")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
For Fiddlers on the Roof and in the Pit: Healthcare and Epidemiology of Playing-Related Problems in Violinists
Authors Zinn-Kirchner ZM , Alotaibi M , Mürbe D, Caffier PP
Received 11 June 2023
Accepted for publication 10 August 2023
Published 28 August 2023 Volume 2023:16 Pages 2485—2497
DOI https://doi.org/10.2147/JMDH.S425406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zahavah M Zinn-Kirchner,1,2 Moonef Alotaibi,2,3 Dirk Mürbe,1,2 Philipp P Caffier1,2
1Berlin Center for Musicians Medicine (BCMM), Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany; 2Department of Audiology and Phoniatrics; Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany; 3King Fahad Medical City, Department of Otorhinolaryngology, Head and Neck Surgery, Riyadh, Kingdom of Saudi Arabia
Correspondence: Philipp P Caffier, Department of Audiology and Phoniatrics, Berlin Center for Musicians Medicine, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany, Campus Charité Mitte, Charitéplatz 1, Berlin, D-10117, Germany, Tel +4930 450 655 097, Fax +4930 450 555 931, Email [email protected]
Abstract: Musicians, specifically violinists, may experience pain or loss of function as a result of poor playing hygiene, environmental factors, and insufficient guidance from teachers, parents, conductors, and physicians. The causal occurrence of these pathologies and the efficacy of general treatment, along with referral to other specialists for adjunct therapies and rehabilitation, were examined in this literature review. A systematic PubMed search was conducted in May 2022 to gain insight into the current state of the published literature. Inclusion criteria were cross-sectional or comparative studies that address relevant pathologies among violinists by specialty. The search resulted in 25 cross-sectional, 5 comparative studies, and 1 case review including a total of 6010 musicians, among them at least 920 violinists. Orthopedists, neurologists, dentists/orthodontists, dermatologists, and audiologists are most commonly consulted to treat violinists’ complaints. Other internists and various paramedical specialists can equally be affected and should be sensitive to the complaints of musicians. In conclusion, the field of performing arts medicine is extremely wide and requires multidisciplinary specialist attention. The studies chosen highlight that violinists may suffer great discomfort at the hands of their instrument and merit adequate guidance from physicians in order to be able to continue playing in a safe, ergonomic way.
Keywords: performing arts medicine, string health, upper strings, musico-medical care, instrument-associated disease, musician-associated injuries, music pathology
Introduction
In his seminal piece, De morbis artificum diatriba, Italian physician Bernardino Ramazzini spoke in as early as 1713 of,
Workers in whom certain morbid affections gradually arise from some particular posture of the limbs or unnatural movements of the body called for while they work.1
The ways in which this wisdom applies to musicians, specifically violinists, will be examined in this literature review.
There is a long-standing tradition of performing arts medicine in Germany that has set the standard for understanding two facets of our human experience that have the potential to enrich our lives: music and medicine. “Die Berufskrankheiten der Musiker” (Diseases of the musical profession) by German-Jewish neurologist Kurt Singer was translated and published in 1932.2 His aim was to more closely examine the physical symptoms of musicians who, like those in other professional groups, had specific complaints associated with their playing. Carl Flesch,3 Friedrich A. Steinhausen and Wilhelm Trendelenburg are other notable figures in this field. Siegfried Kahle was one of the first physicians to examine violinists specifically in “Die Geigerkrankheit” (Fiddler’s disease).4 Former East Germany instated the “Betriebsambulatorium der Berliner Bühnen” in cooperation with the Charité University Hospital Berlin in 1975, an interdisciplinary organization that offered a range of medical assessments to musicians employed on Berlin’s stages. The string initiative, founded in 1978, is especially noteworthy and was created to examine maladies specific to string instruments, offer psychological support, arrange appointments with specialists, and offer strategies for maintaining good playing hygiene/technique.5 This aim has been carried into the Federal Republic of Germany by the German Association for Music Physiology and Musicians’ Medicine (Deutsche Gesellschaft für Musikphysiologie und Musikermedizin, DGfMM) which publishes a monthly journal and is committed to supporting healthy playing.6 On an international level, the ICSOM (International Conference of Symphony and Orchestra Musicians) laid the foundation for studying pathologies among performing artists by publishing the results of a comprehensive survey of 2212 musicians in 1987 though it made no specific points that pertained to violin players.7
There are several pathologies that may arise specifically among violinists that have yet to be tallied comprehensively in a review of the current literature. In order to do so, an understanding of the instrument itself is necessary. The violin is a hollow, wooden, four-stringed instrument, which is played by placing the neck portion in the left hand and allowing the body to rest on the left shoulder. The chin is placed on its respective rest as shown in Figure 1.
 |
Figure 1 The violin and its use. (A) Structure of the instrument (1, corpus; 2, fingerboard; 3, tuning pegs; 4, fine tuners; 5, bridge; 6, chinrest; 7, Tourte bow; 8, tip; 9, frog). (B) Physiological body posture and position of head, shoulders, arms, hands and fingers while playing the violin. The person in (B) has provided written informed consent for the image to be published. |
The right hand holds the bow at the weighted bottom and pulls it across the strings horizontally. The bow evokes vibrations on the strings which resonate through the body of the instrument and serve to amplify the sound. Pitch is modulated by the placement of the left hand on the finger board. During childhood, the size of instruments varies as the player ages, adapting to their own growing limbs. Typically, a violin weighs around 500g, while bows range from 51–60g. Violin-playing requires an outer rotation of the left upper arm whilst holding the forearm in supination; the elbow joint should bend no less than 50°. Abduction in the frontal plane, anteversion in the sagittal plane and outer rotation are necessary to successfully play the violin.5 Excellent control of the fine muscles of all fingers is equally important. While playing the instrument should be pain-free under physiological circumstances, there are some pathologies that may arise among those who play frequently and some pre-existing conditions that may predispose players to pain during playing. As stated above, there are numerous multidisciplinary organizations, within Germany alone, which have examined these issues over the course of the past several decades. As many of these organizations are not strictly medical, there has yet to be a conclusive tally of pathologies among violinists from a medical perspective. This literature review will attempt to answer the following questions:
- What long-term effects may arise from playing the violin?
- What pre-existing conditions make it difficult to play the violin?
The role of the physician and other specialists will be evaluated based on the current literature, in an attempt to uncover the nuances of interdisciplinary musico-medical care.
Materials and Methods
Inclusion and Exclusion Criteria
The data obtained in the studies analyzed in this literature review were among a human population of cross-sectional or comparative studies and include one case review. The data selected was published in English, German, Spanish or French and examined the potential occupational and recreational hazards of violin-playing. Individual case reports that showed pathologies that had more homogeneously been recorded and analyzed elsewhere were excluded. Papers that suggested ergonomic alterations to prevent such pathologies from arising were not included though their central points were useful in considering questions answered in the discussion. In addition, studies were excluded if they were not accessible online or if they were correspondence letters that did not retrieve original data. Studies and case reports that spoke of violinists who had been injured in other contexts and thus suffered consequences in their playing were also not included.
Search Strategy
The following database was searched on May 15th, 2022: PubMed/NLM/NIH: 2243 hits, 169 potentially relevant, 30 included. The following search strategy was used:
Violin OR violins OR violinist OR violin players OR high strings NOT violin spider NOT Thomson OR fiddle OR fiddler NOT violin making NOT fiddler crab NOT violin plot.
A further filter was applied to limit search results to human subjects. Specifying the search to include terms such as “performing arts medicine” or “injury” was not necessary, seeing as the results were accurate enough to fully encompass the extent of the search. No limit for time was applied; results ranged from 1948 to 2022. 2243 papers were found in total, most of which could be eliminated by title only. 169 papers were considered for closer revision, 80 of which were specific enough to be examined based on their abstracts. 30 of these were cross-sectional studies or comparative studies and addressed this review’s central questions in a significant way. Additionally, three books were used to gain additional background and source material though only one of these contained a case report included in Table 1. A flowchart of the steps in our article search with the number of publications found and included in this review is shown in Figure 2.
 |
Table 1 Overview of Included Studies |
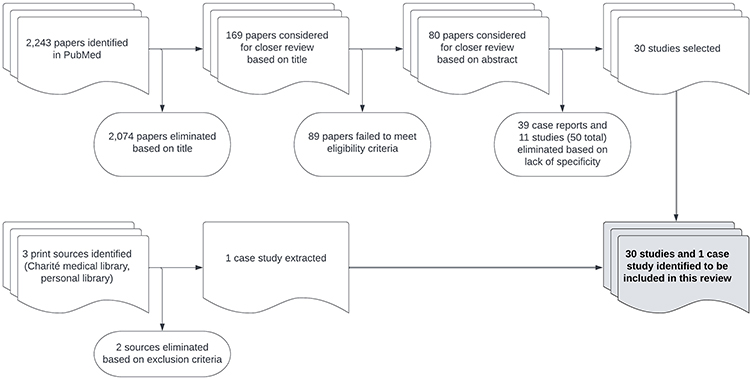 |
Figure 2 Schematic representation of selection process following PubMed search and print sources. |
Data Extraction and Study Quality Assessment
The studies and case review chosen were reviewed according to the inclusion and exclusion criteria enumerated above, as well as their novelty of presentation or unique individual data points that lent a deeper understanding of the respective pathophysiology they were observing. All research was performed in accordance with the Charité ethics committee’s regulations. Seeing as all of the studies chosen were of a comparative or cross-sectional nature and there were no clinical trials that involved the specific pursuit of treatment options, no inherent bias relating to conflicts of interest or sponsorship is to be suspected.
Results
The systematic search on PubMed following the criteria listed above yielded 30 papers with 6010 subjects, containing at least 920 violinists. One case review including one violinist among 33 total participants was included from a print source. Table 1 shows the studies listed by symptoms in the medical specialties in which they present and sorted alphabetically, containing the relevant information pertaining to the study population and the study design. 25 cross-sectional and/or observational studies and five comparative studies were included, along with one case review. Some papers listed age, gender, and playing time in years as exclusion criteria.
Owing to the instrument’s architecture and playing method, there are pathologies that may arise for at least four distinct reasons: first, the places on the body on which contact is established or pressure is exerted by the placement of the instrument (neck, clavicle, jaw, and temporomandibular joint) or the strain of playing it (shoulder, elbow, and hand). Second, allergens that may be present in the body of the instrument, the bow, or the rosin; third, increased sound exposure over extended periods, and finally, practice conditions that lend themselves to poor physical and mental hygiene (eg, chairs, lighting, extended workload with insufficient breaks, fear of failure, excessive expectations with pressure from teachers, conductors or oneself). The specialty-dependent pathologies are briefly summarized below.
Orthopedics and Neurology
Playing-Related Musculoskeletal Disease (PRMD)
Playing-related muscular disease is perhaps one of the best recorded ailments afflicting violinists. Over time, fine, deliberate movements necessary to produce clean, resonant sound can cause painful cramping and chronic illness, which may result in discontinuing practice.5 14 studies were found including 4043 participants and 1322 violinists/high strings. The subjects of all 14 studies complained of sustained muscular and joint pain, almost exclusively in the upper extremities.8–21 An Australian study on adolescents including 135 violinists reported a statistically significant lifetime OR of 2.13 of developing PRMD. Symptoms ranged from jaw, shoulder, elbow, wrist, and hand pain to measured spinal hyperlordosis, scapular dyskinesia, paresthesia and tendinitis.14 One study noted 12% of players being forced to quit as a result of pain or function-related issues.8 Nearly all studies relayed players reporting of an improved playing experience after implementing more frequent breaks, mobility exercises, relaxation techniques and positive relationships with teachers.
Focal Dystonia
Focal dystonia is a pathology commonly affecting the hand that appears with a frequency of 1:3400 among the general population and 1:200 among violinists.38 Spahn et al define dystonia as an unwarranted, painless dyscoordination which manifests in curling or splaying of the fingers with compensatory stretching out of others. One of the hypotheses for this phenomenon is an increased activity of basal ganglia with defective lateral inhibition on spinal and cortical levels. Focal dystonia is limited to a specific motor context and leads to a worsening of playing quality, never appearing while the performer is at rest. If dystonia persists over long periods of time, the performer may be forced to end their career.39 One study and one case review that examined focal dystonia in musicians considered violinists. Wilson et al reported the case of a conservatory student whose primary instrument was the violin in a cohort of 33 students total. She began to play her secondary instrument (piano) at a high frequency to achieve improvement quickly and observed fine muscle fiber deterioration and difficulty and pain in her violin practice. It is also relevant to distinguish between bowing arm and fingering arm dystonia, the former usually resulting in more serious ramifications.23 Schuele et al observed this in a cross-sectional study with 15 violinists. Contrary to Spahn et al’s definition, Schuele observed difficulties performing other activities like writing in 24% of participants. Dystonic symptoms occurred in the fingering hand in 76% of participants, while only 24% noticed dystonia in the bowing arm and on average this pathology arose several years later. EMGs of four patients showed signs of neural impingement of the median, ulnar and some segments of the radial nerve which may explain the pain. 62% of performers altered career paths to accommodate for their loss of movement and/or pain, including all five participants who suffered from bow arm dystonia.22 Figure 3 shows the dyscoordination of bowing arm and fingering arm dystonia in a violinist presenting at our Berlin Center for Musicians Medicine.
 |
Figure 3 Patient example with bowing arm (upper row) and fingering arm dystonia (lower row). Initial playing with physiological position of fingers (A and D), followed by pathological dyscoordination: (B and E), stretching out of digitus minimus. (C) Cramping of right hand with increased pronation during intense playing (curling of index finger, splaying of ring finger, hyperextension of digitus minimus). (F) cramping of left hand during intense ring finger vibrato with large amplitude and high frequency (compensatory splaying of other fingers). |
Dental Medicine and Orthodontics
Cranial Bone Development
Players that begin to study the violin seriously from a young age may observe changes in the development of their facial structures. Three studies described this phenomenon. A Lithuanian study found a crossbite in 62% of participants, and 42% with a forward-leaning head position.28 Kovero et al studied cranial bone development among musicians in two studies and observed a dominance of musculature on the right side of the face and more proclined incisors in the upper and lower jaws among a younger cohort (range 11–18 years of age), while the older group (22–58 years of age) showed no notable facial asymmetry but a smaller total facial height.26,27
Temporomandibular Disorders (TMD)
Temporomandibular disorders can occur among members of any professional group and describe a disharmonious articulation of the temporomandibular joints that usually attach the temporal bone to the mandible. TMD can cause clicking of the jaw while speaking or chewing and may cause discomfort upon movement, headaches, palpatory tenderness or deflection in a specific direction.24 Two studies could be identified that addressed this pathology. In a comparative paper of adolescents, Kovero et al observed that weekly playing hours correlated with some form of TMD and noted more palpatory tenderness, more clicking, and more painful mandibular movements in students with TMD compared to controls.40 Rodriguez et al also observed pain in maximum mouth opening, clicking, or other unwarranted sounds and even statistical significance for nail-biting, which the authors describe as a “parafunctional habit”.25
Audiology
Hearing loss is a pathology afflicting many orchestral musicians to varying degrees. Violin players may be especially at risk for developing left-ear hearing impairment, seeing as the instrument is played on the left shoulder and thus sound finds its shortest path here.32 First violinists have the benefit of sitting at the edge of the orchestra, with distance separating them from those seated within the brass section. The sounds they hear most loudly are merely those of their own section, while second violinists are submerged not only between the first violin and viola section but may border flutes, piano, harpists and percussion in addition.35 Five studies were identified that more closely evaluated the impact of high sound exposure over time on the violinist’s ear. Kahäri et al identified an altered hearing threshold, especially in the left ear, as a result of more proximal sound exposure.32 Similar results were found by four studies.31,33–35 Schmidt et al, specifically, observed that the left-ear sound pressure level peaks with a higher dB mean than other strings.34 Ostri et al observed an overall hearing disability of 10% among violinists.33 Figure 4 shows the inner ear hearing loss at the left side in a violinist presenting at our Berlin Center for Musicians Medicine.
 |
Figure 4 Sensorineural hearing loss at the left inner ear in a 20-year old professional violinist. History of 16 years of playing and > 20,000 cumulative practice hours (average 3–5h/day). Above: Pure-tone audiometry with left-sided noise induced c5-dip (ie, 4 kHz loss) caused by asymmetric long-term exposure to higher loudness levels of own instrument. Below: Transitory evoked otoacoustic emissions (TEOAE) with corresponding evidence of damage to the outer hair cells. |
Dermatology and Allergology
The violin is held in the crook of the neck, supported between the left shoulder and left side of the mandible. During prolonged practice sessions or performance, the constant pressure exerted against the neck in combination with friction may result in lesions. This phenomenon is more commonly known as “fiddler’s neck”. Myint et al argue that there should be two varying definitions, depending on the point in which the pressure focuses. They posit that fiddler’s neck “type 1” is a submandibular form, while type 2 relates to a supraclavicular form.41 Two large cross-sectional studies could be identified that assessed fiddler’s neck and related forms of contact eczema in violinists.
Gambichler et al reported various skin-related changes in 68.5% of players with 15% of violinists/violists suffering from fiddler’s neck. One violinist reported a colophonium/resin allergy while many other callosities, contact dermatitis, and erosions.29 Onder et al found similar results (18% fiddler’s neck) in addition to a high frequency of allergic reactions.30 Morphology may vary from lichenification, pigmentation, and scaling, vesicular irritant contact dermatitis of fiddler’s neck type 1 to type 2, which more frequently displays allergic, pruritic contact dermatitis caused by the metal brackets attaching the chin rest to the violin. Figure 5 shows different appearances of fiddler’s neck type 1 in two violinists presenting at our Berlin Center for Musicians Medicine.
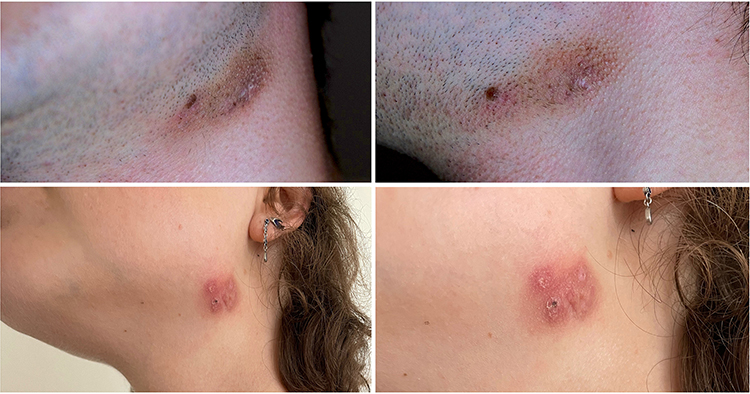 |
Figure 5 Variable manifestations of fiddler’s neck type 1 caused by mechanical pressure and shear stress on the submandibular skin. Upper row: secondary flat darkening of a patch of skin due to hyperpigmentation in a male violinist. Lower row: more erythematous and prominent finding with eczematous, papular and scaly thickening of the skin due to lichenification in a female violinist. |
A violinist developed occupational asthma from unheated colophony with a decrease in FEV1 of 30% within the first 60 minutes.42 Allergies may include nickel sulfate, cobalt chloride, colophonium, formaldehyde, and shavings of ebony wood. Violin varnish containing propolis has been shown to provoke a reaction in some.43 Other patients have shown allergies to rosewood, abietic acid, turpentine, carbamate, para-phenylenediamine, balsam of Peru,44 chlorineacetamide and rubber.39 Changing the strings45 or playing with synthetic strings,46 implementing a chin rest, surgical tape, a cloth, applying desonide 0.05%47 or other topical steroids,43 calamine, cetirizine, or even excision may be treatment options, depending on the specific pathophysiology.
Psyche
While psychosomatic medicine and musical psychology are specialties unto themselves, it seems pertinent to mention, at least briefly, the psychological aspect of being a professional musician. Musical performance anxiety (MPA) is a phenomenon observed frequently among musicians though it is seldom spoken about as a serious medical diagnosis that requires specialist attention. Both the Karasek demand-control model, as well as the Yerkes-Dodson-curve may help to delineate a healthy relationship between expectation and output. Astoundingly, a musician may become unable to perform without a basal, self-imposed, unphysiological strain over time.39 Two studies were found that evaluated this intersection. Amorim et al found a significant correlation between temporomandibular disorders and performance anxiety among violinists in Portugal, so that physical ailment may manifest as psychological or vice versa.36 Bourne et al observed a vicious cycle in orchestral musicians: pain was exacerbated by overpracticing and constant comparison to others and pressure imposed by conductors, while players were so plagued by pain that it became impossible to focus on the music. Recreational activities were no longer enjoyable for fear of injury. Players expressed a desire for more open dialogue on such issues.37
Other Specialties
While the results tallied in Table 1 have most commonly been the subject of research, there are case reports from many other specialties that warrant mention. Ophthalmologists may encounter violinists with presbyopia or cataracts and those struggling to accommodate between the distance to conductor and their music stand.39 There are many further aspects of neurology, ie, carpal tunnel syndrome, fingertip anaesthesia, and bowing tremors to name a few.48 Some of these are mentioned in other papers relating to PRMD and focal dystonia though none choose to focus on them specifically. Patients with rheumatoid arthritis may struggle with learning the instrument though no studies have been performed to examine whether or not they should be deterred from learning how to play.39
Discussion
After having evaluated these studies, violin-specific pathologies could be identified in several specialties. While these studies did not directly advise nor deter subjects from pursuing a career in violin, there are sources that have found some pathologies that may be unadvisable. The exact process of when and to what extent specialists of other medical and paramedical disciplines should be consulted for co-treatment or rehabilitation has also not been sufficiently described in the published literature.
Improvement by Field
Physicians of many different specialties may be responsible for the specific care for violinists – violinists may not know whom to address for help or what the origin of their complaints is. Doctors may not feel responsible, as violinists may experience multiple complaints simultaneously. In our experience, it is advisable in these cases to introduce multi-disciplinary treatment specialists (eg, physiotherapists, osteopaths, and psychologists) as early as possible to prevent chronification. The benefits of multidisciplinary approaches in healthcare are widely documented and include but are not limited to, better access to health information, shorter time from diagnosis to treatment, improved treatment and quality care, higher patient satisfaction, and better overall outcomes.49–51
There are several questions that remain to be answered, one of the most central being if it is possible to predict whether or not someone may develop a pathology over time. Considering the data tallied here, more cross-sectional and comparative studies would be required in different populations, preferably taking into account gender, age, playing time, and overall health, in order to make proper assessments. While this literature review is by no means the first to observe that a violinist may experience different types of pain as a result of playing, it is important to underline that performing arts medicine is a broad field that encompasses the expertise of many different kinds of specialists. The complaints raised by players and recorded in the studies tallied here may be aided by simple changes to the playing and practice regimen.
Some attempts have already been made to mitigate violinists’ complaints:
In orthopedics, correct posture is the key component for good playing hygiene. Bearing this in mind, Günter Heidrich designed an ergonomically modified orchestra chair in as early as 1978 in cooperation with the Charité University in Berlin, Germany, that would lend support especially to the lumbar and sacral spine and would enable upright posture without additional muscle work from the player.5 Though this chair never successfully made it into practicing rooms, something like it would potentially solve many of the PRMD-related complaints violinists may experience. Other practices and prevention strategies such as frequent breaks, progressive muscle relaxation, Alexander Technique, osteopathy, warmth and/or cold seem feasible for musicians to perform regularly, especially if emphasized within the community and by private teachers. Focal dystonia will be able to be more successfully remedied when its pathophysiology has been more fully understood. Neurological experts such as Eckart Altenmüller and Mark Hallett have championed the use of Botox treatments, among other things in patients with bowing tremors and have observed great success.52,53 Above all, adequate rest must be implemented into practice regimes and orchestral rehearsals.
Hearing loss poses complications for musicians as they age. The margin by which hearing worsens compared to presbycusis in non-musicians would need to be explored specifically. Seeing as blocking sound completely would be counter-productive in an orchestra setting, something like selectively filtering earbuds in different frequency ranges would need to be implemented, as tested by a Polish study.54
One of the most vital preventative measures in avoiding the occurrence of fiddler’s neck is proper education. Teachers should make a point of finding chin and shoulder rests fitted to the player, test for allergens in the instrument and accessories should symptoms arise, and emphasize the importance of ample rest during intensive practice periods. The study did not explore the concept of fiddler’s neck as a symbol of diligent practice and a source of pride - a notion which pervades much of the playing world. This would need to be dismantled in order to achieve a healthy working environment.55
There have also been some efforts to alleviate discomfort caused by temporomandibular disjunction, most notably oral splints.56 These could prove useful in preventing crossbites and manifestations of TMD. It seems prudent to add, however, that if a young person spends so much time with an instrument that their cranial bone development is impacted, it may be a sign to invest fewer hours or speak with parents, who are often responsible for mandating them.
Finally, as stated at the beginning, the psychological components of professional musicianship warrant much research of their own. More than likely, stress experienced before or during a performance is not merely a fear of playing the wrong tones, but an interwoven tapestry of self-doubt, the expectations of others, competition with fellow players, and future opportunities. The Freiburg Model was created by physicians at the University of Freiburg, Germany, to help individuals develop grounding practices for high-stress performance situations. The key to dismantling fear may be breaking it down into preparation, performance and assessment.39 Other frameworks have been suggested more recently in order to nip pathologies in the bud. One suggests evaluating the player’s individual medical history, observing their everyday playing posture by standardized assessment or video analysis and tracking their overall playing habits in a practice versus a performance setting. Implementing warm-ups and other ergonomic habits, as well as educating all musicians on the importance of looking after their health, may be able to affect the necessary paradigm shift.57
There are other pre-existing conditions not touched upon by these studies, which may make playing difficult and would require a review of their own. Any medical specialist should make a point of evaluating the health of their patients in a holistic way, taking into account the myriad physical and mental strains imposed on such high-performance musicians by the nature of their profession.
Limitations of This Review
The field of performing arts medicine is extremely broad and constantly developing in new directions. Focusing on even one instrument heralds a multitude of search results that could have been explored far more in detail barring the word count of this brief review. There are specialties outside those mentioned that may be relevant. This review could only encompass information published in the studies found – there are simply many areas that have not yet been the subject of research and there may very well be relevant studies that the search strategy was simply not sensitive enough to find. At least one study cited a potential selection bias owing to the musicians’ fears of suffering consequences at reporting their physical complaints or comments on their experiences at work.37 Cross-sectional studies may be insufficient to accurately understand the scope of these pathologies seeing as they represent a singular point of measurement at one point in time. However, some of the questionnaires answered by participants did include questions such as, “Have you experienced pain while playing your instrument in the past?” vs “Have you experienced pain in the past 12 months?”.11 Similarly, comparative studies, like those chosen here, also rely on observations and comparisons where correlation may not equal causation. These limitations were considered upon selection but were deemed an inconsequential hurdle to extracting valid data in the studies listed in Table 1.
Conclusion
To conclude, violin players may be afflicted by many pathologies owing to both their playing habits and the environments in which they perform. Orthopedists, neurologists, dentists and orthodontists, dermatologists, audiologists, psychosomatic physicians, and psychologists may treat violinists more frequently than other groups. Players with pre-existing conditions in any of these fields may find difficulties in playing. Involving specialists from a plethora of medical and paramedical backgrounds can not only enrich the treatments offered but may also show improved patient health and satisfaction overall.
Players may not always take their medics’ advice and choose to continue practicing despite pain; not every physician can be a violinist and understand the keen passion for an instrument. Sensitivity, care, and time are required among physicians, teachers, and conductors to ensure the health of musicians in their playing, as their instruments often accompany them throughout the course of their lives – it would be prudent to prevent pain and discomfort from being unwanted passengers on this journey.
To strengthen the health of string players, the education of all students in music physiology should be a fundamental part of their training, in addition to the prevention of playing-related diseases. Medical and paramedical professionals recognizing performing arts medicine as a form of occupational medicine are a crucial step toward developing the sensitivity to track epidemiological trends in this group, in order to better recognize and treat pathologies in the future.
Disclosure
The authors report no conflicts of interest.
References
1. Ramazzini B. De morbis artificum diatriba [diseases of workers]. Am J Public Health. 2001;91(9):1380–1382. Latin. doi:10.2105/ajph.91.9.1380
2. Singer K. Diseases of the Musical Profession: A Systematic Presentation of Their Causes, Symptoms and Methods of Treatment. Greenberg; 1932.
3. Flesch C. Urstudien (Basic Studies) for Violin. Fischer; 1911.
4. Kahle S. Die Geigerkrankheit [Fiddler’s Disease] [Medical Dissertation]. Berlin Academy for Continuing Medical Education; 1966. German.
5. Wagner C. Medizinische Probleme Bei Instrumentalisten: Ursachen Und Prävention. [Medical Problems in Instrumentalists: Causes and Prevention]. Laaber: Laaber; 1995. German.
6. Satzung deutsche Gesellschaft für musikphysiologie und musikermedizin [Statutes of the German association for music physiology and musicians’ medicine]. Available from: https://dgfmm.org/gesellschaft/satzung.
7. Middlestadt SE, Fishbein M. Health and occupational correlates of perceived occupational stress in symphony orchestra musicians. J Occup Med. 1988;30(9):687–692.
8. Kaufman-Cohen Y, Ratzon NZ. Correlation between risk factors and musculoskeletal disorders among classical musicians. Occup Med. 2011;61(2):90–95. doi:10.1093/occmed/kqq196
9. Kok LM, Schrijvers J, Fiocco M, van Royen B, Harlaar J. Differences in violin fixation force and muscle activity among violinists with and without complaints of the neck shoulder region. J Electromyogr Kinesiol. 2018;43:217–225. doi:10.1016/j.jelekin.2018.11.002
10. Lahme A, Eibl I, Reichl FX. Typical musculoskeletal patterns in upper string players with neck and arm problems. Med Probl Perform Art. 2014;29(4):241–242. doi:10.21091/mppa.2014.4047
11. Leaver R, Harris EC, Palmer KT. Musculoskeletal pain in elite professional musicians from British symphony orchestras. Occup Med. 2011;61(8):549–555. doi:10.1093/occmed/kqr129
12. Lima RC, Pinheiro TM, Dias EC, de Andrade EQ. Development and prevention of work related disorders in a sample of Brazilian violinists. Work. 2015;51(2):273–280. doi:10.3233/WOR-141904
13. Nyman T, Wiktorin C, Mulder M, Johansson YL. Work postures and neck-shoulder pain among orchestra musicians. Am J Ind Med. 2007;50(5):370–376. doi:10.1002/ajim.20454
14. Ranelli S, Straker L, Smith A. Playing-related musculoskeletal problems in children learning instrumental music: the association between problem location and gender, age, and music exposure factors. Med Probl Perform Art. 2011;26(3):123–139. doi:10.21091/mppa.2011.3021
15. Savino E, Iannelli S, Forcella L, et al. Musculoskeletal disorders and occupational stress of violinists. J Biol Regul Homeost Agents. 2013;27(3):853–859.
16. Siemon B, Borisch N. Problems of the musculoskeletal system in amateur orchestra musicians under special consideration of the hand and wrist. Handchir Mikrochir Plast Chir. 2002;34(2):89–94. doi:10.1055/s-2002-32310
17. Steinmetz A, Scheffer I, Esmer E, Delank KS, Peroz I. Frequency, severity and predictors of playing-related musculoskeletal pain in professional orchestral musicians in Germany. Clin Rheumatol. 2015;34(5):965–973. doi:10.1007/s10067-013-2470-5
18. Tawde P, Dabadghav R, Bedekar N, Shyam A, Sancheti P. Assessment of cervical range of motion, cervical core strength and scapular dyskinesia in violin players. Int J Occup Saf Ergon. 2016;22(4):572–576. doi:10.1080/10803548.2016.1181892
19. van Selms MKA, Wiegers JW, van der Meer HA, Ahlberg J, Lobbezoo F, Visscher CM. Temporomandibular disorders, pain in the neck and shoulder area, and headache among musicians. J Oral Rehabil. 2020;47(2):132–142. doi:10.1111/joor.12886
20. Vastamaki M, Vastamaki H, Ristolainen L, Laimi K, Saltychev M. Violists and violinists report more intense hand pain on NRS than other orchestra musicians. Med Probl Perform Art. 2020;35(3):162–166. doi:10.21091/mppa.2020.3024
21. Vilela AC, Nogueira LA, Ferreira AS, Kochem FB, Almeida RS. Musculoskeletal pain and musical performance in first and second violinists of professional youth chamber orchestras: a comparative study. Med Probl Perform Art. 2021;36(4):263–268. doi:10.21091/mppa.2021.4029
22. Schuele S, Lederman RJ. Long-term outcome of focal dystonia in string instrumentalists. Mov Disord. 2004;19(1):43–48. doi:10.1002/mds.10647
23. Wilson FR, Wagner C, Homberg V. Biomechanical abnormalities in musicians with occupational cramp/focal dystonia. J Hand Ther. 1993;6(4):298–307. doi:10.1016/s0894-1130(12)80331-0
24. Kovero O, Kononen M. Signs and symptoms of temporomandibular disorders in adolescent violin players. Acta Odontol Scand. 1996;54(4):271–274. doi:10.3109/00016359609003536
25. Rodriguez-Lozano FJ, Saez-Yuguero MR, Bermejo-Fenoll A. Prevalence of temporomandibular disorder-related findings in violinists compared with control subjects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(1):e15–19. doi:10.1016/j.tripleo.2009.08.032
26. Kovero O, Kononen M, Pirinen S. The effect of violin playing on the bony facial structures in adolescents. Eur J Orthod. 1997;19(4):369–375. doi:10.1093/ejo/19.4.369
27. Kovero O, Kononen M, Pirinen S. The effect of professional violin and viola playing on the bony facial structures. Eur J Orthod. 1997;19(1):39–45. doi:10.1093/ejo/19.1.39
28. Masiulyte V, Zaroviene A, Svalkauskiene V. Orthodontic problems among string and wind instrument players. Stomatologija. 2021;23(2):41–47.
29. Gambichler T, Uzun A, Boms S, Altmeyer P, Altenmuller E. Skin conditions in instrumental musicians: a self-reported survey. Contact Dermatitis. 2008;58(4):217–222. doi:10.1111/j.1600-0536.2007.01310.x
30. Onder M, Aksakal AB, Oztas MO, Gurer MA. Skin problems of musicians. Int J Dermatol. 1999;38(3):192–195. doi:10.1046/j.1365-4362.1999.00656.x
31. Jansen EJ, Helleman HW, Dreschler WA, de Laat JA. Noise induced hearing loss and other hearing complaints among musicians of symphony orchestras. Int Arch Occup Environ Health. 2009;82(2):153–164. doi:10.1007/s00420-008-0317-1
32. Kahari KR, Axelsson A, Hellstrom PA, Zachau G. Hearing assessment of classical orchestral musicians. Scand Audiol. 2001;30(1):13–23. doi:10.1080/010503901750069536
33. Ostri B, Eller N, Dahlin E, Skylv G. Hearing impairment in orchestral musicians. Scand Audiol. 1989;18(4):243–249. doi:10.3109/01050398909042202
34. Schmidt JH, Pedersen ER, Juhl PM, et al. Sound exposure of symphony orchestra musicians. Ann Occup Hyg. 2011;55(8):893–905. doi:10.1093/annhyg/mer055
35. Schmidt JH, Pedersen ER, Paarup HM, et al. Hearing loss in relation to sound exposure of professional symphony orchestra musicians. Ear Hear. 2014;35(4):448–460. doi:10.1097/AUD.0000000000000029
36. Amorim MI, Jorge AI. Association between temporomandibular disorders and music performance anxiety in violinists. Occup Med. 2016;66(7):558–563. doi:10.1093/occmed/kqw080
37. Bourne D, Hallaran A, Mackie J. The lived experience of orchestral string musicians with playing related pain. Med Probl Perform Art. 2019;34(4):198–204. doi:10.21091/mppa.2019.4031
38. Altenmuller E, Jabusch HC. Focal dystonia in musicians: phenomenology, pathophysiology, triggering factors, and treatment. Med Probl Perform Art. 2010;25(1):3–9. doi:10.21091/mppa.2010.1002
39. Spahn C, Richter B, Altenmüller E. MusikerMedizin: Diagnostik, Therapie Und Prävention von Musikerspezifischen Erkrankungen [Musicianmedicine: Diagnostics, Therapy and Prevention of Musician-Associated Diseases]. Schattauer; 2010. German.
40. Kovero O, Kononen M. Signs and symptoms of temporomandibular disorders and radiologically observed abnormalities in the condyles of the temporomandibular joints of professional violin and viola players. Acta Odontol Scand. 1995;53(2):81–84. doi:10.3109/00016359509005951
41. Myint CW, Rutt AL, Sataloff RT. Fiddler’s neck: a review. Ear Nose Throat J. 2017;96(2):76–79. doi:10.1177/014556131709600210
42. Hanon S, Ronge R, Potvin M, Schuermans D, Vincken W. Occupational asthma due to colophony in a violin player. J Allergy Clin Immunol Pract. 2014;2(5):624–625. doi:10.1016/j.jaip.2014.06.018
43. Lieberman HD, Fogelman JP, Ramsay DL, Cohen DE. Allergic contact dermatitis to propolis in a violin maker. J Am Acad Dermatol. 2002;46(2):S30–31. doi:10.1067/mjd.2002.106349
44. Knierim C, Goertz W, Reifenberger J, Homey B, Meller S. Fiddler’s neck. Hautarzt. 2013;64(10):724–726. doi:10.1007/s00105-013-2647-5
45. Buckley DA, Rogers S. ‘Fiddler’s fingers’: violin-string dermatitis. Contact Dermatitis. 1995;32(1):46–47. doi:10.1111/j.1600-0536.1995.tb00841.x
46. Alvarez MS, Brancaccio RR. Multiple contact allergens in a violinist. Contact Dermatitis. 2003;49(1):43–44. doi:10.1111/j.0105-1873.2003.0120c.x
47. Caero JE, Cohen PR. Fiddler’s neck: chin rest-associated irritant contact dermatitis and allergic contact dermatitis in a violin player. Dermatol Online J. 2012;18(9):10. doi:10.5070/D30T23P44W
48. Lederman RJ. Primary bowing tremor: a task-specific movement disorder of string instrumentalists. Med Probl Perform Art. 2012;27(4):219–223. doi:10.21091/mppa.2012.4040
49. Denk-Linnert DM, Farneti D, Nawka T, et al. Position Statement of the Union of European Phoniatricians (UEP): fees and phoniatricians’ role in multidisciplinary and multiprofessional dysphagia management team. Dysphagia. 2023;38(2):711–718. doi:10.1007/s00455-022-10502-9
50. Macdonell RA, Dewey HM. Neurological disability and neurological rehabilitation. Med J Aust. 2001;174(12):653–658. doi:10.5694/j.1326-5377.2001.tb143482.x
51. Warrington J. Hand therapy for the musician: instrument-focused rehabilitation. Hand Clin. 2003;19(2):287–301, vii. doi:10.1016/s0749-0712(02)00095-1
52. Lee A, Chadde M, Altenmüller E, Schoonderwaldt E. Characteristics of task-specific tremor in string instrument players. Tremor Other Hyperkinet Mov. 2014;4:198. doi:10.7916/D86Q1V9W
53. Sacks O. Musicophilia: Tales of Music and the Brain. Knopf Canada; 2007.
54. Kozlowski E, Zera J, Mlynski R. Effect of musician’s earplugs on sound level and spectrum during musical performances. Int J Occup Saf Ergon. 2011;17(3):249–254. doi:10.1080/10803548.2011.11076890
55. Blum J, Ritter G. Violinists and violists with masses under the left side angle of the jaw known as “fiddler’s neck”. Med Probl Perform Art. 1990;5(4):155–160.
56. Steinmetz A, Ridder PH, Methfessel G, Muche B. Professional musicians with craniomandibular dysfunctions treated with oral splints. Cranio. 2009;27(4):221–230. doi:10.1179/crn.2009.033
57. Yang N, Fufa DT, Wolff AL. A musician-centered approach to management of performance-related upper musculoskeletal injuries. J Hand Ther. 2021;34(2):208–216. doi:10.1016/j.jht.2021.04.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.