Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
Frequency of anemia in chronic psychiatry patients
Authors Korkmaz S, Yıldız S, Korucu T, Gundogan B, Sunbul ZE, Korkmaz H ![]() , Atmaca M
, Atmaca M
Received 1 July 2015
Accepted for publication 9 September 2015
Published 22 October 2015 Volume 2015:11 Pages 2737—2741
DOI https://doi.org/10.2147/NDT.S91581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Sevda Korkmaz,1 Sevler Yildiz,1 Tuba Korucu,1 Burcu Gundogan,1 Zehra Emine Sunbul,1 Hasan Korkmaz,2 Murad Atmaca1
1Department of Psychiatry, 2Department of Cardiology, Faculty of Medicine, Firat University, Elazig, Turkey
Purpose: Anemia could cause psychiatric symptoms such as cognitive function disorders and depression or could deteriorate an existing psychiatric condition when it is untreated. The objective of this study is to scrutinize the frequency of anemia in chronic psychiatric patients and the clinical and sociodemographic factors that could affect this frequency.
Methods: All inpatients in our clinic who satisfied the study criteria and received treatment between April 2014 and April 2015 were included in this cross-sectional study. Sociodemographic data for 378 patients included in the study and hemoglobin (Hb) and hematocrit values observed during their admission to the hospital were recorded in the forms. Male patients with an Hb level of <13 g/dL and nonpregnant female patients with an Hb level of <12 g/dL were considered as anemic.
Findings: Axis 1 diagnoses demonstrated that 172 patients had depressive disorder, 51 patients had bipolar disorder, 54 patients had psychotic disorder, 33 patients had conversion disorder, 19 patients had obsessive-compulsive disorder, 25 patients had generalized anxiety disorder, and 24 patients had other psychiatric conditions. It was also determined that 25.4% of the patients suffered from anemia. Thirty-five percent of females and 10% of males were considered as anemic. The frequency of anemia was the highest among psychotic disorder patients (35%), followed by generalized anxiety disorder patients (32%), and obsessive-compulsive disorder patients (26%). Anemia was diagnosed in 22% of depressive disorder patients, 25% of bipolar disorder patients, and 24% of conversion disorder patients.
Results: The prevalence of anemia among chronic psychiatry patients is more frequent than the general population. Thus, the study concluded that it would be beneficial to consider the physical symptoms and to conduct the required examinations to determine anemia among this patient group.
Keywords: anemia, hemoglobin, physical disease
Introduction
Anemia is a significant public health issue that affects a great number of people in developed and developing countries. Anemia is defined as the fall of hemoglobin (Hb) concentration in blood below the normal level, which is determined by age and sex.1 World Health Organization determined that when the Hb value is <13 g/dL in an adult male and <12 g/dL in a nonpregnant female, the individual is considered as anemic.2 Several factors, such as insufficient erythrocyte production in bone marrow, nutrition disorders, blood loss, and decrease in iron absorption, could cause anemia. However, age, sex, race, socioeconomic status, the altitude of the habitat, posture, and changes in plasma volume could result in specific changes in hematocrit values.3 Anemia, when untreated, could cause physical symptoms, such as exhaustion, fatigue, and palpitation, and psychiatric symptoms, such as cognitive function disorders and depression. Anemia also could accompany several psychiatric diseases. This coexistence could cause certain complications or an increase in the severity of the preexisting condition in the patients. The relationship between anemia and psychiatric diseases is known for a long period of time.4–8 However, there are only a limited number of studies investigating Hb values, an indicator of anemia, among chronic psychiatric patients.9 Also, none of these studies scrutinized the relationship between anemia and psychiatric diagnosis and clinical and sociodemographic data that could affect this very relationship. Thus, this study aims to examine the frequency of anemia among chronic psychiatric patients based on their diagnoses and clinical and sociodemographic data, which could affect this frequency.
Methodology
All inpatients in our clinic who satisfied the study criteria and received treatment between April 2014 and April 2015 were included in this cross-sectional study. Upon the approval of the Firat University ethics committee, all inpatients in Firat University Psychiatry Clinic diagnosed with any psychiatric condition based on DSM 4-TR10 diagnostic criteria and over the age of 18 years provided written informed patient consent and were included in the study. Patients with a significant physical pathology or disease that could affect the distribution of existing psychological symptoms or those with a preexisting blood disease other than anemia were excluded from the study. Hb values were examined by ADVIA 2120i (Siemens Diagnostics, Tarrytown, NY, USA) equipment on the full blood samples taken from the patients in 2 mL complete blood count cartridges. Males with an Hb level of <13 g/dL and nonpregnant females with an Hb level of <12 g/dL were considered as anemic. Medical histories, general medical conditions, profiles, and family histories of the patients taken from their clinical files and sociodemographic data, such as age, sex, and educational background, were recorded in the forms designed by the author of this study. Hematological parameters such as Hb, hematocrit, erythrocytary mean, corpuscular volume, and erythrocyte range, which were indicated during admission, and biochemical parameters such as urea, keratin, free T3 hormone, free T4 hormone, and thyroid-stimulating hormone were also recorded in the forms.
Statistical method
Existing data were examined along with a literature review. SPSS for Windows 21.0 software (Chicago, IL, USA) was used for data analysis. Student’s t-test was conducted for paired comparisons, and chi-square test was used for categorical comparisons; both tests were available in the aforementioned software.
Findings
The study included all inpatients who fitted the study criteria and were treated in our clinic during the last 1-year period. Based on Axis 1 diagnosis, 172 patients were diagnosed with depressive disorder, 51 patients were diagnosed with bipolar disorder, 54 patients were diagnosed with psychotic disorder, 33 patients were diagnosed with conversion disorder, 19 patients were diagnosed with obsessive-compulsive disorder, 25 patients were diagnosed with generalized anxiety disorder, and 24 patients were diagnosed with other psychiatric conditions. One hundred and forty-nine (39.4%) patients were male, and 229 (60.6%) patients were female. Patients’ mean age was determined as 41.15±15.5 (41±16 among males and 41±14 among females; P=0.927). Sociodemographic characteristics of the study group are presented in Table 1. Anemia was indicated in 25.4% of the patients who participated in the study. Table 2 demonstrates the hematological and biochemical parameters for the study group. Anemia was identified in 35% of the psychotic disorder patients, 22% of the depressive disorder patients, and 25% of the bipolar disorder patients (Table 3). Thirty-five percent of females and 10% of males were considered as anemic. The difference of this rate between males and females was statistically significant (P<0.001). Hematological parameters based on sex are presented in Table 4. Table 5 shows the mean Hb values based on age.
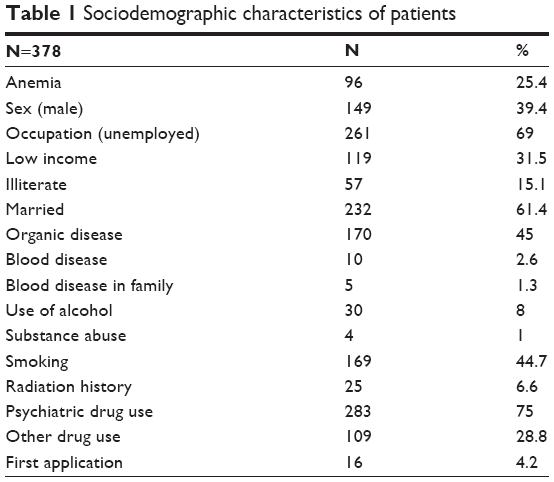 | Table 1 Sociodemographic characteristics of patients |
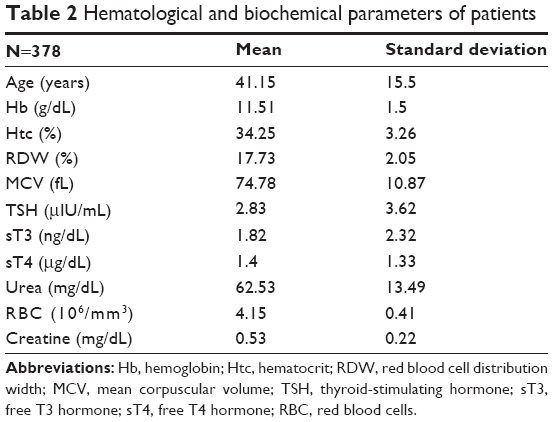 | Table 2 Hematological and biochemical parameters of patients |
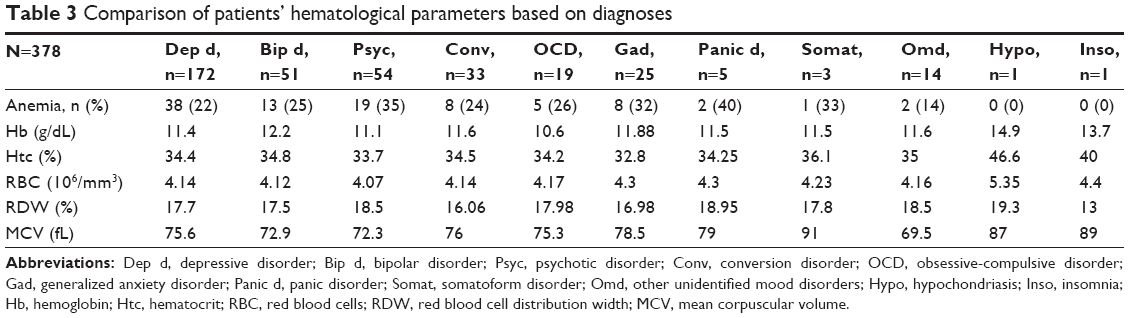 | Table 3 Comparison of patients’ hematological parameters based on diagnoses |
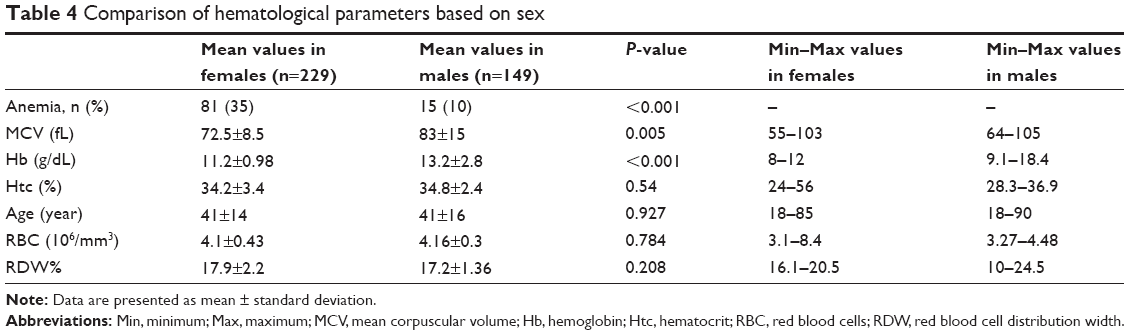 | Table 4 Comparison of hematological parameters based on sex |
 | Table 5 Hemoglobin value distribution by age group |
As a result of the analysis conducted by dividing the patients into groups of anemic patients and nonanemic patients, it was determined that 93% of the anemic patients were previously treated in an institution as inpatients. It was found that 29 individuals (32%) in the anemic group had low-income levels. Fifty-five individuals (60%) in the anemic group had an organic disease: nine of them had previous anemia history, and one of them had blood disease history in the family. Among the anemic patients, 67 (73%) patients were on psychiatric drugs during the previous month of study, while 33 (36%) patients were on nonpsychiatric drugs. Nine (10%) anemic patients reported that they were exposed to radiation during the previous month of study. Forty-eight (60%) female anemic patients stated that their menstrual cycles were regular.
Discussion
It was determined that 25.4% of the psychiatric patients also had anemia in the study. In a different study, which indicated the frequency of physical diseases among psychiatric inpatients, it was determined that 38% of the patients had at least one or more conditions on different systems. The same study indicated anemia in 12.2% of psychiatric patients.11 In another study where 6,688 inpatients in a psychiatric hospital were investigated, the same ratio was found as 6%.12 Anemia is seen predominantly in individuals with poor socioeconomic backgrounds, who have little access to the center and have difficulties in expressing physical symptoms. Thus, it is inevitable that the rate of anemia among psychiatric patients would be higher than the general population. However, the findings of this study were observed to be higher than the results of other studies in the literature. Our hospital predominantly serves a patient population that demonstrates severe symptoms, resistant to treatment, and intake of additional drugs due to other diagnoses. Among our patients, it could be possible that high frequency of drug use in high doses could have increased hematological side effects that develop due to drug use, and thus increasing the prevalence of anemia. Also intervening organic conditions could have increased the prevalence of anemia types, such as chronic disease anemia.
It is known that among women of reproductive age who experience blood loss due to menstrual bleeding, anemia is more frequent. In this study, 35% of females and 10% of males were determined as anemic. Although it varies based on the age group and domicile, anemia prevalence is generally reported as 28% among females and 10.4% among males in the literature.13 Although the mean anemia prevalence among males in the study was parallel to the findings in the literature, the anemia rates among females were higher than the rates reported in the literature.
The study findings demonstrated that anemia frequency was the highest (35%) among the psychotic disorder patients based on diagnostic groups. This ratio was 40% among panic disorder patients. However, since there were only five participating panic disorder patients in the study, that finding could be misleading. In the literature, one study reported that 4.5% of schizophrenia patients also suffered anemia, and another study reported that 2.8% of anemic patients also suffered schizophrenia.14,15 The findings of this study reflected quite higher figures when compared to the findings reported in other studies in the literature. Psychotic disorder patients face negative living conditions where they could not express themselves and could not even sustain their basic needs of nourishment and accommodation. Since there are insufficient social support systems available to help with the follow-up and treatment of psychiatric patient group and since they could not benefit from treatment services effectively, the therapies they receive are deficient and inadequate. As a result of these factors and also since health professionals tend to prioritize their mental condition and ignore their physical complaints, the physical symptoms are usually passed over, and their preexisting psychiatric disorder aggravates. In a study conducted with medical students, low serum ferritin and Hb levels were indicated among students with depression.16 There are other studies in the literature that reported a relationship between Hb levels and depressive disorder and anxiety disorder.17,18
The prevalence of anemia in the depressive disorder patient group (22%) was found to be higher than the general population in this study, parallel to the findings in the literature.13 It was determined in the study that 25% of bipolar patients suffered from anemia as well. Psychotropic drugs used for chronic psychiatric diseases cause significant hematological side effects, such as anemia, leukopenia, thrombocytopenia, and thrombocytosis. These side effects are observed more frequently in patients who use mood stabilizer drugs, such as lithium, clozapine, carbamazepine, valproic acid, and reuptake inhibitors.19 The reason for high anemia rates among bipolar patients in the study could be related to the long-term use of these mood stabilizer drugs.
In chronic psychiatric patients, the rate of existence of an accompanying physical disease in addition to the primary disorder is usually high.9 This coexistence deteriorates the quality of life of the patients, prolongs the psychiatric treatment period, and could even cause an increase in morbidity and mortality. Factors such as negligence of physical symptoms by mental health professionals, assessment of physical complaints as psychosomatic, reluctance of nonpsychiatrist physicians to provide services to psychiatric patients, lack of time and resources for checkups in mental health services, and inefficiency of patients in explaining their medical problems and difficulties related to implementing changes in lifestyle, could prevent psychiatric patients from receiving appropriate health care services.20 Treatment-related factors, drugs taken, physical conditions, negative lifestyle habits, and nutritional disorders are the reasons for anemia among chronic psychiatric patients. Detailed identification of the physical symptoms of psychiatric patients and providing health care services to them, who experience problems in expressing their complaints and are often labeled by the society, are quite important for early diagnosis and treatment.
Results
Prevalence of anemia observed among chronic psychiatric patients is higher than the mean prevalence in the general population. Thus, this study concludes that it would be beneficial for this group of patients for the health professionals to recognize the physical symptoms and provide the required examinations for anemia. Also, the findings of the study deemed especially important that the patients and caretakers should be informed about the necessity to change the negative lifestyles and malnutrition habits of the patients.
Limitations
The data were analyzed based on the information gathered from the records in the health automation system in this study. Thus, further parameters to help determine the type of anemia diagnosis were not available. Clinical psychiatric test results were also not available since face-to-face interviews with the patients were not possible.
Disclosure
The authors report no conflicts of interest in this work.
References
Johnson-Spear MA, Yip R. Hemoglobin difference between black and white women with comparable iron status: justification for race-specific anemia criteria. Am J Clin Nutr. 1994;60:117–121. | ||
World Health Organization. Tech. Rep. Ser. 1968:405, Tech Rep. 1975:580. | ||
Soysal T. Classification of anemia. In: Yazici H, Hamuryudan V, Sonsuz A. Cerrahpasa Internal medicine. Istanbul: Istanbul Medical Publishing; 2005;142–144. | ||
Allen RP, Walters AS, Montplaisir J, et al. Restless legs syndrome prevalence and impact. REST General Population Study. Arch Intern Med. 2005;165:1286–1292. | ||
Swanson JM, Kinsbourne M, Nigg J, et al. Etiological subtypes of attention deficit hyperactivity disorder: brain imaging, molecular genetics and environmental factors and the dopamine hypothesis. Neuropsychol Rev. 2007;17:39–59. | ||
Stewart R, Hirani V. Relationship between depressive symptoms, anemia, and iron status in older residents from a national survey population. Psychosom Med. 2012;74:208–213. | ||
Chen MH, Su TP, Chen YS, et al. Association between psychiatric disorders and iron deficiency anemia among children and adolescents: a nationwide population-based study. BMC Psychiatry. 2013;13:161. | ||
Becker M, Axelrod DJ, Oyesanmi O, Markov DD, Kunkel EJ. Hematologic problems in psychosomatic medicine. Psychiatr Clin North Am. 2007;30:739–759. | ||
Kisa C, Cebeci S, Uysal Z, Aydemir Ç, Göka E. Co-Occurring of physical illness in psychiatry inpatients. New Symp J. 2008;46:66–69. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000. | ||
Karlidağ Ç, Aksoy UM, Yüksel G, Alpay N, Uysal A. common medical problems in inpatient psychiatric care clinics. Klinik Psikiyatri. 2013;16:47–52. | ||
Leung MW, Xiong GL, Leamon MH, McCarron RM, Hales RE. General medical hospital admissions from a public inpatient psychiatric health facility: a review of medical complications over 30 months. Psychosomatics. 2010;51:498–502. | ||
Eraslan E, Aydoğan E, Albayrak E, Denizli N. A comparison of the prevalence of iron deficiency anemia between adult women and men and between premenopausal and postmenopausal women. Yeni Tip Dergisi. 2011;28:109–112. | ||
Carney CP, Jones L, Woolson RF. Medical comorbidity in women and men with schizophrenia a population-based controlled study. J Gen Intern Med. 2006;21:1133–1137. | ||
Schoepf D, Uppal H, Potluri R, Heun R. Physical comorbidity and its relevance on mortality in schizophrenia: a naturalistic 12-year follow-up in general hospital admissions. Eur Arch Psychiatry Clin Neurosci. 2014;264:3–28. | ||
Vahdat Shariatpanaahi M, Vahdat Shariatpanaahi Z, Moshtaaghi M, Shahbaazi SH, Abadi A. The relationship between depression and serum ferritin level. Eur J Clin Nutr. 2007;61:532–535. | ||
Lever-van Milligen BA, Vogelzangs N, Smit JH, Penninx BW. Hemoglobin levels in persons with depressive and/or anxiety disorders. J Psychosom Res. 2014;76:317–321. | ||
Onder G, Penninx BW, Cesari M, Bandinelli S, Lauretani F, Bartali B, et al. Anemia is associated with depression in older adults: results from the InCHIANTI study. J Gerontol A Biol Sci Med Sci. 2005;60: 1168–1172. | ||
Mazaira S. Haematological adverse effects caused by psychiatric drugs. Vertex. 2008;19:378–386. | ||
Muir Cochrane E. Medical co-morbidity risk factors and barriers to care for people with schizophrenia. J Psychiatr Ment Health Nurs. 2006;13:447–452. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.