")
Back to Journals » Infection and Drug Resistance » Volume 16
Fractional Dosing of Yellow Fever Live Attenuated 17D Vaccine: A Perspective
Authors Hansen CA , Staples JE, Barrett AD
Received 24 May 2023
Accepted for publication 20 September 2023
Published 8 November 2023 Volume 2023:16 Pages 7141—7154
DOI https://doi.org/10.2147/IDR.S370013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Clairissa A Hansen,1 J Erin Staples,2 Alan DT Barrett1
1Department of Pathology and Sealy Institute for Vaccine Sciences, University of Texas Medical Branch, Galveston, TX, 77555-4036, USA; 2Arboviral Diseases Branch, U.S. Centers for Disease Control and Prevention, Fort Collins, CO, USA
Correspondence: Alan DT Barrett, Sealy Institute for Vaccine Sciences, University of Texas Medical Branch, Galveston, TX, 77555-0436, USA, Tel +1 409 772 6662, Fax +1 409 772 6663, Email [email protected]
Abstract: Yellow fever virus (YFV) is a mosquito-borne flavivirus that causes over 109,000 severe infections and over 51,000 deaths annually in endemic areas of sub-Saharan Africa and tropical South America. The virus has a transmission cycle involving mosquitoes and humans or non-human primates (NHPs) as the vertebrate hosts. Although yellow fever (YF) is prevented by a live attenuated vaccine (strain 17D), recent epidemics in Angola, the Democratic Republic of the Congo (DRC), and Brazil put great pressure on vaccine stockpiles. This resulted in the World Health Organization (WHO) and Pan American Health Organization (PAHO) implementing, on an emergency basis only, off-label dose-sparing techniques and policies during 2016– 2018 to protect as many people in DRC and Brazil as possible from disease during unexpected large outbreaks of YF. Subsequently non-inferiority studies involving full doses compared to fractional doses indicated promising results, leading some policy-makers and scientists to consider utilizing YF vaccine fractional doses in non-emergency scenarios. Although the additional data on the immunogenicity and safety of fractional doses are promising, there are several questions and considerations that remain regarding the use of fractional doses, including differences in the initial antibody kinetics, differences in the immune response in certain populations, and durability of the immune response to fractional doses compared to full doses. Until the remaining knowledge gaps are addressed, full doses instead of fractional doses should continue to be used unless there are insufficient doses of the vaccine available to control outbreaks of YF.
Plain Language Summary: Yellow fever (YF) disease is prevented by a live attenuated vaccine, strain 17D. Its production is confined by the need to be grown and harvested in embryonated chicken eggs. This can result in limited supplies of 17D vaccine, particularly during periods of increased demand. In 2016– 2018, the vaccine stockpile was exhausted on multiple occasions. This led to the vaccine being used at one-fifth of a dose, so-called “dose-sparing” or “fractional dosing”. Clinical trials support the safety and immunogenicity of fractional dosing, with all 17D vaccines used as a fractional dose having a non-inferior antibody response (ie, seroconversion) to a full dose at 28 days. The use of fractional dosing during 2016– 2018 was very successful in controlling outbreaks. However, there are limited data on the use of fractional doses in populations who might have an altered immune response and the durability of the immune response. As such, the World Health Organization only approves use of fractional dosing in emergency scenarios. The successes of fractional dosing campaigns and clinical trials are encouraging and could lead to further consideration of the use of fractional doses of YF vaccine once the remaining knowledge gaps have been addressed.
Keywords: dose-sparing, vaccinology, outbreak response, virus
The Disease and Transmission
Yellow fever virus (YFV) is the prototypic flavivirus and causes yellow fever (YF). YFV infection can result in asymptomatic infection, or mild to severe disease. Severe disease with hemorrhage and multisystem organ dysfunction is seen in approximately one in every seven infected people and results in 30–60% mortality.1 Despite the availability of a live attenuated vaccine to control the disease, it is estimated that there are 109,000 severe infections and 51,000 deaths due to YF each year and occurrence of outbreaks have increased in the last decade.2,3 The disease is considered endemic in 47 countries in tropical South America and sub-Saharan Africa, with 90% of cases reported in Africa.4
Yellow fever virus is a mosquito-borne flavivirus that exists in a sylvatic transmission cycle involving mosquitoes (namely, Aedes africanus in Africa and Haemagogus or Sabethes species in South America) and non-human primates (NHPs).5,6 Humans are involved with YFV amplification in either the intermediate transmission cycle involving semi-domestic Aedes species (eg, Aedes simpsoni) mosquitoes or the urban transmission cycle involving Aedes aegypti. Although the intermediate and urban cycles have been traditionally linked to large outbreaks of YF, the recent large outbreaks in Brazil were associated with sylvatic transmission occurring in areas where there was little to no population immunity.
The Vaccine
Yellow fever disease can be prevented by a live-attenuated vaccine, strain 17D, which was developed by Max Theiler and colleagues and has been in use since the 1930s. 17D was derived by 176 passages of the wild type Asibi strain in various tissue preparations, namely, minced mouse embryo, minced chick embryo, and minced chick embryo without central nervous tissue. There are three substrains of 17D in use today (17D-204, 17DD, and 17D-213) – all of which are derived from the original 17D strain – that are produced in embryonated chicken eggs by six manufacturers (Institut Pasteur, Senegal; Bio-Manguinhos/Fiocruz, Brazil; Chumakov Institute of Poliomyelitis and Viral Encephalitides, Russia; Sanofi Pasteur, France; Sanofi Pasteur, United States; and Wuhan Institute of Biological Products, China) (Figure 1). All vaccines except those produced in the US and China are prequalified by the World Health Organization (WHO) and can be used in YFV-endemic countries.7 Per manufacturing requirements, each vaccine dose contains a minimum of 1000 International Units (IU) of virus. In practice, each dose usually contains more than 10,000 IU, in part to protect vaccine stability and compensate for the potential of virus degradation over the shelf life.8 There is no requirement of a maximum amount of virus in a vaccine dose. YF vaccines typically take months, if not more than one year (if stock is not available), to be produced and released for use in humans.
 |
Figure 1 YF vaccines currently produced around the world. Those on top and in green boxes are WHO prequalified and are used in routine, preventive, and reactive vaccination campaigns in endemic areas. Those on the bottom and in purple are not WHO prequalified and are mostly used as travel vaccines in the country of manufacture, with limited exportation to other countries (eg, YF-VAX ® is imported and used in Canada and Japan). |
Clinical studies have shown that antibodies against YFV elicited by the vaccine can be detected up to 60 years after vaccination and it is thought that one dose gives life-long protection.4,9–11 Because of the empirical nature of the development of the 17D strain in the 1930s, there is limited understanding of the molecular basis of attenuation and immunogenicity.
Recent Outbreaks and Response
Despite the presence of a vaccine, YF occurrence has been increasing, with recent outbreaks of significant public health concern occuring in multiple countries (Figure 2). In Angola from 2015–2016, there were 4347 suspected cases, 884 confirmed cases, and 377 deaths associated with YF.12 This outbreak also infected 11 people who returned to their home in China, highlighting the potential ease with which the virus can be spread (Figure 2).13 In addition, there was an outbreak in Uganda in 2016, with 42 confirmed and probable cases of YF from likely sylvatic transmission.14 Concurrent with the 2015–2016 outbreak in Angola, there were 78 confirmed cases of YF in the Democratic Republic of the Congo (DRC), several of which were in Kinshasa, the capital city, where traditionally YFV has not circulated.15 In Brazil, there were >2000 confirmed cases, >500 deaths, and >4000 epizootics (disease in NHPs) between December 2016 and March 2018.16 The outbreaks in Brazil occurred not only in endemic areas but also in regions that had not had YF cases since the 1940s and had minimal vaccination coverage in their population. During this same timeframe, Nigeria saw an increase in case recognition, with almost 8000 suspected cases and 287 laboratory-confirmed cases.17
 |
Figure 2 Timeline of events and clinical trials relating to fractional dosing of the YF vaccine. Grey triangles indicate periods of time when significant outbreaks occurred. Not all clinical trials are listed. Abbreviations: ARD – Autoimmune rheumatic diseases; CATMAT – Canadian Committee to Advise on Tropical Medicine and Travel; DRC – Democratic Republic of Congo; eIND – emergency investigation new drug; EYE – Eliminate Yellow fever Epidemics; FDA – Food and Drug Administration; PLWH – persons living with human immunodeficiency virus; SAGE – Strategic Advisory Group of Experts on Immunization; USA – United States of America; WHO – World Health Organization; YF – yellow fever. The figure was created with BioRender.com. |
There are several factors that have likely contributed to the resurgence of YF. Competing public health priorities (eg, Ebola, COVID) and increased regional conflicts in risk areas have resulted in decreased childhood vaccination rates and limited capacity to prevent and respond to outbreaks. For areas impacted with cases often for the first time in decades, the increase is likely multifactorial involving climate change, vector factors, population movement, and improvements in surveillance and testing for YF.18 While routine immunization is the approach of choice to reach people in endemic areas, many such areas lack adequate vaccination coverage because of lapses in prior vaccine programs and no or low coverage in the routine childhood program. YF virus cannot be eradicated due to its enzootic circulation and, without high sustained vaccination coverage, outbreaks of the disease will occur. Since 2010, WHO has maintained an annual stockpile of up to 6 million doses of vaccine for outbreak control. However, these reserves have not always been sufficient.19 The large outbreak that took place in Angola and the DRC in 2016 exhausted the vaccine stockpile multiple times (Figure 2). Similarly, high demand for vaccine in Brazil in the 2017–2018 outbreaks resulted in exhaustion of available vaccine.20,21
In response to these large outbreaks and limited vaccine supply, WHO developed and implemented the Eliminate Yellow fever Epidemics (EYE) strategy, with the following main objectives: (1) to protect at-risk populations; (2) to prevent international spread of the disease; and (3) to contain outbreaks rapidly. To achieve these objectives by 2026, EYE strategy is working to increase surveillance and testing for YF as well as to improve YF vaccine availability and YF vaccination coverage by vaccinating over 1 billion people.19 Under the EYE strategy and with support of international organizations, there are currently 50–150 million doses of 17D vaccine produced annually, an increase in the over 20 million that were previously available. In addition, the EYE strategy changed annual allocation of doses to stockpile to a revolving stockpile. Even with the potential increase this creates for the stockpile, any doses needed for outbreak beyond the initial 6 million will be taken from planned preventive campaigns and lead to potential exhaustion of stocks (also known as stock outs) for the routine program.
Vaccine “Fractional Dosing” or “Dose Sparing”
One potential approach to expand availability of vaccine in times of shortage is to use a fraction of each approved dose. For example, an ampule that contains one full dose of YF vaccine is presented freeze-dried and reconstituted such that each full dose has 0.5mL volume and is given by the approved subcutaneous (s.c.) or intramuscular (i.m.) routes.22 This vaccine ampule could be used to vaccinate two to five individuals with a fractional dose of 0.25mL to 0.1mL, respectively, by using an appropriately gauged syringe (eg, tuberculin). With this technique, the vaccinator does not have to change the route of administration and can accurately deliver the desired amount. Two terms used interchangeably for this process are “dose-sparing” and “fractional dosing”. Dose-sparing typically refers to the action of using minimal doses to save the vaccine in times of need, while fractional dosing is a method of dose-sparing. The WHO Strategic Advisory Group of Experts on Immunization (SAGE) has referred to this as “fractional dosing” because this method meets the requirement for the vaccine’s minimal effective dose and uses a fraction of the volume of the normal dose.23 The use of a fraction of the volume of the YF vaccine was preferred in comparison to diluting the vaccine because adding extra diluent could alter vaccine composition and impact its viability.
Fractional dosing was used when the YF vaccine stockpiles were exhausted by the responses in Angola, DRC, and Uganda in 2016 and in Brazil in 2018 (Figure 2). In 2016, WHO discussed the use of fractional dosing and enlisted subject matter experts to analyze the available data on the efficacy and feasibility of fractional dosing. WHO SAGE then reviewed the findings and approved the use of vaccine as a preemptive measure to control outbreaks of the disease when there were insufficient doses of the vaccine available.
The first implementation of this recommendation came in August 2016, when ongoing YF cases in and around Kinshasa and minimal to no vaccine doses were available. WHO recommended that one-fifth (0.1mL) of the standard dose (0.5mL) of 17DD from Bio-Manguinhos/Fiocruz be given to approximately 7 million non-pregnant adults and children aged 2 years and above in Kinshasa, DRC. Children under 2 years of age and pregnant women were prioritized to receive a full dose given the lack of data about these groups at the time to support the use of fractional doses.24 The goal was to protect as many people as possible before the rainy season began and was considered one of the largest emergency vaccination campaigns for YF in Africa.25 Similarly, 17 million people out of over 22 million vaccinees were given fractional doses in Sao Paolo, Rio de Janeiro, and Bahia, Brazil in 2018.12,26
One smaller fractional dosing event took place in Canada in 2016–2018.27 Canada utilizes YF vaccine produced in the US (YF-VAX®, Sanofi Pasteur, 17D-204) to immunize travelers going to YF-endemic areas. Delays in building a new production facility for YF-VAX® in the US led to a stock out of the vaccine starting in 2016. The US Food and Drug Administration (FDA) approved an emergency Investigational New Drug (eIND) authorization for Stamaril®, YF 17D-204 vaccine produced by Sanofi Pasteur in France, to be imported and used as a full dose among US travelers. In contrast, the Canadian Committee to Advise on Tropical Medicine and Travel (CATMAT) did not have the authority to make decisions to import or license vaccines, but they were able to propose off-label recommendations for existing vaccines in Canada. When there was a shortage of YF-VAX®, CATMAT recommended fractional dosing for travelers, especially because of the outbreaks occurring in endemic areas.27,28
Justification of Dose-Sparing Response
The first group to test lower doses of the YF vaccine were Max Theiler and colleagues. Using minimum mouse lethal doses (MLD) as a measure of infectivity (as these studies were undertaken before cell culture had been established), they inoculated Rhesus monkeys by the s.c. route with vaccine doses varying between 0.13 and 73,000,000 MLD.29 One month post-inoculation, seven of the eight monkeys seroconverted with only the monkey receiving 13 MLD being seronegative. There did not seem to be a correlation between titer of virus given and resulting titer of serum antibodies.
The decision by the WHO and other public health entities to utilize this dose-sparing response in the DRC was supported scientifically by more recent literature, including four main studies: Lopes et al, 1988, Roukens et al, 2008, Martins et al, 2013, and Campi-Azevedo et al, 2014 (Table 1) (Figure 2).30–34 All but Roukens et al utilized the 17DD substrain in their clinical trials, while Roukens utilized Stamaril® 17D-204 substrain from Sanofi Pasteur. Subsequent studies have shown that the data on dose-sparing are relevant to all 17D vaccines in use today (see below).35 For context, standard doses of 17D-204, 17DD, and 17D-213 substrain vaccines have been found to be on average over 16,000, 38,000, and 43000 IU, respectively.35
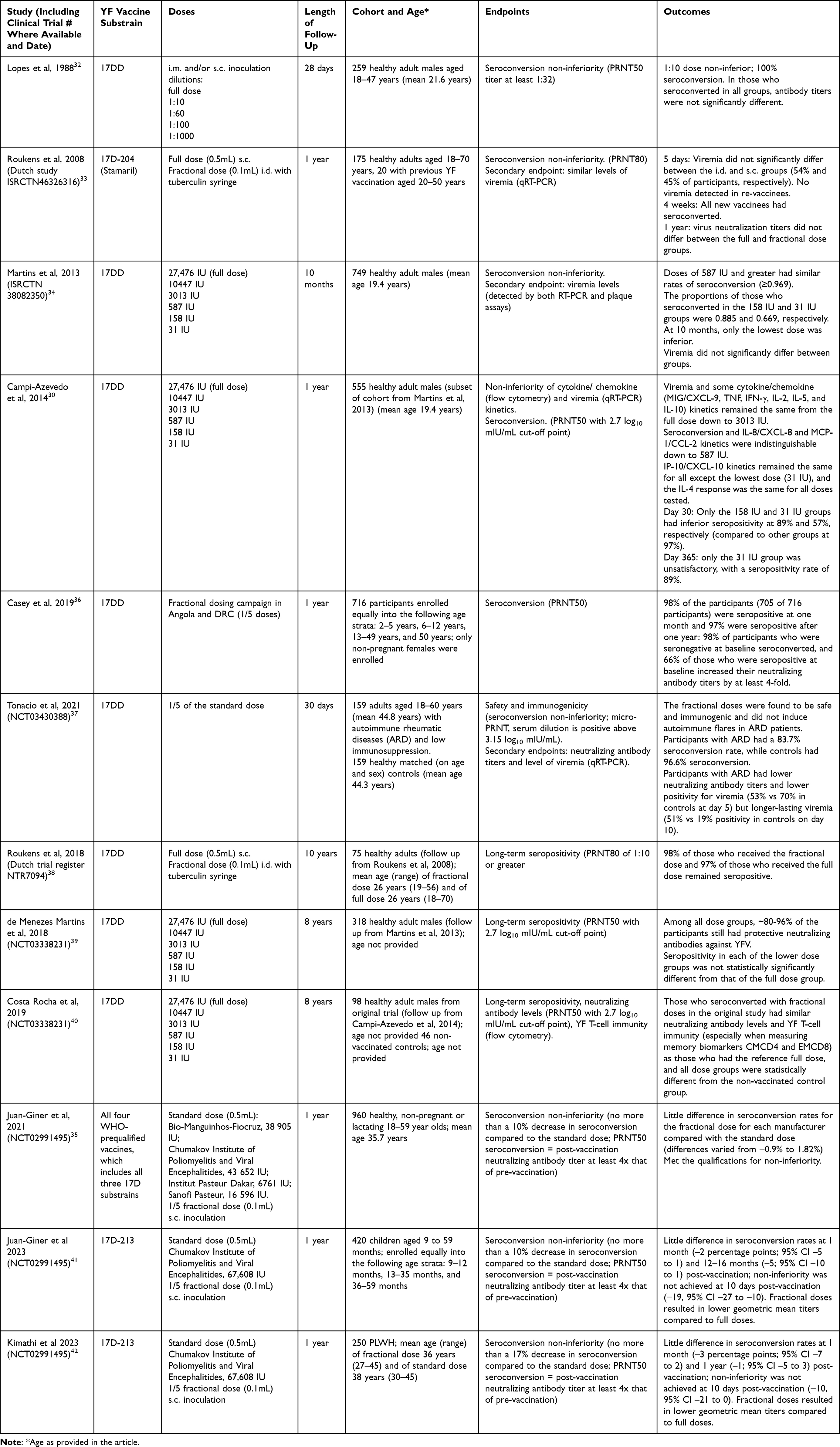 |
Table 1 Current Data from Clinical Trials on YF Vaccine Dose-Sparing |
To analyze YFV immunity, most studies utilize seroconversion and neutralizing antibodies as the correlate of protection, usually quantifying these outcomes with the 50–80% Plaque Reduction Neutralization Test (PRNT50 and/or PRNT80).10,20,43 Lopes et al tested 17DD from Bio-Manguinhos/Fiocruz via the traditional i.m. and/or s.c. injection route as full and fractional doses at dilutions from 1:10 to 1:1000 of a full dose in healthy adult males (Table 1).32 The 1:10 dilution of 17DD vaccine elicited seroconversion in 100% of the trial participants in that group, suggesting it was non-inferior to a full dose. All participants who seroconverted to YFV had approximately the same neutralizing antibody titers, regardless of which dilution/dose of vaccine they received.
In 2013, Martins et al conducted a non-inferiority study of five alternative vaccine formulations (ISRCTN 38082350) (Table 1).34 The six arms of the study were the 17DD reference vaccine from Bio-Manguinhos/Fiocruz at 27476 IU and serial 3-fold dilutions of the vaccine, which were titrated and found to range from 31 to 10447 IU. All 749 participants in the per-protocol analysis were healthy male soldiers from Rio de Janeiro. Blood was collected before vaccination, at 5 days, 30 days, and 10 months post-vaccination. Those who did not seroconvert were re-vaccinated with a full dose after the completion of the study. The rate of seroconversion by day 30 was approximately the same in the groups with the four highest doses, ie, 587 IU or greater (≥0.969; proportion of participants who seroconverted). After 10 months, only the 31 IU group had a lower seroconversion rate. Mean antibody titers waned after 10 months in all groups but were not statistically different from those participants given the reference vaccine as a full dose. Some participants in all groups had viremia from 3–6 days post-vaccination, but there was no statistically significant difference in level or timing of viremia among the groups. There was also no apparent relationship between viral particles detected, amount of virus given as vaccine, and no statistically significant difference in adverse events when controlling for level of viremia. The only adverse event that significantly differed between the different groups was more pain in the reference group with the full dose. The authors concluded that it is not “justifiable” to continue with the reference full dose as the standard dose, except for in children where there were no data. They also noted the need to determine longer-term immunity in all vaccinees.
Utilizing the same cohort as Martins et al, Campi-Azevedo et al published additional data on cytokine and chemokine kinetics (Table 1).30 They utilized blood collected up to 30 days post-vaccination. They found that viremia and certain cytokine/chemokine (MIG/CXCL-9, TNF, IFN-γ, IL-2, IL-5, and IL-10) kinetics (measured as fold-changes from baseline) remained the same for the three highest doses tested (down to 3013 IU). Seroconversion and IL-8/CXCL-8 and MCP-1/CCL-2 kinetics were indistinguishable for the four highest doses (ie, down to 587 IU). IP-10/CXCL-10 kinetics remained the same for all except the lowest dose (31 IU), and the IL-4 response was the same for all the doses tested. No association was found between the level of viremia and the cellular immune response though the numbers were limited; this is an area for further research.
In 2008, Roukens et al tested fractional 17D-204 YF vaccine via the intradermal (i.d.) route, recruiting 175 healthy adults, 20 of whom had received a previous YF vaccination (Dutch study ISRCTN46326316) (Table 1).33 One group received the standard Stamaril (17D-204 substrain) dose of 0.5mL s.c. while the other group received a fractional dose at 0.1mL i.d. via a tuberculin syringe. Blood was collected for serology up to 1 year. The cutoff for seropositivity for vaccinees was set at 80% reduction in viral infectivity (measured by PRNT80). All new vaccinees had seroconverted by four weeks and virus neutralization titers did not differ between the full and fractional dose groups when they were measured at one year post-vaccination. Blood collected and tested at 5 days post-vaccination did not find a significant difference between a subset of the i.d. and s.c. groups (54% and 45% of participants, respectively), with no viremia seen in re-vaccinees. The level of viremia did not correlate with virus neutralization. The safety and tolerability profile of the i.d. administration was similar to that of s.c. administration, although more frequent adverse events such as pain, swelling, and redness at the injection site were reported after i.d. administration.
From these studies, WHO concluded that a fractional dose of the 17DD substrain YF vaccine would be preferred and should contain ideally no less than 3013 IU because this was the lowest dose that had all virologic and immunologic measurements non-inferior to a full dose. Five years of batch potency data on the 17DD vaccine indicated that one-fifth of a dose of the average batch potency was 8709 IU and one-fifth of a dose of the minimum batch potency was 2692 IU, which are well above the current minimum dose of 1000 IU and close to the preferred minimum dose of 3013 IU.23,30,32,34 Based on this information, the 17DD vaccine substrain was used at one-fifth of a full dose in DRC.
During the fractional dose campaign in Kinshasa, immunogenicity data were collected on a subset of individuals who sought vaccination at six of the over 1000 vaccine posts placed throughout the city. Samples were collected at baseline prior to vaccination, and at one month and one year post-vaccination in children two years of age or older and in non-pregnant adults.36 Of participants, 98% (705/716) were seropositive at one month and 97% (666/684) were seropositive after one year, as measured by PRNT50 neutralization test, the cutoff for which had been previously established in vaccine clinical trials and by the WHO.8,44,45 98% (483/493) participants who were seronegative at baseline seroconverted. Of participants who were seropositive at baseline, 66% (148/223) had an immune response defined as a 4-fold or greater increase in neutralizing antibody titer compared to their titer before vaccination. Those individuals with higher baseline titers were significantly less likely to have an immune response, likely due to sterilizing immunity. The outcome of dose-sparing in DRC has protected millions of people against YF. To date, there have been no reports of vaccine failures in persons who received fractional doses of the vaccine.
Following the availability of the immunogenicity data from the DRC campaign suggesting that the fractional dosing campaign was successful, SAGE concluded that this approach was logistically, operationally, and scientifically feasible because of the relative ease of administering 0.1mL of a 0.5mL full dose using a tuberculin syringe to protect at-risk populations that would be unprotected otherwise. However, SAGE noted that additional data were needed to understand if (1) fractional doses for all prequalified vaccines could result in non-inferior immunogenicity and have equivalent safety to full doses, (2) fractional doses were safe and immunogenic in younger children and those who might not have optimal response to yellow fever vaccine (eg, people living with human immunodeficiency virus (HIV [PLWH]), and (3) the immune response elicited by a fractional dose was as durable as a full dose.23
New Data on Dose-Sparing Outcomes
Following the final endorsement of fractional dose recommendations by SAGE, several groups conducted, and continue to conduct, research studies on fractional doses aimed at addressing knowledge gaps.
Two groups have published data on long-term immune response to fractional doses and a third is working to finalize their analyses. Roukens et al conducted a 10-year follow-up on the fractional dosing study from the Netherlands which included 49% (75/155) of the initial participants (Table 1). The lower number of participants unfortunately did not provide enough statistical power for non-inferiority analysis, but still yielded useful results (Dutch trial register NTR7094).38 Forty of these participants received fractional i.d. doses of the YF vaccine and 35 received the full s.c. dose. Of these, 39 (98%) and 34 (97%) participants, respectively, still had protective levels of neutralizing antibodies after 10 years.
An 8-year post-vaccination follow up on the fractional dosing study in Brazil was able to recruit 48% (318) of its initial participants, who all originally seroconverted and had not been re-vaccinated against YF (NCT03338231) (Table 1).39 Among all dose groups, ~80-96% of the participants still had protective neutralizing antibodies against YFV after 8 years. Seropositivity in each of the lower dose groups was not statistically significantly different from that of the full dose group. Surprisingly, the lowest dose group (31 IU) had the highest continuing seropositivity rate, at 96%. However, the researchers note that the small sample size in this group (n=23) could have caused statistical distortion and could have been due to unintended selection of people that were high responders to the YF vaccine in the follow up. A separate analysis was done to exclude those with possible re-vaccination, and those who had missions to, lived in, or traveled to endemic areas (and could have been re-vaccinated or infected with wild-type YFV via mosquito bite). Even after removing these groups and analyzing them on their own, the results did not differ from the original protocol analysis.
A related study of a subset of the Brazil cohort was also performed at the 8-year follow-up to examine humoral and cellular immunity in more detail (Table 1).40 Ninety-eight participants from the original trial and 46 non-vaccinated controls were included. Those who seroconverted with fractional doses in the original study had similar neutralizing antibody levels and YF T-cell immunity (especially when measuring memory biomarkers CMCD4 and EMCD8) to those who had the reference full dose, and all dose groups were statistically different from the non-vaccinated control group.
Finally, a meta-analysis was performed that included the published studies noted above (2371 total participants) stratified by vaccine dose.46 Seroconversion at 4–5 weeks post-vaccination was similar among the standard dose group and the 1:3, 1:5, 1:10, and 1:50 fractional dose groups. Rates of seroconversion were significantly lower in people who received the 1:100 or smaller doses. Immunogenicity persisted for at least 8–10 years for all groups and there was no statistically significant difference in adverse events between groups. Currently, results of a 5-year follow-up study conducted in DRC for those who participated in the initial evaluation of the immune response are being analyzed. Data from this study are similar to those noted above in that the vast majority of participants continue to have a detectable neutralizing antibody titer against YFV at 5 years following the large-scale vaccination campaign (author, personal communication).
A double-blinded non-inferiority trial took place in Mbarara, Uganda and Kilifi, Kenya utilizing all four WHO-prequalified vaccines at the standard dose (0.5mL) and the one-fifth fractional dose (0.1mL) administered s.c. (NCT02991495) (Table 1).35 Participants were healthy, non-pregnant or lactating, and aged 18–59 years. Eligibility criteria included no previous YF vaccination or infection and no YF vaccination travel requirements. The mean standard doses in IU for each vaccine were as follows: Bio-Manguinhos-Fiocruz, 38 905 IU; Chumakov Institute of Poliomyelitis and Viral Encephalitides, 43 652 IU; Institut Pasteur Dakar, 6761 IU; and Sanofi Pasteur, 16 596 IU. Nine hundred participants randomized into 8 groups corresponding to the full and fractional dose of each vaccine were included in the per-protocol analysis; 60 participants were excluded because of missing PRNT50 results or detectable neutralizing antibodies at baseline. The study showed that there was little difference in seroconversion rates for the fractional dose for each manufacturer compared with the standard dose. These differences varied from −0.9% to 1.82% (not statistically significantly different) and met the qualifications for non-inferiority (defined as −10%). Mean neutralizing antibody titers were comparable between each fractional dose and their respective standard doses and titers trended higher in those who received fractional doses after one year (range of 2974–5088 vs 2261–4047). All vaccine doses were determined to be safe and seroconversion was stable through day 365. However, interestingly, data on seroconversion and antibody titer at 10 days post-vaccination for both full and fractional doses found that three of the four vaccines had lower seroconversion rates and titer for fractional doses than full doses.
Three additional studies have been published on the safety and immunogenicity of fractional doses of 17DD in young children and populations who might have an altered immune response to vaccination (Table 1). Children aged 9–59 months in Kenya and Uganda were enrolled and vaccinated with one-fifth and full doses of 17D-213 YF vaccine.41,47 The seroconversion rates at 28 days and at 12–16 months among those receiving a fractional dose were non-inferior to those receiving a full dose using a −10% margin. However, non-inferiority was not achieved in all age groups in the analysis (9–12 months, 13–35 months, and 36–59 months) and at 10 days after vaccination. Geometric mean titers (GMTs) were also lower at all time points and for all age groups in children who received fractional doses compared to full doses of the vaccine.
In Brazil during 2018, 159 people with autoimmune rheumatic diseases (ARD) with low immunosuppression (defined by many variables for this specific disease risk) and 159 matched healthy controls were given a one-fifth dose of 17DD.37 Participants with ARD had 84% seroconversion at 30 days post-vaccination while controls had 97% seroconversion. Also, those individuals with ARD had lower neutralizing antibody titers and a lower proportion had viremia (53% vs 70%) in controls at day 5 but longer-lasting viremia (51% vs 19% positive in controls at day 10). The fractional doses were found to be safe, immunogenic, and did not induce autoimmune flares in ARD patients. The authors stated that fractional doses could be considered for these higher risk ARD patients when there are YF outbreaks, but durability of seroconversion must be investigated.
In the last study, PLWH with CD4+ counts >200 cells per mL in Kenya either received one-fifth or a full dose of 17D-213 YF vaccine.42 Similar to the results in young children, participants receiving a fractional dose had non-inferior seroconversion rates at 1 month and 1 year compared to the rates seen in those who received a full dose. The seroconversion rates were lower at 10 days for fractional doses and the GMTs were lower at all time points among those who received fractional doses compared to those who received full doses.
A few other clinical trials to further test YF vaccine fractional dosing are currently in progress or planned. A Phase 4 trial undertaken by the Infectious Disease Institute in Kampala, Uganda; the MRC/UVRI (Uganda Virus Research Institute) and LSHTM (London School of Hygiene and Tropical Medicine) Uganda Research Unit; and the US CDC (Center for Disease Control and Prevention) have completed enrollment for a study of the effects of a one-fifth and one-half fractional dose of 17DD administered s.c. in children aged 9–23 months (NCT03725618). Finally, the Non-Inferiority Fractional-doses Trial for Yellow Fever Vaccine (NIFTY) is still recruiting participants (NCT04059471) and another trial is active but not yet recruiting to test 1/5 and 1/10 doses of the US YF-VAX® 17D-204 vaccine in healthy adults (NCT05374317).
These additional data continue to support and will help to refine, if necessary, SAGE and WHO recommendations for the use of fractional doses of YF vaccine. However, the data generated to date does raise some concern about the lower GMTs and in some cases seroconversion rates in younger children and populations who might have an altered immune response to vaccination (eg, PLWH, individuals with autoimmune diseases receiving treatment). Also, the delayed antibody formation with lower doses of the vaccine is of concern given the current indication of fractional doses for use when doses of vaccine are insufficient in the face of an outbreak. More data are needed on the kinetics of the antibody response to fractional vaccine doses to identify if lower doses of antigen can be administered and result in the same rapid and sustained protection seen with full doses.
Current Recommendations
Currently, fractional dosing is only recommended by the WHO in emergency outbreak situations where it is likely that the vaccine stockpiles will be/are exhausted. Fractional dosing is not approved for travel requirements by national regulators. It is the WHO’s position that people who receive fractional doses are not issued an International Certificate of Vaccination or Prophylaxis (ie, yellow card) until they can receive a standard dose.48,49 The EYE secretariat has included fractional dosing within the list of responses to emergency situations.19
Future Use of Fractional Dosing
Vaccination is the main effective method of preventing YF. Fractional dosing as a dose-sparing technique allows for larger numbers of vaccinees among populations in need, especially in an outbreak emergency where large populations need to be vaccinated quickly. Using one-fifth doses of the YF vaccines would expand vaccine stockpiles and annual manufacturing needs substantially and could help the EYE strategy reach its goals of vaccinating 1.3 billion people against YF during 2017–2026 and providing a vaccination coverage rate of 80% in high-risk areas.19 The WHO hypothesized that 80% coverage would provide enough immunity to stem most outbreaks, though some researchers hypothesize that 90–95% vaccination coverage is needed to stop urban outbreaks.50 With fractional dosing the burden of transportation and cost of the vaccine would be lessened since there would be much less product to transport and manufacture; however, it could lead to vaccine wastage if vials containing multiple doses are not used within the typical six-hour window of reconstitution.
Reports have shown that the off-label use of fractional doses is as effective as standard doses at one month and one year post-vaccination for the four prequalified YF vaccines and up to 8–10 years for 17DD and 17D-204 substrains, as determined by seroconversion rates. However, data from long-term studies are needed to determine if the fractional doses elicit life-long immunity, particularly in certain populations where fractional doses elicit lower antibody titers when compared to full doses, which will be important in low- and middle-income countries in endemic areas. Questions regarding the differences between i.d. and s.c. vaccine administration still need to be investigated as well as longer-term studies on all four WHO prequalified vaccines. Clinical trials of fractional dosing of other vaccines, including inactivated poliovirus, rabies, hepatitis A, influenza, and more, have yielded promising results for achieving immunity with i.d. administration.51,52 However, the different administration procedure for i.d. vaccination requires specific training for those administering the vaccines as well as different types of needles, which may not be feasible in some settings. Microneedle patches could help fill this gap, though these have not yet been utilized to the extent that was hoped and have not been tested with YF vaccines. Recently, fractional dosing has been used for other diseases, such as mpox with the Jynneos vaccine, and has been considered for certain COVID-19 vaccines.53 However, it is currently unclear whether COVID-19 vaccines have excess potency like YF vaccines and if fractional dosing by i.d. administration may change the reactogenicity and safety profiles of COVID-19 vaccines.54 For these reasons and also concern regarding increasing anti-vaccination sentiment and time-consuming vaccine administration training, fractional dosing of COVID-19 vaccines has not been approved.
Current data on the effectiveness of YF vaccine fractional doses are encouraging and it is possible that they could be useful outside of outbreak scenarios, especially as most 17D vaccine standard doses include far higher quantities than is thought to be necessary. However, the antibody kinetics for the first month after vaccination need to be further explored as the International Health Regulations (IHR) use 10 days as the period between initial vaccination and being considered “protective” and able to travel to another location, since there is ~85% protection after 10 days. This protection increases up to 99% at 30 days post-vaccination. If fractional doses of YF vaccine lead to lower rates of seroconversion at 10 days, consideration will need to be given to their use in an active outbreak as well as their broader use within the context of IHR. As time goes on, more long-term data will become available from the studies involving those who received fractional doses in the outbreaks in DRC and Brazil, as well as subsequent clinical trials. For these reasons, it is advisable that the recommendation to give standard doses of the YF 17D vaccine in non-emergency situations rather than the fractional dose should be followed. Based on early clinical trials data, the efficacy of fractional doses of all substrains of 17D are non-inferior to the full doses in at least the first year following vaccination, which allows emergency fractional dosing to be used with all substrains. On the other hand, the full dose 17D vaccine has been in use since the 1930s and has proven to be very safe and effective. There is the possibility that lowering the standard dose of the YF vaccines could complicate the global systems that are already in place, which would further stymie 17D vaccination efforts.
Conclusion
Fractional dosing as a dose-sparing technique remains a credible and viable option for emergency outbreaks. Gaps in knowledge on dose-sparing still include fractional dosing efficacy in certain populations, and those with differing genetic and circumstantial backgrounds, including environmental stressors, malnutrition, and presence of parasitic diseases. Knowledge on cellular immunity (including memory B cells) and timing of waning immunity post-vaccination still needs to be expanded. Measuring of immunity over the past 10 years and monitoring for serious adverse events must continue. Some subgroups of people may not mount a robust response to the vaccine; therefore, the minimum dose of 1000–3000 IU continues to be warranted. Until other proposals for YF vaccines (like more stable formulations, microneedle patches, etc.) and long-term data on YF immunity after fractional dosing come to fruition, fractional dosing is an ideal outbreak response, but not an ideal option for routine immunizations.
Acknowledgments
The findings and conclusions of the paper are those of the authors and do not necessarily represent the official views of the CDC.
Funding
CAH was supported by the John Sealy Distinguished University Chair in Vaccinology at the Universty of Texas Medical Branch.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johansson MA, Vasconcelos PFC, Staples JE. The whole iceberg: estimating the incidence of yellow fever virus infection from the number of severe cases. Trans R Soc Trop Med Hyg. 2014;108(8):482–487. doi:10.1093/trstmh/tru092
2. Beck AS, Barrett AD. Current status and future prospects of yellow fever vaccines. Expert Rev Vaccines. 2015;14(11):1479–1492. doi:10.1586/14760584.2015.1083430
3. Gaythorpe KA, Hamlet A, Jean K, et al. The global burden of yellow fever. eLife. 2021;10:e64670. doi:10.7554/eLife.64670
4. Yellow fever. Available from: https://www.who.int/news-room/fact-sheets/detail/yellow-fever.
5. Haddow AJ. X.—The Natural History of Yellow Fever in Africa. Proc Sect B Biol. 1969;70(3):191–227. doi:10.1017/S0080455X00001338
6. Ellis BR, Barrett ADT. The enigma of yellow fever in East Africa. Rev Med Virol. 2008;18(5):331–346. doi:10.1002/rmv.584
7. List of Prequalified Vaccines. WHO - Prequalification of Medical Products (IVDs, Medicines, Vaccines and Immunization Devices, Vector Control); 2019. https://extranet.who.int/pqweb/vaccines/list-prequalified-vaccines. Available from:
8. Recommendations to assure the quality, safety and efficacy of live attenuated yellow fever vaccines, Annex 5, TRS No 978; 2013. Available from: https://www.who.int/publications/m/item/yellow-fever-vaccines-live-attenuated-annex-5-trs-no-978. Available from:
9. Coulange Bodilis H, Benabdelmoumen G, Gergely A, et al. Persistance à long terme des anticorps neutralisants de la fièvre jaune chez les personnes âgées de 60 ans et plus. Bull Soc Pathol Exot. 2011;104(4):260–265. doi:10.1007/s13149-011-0135-7
10. Staples JE, Barrett ADT, Wilder-Smith A, Hombach J. Review of data and knowledge gaps regarding yellow fever vaccine-induced immunity and duration of protection. Npj Vaccines. 2020;5(1):54. doi:10.1038/s41541-020-0205-6
11. Wieten RW, Jonker EFF, van Leeuwen EMM, et al. A Single 17D Yellow Fever Vaccination Provides Lifelong Immunity; Characterization of Yellow-Fever-Specific Neutralizing Antibody and T-Cell Responses after Vaccination. PLoS One. 2016;11(3):e0149871. doi:10.1371/journal.pone.0149871
12. Barrett ADT. The reemergence of yellow fever. Science. 2018;361(6405):847–848. doi:10.1126/science.aau8225
13. Song R, Guan S, Lee SS, et al. Late or Lack of Vaccination Linked to Importation of Yellow Fever from Angola to China. Emerg Infect Dis. 2018;24(7):1383–1386. doi:10.3201/eid2407.171868
14. Kwagonza L, Masiira B, Kyobe-Bosa H, et al. Outbreak of yellow fever in central and southwestern Uganda, February–may 2016. BMC Infect Dis. 2018;18(1):548. doi:10.1186/s12879-018-3440-y
15. Ingelbeen B, Weregemere NA, Noel H, et al. Urban yellow fever outbreak—Democratic Republic of the Congo, 2016: towards more rapid case detection. PLoS Negl Trop Dis. 2018;12(12):e0007029. doi:10.1371/journal.pntd.0007029
16. Epidemiological Update: yellow Fever. 1 Pan American Health Organization / World Health Organization; 2018. Available from: http://bit.ly/2BympPo.
17. Nomhwange T, Jean Baptiste AE, Ezebilo O, et al. The resurgence of yellow fever outbreaks in Nigeria: a 2-year review 2017–2019. BMC Infect Dis. 2021;21(1):1054. doi:10.1186/s12879-021-06727-y
18. Lindsey NP, Horton J, Barrett ADT, et al. Yellow fever resurgence: an avoidable crisis? Npj Vaccines. 2022;7(1):137. doi:10.1038/s41541-022-00552-3
19. World Health Organization. A Global Strategy to Eliminate Yellow Fever Epidemics (EYE) 2017–2026. World Health Organization; 2018. Available from: https://apps.who.int/iris/handle/10665/272408.
20. Barrett ADT. Yellow Fever Vaccine: the Conundrum of 2 Doses, One Dose, or One-Fifth Dose to Induce and Maintain Protective Immunity. J Infect Dis. 2020;221(12):1922–1924. doi:10.1093/infdis/jiz379
21. World Health Organization. Fractional Dose Yellow Fever Vaccine as a Dose-Sparing Option for Outbreak Response; 2016.
22. 17DD Yellow Fever Vaccine Package Insert. 2018.
23. SAGE. Summary of the October 2016 Meeting of the Strategic Advisory Group of Experts on Immunization (SAGE); 2016.
24. World Health Organization. Global Advisory Committee on Vaccine Safety, 30 November – 1 December 2016. World Health Organization; 2017:Available from: https://apps.who.int/iris/handle/10665/253066.
25. World Health Organization. Mass Yellow Fever Vaccination Campaign Launched in Democratic Republic of Congo. WHO Africa; 2016. Available from: https://www.afro.who.int/news/mass-yellow-fever-vaccination-campaign-launched-democratic-republic-congo.
26. World Health Organization. Yellow Fever in Africa and the Americas, 2018. WHO. 2019;94(33):365–378
27. Teitelbaum P, Bui YG, Libman M, McCarthy A. Fractional dosing of yellow fever vaccine during shortages: perspective from Canada. J Travel Med. 2018;25(1). doi:10.1093/jtm/tay098
28. Yellow Fever Working Group. Interim Canadian recommendations for the use of a fractional dose of yellow fever vaccine during a vaccine shortage. Can Commun Dis Rep. 2016;42(8):158–160. doi:10.14745/ccdr.v42i08a02
29. Theiler M, Smith HH. THE USE OF YELLOW FEVER VIRUS MODIFIED BY IN VITRO CULTIVATION FOR HUMAN IMMUNIZATION. J Exp Med. 1937;65(6):787–800. doi:10.1084/jem.65.6.787
30. Campi-Azevedo AC, de Almeida Estevam P, Coelho-dos-Reis JG, et al. Subdoses of 17DD yellow fever vaccine elicit equivalent virological/immunological kinetics timeline. BMC Infect Dis. 2014;14(1):391. doi:10.1186/1471-2334-14-391
31. Department of Immunization, Vaccines and Biologicals. Fractional Dose Yellow Fever Vaccine as a Dose-Sparing Option for Outbreak Response: WHO Secretariat Information Paper; 2016.
32. de Souza Lopes O, de Almeida Guimarães SSD, de Carvalho R. Studies on yellow fever vaccine III—dose response in volunteers. J Biol Stand. 1988;16(2):77–82. doi:10.1016/0092-1157(88)90034-0
33. Roukens AH, Vossen AC, Bredenbeek PJ, van Dissel JT, Visser LG. Intradermally Administered Yellow Fever Vaccine at Reduced Dose Induces a Protective Immune Response: a Randomized Controlled Non-Inferiority Trial. PLoS One. 2008;3(4):e1993. doi:10.1371/journal.pone.0001993
34. Martins RM, Farias RHG. 17DD yellow fever vaccine: a double blind, randomized clinical trial of immunogenicity and safety on a dose-response study. Hum Vaccin Immunother. 2013;9(4):879–888. doi:10.4161/hv.22982
35. Juan-Giner A, Kimathi D, Grantz KH, et al. Immunogenicity and safety of fractional doses of yellow fever vaccines: a randomised, double-blind, non-inferiority trial. Lancet. 2021;397(10269):119–127. doi:10.1016/S0140-6736(20)32520-4
36. Casey RM, Harris JB, Ahuka-Mundeke S, et al. Immunogenicity of Fractional-Dose Vaccine during a Yellow Fever Outbreak — final Report. N Engl J Med. 2019;381(5):444–454. doi:10.1056/NEJMoa1710430
37. Tonacio AC, Do Nascimento Pedrosa T, Borba EF, et al. Immunogenicity and safety of primary fractional-dose yellow fever vaccine in autoimmune rheumatic diseases. PLoS Negl Trop Dis. 2021;15(11):e0010002. doi:10.1371/journal.pntd.0010002
38. Roukens AHE, van Halem K, de Visser AW, Visser LG. Long-Term Protection After Fractional-Dose Yellow Fever Vaccination: follow-up Study of a Randomized, Controlled, Noninferiority Trial. Ann Intern Med. 2018;169(11):761. doi:10.7326/M18-1529
39. de Menezes Martins R, Maia LS, de Lima SMB, et al. Duration of post-vaccination immunity to yellow fever in volunteers eight years after a dose-response study. Vaccine. 2018;36(28):4112–4117. doi:10.1016/j.vaccine.2018.05.041
40. Costa-Rocha IA, Campi-Azevedo AC, Peruhype-Magalhães V, et al. Duration of Humoral and Cellular Immunity 8 Years After Administration of Reduced Doses of the 17DD-Yellow Fever Vaccine. Front Immunol. 2019;10:1211. doi:10.3389/fimmu.2019.01211
41. Juan-Giner A, Namulwana ML, Kimathi D, et al. Immunogenicity and safety of fractional doses of 17D-213 yellow fever vaccine in children (YEFE): a randomised, double-blind, non-inferiority substudy of a phase 4 trial. Lancet Infect Dis. 2023;23(8):965–973. doi:10.1016/S1473-3099(23)00131-7
42. Kimathi D, Juan-Giner A, Orindi B, et al. Immunogenicity and safety of fractional doses of 17D-213 yellow fever vaccine in HIV-infected people in Kenya (YEFE): a randomised, double-blind, non-inferiority substudy of a phase 4 trial. Lancet Infect Dis. 2023;23(8):974–982. doi:10.1016/S1473-3099(23)00114-7
43. Vasconcelos PFC, Barrett ADT. Are booster doses of yellow fever vaccine needed? Lancet Infect Dis. 2019;19(12):1275–1276. doi:10.1016/S1473-3099(19)30411-6
44. Hombach J, Solomon T, Kurane I, Jacobson J, Wood D. Report on a WHO consultation on immunological endpoints for evaluation of new Japanese encephalitis vaccines. Vaccine. 2005;23(45):5205–5211. doi:10.1016/j.vaccine.2005.07.002
45. Roehrig JT, Hombach J, Barrett ADT. Guidelines for Plaque-Reduction Neutralization Testing of Human Antibodies to Dengue Viruses. Viral Immunol. 2008;21(2):123–132. doi:10.1089/vim.2008.0007
46. Nnaji CA, Shey MS, Adetokunboh OO, Wiysonge CS. Immunogenicity and safety of fractional dose yellow fever vaccination: a systematic review and meta-analysis. Vaccine. 2020;38(6):1291–1301. doi:10.1016/j.vaccine.2019.12.018
47. Roukens AHE, Visser LG. Fractional dose yellow fever vaccination, coming of age. Lancet Infect Dis. 2023;23(8):889–890. doi:10.1016/S1473-3099(23)00205-0
48. Roukens AHE, Visser LG. Fractional-dose yellow fever vaccination: an expert review. J Travel Med. 2019;26(6):taz024. doi:10.1093/jtm/taz024
49. World Health Organization. WHO position on the use of fractional doses – June 2017, addendum to vaccines and vaccination against yellow fever WHO: position paper – June 2013. Vaccine. 2017;35(43):5751–5752. doi:10.1016/j.vaccine.2017.06.087
50. Ndeffo-Mbah ML, Pandey A. Global Risk and Elimination of Yellow Fever Epidemics. J Infect Dis. 2020;221(12):2026–2034. doi:10.1093/infdis/jiz375
51. Migliore A, Gigliucci G, Di Marzo R, Russo D, Mammucari M. Intradermal Vaccination: a Potential Tool in the Battle Against the COVID-19 Pandemic? RMHP. 2021;14:2079–2087. doi:10.2147/RMHP.S309707
52. Clarke E, Saidu Y, Adetifa JU, et al. Safety and immunogenicity of inactivated poliovirus vaccine when given with measles–rubella combined vaccine and yellow fever vaccine and when given via different administration routes: a phase 4, randomised, non-inferiority trial in The Gambia. Lancet Global Health. 2016;4(8):e534–e547. doi:10.1016/S2214-109X(16)30075-4
53. Więcek W, Ahuja A, Chaudhuri E, et al. Testing fractional doses of COVID-19 vaccines. Proc Natl Acad Sci USA. 2022;119(8):e2116932119. doi:10.1073/pnas.2116932119
54. Wilder-Smith A, Desai S, Cravioto A, Nohynek H, Hombach J. Caution before fractionating COVID-19 vaccines. Nat Med. 2021;27(11):1856–1857. doi:10.1038/s41591-021-01534-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.