Back to Journals » Clinical Ophthalmology » Volume 19
Flutter Sign – An Indicator of Intact Anterior Hyaloid Face After Posterior Capsule Rupture During Phacoemulsification
Authors Om Parkash R, Om Parkash T ![]() , Sharma T
, Sharma T ![]() , Vajpayee RB
, Vajpayee RB ![]() , Megur D, Patwardhan SD, Desai A, Tassignon MJ
, Megur D, Patwardhan SD, Desai A, Tassignon MJ
Received 10 August 2025
Accepted for publication 18 November 2025
Published 26 November 2025 Volume 2025:19 Pages 4313—4321
DOI https://doi.org/10.2147/OPTH.S559799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Supplementary video of “Flutter Sign during Phacoemulsification” [559799]
Views: 348
Rohit Om Parkash,1 Tushya Om Parkash,1 Trupti Sharma,2 Rasik Behari Vajpayee,3 Deepak Megur,4 Sourabh D Patwardhan,5 Abhijeet Desai,6 Marie-José Tassignon7
1Department of Cataract Surgery, Dr Om Parkash Eye Institute, Amritsar, Punjab, India; 2Department of Cataract Surgery, Dr Om Parkash Eye Institute, Pathankot, Punjab, India; 3Vision Eye Institute Melbourne; Royal Victorian Eye and Ear Hospital, University of Melbourne, Melbourne, VIC, Australia; 4Megur Eye Centre, Bidar, Karnataka, India; 5Nandadeep Eye Hospital, Sangli, Maharashtra, India; 6Sohum Eye Care Centre, a Unit of Dr Agarwals Eye Hospital, Mumbai, MH, India; 7Department of Ophthalmology, University of Antwerp, VAN, Belgium; Department of Ophthalmology, University Hospital VUB Brussels, Brussels, Belgium
Correspondence: Tushya Om Parkash, Email [email protected]
Purpose: To describe the intraoperative Flutter Sign as a real-time indicator of anterior hyaloid face (AHF) integrity following posterior capsule tear (PCT) during phacoemulsification.
Design: Single-centre observational study combining retrospective review of twelve intraoperative PCT cases with prospective evaluation of eight additional cases. Retrospective observations guided structured assessment in the prospective arm, focusing on PCT edge behaviour and AHF integrity.
Methods: Surgical videos of twelve eyes with intraoperative PCT were analysed for tear edge morphology and motility. Based on these findings, eight prospectively observed PCT cases were examined intraoperatively for edge behaviour and AHF status. Additional parameters included need for vitreous surgery, type of intraocular lens (IOL) implanted, and intraoperative and postoperative complications associated with PCT.
Results: Eleven eyes demonstrated sharp, fluttering PCT edges with intact AHF, no vitreous prolapse, and no need for anterior vitrectomy. Of these, five received in-the-bag IOLs, while six underwent sulcus fixation. All achieved a best corrected visual acuity (BCVA) of 20/20. Nine eyes exhibited scalloped, non-fluttering edges, consistent with AHF rupture and vitreous prolapse. All required anterior vitrectomy and sulcus-fixated IOLs. Three patients in this group experienced posterior migration of lens material: two had small cortical or nuclear fragments that were clinically insignificant and required no intervention, while one patient had a large nuclear fragment that necessitated a secondary procedure for removal. BCVA was reduced in two eyes to 20/30. Two patients experienced transient elevation of intraocular pressure. No cases of retinal detachment or endophthalmitis were observed.
Conclusion: The Flutter Sign is a simple, dye-free, real-time indicator of AHF integrity after PCT, with fluttering edges signifying intact AHF and scalloped static edges indicating vitreous prolapse.
Keywords: anterior hyaloid face, posterior capsule tear, vitreous body, phacoemulsification, cataract extraction, intraoperative complications, Flutter Sign
Introduction
Posterior capsule tear (PCT) remains one of the most significant intraoperative complications during phacoemulsification and can adversely affect visual outcomes.1 Importantly, PCT and vitreous prolapse are separate events; a tear in the posterior capsule does not necessarily result in vitreous loss. Vitreous prolapse occurs only when the anterior hyaloid face (AHF) is breached.
Determining the status of the AHF is central to PCT management, as its integrity dictates the risk of vitreous prolapse, guides intraoperative strategy, and influences surgical outcomes.2
Many techniques have been described to assess the integrity of AHF during phacoemulsification surgery. These include Intraoperative Optical Coherence Tomography(OCT),3,4 triamcinolone staining and observing the spread of ophthalmic viscosurgical devices (OVDs) into Berger’s space.5,6 Of all these modalities, staining by Triamcinolone is most commonly used by ophthalmic surgeons to diagnose disruption of AHF, presence of vitreous strands in the anterior chamber, vitreous attachment to the posterior capsular flap, and deformation of capsule margin.7 However, none of these signs and techniques provide real-time assessment of intact nature of AHF.
A critical gap in current practice is the lack of a simple, reliable, and immediately visible intraoperative sign that identifies both the integrity of the AHF and the precise moment of its rupture, when vitreous prolapse begins and surgical steps must be promptly modified.
We introduce the Flutter Sign as a novel intraoperative indicator of AHF integrity, based on two distinct visual characteristics of the PCT edges during phacoemulsification: morphology and motility. When the AHF is intact, PCT edges appear sharp and well-defined, exhibiting a characteristic fluttering motion in response to irrigation currents. In contrast, rupture of the AHF with vitreous prolapse results in scalloped, non-fluttering edges that appear static.
This simple, dye-free, and equipment-independent sign provides surgeons with an immediate, real-time assessment of anterior hyaloid face integrity during posterior capsule tear, enabling timely adjustment of surgical strategy to maintain control, minimize complications, and improve patient safety.
The Flutter Sign, as described in our study, is distinct from the flap motility sign that we previously reported for anterior capsular tears.8 In that work, pre-equatorial tears exhibited everted, fluttering flaps, whereas post-equatorial extension resulted in inverted, non-fluttering flaps. By contrast, the Flutter Sign pertains to PCT and reflects the status of the AHF. Here, the morphology and motility of the PCT edges are determined by the integrity of the AHF.
Materials and Methods
This was a single-centre ambidirectional study of patients who experienced PCT during phacoemulsification. The retrospective arm included 12 cases operated between November 2019 and March 2022, and the prospective arm comprised 8 cases evaluated between April 2022 and March 2025. The study was approved by the Institutional Ethics Committee of Dr. Om Parkash Eye Institute (Approval No. DOPEI/EC/ASR/10-2022) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from all participants.
Patient demographics (age, sex, laterality, axial length, and lens hardness grading using the Lens Opacities Classification System III (LOCS III)) were recorded.
Inclusion criteria were eyes undergoing phacoemulsification complicated by PCT, with complete video documentation and clear visualization of the PCT and AHF. Exclusion criteria were incomplete or poor-quality videos, small pupils requiring mechanical dilation, traumatic cataracts, prior vitreoretinal surgery, or combined anterior/posterior segment procedures.
For the retrospective arm, surgical videos of 12 PCT cases were retrieved from the archive. Only cases with adequate clarity allowing assessment of the PCT and AHF were included. Videos were reviewed for PCT edge morphology (sharp vs scalloped), motility (fluttering vs non-fluttering), and evidence of vitreous prolapse.
For the prospective arm, eight consecutive PCT cases were evaluated intraoperatively. Real-time assessment was performed under the operating microscope, with systematic documentation of PCT edge morphology, motility, and vitreous status at the time of surgery. Post-operatively the detailed review of the videos was done for PCT edge morphology, motility and state of vitreous.
Additional parameters in both groups included the need for anterior vitrectomy, type of intraocular lens (IOL) implanted (in-the-bag vs sulcus-fixated), and intraoperative or postoperative complications.
All surgeries were performed under topical anesthesia using the Centurion® Vision System (Alcon Laboratories, Inc., Fort Worth, TX, USA). Low Intraocular pressure (IOP) settings were routinely used. When a PCT was identified, surgery was paused and the tear edges observed. The phaco tip was not withdrawn. Subsequent steps were guided by PCT morphology and motility: if the edges were sharp and fluttering, phacoemulsification was continued; if scalloped and immobile, anterior vitrectomy was performed.
When the edges appeared sharp and fluttering, consistent with an intact AHF, surgery was continued (Figures 1 and 2).
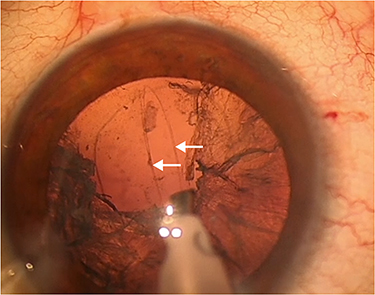 |
Figure 1 Surgical photograph demonstrating sharp, fluttering posterior capsular tear edges, indicating an intact anterior hyaloid face without vitreous prolapse. |
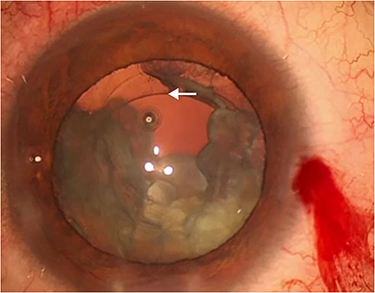 |
Figure 2 Surgical photograph demonstrating non-fluttering, scalloped posterior capsular tear edges, consistent with rupture of the anterior hyaloid face and associated vitreous prolapse. |
Measures to prevent AHF rupture were applied. IOP settings were reduced further to allow slow-motion phacoemulsification minimizing turbulence. Chamber stability was maintained, and fluctuations such as over-deepening or shallowing of the anterior chamber were avoided. Nuclear manipulations were gentle, with guarded and minimal rotation to reduce stress on the AHF. PCT edges were continuously observed in real time to assess AHF integrity (Figure 3a and b) (Figure 4a and b). The presence of the Flutter Sign allowed the surgery to continue conservatively, without initiating anterior vitrectomy or making further changes to the surgical parameters. Under these conditions, the intact AHF helped compartmentalize the vitreous and maintain stability in the posterior segment throughout the procedure.
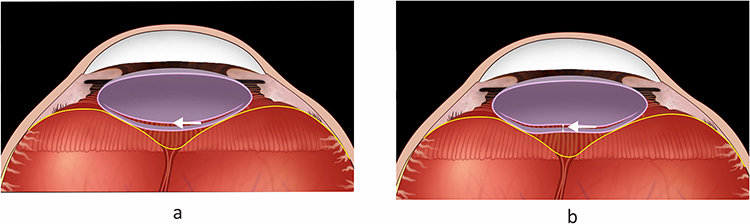 |
Figure 3 Diagrammatic sequence illustrating the “Flutter Sign”. Initial and shifted positions of sharp posterior capsular tear edges demonstrate fluttering movement indicating an intact anterior hyaloid face. (a) Diagrammatic representation showing the initial position of sharp posterior capsular tear edges, indicating an intact anterior hyaloid face. (b) Diagrammatic representation showing a shifted position of the same sharp posterior capsular tear edges, demonstrating fluttering and indicating an intact anterior hyaloid face. |
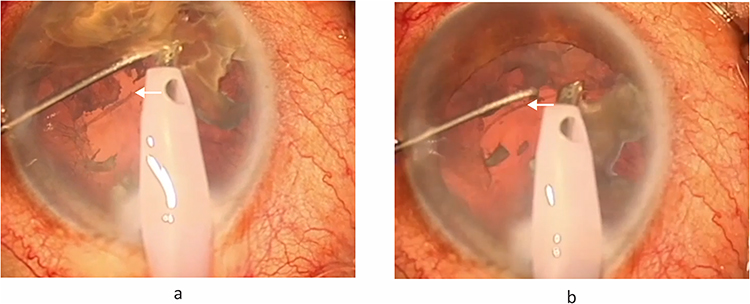 |
Figure 4 Surgical video stills demonstrating the “Flutter Sign”. Intraoperative views showing the dynamic movement of sharp posterior capsular tear edges confirming an intact anterior hyaloid face under stable, low-fluidic conditions. (a) Surgical video still showing the initial position of sharp posterior capsular tear edges, indicating an intact anterior hyaloid face. (b) Surgical video still showing the same sharp posterior capsular tear (PCT) edges in a shifted position, demonstrating fluttering that indicates an intact anterior hyaloid face (AHF). Small nuclear fragments can be seen freely floating in the anterior chamber under stable, low-fluidic conditions, confirming the absence of vitreous prolapse or retained lens material. |
The PCT edges were monitored continuously for any change in morphology or motility. At the end of slow-motion nuclear emulsification, particular care was taken to maintain stable chamber dynamics to avoid rupture of the AHF. OVD was injected through the side port incision to maintain to maintain anterior chamber stability and tamponade the PCT before withdrawing the phaco handpiece from the anterior chamber., ensuring minimal fluctuation, preventing chamber collapse, and avoiding any stress to the integrity of the AHF.
During irrigation and aspiration (IA), low IOP settings were continued. Bimanual IA or sleeve-retracted coaxial IA was used to create two separate I&A planes, reducing turbulence near the posterior capsule. In select cases, dry aspiration was employed to further limit fluid movement and preserve AHF integrity.
Thereafter, the PCT edges were evaluated. When the end point of tear edges were clearly visible, a posterior capsulorhexis was performed to round them off. This facilitated in-the-bag IOL implantation.
When the PCT edges appeared scalloped and non-fluttering, indicating AHF rupture with vitreous prolapse (Figure 5a and b), the surgical approach was modified to minimize further vitreous disturbance. The handpiece was not removed from the anterior chamber, as removal without stabilization could have extended the PCT and caused vitreous loss. The anterior chamber was first stabilized by injecting a viscodispersive OVD. Once IOP was equilibrated, the phaco tip was withdrawn.
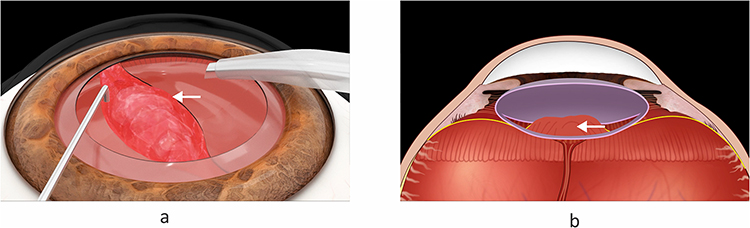 |
Figure 5 Diagrammatic representation of anterior hyaloid face rupture. Non-fluttering, scalloped posterior capsular tear edges with anterior vitreous herniation indicating rupture of the anterior hyaloid face. (a) Diagrammatic representation of non-fluttering, scalloped posterior capsular tear edges, indicating rupture of the anterior hyaloid face with vitreous prolapse. (b) Diagrammatic representation showing anterior herniation of vitreous through the posterior capsular tear edges. |
Triamcinolone acetonide (0.1 mL of 40 mg/mL) was injected into the anterior chamber to confirm the presence or absence of vitreous strands. The presence of OVD, however, limited complete binding of triamcinolone particulates with vitreous strands.
Anterior vitrectomy was then performed through two side-port incisions created at the limbus. Pars plana vitrectomy helps to prevent extension of PCT with vitreous prolapse. However, in our limbal approach of vitrectomy was used. The vitreous cutter was directed posteriorly at the level of PCT to prevent tear extension.
In cases where nuclear fragments had to be managed in the presence of AHF rupture and vitreous prolapse, an IOL scaffold was used to prevent posterior migration of the fragments. The IOL was implanted in the sulcus, and optic capture was performed when the capsulorhexis size permitted.
Post operatively, the patients were managed with close follow ups for inflammation, intraocular pressure, and for any retained lenticular particles.
With modern phacoemulsification techniques, PCT is a relatively uncommon complication. Accordingly, the sample size in this study was determined by case availability rather than by formal statistical calculation. All consecutive cases meeting strict inclusion criteria over a 5-year period were included. This approach was appropriate for an observational, proof-of-concept study aimed at describing the novel Flutter Sign rather than establishing prevalence estimates. The authors acknowledge that these preliminary findings warrant validation in larger, multicentric studies.
Descriptive statistics and Fisher’s exact test/Chi-square test were used where applicable, and results are interpreted in the context of a hypothesis-generating study. Although p-values did not reach statistical significance, the observed trends indicate clinically meaningful patterns worth further exploration. Since this was an observational, ambidirectional study of consecutive real-world cases, a priori power calculation was not feasible due to the unpredictable incidence of PCT with adequate documentation.
Results
A total of 20 eyes with intraoperative PCT during phacoemulsification were included in this study. The retrospective arm, comprising 12 cases, was conducted from November 2019 to March 2022, while the prospective arm, consisting of 8 cases, was evaluated from April 2022 to March 2025.
Preoperatively, the parameters recorded included age, sex, laterality, axial length, and lens hardness graded using the Lens Opacities Classification System III (LOCS III). The mean age was 61.2 years in the AHF Intact group and 61.7 years in the AHF Rupture group. Laterality distribution showed 12 right eyes (60%) and 8 left eyes (40%). The overall cohort comprised 11 males and 9 females. The mean axial length was 23.33 ± 1.44 mm, and the mean cataract grade (LOCS III) was 3.15 ± 1.35. Of the six patients with posterior polar cataracts, two exhibited no nuclear sclerosis.
Based on intraoperative findings, eleven eyes demonstrated sharp, fluttering PCT edges and were categorized as the AHF Intact group, while the remaining nine showed scalloped, non-fluttering PCT edges, constituting the AHF Rupture group.
In the AHF intact group, IOL implantation was completed in the capsular bag in five cases and in the sulcus in six, whereas sulcus fixation was necessary in all AHF Rupture cases.
Postoperative management varied between the two groups. Patients in the AHF intact group followed a standard regimen with routine monitoring of inflammation, intraocular pressure, and visual recovery. As vitreous prolapse and posterior segment complications were absent, follow-up was less intensive, and recovery was rapid and uneventful. In contrast, the AHF rupture group required closer observation, with management focused on inflammation control, intraocular pressure stabilization, and detection of retained lens material or other posterior segment complications.
All patients in the AHF Intact group achieved postoperative visual acuity of 20/20 and did not require anterior vitrectomy. In contrast, two patients in the AHF Rupture group had visual acuity of 20/30, one with cystoid macular oedema (CME) and the other with sub clinical macular oedema. Transient elevation in intraocular pressure occurred in two eyes with vitreous prolapse.
Three patients in the AHF Rupture group experienced posterior migration of lens material: two had small cortical or nuclear fragments that were clinically insignificant and required no intervention, while one patient had a large nuclear fragment necessitating a secondary removal procedure. No such posterior migrations were noted in the AHF Intact group.
A comparison of the clinical and surgical outcomes is summarized in Table 1.
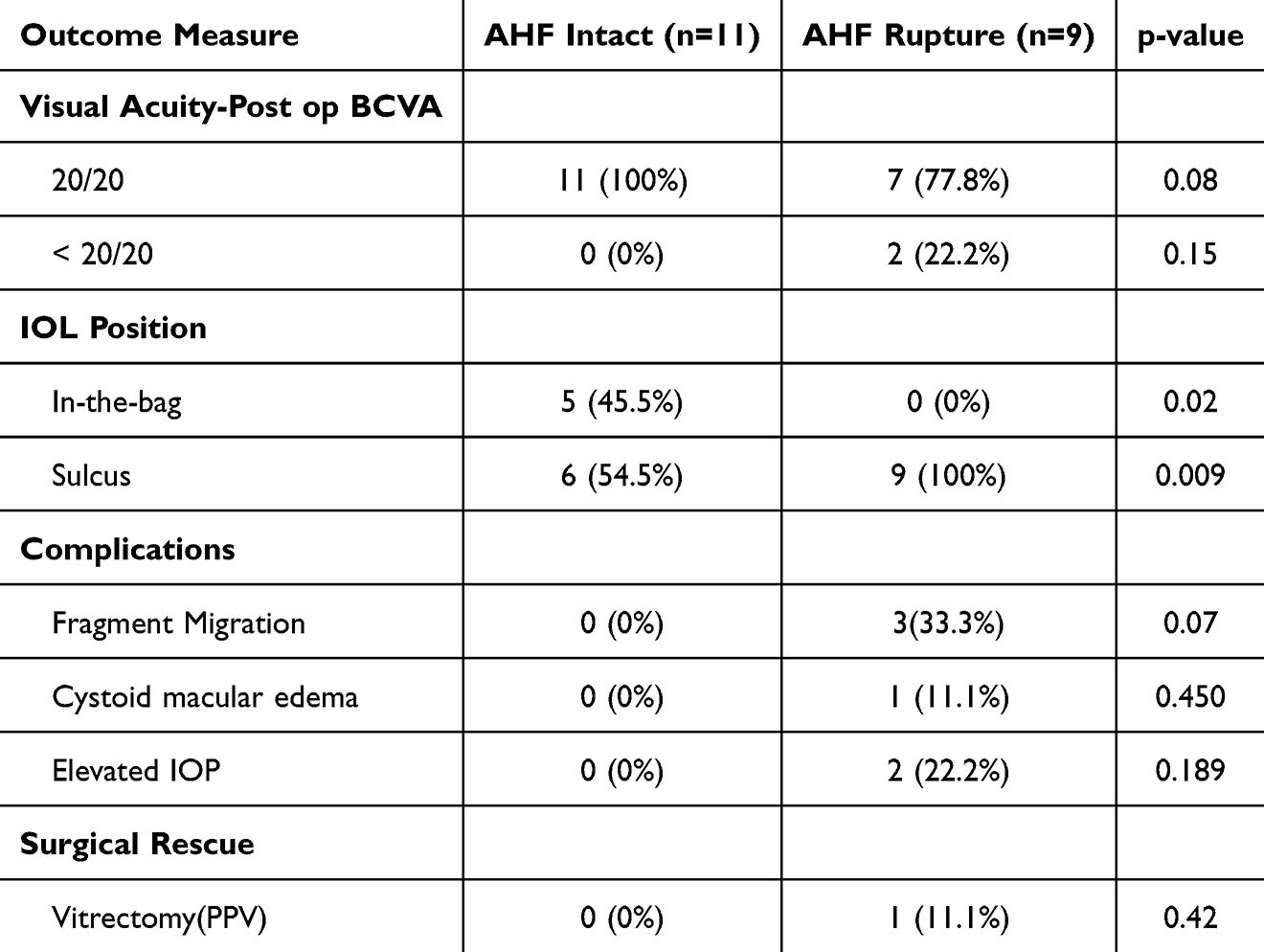 |
Table 1 Comparative Outcomes by AHF Status |
Postoperative best-corrected visual acuity (BCVA) of 20/20 was achieved in all eyes in the AHF Intact group compared to 77.8% in the AHF Rupture group; however, this difference did not reach statistical significance (p = 0.08). Sulcus fixation of the IOL was required in all cases in the AHF Rupture group, whereas 45.5% of the AHF Intact group received in-the-bag fixation (p = 0.009).
Posterior migration of lens fragments occurred exclusively in the AHF Rupture group (33.3% vs 0%), a difference that approached but did not achieve statistical significance (p = 0.07). CME was observed in one patient (11.1%) in the AHF Rupture group and in none of the AHF Intact eyes (p = 0.450). Transient postoperative elevation in intraocular pressure was noted in 22.2% of AHF Rupture eyes, while no such events occurred in the AHF Intact group (p = 0.189). Pars plana vitrectomy was required in one AHF Rupture case (11.1%) and in none of the AHF Intact eyes (p = 0.42).
Although none of the differences reached statistical significance, the observed trends suggest clinically meaningful patterns that merit further exploration.
Our findings demonstrate that AHF integrity is a critical determinant of surgical success in PCT management, underscoring the importance of AHF-preserving surgical strategies, such as low-flow phacoemulsification and anterior vitreous stabilization.
Discussion
PCT during phacoemulsification poses a critical intraoperative challenge and is relatively common, with significant implications for postoperative outcomes. Timely recognition and appropriate intraoperative decision-making are crucial, particularly with regard to preserving the integrity of the AHF. This delicate transparent membrane serves as an important barrier to vitreous prolapse and plays a central role in maintaining posterior segment compartmentalization following PCT.
An intact AHF is consistently associated with more favourable outcomes than when it is ruptured and vitreous prolapses.9–11
AHF rupture may result from the combined effect of mechanical stress and intraocular fluid dynamics during surgery. Risk factors include engagement of vitreous by the phacoemulsification tip, instability or shallowing of the anterior chamber, and elevated fluidic parameters such as high bottle height or IOP. These conditions can transmit disruptive forces to the anterior vitreous face, leading to rupture and subsequent vitreous prolapse.
Several intraoperative signs have been described to aid in recognizing AHF rupture, such as sudden deepening of the anterior chamber, the pupillary snap sign, unusual nuclear followability, nuclear tilt, brightening or loss of the red reflex, web-like striae, and direct visualization of a capsular defect.12–20 Additional clues include difficulty in cortical aspiration and a trampoline-like posterior capsule. However, these signs are indirect, often appearing after AHF rupture has occurred. Triamcinolone staining, though useful, is not a real-time indicator and disrupts surgical flow. As such, a reliable, intraoperative, real-time method to confirm AHF integrity remains an unmet need.
Richard Packard suggested that a sharp-edged PCT may indicate an intact AHF, while a scalloped edge may suggest rupture and vitreous prolapse.21
Building on this principle, we describe the Flutter Sign as a direct, real-time intraoperative indicator of AHF integrity. The sign is based on the visual behaviour of the PCT edges under irrigation during phacoemulsification. When the AHF is intact, irrigation currents circulate freely through the PCT into Berger’s space causing the tear edges to flutter visibly, their sharp margins reflecting the absence of vitreous contact. Once the AHF ruptures, herniating vitreous dampens fluid movement, abolishes fluttering, and produces a scalloped, static contour.
Timely recognition of the Flutter Sign allows the surgeon to distinguish between an intact and breached AHF in real time, guiding intraoperative decision-making. When fluttering is present, the surgeon may cautiously proceed with the planned steps while employing AHF-preserving techniques. Surgical strategies that help preserve AHF integrity include maintaining anterior chamber stability, avoiding sudden withdrawal of instruments, using low-flow and low-vacuum settings, applying low IOP or a low bottle height to minimize turbulence, and mobilizing nuclear material gently to reduce capsular stress. The sudden cessation of fluttering, accompanied by scalloped edges, signals AHF rupture and the need to modify the surgical approach to prevent further complications.
The Flutter Sign should be distinguished from the flap motility sign previously described by Om Parkash et al for anterior capsular tears. While the Flutter Sign is used to evaluate anterior hyaloid face integrity, the flap motility sign was designed to assess the extent of anterior capsular tears, with pre-equatorial tears showing everted, fluttering flaps and post-equatorial extension resulting in inverted, non-fluttering flaps.
In this series, retrospective video analysis consistently associated sharp fluttering PCT edges with an intact AHF and non-fluttering, scalloped edges with rupture. These observations prompted a prospective evaluation, which confirmed the reproducibility and clinical utility of the Flutter Sign.
Our findings also support the routine use of low fluidic parameters during phacoemulsification to preserve AHF integrity.22 Lower infusion rates and reduced turbulence limit mechanical stress on the AHF, thereby increasing the likelihood of its preservation in the event of PCT. This AHF-friendly environment reduced the risk of vitreous prolapse and allows surgery to proceed more safely, reinforcing that PCT and AHF rupture are not obligatorily linked events.
These results underscore the importance of surgical strategies that preserved AHF integrity during PCT management, such as low-flow phacoemulsification and anterior vitreous stabilization. They also highlight the value of real-time intraoperative indicators for early detection of AHF rupture and safer surgical decision-making.
Eyes with ruptured AHF required an immediate change in operative strategy, more intensive postoperative surveillance, reflecting their greater susceptibility to inflammation, IOP fluctuations, and vitreous-related complications.
The power of this study lies in its novelty and clinical applicability. It introduces a simple, reproducible, and equipment independent intraoperative sign derived from real surgical scenarios. The inclusion of both retrospective and prospective arms adds methodological strength and provides an early but reliable foundation for future validation through larger, multicentric studies.
Limitations and Recommendations
This study has certain limitations. The retrospective component and relatively small sample size may limit generalizability. As a single-centre study, observer bias cannot be excluded. The assessment of “fluttering” versus “non-fluttering” PCT edges was partly subjective despite standardized evaluation. Long-term outcomes were not assessed. Future multicentric studies with larger cohorts and objective validation methods are warranted.
What This Study Adds
This study introduces the Flutter Sign as a novel, real-time, dye-free intraoperative indicator of anterior hyaloid face integrity during posterior capsule tear. It bridges an important gap by offering surgeons an immediate, equipment-independent method to distinguish intact from ruptured AHF, guiding safer intraoperative decisions and improving surgical awareness during cataract surgery.
Conclusion
The Flutter Sign offers a simple, dye-free, real-time method to differentiate between intact and ruptured AHF, aiding safer intraoperative decision-making. While findings are promising, they represent preliminary observations that warrant validation through larger, multicenter studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Marie-José Tassignon reports a patent Bag-in-the-lens design with royalties paid to Morcher. The authors report no other conflicts of interest in this work.
References
1. Johansson B, Lundström M, Montan P, Stenevi U, Behndig A. Capsule complication during cataract surgery: long-term outcomes: Swedish capsule rupture study group report 3. J Cataract Refract Surg. 2009;35(10):1694–1698. doi:10.1016/j.jcrs.2009.05.027
2. Thanigasalam T, Sahoo S, Ali MM. Posterior capsule rupture with/without vitreous loss during phacoemulsification in a hospital in Malaysia. Asia Pac J Ophthalmol. 2015;4(3):166–170. doi:10.1097/APO.0000000000000056
3. Tassignon MJ, Ní Dhubhghaill S. Real-time intraoperative optical coherence tomography imaging confirms older concepts about the Berger space. Ophthalmic Res. 2016;56(4):222–226. doi:10.1159/000446242
4. Vael A, Van Os L, Melis K, Tassignon MJ. Evaluation of the vitreolenticular interface with intraoperative OCT. J Cataract Refract Surg. 2022;48(7):826–830. doi:10.1097/j.jcrs.0000000000000866
5. Sudhalkar AA, Praveen MR, Vasavada VA, et al. Subtle signs of an intact anterior vitreous face during pediatric cataract surgery. J Cataract Refract Surg. 2012;38(9):1690–1693. doi:10.1016/j.jcrs.2012.07.016
6. O’hEineachain R, Tassignon MJ. It’s in the bag. EuroTimes. 2024;29(Feb):20–21.
7. Praveen MR, Vasavada AR, Koul A, Trivedi RH, Vasavada VA, Vasavada V. Subtle signs of anterior vitreous face disturbance during posterior capsulorhexis in pediatric cataract surgery. J Cataract Refract Surg. 2008;34(1):163–167. doi:10.1016/j.jcrs.2007.08.039
8. Om Parkash R, Mahajan S, Biala V, Om Parkash T, Tasneem AF. Flap motility as a sign of posterior capsule rupture in peripherally extended anterior capsular tears. Clin Ophthalmol. 2017;11:1445–1451. doi:10.2147/OPTH.S136532
9. Chan FM, Mathur R, Ku JJ, et al. Short-term outcomes in eyes with posterior capsule rupture during cataract surgery. J Cataract Refract Surg. 2003;29(3):537–541. doi:10.1016/S0886-3350(02)01622-X
10. Tan JH, Karwatowski WS. Phacoemulsification cataract surgery and unplanned anterior vitrectomy—is it bad news? Eye. 2002;16(1):117–120. doi:10.1038/sj.eye.6700084
11. Ozyol E, Ozyol P, Erdoğan BD, Onen M. The role of anterior hyaloid face integrity on retinal complications during Nd: YAG laser capsulotomy. Graefes Arch Clin Exp Ophthalmol. 2014;252(1):71–75. doi:10.1007/s00417-013-2526-x
12. Kim SS, Davidson MG. Anterior chamber deepening as a sign of posterior capsule rupture during cataract surgery. J Cataract Refract Surg. 2008;34(1):123–125. doi:10.1016/j.jcrs.2007.08.042
13. Yeoh R. The pupillary snap sign: a clinical sign indicative of posterior capsular rupture and possible vitreous disturbance. J Cataract Refract Surg. 2002;28(10):1983–1985. doi:10.1016/S0886-3350(02)01424-4
14. Oshima Y, Emi K, Motokura M. Sudden sinking of nuclear fragments: a warning sign of zonular dialysis or posterior capsule rupture. Ophthalmic Surg Lasers. 1999;30(5):386–389.
15. Davison JA, Sanders DR, Azar R, Lamielle H. Capsule rupture with nuclear displacement: when followability fails. J Cataract Refract Surg. 2004;30(3):576–578. doi:10.1016/j.jcrs.2003.06.004
16. Osher RH. The loss of red reflex: a subtle but telling sign of posterior capsule rupture. J Cataract Refract Surg. 2007;33(7):1109–1110. doi:10.1016/j.jcrs.2007.03.055
17. Cionni RJ, Osher RH. Surgical techniques and results of intraoperative management of posterior capsule rupture. J Cataract Refract Surg. 1995;21(2):182–185. doi:10.1016/S0886-3350(13)80581-3
18. Chang DF. Managing residual lens material after posterior capsular rupture. Cataract Refract Surg Today. 2003;56–58.
19. Osher RH, Yu BC, Koch DD. Posterior polar cataracts: a predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16(2):157–162. doi:10.1016/S0886-3350(13)80724-9
20. Vajpayee RB, Sharma N, Dada T, Gupta V, Dada VK, Dada VK. Posterior capsular tears. Surv Ophthalmol. 2001;45(6):473–488. doi:10.1016/S0039-6257(01)00191-6
21. McGrath D, Packard R. When posterior capsule rupture strikes. EuroTimes. 2021. Available from: https://www.escrs.org/eurotimes/when-posterior-capsule-rupture-strikes.
22. Vasavada V, Srivastava S, Vasavada V, Vasavada AR, Sudhalkar A, Bilgic A. Impact of fluidic parameters during phacoemulsification on the anterior vitreous face behavior: experimental study. Indian J Ophthalmol. 2019;67(12):1634–1637. doi:10.4103/ijo.IJO_1840_18
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Efficacy of Combined Phacoemulsification and iStent Inject versus Combined Phacoemulsification and Hydrus Microstent
Chee WK, Yip VCH, Tecson IO, Chua CH, Ang BCH, Kee AR, Hu JY, Kan TCJ, Yip LWL
Clinical Ophthalmology 2023, 17:1151-1159
Published Date: 14 April 2023
Risk Factors for Intraocular Lens Dislocation Requiring Surgical Intervention After Initial Phacoemulsification Cataract Surgery
Karimaghaei S, Shakarchi AF, Shakarchi FF, Chandra A, Soliman MK, Elhusseiny AM, Sallam AB
Clinical Ophthalmology 2026, 20:542807
Published Date: 14 April 2026