Back to Journals » Advances in Medical Education and Practice » Volume 17
From Conventional OSCE to Virtual Reality–Enhanced OSCE: A Narrative Review of Promise and Pitfalls in Medical Education
Authors Zhang X, Lyu X, Weng X, Zhou Y
Received 11 November 2025
Accepted for publication 25 January 2026
Published 6 February 2026 Volume 2026:17 580766
DOI https://doi.org/10.2147/AMEP.S580766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Xiaohui Zhang,1,* Xiaohong Lyu,1,* Xisheng Weng,2 Yidong Zhou1
1Department of Breast Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Orthopedic Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xisheng Weng, Department of Orthopedic Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China, Email [email protected] Yidong Zhou, Department of Breast Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China, Email [email protected]
Background: Objective Structured Clinical Examinations (OSCEs) are widely used to assess clinical competence but face growing challenges related to cost, scalability, standardization, and the assessment of complex clinical scenarios. Advances in virtual reality (VR) technology have prompted increasing interest in VR-enhanced OSCEs (VR-OSCEs) as a potential solution.
Methods: This review examined the existing literature on the application of VR in OSCEs. Relevant studies were identified through searches of major electronic databases to provide a narrative overview of representative literature.
Results: The included studies indicate that VR-OSCEs are primarily applied in virtual patient simulations, immersive clinical environments, and interactive procedural training. Overall, VR-OSCEs demonstrate improved standardization, enhanced learner engagement, objective performance tracking, and timely feedback compared with traditional OSCE formats. Evidence also suggests potential benefits in assessing rare or high-risk clinical scenarios, although variability exists in technological maturity and validation approaches.
Conclusion: VR-OSCEs represent a promising evolution of clinical assessment in medical education, offering scalable, immersive, and data-driven evaluation opportunities. However, challenges related to cost, technical infrastructure, faculty training, and standardization remain. Further rigorous validation studies and hybrid assessment models are needed to support broader implementation and ensure educational effectiveness.
Keywords: virtual reality, objective structured clinical examination, clinical skill assessment, medical education, immersive learning
Introduction
Since its introduction in the 20th century by Ronald Harden,1 the Objective Structured Clinical Examination (OSCE) has become the gold standard for assessing clinical competence in medical education. By simulating real-world clinical scenarios, OSCEs aim to evaluate clinical knowledge, communication skills, and practical abilities through structured and standardized patient interactions. Despite their widespread adoption across medical schools worldwide, traditional OSCEs have increasingly faced scrutiny due to several inherent limitations, including predictability and repetition, limited standardization, high costs and substantial resource demands, examiner variability,2 and difficulties in replicating complex or high-risk clinical scenarios.3,4
In parallel with the rapid evolution of educational technologies, there has been growing interest in leveraging virtual reality (VR) to address these challenges. VR offers a unique immersive and interactive approach to clinical training and assessment, enabling the creation of highly realistic and dynamic clinical environments. Through standardized virtual patient interactions, immediate feedback, and integrated data analytics,5 VR has the potential to enhance both learning experiences and assessment reliability. The concept of VR-enhanced OSCEs (VR-OSCEs) therefore represents a logical extension of traditional OSCE methodology, offering a promising strategy to overcome many of the structural and logistical constraints of conventional assessments.
However, integrating VR into OSCEs is not without its challenges. The initial costs, technological complexity, and potential disparities in access may limit widespread implementation. Additionally, questions remain about the validity and reliability of VR-OSCEs as assessment tools and their acceptance among educators and learners. As with any innovation, understanding both the benefits and limitations is essential to effectively harness the potential of VR in medical education.
This article aims to explore the promise and pitfalls of VR-OSCEs by synthesizing and discussing representative research on their applications and reported educational outcomes. By analyzing the successes and challenges of VR-OSCEs, we hope to provide insights for educators, policymakers, and researchers seeking to elevate the quality of medical training in an increasingly digital age.
Traditional OSCEs: A Gold Standard in Need of an Upgrade
The Objective Structured Clinical Examination (OSCE) uses multiple stations with specific tasks to test medical knowledge, communication, and practical skills and thus provide a comprehensive assessment of clinical abilities of medical students (6x). Their reliability and versatility have made them a cornerstone of medical assessment worldwide.
However, despite their historical success, traditional OSCEs face significant limitations in today’s rapidly changing medical educational landscape. Firstly, OSCEs are resource-intensive, demanding significant investment in recruiting, training, and employing standardized patients (SPs) and experienced examiners, as well as securing appropriate physical spaces. Moreover, the success of the examination largely depends on the consistency and authenticity of SPs performances, which requires extensive professional training.6 Additionally, the need for multiple SPs to accommodate large-scale examinations further increases the financial burden on institutions.7 Secondly, maintaining consistent standardization across multiple examination environments and evaluators remains challenging. Variations in station layout, available equipment, and the overall atmosphere between different stations can directly affect student performance.8 Moreover, potential examiner bias and inconsistencies in scoring criteria could potentially impact the fairness in the assessment process.9 Thirdly, traditional OSCEs struggle to replicate certain high-risk, rare or complex clinical scenarios, limiting their ability to fully assess a student’s readiness for real-world practice. Moreover, due to ethical and safety considerations, these high-risk procedures or rare conditions cannot be replicated in real-world environments, thereby limiting the comprehensiveness and effectiveness of OSCEs in thoroughly evaluating students’ clinical competencies.10 Finally, traditional OSCEs are characterized by low assessment efficiency. Examiners must manually record and score candidate performance, a process that is not only time-consuming but also prone to subjective bias.11 Furthermore, feedback regarding examination performance is often delayed, reducing the opportunity for timely and constructive guidance to students.12 Additionally, the increasing number of medical students globally has made scaling OSCEs difficult, further complicating their effective implementation.
To address these challenges, educators are exploring technology-enhanced assessment approaches including Tele and virtual OSCE (VOSCE) platforms,13,14 AI-driven case generation with automated assessment,15 high-fidelity simulation using smart mannequins and wearable sensor technology,16 virtual standardized patients (VSPs) along with enhanced feedback through digital data analytics.17 Among the most promising and feasible innovations in the current landscape is the Integration of augmented reality (AR)18 and virtual reality (VR), ensuring an academically rigorous yet engaging learning experience.
Virtual Reality Technology: Fundamentals and Advancements
Virtual Reality (VR) technology is a versatile and powerful tool applied across various fields, from gaming to healthcare, offering immersive and interactive experiences that mimic real-world environments. By utilizing hardware like headsets, motion controllers, and sensors, along with specialized software for simulating environments and interactions, VR creates dynamic three-dimensional spaces.19 The foundation of effective VR technology lies in its core principles: immersion (the sense of being present in a virtual environment), interaction, presence, realism, sensory feedback, real-time rendering, tracking and spatial awareness, adaptability, and multi-user collaboration. Complex algorithms power these systems, rendering real-time graphics, tracking user movements, and providing feedback, which together create an illusion of presence, thus making users feel as if they are physically present in the virtual world.20 This immersive experience is primarily driven by visual and auditory stimuli, with advanced systems incorporating haptic feedback to simulate touch, enhancing the sense of reality and interaction within the virtual environment.
Recent years have witnessed substantial advancements across all facets of VR technology, including hardware, software, and computational frameworks, thereby enhancing both the accessibility and overall performance of VR systems,21 as shown by timeline in Figure 1. One of the most remarkable advancements in VR technology is the improvement in hardware components, particularly VR headsets. Early VR equipment was bulky, expensive, and suffered from limited resolution, high latency, and a narrow field of view, often causing motion sickness and discomfort. However, advancements in hardware have led to lighter, more affordable VR devices such as Oculus Rift, HTC Vive, Meta Quest series, Valve Index and PlayStation VR feature high-definition displays, wider fields of view, and reduced latency, significantly improving user comfort and immersion.18 The integration of eye-tracking technology has further enhanced these systems, allowing for more precise control and dynamic foveated rendering, which allocates computational power to where the user is looking, optimizing both performance and realism. Additionally, the development of standalone VR headsets has made VR more accessible, eliminating the need for expensive, high-end computers. The advancement of motion tracking and haptic feedback has also expanded the realism and interactivity of VR environments.22 Accurate tracking systems, using external sensors or inside-out tracking via built-in cameras, allow users to move naturally within virtual spaces. This accurate tracking is crucial for experiences like medical training, where realistic simulations of surgeries or patient interactions are essential for skill development. Haptic feedback devices, including gloves, vests, and controllers, now provide tactile responses, mimicking the sensation of touch and physical resistance. This not only enhances immersion but also opens up new possibilities for VR in rehabilitation, physical therapy, and sports training. For example, VR-based rehabilitation programs can simulate environments where patients practice motor skills, receiving real-time feedback and motivation through haptic sensations. Concurrently, software advancements have paralleled hardware improvements, making VR environments more dynamic, adaptive, and lifelike. Real-time rendering technologies, powered by advanced graphics processing units (GPUs), enable highly detailed and realistic environments, complete with complex lighting, shadows, and textures.23 The integration of artificial intelligence (AI) has made VR systems more interactive and personalized. AI-driven virtual characters can respond to user inputs intelligently, enabling more natural interactions in training simulations, therapeutic scenarios, and educational experiences. Machine learning algorithms also adapt VR environments to the user’s needs, personalizing the experience based on their actions, preferences, and learning pace. For instance, AI-enhanced VR platforms used in education can adjust difficulty levels or present tailored scenarios, helping learners retain knowledge more effectively.24 Moreover, the rise of wireless and cloud-based VR solutions has broadened the scope of VR technology. By leveraging cloud computing, VR platforms can render complex environments remotely, reducing the need for high-end local hardware. This accessibility is particularly significant for industries like real estate and architecture, where stakeholders can experience realistic virtual walkthroughs without specialized equipment.25 Additionally, the advent of 5G technology has addressed latency issues, enabling seamless streaming of high-quality, cloud-rendered VR experiences, making VR more scalable and cost-effective. Further companies like Meta are working on concepts blend virtual and augmented reality (AR), creating an extended reality (XR) experience that allows for real-time, multi-user interactions in immersive digital spaces.26
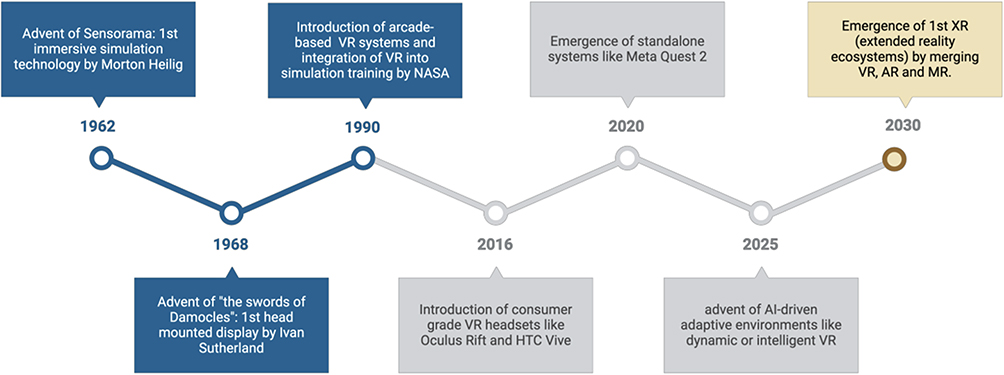 |
Figure 1 Timeline of key technological advancements in virtual reality relevant to medical education. |
Integrating Virtual Reality into OSCEs: A New Frontier in Clinical Assessment
The concept of VR in healthcare training dates back to the early 1990s, initially limited to surgical simulations and procedural training.27 Coinciding with the rise of affordable and sophisticated VR technology. The integration of VR into OSCE began in the early 2000s, with first dated study done at 4 teaching hospitals of Karolinska Institute.28 Early VR-OSCE systems focused on basic procedural skills, such as catheterization and airway management. Over time, advancements in graphics, artificial intelligence, and haptic feedback have enabled the development of complex, immersive clinical scenarios that replicate diverse and realistic patient interactions.
The integration of VR technology In OSCEs is underpinned by the core principles of Immersion, Interactivity, Feedback mechanisms and adaptability which are achieved through stereoscopic displays, head-tracking, hand-tracking, and haptic feedback.29 Stereoscopic displays create a depth perception by presenting separate images to each eye; head-tracking adjusts visual content based on user head movements, enhancing the immersive experience; hand-tracking and haptic feedback enable natural and realistic interactions within virtual environments.30 The application of VR technology in OSCE is primarily evident in three key areas: virtual patient simulation, immersive clinical environment creation, and interactive skill training. Virtual patient simulation uses highly realistic digital models to represent various clinical symptoms and signs, providing candidates with standardized patient interaction experiences.31 This technology not only simulates common cases but also enables the creation of rare or high-risk scenarios, addressing the lack of case diversity in traditional OSCEs.32–36 For Instance, the university of cologne has developed a virtual patient system for history-taking and physical examination components of OSCEs. Candidates interact with virtual patients using VR headsets, asking questions and conducting virtual physical examinations. The system provides immediate feedback based on candidates performance such as whether they correctly identified key clinical signs or missed important questions. Research has shown that candidates using this system perform significantly better in history-taking and physical examinations compared to those in traditional OSCEs.37
Similarly, immersive clinical environment creation utilizes VR technology to build realistic medical scenarios, such as emergency rooms and operating theaters, allowing candidates to be assessed in environments that closely resemble real clinical settings.38 This immersive experience not only increases the authenticity of the examination but also helps alleviate candidates’ anxiety, leading to a more accurate reflection of their clinical capabilities.39 For instance, singapore general hospital has developed a virtual emergency room environment for emergency management within OSCEs. Candidates face various emergency situations, such as cardiac arrest and severe trauma, in the virtual emergency room. The system simulates real emergency room equipment and sounds, enhancing immersion. Several studies have demonstrated that candidates using immersive VR-based emergency scenarios show significantly improved emergency management performance and teamwork skills compared with traditional OSCE formats.37–39 As a result, the VR system CDS100 has been integrated into OSCE courses, allowing instructors to efficiently set up assessments and evaluate students’ learning progress through automated digital reports, thereby reinforcing learning objectives and enabling students to identify errors and improve their clinical skills.40
Similarly, interactive skill training provides real-time feedback and guidance through VR systems, enabling candidates to repeatedly practice various clinical procedures, such as venipuncture and cardiopulmonary resuscitation, in a simulated environment, thereby improving skill proficiency and boosting confidence.41 VR surgical simulators are also used in OSCEs for assessing surgical skills. Candidates perform various surgical procedures, such as laparoscopic surgery, in a virtual operating room. The system precisely tracks candidate’s actions, operation times, and error counts, providing detailed performance reports.42 Studies show that candidates trained with VR surgical simulators perform significantly better in real surgeries compared to those trained through traditional methods.43
Technical Framework and Implementation Strategies for VR-Enhanced OSCEs for Modern Medical Education
Development of an effective VR-OSCE system should be based on 4 pedagogical foundations that are constructivist learning theory, experiential learning, learning by reptation and deliberate practice and authentic assessment. To achieve these, it requires the combination of robust technical infrastructure, evidence-based educational design, and thorough implementation planning. For instance, VR-enhanced OSCE systems are built upon advanced hardware components that include. High-quality head-mounted displays (HMDs), tracking systems, and haptic feedback devices are essential.44 Equally important are the software systems. Modeling virtual patients and clinical environments requires a high degree of realism and interactivity. Commonly used development tools include simulation engines like Unity and Unreal Engine, which offer powerful graphic rendering and physics engines.33 Similarly, customizable authoring platforms such as virti’s immersive learning platform or oxford medical simulation can be used as scenario authoring tools. Additionally, data collection and analysis are also key components. The good system must be capable of recording candidate’s operational data in real time, such as decision-making speed, procedural accuracy, hand-eye coordination, error counts, and operation trajectories. This data can be used to generate detailed assessment reports and provide personalized feedback for candidates.35 Lastly, VR systems must interface seamlessly with existing learning management systems (LMS) and electronic medical record (EMR) systems for better interoperability, which ensures that performance data can be incorporated into broader educational assessments and quality improvement initiatives.36 Moreover, an intuitive, user-friendly interface can significantly enhance candidates’ experience. For example, using voice commands and gesture controls can reduce reliance on traditional input devices, making interactions more natural.45
Apart from technical infrastructure, successful implementation of VR-enhanced OSCEs requires thoughtful integration into existing curricula. Educators must identify competencies best suited for simulation and determine where VR can replace or supplement traditional methods, implementing pilot programs to valuate feasibility and effectiveness could allow for incremental scaling and user-feedback based refinement of VR-enhanced OSCEs.34 Additionally, deployment of multidisciplinary teams of clinical educators, simulation technologists, software developers, and data scientists ensure that VR-enhanced OSCEs are both clinically relevant and technologically robust.
Most importantly the effective use of VR in OSCEs depends on faculty proficiency with the technology. Institutions must invest in training programs that equip educators with the skills to operate VR systems, interpret performance data, and integrate simulations into assessment strategies. Workshops and continuous professional development initiatives are vital to overcome resistance to new technology and ensure optimal use of VR tools.46 Moreover, Robust evaluation frameworks are essential to measure the impact of VR-enhanced OSCEs and data collected from VR systems can facilitate continuous improvement by identifying areas where simulation scenarios require modification, additionally performing comparative studies between traditional OSCEs and VR-enhanced assessments can provide evidence for best practices and inform future innovations.47
In the modern medical training system, VR-OSCE has have already shown most promise in surgical training, Nursing education, General clinical practice and Interprofessional education (IPE). During surgical training, VR-enhanced OSCEs allow surgeons to rehearse complex procedures in a risk-free environment as shown by Medical Realities and 360° Surgical Streams through a live VR-streamed operation that allowed trainees to observe and interact with the procedure in real time, providing a novel approach to surgical rehearsal and assessment.48 Nursing education benefits from VR OSCEs by simulating patient care scenarios that require critical thinking, communication, and hands-on skills as done through oxford medical simulation for nursing at university of Northampton to manage virtual patients presenting with conditions like acute asthma exacerbations or myocardial infarction.49 In core medical subjects like internal medicine, pediatrics, and primary care, VR-OSCEs can assess learners’ abilities to diagnose and manage common to rare conditions, as done in UC Irvine’s VR-OSCE Implementation, during the COVID-19 pandemic. Additionally, VR-OSCEs enable interprofessional teams to practice coordinating patient care in complex scenarios like mass casualty incidents or rapid response team activation, as done through Multi-User VR Simulation pilot project at Midwestern Teaching Hospital.50 A detailed timeline highlighting major milestones in use of VR in medical education is shown in Figure 2.
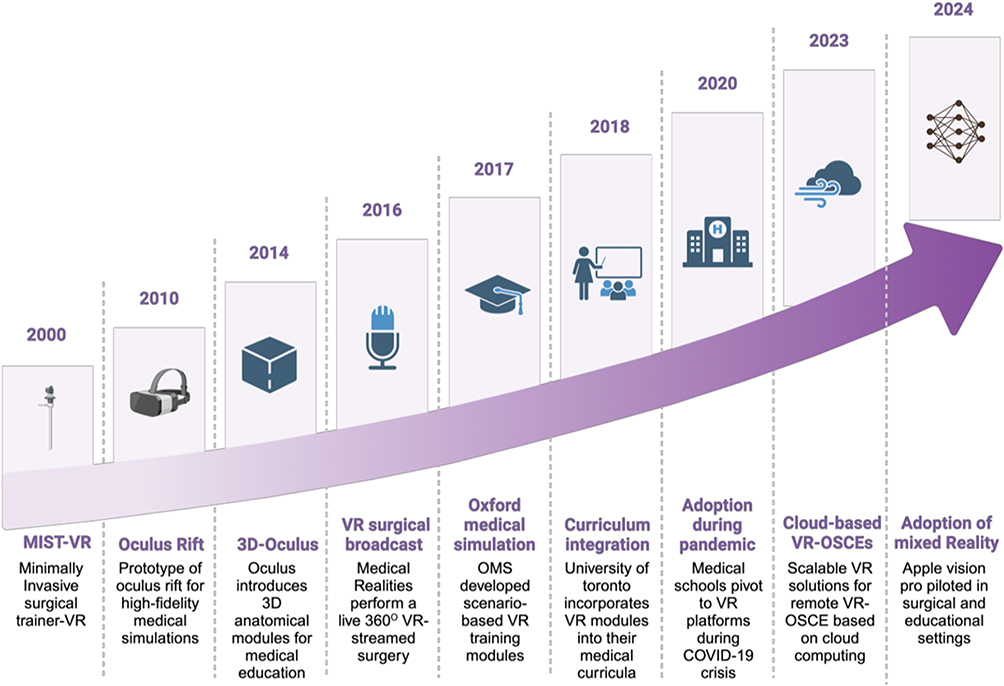 |
Figure 2 Milestones in the application of virtual reality to medical teaching and assessment. |
Advantages of VR-OSCE
In medical education, the application of VR technology is rapidly expanding, with applications ranging from surgical simulations to rehabilitation training, each transforming clinical education and practice. Specifically, the use of VR technology in OSCEs has emerged as a promising alternative that harnesses immersive simulations to enhance clinical training. This approach overcomes many logistical, financial, and ethical challenges associated with traditional OSCEs while offering additional significant benefits.
Firstly, VR-OSCEs markedly improve the standardization and objectivity of clinical examinations. By utilizing pre-programmed virtual patients and scenarios, every candidate encounters identical conditions, which minimizes inconsistencies introduced by human factors and enhances inter-rater reliability. For instance, it was demonstrated that VR-based OSCEs provide more reproducible results compared to traditional formats.51 The University of Toronto’s implementation of VR-OSCE modules further exemplifies how standardized criteria can reduce examiner subjectivity in clinical skills assessments.
Secondly, VR technology offers an immersive learning environment that significantly enhances engagement and skill retention. Students benefit from the opportunity to repeatedly practice clinical scenarios until they achieve proficiency.52 In a meta-analysis it was found that VR-based training improved long-term skill retention by 30% compared to conventional teaching methods.53 This is supported by real-life examples such as The Cleveland Clinic’s use of VR-OSCE for surgical residents, which has led to higher accuracy in laparoscopic procedures.
Thirdly, VR-OSCEs streamline the assessment process by automating the recording and analysis of candidate’s performances. This automation enables the delivery of immediate, objective, and quantifiable feedback on various performance metrics, including clinical decision-making, communication skills, and procedural accuracy thereby enhancing evaluation and reducing the workload of examiners.30 A randomized controlled trial reported a 25% improvement in clinical performance among students receiving real-time feedback via VR-OSCEs.54 The Mayo Clinic has similarly integrated VR-OSCE feedback systems to allow for prompt corrections and improvements during training.
Additionally, VR technology permits the simultaneous operation of multiple examination stations and offers flexible access from any location with internet connectivity, thus improving the overall efficiency of the examination.45 This flexibility was highlighted in a study at Stanford University, which found that VR-based training enabled students in rural areas to complete clinical assessments without the need for extensive travel, thereby increasing participation rates.55
Moreover, despite the potentially high initial investment, VR-OSCEs offer significant cost-effectiveness over time. Virtual patients and scenarios are reusable, reducing the recurrent expenses associated with training and hiring standardized patients.45 A cost-analysis study found that implementing VR-OSCE in medical schools reduced training costs by 40% compared to traditional OSCE setups in long term.56 The NHS in the UK has also embraced VR-based training modules to train junior doctors and nurses, substantially lowering expenses related to physical exam stations and patient actors.34
Safety is another paramount advantage of VR-OSCEs. They enable students to practice high-risk procedures such as emergency resuscitation, surgery, and infectious disease management, in a risk-free environment, addressing ethical concerns inherent in real-patient scenarios without endangering patient safety.48 Moreover, VR technology enables the simulation of rare or extreme cases (eg, cardiac arrest, severe trauma)57 that are impractical to replicate in traditional settings, thus ensuring comprehensive preparation for diverse clinical situations. The immersive nature of VR-OSCE also helps reduce candidate anxiety, thus minimizing errors caused by nervousness.58 A study demonstrated improved performance in high-pressure scenarios, such as neonatal resuscitation, through repeated risk-free exposure in VR simulations.57 Harvard Medical School’s VR simulations for sepsis management similarly underscore the educational value of this technology.
Overall, VR-OSCE is revolutionizing medical education by offering a standardized, cost-effective, and immersive training environment. Their advantages including enhanced objectivity, ethical safety, accessibility, immediate feedback, superior skill retention, and automated performance tracking are well-documented,59 as seen in studies such as the one conducted at Guangzhou Medical University, where the VR experimental group significantly (P-value <0.05) outperformed the control group in a four-station OSCE examination. This innovative approach not only requires less time and space compared to traditional methods but also incurs lower costs, making it a compelling candidate for wider adoption60 to ensure the training of highly competent healthcare professionals ready for real-world challenges.
Measuring the Effectiveness of VR-OSCE in Medical Education
Measuring the effectiveness of VR-OSCE in medical education requires a multi-dimensional approach that integrates objective performance metrics, immediate feedback systems, and user experience evaluations. The first method involves quantitative analysis, which encompasses objective indicators such as exam scores, decision-making speed, procedural accuracy, diagnostic reasoning, and error counts. These metrics are automatically recorded and analyzed by the system, thereby ensuring an objective assessment of clinical skills.30 Research supports the high efficacy and reliability of VR-OSCE in evaluating clinical competence, with candidate performance in VR environments correlating strongly with results from traditional OSCEs, thus confirming the reliability of the assessment.36
The second method assesses candidate acceptance, perceived simulation realism, overall engagement, and satisfaction with VR-OSCE through surveys, focus groups, interviews, and feedback on the system’s effectiveness. Multiple studies have reported that candidates assessed using VR-OSCE exhibit higher levels of confidence, motivation, engagement, and perceived realism compared with conventional OSCE preparation methods.37,54,58 Participants have reported high acceptance of VR technology, citing its ability to offer a more realistic clinical experience.37 Additionally, the integration of real-time data analysis in VR-OSCE facilitates immediate feedback, enabling students to promptly identify and address performance gaps. Academic research has linked immediate feedback to improved skill retention and accelerated learning curves, although some candidates note the need for adaptation time to VR equipment and further improvements to the user interface.33 For example, a study from the University of Leicester found that using VR videos for OSCE preparation significantly increased self-assessed exam confidence while reducing anxiety levels.61 Similarly, research from the University of Alberta demonstrated that VR teaching significantly (P=0.02) lowered anxiety in first-year occupational therapy students preparing for OSCEs.57
Long-term educational outcomes can be evaluated by tracking the performance of students trained with VR-OSCE during subsequent clinical internships and real-world practice. Preliminary findings suggest that these students exhibit greater adaptability and higher skill levels during clinical internships, particularly in managing complex and high-risk scenarios.41 A study from Jinan University revealed that after one year, the VR training group not only performed better in clinical practice but also achieved significantly (P<0.05) higher scores in OSCEs, especially in physical examination, suturing, and imaging interpretation.62
A recent randomized controlled trial involving fifth-year medical students, reported no differences in feasibility and difficulty levels between VR scenarios and traditional physical stations (PHS). However, the VR scenarios excelled in item discrimination and discrimination index, with notable differences in student perceptions of the assessment mode, particularly regarding hesitancy toward its broader future application.54 Moreover, a study conducted in Sulzbach, Germany, demonstrated that students trained with VR achieved a 91% success rate in OSCE exams, significantly higher than the 78% success rate observed in the traditional group.63
Navigating the Ethical and Legal Landscape of VR-OSCE
The integration of Virtual Reality-Objective Structured Clinical Examinations (VR-OSCE) into medical education offers unprecedented benefits in terms of standardization, efficiency, and immersive learning. However, as with any emerging technology, VR-OSCE introduces a range of ethical and legal challenges that must be carefully addressed to ensure responsible and equitable implementation.
Foremost among the ethical concerns is the issue of privacy. The system automatically records and analyzes extensive candidate data, which may include sensitive personal information. It is therefore essential that candidates are fully informed about what data is being collected, how it will be used, and who will have access to it. Obtaining informed consent from examinees can be challenging, and ensuring the security and confidentiality of this data remains a critical issue.36 Transparent data handling policies are vital for building trust and complying with broader ethical mandates regarding privacy and data security.
A second ethical concern is fairness. Candidates may exhibit varying levels of adaptability to VR technology, potentially compromising the fairness of the examination. For instance, some candidates may experience motion sickness, which could hinder their ability to use the VR equipment effectively.64 Moreover, despite VR-OSCE’s potential to reduce examiner bias through standardized scenarios, there is still a risk of algorithmic biases being embedded in the system. Continuous evaluation of these virtual simulations is necessary to ensure that they do not inadvertently favor certain groups over others. Ethical oversight must therefore extend to the design and regular updating of VR scenarios to maintain fairness and objectivity in clinical assessments.65
Thirdly, the digital divide also presents a significant challenge to equitable access. Institutions must consider how to provide the necessary technological resources and training, particularly for students in under-resourced regions or those with limited exposure to advanced technologies. Addressing these disparities is essential to prevent further inequity in educational opportunities and outcomes.66
Finally, ethical review is equally important. VR-OSCE may encompass sensitive or high-risk procedures, and it is imperative that these procedures adhere to established ethical guidelines. A stringent ethical review process is crucial to address these concerns.33
In addition to ethical issues, several legal considerations must be taken into account. VR-OSCE implementations must comply with a complex array of legal frameworks, including data protection regulations (such as GDPR) and educational accreditation standards. Ensuring compliance with national and international laws is paramount, and regular legal audits should be conducted to safeguard against potential breaches.27 The development of VR-OSCE platforms involves sophisticated software and proprietary algorithms, raising important questions regarding intellectual property rights and software licensing. Clear agreements between technology providers and educational institutions must delineate ownership, usage rights, and maintenance responsibilities.67 Another critical legal issue is the determination of liability in cases were technical failures or misinterpretations of VR data result in adverse outcomes. Institutions and developers must establish protocols that clarify responsibility, thereby protecting both legal interests and the credibility of the VR-OSCE system.27
In summary, while VR-OSCE represents a significant advancement in medical education, its ethical and legal dimensions necessitate a balanced and proactive approach. Robust governance frameworks—including ethical review boards and legal advisory committees—are essential in guiding the evolution of VR-OSCE. By addressing these issues proactively, institutions can fully harness the transformative potential of VR technology while safeguarding the rights and interests of all stakeholders.
Addressing Obstacles and Shaping the Next Generation of VR-OSCE
While VR-OSCE has the potential to enhance accessibility, standardization, and engagement in medical training, its widespread adoption faces several challenges, including technological limitations, resistance from educators and students, and the need for robust validation.
Despite the promise of VR-OSCE, technical limitations and high costs remain a primary concern. High-quality VR equipment and haptic feedback devices are expensive and requires substantial computational power, limiting their use in resource-constrained institutions.44 Additionally, creating highly realistic virtual patients and environments demands considerable time and resource investment35 and ensuring software stability and minimizing simulation-related discomfort are crucial to maintaining immersion and effectiveness. Solutions to these challenges include cost reductions through mass production, cloud-based VR solutions to reduce hardware dependence, and continued research on optimizing VR environments to reduce motion sickness. Moreover, artificial intelligence (AI)-driven adaptive learning can enhance VR simulations by personalizing difficulty levels based on student’s performance.68 ChatGPT has been used to create realistic clinical scenarios for active role-play and its feedback, which shows potential for artificial intelligence (AI) in general and specifically in the OSCE training of EM physicians.69
Another challenge is the standardization and validation of the system. Currently, the assessment standards for VR-OSCE have not been fully standardized, and building VR-based assessments to accurately measure clinical competence remains a challenge. Further research is needed to incorporate VR-specific metrics, such as response time, decision-making efficiency, interaction accuracy with virtual patients are needed to ensure the reliability and effectiveness of its evaluation results.41 Developing standardized VR-OSCE scoring rubrics aligned with real-world clinical outcomes is essential. Collaboration among medical educators, VR developers, and regulatory bodies can ensure that VR-OSCE maintains credibility and aligns with competency-based medical education frameworks.70
Resistance from educators and students presents another obstacle. Traditionalists may question the efficacy of VR-OSCE compared to conventional OSCE, while students might struggle with unfamiliar interfaces. The lack of hands-on patient interaction in VR-based assessments also raises concerns about the authenticity of clinical skills evaluation.71 To foster acceptance, rigorous validation studies comparing VR-OSCE to traditional methods must be conducted. Training programs for faculty and students can ease the transition, ensuring they recognize VR’s value in medical training. Gamification elements, such as achievement badges and competitive leaderboards, may also increase student engagement and motivation.
To shape the next generation of VR-OSCE, future developments should prioritize both technological enhancements and cost reduction. As VR technology advances, it is anticipated that the price of equipment will decline while performance continues to improve.27 Moreover, the creation of more intelligent, AI-driven virtual patients and the refinement of realistic interaction methods are crucial areas for focus. Further, by integrating traditional and virtual assessment methods, future OSCEs may adopt a hybrid model that combines the strengths of standardized patients and VR technology.36 Additionally, exploring the use of VR-OSCE in remote assessments and cross-regional standardized examinations presents a promising avenue for future research.57
Further technological integration, such as the combination of augmented reality (AR) and mixed reality (MR) with VR, could yield more enriched and flexible examination environments.72 In parallel, the deep incorporation of artificial intelligence (AI) is essential; advanced AI algorithms can facilitate the development of intelligent and adaptive virtual patients capable of dynamically adjusting difficulty based on candidate performance.73 Additionally, specialized AI algorithms need to be developed to simulate patient’s physiological responses and the progression of diseases.74
Remote assessments also represent a critical area for future expansion. With the widespread adoption of 5G networks, it becomes feasible to implement cross-regional VR-OSCEs, thereby enabling candidates from diverse regions to participate within a unified virtual environment.75
Finally, personalized learning is emerging as a significant trend. By analyzing candidate’s operational data, systems can offer customized learning recommendations and targeted training plans to enhance clinical skills.35 The integration of biometric feedback systems such as eye tracking and physiological monitoring can further deepen insights into student’s cognitive and emotional responses during assessments.
Discussion
As we stand at the nexus of traditional excellence and digital innovation, the evolution of VR-OSCE represents not merely an upgrade but a transformative leap in medical education.
The journey beyond conventional OSCEs heralds a transformative era in medical education. This article has illuminated how the venerable traditional OSCE, despite its long-standing excellence, now stands at the threshold of a revolutionary upgrade through VR technology. We have unraveled the fundamentals and groundbreaking advancements in virtual reality, showcasing its dynamic application within the OSCE framework. With innovative technical blueprints and strategic implementation methods, VR-enhanced OSCEs promise to deliver immersive, adaptive, and rigorously effective assessments that resonate with the evolving needs of modern medical training.
The compelling advantages of VR-OSCEs ranging from enriched interactivity and objective performance metrics to heightened realism in clinical simulations, offer a tantalizing glimpse into a future where educational efficacy is measured not only by knowledge but by the dexterity of clinical competence. At the same time, we have navigated the intricate ethical and legal landscapes, acknowledging the challenges and paving the way for solutions that uphold integrity and fairness.
Conclusion
Embracing both the promise and the pitfalls, this review positions VR-OSCE as a beacon of innovation, inviting us to reimagine how we assess, teach, and ultimately enhance patient care. As obstacles are methodically addressed and new horizons explored, the next generation of VR-enhanced OSCEs is set to redefine the educational paradigm, ensuring that our future medical professionals are not just tested, but truly transformed.
Consent for Publication
All authors have reviewed and approved the final version of this manuscript and consent to its publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research Projects Approved for Medical Education in 2025 by the Medical Education Branch of the Chinese Medical Association and the National Center For Health Professions Education Development (No.2025B20).
Disclosure
Xiaohui Zhang and Xiaohong Lyu are co-first authors for this study. The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Harden RM, Stevenson M, Downie WW, Wilson GM. Assessment of clinical competence using objective structured examination. Br Med J. 1975;1(5955):447–13. doi:10.1136/bmj.1.5955.447
2. Alkhateeb N, Salih AM, Shabila N, Al-Dabbagh A. Objective structured clinical examination: challenges and opportunities from students’ perspective. PLoS One. 2022;17(9):e0274055. doi:10.1371/journal.pone.0274055
3. Behera P, Gopi G, Siddaiah A, et al. Challenges of objective structured clinical examination as a tool in medical assessment. Indian J Commun Family Med. 2022;8(2):156–160. doi:10.4103/ijcfm.ijcfm_12_22
4. Turner JL, Dankoski ME. Objective structured clinical exams: a critical review. Fam Med. 2008;40(8):574–578.
5. Kononowicz AA, Woodham LA, Edelbring S, et al. Virtual patient simulations in health professions education: systematic review and meta-analysis by the digital health education collaboration. J Med Internet Res. 2019;21(7):e14676. doi:10.2196/14676
6. Boulet JR, Smee SM, Dillon GF, Gimpel JR. The use of standardized patient assessments for certification and licensure decisions. Simul Healthc. 2009;4(1):35–42. doi:10.1097/SIH.0b013e318182fc6c
7. Adamo G. Simulated and standardized patients in OSCEs: achievements and challenges 1992-2003. Med Teach. 2003;25(3):262–270. doi:10.1080/0142159031000100300
8. Hodges B. OSCE! Variations on a theme by Harden. Med Educ. 2003;37(12):1134–1140. doi:10.1111/j.1365-2923.2003.01717.x
9. Reznick RK, Smee S, Baumber JS, et al. Guidelines for estimating the real cost of an objective structured clinical examination. Acad Med. 1993;68(7):513–517. doi:10.1097/00001888-199307000-00001
10. Weller JM, Nestel D, Marshall SD, Brooks PM, Conn JJ. Simulation in clinical teaching and learning. Med J Aust. 2012;196(9):594. doi:10.5694/mja10.11474
11. Khan KZ, Ramachandran S, Gaunt K, Pushkar P. The objective structured clinical examination (OSCE): AMEE guide no. 81. part I: an historical and theoretical perspective. Med Teach. 2013;35(9):e1437–e1446. doi:10.3109/0142159X.2013.818634
12. Patrício MF, Julião M, Fareleira F, Carneiro AV. Is the OSCE a feasible tool to assess competencies in undergraduate medical education? Med Teach. 2013;35(6):503–514. doi:10.3109/0142159X.2013.774330
13. Shaban S, Tariq I, Elzubeir M, Alsuwaidi AR, Basheer A, Magzoub M. Conducting online OSCEs aided by a novel time management web-based system. BMC Med Educ. 2021;21(1):508. doi:10.1186/s12909-021-02945-9
14. Blythe J, Patel NSA, Spiring W, et al. Undertaking a high stakes virtual OSCE (“VOSCE”) during Covid-19. BMC Med Educ. 2021;21(1):221. doi:10.1186/s12909-021-02660-5
15. Cianciolo AT, LaVoie N, Parker J. Machine scoring of medical students’ written clinical reasoning: initial validity evidence. Acad Med. 2021;96(7):1026–1035. doi:10.1097/ACM.0000000000004010
16. Bayoumy K, Gaber M, Elshafeey A, et al. Smart wearable devices in cardiovascular care: where we are and how to move forward. Nat Rev Cardiol. 2021;18(8):581–599. doi:10.1038/s41569-021-00522-7
17. Talbot T, Rizzo AS. Virtual human standardized patients for clinical training. In: Rizzo AS, Bouchard S, editors. Virtual Reality for Psychological and Neurocognitive Interventions. New York: Springer; 2019:387–405.
18. Mahmud M, Sari DCR, Sari D, Arfian N, Zucha MA. The application of augmented reality for improving clinical skills: a scoping review. Korean J Med Educ. 2024;36(1):65–79. doi:10.3946/kjme.2024.285
19. Cummings JJ, Bailenson JN. How immersive is enough? A meta-analysis of the effect of immersive technology on user presence. Media Psychol. 2016;19(2):272–309. doi:10.1080/15213269.2015.1015740
20. Cipresso P, Giglioli IAC, Raya MA, Riva G. The past, present, and future of virtual and augmented reality research: a network and cluster analysis of the literature. Front Psychol. 2018;9:2086. doi:10.3389/fpsyg.2018.02086
21. Radianti J, Majchrzak TA, Fromm J, Wohlgenannt I. A systematic review of immersive virtual reality applications for higher education: design elements, lessons learned, and research agenda. Comput Educ. 2020;147:103778. doi:10.1016/j.compedu.2019.103778
22. Berkman MI, Akan E. Presence and immersion in virtual reality. Encyclopedia of Computer Graphics and Games. Springer; 2018.
23. Adamovich SV, Fluet GG, Tunik E, Merians AS. Sensorimotor training in virtual reality: a review. Neurorehabilitation. 2009;25(1):29–44. doi:10.3233/NRE-2009-0497
24. Cinar OE, Rafferty K, Cutting D, Wang H. AI-powered VR for enhanced learning compared to traditional methods. Electronics. 2024;13(23):4787. doi:10.3390/electronics13234787
25. Vemuri N, Thaneeru N, Tatikonda V. Cloud-based virtual reality (VR) in education. Int J Res Pub Rev. 2024;5(2):2300–2309. doi:10.55248/gengpi.5.0224.0543
26. Morin DG, Perez P, Armada AG. Toward the distributed implementation of immersive augmented reality architectures on 5G networks. IEEE Commun Mag. 2022;60(2):46–52. doi:10.1109/MCOM.001.2100225
27. Pottle J. Virtual reality and the transformation of medical education. Future Healthc J. 2019;6(3):181–185. doi:10.7861/fhj.2019-0036
28. Courteille O, Bergin R, Stockeld D, Ponzer S, Fors U. The use of a virtual patient case in an OSCE-based exam--a pilot study. Med Teach. 2008;30(3):e66–e76. doi:10.1080/01421590801910216
29. Slater M, Sanchez-Vives MV. Enhancing our lives with immersive virtual reality. Front Robot AI. 2016;3:74.
30. LaValle SM. Virtual Reality. Cambridge University Press; 2019.
31. Cook DA, Erwin PJ, Triola MM. Computerized virtual patients in health professions education: a systematic review and meta-analysis. Acad Med. 2010;85(10):1589–1602. doi:10.1097/ACM.0b013e3181edfe13
32. Tong K, McMahon E, Reid-McDermott B, Byrne D, Doherty AM. SafePsych: improving patient safety by delivering high-impact simulation training on rare and complex scenarios in psychiatry. BMJ Open Qual. 2021;10(3):e001533. doi:10.1136/bmjoq-2021-001533
33. Alruwaili AN, Alshammari AM, Alhaiti A, Elsharkawy NB, Ali SI, Ramadan OME. Virtual reality simulation for high-risk neonatal emergency nursing training: a mixed-methods study on nurse competency and outcomes. BMC Nurs. 2025;24(1):367. doi:10.1186/s12912-025-03038-4
34. Schmidt C, Kesztyüs D, Haag M, Wilhelm M, Kesztyüs T. Proposal of a method for transferring high-quality scientific literature data to virtual patient cases using categorical data generated by bernoulli-distributed random values: development and prototypical implementation. JMIR Med Educ. 2023;9:e43988. doi:10.2196/43988
35. Borg Sapiano A, Sammut R, Trapani J. The effectiveness of virtual simulation in improving student nurses’ knowledge and performance during patient deterioration: a pre and post test design. Nurse Educ Today. 2018;62:128–133. doi:10.1016/j.nedt.2017.12.025
36. Ziv A, Wolpe PR, Small SD, Glick S. Simulation-based medical education: an ethical imperative. Acad Med. 2003;78(8):783–788. doi:10.1097/00001888-200308000-00006
37. Kleinert R, Wahba R, Chang DH, Plum P, Hölscher AH, Stippel DL. 3D immersive patient simulators and their impact on learning success: a thematic review. J Med Internet Res. 2015;17(4):e91. doi:10.2196/jmir.3492
38. Lateef F. Simulation-based learning: just like the real thing. J Emerg Trauma Shock. 2010;3(4):348–352. doi:10.4103/0974-2700.70743
39. McGaghie WC, Issenberg SB, Petrusa ER, Scalese RJ. A critical review of simulation-based medical education research: 2003-2009. Med Educ. 2010;44(1):50–63. doi:10.1111/j.1365-2923.2009.03547.x
40. Huang TK, Yang CH, Hsieh YH, Wang JC, Hung CC. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J Med Sci. 2018;34(4):243–248. doi:10.1016/j.kjms.2018.01.009
41. Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005;27(1):10–28. doi:10.1080/01421590500046924
42. Yiannakopoulou E, Nikiteas N, Perrea D, Tsigris C. Virtual reality simulators and training in laparoscopic surgery. Int J Surg. 2015;13:60–64. doi:10.1016/j.ijsu.2014.11.014
43. Alaker M, Wynn GR, Arulampalam T. Virtual reality training in laparoscopic surgery: a systematic review & meta-analysis. Int J Surg. 2016;29:85–94. doi:10.1016/j.ijsu.2016.03.034
44. Marougkas A, Troussas C, Krouska A, Sgouropoulou C. Virtual reality in education: a review of learning theories, approaches and methodologies for the last decade. Electronics. 2023;12(13):2832. doi:10.3390/electronics12132832
45. Proceedings of the 30th ACM symposium on virtual reality software and technology. Association for Computing Machinery, New York, NY, USA; 2024.
46. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
47. Neher AN, Bühlmann F, Müller M, Berendonk C, Sauter TC, Birrenbach T. Virtual reality for assessment in undergraduate nursing and medical education - a systematic review. BMC Med Educ. 2025;25(1):292. doi:10.1186/s12909-025-06867-8
48. Gandsas A, Dorey T, Park A. Immersive live streaming of surgery using 360-degree video to head-mounted virtual reality devices: a new paradigm in surgical education. Surg Innov. 2023;30(4):486–492. doi:10.1177/15533506231165828
49. Kiegaldie D, Shaw L. Virtual reality simulation for nursing education: effectiveness and feasibility. BMC Nurs. 2023;22(1):488. doi:10.1186/s12912-023-01639-5
50. Tabatabai S. Simulations and virtual learning supporting clinical education during the COVID 19 pandemic [Response To Letter]. Adv Med Educ Pract. 2020;11:669–671. doi:10.2147/AMEP.S280840
51. Chao YP, Chuang HH, Hsin LJ, et al. Using a 360° virtual reality or 2D video to learn history taking and physical examination skills for undergraduate medical students: pilot randomized controlled trial. JMIR Serious Games. 2021;9(4):e13124. doi:10.2196/13124
52. Long Y, Zhang X, Zeng X. Application and effect analysis of virtual reality technology in vocational education practical training. Educ Inf Technol. 2024;30(7):9755–9786.
53. Yang H, Cai M, Diao Y, Liu R, Liu L, Xiang Q. How does interactive virtual reality enhance learning outcomes via emotional experiences? A structural equation modeling approach. Front Psychol. 2023;13:1081372. doi:10.3389/fpsyg.2022.1081372
54. Mühling T, Schreiner V, Appel M, Leutritz T, König S. Comparing virtual reality-based and traditional physical objective structured clinical examination (OSCE) stations for clinical competency assessments: randomized controlled trial. J Med Internet Res. 2025;27:e55066. doi:10.2196/55066
55. Shaikh TA, Dar TR, Sofi S. A data-centric artificial intelligent and extended reality technology in smart healthcare systems. Soc Netw Anal Min. 2022;12(1):122. doi:10.1007/s13278-022-00888-7
56. Farra SL, Gneuhs M, Hodgson E, et al. Comparative cost of virtual reality training and live exercises for training hospital workers for evacuation. Computers Inform Nurs. 2019;37(9):446–454. doi:10.1097/CIN.0000000000000540
57. Al-Mfarej D, Vojtech JM, Roy SH, et al. A virtual reality exergame: clinician-guided breathing and relaxation for children with muscular dystrophy. 2023 IEEE Conf Virtual Real 3D User Interfaces Abstr Workshops. 2023;2023:270–276. doi:10.1109/vrw58643.2023.00065
58. Concannon BJ, Esmail S, Roduta Roberts M. Immersive virtual reality for the reduction of state anxiety in clinical interview exams: prospective cohort study. JMIR Serious Games. 2020;8(3):e18313. doi:10.2196/18313
59. Riddle EW, Kewalramani D, Narayan M, Jones DB. Surgical simulation: virtual reality to artificial intelligence. Curr Probl Surg. 2024;61(11):101625. doi:10.1016/j.cpsurg.2024.101625
60. Huang H, Yin J, Lv F, Lin Y, Zou J. A study on the impact of open source metaverse immersive teaching method on emergency skills training for medical undergraduate students. BMC Med Educ. 2024;24(1):859. Erratum in: BMC Med Educ. 2024 Dec 11;24(1):1427. doi:10.1186/s12909-024-05862-9
61. Khan A, Rodwell V, Luhar L, et al. Virtual reality 360-degree films for objective structured clinical examination preparation: a descriptive study. Cureus. 2025;17(1):e78120. doi:10.7759/cureus.78120
62. Gan W, Mok TN, Chen J, et al. Researching the application of virtual reality in medical education: one-year follow-up of a randomized trial. BMC Med Educ. 2023;23(1):3. doi:10.1186/s12909-022-03992-6
63. Boden KT, Rickmann A, Fries FN, et al. Evaluierung eines VR-Simulators zum Erlernen der direkten Ophthalmoskopie in der studentischen Lehre [Evaluation of a virtual reality simulator for learning direct ophthalmoscopy in student teaching]. Ophthalmologe. 2020;117(1):44–49. doi:10.1007/s00347-019-0909-z
64. Chang E, Kim HT, Yoo B. Virtual reality sickness: a review of causes and measurements. Int J Hum Comput Interact. 2020;36(17):1658–1682. doi:10.1080/10447318.2020.1778351
65. Schleicher I, Leitner K, Juenger J, et al. Examiner effect on the objective structured clinical exam - a study at five medical schools. BMC Med Educ. 2017;17(1):71. doi:10.1186/s12909-017-0908-1
66. Afzal A, Khan S, Daud S, Ahmed Z, Butt A. Addressing the digital divide: access and use of technology in education. J Soc Sci Rev. 2023;3:883–895.
67. Gorshkov M. To Err is Human, To Teach VR. In: Virtual Reality and Artificial Intelligence in Medical Education. Germany: EuroMedSim; 2024.
68. Eswaran M, Bahubalendruni MVAR. Challenges and opportunities on AR/VR technologies for manufacturing systems in the context of industry 4.0: a state of the art review. J Manuf Syst. 2022;65:260–278. doi:10.1016/j.jmsy.2022.09.016
69. Misra SM, Suresh S. Artificial intelligence and objective structured clinical examinations: using ChatGPT to revolutionize clinical skills assessment in medical education. J Med Educ Curric Dev. 2024;11. doi:10.1177/23821205241263475
70. Lin PY, Tsai YH, Chen TC, et al. The virtual assessment in dental education: a narrative review. J Dent Sci. 2024;19(Suppl 2):S102–S115. doi:10.1016/j.jds.2024.10.012
71. Liu P, Dong X, Liu F, Fu H. Effects of virtual reality OSCE on nursing students’ education: a study protocol for systematic review and meta-analysis. BMJ Open. 2024;14(5):e082847. doi:10.1136/bmjopen-2023-082847
72. Crogman HT, Cano VD, Pacheco E, Sonawane RB, Boroon R. Virtual reality, augmented reality, and mixed reality in experiential learning: transforming educational paradigms. Educ Sci. 2025;15(3):303. doi:10.3390/educsci15030303
73. Maleki Varnosfaderani S, Forouzanfar M. The role of AI in hospitals and clinics: transforming healthcare in the 21st century. Bioengineering. 2024;11(4):337. doi:10.3390/bioengineering11040337
74. Alowais SA, Alghamdi SS, Alsuhebany N, et al. Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Med Educ. 2023;23(1):689. doi:10.1186/s12909-023-04698-z
75. Hazarika A, Rahmati M. Towards an evolved immersive experience: exploring 5G- and beyond-enabled ultra-low-latency communications for augmented and virtual reality. Sensors. 2023;23(7):3682. doi:10.3390/s23073682
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.