Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Frequent nightmares in Chinese patients undergoing methadone maintenance therapy: prevalence, correlates, and their association with functional impairment
Authors Zhong BL ![]() , Xu YM, Xie WX, Lu J
, Xu YM, Xie WX, Lu J
Received 24 January 2019
Accepted for publication 2 July 2019
Published 18 July 2019 Volume 2019:15 Pages 2063—2072
DOI https://doi.org/10.2147/NDT.S202813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jun Chen
Bao-Liang Zhong,1,2 Yan-Min Xu,2 Wu-Xiang Xie,3 Jin Lu4
1Research Center for Psychological and Health Sciences, China University of Geosciences, Wuhan, Hubei Province, People’s Republic of China; 2Affiliated Wuhan Mental Health Center, Tongji Medical College of Huazhong University of Science & Technology, Wuhan, Hubei Province, People’s Republic of China; 3Peking University Clinical Research Institute, Peking University Health Science Center, Beijing, People’s Republic of China; 4Department of Psychiatry, The First Affiliated Hospital of Kunming Medical University, Kunming, People’s Republic of China
Purpose: Nightmares are associated with many negative health outcomes; however, little is known about the characteristics of nightmares in heroin-dependent patients (HDPs). This study examined the prevalence and correlates of frequent nightmares (FNs) and their association with functional impairment in Chinese patients undergoing methadone maintenance therapy (MMT).
Patients and methods: In total, 603 Chinese HDPs from three MMT clinics in Wuhan, China, completed this survey. FNs were defined as reporting nightmares at least once a week. The Sheehan Disability Scale (ShDS) was used to assess the severity of functional impairment of patients. A standardized questionnaire was used to collect data on socio-demographics, drug use characteristics, physical health, mental health, and insomnia.
Results: The prevalence of FNs in Chinese HDPs receiving MMT was 25.9%. Factors significantly associated with nightmares among MMT HDPs included an educational attainment of senior high school and above (OR=2.73, P<0.001), unemployment (OR=3.16, P<0.001), a history of re-education through forced labor (OR=3.14, P<0.001), injecting heroin before MMT (OR=3.62, P=0.002), a high dose of methadone (>70 mg/day) (OR=2.03, P=0.006), use of hypnotics (OR=1.91, P=0.044), the presence of hepatitis B virus core antibody (OR=4.63, P<0.001), pain (OR=3.20, P<0.001), anxiety (OR=2.06, P=0.039), and insomnia (OR=5.75, P<0.001). After controlling for potential confounders, nightmares were still significantly associated with a higher ShDS score (β=2.718, P=0.006).
Conclusion: FNs are prevalent among Chinese HDPs receiving MMT and significantly associated with functional impairment. Nightmares are a clinically relevant phenomenon in Chinese MMT clinics, which deserves more clinical and research attention.
Keywords: nightmare, methadone maintenance therapy, functional impairment, sleep disorder
Introduction
A nightmare is a disturbing dream that leads to intense emotional reactions such as anxiety, distress, and fear and often wakes the dreamer.1 Nightmares are common in the general population, occurring weekly in 2–6% and 20% of the adults and children in western countries, and in 5.1% and 5.2% of the adults and children in China, respectively.2–6 Although the underlying etiology of nightmares is still unclear, accumulating evidence suggests that frequent nightmares (FNs) are significantly associated with considerable personal distress, a constellation of psychopathological symptoms, fatal and non-fatal suicidal behaviors, insomnia, and poor sleep quality.5,7–10 Compared to the general population, patients with mental disorders experience more FNs and have a greater number of nightmare episodes.3,9,11 Further studies have revealed the significant associations of FNs with higher risk of suicide in patients with major depression, greater level of distress in patients with schizophrenia, poorer sleep quality and greater delusion severity in patients with psychosis, and interrupted rapid eye movement (REM) sleep and poorer treatment outcome in patients with post-traumatic stress disorder.12–16
Sleep disorders are a major health concern for both patients with heroin dependence and heroin-dependent patients (HDPs) receiving methadone maintenance therapy (MMT).17 It has been estimated that prevalence rates of difficulty in initiating sleep (DIS), difficulty in maintaining sleep (DMS), and poor sleep quality of clients receiving MMT are 30.8%, 29.8%, and 80.8%, respectively.18–20 However, in contrast to the numerous studies on sleep quality and insomnia of HDPs, few studies have investigated nightmares in HDPs, including those under MMT. As far as we know, only one previous qualitative study with a small sample of 32 MMT clients described “horrible nightmares” as a negative effect of MMT, but provided little information on the clinical characteristics of nightmares.21 Nightmares can be triggered or caused by many factors, including traumatic events, medications, depression and other psychiatric disorders, and withdrawal from psychoactive drugs such as heroin.22–24 In the case of MMT HDPs, because they frequently suffer from depression and anxiety, use multiple drugs, and are in the prolonged withdrawal period, it would be reasonable to hypothesize that nightmares would be very prevalent among HDPs undergoing MMT, and they will be associated with a number of drug use characteristics and clinical factors.25–28 Nonetheless, empirical evidence for this is lacking.
In China, MMT is a national strategy to address the issue of heroin and other opioids use. Chinese researchers have found that MMT is effective in relieving patients’ withdrawal symptoms and cravings for heroin, improving patients’ health and social well-being, and reducing the transmission of infectious diseases (ie, hepatitis and HIV) and criminal activities associated with heroin use.29,30 However, results from comparative studies show that physical and psychological quality of life and functioning of Chinese MMT patients are still poorer than healthy controls, largely because most MMT clinics in China provide MMT only and many psychosocial and sleep problems of Chinese MMT patients are neglected and undertreated.17,31–35 To increase health care providers’ awareness on the importance of these issues and to meet the psychosocial needs of these patients, a first necessary step is to provide data on the magnitude and characteristics of these psychosocial and sleep problems. Because nightmares are treatable and they have been associated with many health and psychosocial issues, as we reviewed above, interventions aiming at reducing nightmares would produce multiple beneficial effects for the health of MMT patients.36 Further, MMT clinics are very well-placed to provide psychosocial services to address nightmares of HDPs, because this patient population treated at MMT clinics is relatively stable and can be easily followed up. Unfortunately, so far, the lack of data on the clinical characteristics of nightmares in patients may have hindered the clinical application of several effective treatments for nightmares in China’s MMT settings.
Social and occupational dysfunctions resulted from nightmares have been reported in studies with patients other than HDPs.37 Although several factors such as depression and poor physical health have been found to be associated with functioning impairment in patients receiving MMT, it remains unclear whether nightmares are significantly associated with functional impairment of HDPs.31 Given the ultimate treatment goal of “returning to a normal life” of MMT, it is also important to investigate potentially modifiable factors associated with functional impairment such as nightmares.38
The current study was carried out to examine the prevalence and correlates of FNs in a large sample of HDPs of Chinese MMT clinics and the relationship between nightmares and functional impairment.
Materials and methods
Participants
Participants were subjects of a previous cross-sectional study at three municipality-owned MMT clinics in Wuhan, a large metropolitan city with over 10 million inhabitants in central-south China.27,39 Participants were outpatients of the three clinics during the study period. To be eligible for the study, patients must be at least 20 years old, meet Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria for a lifetime diagnosis of heroin dependence, be receiving MMT at the time of the survey, and voluntarily join the study.40 We excluded patients who suffered from severe physical illnesses, alcohol addiction, or psychotic symptoms. During the study period, all patients of the three selected clinics (n=743) were screened for eligibility and 652 met the study inclusion criteria. Because 33 patients did not complete the survey questionnaires and 16 withdrew informed consent, a final sample of 603 MMT patients was obtained for the current analysis.
Prior to the formal study, the study protocol was approved by the Ethics Committee of Wuhan Mental Health Center. The protocol including the methods was performed in accordance with the Declaration of Helsinki and the relevant ethical guidelines and regulations in China. All patients signed the informed consent before inclusion.
Procedures and instruments
After the informed consent, all patients were instructed to independently and anonymously complete the survey questionnaire, which was standardized and finalized after a pilot testing with a sample of 48 MMT patients. Trained investigators were assigned to assist patients who had difficulty in filling the questionnaires and collect patients’ clinical data from their medical records, including methadone dose and infection status of hepatitis B virus (HBV) and hepatitis C virus (HCV).
The survey questionnaire had seven parts: a) socio-demographic variables (gender, age, education, marital status, and self-rated economic status); b) drug use characteristics (history of “re-education through forced labor,” main route of heroin use, duration of heroin use, length of MMT, current methadone dose, currently smoking, currently drinking, and current use of hypnotics); c) physical health (infection status of HBV and HCV, and pain); d) mental health (depressive and anxiety symptoms); e) insomnia (DIS, DMS, and early morning awakening [EMA]); f) nightmares; and g) functional impairment.
Two questions were used to elicit cigarette smoking behavior: a) “On average, do you smoke daily now?” and b) “How long have you smoked?”. Questions used for drinking and use of hypnotics were: “Did you drink at least once per month over the past 6 months?” and “During the past month, did you take sleeping pills (prescribed or ‘over the counter’) at least once per week?”, respectively. Currently, smoking was defined as having smoked for at least half a year and now smoked at least one cigarette per day.41 Currently drinking referred to drinking monthly during the past 6 months.42 Current use of hypnotics was defined as the use of any hypnotics at least once a week during the past month. Although the use of sedative hypnotics is generally the result of nightmares and nightmares-associated insomnia, there is also evidence that the use of some hypnotics (ie, temazepam and triazolam) would cause nightmares.43,44 We therefore considered the use of hypnotics as a candidate correlate of nightmares in this study.
HBV infection status was denoted by the test results of HBV surface antigen (HBsAg) and HBV core antibody (HBcAb). HCV infection status was denoted by the test result of HCV antibody (HCAb). The 5-point Verbal Rating Scale was used to measure pain intensity: “Overall, how intense is your pain now?,“ which was rated on a 5-point scale from 1=none to 5=very severe. Respondents who answered “moderate,” “severe,” and “very severe” were categorized as having clinically significant pain.26
Depressive and anxiety symptoms were evaluated with the validated Chinese Zung’s Self-rating Depression Scale (SDS) and Zung’s Self-rating Anxiety Scale (SAS), respectively.45 Both scales have 20 items and responses to all items are scored from 1=a little of the time to 4=most of the time. In China, total crude scores of ≥40 on SDS and ≥43 on SAS are used to denote clinically significant depression and anxiety, respectively.25,46
In this study, insomnia during the prior month included three basic forms: DIS (“How often have you had difficulties in getting to sleep?”), DMS (“How often have you had difficulties in maintaining sleep and waked up in the middle of night?”), and EMA (“How often have you waked up in the early morning and had difficulties in falling sleep again?”).5,47 The presence of insomnia was defined by an “often” response to any of the three questions.
In accordance with previous studies, we used one single question to assess nightmares: “How often have you had nightmares during the past month?” with a particular definition of nightmares given: “Here ‘nightmares’ refer to intense, emotionally negative mental experiences that often occur during late-night sleep and lead to abrupt awakenings”.5,7,48,49 Frequency of nightmares was rated on a 4-point scale (1=none, 2=less than once a week, 3=once or twice a week, 4=three or more times a week). FNs refer to reporting nightmares at least once a week.5,7,48,49 As one of our quality control measures, six trained psychiatrists were required to immediately check the completeness of all answers in the questionnaires before collecting patients’ questionnaires. Patients who endorsed nightmares in their questionnaires were further interviewed face-to-face by these psychiatrists to ascertain the presence of nightmares and exclude the false-positive cases with bad dreams, sleep terrors, sleep walking, and nocturnal panic attack.
The validated Chinese Sheehan Disability Scale (ShDS) was used to assess the severity of functional impairment of MMT patients.50,51 The ShDS has three items, which assess functional impairments associated with work/school, social life and leisure activities, and family life and home responsibilities. Each item is rated on an ordered metric scale from 0 (not at all) to 10 (very severely). The total score of ShDS ranges from 0 (unimpaired) to 30 (highly impaired), with a higher total score representing a greater functional impairment.
Statistical analysis
Prevalence rates of FNs in the whole patient sample and different patient cohorts were calculated and the chi-squared test was used to compare rates between groups. Multivariable logistic regression model with backward stepwise selection that entered significant variables in the chi-squared test as independent variables and nightmares as the dependent variable was used to identify factors significantly and independently associated with nightmares. OR and 95% CIs were used to quantify the associations between factors and nightmares. Independent samples Mann–Whitney U test was used to compare ShDS scores of patients with and without nightmares. Multiple linear regression models were used to examine the strength of association between nightmares and ShDS score, controlling for socio-demographic variables, drug use characteristics, physical health, mental health, and insomnia. The statistical significance level was set P<0.05 (two-sided). SPSS software version 15.0 package was used for all analyses (SPSS Inc., Chicago, IL, USA).
Results
The mean age of the 603 MMT HDPs was 38.1 years (SD=7.0, range=21–59) and 69.8% were males. The prevalence of HBsAg, HBcAb, and HCAb was 22.7%, 20.6%, and 78.1%, respectively. Detailed socio-demographic and drug use characteristics of the patient sample are shown in Table 1.
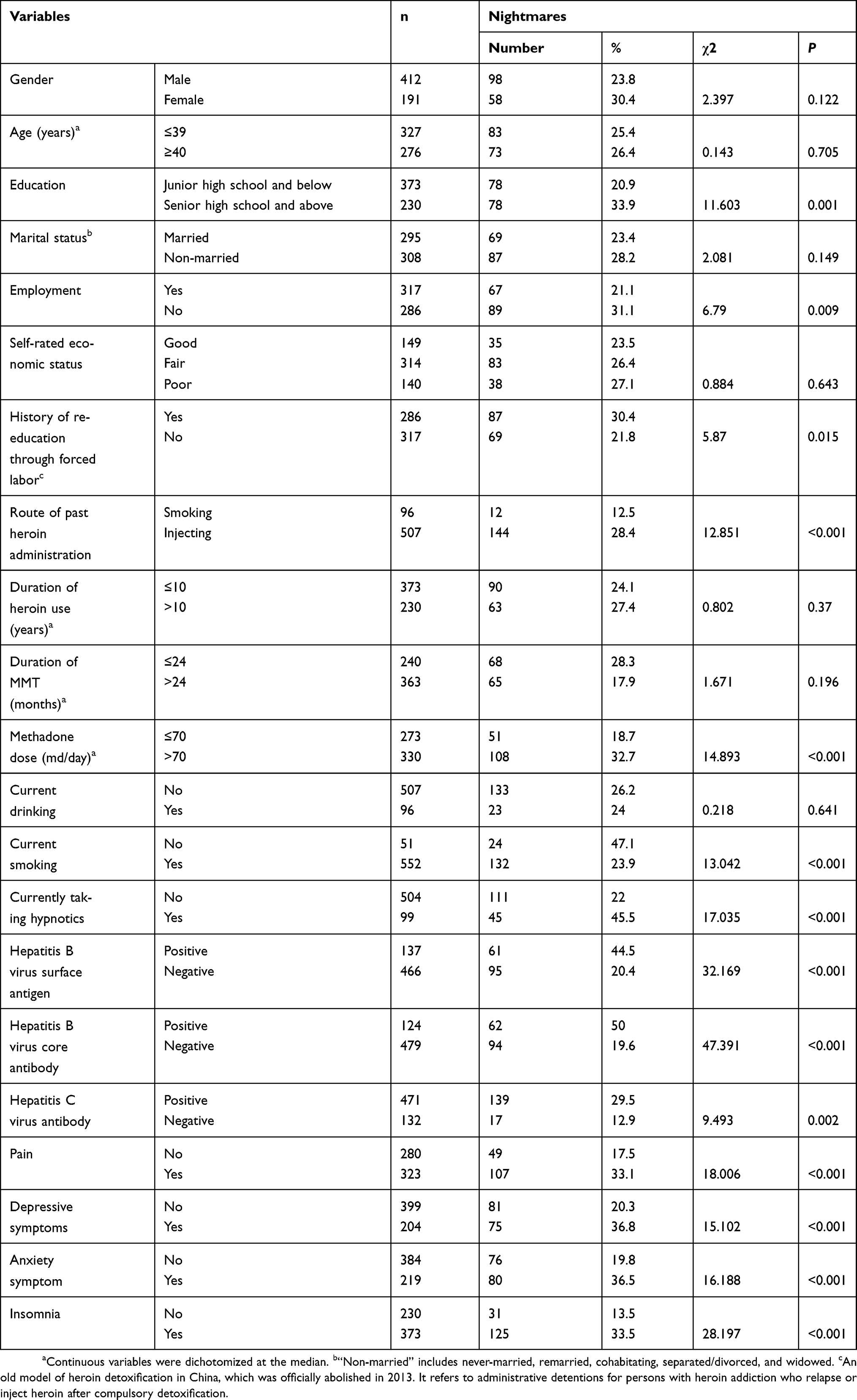 |
Table 1 Characteristics of the sample of Chinese methadone-maintained heroin-dependent patients, and prevalence rates of frequent nightmares according to variables |
In total, 156 MMT clients endorsed FNs. Prevalence of FNs was 25.9% in the whole sample of Chinese HDPs receiving MMT, with 23.8% in men and 30.4% in women. Although higher rates of nightmares in women than men were observed, their difference did not reach statistically significant level (P=0.122). Results from Chi-squared tests (Table 1) show that patients having nightmares were more likely to have an educational attainment of senior high school and above (P=0.001), be unemployed (P=0.009), have a history of re-education through forced labor (P=0.015), inject heroin before MMT (P<0.001), take a high dose of methadone (>70 mg/day) (P<0.001), be non-smokers (P<0.001), take hypnotics (P<0.001), have a positive HBsAg test result (P<0.001), have a positive HBcAb test result (P<0.001), have a positive HCAb test result (P=0.002), feel pain (P<0.001), be depressed (P<0.001), be anxious (P<0.001), and have insomnia (P<0.001).
Multivariable logistic regression analysis (Table 2) shows that an educational attainment of senior high school and above (OR=2.73, P<0.001), unemployment (OR=3.16, P<0.001), a history of re-education through forced labor (OR=3.14, P<0.001), injecting heroin before MMT (OR=3.62, P=0.002), a high dose of methadone (>70 mg/day) (OR=2.03, P=0.006), use of hypnotics (OR=1.91, P=0.044), the presence of HBcAb (OR=4.63, P<0.001), pain (OR=3.20, P<0.001), anxiety (OR=2.06, P=0.039), and insomnia (OR=5.75, P<0.001) were significantly associated with nightmares among MMT HDPs.
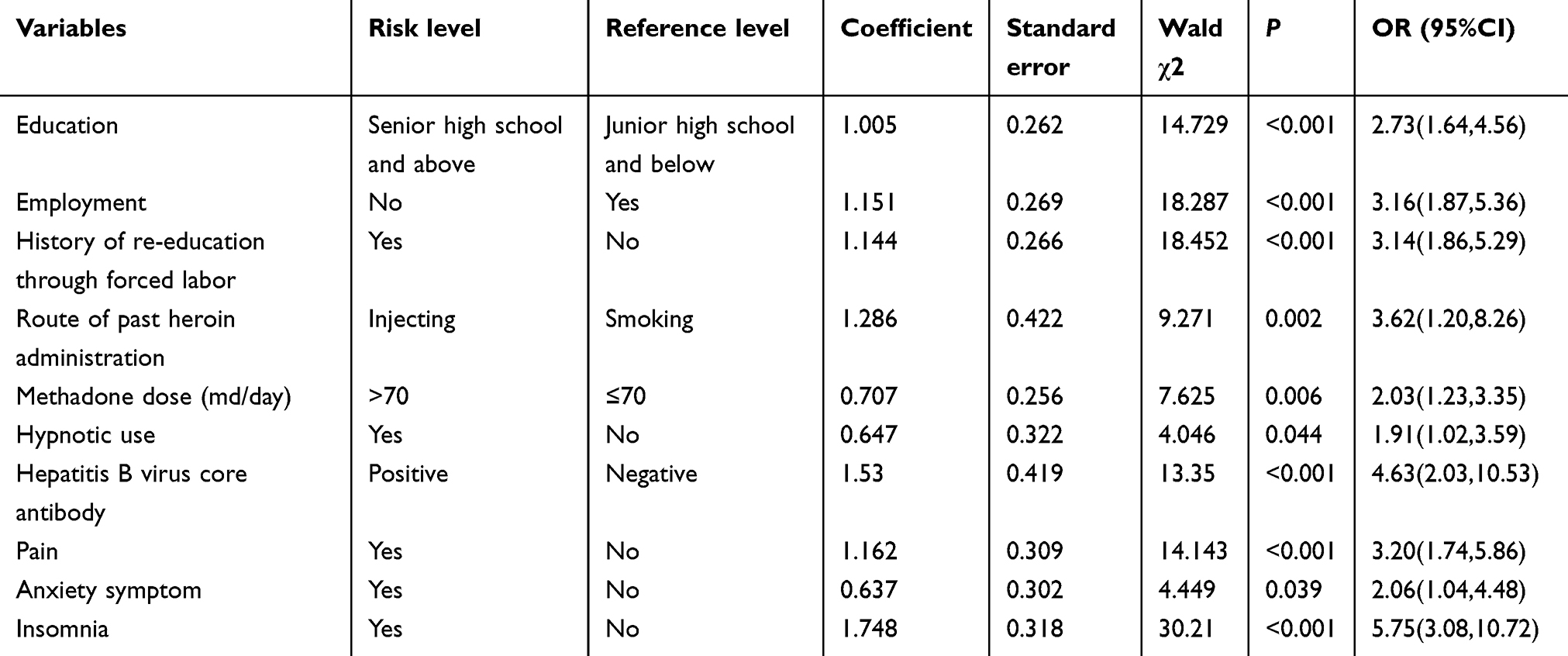 |
Table 2 Results of multiple logistic regression analysis on factors significantly associated with frequent nightmares in Chinese methadone-maintained heroin-dependent patients |
Total ShDS scores were significantly higher in clients with nightmares than those without nightmares ([median, interquartile]: [9, 13] vs [6, 14], z=3.887, P<0.001). After controlling for potential confounders (including socio-demographic variables, drug use characteristics, physical health, mental health, and insomnia), results from multiple linear regression analysis (Table 3) reveal that nightmares were still significantly associated with a higher ShDS score (β=2.718, P=0.006).
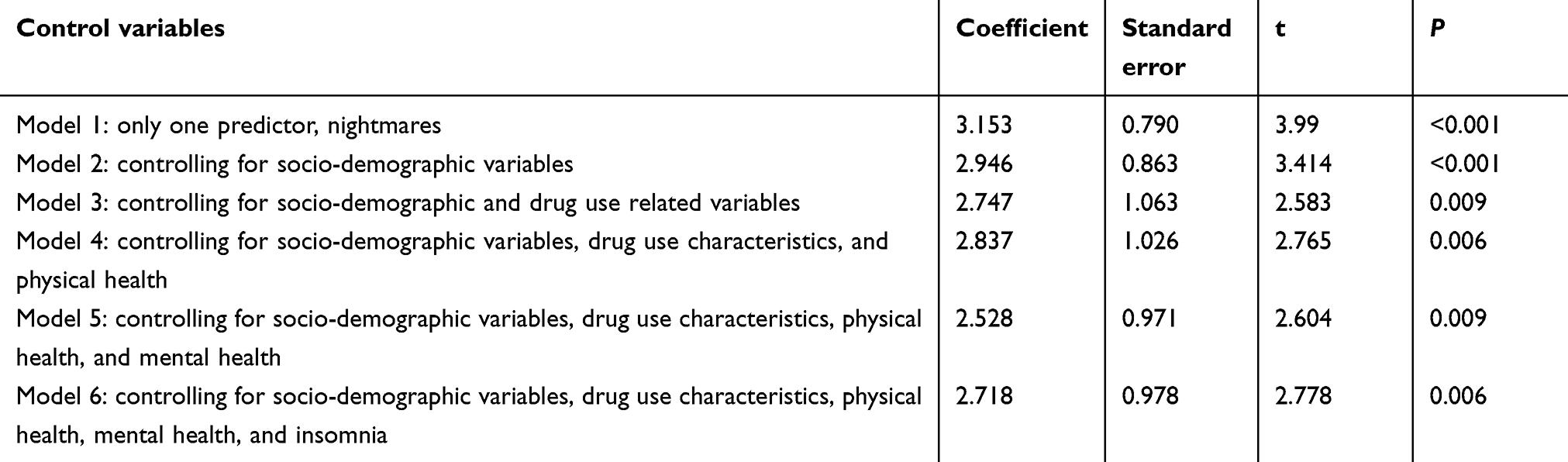 |
Table 3 Results of multiple linear regression analysis on the relationship between frequent nightmares and functional impairment, as measured by Sheehan Disability Scale |
Discussion
To the best of our knowledge, this is the first study examining the clinical characteristics of nightmares in Chinese MMT HDPs, as well as their association with functional impairment. Main findings of this study are: a) an overall prevalence of 25.9% of FNs in Chinese MMT patients, without significant gender difference; b) significant correlates of nightmares of Chinese MMT HDPs: an educational attainment of senior high school and above, unemployment, a history of re-education through forced labor, injecting heroin before MMT, a high dose of methadone (>70 mg/day), use of hypnotics, the presence of HBcAb, pain, anxiety, and insomnia; and c) a significant positive association between nightmares and a greater degree of functional impairment in Chinese MMT HDPs, net of potential confounding effects of socio-demographic variables, drug use characteristics, physical health, mental health, and insomnia.
In the general populations of Western countries, FNs are more common in children (20%) than adults (2–6%), and in women than men.2,3,52 In the Chinese general population, the prevalence of FNs in children and adults is 5.2% and 5.1%, respectively.5,6 Compared to these estimates of general population, we found a higher prevalence of FNs in Chinese MMT HDPs (25.9%); this finding is in line with the assertion that nightmares are more frequent among psychiatric populations.3 Because nightmares are often viewed as a sign of psychopathology, the high prevalence of FNs in MMT patients is expected.3 Moreover, in addition to the aforementioned high levels of depression and anxiety, and withdrawal from psychoactive drugs, we speculate that a high level of stress also explains the high prevalence of nightmares in MMT patients, because this patient population often experiences stressful events and nightmares tend to occur during periods of stress.3,53 Because socialization processes differ between genders, nightmares are more common in females than males.54 Nevertheless, we failed to replicate such gender difference in MMT patients. Given the relatively large gap in the prevalence of nightmares between males and females (6.6%), the primary reason for this inconsistency should be the relatively small sample size of MMT patients, which is not large enough to detect this difference. Other strong risk factors of nightmares such as insomnia might also influence or mask the effect of gender on the occurrence of nightmares.
Previous studies have reported the significant link between nightmares and lower socioeconomic status such as low family income.5,6 Both education and employment status are important indicators of socioeconomic status, but we found opposite associations between the two indicators and nightmares.55 Strictly speaking, the presence of nightmares may partly depend on an individual’s ability to remember a dream upon awakening, because some persons may simply forget their dreams, even if they have experienced nightmares during sleep. Considering the positive association between education and cognitive reserve, and impaired memory resulted from heroin use, higher prevalence of nightmares in patients with an educational attainment of senior high school (vs junior high school and below) might be due to their less severe memory impairment.56,57
Re-education through forced labor was a problematic treatment approach for heroin detoxification in China, which contained some compulsory measures, including restricting the freedom of heroin users and “re-educating” them through penal labor without judicial review. Due to some reasons, this treatment would become a stressor for Chinese HDPs, possibly resulting in elevated risk of nightmares.
Most dreams (including nightmares) occur during the REM stage of sleep. Evidence from polysomnography studies has shown that REM rebound, the lengthening and increasing frequency and depth of REM, plays an important role in the occurrence of dreaminess and nightmares.58,59 Because of the suppression effect of opioid administration on REM sleep, REM rebound happens after heroin withdrawal, as a result of a compensatory increase in REM sleep.60 Since injecting heroin is indicative of more severe heroin dependence, patients who injected heroin would have more severe REM rebound after withdrawal, resulting in an increased risk of nightmares.61 The positive association between hypnotics use and nightmares seems not consistent with the fact that many hypnotics are REM sleep-suppressant medications. We speculate that MMT patients may use hypnotics irregularly or at an insufficient dose; therefore, they also frequently suffer from REM rebound resulted from hypnotics withdrawal. The other alternative explanation is that nightmares, as a side effect, can be caused by some hypnotics.41,42 The relationship between a high dose of methadone and nightmares is difficult to explain, because the use of methadone and other opioids is generally associated with REM sleep suppression.23 Nevertheless, some researchers also speculate that the REM sleep suppression would result in an increased intensity of the REM episodes, which in turn increases the likelihood of nightmares.43
One previous study has reported more worries about contamination and illnesses related to HBV infection in HBV carriers, which may be reflected by the content of dreams of patients and result in a higher likelihood of nightmares.62 This may explain the association between nightmares and the presence of HBcAb. Because persons suffering from pain are more likely to have dreams containing pain, the pain-nightmares relationship might be attributed to the painful experience in dreams.63
Consistent with findings from a study based on the Finnish general adult population, insomnia was found to be the strongest correlate of nightmares among MMT patients (OR=5.75).4 This may be due to the reciprocal relationship between the two, for example, nightmares can disrupt the continuity of sleep, leading to DMS, whereas insomnia can cause sleep deprivation, resulting in REM rebound and nightmares.
Indeed, it is not surprising to find the significant contribution of FNs on functional impairment of MMT patients, because their associated psychopathology may mediate the effect of FNs on functional impairment. Nevertheless, we further found the nightmares-functioning association was independent of a variety of covariates, including psychopathology and insomnia, suggesting that nightmares may also independently influence the function of MMT patients.
This study has some limitations. First, stress plays an important role in the etiology of nightmares but we did not measure stressful life events and level of stress of MMT patients. Second, we did not assess the type of nightmares and collect data on the nightmare content. Third, although REM rebound involves in the occurrence of nightmares, we did not use polysomnography to evaluate the sleep architecture due to our limited research budget. Further studies using polysomnography and collecting data on past traumatic events, and type and content of nightmares would deepen our understanding on nightmares of MMT patients. Fourth, since this is a self-report survey, the prevalence of FNs might be underestimated due to recall bias. Fifth, no age- and gender-matched healthy controls were recruited for this study. Prevalence rates of FNs reported in the general population-based studies were used as the comparison references. Results from such comparison might be problematic due to problematic comparability between MMT HDPs and the populations studied in the literature.
Conclusion
Nightmares are a treatable sleep condition. There is convincing evidence that nightmares can be effectively treated with pharmacological and psychological treatments such as prazosin and Image Rehearsal Therapy (IRT).36 Given the high prevalence of nightmares and their associations with many negative health outcomes, including functional impairment as revealed in this study, nightmares should be a therapeutic target for improving the health and functioning of patients in China’s MMT clinics. Nevertheless, nightmares are often underreported by methadone-maintained patients or ignored by health care providers in China’s MMT settings. Specialized educational and training programs in sleep medicine are warranted to strengthen health care providers’ ability to recognize, diagnose, and manage nightmares and other sleep problems in MMT clinics. Sleep health education should also be provided to MMT patients to increase their sleep health literacy.
The great number of correlates of nightmares identified in this study also suggest the complexity of nightmares in methadone-maintained HDPs, particularly nightmares’ associations with a high dose of methadone and use of hypnotics. Considering HDPs’ susceptibility to polydrug abuse and the possible interplay among medications, which might complicate the treatment, psychological treatments such as IRT should be considered as the first choice for treating nightmares. Moreover, nightmares of MMT patients are also significantly associated with HBV infection, pain, anxiety, and insomnia, making it necessary to provide appropriate and timely treatments for co-occurring infectious diseases, pain, mental health problems, and other sleep problems in Chinese MMT patients.
Acknowledgments
This study was funded by the Subject Leadership Training Programme for Medicine Discipline of Health and Family Planning Commission of Yunnan Province (D-2017048, J Lu, PI), National Natural Science Foundation of China (71774060, BL Zhong, PI), Wuhan Health and Family Planning Commission (WX17Q30, YM Xu, PI; WG16A02, BL Zhong, PI), and Health and Family Planning Commission of Yunnan Province (2016NS027, J Lu, PI). The funding sources listed here had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. Gauchat A, Seguin JR, Zadra A. Prevalence and correlates of disturbed dreaming in children. Pathol Biol (Paris). 2014;62(5):311–318. doi:10.1016/j.patbio.2014.05.016
3. Nielsen T, Levin R. Nightmares: a new neurocognitive model. Sleep Med Rev. 2007;11(4):295–310. doi:10.1016/j.smrv.2007.03.004
4. Sandman N, Valli K, Kronholm E, Revonsuo A, Laatikainen T, Paunio T. Nightmares: risk factors among the Finnish general adult population. Sleep. 2015;38(4):507–514. doi:10.5665/sleep.4560
5. Li SX, Yu MW, Lam SP, et al. Frequent nightmares in children: familial aggregation and associations with parent-reported behavioral and mood problems. Sleep. 2011;34(4):487–493. doi:10.1093/sleep/34.4.487
6. Li SX, Zhang B, Li AM, Wing YK. Prevalence and correlates of frequent nightmares: a community-based 2-phase study. Sleep. 2010;33(6):774–780. doi:10.1093/sleep/33.6.774
7. Sandman N, Valli K, Kronholm E, Vartiainen E, Laatikainen T, Paunio T. Nightmares as predictors of suicide: an extension study including war veterans. Sci Rep. 2017;7:44756. doi:10.1038/srep44756
8. Sjostrom N, Hetta J, Waern M. Persistent nightmares are associated with repeat suicide attempt: a prospective study. Psychiatry Res. 2009;170(2–3):208–211. doi:10.1016/j.psychres.2008.09.006
9. van Schagen A, Lancee J, Swart M, Spoormaker V, van den Bout J. Nightmare disorder, psychopathology levels, and coping in a diverse psychiatric sample. J Clin Psychol. 2017;73(1):65–75. doi:10.1002/jclp.2017.73.issue-1
10. Simor P, Horvath K, Gombos F, Takacs KP, Bodizs R. Disturbed dreaming and sleep quality: altered sleep architecture in subjects with frequent nightmares. Eur Arch Psychiatry Clin Neurosci. 2012;262(8):687–696.
11. Mume CO. Nightmare in schizophrenic and depressed patients. Eur J Psychiat. 2009;23(3):177–183.
12. Sheaves B, Onwumere J, Keen N, Stahl D, Kuipers E. Nightmares in patients with psychosis: the relation with sleep, psychotic, affective, and cognitive symptoms. Can J Psychiatry. 2015;60(8):354–361. doi:10.1177/070674371506000804
13. Agargun MY, Cilli AS, Kara H, Tarhan N, Kincir F, Oz H. Repetitive and frightening dreams and suicidal behavior in patients with major depression. Compr Psychiatry. 1998;39(4):198–202. doi:10.1016/S0010-440X(98)90060-8
14. Michels F, Schilling C, Rausch F, et al. Nightmare frequency in schizophrenic patients, healthy relatives of schizophrenic patients, patients at high risk states for psychosis, and healthy controls. Int J Dream Res. 2014;7(1):9–13.
15. Habukawa M, Uchimura N, Maeda M, Ogi K, Hiejima H, Kakuma T. Differences in rapid eye movement (REM) sleep abnormalities between posttraumatic stress disorder (PTSD) and major depressive disorder patients: REM interruption correlated with nightmare complaints in PTSD. Sleep Med. 2018;43:34–39. doi:10.1016/j.sleep.2017.10.012
16. Harb GC, Thompson R, Ross RJ, Cook JM. Combat-related PTSD nightmares and imagery rehearsal: nightmare characteristics and relation to treatment outcome. J Trauma Stress. 2012;25(5):511–518. doi:10.1002/jts.21748
17. Li DJ, Chung KS, Wu HC, Hsu CY, Yen CF. Predictors of sleep disturbance in heroin users receiving methadone maintenance therapy: a naturalistic study in Taiwan. Neuropsychiatr Dis Treat. 2018;14:2853–2859. doi:10.2147/NDT.S177370
18. Dunn KE, Finan PH, Andrew Tompkins D, Strain EC. Frequency and correlates of sleep disturbance in methadone and buprenorphine-maintained patients. Addict Behav. 2018;76:8–14. doi:10.1016/j.addbeh.2017.07.016
19. Zhang HS, Xu YM, Zhu JH, Zhong BL. Poor sleep quality is significantly associated with low sexual satisfaction in Chinese methadone-maintained patients. Medicine (Baltimore). 2017;96(39):e8214. doi:10.1097/MD.0000000000008214
20. Xu YM, Zhong BL, Zhu JH, Liu TB. Sleep characteristics of heroin addicts receiving methadone maintenance treatment. Chin J Drug Depend. 2014;23(6):458–463.
21. Kheradmand A, Banazadeh N, Abedi H. Physical effects of methadone maintenance treatment from the standpoint of clients. Addict Health. 2010;2(3–4):66–73.
22. Hasler B, Correlates GA. Treatments of nightmares in adults. Sleep Med Clin. 2009;4(4):507–517. doi:10.1016/j.jsmc.2009.07.012
23. Angarita GA, Emadi N, Hodges S, Morgan PT. Sleep abnormalities associated with alcohol, cannabis, cocaine, and opiate use: a comprehensive review. Addict Sci Clin Pract. 2016;11(1):9. doi:10.1186/s13722-016-0056-7
24. Rochelle Z, Anoop K. 2019. Nightmares and nightmare disorder in adults. In: Eichler AF, Hermann R, editors. UptoDate. Available from: https://www.uptodate.com/contents/nightmares-and-nightmare-disorder-in-adults.
25. Zhong BL, Xu YM, Zhu JH, Liu XJ. Non-suicidal self-injury in Chinese heroin-dependent patients receiving methadone maintenance treatment: prevalence and associated factors. Drug Alcohol Depend. 2018;189:161–165. doi:10.1016/j.drugalcdep.2018.05.006
26. Yang YJ, Xu YM, Chen WC, Zhu JH, Lu J, Zhong BL. Prevalence of pain and its socio-demographic and clinical correlates among heroin-dependent patients receiving methadone maintenance treatment. Sci Rep. 2017;7(1):8840. doi:10.1038/s41598-017-09404-w
27. Xu YM, Zhong BL, Chen WC, Zhu JH, Lu J. Suicidal ideation among Chinese methadone-maintained patients: prevalence and correlates. Oncotarget. 2017;8(49):86181–86187.
28. Chen T, Zhong N, Du J, et al. Polydrug use patterns and their impact on relapse among heroin-dependent patients in Shanghai, China. Addict. 2019;114(2):259–267. doi:10.1111/add.14451
29. Sun HM, Li XY, Chow EP, et al. Methadone maintenance treatment programme reduces criminal activity and improves social well-being of drug users in China: a systematic review and meta-analysis. BMJ Open. 2015;5(1):e005997. doi:10.1136/bmjopen-2014-005997
30. He Q, Wang X, Xia Y, et al. New community-based methadone maintenance treatment programs in Guangdong, China, and their impact on patient quality of life. Subst Use Misuse. 2011;46(6):749–757. doi:10.3109/10826084.2010.534124
31. Liu X, Zhong B, Zhu J. 30-day functioning and associated factors of heroin addicts receiving methadone maintenance treatment. Chin J Drug Depend. 2014;23(1):43–50.
32. Xu YM, Zhong BL, Zhu JH, Liu TB. Quality of life and its associated factors of heroin dependent patients receiving methadone-maintainance treatment. Chin J Drug Depend. 2014;23(4):299–304.
33. Yang YJ, Xu YM, Chen WC, Zhu JH, Lu J, Zhong BL. Loneliness and its impact on quality of life in Chinese heroindependent patients receiving methadone maintenance treatment. Oncotarget. 2017;8(45):79803–79808.
34. Zhong B, Xiang Y, Cao X, Li Y, Zhu J, Chiu HF. Prevalence of antisocial personality disorder among Chinese individuals receiving treatment for heroin dependence: a meta-analysis. Shanghai Arch Psychiatry. 2014;26(5):259–271.
35. Xu YM, Zhong BL, Liu TB. The prevalence of sleep problem among heroin addicts: a meta-analysis. Chin J Drug Depend. 2014;23(5):369–374.
36. Cranston CC, Davis JL, Rhudy JL, Favorite TK. Replication and expansion of “Best practice guide for the treatment of nightmare disorder in adults”. J Clin Sleep Med. 2011;7(5):
37. Hansen K, Hofling V, Kroner-Borowik T, Stangier U, Steil R. Efficacy of psychological interventions aiming to reduce chronic nightmares: a meta-analysis. Clin Psychol Rev. 2013;33(1):146–155. doi:10.1016/j.cpr.2012.10.012
38. Davoli M, Perucci CA. Appropriateness of methadone maintenance treatment for opiate addiction: treatment goals and effectiveness. Soz Praventivmed. 2003;48 Suppl 1:
39. Zhong BL, Xu YM, Xie WX, Lu J. Cigarette smoking is significantly linked to sexual dissatisfaction in chinese heroin-dependent patients receiving methadone maintenance treatment. Front Psychiatry. 2019. doi:10.3389/fpsyt.2019.00306.
40. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
41. World-Health-Organization. WHO report on the global tobacco epidemic, 2009: implementing smoke-free environments. Geneva: World Health Organization Press; 2010.
42. Zhong BL, Xu YM, Xie WX, Lu J, Yu WB, Yan J. Alcohol drinking in Chinese methadone-maintained clients: a self-medication for depression and anxiety? J Addict Med. 2019. doi:10.1097/ADM.0000000000000500
43. Thompson DF, Pierce DR. Drug-induced nightmares. Ann Pharmacother. 1999;33(1):93–98. doi:10.1345/aph.18150
44. Callen ED, Kessler TL, Brooks KG, Davis TW. Management of nightmare disorder in adults. US Pharm. 2018;43(11):21–25.
45. Wang X, Jiang C, Ma H. Handbook of Mental Health Rating Scales. Beijing: Chinese Mental Health Journal Press; 1999.
46. Zhong BL, Liu TB, Chan SS, et al. Common mental health problems in rural-to-urban migrant workers in Shenzhen, China: prevalence and risk factors. Epidemiol Psychiatr Sci. 2018;27(3):256–265. doi:10.1017/S2045796016001141
47. Chiu HF, Xiang YT, Dai J, et al. The prevalence of sleep problems and their socio-demographic and clinical correlates in young Chinese rural residents. Psychiatry Res. 2012;200(2–3):789–794. doi:10.1016/j.psychres.2012.03.050
48. Sjostrom N, Waern M, Hetta J. Nightmares and sleep disturbances in relation to suicidality in suicide attempters. Sleep. 2007;30(1):91–95. doi:10.1093/sleep/30.1.91
49. Tanskanen A, Tuomilehto J, Viinamaki H, Vartiainen E, Lehtonen J, Puska P. Nightmares as predictors of suicide. Sleep. 2001;24(7):844–847.
50. Sheehan DV, Mancini M, Wang J, et al. Assessment of functional outcomes by Sheehan Disability Scale in patients with major depressive disorder treated with duloxetine versus selective serotonin reuptake inhibitors. Hum Psychopharmacol. 2016;31(1):53–63. doi:10.1002/hup.2500
51. Zhu JH, Zhong BL. Reliability and validity of Sheehan Disability Scale for outpatients receiving methadone maintenance treatment. Chin J Drug Depend. 2010;19(4):281–283.
52. Schredl M, Reinhard I. Gender differences in nightmare frequency: a meta-analysis. Sleep Med Rev. 2011;15(2):115–121. doi:10.1016/j.smrv.2010.06.002
53. Himelhoch S, Weber E, Medoff D, et al. Posttraumatic stress disorder and one-year outcome in methadone maintenance treatment. Am J Addict. 2012;21(6):524–530. doi:10.1111/j.1521-0391.2012.00271.x
54. Schredl M. Explaining the gender difference in nightmare frequency. Am J Psychol. 2014;127(2):205–213. doi:10.5406/amerjpsyc.127.2.0205
55. Zhong BL, Chen SL, Tu X, Loneliness CY. Cognitive function in older adults: findings from the Chinese longitudinal healthy longevity survey. J Gerontol B Psychol Sci Soc Sci. 2017;72(1):120–128. doi:10.1093/geronb/gbw037
56. Luerding R, Gebel S, Gebel EM, Schwab-Malek S, Weissert R. Influence of formal education on cognitive reserve in patients with multiple sclerosis. Front Neurol. 2016;7:46.
57. Mitrovic SM, Dickov A, Vuckovic N, Mitrovic D, Budisa D. The effect of heroin on verbal memory. Psychiatr Danub. 2011;23(1):53–59.
58. Gupta MA, Pur DR. Prolongation of REM sleep latency in nightmare disorder may indicate subtle REM sleep fragmentation and decreased REM sleep propensity. J Clin Sleep Med. 2018;14(8):1441. doi:10.5664/jcsm.7300
59. Marquis LP, Paquette T, Blanchette-Carriere C, Dumel G, Nielsen T. REM sleep thetachanges in frequent nightmare recallers. Sleep. 2017;40:9. doi:10.1093/sleep/zsx110
60. Dimsdale JE, Norman D, DeJardin D, Wallace MS. The effect of opioids on sleep architecture. J Clin Sleep Med. 2007;3(1):33–36.
61. Gossop M, Griffiths P, Powis B, Strang J. Severity of dependence and route of administration of heroin, cocaine and amphetamines. Br J Addict. 1992;87(11):1527–1536. doi:10.1111/j.1360-0443.1992.tb02660.x
62. Atesci FC, Cetin BC, Oguzhanoglu NK, Karadag F, Turgut H. Psychiatric disorders and functioning in hepatitis B virus carriers. Psychosomatics. 2005;46(2):142–147. doi:10.1176/appi.psy.46.2.142
63. Sessle BJ, Soja PJ, Choinière M. Sleep and Pain. Seattle: IASP Press; 2007.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.