Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Forming Nursing Home Practices That Support Quality of Care for Residents. A Qualitative Observational Study
Authors Stokke R ![]() , Wibe T
, Wibe T ![]() , Sogstad M
, Sogstad M
Received 21 June 2023
Accepted for publication 21 August 2023
Published 11 September 2023 Volume 2023:16 Pages 2667—2680
DOI https://doi.org/10.2147/JMDH.S426913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Randi Stokke.
Views: 95
Randi Stokke,1 Torunn Wibe,2 Maren Sogstad1
1Faculty of Medicine and Health Sciences, Centre for Care Research, Norwegian University of Science and Technology NTNU, Gjøvik, Norway; 2Centre for Development of Institutional and Home Care Services in Oslo, Oslo, Norway
Correspondence: Randi Stokke, Tel +4795158088, Email [email protected]
Background: Residents of nursing homes are increasingly frail and dependent. At the same time, there are increased demands for quality of care and social life for individual residents. In this article, we explore how care workers contribute to quality of care and social life in shared living rooms in nursing homes.
Methods: An ethnographically inspired design was applied, and a purposive sample of six units for long-term care in three nursing homes in Norway was included in the study. Data were collected by participant observation, including informal conversations with the staff and residents, and the data were analyzed using thematic analysis.
Results: The analysis identified three main themes: working within the given context, creating care practices and organizing activities. The empirical findings demonstrate that care work focuses on meeting both the residents’ physical and social needs and aiming for high-quality care and social life for the residents in nursing homes.
Conclusion: The results of this study illustrate that nursing home practices are focused on residents as a group. However, care workers take advantage of personal skills and resources to work towards person-centred care within the given context. The quality of care is recognized in terms of how care workers meet individual residents’ needs. The quality of care seems highly related to the capability and skills of individual care workers.
Keywords: nursing home, quality of care, person-centred care, social needs, activity, qualitative study, participant observation
Introduction
Internationally, there has been an increased focus on ageing in place, and frail older people are living in their own homes more often than before.1 However, because more people are reaching old age, there is still a consistent number of older people in need of nursing home care, which involves 24/7 care and supervision. The population living in nursing homes is thereby increasingly characterised by old age, frailty and multimorbidity, and more than 80% of the residents have some diagnostic signs of dementia.2,3 Care workers in nursing homes have a heavy workload and must often prioritize important tasks such as assisting with physical needs.4 Providing high-quality care in nursing homes is therefore demanding.
Until the end of the last century, the hospital was seen as the ideal nursing home model, aimed at offering residents, who were then called patients, treatment and care.5 Despite the increasing degree of frailty, multimorbidity and increased need for advanced nursing care of today’s nursing home residents, a cultural change moving away from the institutional hospital-like model of care is impacting the provision of aged-care services around the world.6,7 Currently, policymakers and healthcare workers have characterised nursing homes as “real” homes by reducing or eliminating obvious “hospital-like” structures, such as nurses’ stations and offices. Many nursing homes have been designed to be more reflective of a homely environment through the construction of smaller residential units and open-plan kitchen/dining/living areas. The residents usually are offered single rooms with baths, and they can have some of their personal belongings in their room making it more home-like.5,7–10 Nursing homes today are both care institutions and places where residents can live their lives.11 Such home-like settings have been linked to a feeling of home for residents.12,13
The development and delivery of high-quality care for residents in nursing homes are at the heart of policies both internationally and in Norway, where this study is conducted. However, the goals of delivering quality care for residents in nursing homes are challenging to achieve in practice due to limited resources, lack of qualified staff, demography and patient preferences in a complex healthcare service.14
Many studies of quality in nursing homes have focused on the medical and technical aspects of quality. Less attention has been given to the interpersonal aspects of care practices in a nursing home and how they affect the quality of care and the patient’s/resident`s quality of life.15 Residents’ well-being also depends on how they experience the social life in a nursing home and the quality of the care that they receive.16
Person-centred care is an approach to care practices that includes the interpersonal aspects of care by including the formation and fostering of therapeutic relationships among care providers, patients, and significant others.8 Person-centred care is stated to be an important value internationally within laws and regulations.15
In this study, we used the theory of person-centred care as presented by Kitwood17 as a frame for understanding practices facilitating quality of care. Central to person-centred care is addressing the nursing home resident as a person with needs and preferences beyond just the physical or medical perspective. Based on what Kitwood17 describes as “the old culture” in nursing homes, care is concerned primarily with such matters as providing a safe environment, meeting basic needs (food, clothing, toileting, warmth, cleanliness, adequate sleep, etc.) and skillfully giving physical care. According to Kitwood,17 “the new culture” of person-centred care is concerned primarily with the maintenance and enhancement of personhood. Providing a safe environment, meeting basic needs, and providing physical care are essential but only part of the care of the whole person.17 Person-centred care emphasizes well-being and quality of life as defined by the individual. The locus of decision-making is with the resident, ensuring that his or her wishes and desires are respected and valued. To achieve person-centred care, person-centred moments, such as those between a care worker and a resident, should be promoted to become a regular cultural pattern or norm.6
Relationships with others, social engagement, activities, experienced choice and perceived autonomy and the quality of the relationship between the resident and the care worker are important factors to provide quality of everyday life in nursing homes.18 Even so, little attention has been given to these aspects of interpersonal care and how care workers in a nursing home contribute to social life in the common areas of the nursing home. To improve these aspects of care, we need more insights into how care workers form nursing home practices that support quality care for residents.
Materials and Methods
This study aimed to explore which care practices, by focusing on the interpersonal aspects of care, can contribute to the quality of care and social life in the common living rooms of nursing homes. This was achieved by focusing on the care work practices provided in the common areas of nursing homes. Undoubtedly, much of the care and interactions between healthcare workers and residents occur in residents’ private rooms. However, in nursing homes, at least in Norway, residents spend much of their time in shared living rooms.5,10
We conducted an ethnographically inspired study involving participant observation in six units of three nursing homes in a large city in Norway. The nature of care work is often distributed and unpredictable, and a large part of care activities can be described as “invisible work”.19 This makes it challenging to articulate these practices,19 and we, therefore, chose participant observation as the data collection method. This allowed us to focus on the care practices the care workers enacted to provide quality care and social life for the residents in the nursing homes.
Nursing Home Selection
Since the study focused on exploring good practices, we wanted to collect data from various popular and reputable nursing homes. Since Norway does not rank nursing homes, we contacted the Centre for Development of Institutional and Home Care Services in a large city in Norway and they helped select three popular nursing homes. Within this group, we aimed for variation and diversity and therefore requested nursing homes with different business models that were in different sociodemographic areas of the city, as illustrated in Table 1. They selected three nursing homes valued as reputable according to the number of applications for residents’ placements as this might provide a proxy measure for popularity. Furthermore, the leaders of the three nursing homes chose which units would participate in the study, aiming for diversity.
 |
Table 1 Characteristics of the Included Nursing Homes |
In Norway, municipalities are at the lowest administrative and political organizational levels and are responsible for providing care services and assisting people in need. The content of municipal care services varies across different countries;20 Norway has a substantial public healthcare sector, recognized by universal access. This is often described as the Scandinavian model.
Study Context
All six included nursing home units were long-term units. The residents of the nursing homes varied in terms of functional level, but overall, the people living in the nursing homes were frail and dependent and suffered from different forms of reduced levels of physical, mental, and social functioning. Dementia was described by the care workers to be common. All the data collection took place within the common areas. Residents of long-term nursing home units usually live in these units from the time of their admission until they die. In Norway, the average time living in a long-term nursing home is two years.21
In Norway, the workforce doing the daily care work in nursing homes consists of registered nurses, nursing assistants and untrained staff. Even though registered nurses provide some specialized nursing tasks like handling medications, all different kinds of care workers to a large extent perform the tasks in the daily life of nursing homes, like preparing mealtimes. In this study, they are therefore described as care workers.
Even though the included nursing homes differed by size, organisation, business model and location in the city, they had many similarities. As caring for dependent citizens is a public responsibility, private nursing homes have an operating agreement and follow the same rules and regulations as public care services.15 The municipality allocates rooms in all nursing homes based on an application and an evaluation of the individual’s need for care. In all the units, the residents had private rooms with ensuite bathrooms. In addition, the organisation of practices in the common areas appeared similar in all the included units. The residents’ time spent in the shared living space varied from none to almost all waking hours, depending on the residents’ interests, wishes and physical and cognitive conditions.
All units had a combined kitchen and eating area as described in Table 1. Four of the six units had an open or semi-open arrangement between the kitchen/eating area and the living rooms. The other two units had separate living and TV rooms and a kitchen/eating area. In these units, the residents moved more between the different areas at mealtimes.
All living rooms had nice art on the walls, and five of the six units had a piano. All living rooms had large windows, some with nice views, and they all had an outdoor garden or large balcony where the residents could spend time when the weather allowed it.
Data Collection
The participant observations were carried out over 6 weeks in the winter of 2019. The first author spent approximately 6 hours each day (in total approximately 180 hours) focusing the observations on the care work and interactions between the care workers and the residents in the living rooms of the six nursing home units throughout the day and evening. The first author is a registered nurse and researcher with previous experience in observational ethnographic research. The researcher often sat on the outer edge of the room to not be in the way of the care work, which allowed for direct passive observations and opportunities for extensive writing of field notes.22 The first author found that the residents and the staff became accustomed to her presence. Sometimes the observations included informal conversations with the care workers and residents, aiming to discuss and validate the data with the unit leaders, care workers, or residents. These informal conversations took place ad hoc approximately once a day and were included as part of the data material. The first author took notes during these conversations. Extensive field notes were taken during observations and transcribed after every observation session. In total, the field notes included 338 pages, totaling 130,228 words including the informal conversations, providing thick descriptions of the care workers’ practices to create quality care and social life for the residents.
Analysis
The field notes were analyzed using reflexive thematic analysis according to Clarke, Braun and Hayfield.23,24 The analysis started with reading and rereading the data and noting initial ideas. Second, detailed coding resulted in a total of 60 empirically close codes. All the codes were further explored and collated into 9 candidate themes, and after repeated discussions and going back and forth between theory and data among the authors, three themes were developed. The process of analysis with examples is presented in Table 2.
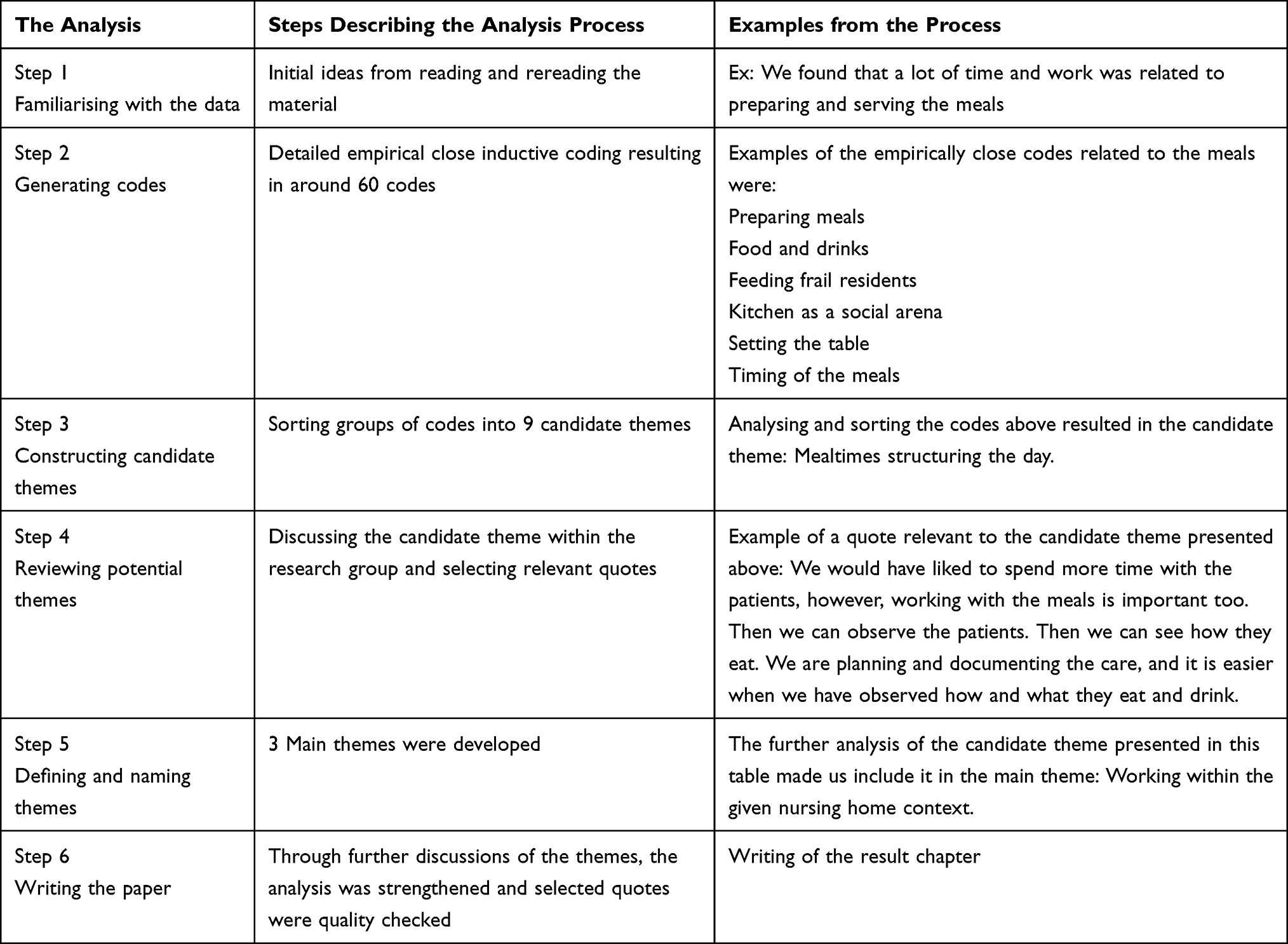 |
Table 2 The Thematic Analysis with Examples from the Different Steps of the Process |
The three themes that were developed are presented in Table 3 in the result chapter. The themes were related to the care workers’ practices to support the quality of care in the shared living spaces of the nursing home units, focusing on the interpersonal aspects of care. NVivo software for qualitative analysis was used to organize the analysis.
 |
Table 3 The Main Themes and the Candidate Themes from the Analysis |
Ethical Considerations and Trustworthiness
According to Norwegian legislation on research in medicine and health (Health Research Act),25 ethical approval was not needed as this study does not include any health data. The ethics of the study was guided by the World Medical Association’s Declaration of Helsinki. For this study, approvals on the protection of privacy were obtained from the delegated IRB, the Norwegian Centre for Research Data (NSD), project number 59,957, and the municipality involved. All the methods and procedures (observations) were carried out following their guidelines and regulations. The first author had meetings with the head nurses of the included units and presented the study, and the head nurses in turn informed the staff. In addition, written information was placed strategically in all units before and during the data collection. The care workers, residents and their next of kin (the latter was especially relevant for residents not competent to give informed consent) received written and oral information about the project before, at the initialization and during the data collection following the approvals from the Norwegian Centre for Research Data. This included information regarding the aim of the study, data confidentiality, publication of anonymized responses, that their participation was voluntary, and that they had the right to withdraw at any time without stating a reason. Verbal informed consent was obtained from all participants before and at the initialization of each observation period for permission to observe the care work in common areas of the nursing homes. Verbal consent was chosen as this study took place in the common areas of nursing homes, which are public areas, and the persons present are many and vary during the day and from day to day. Consent was not obtained from persons dropping by the rooms as data involving interactions with these persons were not collected. This was approved by the Norwegian Centre for Research Data and the municipality. The individual participant could refuse to be observed, however, no one chose to withdraw during or after data collection.
It is always complicated to evaluate the researcher’s influence on the production and interpretation of data and to be aware that his or her life is completely different from that of the residents.26 Informal discussions with the care workers were used to validate the impressions and experiences from the observations. Furthermore, the transcripts were repeatedly discussed within the research group aiming for increased credibility.27
The focus of the observations was on the interactions between the care workers and the residents searching for quality of care and social life for the residents, not on the individual resident, and no personal data was collected. All names presented in the transcripts are pseudonyms.
Results
The following section presents the results from the analysis focusing on which practices provided quality of care and social life for the residents in the shared living spaces of the nursing home. From the data, we identified three interlinked themes: working within the given nursing home context, creating care practices, and organizing activities, as presented in Table 3.
Working Within the Given Nursing Home Context
When observing care workers, the importance of the nursing home context as a premise for care practices was evident. We identified four different contextual factors influencing the practices in the shared living space of nursing homes: Architecture facilitating care, mealtimes structuring the day, residents’ health situations and available care resources. Overall, there were substantial similarities in how daily life in the shared living spaces was carried out across the six units, and we did not observe any major differences in practices that could be related to the nursing homes’ size, organisation, business model or location in the city.
Architecture Facilitating Care
The physical design of the shared living areas, such as the architecture, furnishing and decorations, represented opportunities and limitations in providing quality care for the residents.
For example, the care workers spent a large amount of time in the kitchen related to meals, but they could to some extent observe and communicate with the residents while working there. In this way, the care workers were available and present for the residents while doing other tasks. This was important, as the care workers had busy days and were constantly working and moving around. The residents always had a personal choice of where to spend their time; however, the care workers often encouraged them to spend time in the common areas, in part to increase the residents’ social lives and in part for organizational reasons, as it was easier to take care of all the residents when they were in the same room. In all nursing home units, the residents paid much attention to the care workers’ activities in the kitchen. In one of the units, the architectural layout even situated the kitchen as something of a theatre scene, where the residents could sit like an audience paying attention to the care workers “acting” out the kitchen work.
Aesthetics were highly valued by the care workers as important for the resident’s well-being, and they took pride in keeping the living rooms tidy and nicely decorated with tablecloths, flowers, and décor, as well as setting the table nicely for meals by using napkins and candles. The quotation of a care worker below provides a typical example.
At the weekends and birthdays, we lay the table with nice tablecloths and napkins. We have a patient here that attended fine restaurants. She seldom wants to join the others at the table, but when it is nicely done, she sits by the table and enjoys the meal. It makes a difference you know, having nice surroundings. But look at the flower over there (points at a rather sad potted plant). It is dreadful, it should have been thrown away. However, a resident owns it, and she loves it.
The quotation also illustrates one of many examples of how care workers were attentive to the residents’ wishes even when they conflicted with other values, such as aesthetics. The care work included a constant negotiation between different values, such as keeping the interior nice and tidy and meeting the personal wishes of the residents.
Mealtimes Structuring the Day
Mealtimes structured the day in the nursing homes, starting with breakfast (typically 9 am), followed by lunch (approximately 1 pm), dinner (approximately 4 pm) and an evening meal (approximately 7 pm). In addition, coffee with snacks or fruit was served in between. Normally, the residents had all their meals in the social eating area, and a large part of life in the common areas revolved around the meals. At first glance, it seemed that the time-consuming work related to preparing and serving meals was taking time away from other forms of care. However, throughout the observations, it appeared that the care workers used the mealtimes for several purposes in addition to fulfilling the residents’ nutritional needs, such as making conversation, making jokes, and performing observations.
The care workers acknowledged that they spent a large amount of time preparing and serving meals and that this could be stressful. At the same time, several care workers argued that work related to food and drink was an essential part of care work and a gateway to observing the residents’ condition and needs and looking for symptoms of deterioration or different problems that the care workers needed to act on.
We would have liked to spend more time with the patients, however, working with the meals is important too. Then we can observe the patients. Then we can see how they eat. We are planning and documenting the care, and it is easier when we have observed how and what they eat and drink.
Even though work related to mealtimes constituted a large part of the day in the nursing homes, the residents were never involved in setting the table, and only once was a resident observed helping to clean up after a meal.
The dinner menu was fixed, but the residents were asked how much food they wanted, what they wanted to drink, etc. The residents often praised the food and ate with a good appetite. A few times, the food was not quite to their taste, but then a typical comment would be “I have always eaten what I have been served”. If the care workers noticed that a resident was eating less than normal or if the residents signaled that they would prefer something else, they were offered alternatives. Such individual adjustments sometimes made a substantial difference for the residents:
Don’t you want soup? – the care worker asks. The resident shakes her head. She mimes that she eats something. Do you want a sandwich? - The care worker asks. The resident nods. With cheese, the care worker asks. Again, the resident nods. Always with cheese, the care worker says. I will find you a variety of sandwiches to choose from. She goes to the refrigerator and fetches a platter that she shows the resident. She asks the resident kindly what she wants. The resident points to some sandwiches and the care workers serve them to her.
Occasionally, the care workers sat by the table during the meal, especially when some of the residents needed assistance with eating. They usually sat down facing the person they were helping. Assisting someone in eating a meal could take as much as an hour. This time was spent talking to the resident whom they were helping as well as to the others around the table while observing, offering, and serving drinks in between, etc.
The care worker is sitting beside one resident and helps her to eat. Another resident starts coughing. The care worker stands up and goes over to him immediately. She strokes his forehead and says, “Are you okay? You must eat carefully so you don’t have to cough.” Then, she sits down and continues helping the other resident again. She says, “So you like fish – that is good! Here comes another piece.” Then, the care worker raises her glass and proposes a toast to everyone around the table.
This quotation illustrates how the care workers typically combined tasks, eg, caring for one person while carrying out a social conversation with the group and additionally motivating them to drink by toasting to them all. There was generally a lot of toasting, often in a humorous way.
Talking about food was an important area of conversation, both among the residents and between the residents and the care workers. What to eat and drink and when to do so were probably the most common topics of conversation.
Residents’ Health Situations
Another important determinant of social life in the nursing home units was residents’ health and functional capacity.
Most residents were frail and suffered from multimorbidity, and saving energy for the most important activities was crucial. The care workers took this into account when organizing the day. There were always opportunities for resting before and after planned activities, and the activities usually lasted no longer than 1 hour. The care workers focused on finding a balance between activities and rest as illustrated in the quote below:
Some of the residents are so frail that morning care is a huge strain. They get so exhausted that they don’t have the energy to eat breakfast and just fall asleep afterwards. Food is most important, so then we serve breakfast in bed before the morning routine.
Available Care Resources
The care practices in the nursing home are created within, what is experienced by the care workers as, limited resources. Thus, there was a major focus on the basic physical needs of the residents, and the care workers spent most of their time meeting the residents’ physical needs, such as providing the appropriate nutrition and helping the residents move around and go to the toilet, leaving most of the social interaction between the care workers and residents to occur during or in between these practical tasks. This left rather little time left over for more joyful and engaging social activities with each resident.
Creating Care Practices
We identified three major strategies used by the care workers in creating care practices to support the quality of care for the residents: Being alert, utilizing personal resources and engaging in relational work.
Being Alert
The care workers rarely sat down for more than a couple of minutes to talk with residents, as they were always on the go to complete new tasks. Many of the care workers managed to be calm and create an impression of not being busy, showing attentiveness when sitting with the residents. However, they were constantly watching out, observing the rest of the room to ensure that everybody was alright, putting the walker to the side so that nobody fell, adjusting the position of a resident slipping down in his chair, finding a jumper for a resident who felt cold, etc.; they were always alert. They reacted quickly but calmly to prevent agitation and turbulence between residents when there was a sign of any escalating behavior, as illustrated below.
The care worker helps a resident move from her wheelchair into an armchair while communicating calmly. Afterwards, she makes sure that the wheelchair is placed safely and not in the way of someone. While doing this she observes that another resident looks cold and offers her a scarf. She also puts a pillow behind her back to comfort her seating. Then she leans over to another resident and asks if she wants to watch the TV. Suddenly a resident shout out angrily. The care worker gently takes his hand and calms him down. She sits next to him and talks calmly while also smiling at the other residents.
Utilizing Personal Resources
There were opportunities for the care workers to use their personal skills and interests at work. For example, one care worker who enjoyed singing often sang old songs with the residents when she had time. Another care worker who enjoyed physical activities played with a ball and went for walks with some of the residents. Another care worker often baked a cake for the residents when at work. The work culture in all units seemed to encourage individual initiative from the care workers to utilize their resources.
All units were staffed with both registered nurses and other care workers with different competencies, ages, and cultural backgrounds. In total, in the six units, only two residents were from another country. They both suffered from dementia and no longer spoke or understood Norwegian. Care personnel who spoke their language knew them and could reach out to them, which became important.
In one unit, a care worker was speaking one of the resident’s languages. She used to join him and talk to him in his native language. His face lit up in a smile. Often, he walked around mumbling words to himself with his eyes closed, looking stressed. The care worker took her mobile phone, uploaded old folk songs from his country and slipped the mobile phone into his pocket while gently talking to him and telling him about it. When the music started, he stopped mumbling. He started to hum and clap, tears came into his eyes, and he was smiling. He seemed calmer in his body, and his hands carefully moved along with the beat of the music.
Engaging in Relational Work
It was observable that the personal knowledge the care workers had of each resident to a large extent guided their care, even when they were addressing a resident as part of a group. One example is how the residents were seated during the meals. The care workers described how the seating plan was carefully designed to create a nice atmosphere. Residents who enjoyed each other’s company were placed close to each other, and residents who were jumpy were placed away from those who needed peace.
Most of the social interaction observed in the common areas was initiated by the care workers. Small talk and conversations in the living/dining rooms were almost always initiated by the care workers. They often assisted their words by physically touching the residents to capture their attention while talking.
The care worker always has her face at the eye level of the resident. She often puts her hand gently on their shoulder before she talks. This gives the residents time to be aware of her and seems to improve the communication between them.
If a care worker initiated a conversation and the residents joined in, the conversations seemed to dwindle if the care worker left the conversation. There were many examples of how the care workers adjusted communication and care to the resident’s individuality and related differently to individual residents depending on their personalities and backgrounds to initiate conversations. Some of the care workers also shared aspects of their personal lives with the residents by telling them news about their children or their pets. These personal small conversations often generated engagement from the residents and formed a basis for talking about memories from their own lives, creating an atmosphere of presence, happiness, and laughter.
Organizing Activities
Due to cognitive or physical impairment, most residents had limited possibilities to initiate and perform activities by themselves. The number of practical tasks to solve during the day, related to meals and physical care of the residents, left the limited number of staff with few opportunities for initiating individual activities with the residents. Consequently, group activities had a prominent place.
Likewise, there were several situations in which the residents’ physical and cognitive functional levels guided which activities the care workers chose to do. The residents decided for themselves which activities to attend. However, care workers often actively motivated or nudged residents to attend a concert or other activities based on their knowledge of the resident’s preferences.
Planned Activities
All the units had a weekly activity plan describing the activities offered in the nursing home each week. There were both institutional and unit activities presented. Examples of group activities included visits from kindergarten children, a singsong and group training with the physiotherapist. Some activities took place in the common areas and were open to all residents in the nursing home, not only those in the unit. Examples of these activities were church services, bowling, concerts, etc., as illustrated in Table 4, the fictive weekly plan.
 |
Table 4 An Example of a Weekly Activity Plan |
The goal of the activity plan was to have something for everybody’s taste. Many of the activities were very popular, and most of the residents participated. One example was visiting from the music therapist.
Observations: The music therapist sings old familiar songs. Some songs make the residents applaud and make approval comments. Some residents sing along to some of the songs. The music therapist has a beautiful voice, and one lady sits with her eyes closed during the singing. She opens them when the song is finished. Another resident sits up straight in her wheelchair and mimes the lyrics while looking at the singer.
While singing, one of the residents rolls her wheelchair out of the room. While passing me, the resident says, I can’t take this anymore. I think this is dreadful.
This provides an example of how not all group activities had the same appeal to all the residents All residents were invited to the group activities, but participating was voluntary, leaving the residents to decide to participate or not, or withdraw whenever wanted.
Some of the activities appeared to have a considerable impact on the residents and the atmosphere in the unit. Visits from kindergarten children and therapy dogs especially created lively engagement among the residents.
One resident had been sitting without talking or moving the whole day. When the therapy dog came into the room, she smiled and reached for the dog. The dog owner placed the dog close to her chair and the care worker helped the resident so that she could pet the dog. A smile animated her face.
The care workers extended the value of the activities by talking about them before and after they took place. This created room for discussion and reflection and gave the residents joy in remembering their experiences.
Spontaneous Activities
There were some examples of individual activities, such as a resident going for a walk with a student and a resident having her nails polished when a care worker had a spare moment. However, it was striking during the observation how few individual activities took place. It also seemed that individual activities were more often spontaneous, meaning that they were not planned but took place if by chance there was time for it. The main exception to this was when relatives or visitors involved individual residents in activities.
In addition to the regular care workers, the nursing home often had students present. Several of the care workers mentioned the students as a resource contributing to social activities that they had problems finding time for. The students generally spent more time socializing with the residents than the care workers, which was important in initiating spontaneous activities for individual residents.
Discussion
This study highlights how care workers form practices to provide quality of care and social life for residents living in nursing homes. In the discussion, we use Kitwood’s theory of person-centred care as a frame for understanding practices facilitating quality of care. Central to person-centred care is addressing the nursing home resident as a person with needs and preferences beyond just the physical or medical perspective.17 The results from this study illustrate how care workers while meeting physical and medical needs are simultaneously addressing the residents as persons and using the meals as arenas for creating a social life.
Creating Meaning and Community While Fulfilling Basic Physical Needs
The care workers’ practices observed in the included nursing homes occurred within a context formed by architecture, organisation, and frailty. Donabedian28 describes the importance of the setting in which care is provided, ie, the setting or context may both enable and restrict the practice of providing person-centred care. The care workers in our study demonstrated a desire to perform person-centred care by aiming to provide meaningful activities and a social life for the residents within the given context.
As presented in the results, food and mealtimes were the centers of daily activities and also an important arena for social life. Interestingly, Sandvoll et al29 described a similar finding in their qualitative study in two Norwegian nursing homes, illustrated by the quote “The meals rule the day”. The care workers also showed knowledge and understanding of each resident’s food preferences, adjusting the meals to the residents’ tastes and abilities etc. The contribution of care workers’ knowledge of each resident and his or her preferences for person-centred care is generally recognized.6,17,29–31 However, a dilemma was observed in our study: In one way, the mealtimes represented an activity and an opportunity for conversations in the living area. At the same time, preparing the meals was very time-consuming and occupied many resources, reducing opportunities for other more individually targeted activities and conversations that could support the “personhood” of the residents in a better way. It is also worth noting that the residents never participated in activities such as setting the table or preparing food, which for some residents could have been experienced as meaningful activities. This aligns with a study by Grøndahl and Aagaard32 that found that the residents in Norwegian nursing homes seldom participated in activities related to meals. The lack of participation might have been due to the residents’ frailty and hygiene regulations hindering these kinds of activities. However, this made the organisation of the meals more like that in a restaurant than that in a home, which perhaps was consistent with most residents’ expectations but not necessarily all residents’ expectations.
Harnett and Jönson33 describe that meals in nursing homes may be shared in different frames: 1. Institution frame, which had a meta-message: “This is an institution governed by medical routines, and staff should be in control”. 2. Private frame, with the meta-message: “This is a private situation”. 3. Restaurant frame, which had the meta-message: “This is a restaurant and customers should be in control”.
In our study, we saw traces of all these categories, but the restaurant frame was surprisingly predominant. Nursing homes today are both care institutions and a place to live.11 The restaurant frame is then perhaps to be understood as a compromise between the private frame (for which most of the residents were too much in need of assistance) and the institutional frame (which is not desirable in the culture of person-centred care).
The working culture in the included units allowed the care workers to utilize their personal qualities and resources, making it possible for them to form practices supporting person-centred care for the residents. For instance, some baked cakes or successfully created a pleasant atmosphere through small talk or singing. This finding is comparable with what Edvardsson34 referred to as everydayness and the creation of a homelike environment as elements of quality of care. Similarly, in their study, Vassbø et al31 described how nursing home personnel “play on each other’s talents” by learning from each other and showing mutual respect for each other’s personal and professional skills. An illustrative example in our study was the care worker who played music from a resident’s culture of origin to comfort him. This was possible because she knew the resident’s language and music tastes and because colleagues seemed to value the use of personal skills in meeting residents’ needs.
The Balancing Act Between Standardization and Person-Centeredness
Quality of care in nursing homes may be measured in several different ways. In Norway, it is partly measured through service standards and standardized quality indicators. The indicators cover areas such as dental health; nutrition; the prevalence of falls, infections and pressure ulcers; and resident and next-of-kin satisfaction with the service.35 Earlier research has questioned the importance of national regulations such as those mentioned above for ensuring the quality of care as experienced by the individual nursing home resident. Care workers’ knowledge of the resident as a person and a habitus of caring in the local staff may be more important for the quality of care on an individual level than national regulations.29 The results of our study provide examples of how care workers utilized their knowledge of the residents to provide quality care and ensure that the individual resident’s wishes and desires were respected and valued. This knowledge enabled them to meet the residents’ physical and social individual needs, in line with the aims of person-centred care.17,29–31
Enabling nursing home residents to maintain activities that are important to them can be described as the difference between the quality of care and quality of life.36 In an interview study with residents in Australian residential facilities, Hughes and Moore36 notably found that although participants were reasonably satisfied with the quality of care they received, they expressed that they were not able to live to their full potential.36 Harnett and Jönson37 noted how a nursing home may enable or disable the individual resident in maintaining certain activities that he or she enjoyed earlier in life. In our study, the available resources mainly allowed for group activities. Offering a choice of activities from a “menu” of different group activities is also a way of providing person-centred care, although perhaps not in the most advanced fashion. This can be seen as a way of balancing standardization and person-centeredness due to limited available resources. The care workers also demonstrated insight and knowledge on balancing activities and rest according to the individual residents’ conditions and abilities, thereby contributing to making life in the nursing home as good as possible. If the nursing home staff in this study could have provided more activities based on the individual residents’ interests and conditions, they probably would have been even more able to meet the individual residents’ needs. However, it is also questionable to what extent the residents’ physical and cognitive conditions would have allowed them to enjoy the same activities that they enjoyed earlier in life. Notably, the students who had practice studies in the nursing home managed to offer more individual activities and social dialogues than the regular staff. This is also described in a study by Stabell et al38 who also found that students engaged more in social dialogues than the regular staff. According to our understanding, this illustrates that the students contributed the extra human resources that were necessary to offer more individual activities and that engaging in such activities was regarded as a relevant part of their practices. Skaalvik et al39 found in their study that these activities also were important for the students as part of their training for competence in caring and dialogue with frail people. The students were also in a position to have more liberty to skip the daily practical tasks that the regular staff spent time doing. Therefore, a natural question is whether the staffing of nursing homes is too marginal for the full implementation of person-centred care and not only a light version of this care model in which there is little room for individual activities.
Limitations
Some limitations should be acknowledged in this study. First, we involved only three nursing homes, and from the same city. Because the research was conducted in Norway, the results are affected by culture, laws, and regulations in Norway. However, we did include nursing homes with different business models that were in different sociodemographic areas of the city to provide variety. Second, the observations had a wide focus on all kinds of social activities. This might be both a strength and a limitation, as it opened for observing all kinds of activities, but it might also provide less focused observations. Finally, the observations conducted in this study only took place in the common areas of the nursing home. Work provided to meet the residents’ social needs in their private rooms is therefore not described.
Conclusions
This study aimed to explore how care practices, by focusing on the interpersonal aspects of care, can contribute to the quality of care and social life in the common living rooms of nursing homes.
Person-centeredness was observed both in the care workers’ practices to meet residents’ basic physical needs and in their different practices to attempt to provide quality care and social life. However, due to restricted resources, the care workers seemed to give priority to meeting basic physical needs. In the observed care practices, an accurate understanding of a person’s abilities, tastes, interests, values, and forms of spirituality acted as “the icing on top” to increase quality.
Recommendation for Practice
In this study serving food and helping residents to eat in the common dining area showed to be a valuable possibility to socialize with residents and to meet both their individual physical and social needs although the meal takes place in a group setting. Person-centred care does not necessarily demand one-to-one settings or one-to-one activities. However, the preparation of meals and cleaning of the kitchen is quite time-consuming and has a less obvious value in person-centred care. In the current situation with an increasing shortage of care workers in Norway, the organisation of work tasks related to meals should be taken into consideration. If the care works could spend less time related to the meals this would provide more time to care for the residents social needs.
Data Sharing Statement
The NVivo dataset used and analysed for this study is not made publicly available to protect participants’ privacy but anonymized material is available from the corresponding author upon reasonable request.
Ethics
For this study, approvals on the protection of privacy were obtained from the delegated IRB, the Norwegian Centre for Research Data (NSD), project number 59957, and the municipality involved.
Consent for Publication
The care workers, residents and their next of kin received written and oral information about the project before and during the data collection following the approvals from the Norwegian Centre for Research Data. This included information regarding the aim of the study, data confidentiality, that their participation was voluntary, that they had the right to withdraw at any time without stating a reason, and that the participants informed consent included publication of anonymized responses. Verbal informed consent was obtained from all participants before and during the study for permission to observe their everyday life in common areas of the nursing homes. Verbal consent was chosen as this study took place in the common areas of nursing homes, which are public areas, and the persons present are many and vary during the day and from day to day. Written consent was not obtained because of the fluctuation of people in and out of public areas. This was approved by the Norwegian Centre for Research Data and the municipality. The individual participant could refuse to be observed, however, no one chose to withdraw during or after data collection.
Acknowledgments
The authors would like to thank all the participants of this study.
Funding
This work was supported by the Research Council of Norway grant number 256570. The council did not take part in the design or any other preparation of this manuscript.
Disclosure
The authors declare that they have no financial or non-financial competing interests for this work.
References
1. Pani-Harreman KE, Bours GJ, Zander I, Kempen GI, van Duren JM. Definitions, key themes and aspects of ‘ageing in place’: a scoping review. Ageing Soc. 2021;41(9):2026–2059. doi:10.1017/S0144686X20000094
2. Engedal K, Haugen PK; . DEMENTIA - diseases, diagnostics and treatment (in Norwegian). Forl. aldring og helse akademisk; 2018.
3. Helvik AS, Engedal K, Benth JŠ, Selbæk G. Prevalence and severity of dementia in nursing home residents. Dement Geriatr Cogn Disord. 2015;40(3–4):166–177. doi:10.1159/000433525
4. Gautun H. A development that must be reversed. Staffing and competence in nursing homes and home care (in Norwegian); 2020.
5. Hauge S, Heggen K. The nursing home as a home: a field study of residents’ daily life in the common living rooms. J Clin Nurs. 2008;17(4):460–467. doi:10.1111/j.1365-2702.2007.02031.x
6. Brownie S, Nancarrow S. Effects of person-centered care on residents and staff in aged-care facilities: a systematic review. Clin Interv Aging. 2013;8:1. doi:10.2147/CIA.S38589
7. Rijnaard M, van Hoof J, Janssen B, et al. The factors influencing the sense of home in nursing homes: a systematic review from the perspective of residents. J Aging Res. 2016;2016:1–16. doi:10.1155/2016/6143645
8. McCormack B, Dewing J, Mccance T. Developing person-centred care: addressing contextual challenges through practice development. Online J Issues Nurs. 2011;16(2). doi:10.3912/OJIN.Vol16No02Man03
9. Næss A, Havig AK, Vabø M. Contested spaces–the perpetual quest for change in Norwegian nursing homes. In: Designing Wellbeing in Elderly Care Homes. Aalto University Publication Series; 2013:68.
10. Fjær EG, Vabø M. Shaping social situations: a hidden aspect of care work in nursing homes. J Aging Stud. 2013;27(4):419–427. doi:10.1016/j.jaging.2013.10.002
11. van Hoof J, Verbeek H, Janssen B, et al. A three perspective study of the sense of home of nursing home residents: the views of residents, care professionals and relatives. BMC Geriatr. 2016;16(1):1–15. doi:10.1186/s12877-016-0344-9
12. Cooney A. ‘Finding home’: a grounded theory on how older people ‘find home’in long‐term care settings. Int J Older People Nurs. 2012;7(3):188–199. doi:10.1111/j.1748-3743.2011.00278.x
13. De Veer AJ, Kerkstra A. Feeling at home in nursing homes. J Adv Nurs. 2001;35(3):427–434. doi:10.1046/j.1365-2648.2001.01858.x
14. Johannessen T, Ree E, Aase I, Bal R, Wiig S. Exploring challenges in quality and safety work in nursing homes and home care–a case study as basis for theory development. BMC Health Serv Res. 2020;20(1):1–12. doi:10.1186/s12913-020-05149-x
15. Nakrem S. Understanding organizational and cultural premises for quality of care in nursing homes: an ethnographic study. BMC Health Serv Res. 2015;15(1):508. doi:10.1186/s12913-015-1171-y
16. Ettelt S, Williams L, Damant J, Perkins M, Wittenberg R. What kind of home is your care home? A typology of personalised care provided in residential and nursing homes. Ageing Soc. 2022;42(5):993–1013. doi:10.1017/S0144686X20001142
17. Kitwood TM. Dementia Reconsidered: The Person Comes First. Vol. 20. Open university press Buckingham; 1997.
18. McCabe M, Byers J, Busija L, Mellor D, Bennett M, Beattie E. How important are choice, autonomy, and relationships in predicting the quality of life of nursing home residents? J Appl Gerontol. 2021;40(12):1743–1750. doi:10.1177/0733464820983972
19. Allen D. The Invisible Work of Nurses: Hospitals, Organisation and Healthcare. Rooutledge; 2014:1–154.
20. Genet N; European Observatory on Health S, Policies. Home care across Europe: current structure and future challenges. In: Observatory Studies Series. Vol. 27. World Health Organization; 2012.
21. Helsedirektoratet. Period of residence in nursing homes and duration of services for home residents (in Norwegian). Vol. 02/2017; 2017:16.
22. Ciesielska M, Boström KW, Öhlander M. Observation methods. In: Qualitative Methodologies in Organization Studies. Springer; 2018:33–52.
23. Clarke V, Braun V, Hayfield N. Thematic analysis. Qual Psychol. 2015;222(2015):248.
24. Terry G, Hayfield N, Clarke V, Braun V. Thematic analysis. In: The SAGE Handbook of Qualitative Research in Psychology. Sage; 2017:17–37.
25. Omsorgsdepartementet H-O. Act related to medical and healthare research (Health Rsearch Act). In: Omsorgsdepartementet H-O, editor. Lovdata. 2008, part 6. p.979. Lovdata.no; 2009:2008–2468.
26. Gubrium JF. Living and Dying at Murray Manor. University of Virginia Press; 1997.
27. Lincoln YS, Guba EG. Naturalistic Inquiry. Sage; 1985.
28. Donabedian A. The quality of care: how can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.1988.03410120089033
29. Sandvoll AM, Kristoffersen K, Hauge S. New quality regulations versus established nursing home practice: a qualitative study. BMC Nurs. 2012;11(1):7. doi:10.1186/1472-6955-11-7
30. McCormack B, McCance TV. Development of a framework for person‐centred nursing. J Adv Nurs. 2006;56(5):472–479. doi:10.1111/j.1365-2648.2006.04042.x
31. Vassbø TK, Kirkevold M, Edvardsson D, Sjögren K, Lood Q, Bergland Å. The meaning of working in a person-centred way in nursing homes: a phenomenological-hermeneutical study. BMC Nurs. 2019;18(1):1–8. doi:10.1186/s12912-019-0372-9
32. Grøndahl VA, Aagaard H. Older people’s involvement in activities related to meals in nursing homes. Int J Older People Nurs. 2016;11(3):204–213. doi:10.1111/opn.12111
33. Harnett T, Jönson H. Shaping nursing home mealtimes. Ageing Soc. 2017;37(4):823–844. doi:10.1017/S0144686X1500152X
34. Edvardsson D. Therapeutic environments for older adults: constituents and meanings. J Gerontol Nurs. 2008;34(6):32–40. doi:10.3928/00989134-20080601-05
35. Rambøll. Quality in nursing homes in Oslo (in Norwegian). 2016–2018. 2019. https://www.nhosh.no/contentassets/e2186bb5f34d48b2aab5dc603ef60fb3/rapport-kvalitet-ved-sykehjem-i-oslo-2016-2018.pdf.
36. Hughes K, Moore S. Quality of life versus quality of care: elderly people and their experience of care in South Australian residential facilities. Practice. 2012;24(5):275–285. doi:10.1080/09503153.2012.740451
37. Harnett T, Jönson H. ‘They are different now.’biographical continuity and disruption in nursing home settings. J Aging Stud. 2017;42:1–8. doi:10.1016/j.jaging.2017.05.003
38. Stabell A, Eide H, Solheim GA, Solberg KN, Rustøen T. Nursing home residents’ dependence and Independence. J Clin Nurs. 2004;13(6):677–686. doi:10.1111/j.1365-2702.2004.00942.x
39. Skaalvik MW, Normann K, Henriksen N. Nursing homes as learning environments: the impact of professional dialogue. Nurse Educ Today. 2012;32(4):412–416. doi:10.1016/j.nedt.2011.03.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.