Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Free and Total Thyroxine Levels are Associated with Cardiovascular-Kidney-Metabolic Syndrome Stages in Elderly Cohorts from China and the United States: A Cross-Sectional Study
Authors Wang K, Ke W, Sheng L, Wang K, Wu B, He L, Peng S, Lin Y, Zha B
Received 29 January 2026
Accepted for publication 4 June 2026
Published 16 July 2026 Volume 2026:19 596317
DOI https://doi.org/10.2147/DMSO.S596317
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Kangan Wang,1,2,* Wencai Ke,2,3,* Li Sheng,1,2,* Kai Wang,1,2 Biying Wu,2,3 Leqi He,2,3 Shu Peng,1,2 Yong Lin,4 Bingbing Zha1,2
1Department of Endocrinology, Fifth People’s Hospital of Shanghai Fudan University, Shanghai, People’s Republic of China; 2Department of Community-Based Health Research, Fudan University, Shanghai, People’s Republic of China; 3Department of Clinical Laboratory,Fifth People’s Hospital of Shanghai Fudan University, Shanghai, People’s Republic of China; 4Department of Laboratory Medicine, Huashan Hospital of Fudan University, Shanghai Medical School, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bingbing Zha, Department of Endocrinology, Fifth People’s Hospital of Shanghai Fudan University, 801 Heqing Road, Shanghai, 200240, People’s Republic of China, Tel +8613764181848, Fax +8621-64300477, Email [email protected] Yong Lin, Department of Laboratory Medicine, Huashan Hospital of Fudan University, Shanghai Medical School, Fudan University, Shanghai, 200030, People’s Republic of China, Email [email protected]
Background: Cardiovascular-kidney-metabolic (CKM) syndrome is an emerging multisystem disorder that predominantly affects older adults. The role of thyroid hormones in its pathogenesis remains underexplored. This study aimed to investigate the associations between thyroid hormone levels and CKM stages in elderly populations.
Methods: A total of 3300 participants from the Shanghai Friendship Community Elderly Cohort (SFCEC, enrolled in 2020) and 1153 participants from the US National Health and Nutrition Examination Survey (NHANES 2007– 2012) were included. All participants were elderly, defined as aged 60 to 80 years. Thyroid function markers (TSH, FT4, TT4, FT3, TT3) were measured using standardized assays. CKM syndrome was classified into five stages (0– 4) according to American Heart Association (AHA) criteria. Multivariable ordinal logistic regression and restricted cubic splines (RCS) were employed to evaluate the associations.
Results: The prevalence of CKM (stages 1– 4) was strikingly high in both elderly cohorts (98.33% in SFCEC and 98.76% in NHANES). After full adjustment, consistent associations were observed across both cohorts: each 1 ug/dL increase in TT4 was associated with elevated CKM risk (SFCEC: OR=1.064, 95% CI: 1.030– 1.100; NHANES: OR=1.145, 95% CI:1.070– 1.225). Similarly, each 1 ng/dL increment in FT4 was associated with increased risk (OR=1.538, 95% CI:1.097– 2.157 and OR=3.500, 95% CI:1.745– 7.020, respectively). Participants in the highest tertile of TT4 exhibited significantly elevated CKM risk compared to the lowest tertile group (SFCEC: OR = 1.304, 95% CI: 1.114– 1.528; NHANES: OR = 1.667, 95% CI: 1.219– 2.277). A consistent pattern was observed for FT4, with the highest tertile showing increased odds of CKM compared to the lowest (SFCEC: OR = 1.250, 95% CI: 1.066– 1.466; NHANES: OR = 1.534, 95% CI: 1.046– 2.248). Notably,RCS analyses indicated that both TT4 and FT4 hormone levels were linearly associated with CKM Syndrome. (p- overall < 0.05 and p-nonlinear > 0.05). However, no significant associations were observed for TSH, FT3, or TT3 in the adjusted models.
Conclusion: Elevated levels of TT4 and FT4 are associated with higher CKM stages in elderly populations. These findings suggest that T4 levels may serve as biomarkers for CKM risk stratification. Longitudinal studies are warranted to confirm these associations and to establish causality.
Keywords: cardiovascular-kidney-metabolic syndrome, CKM, thyroid hormone, elderly population
Introduction
Cardiovascular-kidney-metabolic (CKM) syndrome represents an emerging clinical entity recently characterized by the American Heart Association (AHA) as a complex, multisystem disorder. This condition manifests through dynamic interrelationships between obesity, diabetes mellitus(DM), chronic kidney disease (CKD), and cardiovascular disease (CVD), with a five-stage classification system (Stage 0: absence of risk factors; Stage 1: excess or dysfunctional adipose tissue; Stage 2: metabolic risk factors or moderate-to-high risk CKD; Stage 3: subclinical CVD; Stage 4: established CVD) that emphasizes the clinical value of integrated comorbidity management.1 Epidemiological investigations have revealed substantial disease burdens, particularly in aging populations,with CKM-related health impairments showing consistently high prevalence rates in the US adult population,2,3 while demonstrating comparable significance in China.4 Mechanistic studies indicate that persistent metabolic dysregulation initiates a cascade of pathological events including sympathetic overactivation, chronic inflammatory responses, and progressive tissue fibrosis, ultimately leading to multiorgan dysfunction.5 Nevertheless, the complete spectrum of contributing factors and underlying molecular pathways was not fully understood.
Thyroid hormones are present in numerous tissues and play a critical role in controlling energy metabolism and physiologic function of nervous, and cardiovascular systems.6,7 Substantial evidence confirms that thyroid dysfunction significantly disrupts lipid and glucose metabolism while contributing to cardiovascular pathogenesis.8 Notably, even euthyroid obese individuals frequently exhibit activated hypothalamic-pituitary-thyroid axis activity accompanied by elevated circulating thyroid hormone concentrations.9 This observation justifies examining thyroid hormone levels across the full clinical spectrum, rather than focusing solely on overt dysfunction. Furthermore, thyroid dysfunction may impair renal function and alter kidney structure, potentially leading to CKD.10 Notably, patients with CKD commonly exhibit reduced circulating thyroid hormone levels.10 Although extensive research has established connections between thyroid hormone and individual metabolic disorders including metabolic syndrome, obesity, CVD, and CKD,6–10 its association with the integrative concept of CKM syndrome remains unexplored.
Thyroxine (T4) is the primary secretory product of the thyroid gland and can act on peripheral tissues, produced in far greater quantities than triiodothyronine (T3).6,7 In contrast, TSH is a central regulator without direct peripheral action, and T3 depends on peripheral deiodinase conversion, making it less stable as a circulating marker. T4 binds to membrane integrin αvβ3 and triggers signaling cascades that lead to oxidative stress and inflammation11—processes central to CKM pathogenesis.5 Therefore, we hypothesized that FT4 and TT4 levels would be associated with CKM stages.
To address the knowledge gap regarding thyroid hormones and the integrated concept of CKM syndrome, we designed a comprehensive investigation utilizing data from both the Shanghai Friendship Community Elderly Cohort (SFCEC 2020) and the National Health and Nutrition Examination Survey (NHANES 2007–2012). Comparing a community-based Chinese cohort with a nationally representative US cohort allows us to test the generalizability of findings across distinct genetic backgrounds, dietary patterns, lifestyle factors, and healthcare systems. Replication of results in two geographically and ethnically diverse populations provides stronger evidence than a single-country study. We examined potential associations between thyroid hormone levels and CKM staging, while establishing detailed dose-response relationships. All participants were elderly, defined as aged 60 to 80 years.
Methods
Study Population
The Shanghai Friendship Community Elderly Cohort (SFCEC) constitutes a population-based cross-sectional study conducted in Baoshan District, Shanghai between April and September 2020. Eligibility criteria included: (1) 60≤age≤80 years, consistent with the NHANES study population which exclusively comprises individuals under the age of 80; (2) residence in Eastern China; (3) capacity for independent questionnaire completion; and (4) willingness to participate in comprehensive health assessments including questionnaires, physical examinations, and laboratory tests. From the initial pool, we excluded individuals with incomplete thyroid function data (n=21), missing BMI or waist circumference measurements (n=171), missing HbA1c values (n=2), missing eGFR data (n=1), missing disease history records (n=65), missing education status information (n=70), missing marital status (n=7), missing household income data (n=42), and missing systolic blood pressure measurements (n=32), resulting in a final analytical sample of 3,300 participants. The study protocol received approval from the Ethics Review Committee of Huashan Hospital, Fudan University (Approval No. 2020–004), with written informed consent obtained from all participants.
For comparative analysis, we utilized data from the 2007–2012 National Health and Nutrition Examination Survey (NHANES), a nationally representative, stratified multistage probability survey in the United States that collects extensive demographic, clinical, and laboratory data. Applying identical exclusion criteria (age <60 years, missing thyroid function data, or incomplete demographics), we included 1,153 NHANES participants for final analysis. All NHANES participants provided written informed consent. Detailed selection procedures are illustrated in eFigure 1. Additionally, we performed sensitivity analyses restricted to euthyroid participants, defined as those with TSH levels within the normal reference range (0.3–3.6 mIU/L in SFCEC and 0.45–4.5 mIU/L in NHANES).
Thyroid Function Measurement
In both cohorts, thyroid function profiles were assessed, including thyroid-stimulating hormone (TSH), free triiodothyronine (FT3), free thyroxine (FT4), total triiodothyronine (TT3), and total thyroxine (TT4). The units were standardized as follows: TT3 and FT4 in ng/dL, FT3 in pg/mL,TT4 in ug/dL, and TSH in mIU/L. In SFCEC, measurements were performed using chemiluminescence assays (Thorin reagents), while NHANES employed serum-based immuno-enzymatic methods as detailed in the NHANES laboratory protocol (http://wwwn.cdc.gov/nchs/nhanes/2007-2008/THYROD_E.htm).
CKM Syndrome Ascertainment
CKM syndrome was classified into five progressive stages (0–4) following established criteria from the American Heart Association (AHA) and Aggarwal et al1,2 Detailed CKM stage definitions, adapted to data available in NHANES, have been previous described (see eTable 1). Briefly, the staging system was operationalized as follows: Stage 0 comprised individuals with normal body mass index(BMI) and waist circumference without additional metabolic abnormalities; Stage 1 included those meeting criteria for adiposity (elevated BMI or waist circumference) or prediabetes; Stage 2 encompassed participants with multiple metabolic risk factors or moderate-to-high risk chronic kidney disease (CKD) as defined by Kidney Disease Improving Global Outcomes (KDIGO) guidelines;12 Stage 3 identified participants with very-high-risk KDIGO CKD or a high predicted 10-year CVD risk estimated using the PREVENT equations (see eTable 2); Stage 4 represented patients with clinically confirmed CVD.
Covariates
This study adjusted for comprehensive covariates encompassing demographic characteristics (age, sex [male/female], marital status [married/cohabitating, divorced/separated, never married, widowed]), socioeconomic status (educational attainment [<high school, high school, >high school]13 and annual household income [≤14,000, 14,000–28,000, or ≥28,000 USD] converted from RMB at 7:1 exchange rate), and lifestyle factors (current smoking status and alcohol consumption, both dichotomized as yes/no).
Statistical Analysis
We performed analyses in sequential phases: First, continuous variables were summarized as mean ± standard deviation (SD), while categorical variables were expressed as frequencies (percentages). Second, multivariable ordinal logistic regression models were employed to examine associations between thyroid hormone parameters (analyzed as both continuous variables and tertiles [T1–T3]) and CKM syndrome. Two modeling approaches were implemented: Model 1 (unadjusted) and Model 2 (adjusted for age [continuous], sex, educational attainment, smoking status, alcohol consumption, marital status, and household income). For NHANES analyses, we incorporated sampling weights, stratification variables, and primary sampling units to maintain national representativeness. To explore potential effect modification by thyroid axis status, we repeated all multivariable logistic regression analyses within the euthyroid subgroup. Third, we conducted stratified analyses by prespecified subgroups including age (≤70,>70 years), sex, education level, smoking status, alcohol use, marital status, and income levels. Fourth, baseline characteristics were presented as mean ± standard error (SE) for continuous variables and percentages for categorical variables, with participants categorized into tertiles based on TT4 or FT4 levels. Finally, restricted cubic spline (RCS) regression with three knots was performed to assess potential nonlinear relationships between thyroid hormone levels and CKM syndrome, adjusting for Model 2 covariates. Model fit was evaluated using the Akaike Information Criterion (AIC), where lower values indicate superior model performance. All statistical computations were executed using R software (version 4.4.2; R Foundation for Statistical Computing).
Results
Characteristics of the Study Population
Table 1 presents the detailed baseline characteristics of 3,300 SFCEC participants (60.8% female, mean age 74.47±3.35 years) and 1,153 NHANES participants (56.0% female, mean age 69.91±0.28 years). Thyroid function profiles showed cohort-specific patterns: SFCEC participants exhibited mean levels of TSH (2.50±1.97 mIU/L), FT4 (1.13±0.19 ng/dL), TT4 (8.98±1.95 ug/dL), FT3 (2.62±0.41 pg/mL), and TT3 (90.70±15.60 ng/dL), while NHANES participants demonstrated TSH (2.40±0.09 mIU/L), FT4 (0.85±0.01 ng/dL), TT4 (8.18±0.08 ug/dL), FT3 (3.01±0.01 pg/mL), and TT3 (105.45±0.81 ng/dL). Both cohorts revealed remarkably high CKM prevalence, with 98.33% of SFCEC and 98.76% of NHANES participants classified as stages 1–4. Notably, the two databases showed discrepancies in education level, marital status, household income, and alcohol consumption. The proportion of each major CKM-related disease is shown in the eTable 3.
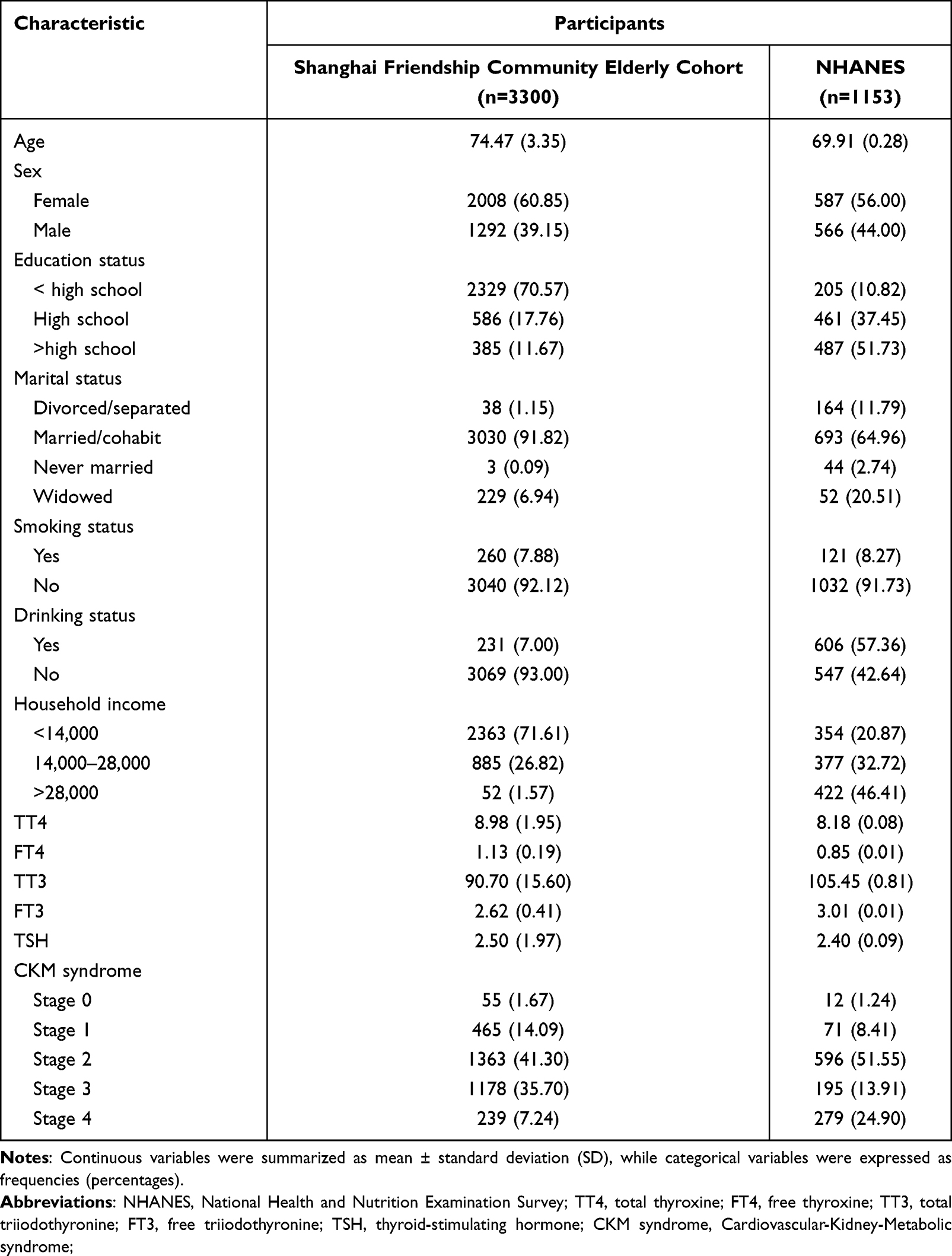 |
Table 1 Baseline Characteristics of the Study Population |
Association Between Thyroid Hormone Levels and CKM Syndrome
Multivariable logistic regression analyses revealed significant associations between thyroid hormone levels and CKM syndrome stages in both cohorts (Table 2). In the SFCEC cohort, after full adjustment for covariates, each unit increase in TT4 (OR=1.064, 95% CI: 1.030–1.100) and FT4 (OR=1.538,95% CI:1.097–2.157) was associated with elevated CKM risk. Participants in the highest tertile of TT4 (OR = 1.304, 95% CI: 1.114–1.528) and FT4 (OR = 1.250, 95% CI: 1.066–1.466) showed significantly increased risk compared to the lowest tertile. Comparable patterns were observed in the NHANES cohort, where each unit increase in TT4 (OR = 1.145, 95% CI: 1.070–1.225) and FT4 (OR = 3.500, 95% CI: 1.745–7.020) was significantly associated with higher CKM stages. Likewise, participants in the highest tertile of TT4 (OR = 1.667, 95% CI: 1.219–2.277) and FT4 (OR = 1.534, 95% CI: 1.046–2.248) demonstrated increased risk relative to the lowest tertile. However, no significant associations were observed between TT3, FT3 or TSH levels and CKM. Given the potential confounding by overt thyroid dysfunction, sensitivity analyses were performed in euthyroid participants. While the positive association of TT4 with advanced CKM stages persisted in this subgroup (SFCEC: OR=1.063, 95% CI: 1.026–1.102; NHANES:OR=1.160, 95% CI: 1.085–1.241), a divergent and protective association emerged for TT3, which was associated with lower odds of CKM (T3 vs. T1 in SFCEC: OR=0.817, 95% CI: 0.685–0.973; T2 vs. T1 in NHANES: OR=0.617, 95% CI: 0.413–0.923). The association for FT4 remained positive in continuous models (SFCEC:OR=1.482, 95% CI: 1.011–2.172; NHANES:OR=3.245, 95% CI: 1.413–7.455) but was attenuated when analyzed categorically. Detailed results are provided in eTable 4.
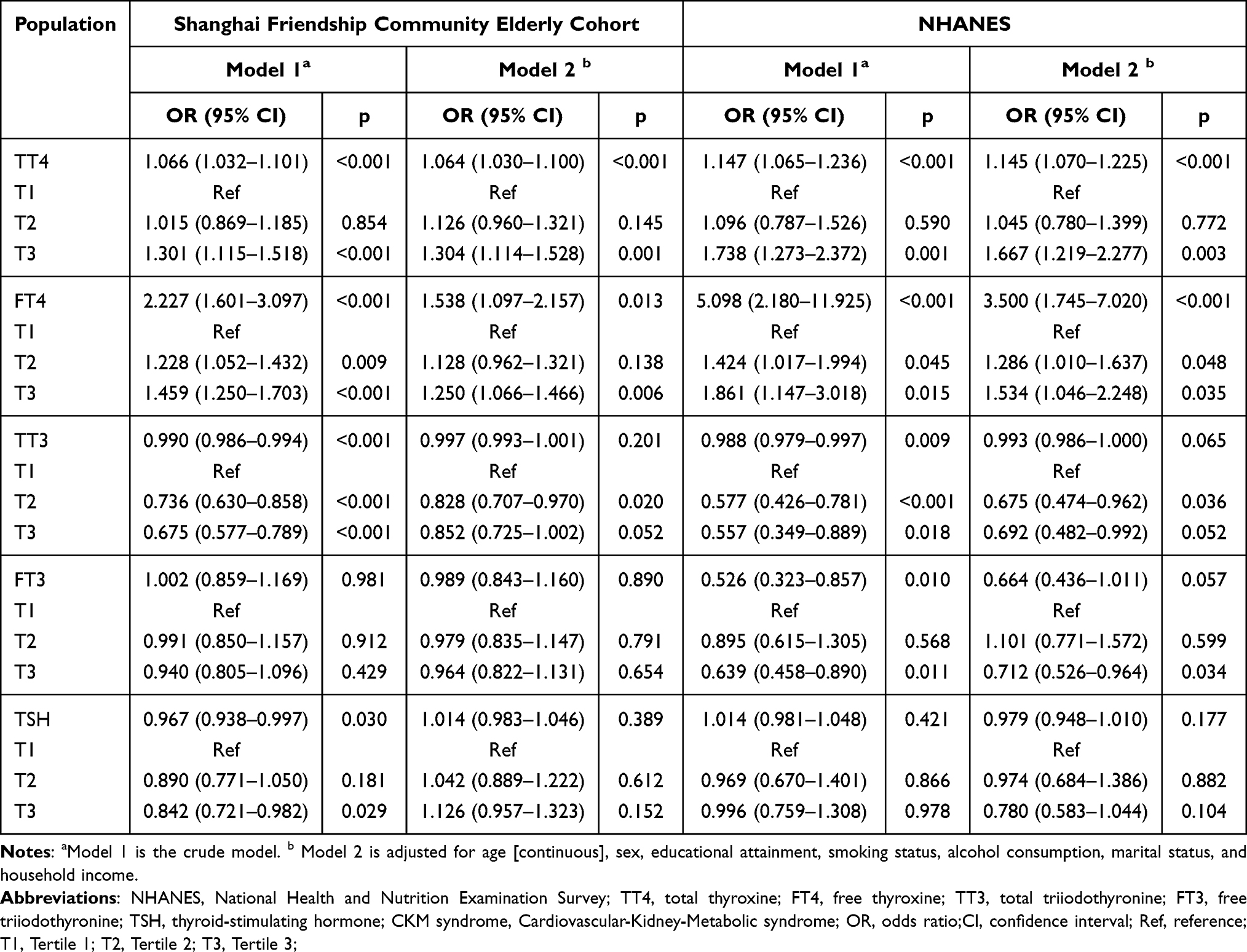 |
Table 2 Association Between Thyroid Hormone Levels and CKM Syndrome |
Subgroup Analyses
Stratified analyses were performed across both cohorts by age group, sex, education level, household income, smoking status, alcohol consumption, and marital status (Table 3). Elevated TT4 and FT4 levels remained significantly associated with increased CKM risk in most subgroups in both cohorts. Furthermore, subgroup analyses based on TT4 levels indicated a more pronounced association between TT4 and CKM among female participants in the NHANES cohort. Similarly, analyses based on FT4 levels showed a stronger association between FT4 and CKM among participants with middle household income (all P < 0.05; P for interaction < 0.05).
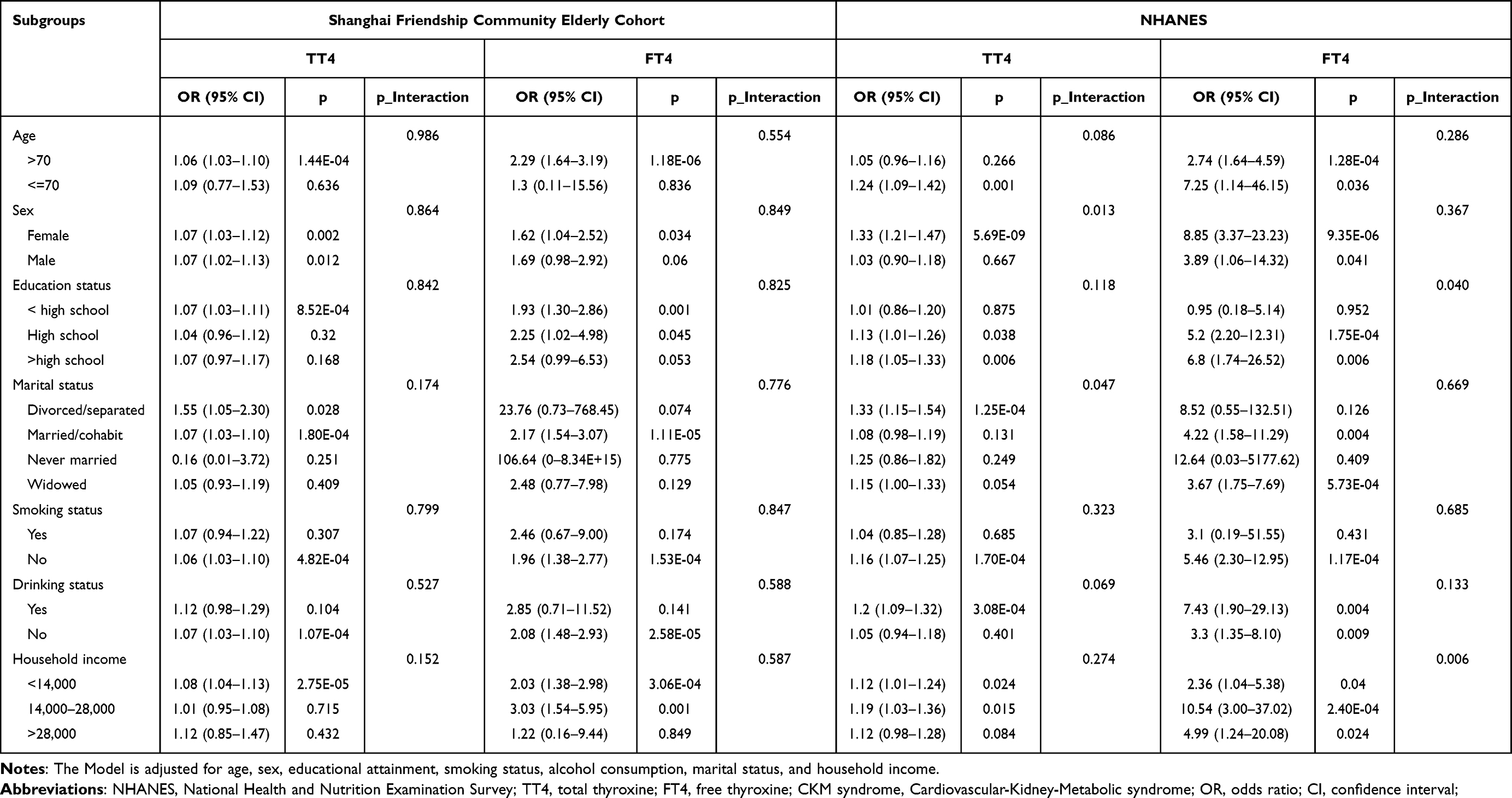 |
Table 3 Associations of TT4 and FT4 Levels with CKM Among Subgroups |
Baseline Characteristics by TT4 and FT4 Tertiles
Table 4 presents the baseline characteristics stratified by TT4 tertiles. Notably, a significant difference in TT4 levels was observed in gender subgroups, with females having higher TT4 levels in both SFCEC and NHANES cohorts (p < 0.05). Participants with higher TT4 tertiles showing greater prevalence of advanced CKM stages (Stages 1–4). However, analysis of FT4 tertiles revealed this association with CKM staging only in the SFCEC cohort, with no significant pattern observed in NHANES (p > 0.05). Related results are detailed in eTable 5.
 |
Table 4 Baseline Characteristics by TT4 Tertiles |
Dose–Response Relationships of TT4 and FT4 with CKM Syndrome
Restricted cubic spline (RCS) analyses revealed significant linear associations between thyroid hormone levels and CKM stages after full covariate adjustment (Figure 1). In the SFCEC cohort, TT4 levels showed a strong linear relationship with CKM risk (P-overall < 0.001; P-nonlinear = 0.379), with similar trends observed in NHANES (P-overall = 0.013; P-nonlinear = 0.404). For FT4, both cohorts demonstrated consistent linear dose-response patterns (SFCEC: P-overall = 0.028, P-nonlinear = 0.340; NHANES: P-overall = 0.016, P-nonlinear = 0.131), indicating progressively higher CKM risk with increasing TT4 or FT4 levels.
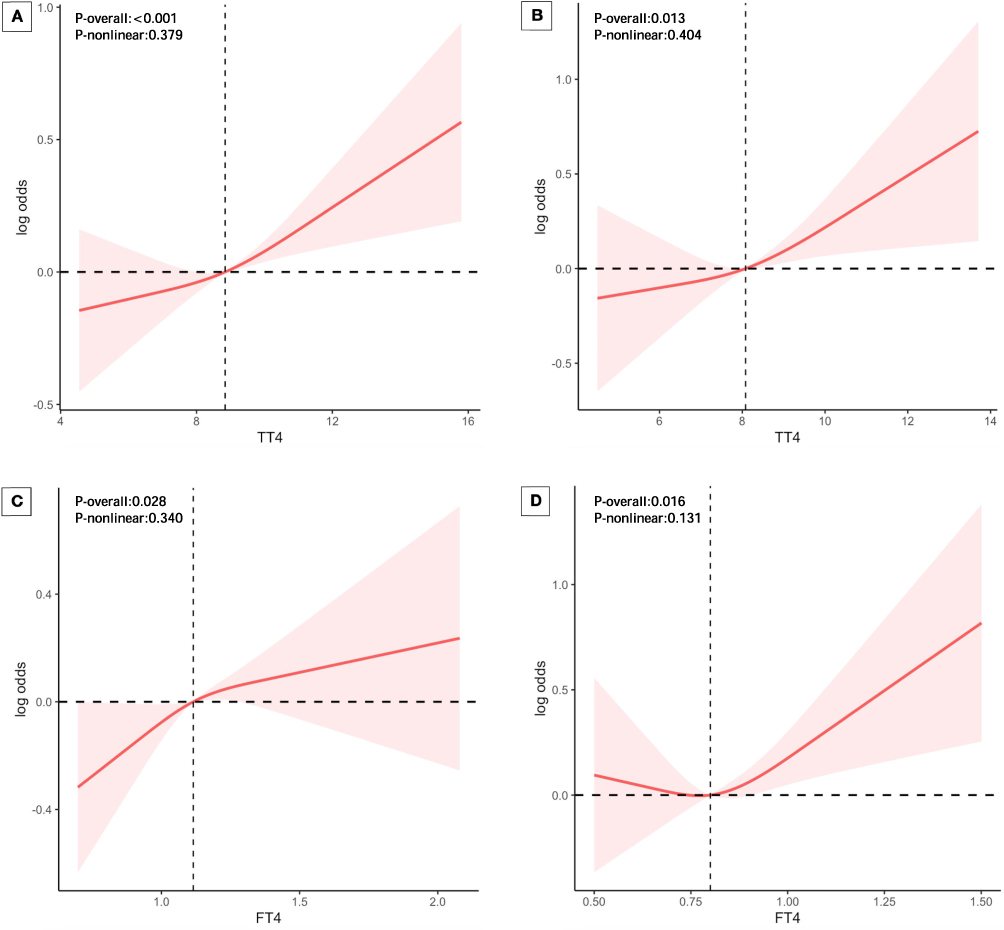 |
Figure 1 Restricted cubic spline plots of the association between TT4 and FT4 levels and CKM. (A) The association between TT4 levels and CKM in Shanghai Friendship Community Elderly Cohort. (B) The association between TT4 levels and CKM in NHANES. (C) The association between FT4 levels and CKM in Shanghai Friendship Community Elderly Cohort. (D) The association between FT4 levels and CKM in NHANES. The Model is adjusted for age, sex, educational attainment, smoking status, alcohol consumption, marital status, and household income. Abbreviations: NHANES, National Health and Nutrition Examination Survey; TT4, total thyroxine; FT4, free thyroxine; CKM syndrome, Cardiovascular-Kidney-Metabolic syndrome. Notes: The reference group (Stage 0) was small (n=55 in SFCEC, n=12 in NHANES); caution is needed when interpreting the slopes at lower T4 levels. |
Discussion
To our knowledge, this represents a large-scale study investigating the association between thyroid hormone levels and CKM syndrome stages using data from both Chinese (SFCEC) and US (NHANES) elderly populations. The remarkably high prevalence of CKM (approximately 98%) in both cohorts underscores the urgent need to identify modifiable risk factors in aging populations. Our key finding of a significant positive association between elevated TT4 and FT4 levels and CKM risk, supported by dose-response analyses, suggests that T4 may serve as potential biomarkers for CKM progression.
Previous research has clearly established important connections between abnormal thyroid hormone levels and key components of CKM syndrome including obesity, DM,CKD, and CVD. First, in our study, the proportion of obese patients was the highest (67.20% in the SFCEC cohort and 72.20% in the NHANES). Multiple studies have demonstrated that in carefully matched comparisons with lean individuals, obese subjects consistently show higher circulating TSH levels while maintaining normal or even slightly elevated FT4 concentrations,9 suggesting a complex relationship between obesity and thyroid function regulation. Importantly, longitudinal data from a Chinese cohort of 256 obese patients with initially normal thyroid function revealed significant reductions in both TT4 and FT4 levels following substantial weight loss achieved through partial gastrectomy,14 providing compelling evidence for reversible thyroid hormone alterations in obesity. These human findings are further supported by parallel observations in animal models where obese cats exhibited elevated TT4 and FT4 levels compared to their normal-weight counterparts.15 Second, regarding DM, well-designed clinical studies including Li Q et al’s investigation of 488 untreated patients from Eastern China have consistently reported significantly higher TT4 and FT4 levels in individuals with diabetes mellitus,16 highlighting thyroid hormones’ crucial role as master regulators of glucose metabolism through multiple mechanisms including modulation of insulin secretion, intestinal glucose absorption, hepatic gluconeogenesis, and peripheral tissue glucose uptake.17 Current evidence strongly suggests that even subtle variations in thyroid hormone levels within the conventional normal reference range may significantly influence diabetes risk,17 underscoring the importance of considering thyroid function in metabolic assessments. Third, regarding the relationship between thyroid function and CKD, existing studies demonstrate that thyroid dysfunction accelerates CKD progression, highlighting the necessity of monitoring thyroid function in CKD management.8 Furthermore, these studies have further elucidated the specific mechanisms by which thyroid abnormalities affect renal function through alterations in thyroid hormone synthesis.8 Interestingly, the study by Rhee CM et al observed a tendency for reduced TT4 levels in CKD patients,18 which differs from our current findings. This discrepancy may stem from the relatively lower proportion of CKD patients in our study population (see eTable 3). Furthermore, extensive research has established that abnormalities in thyroid hormone levels significantly disrupt lipid and glucose homeostasis and contribute to the pathogenesis of CVD.8 In a Turkish study of 95 patients with acute myocardial infarction (AMI), blood TT4 levels were significantly higher in AMI patients compared to controls—a finding consistent with our results.19 Additionally, a substantial proportion of elderly patients with CKM syndrome in our study exhibited dyslipidemia, with prevalence rates of 45.30% in the SFCEC cohort and 39.20% in the NHANES cohort. In conclusion, although existing evidence has established thyroid hormone dysregulation as a contributing factor to individual components of CKM syndrome such as obesity, DM, and CVD, the comprehensive relationship between thyroid function and integrated CKM staging remained poorly characterized prior to this study.
The strikingly high prevalence of CKM stages 1–4 in both elderly cohorts (approximately 98%) likely reflects cumulative age-related metabolic and cardiovascular risk factors. This near-universal burden suggests that CKM staging may have limited utility for early detection in older adults; instead, its clinical value may lie in distinguishing advanced stages (Stage 3–4)3 and predicting progression. Our finding of linear TT4/FT4 associations with higher stages supports their potential to identify individuals at risk for progressing to subclinical or clinical CVD. These results suggest that future studies should test whether CKM staging criteria need to be adjusted for older adults. Additionally, the two cohorts differed substantially in the prevalence of CKD (2.7% in SFCEC vs. 20.5% in NHANES) and established CVD (7.2% vs. 24.9%). These differences reflect underlying population health disparities, healthcare access, and possibly true epidemiologic differences. Despite these baseline differences, the positive association between TT4/FT4 and CKM stages remained consistent in both cohorts, suggesting that the relationship is robust across different disease profiles. Regarding racial composition, the NHANES cohort was predominantly Non-Hispanic White (80.5%, eTable 6). In contrast, the SFCEC cohort was ethnically homogeneous (Han Chinese, >99%). Despite these racial differences, both cohorts showed consistent positive associations between TT4/FT4 and CKM stages, suggesting that the observed relationship is not driven solely by a specific racial group. However, the sample sizes of non-White subgroups in NHANES were insufficient for adequately powered race-stratified analyses. Future multi-ethnic studies are needed to explore whether the thyroid-CKM association differs by race or ethnicity. Furthermore,our RCS analyses demonstrated linear TT4/FT4-CKM associations without a threshold effect, even among euthyroid participants. This raises the question of whether current T4 reference ranges,which are derived from healthy populations,are optimal for elderly risk assessment. Our findings indicate that higher T4 within the normal range is associated with more advanced CKM stages. Clinicians should note that upper-normal T4 may signal increased risk despite normal TSH. Future studies should test whether age-specific reference ranges are needed.
The precise biological mechanisms linking elevated TT4/FT4 levels with CKM syndrome remain to be fully elucidated. As a complex multisystem disorder, CKM syndrome is known to be driven by chronic systemic inflammation and oxidative stress.20 In obesity, overexpression of pro-inflammatory cytokines (eg., TNF-α, IL-6, MCP-1) promotes tissue specific inflammation and oxidative damage, contributing to cardiovascular and metabolic dysregulation.21 The kidneys are particularly susceptible to oxidative injury, where Reactive oxygen species (ROS) mediated damage to glomeruli and tubules may accelerate renal dysfunction.22 Similarly, in the cardiovascular system, oxidative stress promotes pathological remodeling processes underlying left ventricular hypertrophy and atherosclerosis.23,24 Thyroid hormones contribute to oxidative damage and inflammatory activation through multiple molecular pathways. On one hand, the phenolic hydroxyl group in thyroid hormones exhibit intrinsic oxidant capacity, enabling direct DNA damage.25 On the other hand, thyroid hormones enhance nitric oxide synthase (NOS) activity, leading to excessive nitric oxide (NO) production. They also activate the hepatic NF-κB pathway, which elevates cytokine levels and subsequently promotes the generation of reactive oxygen species (ROS).26 Additionally, circulating T4 binds membrane integrin αvβ3 to initiate MAPK-dependent upregulation of HIF-1α and COX2,27,28 which promotes NLRP3 inflammasome assembly.29,30 In parallel, the T4–integrin αvβ3 axis activates PI3K and AKT, thus inducing a robust production of ROS,11 as well as enhancing HIF-1α expression.28,31 These interconnected pathways demonstrate how thyroid hormones can potentiate oxidative stress and inflammatory responses through both direct molecular actions and complex signaling cascades. Notably, the absence of significant associations for TSH, FT3, and TT3 in the primary adjusted models points to a T4-specific peripheral mechanism rather than central hypothalamic-pituitary-thyroid axis dysregulation. This aligns with our hypothesis that T4 may act via integrin αvβ3 and non-genomic pathways to promote inflammation and oxidative stress,11 independent of TSH regulation or T3 conversion. Supporting the inflammatory hypothesis, recent NHANES analyses have provided two key insights: one study identified a positive correlation between thyroid hormone levels (TT4 or FT4) and systemic inflammatory markers (SIRI),32 while another established a link between the systemic immune-inflammation index (SII) and CKM syndrome.33 Collectively, these observations suggest that chronic inflammation may be a central mechanism bridging T4 with CKM pathogenesis.
In sensitivity analyses restricted to euthyroid individuals, higher TT3 levels were associated with lower odds of CKM, a finding that contrasts with the null results from the primary analysis. This inverse association may reflect reduced peripheral conversion of T4 to T3 due to systemic inflammation or illness (eg., low T3 syndrome),34 rather than a direct protective effect of T3 itself. Future studies should measure deiodinase activity and T4/T3 ratios to clarify the underlying mechanisms. We therefore interpret this euthyroid-subgroup finding as hypothesis-generating, requiring confirmation in future mechanistic studies.
Strengths and Limitations
This study possesses several notable strengths. First, we analyzed data from two large, well-characterized cohorts - the Shanghai Friendship Community Elderly Cohort (SFCEC) and the nationally representative US NHANES population - enhancing the generalizability of our findings across distinct ethnic groups. Second, our analytical approach rigorously accounted for NHANES’s complex survey design through appropriate weighting, stratification, and clustering adjustments, ensuring robust population-level estimates.
However, several limitations warrant consideration. First, this is an observational study, and the associations observed cannot establish causality. Second, although we adjusted for comprehensive demographic and lifestyle confounders, residual confounding from unmeasured factors (eg., thyroid autoantibodies) cannot be excluded. Third, the predominantly elderly study population may limit extrapolation of our findings to younger adults. Fourth, despite statistical adjustment, the two cohorts differed substantially in education, income, and alcohol consumption, which may introduce residual bias. However, the consistent TT4/FT4 association across both cohorts argues against major confounding by these factors. Fifth, we lacked detailed information on the severity of hypertension and diabetes, as well as the duration of medication use. Only current use of antihypertensive, antidiabetic, and lipid-lowering drugs (yes/no) was recorded. Furthermore, as a sensitivity analysis, we repeated analyses in euthyroid participants. While the positive association with elevated TT4 and FT4 persisted, the relationship with other hormones (eg., TT3) differed. These exploratory findings underscore the complexity of thyroid-CKM relationships and suggest future mechanistic studies are needed to investigate how specific thyroid hormone signaling pathways contribute to CKM pathogenesis, potentially revealing novel therapeutic targets.
Conclusions
In summary, this study identified elevated TT4 and FT4 levels as potential independent risk markers for CKM syndrome in elderly populations from both China and the United States. The consistency of these findings across diverse cohorts suggests that free and total thyroxine levels could serve as clinically useful biomarkers for monitoring CKM progression in aging adults. Consequently, clinical screening of TT4 and FT4 levels may aid in risk stratification for CKM progression. Further research, particularly prospective longitudinal studies, is warranted to confirm these associations and to elucidate the mechanistic role of thyroxine in the development of CKM over time.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
The authors did not use any AI at all in the writing process.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; TT4, total thyroxine; FT4, free thyroxine; TT3, total triiodothyronine; FT3, free triiodothyronine; TSH, thyroid-stimulating hormone;CKM syndrome, Cardiovascular-Kidney-Metabolic syndrome;DM, diabetes mellitus;CKD,chronic kidney disease;CVD,cardiovascular disease;OR, odds ratio; CI, confidence interval;Ref, reference; T1, Tertile 1; T2, Tertile 2; T3, Tertile 3.
Data Sharing Statement
The NHANES data are publicly available (https://wwwn.cdc.gov/nchs/nhanes/). The SFCEC data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All studies involved in this research adhered to the ethical principles of the Declaration of Helsinki (1975) and were approved by the respective ethics committees. Specifically, the SFCEC study protocol was approved by the Institutional Review Board of Huashan Hospital Affiliated to Fudan University (Approval No. 2020-004). The NHANES study received ethical approval from the National Center for Health Statistics (NCHS) Research Ethics Review Board, and its procedures complied with the Declaration of Helsinki. Further details are available at: https://www.cdc.gov/nchs/nhanes/.All participants executed a written informed consent form before their involvement.
Acknowledgments
The data used in this research were obtained from the Shanghai Friendship Community Elderly Cohort (SFCEC) and US National Health and Nutrition Examination Survey (NHANES). We would like to thank the workers, researchers, and participants involved in the SFCEC and NHANES.
Author Contributions
Kangan Wang: Formal analysis, Writing – original draft. Wencai Ke: Investigation, Resources, Writing – review & editing. Li Sheng: Methodology, Validation, Writing – review & editing. Kai Wang: Funding acquisition, Writing – review & editing. Biying Wu: Investigation, Supervision, Writing – review & editing. Leqi He: Investigation, Supervision, Writing – review & editing. Shu Peng: Investigation,Supervision, Writing – review & editing. Yong Lin: Resources, Funding acquisition, Methodology,Writing – review & editing. Bingbing Zha: Conceptualization, Methodology, Writing – review & editing.All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shanghai Municipal Key Clinical Specialty (No. 2024ZDXK0016),the Medical Specialty Construction Project of Minhang District, Shanghai (No.2025MWTZB01),the Foundation of Shanghai Fifth People’s Hospital (No.2022WYZD01),and the Shanghai Municipal Health Commission Clinical Research Special Fund (No.20254Y0124).
Disclosure
No potential conflict of interest was reported by the author(s).
References
1. Ndumele CE, Neeland IJ, Tuttle KR, et al. A synopsis of the evidence for the science and clinical management of Cardiovascular-Kidney-Metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023;148(20):1636–13. doi:10.1161/CIR.0000000000001186
2. Aggarwal R, Ostrominski JW, Vaduganathan M. Prevalence of cardiovascular-kidney-metabolic syndrome stages in US adults, 2011-2020. JAMA. 2024;331(21):1858–1860. doi:10.1001/jama.2024.6892
3. Zhu R, Wang R, He J, et al. Prevalence of cardiovascular-kidney-metabolic syndrome stages by social determinants of health. JAMA Network Open. 2024;7(11):e2445309. doi:10.1001/jamanetworkopen.2024.45309
4. Chen A, He Q, Wu Y, et al. Incidence of cardiovascular-kidney metabolic syndrome and its risk factors for progression in China. medRxiv. 2024.
5. Ndumele CE, Rangaswami J, Chow SL, et al. Cardiovascular-Kidney-Metabolic health: a presidential advisory from the American Heart Association. Circulation. 2023;148(20):1606–1635. doi:10.1161/CIR.0000000000001184
6. Williams GR. Neurodevelopmental and neurophysiological actions of thyroid hormone. J Neuroendocrinol. 2008;20(6):784–794. doi:10.1111/j.1365-2826.2008.01733.x
7. Danzi S, Klein I. Thyroid hormone and the cardiovascular system. Med Clin North Am. 2012;96(2):257–268. doi:10.1016/j.mcna.2012.01.006
8. Jiang L, Zhou L, Liu J, Wang Y, Wang G. Sex differences in the association between thyroid hormone sensitivity and cardiovascular-kidney-metabolic syndrome. J Clin Endocrinol Metab. 2025. doi:10.1210/clinem/dgaf059
9. Laurberg P, Knudsen N, Andersen S, Carlé A, Pedersen IB, Karmisholt J. Thyroid function and obesity. Eur Thyroid J. 2012;1(3):159–167. doi:10.1159/000342994
10. Iglesias P, Díez JJ. Thyroid dysfunction and kidney disease. Eur J Endocrinol. 2009;160(4):503–515. doi:10.1530/EJE-08-0837
11. De Vito P, Balducci V, Leone S, et al. Nongenomic effects of thyroid hormones on the immune system cells: new targets, old players. Steroids. 2012;77(10):988–995. doi:10.1016/j.steroids.2012.02.018
12. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of Chronic kidney disease. Kidney Int. 2024;105(4S):S117–S314. doi:10.1016/j.kint.2023.10.018
13. Liu F, Wang K, Nie J, et al.Relationship between dietary selenium intake and serum thyroid function measures in U.S. adults: data from NHANES.Front Nutr.2022.9;1002489. doi:10.3389/fnut.2022.1002489
14. Tian Z, Nie Y, Li Z, et al. Total weight loss induces the alteration in thyroid function after bariatric surgery. Front Endocrinol. 2024;15:1333033. doi:10.3389/fendo.2024.1333033
15. Ferguson DC, Caffall Z, Hoenig M. Obesity increases free thyroxine proportionally to nonesterified fatty acid concentrations in adult neutered female cats. J Endocrinol. 2007;194(2):267–273. doi:10.1677/JOE-07-0064
16. Li Q, Lu M, Wang NJ, et al. Relationship between free thyroxine and islet beta-cell function in euthyroid subjects. Curr Med Sci. 2020;40(1):69–77. doi:10.1007/s11596-020-2148-6
17. Jun JE, Jee JH, Bae JC, et al. Association between changes in thyroid hormones and incident type 2 diabetes: a seven-year longitudinal study. Thyroid. 2017;27(1):29–38. doi:10.1089/thy.2016.0171
18. Rhee CM, Brent GA, Kovesdy CP, et al. Thyroid functional disease: an under-recognized cardiovascular risk factor in kidney disease patients. Nephrol Dial Transplant. 2015;30(5):724–737. doi:10.1093/ndt/gfu024
19. Satar S, Seydaoglu G, Avci A, Sebe A, Karcioglu O, Topal M. Prognostic value of thyroid hormone levels in acute myocardial infarction: just an epiphenomenon? Am Heart Hosp J. 2005;3(4):227–233. doi:10.1111/j.1541-9215.2005.04653.x
20. Sebastian SA, Padda I, Johal G. Cardiovascular-Kidney-Metabolic (CKM) syndrome: a state-of-the-art review. Curr Probl Cardiol. 2024;49(2):102344. doi:10.1016/j.cpcardiol.2023.102344
21. Soták M, Clark M, Suur BE, Börgeson E. Inflammation and resolution in obesity. Nat Rev Endocrinol. 2025;21(1):45–61. doi:10.1038/s41574-024-01047-y
22. Daenen K, Andries A, Mekahli D, Van Schepdael A, Jouret F, Bammens B. Oxidative stress in chronic kidney disease. Pediatr Nephrol. 2019;34(6):975–991. doi:10.1007/s00467-018-4005-4
23. Tran N, Garcia T, Aniqa M, Ali S, Ally A, Nauli SM. Endothelial Nitric Oxide Synthase (eNOS) and the cardiovascular system: in physiology and in disease states. Am J Biomed Sci Res. 2022;15(2):153–177.
24. Zhang PY, Xu X, Li XC. Cardiovascular diseases: oxidative damage and antioxidant protection. Eur Rev Med Pharmacol Sci. 2014;18(20):3091–3096.
25. Dobrzyńska MM, Baumgartner A, Anderson D. Antioxidants modulate thyroid hormone- and noradrenaline-induced DNA damage in human sperm. Mutagenesis. 2004;19(4):325–330. doi:10.1093/mutage/geh037
26. Venditti P, Di Meo S. Thyroid hormone-induced oxidative stress. Cell Mol Life Sci. 2006;63(4):414–434. doi:10.1007/s00018-005-5457-9
27. De Vito P, Incerpi S, Pedersen JZ, Luly P, Davis FB, Davis PJ. Thyroid hormones as modulators of immune activities at the cellular level. Thyroid. 2011;21(8):879–890. doi:10.1089/thy.2010.0429
28. Lin HY, Su YF, Hsieh MT, et al. Nuclear monomeric integrin αv in cancer cells is a coactivator regulated by thyroid hormone. FASEB J. 2013;27(8):3209–3216. doi:10.1096/fj.12-227132
29. Hua KF, Chou JC, Ka SM, et al. Cyclooxygenase-2 regulates NLRP3 inflammasome-derived IL-1β production. J Cell Physiol. 2015;230(4):863–874. doi:10.1002/jcp.24815
30. Gupta N, Sahu A, Prabhakar A, et al. Activation of NLRP3 inflammasome complex potentiates venous thrombosis in response to hypoxia. Proc Natl Acad Sci U S A. 2017;114(18):4763–4768. doi:10.1073/pnas.1620458114
31. Hsieh MT, Wang LM, Changou CA, et al. Crosstalk between integrin αvβ3 and ERα contributes to thyroid hormone-induced proliferation of ovarian cancer cells. Oncotarget. 2017;8(15):24237–24249. doi:10.18632/oncotarget.10757
32. Zhai Y, Wang B, Han W, Yu B, Ci J, An F. Correlation between systemic inflammatory response index and thyroid function: 2009-2012 NHANES results. Front Endocrinol. 2024;14:1305386. doi:10.3389/fendo.2023.1305386
33. Gao C, Gao S, Zhao R, et al. Association between systemic immune-inflammation index and cardiovascular-kidney-metabolic syndrome. Sci Rep 2024;14(1):19151. doi:10.1038/s41598-024-69819-0
34. Lubrano V, Pingitore A, Carpi A, Iervasi G. Relationship between triiodothyronine and proinflammatory cytokines in chronic heart failure. Biomed Pharmacother. 2010;64(3):165–169. doi:10.1016/j.biopha.2009.09.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.