Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Free Triiodothyronine Levels are Related to Executive Function and Scene Memory in Type 2 Diabetes Mellitus Patients Without Diagnosed Thyroid Diseases
Authors Zhang H ![]() , Yang S, Zhu W, Niu T, Wang Z, An K, Xie Z, Wang P, Huang X, Wang C, Shangguan H, Yuan Y, Wang S
, Yang S, Zhu W, Niu T, Wang Z, An K, Xie Z, Wang P, Huang X, Wang C, Shangguan H, Yuan Y, Wang S
Received 24 December 2021
Accepted for publication 15 March 2022
Published 5 April 2022 Volume 2022:15 Pages 1041—1050
DOI https://doi.org/10.2147/DMSO.S355656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Haoqiang Zhang,1– 3,* Shufang Yang,2,4,* Wenwen Zhu,1,2 Tong Niu,1,2 Zheng Wang,1,2 Ke An,1,2 Zuoling Xie,1,2 Pin Wang,2 Xi Huang,1,2 Chenchen Wang,1,2 Haiyan Shangguan,2 Yang Yuan,1 Shaohua Wang1
1Department of Endocrinology, Affiliated Zhongda Hospital of Southeast University, Nanjing, People’s Republic of China; 2School of Medicine, Southeast University, Nanjing, People’s Republic of China; 3Department of Endocrinology, The First Affiliated Hospital of University of Science and Technology of China, Hefei, People’s Republic of China; 4Department of Endocrinology, Taizhou People’s Hospital, Taizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaohua Wang; Yang Yuan, Department of Endocrinology, Affiliated Zhongda Hospital of Southeast University, No. 87 Dingjiaqiao Road, Nanjing, 210009, People’s Republic of China, Tel +86-25-83262815 ; +86-13814003661, Fax +86-25-83285132, Email [email protected]; [email protected]
Purpose: We aim to determine the role of free triiodothyronine (FT3), the main active ingredient of thyroid hormones (THs), in type 2 diabetes mellitus (T2DM) patients with mild cognitive impairment (MCI).
Patients and Methods: A total of 255 T2DM patients without diagnosed thyroid diseases were recruited and divided into MCI group and healthy cognition group. Neuropsychological functions were observed by multidimensional cognitive function scales in including MoCA, Digit Span Test (DST), Verbal Fluency Test (VFT), Clock drawing test (CDT), Trail Making Test (TMT) A and B, Instantaneously Recalled Auditory Verbal Learning Test (AVLT-IR), Delayed Recalled Auditory Verbal Learning Test (AVLT-DR) and Logical Memory Test (LMT). Correlation and logistic regression analyses were performed to explore the association between FT3 and diabetic cognitive dysfunction.
Results: Compared with 147 normal cognition patients, 108 MCI patients exhibited lower FT3 and higher HOMA-IR. FT3 level was not only positively correlated with MoCA scores, but DST, VFT and LMT, while negatively associated with TMTB. Furthermore, there is a negative association between FT3 and HOMA-IR. Logistic regression showed that decreased FT3 is a risk factor of MCI in T2DM patients. Although FT3 is not the risk factor of MCI after homeostasis model assessment of insulin resistance (HOMA-IR) was entered as an independent variable, lower FT3 is associated with VFT and LMT adjusted by age, education, BMI, DM duration, HBP duration, smoking, HbA1c and HOMA-IR.
Conclusion: Lower FT3 levels may involve in MCI, especially for executive function and scene memory in T2DM patients without diagnosed thyroid diseases.
Keywords: free triiodothyronine, mild cognitive impairment, insulin resistance, type 2 diabetes mellitus
Introduction
Triiodothyronine (T3) regulates the beta-amyloid precursor protein (APP) gene expression in the brain, which involves in multiple epigenetic regulatory events in vivo or in vitro studies1,2 and maintains the survival of neurons.3 Additionally, beta-amyloid (Aβ) deposition4 derives from APP in the brain, especially in the hippocampus,5 result in MCI, which is an early stage of Alzheimer’s disease (AD).6
Although THs are essential for the maintenance of normal cognitive function, effects of THs’ ingredients upon cognition complex and conflict in a great many specific studies. Chaker et al indicated that abnormal thyroid function is associated with dementia. They also demonstrated that this association does not seem to be mediated through vascular events.7 Additionally, a systematic review and meta-analysis indicated that subclinical hyperthyroidism might be associated with a modestly elevated risk of dementia.8 Moreover, it is suggested that higher thyroid stimulating hormone (TSH) and lower free thyroxine (FT4) concentrations (within the euthyroid range) are associated with lower risk of multiple adverse events, including mortality in older people.9 However, more studies tend to focus on the protective effect of thyroxine on cognitive function.10–13 Indeed, the supplementation of thyroxine can improve cognitive function and mood.14 Additionally, total T3 levels are positively correlated with the Mini-Mental State Examination (MMSE) scores.15 T3 could also alleviate the impairment of cognitive function by sleep deprivation in male Wistar rats.16 Notably, FT3, the main active ingredient of THs, may be possibly associated with better cognitive function and less extrapyramidal symptoms in patients with chronic schizophrenia.17 Moreover, FT3 is associated with regional cerebral blood flow in patients with AD.18 Quinlan et al even demonstrated that low serum concentration of FT3 is associated with increased risk of AD.19
So far, there is no study focusing on the effect of lower FT3 levels (in current reference range for general individuals) on MCI in T2DM patients without diagnosed thyroid diseases. With such a large population with T2DM in China and worldwide,20,21 it is worth to explore the role of FT3 in MCI of patients with T2DM. For diabetic patients, the reference range of FT3 of healthy people may not be appropriate, especially for the perspective of cognitive function. From the perspective of cognitive dysfunction, it is necessary to examine a suitable reference range of FT3 in the diabetic population. Here, we aim to explore the relationship between lower FT3 levels within the current reference range and diabetic cognition dysfunction in this present study.
Materials and Methods
Experiment Design
This cross-section study was conducted in the Endocrinology Department, Affiliated Zhongda Hospital of Southeast University. All 255 patients were recruited and meet the standard of T2DM. In these individuals, 108 T2DM patients were diagnosed as MCI, and 147 patients with normal cognitive function.
Ethics
All participants were informed about the process of this experiment and given a hand-written signature on the informed consent before the experiment. This study was carried out according to the Declaration of Helsinki and approved by the Research Ethics Committee, Affiliated ZhongDa Hospital of Southeast University (approval no. of ethics committee: 2013ZDSYLL040.0).
Inclusion and Exclusion Criteria
In patients with T2DM duration more than 3 years were recruited in the present study. All T2DM patients satisfied the World Health Organization 1999 Criteria.22 MCI patients satisfied criteria for MCI proposed by the MCI Working Group of the European Consortium on Alzheimer’s Disease.23 The excluded subjects were as the follows and according to our previous study24 and be described as follow: (a) severe hypoglycemia, diabetic ketoacidosis, hyperosmolar nonketotic diabetic coma, inflammatory disease, acute cardiovascular or cerebrovascular accident; (b) a history of stroke, alcoholism, head injury, Parkinson’s disease, epilepsy, major depression or other physical and mental illnesses; (c) major medical illness (eg, cancer, anemia, and serious infection); (d) severe visual or hearing loss; (d) thyroid dysfunction (including the history of thyroid disease diagnosis and abnormal laboratory test results).
Clinical Data Collection
Age, gender, and education as well as the duration of diabetes mellitus (DM) and high blood pressure (HBP) were collected. Fasting blood-glucose (FBG), fasting C-peptide (FCP), glycosylated hemoglobin (HbA1c), triglyceride (TG), total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), FT3, FT4 and TSH were determined from blood samples by Laboratory Center of Zhongda Hospital. Body mass index (BMI), HOMA-IR, FT3/TSH, and FT4/TSH were calculated. Laboratory Center of Zhongda Hospital implements internal and external quality control procedures as directed by the Chinese Laboratory Quality Control. All measurements were performed according the following Manufacturer’s instructions: FCP (Roche Group, Basel, Switzerland; 0.007–13.3 nmol/L); TG (Roche Group, Basel, Switzerland; 0.1–10.0 mmol/L); TC (Roche Group, Basel, Switzerland; 0.1–20.7 mmol/L); LDL-C (Ningbo Ruiyuan Biotechnology Co., Ltd., Ningbo, China; 0.2–11.6mmol/L); HDL-C (Roche Group, Basel, Switzerland; 0.08–3.88 mmol/L); FT3 (Roche Group, Basel, Switzerland; 0.6–50 pmol/L), FT4 (Roche Group, Basel, Switzerland; 0.5–100 pmol/L) and TSH (Roche Group, Basel, Switzerland; 0.005–100 µIU/mL).
Neuropsychological Tests
MoCA scores were tested to assess the global cognitive function according to a previously reported method. One score was added if the duration of education was less than 12 years.25 The enrolled patients with T2DM were divided into two groups: MCI group (< 26) and Non-MCI group (≥ 26). CDT was to analyze for visual space function according to the protocol of a previous research.26 DST27 and VFT28 as well as TMTA and TMTB29 were performed according to previous studies. DST, VFT and TMTB were conducted to evaluate patients’ executive functions. TMTA was performed to assess information processing speed function. AVLT-IR and AVLT-DR were conducted to exam the instantaneous memory function and delayed memory function.30 LMT were used to measure the function of scene memory.31
Statistical Methods
Data analyses were conducted by SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Student’s t-test was used for normally distributed variables. The nonparametric Mann–Whitney U was carried out for asymmetrically distributed variables. The Chi-squared test was utilized to test for binary variables. Partial correlation analysis, binary logistic regression analysis and multiple linear regression analysis were performed to explore the relationships between the cognitive function and FT3. P<0.05 was defined statistical significance.
Results
Clinical Parameters and Neuropsychological Test results of MCI and Non-MCI Patients with T2DM
To investigate the potential risk factors of cognitive decline of T2DM patients, baseline data of clinical parameters and neuropsychological test results between T2DM patients with or without MCI were compared. We observed increased HOMA-IR in T2DM patients with MCI. In addition, lower FT3 and FT4 levels as well as FT3/TSH and FT3/TSH values were detected in T2DM patients with MCI than those without MCI. While elevated TSH levels were found in T2DM patients with cognitive decline, there is no significant difference. Not surprisingly, decreased MoCA, DST, VFT, CDT, AVLT-IR, AVLT-DR and LMT as well as increased TMTA and TMTB were discovered in T2DM patients with impaired cognition, compared to those in T2DM patients with normal cognition. Expect these, we also found different age, education level, DM duration, HBP duration and HbA1c between T2DM patients with or without MCI (Table 1).
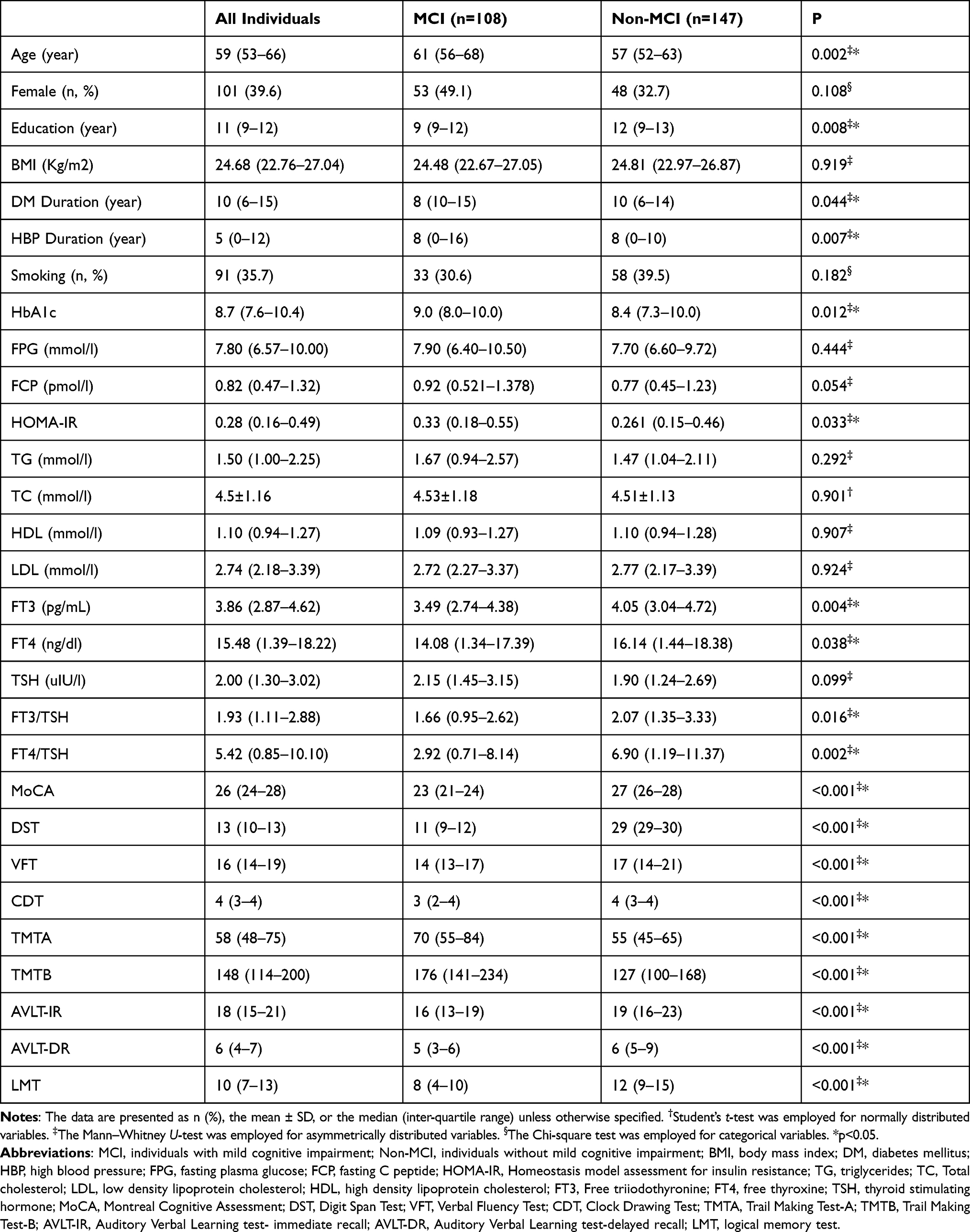 |
Table 1 Comparation of Clinical Parameters and Neuropsychological Test Results Between MCI and Non-MCI Group |
Association Between MoCA and HOMA-IR
Owning to the difference of HOMA-IR between MCI patients and Non-MCI patients, we conducted a partial correlation to explore the relationship between HOMA-IR and MoCA. Indeed, we found that HOMA-IR is negatively related to MoCA (R= −0.264; P<0.001) adjusted by age, education, BMI, DM duration, HBP duration and HbA1c (Supplementary Table 1). Additionally, binary logistic regression analysis showed that HOMA-IR is a risk factor of MCI (OR= 0.394; P= 0.038) (Table 2).
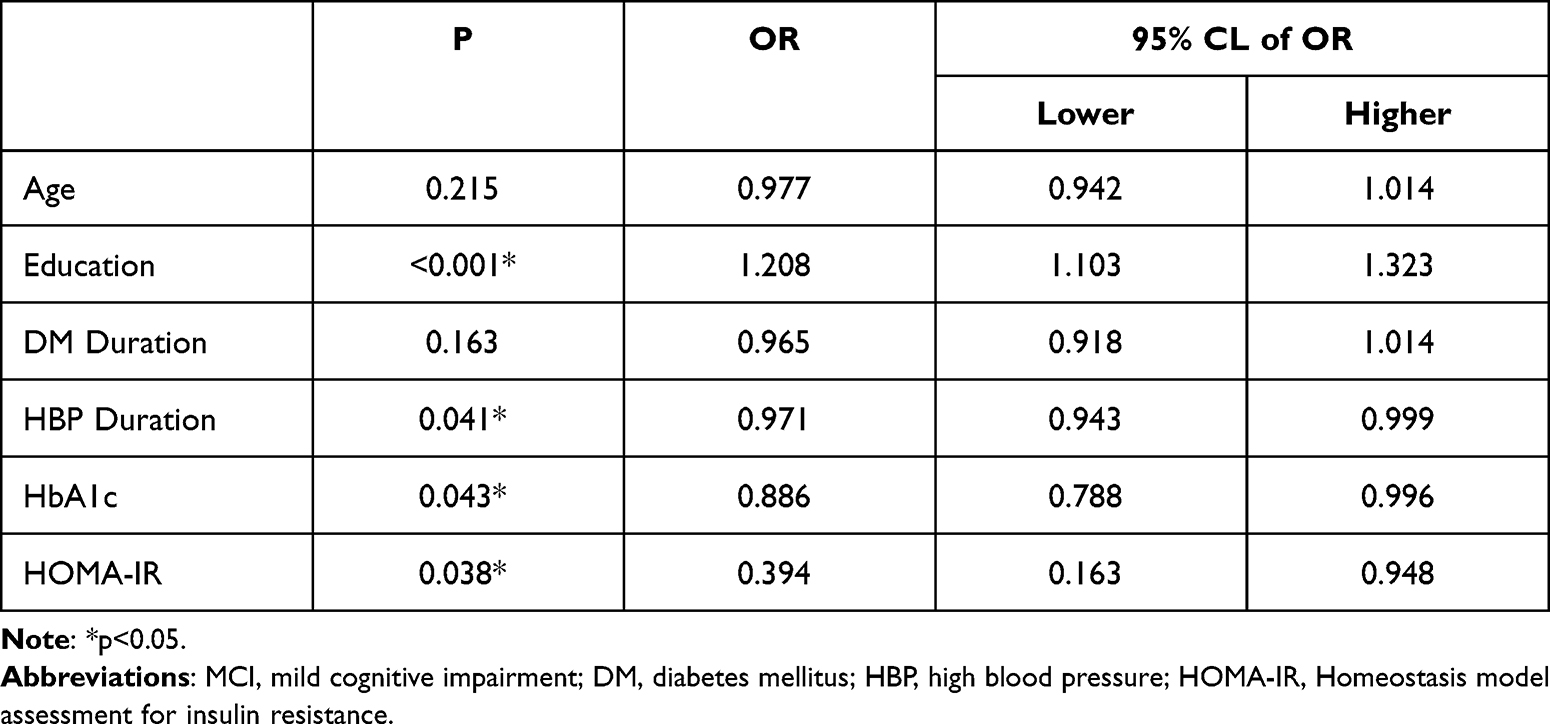 |
Table 2 Binary Logistic Regression Analysis of Independent Risk Factor for MCI Risk |
Correlation Between FT3 and HOMA-IR
After adjusted with age, education, BMI, DM duration, HBP duration and HbA1c, it is demonstrated that FT3 is negatively associated with HOMA-IR (R=−0.215; P<0.001) (Supplementary Table 2).
Correlation Between FT3 and Neuropsychological Test Scores
For the difference between FT3 levels in patients of MCI group and Non-MCI group (showed in the Table 1), the correlation between neuropsychological test scores, such as MoCA, DST, VFT, CDT, TMTA, TMTB, AVLT-IR, AVLT-DR and LMT, were analyzed by partial correlation after adjusted by age, gender, education levels, BMI, DM duration, HBP duration and HbA1c. Not surprisingly, we found a positive correlation between FT3 and MoCA in overall individuals (R= 0.145; P=0.023). In addition, we observed that DST, VFT and LMT scores are positively correlated with FT3 levels (R= 0.137, 0.244 and 0.201; P=0.031, <0.001 and <0.001, respectively), while TMTB scores were negatively associated with FT3 levels (R= - 0.134; P=0.035) (Table 3). Additionally, binary logistic regression analysis showed that lower FT3 is a risk factor of cognitive impairment of T2DM patients independent from age, education, BMI, DM duration, HBP duration smoking and HbA1c (OR = 1.352; P=0.027) (Supplementary Table 3).
 |
Table 3 Association Between FT3 and Cognitive Function |
Correlation Between FT4 (FT3/TSH or FT4/TSH) and Cognitive Function
Although FT4 level as well as FT3/TSH and FT4/TSH values are higher in T2DM patients without MCI than those with MCI, we did not find the association between FT4 (FT3/TSH or FT4/TSH) and MoCA adjusted with age, education, BMI, DM duration, HBP duration and HbA1c (R=0.098, 0.084, and 0.086; P=0.112, 0.184, and 0.117 respectively)) (Supplementary Tables 4–6). Although FT4 (FT3/TSH or FT4/TSH) is not associated with HOMA-IR (R= - 0.090, - 0.087, and - 0.087; P=0.156, 0.172, and 0.170 respectively) (Supplementary Tables 7–9), partial correlation was performed adjusted by age, education, BMI, DM duration, HBP duration, smoking, HbA1c and HOMA-IR. Indeed, there is no significant association between FT4 (FT3/TSH or FT4/TSH) and MoCA adjusted by age, education, BMI, DM duration, HBP duration, HbA1c and HOMA-IR (R=0.077, 0.061, and 0.065; P=0.223, 0.315, and 0.305 respectively) (Supplementary Tables 4–6).
FT3 is Associated with VFT and LMT
Although FT3 is not associated with MoCA in the partial correlation analysis adjusted with age, education, BMI, DM duration, HBP duration, HbA1c and HOMA-IR (R=0.092; P=0.152), FT3 is positively associated with VFT and LMT (R=0.229 and 0.166; P<0.001 and P=0.009, respectively) (Table 3). In addition, there is a significant association between FT3 and VFT (or LMT) independent from age, education, BMI, DM duration, HBP duration, HbA1c and HOMA-IR assessed by multiple linear regression (P<0.001 or P=0.009, respectively) (Table 4).
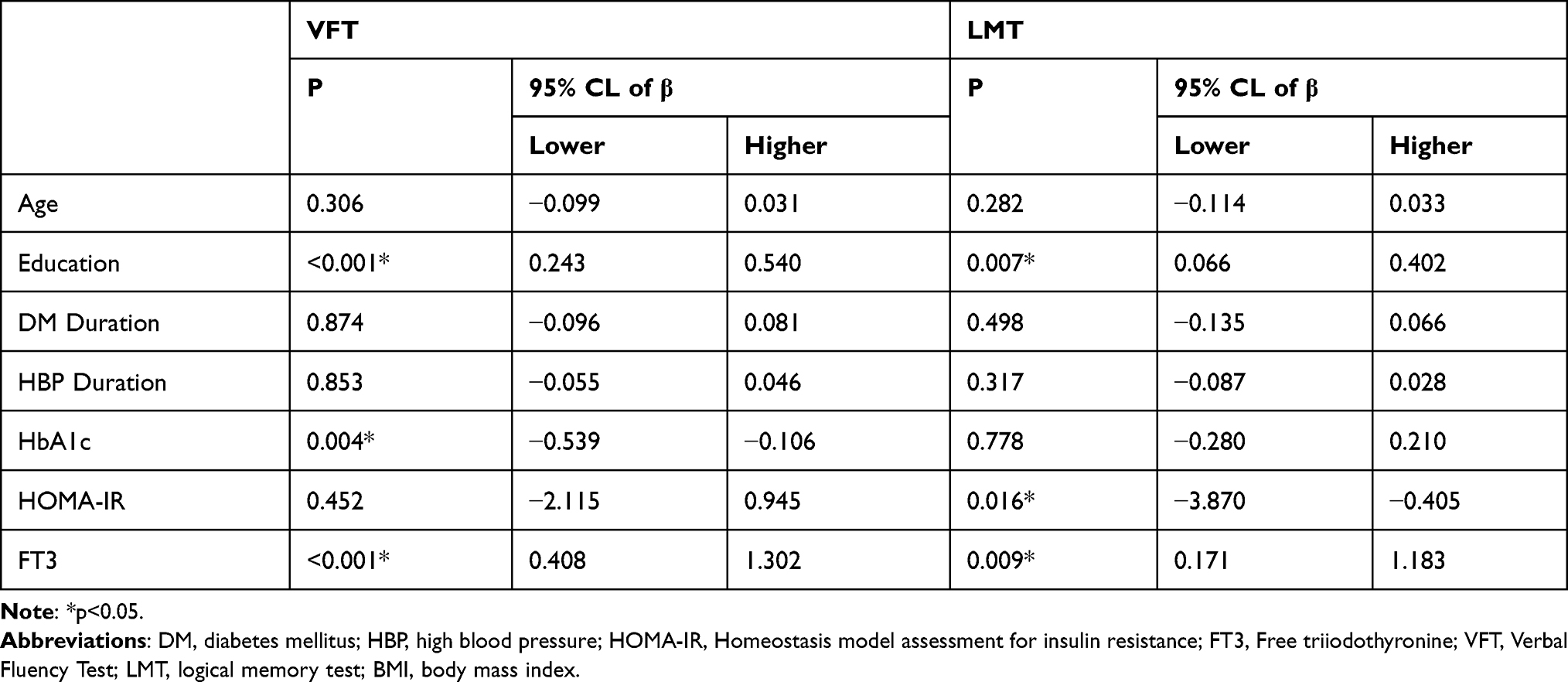 |
Table 4 Multiple Linear Regression Analysis of the Factors Influencing VFT or LMT |
Discussion
It was estimated that in 2017 there are 451 million (age 18–99 years) people with diabetes worldwide. These figures were expected to increase to 693 million by 2045.20 Among adults in China, the estimated overall prevalence of diabetes was 10.9%. With approximately 1.09 billion adults in total in mainland of China, it is projected large numbers of Chinese adults had diabetes with hyperglycemia.21 So, we mainly explored the risk factors of MCI in patients with diabetes in this present work. Additionally, THs are important for the development of the central nervous system (CNS) during perinatal growth, and also influence the CNS of adults by promoting neurogenesis, myelination and cellular repair32 for the widely expressed receptors of THs in the brain.33 Here, the associations between THs and MCI were investigated. To our best knowledge, this present study showed an association between FT3 levels and cognitive function in T2DM patients without diagnosed thyroid diseases. We demonstrated lower FT3 is an independent of MCI in T2DM patients as age, gender, education levels, BMI, DM duration, HBP duration and HbA1c were entered as independent variables. Indeed, similar study demonstrated that low serum concentration of FT3 is associated with increased risk of AD.19
Although the pathogenesis of AD or MCI as results of T2DM is not totally explored, they shared the same mechanisms, such insulin resistance (IR). Local IR in brain and global IR are common exist in T2DM patients, even in AD individuals without T2DM owning to age.34 Some literatures insisted that IR may contribute to Aβ accumulation35 and cognition decline directly for cognitive impairment were observed in genetic36 or high fat diet37,38 induced animal models with obesity and human clinical trials.34,39 In addition, associations between THs (including TSH, total T4, total T3 and FT3) and IR were found,40–42 even in the reference range of THs.43 Moreover, another study showed the regulation role of THs (including total T4, total T3 and FT3) involves in IR with an animal model.44 Some researchers even demonstrated the direct effect of T4 or T3 on IR in a classic THs receptor-α gene knockout mice study45 and mice models with T2DM,46 as well as a clinical trial by T3 withdrawal.47 Here, we confirmed the role of IR involved in diabetic cognition decline by finding the association between HOMA-IR levels and MoCA scores in this work. Moreover, elevated HOMA-IR is a risk factor of MCI in T2DM patients independent from age, gender, education levels, BMI, DM duration, HBP duration and HbA1c. This result is consistent with the previous researches insisted the association between IR and cognitive impairment by a myelin-sensitive neuroimaging technique.39 Above results combined with previous studies investigated the role of FT3 and IR involved in cognition decline, however, the role of FT3 in IR related cognition dysfunction remains need to be further explored. So, HOMA-IR was adjusted and entered as an independent variable in the partial correlation or binary logistic regression analysis respectively. Interestingly, FT3 is not an independent risk factor as HOMA-IR was entered. Although the relationships among FT3, IR and MCI are uncertain, we at least demonstrated the possibility of interactive effect FT3 and IR associated cognitive impairment in T2DM patients.
Although FT3 levels are not related to MoCA scores adjusted with age, education, BMI, DM duration, HBP duration, HbA1c and HOMA-IR, its levels are positively associated with VFT and LMT. This indicates the correlation between FT3 and cognitive function cannot be completely offset by the adjustment by IR. Additionally, VFT is associated with executive function, while LMT is related to scene memory.48 This demonstrated that FT3 is associated with executive function and scene memory, in type 2 diabetes mellitus patients without diagnosed thyroid diseases. Similarly, basic experiment showed that THs could play a neuroprotective role in CNS, especially in hippocampus or hippocampus neurons.49 Li et al clarified the smaller volume of left presubiculum associated with worse executive function and atrophy of the right CA1 related to memory in hippocampus or human with T2DM.50 Although Cappola et al suggest that slightly lower thyroid function within the euthyroid range is associated with lower risk of multiple adverse events in older people,9 this may be due to the fact that the study population is elder.
In this present work, all patients with the diagnostic criteria of T2DM and their FT3, FT4 and TSH levels are in the normal reference ranges. Even in the reference ranges, FT3 levels are associated with executive function and scene memory. In other words, lower FT3 levels may damage the cognitive function, especially for executive function and scene memory in T2DM patients without diagnosed thyroid diseases. Although, we cannot propose a more appropriate reference range due to the limited number of participants, we call for more probes to suitable reference range of THs in the perspective of diabetic cognitive dysfunction owning to the elevated prevalence of T2DM.
In the part of the results, we showed the different age and education levels in T2DM patients with MCI from those without MCI. Apart from this, we also found longer DM duration and HBP duration in those individuals with cognition declines. In our previous study, we found higher HbA1c level, in T2DM patients with MCI than these without MCI.51,52 These factors may limit the accuracy of results as confounding factors for a cross-section study. So, in the later analysis, these factors were corrected. Although FT3 is the most important active ingredient of THs, not only elevated FT3, but also FT4, FT3/TSH and FT4/TSH were observed in T2DM patients with MCI than those without MCI in this study. However, we did not find the significant association between FT4 (FT3/TSH or FT4/TSH) and MoCA in the partial correlation analysis adjusted by age, gender, education levels, DM duration, HBP duration and HbA1c (and HOMA-IR). Based on the above results, despite the essential role of FT4 and TSH may also involve in cognitive function, we focused on the role of FT3 in this present study.
Limitations
Although FT3, FT4 and TSH are very important and measured in daily clinical work, the shortage of total T3, total T4 and thyroid specific antibody data may be party limited the meaning of this study. All patients without diagnosed thyroid diseases were selected. However, these patients with sick euthyroid syndrome did not be excluded in this present work results from limited information were recorded. Additionally, as all data were collected from clinical records, IR was only assessed by HOMA-IR. Moreover, due to the limitations of cross-sectional studies, further cohort studies are needed to confirm the causal relationship between FT3 and diabetic cognition decline. The role of FT3 in MCI associated with IR remains needs to be explored by basic experiments.
Conclusion
To the best of our knowledge, this is the first study focusing on the relationship between the FT3 and MCI associated with IR in T2DM patients without diagnosed thyroid diseases. In this present work, we not only confirmed that FT3 is the risk factor of cognition dysfunction, but also demonstrated that lower FT3 levels are involved in the progress of executive function and scene memory impairment in T2DM patients without diagnosed thyroid diseases. Additionally, we highlighted the possibility of interactive effect FT3 and IR associated cognitive impairment in T2DM patients. Last but not the least, we strongly call for more probes to suitable reference ranges of THs in the perspective of diabetic cognitive dysfunction.
Acknowledgments
This work was partially supported by the National Natural Science Foundation of China (No. 81870568, SW). Haoqiang Zhang and Shufang Yang are co-first authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Contreras-Jurado C, Pascual A. Thyroid hormone regulation of APP (beta-amyloid precursor protein) gene expression in brain and brain cultured cells. Neurochem Int. 2012;60(5):484–487. doi:10.1016/j.neuint.2012.01.027
2. Belakavadi M, Dell J, Grover GJ, Fondell JD. Thyroid hormone suppression of beta-amyloid precursor protein gene expression in the brain involves multiple epigenetic regulatory events. Mol Cell Endocrinol. 2011;339(1–2):72–80. doi:10.1016/j.mce.2011.03.016
3. Oyanagi K, Negishi T, Tashiro T. Action of thyroxine on the survival and neurite maintenance of cerebellar granule neurons in culture. J Neurosci Res. 2015;93(4):592–603. doi:10.1002/jnr.23519
4. Petersen RC, Roberts RO, Knopman DS, et al. Mild cognitive impairment: ten years later. Arch Neurol. 2009;66(12):1447–1455. doi:10.1001/archneurol.2009.266
5. Luo L, Yano N, Mao Q, Jackson IM, Stopa EG. Thyrotropin releasing hormone (TRH) in the hippocampus of Alzheimer patients. J Alzheimers Dis. 2002;4(2):97–103. doi:10.3233/JAD-2002-4204
6. Mariani E, Monastero R, Mecocci P, Mecocci P. Mild cognitive impairment: a systematic review. J Alzheimers Dis. 2007;12(1):23–35. doi:10.3233/JAD-2007-12104
7. Chaker L, Wolters FJ, Bos D, et al. Thyroid function and the risk of dementia: the Rotterdam Study. Neurology. 2016;87(16):1688–1695. doi:10.1212/WNL.0000000000003227
8. Rieben C, Segna D, da Costa BR, et al. Subclinical thyroid dysfunction and the risk of cognitive decline: a meta-analysis of prospective cohort studies. J Clin Endocrinol Metab. 2016;101(12):4945–4954. doi:10.1210/jc.2016-2129
9. Cappola AR, Arnold AM, Wulczyn K, Carlson M, Robbins J, Psaty BM. Thyroid function in the euthyroid range and adverse outcomes in older adults. J Clin Endocrinol Metab. 2015;100(3):1088–1096. doi:10.1210/jc.2014-3586
10. Johansson P, Almqvist EG, Johansson JO, et al. Reduced cerebrospinal fluid level of thyroxine in patients with Alzheimer’s disease. Psychoneuroendocrinology. 2013;38(7):1058–1066. doi:10.1016/j.psyneuen.2012.10.012
11. Davis JD, Podolanczuk A, Donahue JE, et al. Thyroid hormone levels in the prefrontal cortex of post-mortem brains of Alzheimer’s disease patients. Curr Aging Sci. 2008;1(3):175–181. doi:10.2174/1874609810801030175
12. Baldini M, Colasanti A, Orsatti A, Airaghi L, Mauri MC, Cappellini MD. Neuropsychological functions and metabolic aspects in subclinical hypothyroidism: the effects of L-thyroxine. Prog Neuropsychopharmacol Biol Psychiatry. 2009;33(5):854–859. doi:10.1016/j.pnpbp.2009.04.009
13. Gussekloo J, van Exel E, de Craen AJ, Meinders AE, Frolich M, Westendorp RG. Thyroid status, disability and cognitive function, and survival in old age. JAMA. 2004;292(21):2591–2599. doi:10.1001/jama.292.21.2591
14. Reed HL, Reedy KR, Palinkas LA, et al. Impairment in cognitive and exercise performance during prolonged antarctic residence: effect of thyroxine supplementation in the polar triiodothyronine syndrome. J Clin Endocrinol Metab. 2001;86(1):110–116. doi:10.1210/jcem.86.1.7092
15. Chen Z, Liang X, Zhang C, et al. Correlation of thyroid dysfunction and cognitive impairments induced by subcortical ischemic vascular disease. Brain Behav. 2016;6(4):e00452. doi:10.1002/brb3.452
16. Zhang N, Ma Q, Chen XW, et al. [Effects of retinol acid and triiodothyronine on alleviating the impairment of cognitive function by sleep deprivation]. Zhongguo Ying Yong Sheng Li Xue Za Zhi. 2013;29(4):294–297, 300. Chinese.
17. Ichioka S, Terao T, Hoaki N, Matsushita T, Hoaki T. Triiodothyronine may be possibly associated with better cognitive function and less extrapyramidal symptoms in chronic schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(1):170–174. doi:10.1016/j.pnpbp.2012.06.008
18. Nomoto S, Kinno R, Ochiai H, et al. The relationship between thyroid function and cerebral blood flow in mild cognitive impairment and Alzheimer’s disease. PLoS One. 2019;14(4):e0214676. doi:10.1371/journal.pone.0214676
19. Quinlan P, Horvath A, Wallin A, Svensson J. Low serum concentration of free triiodothyronine (FT3) is associated with increased risk of Alzheimer’s disease. PsychoneuroEndocrinology. 2019;99:112–119. doi:10.1016/j.psyneuen.2018.09.002
20. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
21. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. doi:10.1001/jama.2017.7596
22. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(SICI)1096-9136(199807)15:7<539::AID-DIA668>3.0.CO;2-S
23. Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Arch Neurol. 1999;56(3):303–308. doi:10.1001/archneur.56.3.303
24. Tian S, Huang R, Han J, et al. Increased plasma Interleukin-1beta level is associated with memory deficits in type 2 diabetic patients with mild cognitive impairment. Psychoneuroendocrinology. 2018;96:148–154. doi:10.1016/j.psyneuen.2018.06.014
25. Nasreddine ZS, Phillips NA, Bedirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
26. Viscogliosi G, Chiriac IM, Andreozzi P, Ettorre E. Executive dysfunction assessed by Clock-Drawing Test in older non-demented subjects with metabolic syndrome is not mediated by white matter lesions. Psychiatry Clin Neurosci. 2015;69(10):620–629. doi:10.1111/pcn.12296
27. Leung JL, Lee GT, Lam YH, Chan RC, Wu JY. The use of the Digit Span Test in screening for cognitive impairment in acute medical inpatients. Int Psychogeriatr. 2011;23(10):1569–1574. doi:10.1017/S1041610211000792
28. Chen YL, Chen YH, Lieh-Mak F, Felice M. Semantic verbal fluency deficit as a familial trait marker in schizophrenia. Psychiatry Res. 2000;95(2):133–148. doi:10.1016/S0165-1781(00)00166-9
29. Crowe SF. The differential contribution of mental tracking, cognitive flexibility, visual search, and motor speed to performance on parts A and B of the Trail Making Test. J Clin Psychol. 1998;54(5):585–591. doi:10.1002/(SICI)1097-4679(199808)54:5<585::AID-JCLP4>3.0.CO;2-K
30. Vakil E, Blachstein H, Rochberg J, Vardi M. Characterization of memory impairment following closed-head injury in children using the Rey Auditory Verbal Learning Test (AVLT). Child Neuropsychol. 2004;10(2):57–66. doi:10.1080/09297040490911078
31. Won J, Callow DD, Pena GS, et al. Hippocampal functional connectivity and memory performance after exercise intervention in older adults with mild cognitive impairment. J Alzheimers Dis. 2021;82(3):1015–1031. doi:10.3233/JAD-210051
32. Stepien BK, Huttner WB. Transport, metabolism, and function of thyroid hormones in the developing mammalian brain. Front Endocrinol. 2019;10:209. doi:10.3389/fendo.2019.00209
33. Wallis K, Dudazy S, van Hogerlinden M, Nordstrom K, Mittag J, Vennstrom B. The thyroid hormone receptor alpha1 protein is expressed in embryonic postmitotic neurons and persists in most adult neurons. Mol Endocrinol. 2010;24(10):1904–1916. doi:10.1210/me.2010-0175
34. Kotkowski E, Price LR, Franklin C, et al. A neural signature of metabolic syndrome. Hum Brain Mapp. 2019;40(12):3575–3588. doi:10.1002/hbm.24617
35. Rad SK, Arya A, Karimian H, et al. Mechanism involved in insulin resistance via accumulation of beta-amyloid and neurofibrillary tangles: link between type 2 diabetes and Alzheimer’s disease. Drug Des Devel Ther. 2018;12:3999–4021. doi:10.2147/DDDT.S173970
36. Wang SH, Huang Y, Yuan Y, Xia WQ, Wang P, Huang R. LDL receptor knock-out mice show impaired spatial cognition with hippocampal vulnerability to apoptosis and deficits in synapses. Lipids Health Dis. 2014;13:175. doi:10.1186/1476-511X-13-175
37. Park HS, Park SS, Kim CJ, Shin MS, Kim TW. Exercise alleviates cognitive functions by enhancing hippocampal insulin signaling and neuroplasticity in high-fat diet-induced obesity. Nutrients. 2019;11(7):1603. doi:10.3390/nu11071603
38. Cope EC, LaMarca EA, Monari PK, et al. Microglia play an active role in obesity-associated cognitive decline. J Neurosci. 2018;38(41):8889–8904. doi:10.1523/JNEUROSCI.0789-18.2018
39. O’Grady JP, Dean DC
40. Akcan N, Bundak R. Accuracy of tri-ponderal mass index and body mass index in estimating insulin resistance, hyperlipidemia, impaired liver enzymes or thyroid hormone function and vitamin D levels in children and adolescents. J Clin Res Pediatr Endocrinol. 2019;11(4):366–373. doi:10.4274/jcrpe.galenos.2019.2018.0279
41. Ferrannini E, Iervasi G, Cobb J, Ndreu R, Nannipieri M. Insulin resistance and normal thyroid hormone levels: prospective study and metabolomic analysis. Am J Physiol Endocrinol Metab. 2017;312(5):E429–E436. doi:10.1152/ajpendo.00464.2016
42. Jayanthi R, Srinivasan AR, Hanifah M, Maran AL. Associations among insulin resistance, Triacylglycerol/High Density Lipoprotein (TAG/HDL ratio) and thyroid hormone levels-A study on Type 2 diabetes mellitus in obese and overweight subjects. Diabetes Metab Syndr. 2017;11(Suppl 1):S121–S126. doi:10.1016/j.dsx.2016.12.020
43. Kwon H, Cho JH, Lee DY, et al. Association between thyroid hormone levels, body composition and insulin resistance in euthyroid subjects with normal thyroid ultrasound: the Kangbuk Samsung Health Study. Clin Endocrinol. 2018;89(5):649–655. doi:10.1111/cen.13823
44. Martinez B, Ortiz RM. Thyroid hormone regulation and insulin resistance: insights from animals naturally adapted to fasting. Physiology. 2017;32(2):141–151. doi:10.1152/physiol.00018.2016
45. Jornayvaz FR, Lee HY, Jurczak MJ, et al. Thyroid hormone receptor-alpha gene knockout mice are protected from diet-induced hepatic insulin resistance. Endocrinology. 2012;153(2):583–591. doi:10.1210/en.2011-1793
46. Lin Y, Sun Z. Thyroid hormone potentiates insulin signaling and attenuates hyperglycemia and insulin resistance in a mouse model of type 2 diabetes. Br J Pharmacol. 2011;162(3):597–610. doi:10.1111/j.1476-5381.2010.01056.x
47. Brenta G, Celi FS, Pisarev M, Schnitman M, Sinay I, Arias P. Acute thyroid hormone withdrawal in athyreotic patients results in a state of insulin resistance. Thyroid. 2009;19(6):665–669. doi:10.1089/thy.2009.0108
48. Wang J, Yuan Y, Cai R, et al. Association between plasma levels of PAI-1, tPA/PAI-1 molar ratio, and mild cognitive impairment in Chinese patients with type 2 diabetes mellitus. J Alzheimers Dis. 2018;63(2):835–845. doi:10.3233/JAD-171038
49. Salazar P, Cisternas P, Martinez M, Inestrosa NC. Hypothyroidism and cognitive disorders during development and adulthood: implications in the central nervous system. Mol Neurobiol. 2019;56(4):2952–2963. doi:10.1007/s12035-018-1270-y
50. Li M, Huang L, Yang D, et al. Atrophy patterns of hippocampal subfields in T2DM patients with cognitive impairment. Endocrine. 2020;68(3):536–548. doi:10.1007/s12020-020-02249-w
51. Huang R, Han J, Tian S, et al. Association of plasma ghrelin levels and ghrelin rs4684677 polymorphism with mild cognitive impairment in type 2 diabetic patients. Oncotarget. 2017;8(9):15126–15135. doi:10.18632/oncotarget.14852
52. Zhang H, Huang R, Tian S, et al. The CC genotype of insulin-induced gene 2 rs7566605 is a protective factor of hypercholesteremia susceptible to mild cognitive impairment, especially to the executive function of patients with type 2 diabetes mellitus. Biomed Res Int. 2020;2020:4935831. doi:10.1155/2020/4935831
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.