Back to Journals » Infection and Drug Resistance » Volume 19
Candida auris Urinary Tract Colonization and Nosocomial Infection Control Strategies in Shanghai
Authors Fan D ![]() , Fu M, Wei M, Xue Y, Guo J, Qiao D
, Fu M, Wei M, Xue Y, Guo J, Qiao D
Received 15 September 2025
Accepted for publication 17 December 2025
Published 13 January 2026 Volume 2026:19 551745
DOI https://doi.org/10.2147/IDR.S551745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Deping Fan,1,* Mengqiu Fu,2,* Mingjing Wei,3,* Yuyuan Xue,3 Jian Guo,4 Dan Qiao5
1Department of Hospital Infection Control, Nanxiang Branch of Ruijin Hospital, Shanghai, People’s Republic of China; 2Department of Hospital Infection Control, Shanghai Xuhui District Dahua Hospital, Shanghai, People’s Republic of China; 3Department of Dermatology, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China; 4Department of Laboratory Medicine, Shanghai East Hospital, School of Life Sciences and Technology, Tongji University, Shanghai, People’s Republic of China; 5Department of Laboratory Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dan Qiao, Email [email protected] Jian Guo, Email [email protected]
Background: Candida auris is a multidrug-resistant pathogenic fungus that exhibits regional variation and is emerging in new clades worldwide. C. auris predominantly colonizes the urinary tract and respiratory system, thereby increasing the risk of bloodstream infection.
Objective: To evaluate the epidemiological characteristics of C. auris urinary tract colonization in Shanghai and assess the efficacy of prevention and control strategies using molecular epidemiology and clinical interventions to provide evidence-based guidance for hospital infection control.
Methods: Cases were identified using the ECIFIG Surveillance Network. C. auris isolates from urethral samples were cultured and identified by MALDI-TOF MS combined with ITS sequencing. Antifungal susceptibility was tested using microbroth dilution and YeastOne colorimetric assay. Whole-genome sequencing (WGS) was used to analyze mutations in drug resistance genes, and phylogenetic relationships were determined using SNP-based analysis. The patient received amphotericin B bladder irrigation combined with saline. Active surveillance screened close contacts, environmental surfaces, and hands of healthcare workers. The efficacy of various disinfectants on different surfaces was evaluated to optimize disinfection, and all interventions were guided by comprehensive risk assessment.
Results: Between April 2024 and April 2025, C. auris was isolated from the urine samples of 10 long-term bedridden patients with indwelling catheters in Shanghai. All strains were fluconazole-resistant; one strain exhibited amphotericin B resistance, and the other showed echinocandin resistance, harboring the FKS1-S639F mutation. Mutations in ERG11 and CDR1 were also identified. Therefore, amphotericin B bladder irrigation is clinically effective. Environmental monitoring demonstrated that the optimized broad-spectrum composite disinfectant successfully eradicated C. auris. This study demonstrates that the disinfection protocol achieved a success rate of 80% following the intervention, with no subsequent cross-transmission observed.
Conclusion: Candida urinary tract by C. auris poses a risk for hematogenous dissemination. Individualized antifungal treatment combined with enhanced environmental disinfection effectively controls colonization and prevents nosocomial transmission, informing hospital infection-prevention strategies. This study is the first epidemiological investigation of C. auris urinary tract colonization in Shanghai, an open metropolitan area in China.
Keywords: Candida auris, risk assessment, healthcare-associated infections, infection prevention and control
Introduction
In 2018, the first case of Candida auris was reported in Beijing, and sporadic cases appeared across various regions, with notable regional clustering and inter-provincial spread primarily in Guangdong, Liaoning, and Beijing.1–4 C. auris is salt-tolerant and heat-resistant, and is capable of persisting in hospital environments and colonizing human skin, making it a significant risk for immunocompromised individuals and those undergoing invasive treatments.5–7 Currently, the predominant strains are from South African and South Asian clades.8 Resistance monitoring has shown that most C. auris isolates are resistant to fluconazole and some are resistant to amphotericin B and echinocandins.9–11 C. auris primarily colonizes the urethra and respiratory tract in humans and spreads through hospital outbreaks, cross-regional transmission, and international importation.12,13 Healthcare institutions must prioritize the prevention and control of C. auris as this is crucial for interrupting its transmission.
Previous reports indicated significant regional differences in the rate of positive urine cultures.14,15 A single-center study in Europe isolated 5 positive urine cultures from 41 patients with candidemia, and 56% of these patients had colonization prior to the onset of candidemia.16,17
Regarding treatment, echinocandins and amphotericin B are considered the first-line therapeutic agents. However, the development of antifungal resistance remains a major clinical challenge. Combination therapy or amphotericin B bladder instillation (50 mg/L for 5–7 days) may be considered for refractory infections. Although the CDC recommends no treatment for noninvasive infections, early aggressive intervention remains necessary owing to the high mortality rate associated with pan-resistant strains.18–20
From April 2024 to April 2025, Shanghai East Hospital as the ECIFIG central laboratory, assisted other 5 hospitals in jointly consulting and treating 10 patients. Those patients have long-term indwelling urinary catheters complicated by C. auris urinary tract colonization, of which 2 progressed to bloodstream infections. This finding suggests that catheter-associated mucosal injuries may facilitate pathogen migration. The hospital implemented single-room isolation and conducted contact screening while optimizing disinfection protocols based on the evaluation of the surface disinfectant efficacy for different materials. By analyzing patient colonization and environmental data, this study is the first to develop domestic infection control and disinfection guidelines for C. auris in hospitals, providing a vital foundation for improving clinical recognition and management. This study is the first epidemiological investigation of C. auris urinary tract colonization in Shanghai, an open metropolitan area in China.
Materials and Method
Strains
Urine specimens were collected from ten bedridden patients hospitalized with indwelling urinary catheters in whom C. auris was detected. Subsequently, weekly surveillance sampling was conducted, collecting specimens from the urine, perianal area, axilla, oral cavity, nares, and external auditory canal of colonized patients and other patients in the same ward. Environmental surfaces in wards housing C. auris colonized patients were sampled using sterile cotton swabs including patient monitors, infusion pumps, bedside tables, bed rails, bed linens, bathroom countertops, faucets, floors, and door handles. The hands of healthcare workers were sampled in a similar manner. All sampling procedures followed CDC guidelines for C. auris screening (https://www.cdc.gov/fungal/candida-auris/c-auris-screening.html). Following collection, the cotton swabs were vortexed for 20s, and 1 mL of the specimen suspension was inoculated onto Sabouraud dextrose agar (SDA) plates and incubated at 37°C.
This study was approved by the Ethics Board of the Shanghai East Hospital, Shanghai, China (Approval No 2025YS-038). This study did not involve any human participants or animal subjects, nor did it collect or use any personally identifiable information. This study is an in vitro fungal research. The fungal strains used were isolated from clinical samples in the hospital’s laboratory department.
Inclusion Criteria
Timeframe: Patients admitted between April 2024 and April 2025.
Geographical Location: Patients consulted by outpatient experts at Shanghai East Hospital in Shanghai.
Specific Patient Population: Long-term bedridden patients with indwelling urinary catheters.
Microbiological Confirmation: Patients with confirmed Candida auris urinary tract colonization, identified through culture of urethral samples and confirmed by combined MALDI-TOF MS and ITS sequencing.
Surveillance Network: Cases identified through the ECIFIG surveillance network.
Exclusion Criteria
Sample Source: Candida auris isolates from non-urethral sources were excluded.
Timeframe: Cases identified outside the specified timeframe were excluded.
Patient Status: Patients who were not long-term bedridden or without an indwelling urinary catheter were excluded.
Mixed Infection/Unconfirmed Identification: Samples that failed definitive identification as Candida auris by the described molecular methods (MALDI-TOF MS and ITS sequencing), or cases with major mixed pathogen infections, were excluded.
Isolation and Identification of Candida auris
C. auris strains were inoculated on Sabouraud Dextrose Agar (SDA) and CHROMagar Candida medium and were cultured at 37°C for 24 h. All 10 clinical isolates from urinary tract colonization were identified as C. auris using an EXS3000 MALDI-TOF mass spectrometer. PCR amplification and sequencing were performed by Sangon Biotech (Shanghai, China) using ITS1/ITS4 primers with the following sequences: ITS1 5’-TCCGTAGGTGAACCTGCGG-3’ and ITS4 5’-TCCTCCGCTTATTGATATGC-3’. Sequencing results were subsequently verified using BLASTN database alignment.
Monitoring of Candida auris in the Hospital Environment
This study adopted a prospective longitudinal research method to conduct 10-week multisite colonization monitoring of C. auris in hospitalized patients. Urine, perianal area, axillae, and nasal cavity samples were systematically collected weekly, while high-frequency contact surfaces (bedrails, call buttons, etc.) in the ward and hands of healthcare personnel who came into direct contact with patients were sampled and tested continuously for two months. All samples were inoculated onto CGM agar medium and suspicious colonies were confirmed by MALDI-TOF MS mass spectrometry.
In vitro Antifungal Susceptibility Testing
Nine antifungal agents were evaluated in this study. Antifungal susceptibility testing was performed using both the broth microdilution method and the YeastOne colorimetric system according to the Clinical and Laboratory Standards Institute (CLSI) M27-A3 document and the manufacturer’s protocol, respectively.21,22 Because of the absence of established MIC breakpoints for C. auris, the results were interpreted according to the tentative breakpoints published by the CDC (https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html). According to the CDC interim MIC breakpoints (fluconazole ≥32 mg/L, amphotericin B ≥2 mg/L, caspofungin ≥2 mg/L, micafungin ≥4 mg/L, anidulafungin ≥4 mg/L). Candida parapsilosis ATCC 22019 and Candida krusei ATCC 6258 were used as quality control strains to ensure assay reliability and accuracy, respectively.
Whole-Genome Sequencing and Phylogenetic Analysis
Whole-genome sequencing was performed for the systematic analysis of the isolates.23 Genomic DNA was extracted using a commercial DNA extraction kit and sequencing libraries were prepared using the Nextera XT library preparation kit. Sequencing was conducted on the Illumina NextSeq 550 platform generating 75 bp single-end reads. Raw sequencing data were assessed using FastQC (https://www.bioinformatics.babraham.ac.uk/projects/fastqc/) and processed using Trim Galore (http://www.bioinformatics.babraham.ac.uk/projects/trim_galore/) for adapter-trimming and quality filtering. De novo genome assembly was performed using the SPAdes assembler, retaining contigs ≥1000 bp in length. Assembly quality was evaluated using QUAST. Single nucleotide polymorphism (SNP) analysis was performed using the B8441 reference genome (GCA_002759435.3). A maximum-likelihood phylogenetic tree was constructed using IQ-TREE with the TVMe+ASC+R3 substitution model and 1000 bootstrap replicates to assess the phylogenetic relationships and ensure statistical reliability.
Evaluation of Disinfection Effectiveness on Various Surface Materials Through Field Sampling
C. auris suspensions were prepared at concentrations of 1×107-5×107 CFU/mL for experimental use. Three experimental groups were established: the positive control, negative control, and disinfection treatment groups. For the positive control group, sterile cotton swabs were dipped in the fungal suspension and applied to the test surfaces, which were then cut and placed in test tubes containing 2 mL of neutralizing solution and vortexed for 20s. The negative control group was administered a neutralizing solution alone. For the disinfection group, appropriate disinfectants were selected based on the surface material properties and disinfectant characteristics according to the manufacturer’s instructions. Following the treatment, cotton swabs pre-moistened with a neutralizing solution were used for surface sampling. The cloth samples were cut into 1×3 cm fragments and placed in test tubes containing a neutralizing solution. All processed samples were immediately labeled and transported in sterile sampling tubes containing 2 mL physiological saline for microbiological analysis. Each experiment was performed in triplicate to ensure the reliability of the results.
Hospital Infection Prevention and Control Measures
Based on systematic risk assessment, we designed a comprehensive hospital infection prevention and control protocol. Upon C. auris identification, immediate active surveillance was conducted among close contacts and within the surrounding environment. Colonized patients were transferred to single-occupancy rooms and placed under strict contact precautions. Intravenous amphotericin B combined with bladder irrigation was used as therapy. 1000 mg/L chlorine-based disinfectant solution was used for terminal disinfection of the affected wards, strictly following the established “clean-first” disinfection protocol.
Patients underwent daily whole-body bathing with 2% chlorhexidine gluconate solution, with particular attention paid to high-risk anatomical sites including the axillae, perianal region, and nares. A systematic surveillance program incorporating weekly screenings of both patients and environmental surfaces has been established. Surveillance was discontinued only after obtaining two consecutive negative culture results were obtained. The medical equipment was managed under a patient-dedicated policy and disinfected using the triple-wipe technique with 75% ethanol. The medical waste was handled using strict double-bagging protocols.
Patient urine and contaminated textiles were disinfected by immersion in a 1000 mg/L chlorine-based solution. High-touch surfaces were thoroughly disinfected daily using hydrogen peroxide-based wipes. Environmental management included twice-daily natural ventilation via window opening, and supplementation with ultraviolet air disinfection systems.
Regarding personnel management, standard and contact precautions were implemented, with an emphasis on strict adherence to hand hygiene protocols. Patient transport was limited to essential procedures and comprehensive clinical handovers were ensured when transport was necessary. The clinical necessity of indwelling catheters was assessed daily to enable their timely removal. A dedicated staffing model was established and targeted training sessions were conducted to ensure effective infection prevention.
Results
Clinical Characteristics
This study investigated the epidemiological characteristics of 10 Candida auris urinary tract colonization in Shanghai from April 2024 to April 2025. The index patient, who was admitted in April 2024, had C. auris successfully isolated from a urine specimen. Among the 10 patients, 7 were male and 3 were female, with a mean age of 69.1 ± 8.69 years. The mean interval from hospital admission to C. auris colonization diagnosis was 11.1 ± 12.58 days. All patients were discharged without any signs of infection, and no mortality cases occurred. Of the 10 patients, seven had underlying diseases, while three did not have any underlying conditions. Notably, among those with underlying diseases, two cases (accounting for 28.6% of the patients with underlying conditions) progressed from urinary tract infections to bloodstream infections, as shown in Table 1.
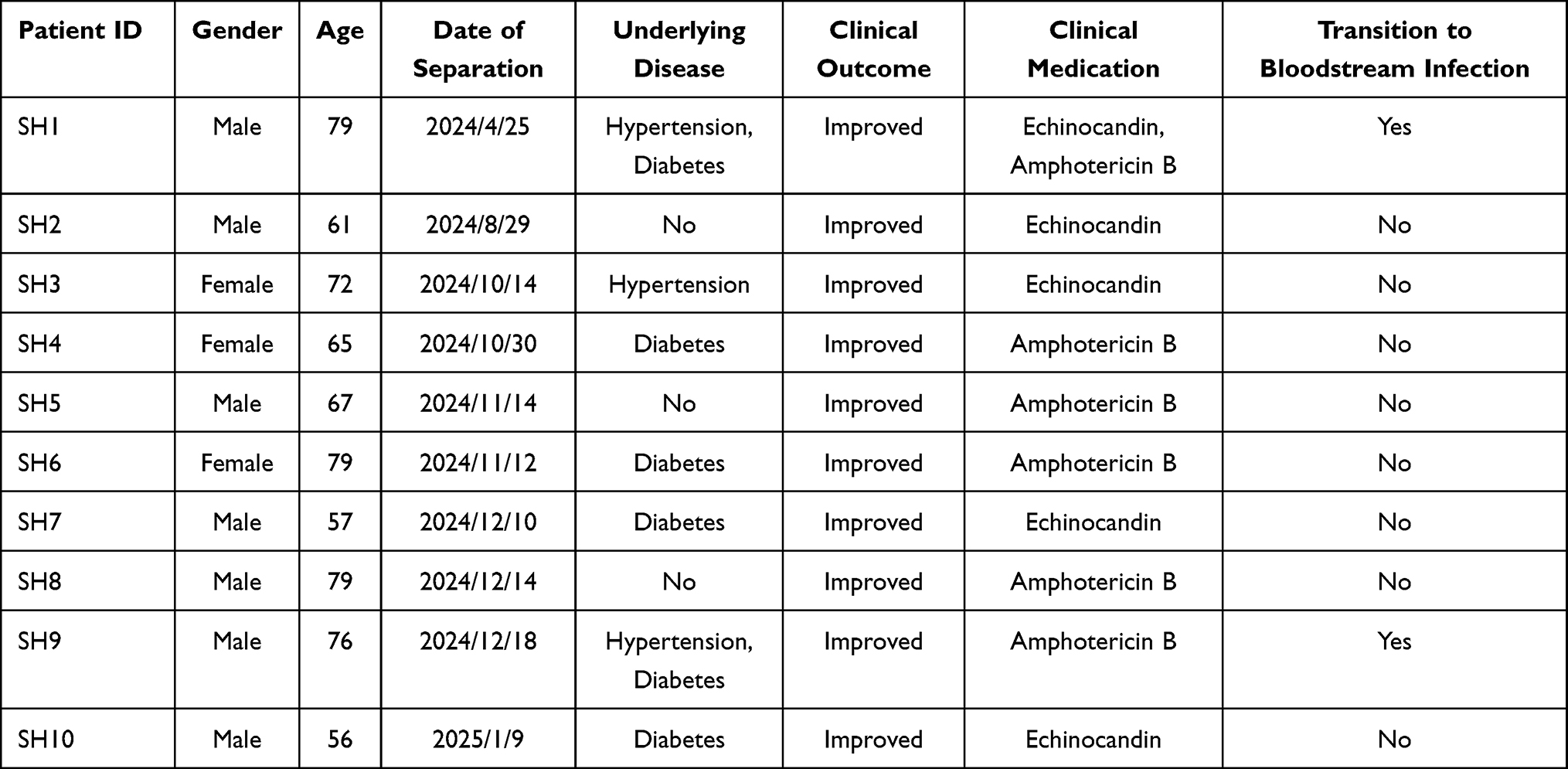 |
Table 1 Distribution of Clinical Characteristics of Patients with C. auris Infection |
Identification of Candida auris
All isolates were identified as C. auris using MALDI-TOF mass, with a confidence score of ≥99.9%. Sanger sequencing was performed for all 10 C. auris isolates and the resulting sequences were analyzed using BLASTN alignment against the NCBI database. The results showed 98%-100% similarity to C. auris, consistent with the mass spectrometry findings. C. auris exhibited smooth and cream-colored colonies on SDA (Figure 1). Among the 10 patients, 7 had underlying comorbidities, while 3 had no documented comorbidities. Notably, two of the seven patients with comorbidities progressed from urinary tract colonization to invasive bloodstream infection (Figure 2).
 |
Figure 1 Colony morphology of C. auris on SDA 35°C for 3 days. |
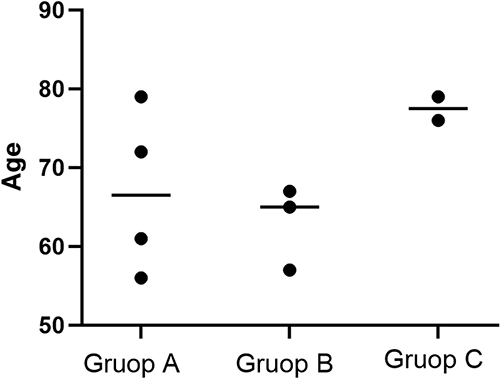 |
Figure 2 Association between comorbidities and progression to C. auris bloodstream infection. Group A: Urinary tract infection with underlying comorbidities. Group B: Urinary tract infection without underlying comorbidities. Group C: Bloodstream infection with underlying comorbidities. |
Candida auris Detection
A 10-week prospective surveillance study was conducted to screen hospitalized patients for C. auris colonization at multiple anatomical sites. Patient 1 exhibited persistent colonization at four anatomical sites (urine, rectum, axilla, and nasal cavity) during the first six weeks of surveillance. Samples from the oral cavity and external auditory canal remained consistently negative throughout the study period. Notably, colonization of the nasal cavity persisted through week 10. In contrast, patients 2 and 3 tested negative for C. auris colonization at all sites during the observation period. The nasal cavity demonstrated persistent colonization, whereas colonization of the urinary, rectal, and axillary sites followed a coordinated temporal clearance pattern. Detailed results are presented in Table 2. During the same period, all 56 environmental samples and 16 hand swabs from HCWs tested negative for C. auris.
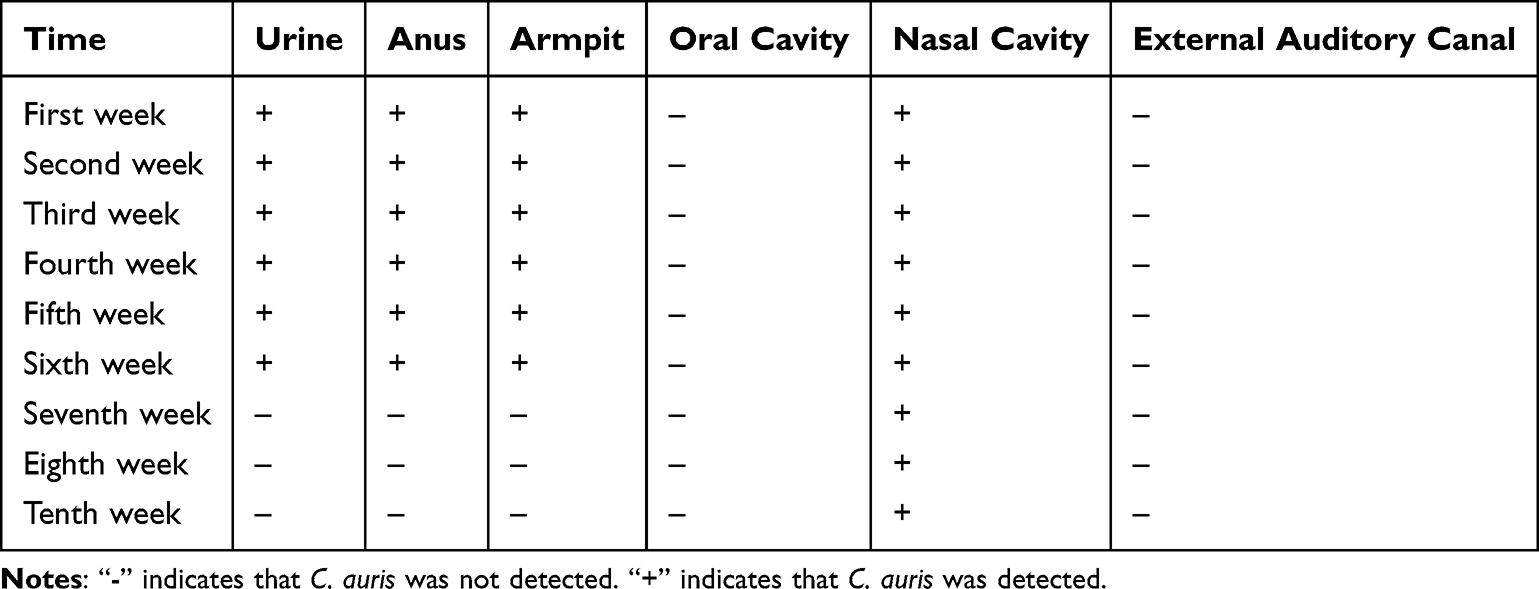 |
Table 2 Active Screening for C. auris in Different Sampling Sites from Patient SH1 |
Antifungal Susceptibility Testing and Changes in Drug Resistance Genes
All isolates exhibited high-level resistance to fluconazole (MIC: 128–256 μg/mL) but remained universally susceptible to 5-flucytosine (MIC: 0.06–0.12 μg/mL). One isolate (Pt05) demonstrated resistance to amphotericin B (MIC: 2 μg/mL) and was resistant to all three echinocandins (FKS1 S639F mutation), while the remaining isolates were susceptible to both amphotericin B and echinocandins. The MIC ranges for itraconazole, posaconazole, and voriconazole were 0.12–0.5 μg/mL, 0.06–0.5 μg/mL, and 0.5–2 μg/mL, respectively.
Phylogenetic Analysis
To obtain high-quality genomic data, whole-genome sequencing (WGS) was performed for all 10 isolates using the Illumina NovaSeq 6000 platform with paired-end 150 bp sequencing (PE150) (Sangon Biotech, Shanghai, China). A phylogenetic tree was constructed using the maximum likelihood method with Candida auris strain B8441 (GCA_002759435.3) as the reference genome. Phylogenetic analysis revealed that the isolates from the 10 patients clustered into two evolutionary clades, Clade I and Clade III, with Clade III being the predominant lineage (Figure 3). Strain Pt01 belonged to Clade I, whereas the remaining isolates were assigned to Clade III.
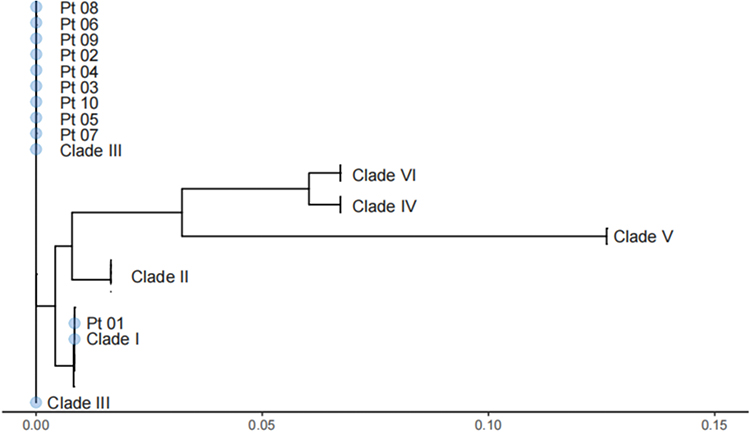 |
Figure 3 Phylogenetic Tree of 10 C. auris Isolates from Shanghai Based on WGS. |
On-Site Simulation and Monitoring of Disinfection Efficacy
This study evaluated the efficacy of eight commonly used disinfectants against Candida auris contamination on various hospital surface materials (Table 3). Quaternary ammonium compound-based wipes (2.0–2.4 g/L), including doorknobs, bedside tables, and computer monitors, failed to achieve adequate disinfection of non-porous surfaces after 2 min of contact. In contrast, ethanol (75% ± 5%), chlorine-based disinfectants (1000 mg/L), and hydrogen peroxide wipes (8.5–11.5 g/L) demonstrated consistent efficacy across all tested surfaces within 2–3 minutes. Notably, chlorine-based disinfectants require extended exposure (30 min) to effectively decontaminate porous materials such as fabric surfaces.
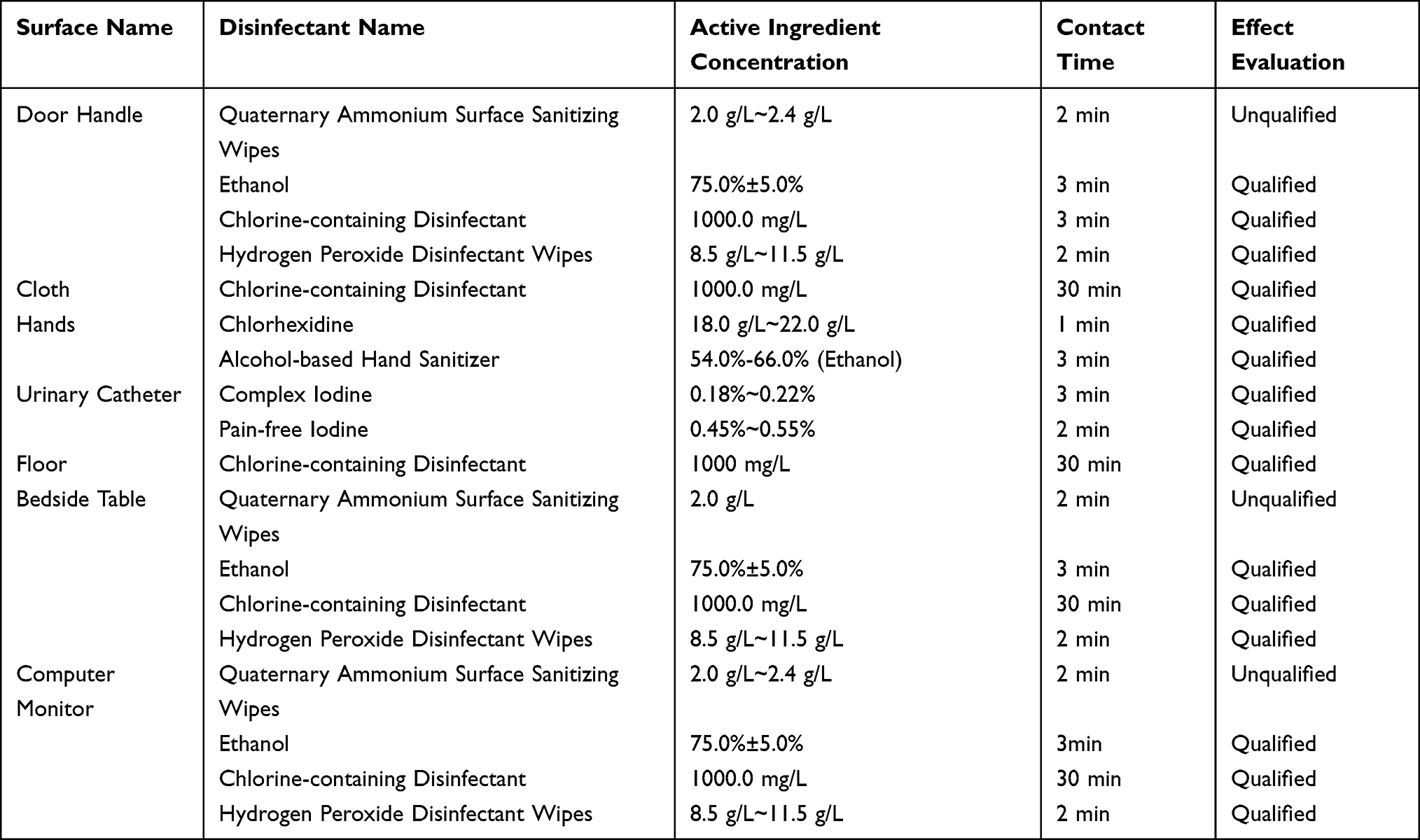 |
Table 3 The Disinfection Efficacy of 8 Commonly Used Disinfectants on Different Material Surfaces Against the C. auris |
For hand hygiene, chlorhexidine-alcohol disinfectants (containing 54–66% ethanol at 18–22 g/L) were effective within 1 min of contact. Medical devices such as urinary catheters were successfully disinfected within 2–3 minutes using compound iodine (0.18–0.22%) and povidone-iodine (0.45–0.55%) solutions. These findings highlight the significant variability in disinfectant performance based on the surface material, with nonporous surfaces generally requiring shorter contact times than porous materials for effective C. auris eradication.
Discussion
In China, Candida auris infections remain sporadic, and most healthcare institutions face challenges including limited diagnostic capacity and insufficient experience in infection prevention.4,24,25 Colonization risk factors are primarily associated with contact with infected individuals or contaminated environments,26,27 highlighting effective environmental disinfection. In clinical practice, disinfectant selection should consider factors such as the surface material, cost-effectiveness, operational safety, and disinfection coverage.28,29
Unlike international studies that retrospectively identified urinary tract colonization in patients with established candidemia,14–16 our study employed prospective active surveillance to detect a defined cluster of C. auris urinary tract colonization prior to the onset of invasive infection. This finding confirms that colonization serves as a high-risk precursor to invasive disease, underscoring the critical early-warning value of proactive screening in high-risk populations. More importantly, while previous studies primarily established an association between colonization and subsequent infection, our research further demonstrates the successful translation of surveillance data into effective infection control practice through the implementation of comprehensive interventions that ultimately interrupted transmission chains.
Our study found that quaternary ammonium-based surface wipes were ineffective against C. auris, whereas 2% chlorhexidine, chlorine-based disinfectants (1000 mg/L), hydrogen peroxide wipes, and other evaluated disinfectants achieved effective eradication. We recommend 2% chlorhexidine for skin decolonization, iodine-based preparations for catheter care, alcohol-based hand rubs for hand hygiene, and chlorine-based disinfectants for environmental decontamination. Between April 2024 and April 2025, a standardized infection control protocol was successfully implemented for 10 patients with C. auris urinary colonization, achieving effective containment without cross-transmission. Future research should expand disinfectant evaluation to provide more comprehensive evidence for clinical infection control strategies.
Current clinical reports indicate that C. auris infections often involve multisite colonization, with a considerable proportion of cases progressing to bloodstream infections.30,31 In this study, two patients developed candidemia with major risk factors, including indwelling urinary catheters, broad-spectrum antibiotic exposure, and underlying comorbidities.32,33 C. auris exhibits environmental persistence and high mortality, and requires tailored treatment based on drug susceptibility, infection site, and patient status.14,26 Positive urine cultures warrant immediate contact and environmental screening, with weekly monitoring until discharge to ensure decontamination. Echinocandins are recommended as first-line monotherapy for initial treatment. Although C. auris exhibits lower resistance rates to echinocandins than to azoles, resistance remains common, and monotherapy may be insufficient for many urinary tract infections.34 In cases of treatment failure, combination therapy with echinocandin and amphotericin B is recommended, which is beneficial for recurrent infections.35 In this study, amphotericin B bladder irrigation was applied only to a small number of selected cases. For refractory cases. Intravesical instillation of amphotericin B deoxycholate (AmB-D) at 50 μg/mL once or twice daily may be recommended. Owing to its smaller molecular size (<1 nm) than liposomal formulations (60–80 nm), AmB-D may achieve better mucosal tissue penetration. However, nephrotoxicity must be carefully considered.19,36 Product labeling supports this indication for UTIs and recommends a 50 μg/mL dosing protocol; however, liposomal amphotericin B is not approved for bladder instillation,37,38 and its clinical utility in C. auris infections requires further evidence. Currently, AmB-D is recommended only as part of combination therapy for persistent, recurrent, or resistant infections. Flucytosine may offer therapeutic potential owing to its high urinary concentrations; however, the risk of acquired resistance should be monitored.39
The persistence of C. auris in the nasal cavity, compared to its clearance from other sites, may be attributed to several interconnected biological factors. The nasal anatomy provides physical shelter, while its immune-tolerant mucosa and potentially weaker microbial competition create a permissive niche. Crucially, C. auris likely forms robust biofilms on the nasal epithelium, which confer enhanced resistance to both antifungals and host defenses. Furthermore, the nasal cavity’s complex anatomical structure makes it particularly difficult to effectively reach and disinfect. This multifactorial explanation underscores the nose’s role as a key reservoir, necessitating its prioritization in future surveillance and control strategies.
Following C. auris detection, comprehensive infection control measures (including contact isolation, environmental disinfection, and intravesical amphotericin B therapy) achieved complete clearance from the urine/rectum/axilla/environment within one month, with only persistent nasal colonization and no new cases. Our tiered treatment protocol recommends observation for asymptomatic colonization, echinocandins for uncomplicated UTIs, combination therapy for complex infections, and ≥14 days of treatment until two consecutive weekly negative cultures are obtained. Monthly post-treatment surveillance is essential for monitoring recurrence. This framework demonstrates that standardized protocols can effectively control C. auris transmission, while providing evidence-based clinical guidance.
Conclusion
The combined antifungal and environmental disinfection strategy successfully eliminated urinary tract colonization and prevented subsequent transmission, demonstrating high clinical effectiveness. This study provides critical evidence for developing hospital infection control protocols, proving that targeted interventions can effectively contain C. auris dissemination.
Ethical Approval
This study was approved by the Ethics Board of the Shanghai East Hospital, Shanghai, China (Approval No 2025YS-038). This study did not involve any human participants or animal subjects, nor did it collect or use any personally identifiable information. This study is an in vitro fungal research. The fungal strains used were isolated from clinical samples in the hospital’s laboratory department. All isolated strains have permanently removed the patient’s personal identifier (such as name, ID number, etc.) and only retained non identifying microbiological data (such as strain, isolation site). These processed samples are considered as anonymized biological materials. According to the scope defined in the Helsinki Declaration of the World Medical Association (Principle 1) and in accordance with the relevant provisions of China’s “Ethical Review Measures for Biomedical Research Involving Human Subjects” (2016, Article 3) and “Personal Information Protection Law” (2021, Article 73), this study does not belong to “biomedical research involving human subjects”, and the processed data is anonymized information. Therefore, it is not necessary to submit it to the ethics committee for review and approval, nor to obtain informed consent. Therefore, this study meets the conditions of exemption from ethical review and informed consent.
Acknowledgments
We gratefully acknowledge funding from the Funds for International Cooperation and Exchange of the National Natural Science Foundation of China (Grant No.W2411075) and the Shanghai Pudong New Area Health Commission General Project (Grant No. PW2024A-02). We would like to thank all participants in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by the Funds for International Cooperation and Exchange of the National Natural Science Foundation of China (Grant No.W2411075) and the Shanghai Pudong New Area Health Commission General Project (Grant No. PW2024A-02).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Wang X, Bing J, Zheng Q, et al. The first isolate of Candida auris in China: clinical and biological aspects. Emerg Microbes Infect. 2018;7(1):93. doi:10.1038/s41426-018-0095-0
2. Genomic epidemiology of Candida auris in a general hospital in Shenyang, China: a three-year surveillance study - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/34027824/.
3. Peng Y, Liu Y, Yu X, et al. First report of Candida auris in Guangdong, China: clinical and microbiological characteristics of 7 episodes of candidemia. Emerg Microbes Infect. 2024;13(1):2300525. doi:10.1080/22221751.2023.2300525
4. Bing J, Du H, Guo P, et al. Candida auris-associated hospitalizations and outbreaks, China, 2018-2023. Emerg Microbes Infect. 2024;13(1):2302843. doi:10.1080/22221751.2024.2302843
5. Jeffery-Smith A, Taori SK, Schelenz S, et al. Candida auris: a review of the literature. Clin Microbiol Rev. 2018;31(1):e00029–11. doi:10.1128/CMR.00029-17
6. Chowdhary A, Jain K, Chauhan N. Candida auris genetics and emergence. Annu Rev Microbiol. 2023;77(1):583–602. doi:10.1146/annurev-micro-032521-015858
7. Horton MV, Holt AM, Nett JE. Mechanisms of pathogenicity for the emerging fungus Candida auris. PLoS Pathog. 2023;19(12):e1011843. doi:10.1371/journal.ppat.1011843
8. Du H, Bing J, Hu T, Ennis CL, Nobile CJ, Huang G. Candida auris: epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020;16(10):e1008921. doi:10.1371/journal.ppat.1008921
9. Forsberg K, Woodworth K, Walters M, et al. Candida auris: the recent emergence of a multidrug-resistant fungal pathogen. Med Mycol. 2019;57(1):1–12. doi:10.1093/mmy/myy054
10. Ostrowsky B, Greenko J, Adams E, et al. Candida auris isolates resistant to three classes of antifungal medications - New York, 2019. MMWR Morb Mortal Wkly Rep. 2020;69(1):6–9. doi:10.15585/mmwr.mm6901a2
11. Dakalbab S, Hamdy R, Holigová P, et al. Uniqueness of Candida auris cell wall in morphogenesis, virulence, resistance, and immune evasion. Microbiol Res. 2024;286:127797. doi:10.1016/j.micres.2024.127797
12. Osei Sekyere J. Candida auris: a systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen. 2018;7(4):e00578. doi:10.1002/mbo3.578
13. Sharma C, Kadosh D. Perspective on the origin, resistance, and spread of the emerging human fungal pathogen Candida auris. PLoS Pathog. 2023;19(3):e1011190. doi:10.1371/journal.ppat.1011190
14. Sayeed MA, Farooqi J, Jabeen K, Awan S, Mahmood SF. Clinical spectrum and factors impacting outcome of Candida auris: a single center study from Pakistan. BMC Infect Dis. 2019;19(1):384. doi:10.1186/s12879-019-3999-y
15. Ahmad S, Khan Z, Al-Sweih N, Alfouzan W, Joseph L. Candida auris in various hospitals across Kuwait and their susceptibility and molecular basis of resistance to antifungal drugs. Mycoses. 2020;63(1):104–112. doi:10.1111/myc.13022
16. Ruiz-Gaitán A, Moret AM, Tasias-Pitarch M, et al. An outbreak due to Candida auris with prolonged colonisation and candidaemia in a tertiary care European hospital. Mycoses. 2018;61(7):498–505. doi:10.1111/myc.12781
17. Hamprecht A, Barber AE, Mellinghoff SC, et al. Candida auris in Germany and previous exposure to foreign healthcare. Emerg Infect Dis. 2019;25(9):1763–1765. doi:10.3201/eid2509.190262
18. Harris E. CDC: candida auris fungal infections and drug resistance on the rise. JAMA. 2023;329(15):1248. doi:10.1001/jama.2023.5255
19. Fisher JF, Sobel JD, Kauffman CA, Newman CA. Candida urinary tract infections--treatment. Clin Infect Dis. 2011;52 Suppl 6(suppl_6):S457–466. doi:10.1093/cid/cir112
20. La Bella AA, Santiago-Tirado FH, Flores-Mireles AL. Candida auris is emerging as a prevalent urinary pathogen. PLoS Pathog. 2025;21(5):e1013138. doi:10.1371/journal.ppat.1013138
21. Altinbaş R, Bariş A, Şen S, Öztürk R, KiRaz N. Comparison of the Sensititre YeastOne antifungal method with the CLSI M27-A3 reference method to determine the activity of antifungal agents against clinical isolates of Candidaspp. Turk J Med Sci. 2020;50(8):2024–2031. doi:10.3906/sag-1909-97
22. Reference method for broth dilution antifungal susceptibility testing of yeasts; approved standard, 3rd edition, CLSI document M27-A3 2008.
23. Lockhart SR, Etienne KA, Vallabhaneni S, et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis. 2017;64(2):134–140. doi:10.1093/cid/ciw691
24. Zhang Y, Han J, Ma Y, et al. Two outbreaks and sporadic occurrences of Candida auris from one hospital in China: an epidemiological, genomic retrospective study. Infection. 2025;53(1):349–358. doi:10.1007/s15010-024-02378-8
25. Jones CR, Neill C, Borman AM, et al. The laboratory investigation, management, and infection prevention and control of Candida auris: a narrative review to inform the 2024 national guidance update in England. J Med Microbiol. 2024;73(5):001820. doi:10.1099/jmm.0.001820
26. Wasylyshyn A, Stoneman EK. Management of Candida auris. JAMA. 2024;331(7):611–612. doi:10.1001/jama.2023.24921
27. Cristina ML, Spagnolo AM, Sartini M, et al. An overview on Candida auris in healthcare settings. J Fungi. 2023;9(9):913. doi:10.3390/jof9090913
28. Ku TSN, Walraven CJ, Lee SA. Candida auris: disinfectants and implications for infection control. Front Microbiol. 2018;9:726. doi:10.3389/fmicb.2018.00726
29. Voorn MG, Kelley AM, Chaggar GK, Li X, Teska PJ, Oliver HF. Contact time and disinfectant formulation significantly impact the efficacies of disinfectant towelettes against Candida auris on hard, non-porous surfaces. Sci Rep. 2023;13(1):5849. doi:10.1038/s41598-023-32876-y
30. Bradley SF. Candida auris Infection. JAMA. 2019;322(15):1526. doi:10.1001/jama.2019.13857
31. Biagi MJ, Wiederhold NP, Gibas C, et al. Development of high-level echinocandin resistance in a patient with recurrent Candida auris candidemia secondary to chronic candiduria. Open Forum Infect Dis. 2019;6(7):ofz262. doi:10.1093/ofid/ofz262
32. Munshi A, Almadani F, Ossenkopp J, et al. Risk factors, antifungal susceptibility, complications, and outcome of Candida auris bloodstream infection in a tertiary care center in the western region of Saudi Arabia. J Infect Public Health. 2024;17(1):182–188. doi:10.1016/j.jiph.2023.11.021
33. Park S, Kim H, Hong D, Oh H. Candida auris: understanding the dynamics of C. auris infection versus colonization. Med Mycol. 2024;62(9):myae086. doi:10.1093/mmy/myae086
34. Chowdhary A, Prakash A, Sharma C, et al. A multicentre study of antifungal susceptibility patterns among 350 Candida auris isolates (2009-17) in India: role of the ERG11 and FKS1 genes in azole and echinocandin resistance. J Antimicrob Chemother. 2018;73(4):891–899. doi:10.1093/jac/dkx480
35. Forgács L, Borman AM, Kovács R, et al. In vivo efficacy of amphotericin b against four Candida auris clades. J Fungi. 2022;8(5):499. doi:10.3390/jof8050499
36. Wang S, Pan J, Gu L, et al. Review of treatment options for a multidrug-resistant fungus: candida auris. Med Mycol. 2024;62(1):myad127. doi:10.1093/mmy/myad127
37. Sullivan KA, Caylor MM, Lin FC, Campbell-Bright S. Comparison of Amphotericin B bladder irrigations versus fluconazole for the treatment of candiduria in intensive care unit patients. J Pharm Pract. 2017;30(3):347–352. doi:10.1177/0897190016645032
38. Tuon FF, Amato VS, Penteado Filho SR. Bladder irrigation with amphotericin B and fungal urinary tract infection--systematic review with meta-analysis. Int J Infect Dis. 2009;13(6):701–706. doi:10.1016/j.ijid.2008.10.012
39. Barchiesi F, Arzeni D, Caselli F, Scalise G. Primary resistance to flucytosine among clinical isolates of Candida spp. J Antimicrob Chemother. 2000;45(3):408–409. doi:10.1093/jac/45.3.408
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
From Evidence to Implementation: A SIMPIOS Multimodal, Continuous Improvement Approach to Prevent Surgical Site Infections
Sartelli M, Labricciosa FM, Moro ML, Pan A, Ripabelli G
Infection and Drug Resistance 2026, 19:565233
Published Date: 22 January 2026