prevention based on the WHO’s continuous improvement model.15. This framework enables healthcare teams to progressively strengthen IPC practices over time, fostering sustainable improvement in SSI prevention and reinforcing a culture of patient safety and organizational resilience (Figure 2).
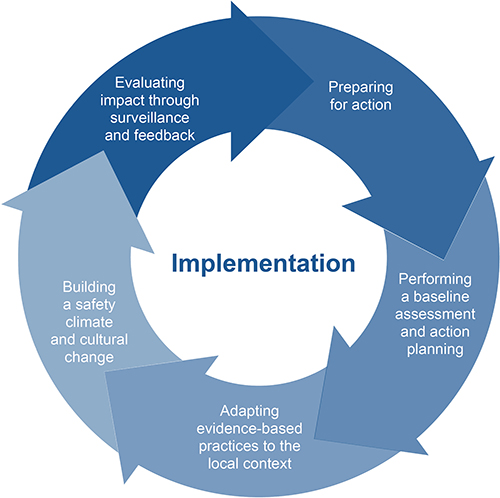 |
Figure 2 Continuous implementation of Surgical Site Infections prevention (SIMPIOS model). |
Preparing for Action
The first phase underscores the fundamental importance of governance in IPC. Every healthcare facility, regardless of size, resources, or setting, should maintain a robust IPC program characterized by clear leadership, defined accountability, and institutional support. A meta-analysis published in 2018 demonstrated that multimodal and system-level IPC interventions can reduce HAIs, including SSIs, by up to 55%, even in resource-limited contexts.16.
IPC programs extend beyond the implementation of clinical protocols; they require the explicit prioritization of IPC by hospital leadership, including the allocation of adequate resources and the integration of IPC objectives into the broader patient safety and quality improvement agenda.17,18. Effective programs should establish clear, measurable goals aligned with local epidemiological priorities and risk profiles.
Functioning IPC teams play a pivotal role in coordinating education and training, developing and updating evidence-based protocols, monitoring clinical practice, and fostering interdisciplinary collaboration. To perform these functions effectively, IPC teams must include dedicated and trained professionals in every acute care facility. Importantly, IPC should not be viewed as the exclusive domain of infection control specialists. Instead, frontline HCWs – including surgeons, anaesthetists, nurses, and operating room staff – should be actively engaged, as their day-to-day practice directly influences SSI risk.19.
Adequate resource allocation is critical to enable IPC teams to function effectively. Essential components include sufficient financial support for surveillance systems, staffing for education and auditing activities, timely access to laboratory and diagnostic services, and appropriate digital infrastructure for data collection, analysis, and feedback. However, institutional commitment must extend beyond mere financial investment. Sustained success depends on visible leadership support, well-defined governance structures, and the integration of IPC objectives within the organization’s overarching quality-of-care and patient safety framework. The WHO IPC guidelines emphasize that resource allocation should be proportionate to each facility’s risk profile, patient volume, and service complexity, ensuring that IPC measures are sustainable and responsive to local realities.20.
The success of an IPC program also heavily relies on cultivating a culture of shared responsibility. Preventing HAIs is a collective duty that involves every HCW. By promoting continuous education, audit and feedback mechanisms, and visible leadership engagement, IPC teams can catalyze behavioral change across clinical departments. Such initiatives foster adherence to core preventive measures – including hand hygiene, antimicrobial stewardship, aseptic technique, and environmental cleaning – thereby embedding IPC into everyday clinical practice.
To align with the continuous improvement cycle, IPC teams should conduct regular performance assessments against key indicators, identify implementation gaps, and adjust interventions accordingly. This iterative approach transforms IPC from a reactive model into a proactive system-driven process.
Performing a Baseline Assessment and Action Planning
Once the pillars of governance are firmly established, the second phase—performing a baseline assessment and action planning—becomes essential. A baseline assessment provides the foundation for measuring IPC performance and identifying priority areas for intervention. It enables healthcare institutions to objectively evaluate existing practices, detect gaps in implementation, and compare current performance against established evidence-based standards. Importantly, such assessments can foster a sense of urgency and collective responsibility by highlighting discrepancies between current practices and best available evidence.
To evaluate the current state of IPC practices and their outcomes in Italian healthcare facilities, six years after the launch of the National Plan for the Control of Antibiotic Resistance (PNCAR), a baseline evaluation of IPC in Italian hospitals was recently conducted.21. The study provides a multicentre, cross-sectional survey of 38 acute care hospitals in Italy during 2023 to assess the state of IPC practices using a questionnaire adapted from the WHO IPC Assessment Framework and national guidelines. The survey revealed that over a quarter of hospitals lacked defined annual IPC programmes, and more than a third did not have an antimicrobial stewardship task force. Key IPC activities—such as regular microbiology reporting, monitoring of alcohol-based hand rub use, and structured surveillance systems—were inconsistently implemented, with fewer than half of facilities engaged in active hand hygiene or isolation compliance monitoring. Surveillance systems for healthcare-associated infections were present in under 20% of hospitals, and only 42% had defined IPC budget goals. The assessment highlighted significant gaps and regional variability in IPC implementation, identifying priority areas for targeted interventions and informing future, tailored IPC improvement strategies.
Healthcare facilities lacking comprehensive or proactive IPC programs should begin by conducting a systematic gap analysis or a point-prevalence survey to identify deficiencies in practice, infrastructure, or compliance. The results of this diagnostic phase form the basis for developing a targeted action plan grounded in a multimodal improvement strategy.
The WHO strongly recommends that all IPC interventions be implemented within a multimodal framework.15. The term multimodal strategy refers to the coordinated use of multiple, synergistic approaches that—when applied together—can more effectively influence HCWs’ behavior, improve patient outcomes, and promote a sustained transformation in institutional safety culture.
A growing body of evidence supports the superiority of multimodal approaches over isolated interventions. Studies consistently demonstrate that multimodal strategies significantly enhance hand hygiene compliance and reduce infection rates more effectively than single-component programs.22,23.
According to WHO guidance, the multimodal improvement strategy comprises five essential components24. (Figure 3). Together, these components create a structured and evidence-based framework for action planning that integrates behavioral, organizational, and technical dimensions of IPC. When applied systematically, they facilitate measurable and sustainable improvements in compliance, performance, and patient outcomes.
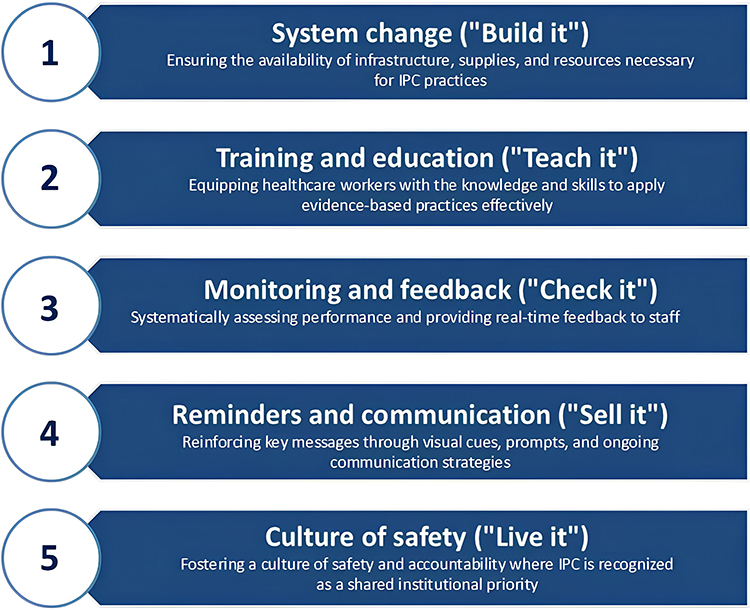 |
Figure 3 The five essential components of the World Health Organization multimodal improvement (adapted from: WHO. A guide to the implementation of the WHO multimodal hand hygiene improvement strategy. Geneve. 2009).24 |
In 2018, Allegranzi et al published a before-and-after cohort study, evaluating the effectiveness of a multimodal strategy to reduce SSI rate across 5 African hospitals, in settings with varying resource levels.25. Four hospitals completed the baseline and follow-up, and three provided suitable data for the sustainability period. In total, 4322 surgical procedures were monitored. The cumulative incidence of SSIs declined significantly after the intervention, from 8.0% (95% CI 6.8–9.5) to 3.8% (3.0–4.8; p<0.0001), and this reduction was maintained during the sustainability phase (3.9%, 2.8–5.4). Compliance with IPC measures improved in both the follow-up and sustainability phases. The likelihood of SSIs during follow-up was significantly lower than in the pre-intervention phase (odds ratio [OR] 0.40, 95% CI 0.29–0.54; p<0.0001), even if the likelihood of death was not significantly reduced (0.72, 0.42–1.24; p=0.2360). The data demonstrated that IPC interventions can be successfully implemented in hospital settings across the African continent. The results from all fields of perioperative IPC were improved. Implementation in tested hospitals significantly reduces the general risk of SSIs. However, the increase was not uniform for all hospitals, and careful examination is recommended.
A study on SSI prevalence before and after the implementation of a multimodal infection control programme was conducted at a large teaching hospital in Italy, to evaluate whether a structured infection control intervention could reduce the burden of SSIs.26. The study employed four one-day point prevalence surveys, conducted in accordance with the HELICS (Hospitals in Europe Link for Infection Control through Surveillance) protocol, to measure SSI rates before and after the intervention. The intervention comprised a multifaceted campaign to improve compliance with antibiotic prophylaxis guidelines, alongside active engagement of surgeons and infection control staff. A total of 600 surgical patients were enrolled. The results showed a significant reduction in SSI prevalence, with rates decreasing from 16.4 to 8.2 per 100 patients following the programme (P = 0.018). Multivariate analysis identified age over 31 years, kidney insufficiency, and infection at admission as significant risk factors for SSI. The study demonstrated that repeated prevalence surveys coupled with multimodal infection control efforts are feasible and can effectively decrease SSI rates in hospital settings.
Adapting Evidence-Based Practices to the Local Context
The third phase of implementation refers to the organizational, and cultural context. While international and national guidelines for SSI prevention provide a robust foundation, their successful adoption depends on contextualization to local workflows, resources, and institutional norms. In recent years, multiple high-quality guidelines for SSI prevention have been published.3–9. Despite the availability of strong evidence and well-established recommendations, adherence in clinical practice remains suboptimal, underscoring the persistent gap between evidence and implementation.
To explore this issue, a qualitative study was conducted in Spain in 2020 using a web-based survey distributed to members of the Association of Perioperative Nurses and ten national surgical associations representing a range of specialties.27. The aim was to capture perspectives from a broad spectrum of healthcare professionals involved in surgical care. Among the 1105 respondents, 50.5% reported that they did not receive feedback on their SSI rates. Overall awareness of key SSI prevention recommendations—including avoidance of routine hair removal, preference for hair removal with a clipper, and use of alcohol-based skin. The antiseptic solutions most frequently used by surgeons were alcohol-based chlorhexidine (57.2%) and aqueous povidone-iodine (23.3%). In 62.8% of cases, respondents allowed the antiseptic to air dry before placing surgical drapes. Adhesive drapes were routinely applied in 33.4% of procedures. Implementation of perioperative measures varied: normothermia was maintained in 84.3% of cases, and glucose control in 65.9%. Advanced preventive techniques were used inconsistently, with antimicrobial sutures employed by 20.2% of teams and incisional negative pressure wound therapy by 43.5%. Before wound closure, 83.9% of respondents reported changing surgical instruments either selectively or routinely, and wound irrigation—primarily with saline—was performed in 78.1% of cases. When asked about strategies to improve adherence to SSI prevention guidelines, participants rated checklists, standardized order sets, active surveillance, performance feedback, and educational programs as most effective. However, these interventions were rarely implemented in their institutions.
Local Protocols
Evidence-based guidelines establish a scientific foundation for best practices; however, they cannot be applied effectively without local adaptation. Contextualization requires a delicate balance between rigor and flexibility – rigor ensures that adaptation preserves the integrity of the underlying evidence, while flexibility promotes feasibility, ownership, and sustainability among HCWs.
The development of locally tailored protocols, involving clinicians, nurses, and IPC specialists, is essential for translating recommendations into actionable procedures aligned with available resources and responsibilities.25. Such locally endorsed documents facilitate acceptance, promote accountability, and enhance adherence.
Bundles
Among the most effective tools for contextualizing and operationalizing guidelines there are care bundles and checklists, both of which convert complex recommendations into structured interventions that can be systematically applied in daily practice.
Bundles are concise sets, typically three to five, of evidence-based practices that, when performed collectively and consistently, yield better clinical outcomes than when implemented individually. The effectiveness of bundles lies in their simplicity, clarity, and their “all-or-nothing” approach, which promotes full compliance with all components. When integrated into broader multimodal improvement strategies, bundles serve as powerful instruments for behavioral and cultural change.
The rationale for SSI prevention bundles is based on the multifactorial nature of SSI risk, which encompasses patient-related, cultural, organizational, and environmental factors. Since no single measure can prevent SSIs in isolation, bundling ensures that critical interventions are applied concurrently and systematically, maximizing their synergistic effects.
Typical measures included in SSI prevention bundles address all phases of surgical care:28.
- Preoperative skin preparation: Ensuring that the patient has taken a shower – or, when necessary, performing bedside hygiene – on the day before or the day of surgery using soap or a liquid cleanser.
- Hair removal: Avoiding hair removal unless strictly necessary; when required, using electric clippers instead of razors.
- Antibiotic prophylaxis:
- Administering the antibiotic within 120 minutes before incision (within 60 minutes for most cephalosporins).
- Re-administering for prolonged procedures or significant intraoperative blood loss.
- Discontinuing prophylaxis promptly after surgery;
- Surgical site antisepsis: Using alcohol-based antiseptic solutions for skin preparation.
- Glycemic control: Maintaining intraoperative blood glucose below 200 mg/dL.
- Normothermia: Maintaining perioperative core temperature ≥36°C.
In 2021, Wolfhagen et al published a meta-analysis providing a rigorous synthesis of evidence regarding the effectiveness of perioperative care bundles in SSI prevention.28. While prior reviews demonstrated a reduction in SSI rates associated with bundle implementation, many were limited by methodological heterogeneity, small sample sizes, and uncontrolled before-and-after study designs.29–31. To address these issues, Wolfhagen et al combined interrupted time-series (ITS) analyses and randomized controlled trials (RCTs), yielding a more precise estimate of bundle effectiveness.
The meta-analysis confirmed that perioperative care bundles are effective in reducing SSIs, although results from RCTs were somewhat inconsistent. Notably, there was no linear relationship between the number of bundle components and SSI reduction and bundles containing a higher proportion of evidence-based measures were more effective than those with more but less-supported elements. The authors concluded that bundles represent an effective strategy for SSI prevention, provided they are implemented within frameworks that ensure contextual adaptation, staff engagement, and compliance monitoring.
In 2024, the Italian National Health Institute (Istituto Superiore di Sanità, ISS), in collaboration with SIMPIOS, issued a national SSI prevention bundle to facilitate the active implementation of evidence-based measures in surgical settings.32. The initiative was designed to address persistent gaps in compliance with recommended preventive measures in Italy. The bundle targets all HCWs directly involved in perioperative care, including surgeons, anaesthesiologists, operating room personnel, and IPC team members. It also aims to inform and engage patients as active participants in SSI prevention. To identify interventions supported by robust scientific evidence, the ISS conducted a systematic review of international and national guidelines on SSI prevention published between 2009 and 2023. Each guideline was appraised using the AGREE (Advancing Guideline Development, Reporting and Evaluation in Health Care) protocol, ensuring methodological rigor and quality. The resulting core bundle includes five evidence-based measures strongly recommended across all major international guidelines. These interventions represent the essential standards that must be consistently applied in all surgical settings to ensure high-quality, safe care (Figure 4).
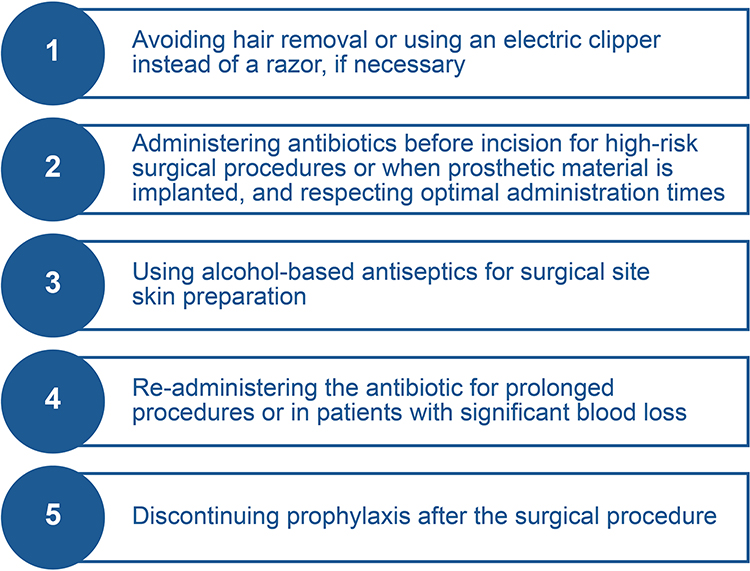 |
Figure 4 Italian National Health Institute and SIMPIOS care bundle for the prevention of surgical site infections (adapted from: Moro ML et al. Bundle for the prevention of surgical site infections. Italian National Health Institute, Rome. 2025).32 |
Beyond the five core measures identified as universally recommended across international guidelines, a second set of supplementary measures has been proposed. The strength of recommendations for these additional interventions varies across guidelines; nonetheless, each is supported by scientific evidence and endorsed by one or more authoritative sources. These measures can further reduce SSI risk and are particularly relevant in institutions where the implementation of the core bundle elements has already been successfully achieved.
In such settings, hospitals are encouraged to progressively adopt these additional evidence-based measures, ensuring that multidisciplinary implementation strategies and systematic monitoring of adherence by surgical teams support their integration.
Importantly, hand hygiene – both within the operating room and in perioperative wards – has been explicitly included among these supplementary measures. Although hand hygiene constitutes a core infection prevention practice, its inclusion in local SSI bundles remains appropriate in contexts where adherence remains suboptimal.30
Checklists
A checklist is a structured tool that guides HCWs through key procedural steps to enhance patient safety and reduce preventable errors.15 Among these, the WHO Surgical Safety Checklist represents one of the most transformative interventions in the history of perioperative safety. Introduced in 2008 as part of the WHO’s “Safe Surgery Saves Lives” initiative, the checklist aims to improve consistency, communication, and adherence to evidence-based standards across all stages of the surgical pathway – from anesthesia induction to postoperative recovery.33.
The WHO Surgical Safety Checklist is organized into three critical steps: (1) “Sign In” – conducted before induction of anesthesia; (2) “Time Out” – performed before the skin incision; and (3) “Sign Out” – completed before the patient exits the operating room.
These checkpoints directly address several determinants of SSI risk, including the timing and appropriateness of antimicrobial prophylaxis, surgical hand hygiene, control of the operating room environment, and team communication during critical procedural moments.
Multiple studies have demonstrated that appropriate and consistent use of the WHO checklist is associated with significant reductions in SSI rates and overall surgical morbidity.34,35. Beyond its technical contributions, the checklist functions as a team coordination, communication, and accountability mechanism fostering a culture of openness among surgeons, anesthesiologists, nurses, and support staff. In this way, it bridges the gap between procedural compliance and the broader cultural dimensions of patient safety. However, the effectiveness of the checklist depends critically on the quality of its implementation. When adopted superficially or treated as a bureaucratic exercise, the checklist loses its capacity to facilitate meaningful behavioral change and may have limited impact on infection rates. Therefore, hospitals should ensure that checklist implementation is interactive, team-based, and regularly reinforced through education, leadership engagement, and feedback mechanisms.
In 2021, de Almeida et al published a case–control study36. evaluating the effectiveness of a surgical safety checklist in improving surgical outcomes. Surgical outcomes before and after checklist implementation were compared, with particular attention to adherence to perioperative safety practices, including antibiotic prophylaxis. The results demonstrated a significant reduction in surgical site infection rates following checklist adoption, alongside improved compliance with recommended antibiotic use. Checklist implementation was also associated with reduced antibiotic consumption, thereby lowering selective pressure for antimicrobial resistance. Consequently, hospital costs related to antibiotic use and postoperative complications decreased. Mortality rates showed a downward trend, indicating improved overall patient safety. These findings support the surgical safety checklist as a low-cost, effective intervention that enhances surgical quality, strengthens antimicrobial stewardship, and reduces preventable adverse outcomes, reinforcing the value of standardized safety tools in improving both clinical and economic outcomes in surgical care.
Posters and Visual Reminders
Educational posters and visual reminders represent additional tools that can play an important role in the implementation of IPC measures as part of a multimodal improvement strategy. Visual communication not only conveys key information but and day-to-day clinical practice15. also serves to reinforce behavioral norms, bridging the gap between formal training.
Strategically placed posters – particularly in high-traffic or high-risk areas such as operating theatres, scrub zones, or staff rest areas – provide continuous cues that promote adherence to evidence-based IPC practices, notably hand hygiene. Effective posters should be clear, visually appealing, and concise, using simple language, pictograms, and colour cues to facilitate comprehension and recall. Messages should emphasize essential preventive behaviors, such as the “Five Moments for Hand Hygiene”, as well as key perioperative measures like the correct administration of antimicrobial prophylaxis.
Nonetheless, posters alone are insufficient to drive sustained behavioral change. Their effectiveness is maximized when integrated into a comprehensive communication and training strategy supported by leadership engagement, continuous feedback, and monitoring. Moreover, the relevance and impact of posters can diminish over time; thus, they should be periodically reviewed, updated, and aligned with current evidence and institutional priorities.
Within the SIMPIOS framework, and in alignment with the WHO’s continuous improvement model, visual communication materials such as posters serve as visible symbols of organizational commitment to patient safety and infection prevention. When combined with active education, supervision, and a strong safety culture, they contribute to embedding IPC principles into the daily routines of healthcare personnel. In this way, visual reminders evolve from simple educational tools into tangible expressions of institutional values, professionalism, and accountability in the prevention of healthcare-associated infections.
Building a Safety Climate and Cultural Change
The fourth phase of implementation is often the most challenging. HCWs must be adequately prepared to navigate complex systems while safeguarding the best interests of patients. Although individual competence and training are essential, the successful application of IPC measures depends largely on organizational culture and systemic engagement. In many healthcare settings, the implementation of IPC and patient safety initiatives is hindered by structural barriers such as limited resources, competing clinical demands, and entrenched hierarchies. Moreover, IPC is frequently perceived as peripheral to direct clinical responsibilities, leading to persistently suboptimal adherence across institutions worldwide.
IPC measures cannot achieve their full potential in environments characterized by a hostile or indifferent organizational culture. A robust culture of safety requires that IPC be recognized as an integral component of patient care, not as an administrative or external requirement. Education represents a cornerstone of this process: it should begin during undergraduate training and continue throughout clinical practice. However, knowledge alone rarely changes behavior; HCWs must be convinced of the personal and professional relevance of IPC and supported by a work environment that enables and values adherence.
To investigate whether safety climate level and safety climate strength are associated with operating room personnel’s commitment to subjective norms toward, and knowledge about SSI prevention measures, in 2023, Pfeiffer et al published the results of a survey.37. Operating room staff from hospitals participating in the Swiss SSI surveillance program were invited to complete a survey, achieving a 38% response rate. A total of 2769 responses from 54 hospitals were included in the analysis. Two adjusted regression analyses were conducted to assess how aspects of the safety climate relate to operating room staff’s perspectives and actions concerning surgical site infection prevention. The models examined the influence of safety climate level and safety climate consistency on three key factors: willingness to adhere to preventive practices under pressure, perceived expectations from colleagues, and understanding of SSI prevention methods. Professional background and hospital-level response numbers were included as control variables. The analysis revealed that higher safety climate levels were significantly associated with stronger commitment to prevention activities and greater perceived social expectations to comply with preventive measures (P < 0.05). However, no significant association was observed between safety climate level and knowledge of preventive strategies. Additionally, safety climate consistency did not show a significant relationship with any of the outcomes studied. These findings indicate that motivation and shared expectations among surgical teams contribute more to a positive safety climate than knowledge alone, although assessing knowledge remains valuable for guiding focused SSI prevention interventions.
SSI prevention extends beyond technical compliance with guidelines. It depends fundamentally on the safety culture and organizational climate within which surgical care is delivered. Hospitals that demonstrate strong safety cultures, characterized by open communication, effective teamwork, leadership engagement, and shared accountability, consistently achieve lower rates of HAIs, including SSIs. Establishing such a culture requires not only procedural adherence but also a transformative shift in attitudes, behaviors, and institutional priorities.
In a 2019 review, van Buijtene et al analyzed 20 studies exploring the relationship between organizational culture and HAI outcomes.38. Although methodological limitations precluded high-quality evidence ratings, the synthesis of quantitative and qualitative research identified eight key characteristics of hospitals with lower HAI rates: (1) a strong and explicit safety culture; (2) generative and engaged leadership; (3) willingness to embrace innovation; (4) adaptation of interventions to local contexts; (5) a long-term strategic perspective; (6) engagement and empowerment of healthcare professionals; (7) open communication and interprofessional collaboration; and (8) a transparent, non-punitive climate that promotes learning.
A 2022 qualitative study involving ten surgeons at a US academic medical center further highlighted the role of mental models in shaping compliance with multifaceted SSI prevention bundles.39. The study revealed that many surgeons considered some SSIs to be inevitable, thereby diminishing motivation to follow IPC protocols. Adherence was stronger for interventions perceived as clinically relevant or endorsed by respected peers, whereas measures viewed as externally imposed were often disregarded. The findings underscored the importance of intrinsic motivation, such as professional pride and commitment to surgical excellence, over extrinsic incentives like financial rewards.
In many surgical environments, IPC continues to be regarded as the sole responsibility of specialized IPC teams, rather than a shared clinical duty among all HCWs. This limited perception undermines compliance and sustainability. For lasting SSI prevention, responsibility must shift from individual compliance to collective ownership of infection outcomes. Successful institutions cultivate a sense of shared purpose among surgeons, anesthesiologists, nurses, and IPC specialists, embedding SSI prevention within the broader framework of surgical quality and patient safety.12.
Leadership commitment remains the cornerstone of cultural transformation. Hospital leaders should visibly prioritize IPC through adequate resource allocation, surveillance support, and recognition of improvement efforts. When senior management models safety-oriented behavior and treats SSI prevention as a core organizational value, frontline staff are more likely to internalize these principles. Leadership thus serves not only an administrative role but also acts as a cultural signal, defining institutional norms and expectations.12.
Equally important is effective communication across professional hierarchies. Surgical environments are often characterized by rigid structures, which can discourage junior staff from questioning aseptic lapses or addressing protocol deviations. Teams that promote psychological safety, open dialogue, and mutual respect are better positioned to identify and correct IPC breaches in real time.
While education alone does not change culture, continuous, context-specific training within a supportive environment can reinforce professional accountability. Programs that link IPC performance to patient outcomes and engage HCWs in analyzing their own compliance data have been shown to improve adherence to preventive bundles and checklists. Empowering nurses, anesthesiologists, and operating room technicians to take an active role in maintaining aseptic standards fosters bottom-up ownership of IPC and sustains behavioral change.
A particularly effective strategy involves identifying a local opinion leader, often referred to as a “surgeon champion”, within the surgical department. This individual acts as an internal advocate for evidence-based practice, bridging the gap between clinical teams and institutional policy.40.
When implemented collaboratively with the IPC team, this approach enhances cohesion, fosters behavioral change, and strengthens the culture of patient safety.
The effectiveness of the champion model lies in its peer-driven nature – behavioral change in clinical settings is more sustainable when driven by respected colleagues rather than by external mandates.
Finally, the active involvement of patients in their own care has emerged as a vital component of modern patient safety strategies. In the context of SSI prevention, engaging patients as informed partners encourages shared responsibility and promotes adherence to IPC measures.41. Practical interventions – such as providing preoperative education, involving patients in wound care, and encouraging communication about concerns – can enhance compliance and improve outcomes. Although the Italian healthcare context remains influenced by traditional paternalistic models of doctor–patient relationships, increasing emphasis on patient engagement represents a promising avenue for strengthening IPC and fostering a more collaborative safety culture.
Evaluating Impact Through Surveillance and Feedback
The final phase of the continuous improvement cycle is critical to ensuring the effectiveness and sustainability of IPC interventions. Surveillance provides the empirical foundation for assessing whether implemented measures are achieving their intended outcomes, while feedback mechanisms ensure that data are translated into actionable improvements.42.
Standardized surveillance systems, such as those promoted by the European Centre for Disease Prevention and Control (ECDC), enable hospitals to benchmark their performance, share data, and monitor progress over time. The ECDC’s 2025 “Protocol for the Surveillance of Surgical Site Infections and Prevention Indicators” (version 2.3),43. developed under the Healthcare-Associated Infections Surveillance Network (HAI-Net), offers a unified framework for SSI monitoring across Europe. The protocol emphasizes that surveillance is not merely a data collection exercise but a continuous quality improvement process, providing structured methods for case identification, classification, and follow-up. SSIs are categorized according to standardized definitions—superficial incisional, deep incisional, and organ/space infections—with explicit diagnostic criteria. The document also delineates which surgical procedures require routine monitoring and specifies appropriate follow-up periods to ensure consistency and comparability across institutions.
Recent innovations are transforming how surveillance is conducted. In 2023, Denkel et al published a forward-looking analysis exploring how automation and digital innovation can revolutionize SSI surveillance within Europe.44. Conducted within the PRAISE (Providing a Roadmap for Automated Infection Surveillance in Europe) network, the study identified the key design elements for future automated systems. Traditional SSI surveillance remains labor-intensive, heavily reliant on manual chart reviews, and vulnerable to variability in interpretation – all factors that constrain scalability and delay feedback to clinical teams. Automated surveillance, leveraging routinely collected electronic health record (EHR) data, microbiological results, and administrative information, has the potential to enhance accuracy, timeliness, and sustainability.
The PRAISE network identified several key domains for successful implementation of automated SSI surveillance:
- Providing a clear mandate from higher management levels.
- Providing sufficient resources for information technology support to assure successful implementation, but also maintenance and sustainability of automated surveillance systems of SSIs.
- Providing permanent resources for project management and intersection teams for automated surveillance systems of SSIs.
- Supporting databases that allow interoperability and are compatible between hospitals, regions, and, if possible, even countries throughout Europe.
Properly validated automated systems can enable real-time SSI detection, facilitate large-scale benchmarking, and support comparative analyses across healthcare systems. However, automation should complement, not replace, human expertise. IPC specialists remain indispensable for case validation, contextual interpretation, and the translation of surveillance findings into clinical action. A major challenge identified by Denkel et al concerns data standardization: heterogeneity in data formats, inconsistent access to microbiological results, and variable SSI definitions continue to limit inter-institutional comparability.43 When integrated into a structured governance framework, automated surveillance represents the future direction of IPC. Its success depends on multidisciplinary collaboration among clinicians, IPC professionals, data scientists, and policymakers, ensuring that technological innovation serves the overarching goal of patient safety.
Audit and feedback mechanisms are essential complements to surveillance. When directed toward both frontline HCWs and institutional leadership, feedback provides clarity on performance gaps and fosters accountability.45. Quality indicators, including structural, process-oriented, or outcome-based, serve as benchmarks for evaluating progress and guiding continuous improvement.
A 2021 study by Manivannan et al offers a clear demonstration of how sustained surveillance and structured feedback can drive measurable improvement in SSI prevention.46. Conducted within a high-volume surgical center, the implementation program engaged IPC specialists, surgeons, anesthesiologists, and nurses in iterative performance review and corrective action cycles. Importantly, the process was non-punitive, fostering a learning-oriented environment that promoted collective ownership of outcomes. Over the course of implementation, SSI rates significantly declined – approaching near-zero levels in several surgical specialties. These improvements were not the result of a single intervention but rather of consistent adherence to evidence-based practices reinforced by feedback-driven behavioral change. The findings underscore that when clinical teams are provided with accurate, timely data and actively participate in interpreting and responding to it, sustainable gains in patient safety can be achieved.
Crucially, the evaluation phase should never represent an endpoint. Instead, it serves as a feedback loop that informs ongoing reassessment, adaptation, and renewal of preventive strategies. As new evidence emerges and local contexts evolve, IPC programs must re-evaluate priorities and restart the cycle of continuous improvement – thereby maintaining alignment with the principles of implementation science and organizational learning.
Finally, a 2023 review by Rosa et al emphasized the importance of integrating SSI prevention within a continuum-of-care perspective that spans the preoperative, intraoperative, and postoperative phases.47. Rather than focusing solely on the identification of discrete clinical measures, the authors advocate for systematic, consistent, and sustainable implementation across the entire surgical pathway. This holistic approach reflects the principles of the multimodal improvement model, recognizing that surgical IPC is inherently multidisciplinary and dependent on the coordination of surgeons, anesthesiologists, nurses, IPC specialists, and hospital administrators. Such integration ensures that SSI prevention remains a dynamic, learning-oriented process, grounded in evidence and sustained through continuous monitoring, evaluation, and feedback (Figure 5).
 |
Figure 5 Multidisciplinarity in Infection Prevention and Control. |
Evaluation Strategies and Metrics for Success in the SIMPIOS Framework for SSI Prevention
The SIMPIOS framework for SSI prevention highlights evaluation as an integral, continuous, and iterative process rather than a standalone activity. Its strategy encompasses outcome, process, and organizational metrics, providing a multidimensional assessment of clinical effectiveness and institutional performance. Outcome measures focus on SSI incidence—superficial, deep, and organ/space infections—alongside related endpoints such as postoperative complications, readmission rates, length of hospital stay, and mortality, offering a direct reflection of patient-centered impact.
Process metrics monitor adherence to evidence-based preventive practices across the perioperative pathway, including timely antibiotic prophylaxis (timing and duration), maintenance of normothermia, perioperative glycemic control, surgical site antisepsis, hair removal techniques, and consistent use of the WHO Surgical Safety Checklist. Such monitoring identifies gaps in compliance and informs targeted interventions.
Organizational and behavioral metrics evaluate institutional engagement, considering factors such as safety culture strength, team communication, leadership commitment, training participation, and the influence of local “surgeon champions” in driving protocol adherence. Multimodal strategies, including visual reminders and educational initiatives, are assessed for their effectiveness in reinforcing desired behaviors.
Audit and feedback mechanisms form a cornerstone of the evaluation process, translating surveillance data into actionable insights for both frontline staff and leadership. This continuous feedback fosters accountability, iterative learning, and timely corrective action. By integrating these indicators within a continuous improvement framework, SIMPIOS ensures that success extends beyond reductions in SSI rates to encompass lasting behavioral, procedural, and cultural change, embedding IPC into routine practice and strengthening institutional resilience.
The HAI-Net SSI protocol,43. recently published by the ECDC, defines structure and process indicators (SPIs) to monitor adherence to evidence-based practices for SSI prevention. SPIs were selected based on the strength of available evidence and the feasibility of data collection. Data collection is recommended for a minimum of three months or 30 surgical procedures of each selected type per surveillance year. Two SPIs are collected at the hospital/unit level, while others are aggregated by surgical procedure type.
Hospital/unit-level SPIs include:
- Alcohol handrub (AHR) consumption per 1000 patient-days in surgical wards participating in SSI surveillance, reflecting hand hygiene infrastructure and usage.
- Existence of a root cause analysis system for SSIs, including circumstances triggering the review, to support continuous quality improvement.
SPIs aggregated by operation type are grouped into three categories:
- Perioperative Antibiotic Prophylaxis
- Administration within 60 minutes before incision (except vancomycin/fluoroquinolones).
- Discontinuation within 24 hours of surgery initiation.
- Preoperative Skin Preparation
- No hair removal, or clipping only if necessary.
- Use of alcohol-based antiseptic solutions containing chlorhexidine gluconate in the operating room, if no contraindication exists.
- Other SSI Prevention Indicators
- Maintenance of normothermia during the perioperative period (36–38°C rectal, 35.5–37.5°C non-rectal).
- Use of a protocol for intensive perioperative blood glucose control in adult patients, with monitoring intra- and postoperatively.
SPIs provide actionable metrics to evaluate hospital readiness, compliance with preventive measures, and opportunities for quality improvement, aligning with WHO9. and SHEA8. recommendations for SSI prevention.
Conclusion
The SIMPIOS framework is a comprehensive, evidence-based approach to SSI prevention that views implementation as a continuous and adaptive process rather than a single intervention. It is grounded in international guidelines and implementation science principles, translating scientific evidence into routine clinical practice through structured, multimodal strategies.
A defining characteristic of the SIMPIOS framework is its cyclical improvement model, derived from the WHO implementation approach. Prevention activities are organized into iterative phases—preparation, baseline assessment, action planning, implementation, evaluation, and sustainability—allowing institutions to progressively refine practices over time. This structure emphasizes learning, feedback, and adaptation rather than linear compliance.
SIMPIOS places strong emphasis on governance and leadership, recognizing that effective SSI prevention depends on institutional commitment, clear accountability, and adequate resource allocation. Infection prevention and control is embedded within broader quality and patient safety strategies, supported by trained IPC teams and engaged hospital management.
Another core feature is the use of multimodal interventions. The SIMPIOS framework integrates education, standardized protocols, care bundles, checklists, surveillance, audit and feedback, and visual reminders to address behavioral, organizational, and technical determinants of infection risk simultaneously. This multimodality reflects the multifactorial nature of SSIs and enhances the likelihood of sustainable change.
Contextual adaptation is central to the framework. While grounded in robust evidence, the SIMPIOS framework promotes the development of locally tailored protocols and bundles that align with available resources, workflows, and cultural norms. This balance between scientific rigor and practical feasibility fosters ownership among healthcare workers and improves adherence.
The framework is inherently multidisciplinary, actively involving surgeons, anesthesiologists, nurses, operating room staff, IPC specialists, leadership, and patients. By promoting shared responsibility and the identification of local clinical champions, SIMPIOS strengthens collaboration and accountability across professional boundaries.
Evaluation is treated as a continuous process rather than an endpoint. Through standardized surveillance, process and outcome indicators, and structured audit and feedback, SIMPIOS ensures that performance data inform real-time improvement and strategic decision-making. This feedback loop supports sustained reductions in SSI rates and ongoing quality improvement.
Finally, the SIMPIOS framework explicitly addresses safety culture and behavioral change. It recognizes that lasting improvements in SSI prevention depend on psychological safety, open communication, leadership role modeling, and intrinsic professional motivation. By embedding IPC into everyday practice and organizational values, the framework promotes durable improvements in patient safety and institutional resilience.
Acknowledgments
The authors used ChatGPT (OpenAI in San Francisco, CA, USA) for language editing of the manuscript. All content generated by ChatGPT was reviewed, verified, and validated by the authors to ensure accuracy, clarity, and adherence to scientific standards.
The authors thank Alice Pietrella for technical support in preparing and refining the figures for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sartelli M, Guirao X, Hardcastle TC, et al. 2018 WSES/SIS-E consensus conference: recommendations for the management of skin and soft-tissue infections. World J Emerg Surg. 2018;13:58. doi:10.1186/s13017-018-0219-9
2. McFarland A, Manoukian S, Mason H, Reilly J. A cost-utility analysis of surgical site infection prevention: broadening the scope. Appl Health Econ Health Policy. 2025. doi:10.1007/s40258-025-01015-1
3. WHO Guidelines Development Group; Allegranzi B, Zayed B, Bischoff P, et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e288–18. doi:10.1016/S1473-3099(16)30402-9
4. WHO Guidelines Development Group; Allegranzi B, Bischoff P, de Jonge S, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e276–e287. doi:10.1016/S1473-3099(16)30398-X
5. Healthcare Infection Control Practices Advisory Committee; Berríos-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg. 2017;152(8):784–791. doi:10.1001/jamasurg.2017.0904
6. Ban KA, Minei JP, Laronga C, et al. American college of surgeons and surgical infection society: surgical site infection guidelines, 2016 update. J Am Coll Surg. 2017;224(1):59–74. doi:10.1016/j.jamcollsurg.2016.10.029
7. National institute for health and care excellence surgical site infections: prevention and treatment. NICE guideline [NG125]. Available from: https://www.nice.org.uk/guidance/ng125.
8. Calderwood MS, Anderson DJ, Bratzler DW, et al. Strategies to prevent surgical site infections in acute-care hospitals: 2022 Update. Infect Control Hosp Epidemiol. 2023;44(5):695–720. doi:10.1017/ice.2023.67
9. World Health Organization. Global guidelines for the prevention of surgical site infection. Second edition. 2018. Available from: https://iris.who.int/server/api/core/bitstreams/5c422323-5c27-4e6a-812e-dbd76023ba48/content.
10. Italian PPS network; Vicentini C, Russotto A, Bussolino R, et al. Quality indicators for appropriate inpatient antibiotic use: results from two national surveys in Italy, 2016–2022. J Hosp Infect. 160;2025:34–44. doi:10.1016/j.jhin.2025.03.007
11. Pronovost PJ, Murphy DJ, Needham DM. The science of translating research into practice in intensive care. Am J Respir Crit Care Med. 2010;182(12):1463–1464. doi:10.1164/rccm.201008-1255ED
12. Tomsic I, Heinze NR, Chaberny IF, et al. Implementation interventions in preventing surgical site infections in abdominal surgery: a systematic review. BMC Health Serv Res. 2020;20(1):236. doi:10.1186/s12913-020-4995-z
13. Ariyo P, Zayed B, Riese V, et al. Implementation strategies to reduce surgical site infections: a systematic review. Infect Control Hosp Epidemiol. 2019;40(3):287–300. doi:10.1017/ice.2018.355
14. World Health Organization. Implementation manual to support the prevention of surgical site infections at the facility level—turning recommendations into practice (interim version). Geneva; 2018. Available from: https://apps.who.int/iris/handle/10665/330071.
15. Sartelli M, Bartoli S, Borghi F, et al. Implementation strategies for preventing healthcare-associated infections across the surgical pathway: an Italian multisociety document. Antibiotics. 2023;12(3):521. doi:10.3390/antibiotics12030521
16. Schreiber PW, Sax H, Wolfensberger A, et al. The preventable proportion of healthcare-associated infections 2005–2016: systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2018;39(11):1277–1295. doi:10.1017/ice.2018.183
17. systematic review and evidence-based guidance on organization of hospital infection control programmes (SIGHT) study group; Zingg W, Holmes A, Dettenkofer M, et al. Hospital organisation, management, and structure for prevention of health-care-associated infection: a systematic review and expert consensus. Lancet Infect Dis. 2015;15(2):212–224. doi:10.1016/S1473-3099(14)70854-0
18. Thandar MM, Matsuoka S, Rahman O, et al. Infection control teams for reducing healthcare-associated infections in hospitals and other healthcare settings: a protocol for systematic review. BMJ Open. 2021;11(3):e044971. doi:10.1136/bmjopen-2020-044971
19. Sartelli M, Labricciosa FM, Coccolini F, et al. It is time to define an organizational model for the prevention and management of infections along the surgical pathway: a worldwide cross-sectional survey. World J Emerg Surg. 2022;17(1):17. doi:10.1186/s13017-022-00420-4
20. World Health Organization. Guidelines on core components of infection prevention and control programmes at the national and acute health care facility level. Geneva; 2016. Available from: https://apps.who.int/iris/handle/10665/251730.
21. Meschiari M, Segala FV, Gallerani A, et al. Implementation of infection prevention and control components in Italian hospitals based on a nationwide survey on behalf of INSIEME project. Sci Rep. 2025;15(1):36977. doi:10.1038/s41598-025-20893-y
22. Midturi JK, Narasimhan A, Barnett T, et al. A successful multifaceted strategy to improve hand hygiene compliance rates. Am J Infect Control. 2015;43(5):533–536. doi:10.1016/j.ajic.2015.01.024
23. Brocket J, Shaban RZ. Characteristics of a successful hospital hand hygiene program: an Australian perspective. Healthcare Infect. 2015;20:101–107. doi:10.1071/HI15007
24. World Health Organization. A guide to the implementation of the WHO multimodal hand hygiene improvement strategy. Geneve; 2009. Available from: https://www.who.int/publications/i/item/a-guide-to-the-implementation-of-the-whomultimodal-hand-hygiene-improvement-strategy.
25. Allegranzi B, Aiken AM, Zeynep Kubilay N, et al. A multimodal infection control and patient safety intervention to reduce surgical site infections in Africa: a multicentre, before-after, cohort study. Lancet Infect Dis. 2018;18(5):507–515. doi:10.1016/S1473-3099(18)30107-5
26. Barchitta M, Matranga D, Quattrocchi A, et al. Prevalence of surgical site infections before and after the implementation of a multimodal infection control programme. J Antimicrob Chemother. 2012;67(3):749–755. doi:10.1093/jac/dkr505
27. Badia JM, Rubio-Pérez I, López-Menéndez J, et al. The persistent breach between evidence and practice in the prevention of surgical site infection. Qualitative study. Int J Surg. 2020;82:231–239. doi:10.1016/j.ijsu.2020.08.027
28. Wolfhagen N, Boldingh QJJ, Boermeester MA, de Jonge SW. Perioperative care bundles for the prevention of surgical-site infections: meta-analysis. Br J Surg. 2022;109(10):933–942. doi:10.1093/bjs/znac196
29. Tanner J, Padley W, Assadian O, et al. Do surgical care bundles reduce the risk of surgical site infections in patients undergoing colorectal surgery? A systematic review and cohort meta-analysis of 8515 patients. Surgery. 2015;158:66–77. doi:10.1016/j.surg.2015.03.009
30. Zywot A, Lau CSM, Fletcher HS, Paul S. Bundles prevent surgical site infections after colorectal surgery: meta-analysis and systematic review. J Gastrointest Surg. 2017;21:1915–1930. doi:10.1007/s11605-017-3465-3
31. Pop-Vicas AE, Abad C, Baubie K, et al. Colorectal bundles for surgical site infection prevention: a systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2020;41:805–812. doi:10.1017/ice.2020.112
32. Moro ML, Sartelli M, Gastaldi S, et al. Bundle for the prevention of surgical site infections. Rome: Istituto Superiore di Sanità; 2025. Available from: https://www.iss.it/documents/20126/6703853/Bundle+ISC+EN.pdf.
33. World Health Organization. WHO Guidelines for Safe Surgery 2009. Geneva; 2009. Available from: https://iris.who.int/server/api/core/bitstreams/c2ea24bb-10f7-48e4-8f63-55932e817ddc/content.
34. International Surgical Outcomes Study (ISOS) group; Abbott TEF, Ahmad T, Phull MK, et al. The surgical safety checklist and patient outcomes after surgery: a prospective observational cohort study, systematic review and meta-analysis. Br J Anaesth. 2018;120(1):146–155. doi:10.1016/j.bja.2017.08.002
35. Shankar R. Implementation of the WHO surgical safety checklist at a teaching hospital in India and evaluation of the effects on perioperative complications. Int J Heal Plann Manag. 2018;33:836–846. doi:10.1002/hpm.2533
36. de Almeida SM, de Menezes FG, Martino MDV, et al. Impact of a surgical safety checklist on surgical site infections, antimicrobial resistance, antimicrobial consumption, costs and mortality. J Hosp Infect. 2021;116:10–15. doi:10.1016/j.jhin.2021.05.003
37. Pfeiffer Y, Atkinson A, Maag J, et al. Preventing surgical site infections: are safety climate level and its strength associated with self-reported commitment to, subjective norms toward, and knowledge about preventive measures? J Patient Saf. 2023;19(4):264–270. doi:10.1097/PTS.0000000000001111
38. van Buijtene A, Foster D. Does a hospital culture influence adherence to infection prevention and control and rates of healthcare associated infection? A literature review. J Infect Prev. 2019;20(1):5–17. doi:10.1177/1757177418805833
39. Pop-Vicas AE, Young A, Knobloch MJ, et al. Surgeons’ mental models of surgical site infection: insights into adherence with complex prevention bundles. Infect Control Hosp Epidemiol. 2022;43(9):1249–1255. doi:10.1017/ice.2021.161
40. Sartelli M, Coccolini F, Abu-Zidan FM, et al. Hey surgeons! It is time to lead and be a champion in preventing and managing surgical infections! World J Emerg Surg. 2020;15:28. doi:10.1186/s13017-020-00308-1
41. Tartari E, Weterings V, Gastmeier P, et al. Patient engagement with surgical site infection prevention: an expert panel perspective. Antimicrob Resist Infect Control. 2017;6:45. doi:10.1186/s13756-017-0202-3
42. Gastmeier P, Schwab F, Sohr D, et al. Reproducibility of the surveillance effect to decrease nosocomial infection rates. Infect Control Hosp Epidemiol. 2009;30(10):993–999. doi:10.1086/605720
43. European Centre for Disease Prevention and Control. Protocol for the surveillance of surgical site infections and prevention indicators in European hospitals. Stockholm; 2025. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/surgical-site-infections-protocol-surveillance-2-3.pdf.
44. PRAISE SSI working group; Denkel LA, Arnaud I, Brekelmans M, et al. Automated surveillance for surgical site infections (SSI) in hospitals and surveillance networks-expert perspectives for implementation. Antimicrob Resist Infect Control. 2024;13(1):155. doi:10.1186/s13756-024-01505-2
45. Sartelli M, Marini CP, McNelis J, et al. Preventing and controlling healthcare-associated infections: the first principle of every antimicrobial stewardship program in hospital settings. Antibiotics. 2024;13(9):896. doi:10.3390/antibiotics13090896
46. Manivannan B, Gowda D, Bulagonda P, et al. Surveillance, auditing, and feedback can reduce surgical site infection dramatically: toward zero surgical site infection. Surg Infect. 2018;19(3):313–320. doi:10.1089/sur.2017.272
47. Rosa R, Sposato K, Abbo LM. Preventing surgical site infections: implementing strategies throughout the perioperative continuum. AORN J. 2023;117(5):300–311. doi:10.1002/aorn.13913
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Candida auris Urinary Tract Colonization and Nosocomial Infection Control Strategies in Shanghai
Fan D, Fu M, Wei M, Xue Y, Guo J, Qiao D
Infection and Drug Resistance 2026, 19:551745
Published Date: 13 January 2026