Back to Journals » Clinical Ophthalmology » Volume 20
Risk Factors for Intraocular Lens Dislocation Requiring Surgical Intervention After Initial Phacoemulsification Cataract Surgery
Authors Karimaghaei S ![]() , Shakarchi AF, Shakarchi FF, Chandra A, Soliman MK
, Shakarchi AF, Shakarchi FF, Chandra A, Soliman MK ![]() , Elhusseiny AM, Sallam AB
, Elhusseiny AM, Sallam AB
Received 26 May 2025
Accepted for publication 17 November 2025
Published 14 April 2026 Volume 2026:20 542807
DOI https://doi.org/10.2147/OPTH.S542807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sam Karimaghaei,1 Ahmed F Shakarchi,1 Fatma F Shakarchi,1 Aman Chandra,2,3 Mohamed K Soliman,4,5 Abdelrahman M Elhusseiny,1 Ahmed B Sallam1,6
1Harvey and Bernice Jones Eye Institute, Department of Ophthalmology, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 2Mid & South Essex NHS Foundation Trust (Southend University Hospital NHS Foundation Trust), Essex, UK; 3Vision and Eye Research Institute, Anglia Ruskin University, Cambridge, UK; 4University Hospitals Eye Institute, Department of Ophthalmology and Visual Sciences, Case Western Reserve University, Cleveland, OH, USA; 5Department of Ophthalmology, Assiut University Hospitals, Faculty of Medicine, Assiut, Egypt; 6Ophthalmology Department, Ain Shams University, Cairo, Egypt
Correspondence: Ahmed B Sallam, Harvey and Bernice Jones Eye Institute, Department of Ophthalmology, University of Arkansas for Medical Sciences, 4105 Outpatient Circle, Little Rock, AR, 72205, USA, Tel +1 501 686-5150, Email [email protected]
Background/Aims: To identify pre-, intra-, and postoperative risk factors for developing IOL dislocation that required surgical intervention for IOL dislocation after an initial planned phacoemulsification cataract surgery.
Methods: A retrospective multicenter clinical database study collected over 12 years from 8 clinical centers in the United Kingdom. We included all eyes that underwent planned phacoemulsification cataract surgery. We excluded eyes that underwent planned large incision cataract surgery, were left aphakic during initial surgery and those that underwent retina or other intraocular surgery between initial cataract surgery and development of IOL dislocation. We used the Poisson model with robust approximation of variance for multivariable estimations to calculate adjusted relative risk (ARR).
Results: Of 176,572 eyes that underwent planned phacoemulsification cataract surgery, 145 (0.08%) developed IOL dislocation requiring surgery. Factors that increased the risk for developing IOL dislocation included age between 18 and 40 years (ARR = 4.5 [1.7– 12.0]), age between 40 and 60 years (ARR = 2.6 [1.6– 4.5]), male sex (ARR = 1.5 [1.1– 2.1]), pseudoexfoliation (ARR = 5.7 [3.1– 10.5]), zonular dialysis (ARR = 3.3 [1.5– 7.1]), posterior capsule rupture (PCR) (ARR = 16.4 [9.7– 27.1]), iris damage (ARR = 4.2 [1.5– 11.6]), combined phacoemulsification-pars plana vitrectomy (ARR = 3.2 [1.7– 6.2]), and YAG capsulotomy (ARR = 2.8 [1.5– 5.2]) (p < 0.05 for all).
Conclusion: This large database study quantified the risk factors for IOL dislocation after cataract surgery. This information is clinically useful for surgeons for preoperative risk stratification and surgical planning.
Keywords: intraocular lens dislocation, phacoemulsification, pseudoexfoliation, posterior capsule rupture, zonular dialysis, vitrectomy, capsulotomy
Introduction
Phacoemulsification cataract surgery is a widely performed procedure globally with excellent visual outcomes.1,2 Although not common, problems with the implanted intraocular lens (IOL) may arise that necessitate additional surgery.2 One of these complications is IOL dislocation, which generally requires surgical IOL repositioning or exchange if the patient develops visual symptoms or other secondary complications.3 Incidence of IOL subluxation/dislocation occurs in a bimodal distribution. Early dislocation, defined as occurring within 3 months of cataract surgery, is generally due to inadequate IOL fixation within a secure capsular bag. Predisposing factors include posterior capsule rupture (PCR) and zonular dialysis. Late dislocation, defined as occurring 3 or more months after an uncomplicated cataract surgery, is due to progressive zonular weakness and capsular contraction (ie, anterior capsule phimosis). Reported predisposing factors include aging, high myopia, uveitis, trauma, retinitis pigmentosa, diabetes mellitus, atopic dermatitis, connective tissue disorders, previous vitreoretinal surgery, and previous acute angle closure attack.2
To date, few large studies have analyzed the risk factors of developing IOL dislocation after cataract surgery that requires additional surgical intervention. Some risk factors identified in previous studies have included ocular co-morbidities, such as pseudoexfoliation, zonular laxity, high myopia, glaucoma, and uveitis, type of cataract, such as traumatic or brunescent, and operative factors, such as anterior vitrectomy, iris and ciliary injury, and zonular dehiscence.4–6 However, these studies are limited by choice of exclusion criteria, presence of unaccountable confounders, and small sample size. The study by Lee et al from Korea was a large population-based study; however, the authors excluded IOL dislocation events that occurred during the first postoperative week, and their analysis was adjusted only for age, sex, and preoperative variables4 Peuringer et al identified only 16 cases of IOL dislocation from 14,471 cases, and the study by Dabrowska-Kloda was a nested case–control study of only 123 eyes.5,6
The purpose of our study was to identify ocular, intraoperative, and postoperative risk factors for developing IOL dislocation that required additional surgical intervention after an initial planned phacoemulsification cataract surgery using a large clinical dataset of 176,954 eyes from 8 clinical centers. Our study is the largest in the Western hemisphere to assess the risk of IOL dislocation and addresses limitations of other studies by including a large sample size, adjusting for all analyzed variables, and including all cases of IOL dislocations from the date of initial cataract surgery. We hypothesize that a range of preoperative, intraoperative, and postoperative factors independently contribute to the risk of IOL dislocation. An understanding of risk factors has important implications for preoperative risk stratification and surgical planning.
Methods
Data
We extracted anonymized data pertaining to cataract surgery from eight UK National Health Service centers and pooled them into a single database. All centers had large ophthalmology departments with a representative mix of patients undergoing cataract surgery and used the same electronic medical record system (Medisoft Ophthalmology; Medisoft Limited). The study period spanned 12 years (July 2003 to March 2015).
The standards of care at the study sites and the data extraction process have been described in previous publications.7,8 In brief, all sites performed day-case phacoemulsification surgery. Routine postoperative care for each site included at least one visit conducted by a specialist nurse or an optometrist 4–6 weeks postoperatively. All patients received a tapering postoperative course of topical steroids and antibiotic drops for 4 weeks. This study was conducted in accordance with the Declaration of Helsinki. The Institutional Review Board of the University of Arkansas for Medical Sciences reviewed the study and deemed it not to require ethics approval as the extracted patient information was de-identified. Neither patients nor the public was involved in the design, conduct, reporting, or dissemination of this study.
Population
Our study included all eyes that underwent planned phacoemulsification cataract surgery. Eyes were grouped in those requiring second surgery for IOL dislocation and those that did not. We excluded all eyes that underwent planned intracapsular or non-phacoemulsification extracapsular cataract surgery. We excluded eyes that were left aphakic during initial surgery and underwent subsequent secondary IOL implantation. We also excluded eyes that underwent retina or other intraocular surgery in the interval between initial cataract surgery and development of IOL dislocation. Figure 1 details the filtering process that we used to reach the eligible study population.
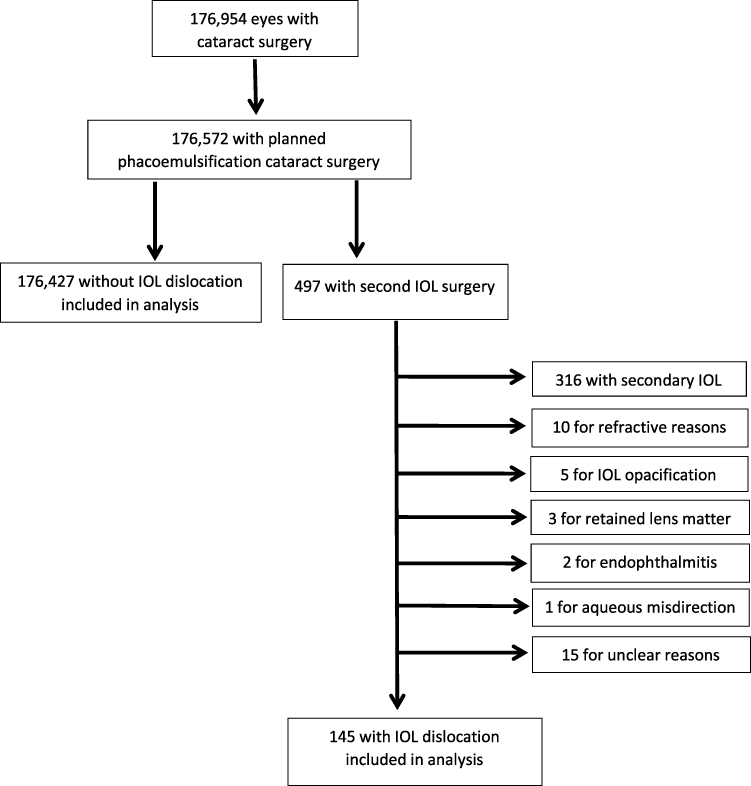 |
Figure 1 The filtration process to identify cases with intraocular lens dislocation. |
Outcomes and Covariates
We assessed the risk of requiring second surgery for a post-operative IOL dislocation for various preoperative ocular and systemic factors, intraoperative findings, and post-operative factors. Preoperative variables included patients’ demographics, diabetes status, the presence of advanced white or brunescent cataract, pupil size, diabetic retinopathy/diabetic macular edema, glaucoma, pathological myopia (defined as axial length of 26.5 mm or greater), previous trabeculectomy, retinal vein occlusion, uveitis, pseudoexfoliation, previous vitrectomy, and previous intravitreal injection.
Intraoperative factors analyzed included the use of a pupil expansion device (such as pupil rings or iris hooks), use of a capsular tension ring (CTR), zonular dialysis with or without vitreous loss, posterior capsular rupture (PCR), conversion to extracapsular extraction, iris damage, combined phacoemulsification-trabeculectomy surgery, and combined phacoemulsification-vitrectomy. Post-operative factors included YAG capsulotomy. Recording of intraoperative complications in the electronic medical record (EMR) was a compulsory field. The surgeon was mandated to record whether there were any intraoperative complications to be able to close the operation record.
Statistical Analysis
We reported the outcome variables overall and for each of the study groups. We compared categorical and continuous variables using the chi-square and analysis of variances tests. We used the Poisson model with robust estimation of standard error to calculate adjusted relative risks and multivariable linear regression to calculate adjusted differences. We calculated the relative risk (RR) and the adjusted relative risk (ARR) of developing IOL dislocation for all factors included in the analysis. We conducted the analyses using the R statistical software package version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria. www.R-project.org).
Results
Our study included 176,572 eyes that underwent planned phacoemulsification cataract surgery, 176,427 of which did not develop IOL dislocation and 145 (0.08%) of which developed IOL dislocation necessitating additional surgery. The ARR for IOL dislocation was 4.5 (1.7–12.0) for age between 18 and 40 years and 2.6 (1.6–4.5) between 40 and 60 years. The ARR for IOL dislocation with age between 60 and 80 years was not statistically significant. Male sex had a statically increased ARR for IOL dislocation at 1.5 (1.1–2.1). The rate of diabetes mellitus was equal in both groups. Table 1 displays the risk of IOL dislocation by demographic data. Among the preoperative ocular factors, the ARR of developing an IOL problem for eyes affected by pseudoexfoliation was significant, with a value of 5.7 (3.1–10.5). Table 2 displays the results for preoperative ocular factors. Figure 2 displays the rate of IOL dislocation by analyzed preoperative factor.
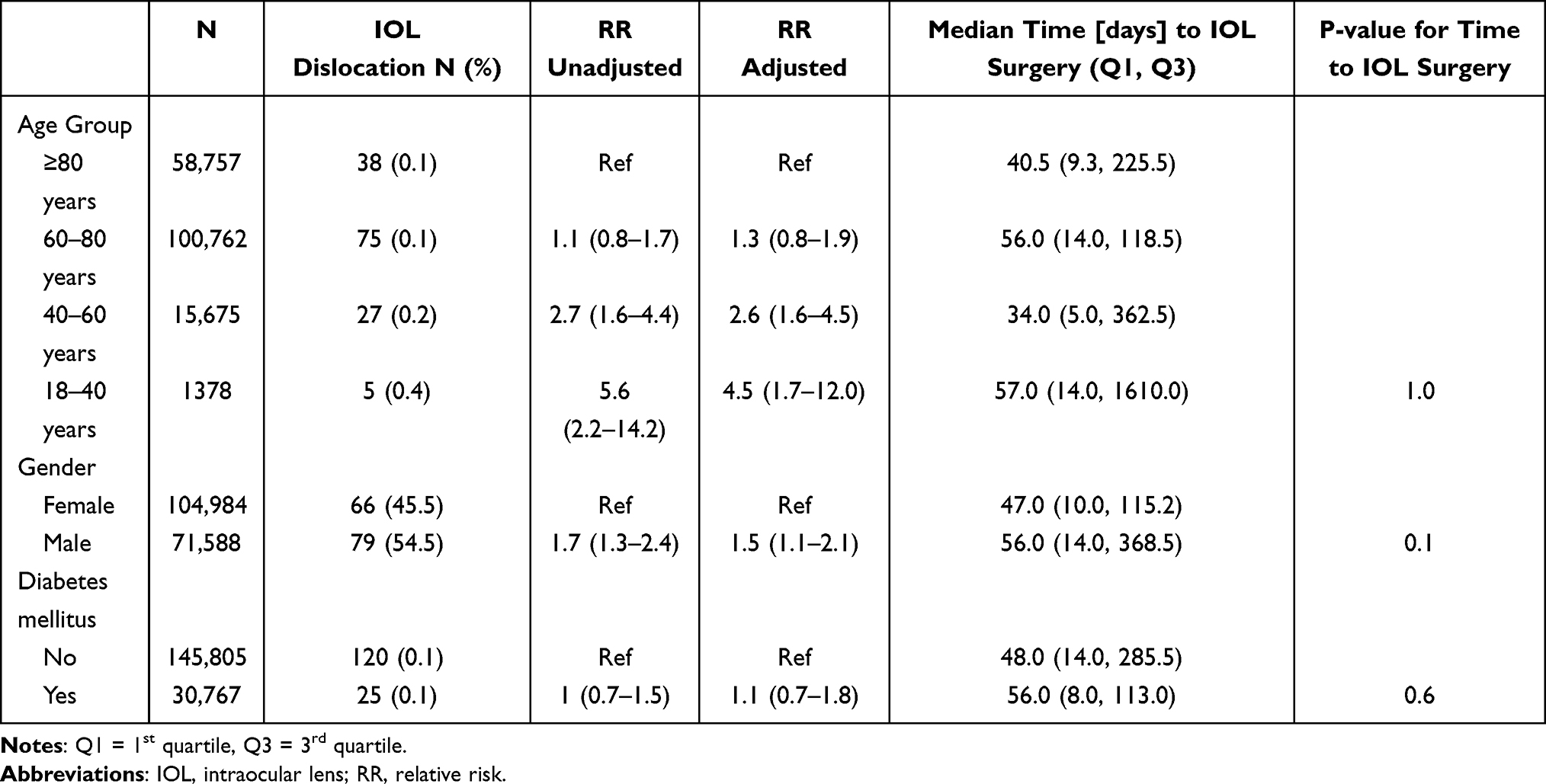 |
Table 1 Demographic Data of Patients with Intraocular Lens Dislocation |
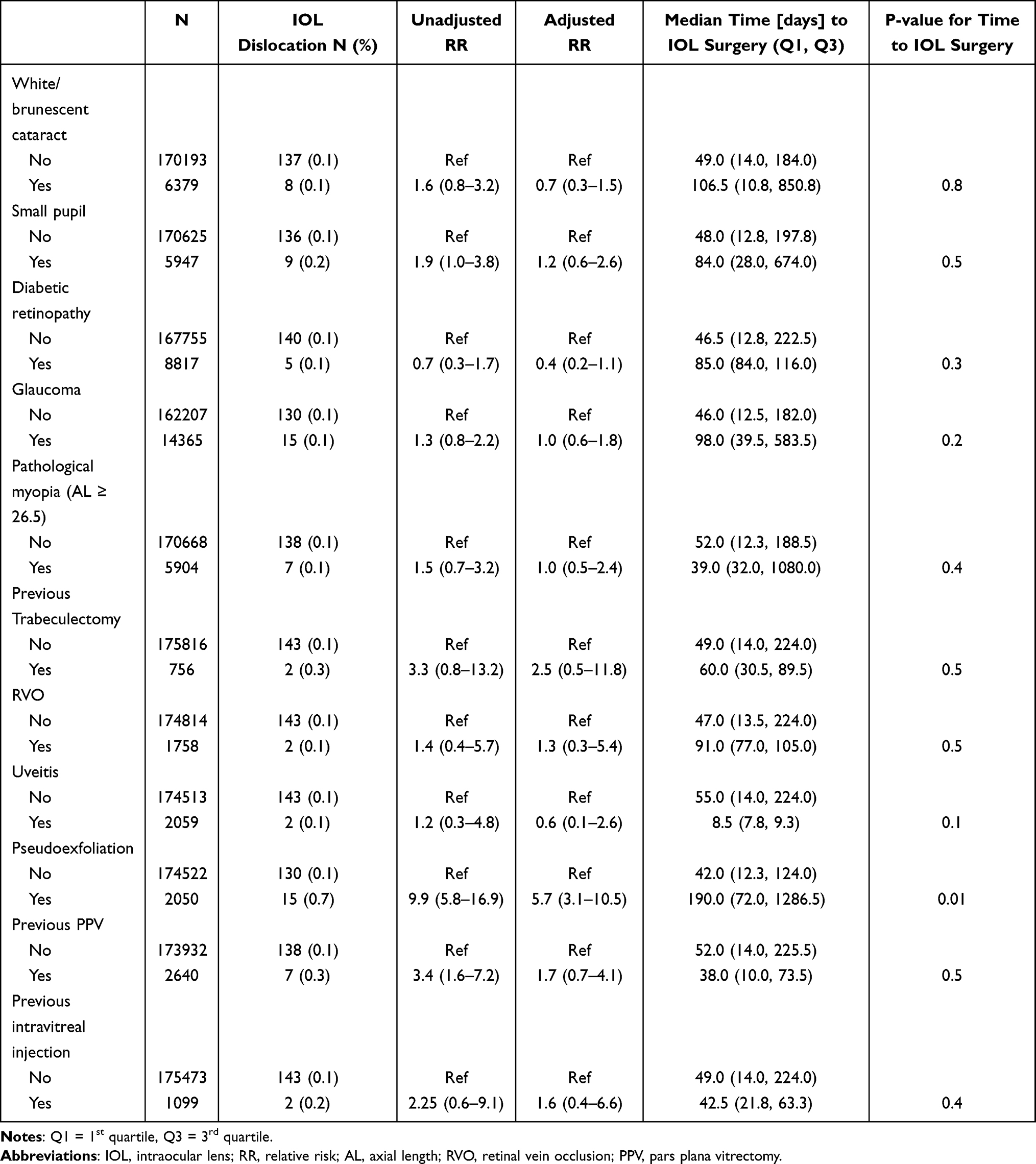 |
Table 2 Preoperative Risk Factors for Intraocular Lens Dislocation |
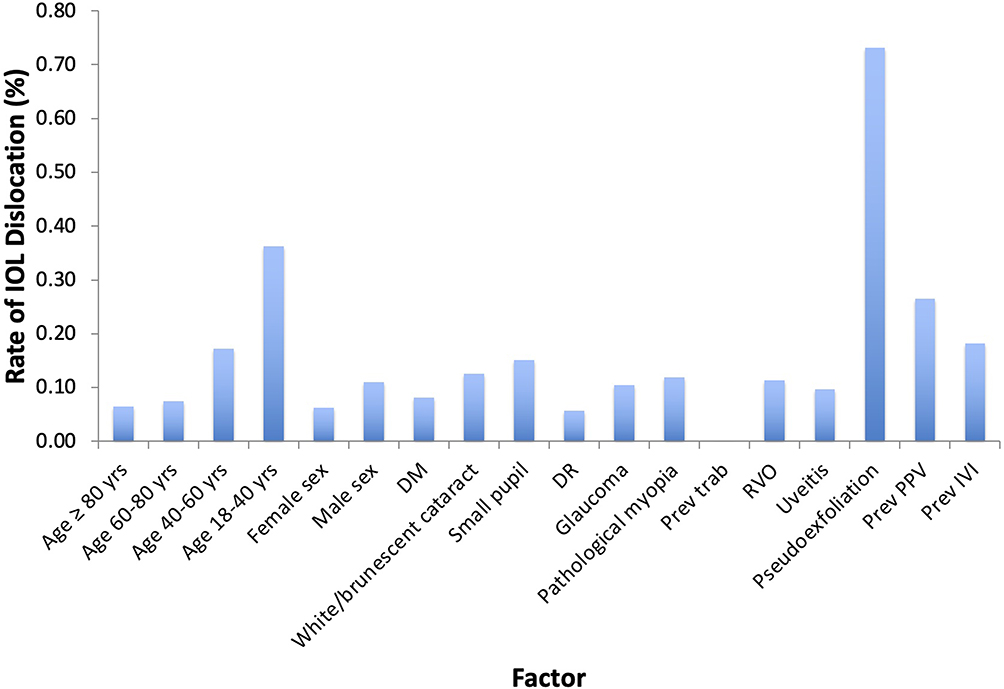 |
Figure 2 Rate of IOL dislocation by analyzed preoperative factor. |
Among the intraoperative factors, the ARR of developing IOL dislocation for eyes with zonular dialysis, PCR, iris damage, and those that underwent combined phaco-vitrectomy were statistically significant. The ARR was 3.3 (1.5–7.1) for zonular dialysis, 16.2 (9.7–27.1) for PCR, 4.2 (1.5–11.6) for iris damage, and 3.2 (1.7–6.2) for combined phaco-vitrectomy. The postoperative factor we analyzed was YAG capsulotomy. The ARR of 2.8 (1.5–5.2) was also significant. Table 3 displays the results for intraoperative and postoperative factors. Figure 3 displays the rate of IOL dislocation by analyzed intraoperative and postoperative factors. Figure 4 displays the ARR of statistically significant risk factors for development of IOL dislocation requiring surgical intervention.
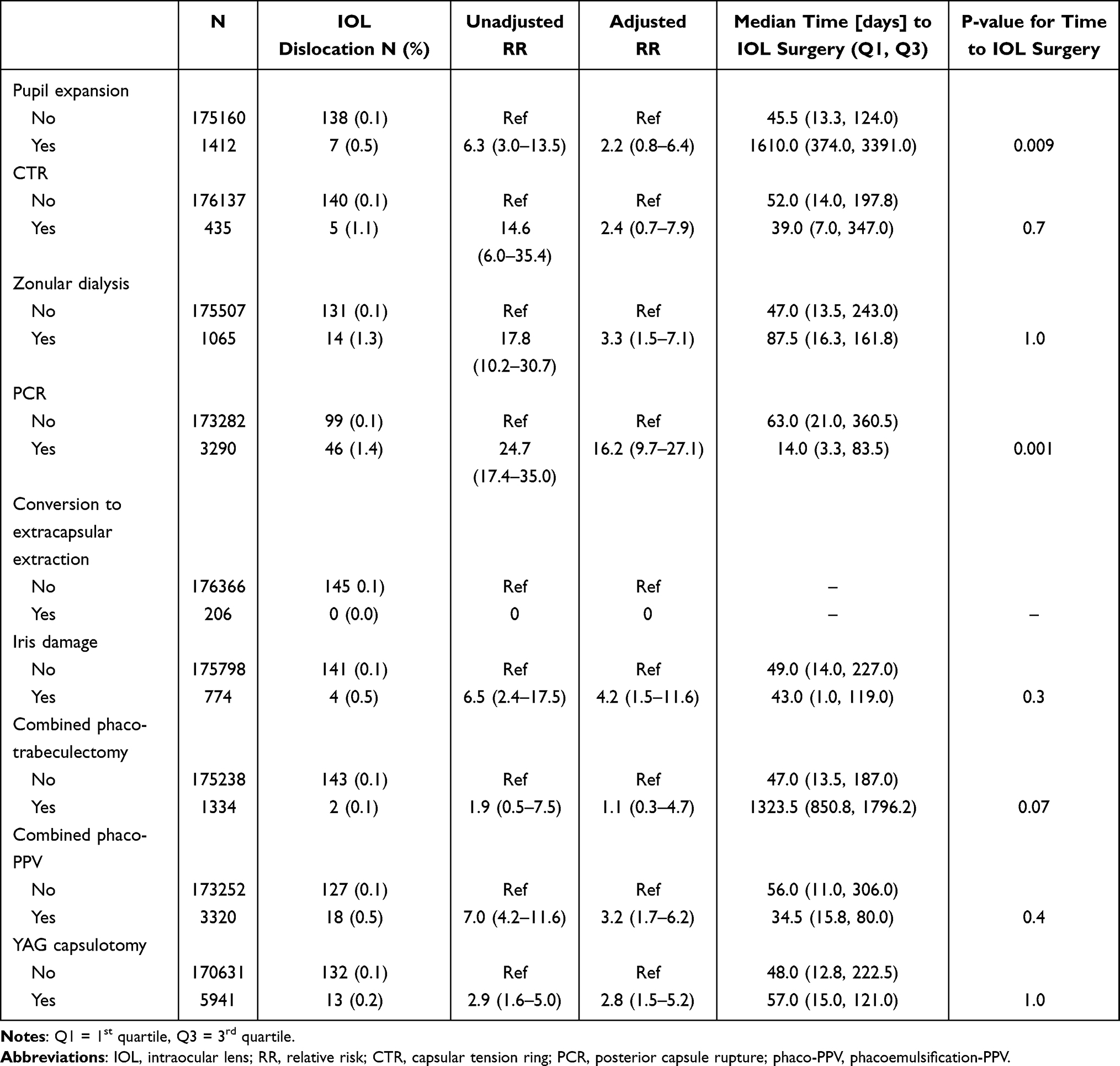 |
Table 3 Intraoperative and Postoperative Risk Factors for Intraocular Lens Dislocation |
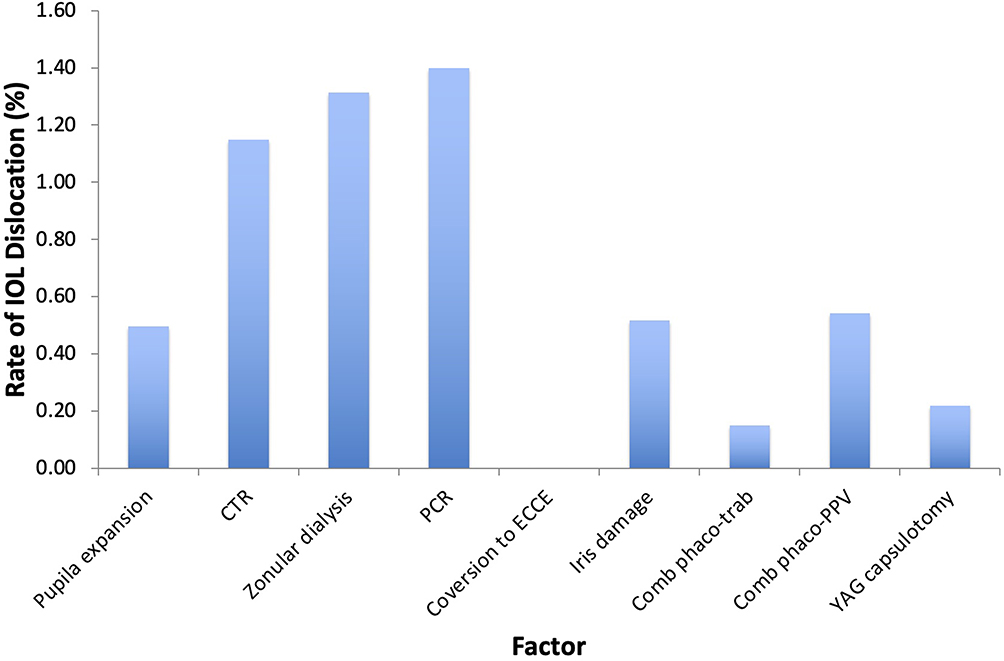 |
Figure 3 Rate of IOL dislocation by analyzed intraoperative and postoperative factor. |
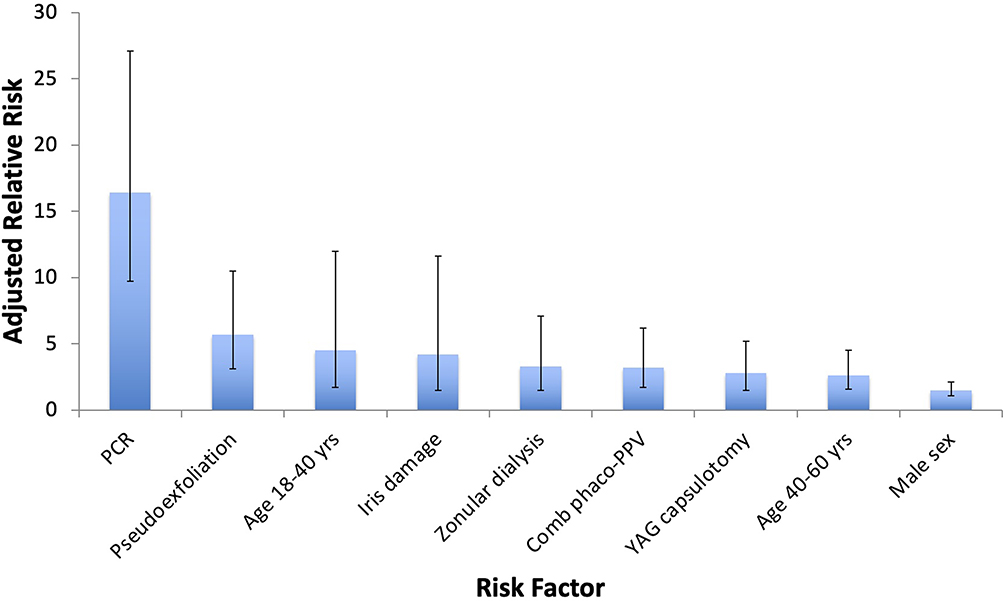 |
Figure 4 Statistically significant risk factors for development of IOL dislocation requiring surgical intervention. |
Among the eyes with IOL dislocation, the average time to surgery was 408.6 days, and the median time to surgery was 49 days (range: 1–3628 days); 92 eyes (63.4%) had IOL surgery within 90 days of the initial cataract surgery, while 53 eyes (36.6%) had IOL surgery more than 90 days after cataract surgery. The median time to IOL surgery associated with each analyzed factor is listed in Tables 1–3.
Discussion
This multicenter study analyzed the demographic, preoperative ocular, intraoperative, and post operative risk factors for developing IOL dislocation requiring a second surgery after initial planned phacoemulsification cataract surgery. Of 176,572 eyes that underwent planned phacoemulsification cataract surgery, 145 (0.08%) required a second surgery for postoperative IOL dislocation. Identified risk factors included younger age, male sex, pseudoexfoliation, PCR, zonular dialysis, iris damage, combined phaco-vitrectomy, and YAG capsulotomy.
YAG capsulotomy statistically increased the risk for IOL dislocation by almost three-fold. This increased risk associated with posterior capsulotomy is consistent with previous smaller studies and case series.9–12 Contrary to our study, however, Lee et al found that posterior capsulotomy after cataract surgery reduced the risk of IOL dislocation. However, the authors excluded IOL dislocation events during the first postoperative week, and their analysis was adjusted only for age, sex, and preoperative variables but not intraoperative factors. As demonstrated in our studies, intraoperative complications such as PCR can significantly affect the results. The increased risk with YAG capsulotomy may be due to photodisruptive damage to the posterior zonular fibers that are connected to the anterior hyaloid during the laser procedure.10 For patients with visually significant posterior capsule opacification after cataract surgery, clinicians should take caution performing YAG capsulotomy in patients predisposed to zonular weakness.
In addition, younger age and male sex significantly increased risk for IOL dislocation. The risk was highest in the youngest age group and steadily decreased until no longer significant in older age groups. Age between 18 and 40 years increased the risk for IOL dislocation nearly five-fold, and age between 40 and 60 years increased the risk by slightly less at almost three-fold. Male sex increased the risk for IOL dislocation by nearly two-fold. Lee et al also found that IOL dislocation tended to occur most frequently in young males4 We hypothesize that younger males are more likely to experience trauma causing zonular weakness and, therefore, are more likely to develop postoperative IOL dislocation. Furthermore, among analyzed preoperative ocular factors, pseudoexfoliation statistically increased the risk of IOL dislocation nearly six-fold. The increased risk associated with pseudoexfoliation is expected given it is well known to increase the risk of zonular weakness.13
Multiple intraoperative factors statistically increased the risk for IOL dislocation, the greatest being associated with PCR. Intraoperative PCR increased the risk for IOL dislocation by about sixteen-fold, the highest among all analyzed factors in the study. Both zonular dialysis and combined phaco-vitrectomy increased risk by about three-fold, while iris damage was associated with a four-fold increase in risk. These findings are supported by other studies in the ophthalmic literature. In their large population-based cohort study, Lee et al found several risk factors for dislocation in Korean patients, including brunescent cataract, uveitis, anterior vitrectomy, iris and ciliary injury, uveitis, glaucoma surgery, and retina surgery4 It is noteworthy that Lee et al excluded IOL dislocation events occurring within the first postoperative week and adjusted solely for age, sex, and preoperative variables4 In contrast, our study analyzed all postoperative IOL dislocation events and conducted a comprehensive adjustment for demographic, preoperative ocular, intraoperative, and postoperative variables. As such, we posit that our findings provide a more accurate depiction of the factors influencing IOL dislocation. In their nested case–control study of 123 eyes with IOL dislocation, Dabrowska-Kloda et al identified risk factors for late in-the-bag IOL dislocation Factors associated significantly with increased risk included longer duration of psuedophakia, long phacoemulsification time during surgery, pseudoexfoliation, zonular dehiscence, pseudophakodenesis, and increased axial length.6 Of note, notable preoperative factors that did not increase the risk of IOL dislocation included white/brunescent cataracts, small pupil, diabetes mellitus, high axial length, prior PPV, and prior intravitreal injections. Notable intraoperative factors that did not increase risk of IOL dislocation included a combined phaco-trabeculectomy and use of a PED or CTR. Use of CTR was not associated with increased risk, but zonular dialysis was identified as a risk factor. This inconsistency may be because not all cases of zonular dialysis received a CTR intraoperatively. Therefore, the cohort with CTR insertion had overall more stable IOL-capsular bag complexes than the broader zonular dialysis cohort.
The majority of eyes in our study (63.4%) had second surgery for IOL dislocation within 90 days of cataract surgery, with the earliest occurring 1 day postoperatively. It is unclear if the wide range of time-to-surgery could be due to outliers or mistakes in the data and was the justification for reporting median time-to-surgery rather than averages. IOL dislocation most commonly manifests in the early postoperative period because of inadequate capsular support. However, late IOL dislocation can occur months to years after uncomplicated cataract surgery due to progressive zonular weakness.14 In a series of 284 eyes that underwent surgery for dislocated IOL, IOL dislocation occurred within 1 month of cataract surgery in 37% of eyes, between 1 month to 1 year in 18% of eyes, and after 1 year in 44% of eyes. Twenty-five percent of eyes had dislocation within 1 day of cataract surgery.14 The higher prevalence of early dislocation ≤90 days after cataract surgery in our series stems from the fact that the most common factor to affect eyes with IOL dislocation was PCR, affecting 46 of 145 eyes (31.7%). Progressive zonular weakness and/or capsular phimosis were likely contributing factors to dislocations occurring >90 days after initial cataract surgery.
The retrospective, non-randomized design of this study is a limiting factor that may have introduced bias. Additionally, the extent or severity of zonular dialysis and iris damage encountered during initial surgery was not documented, which can have implications on the risk of IOL dislocation. Additionally, we based the rates of IOL dislocation in our study on the numbers of cases requiring surgery for IOL dislocation, rather than a clinical diagnosis of IOL dislocation. Although this method may miss cases with minor IOL dislocation and cannot derive the true incidence of IOL dislocation, it should give an accurate estimation of the burden of IOL dislocations in a certain volume of cataract operations, and thus may be a more useful statistic in the real-world setting. In addition, specific data regarding surgical technique and IOL type used among centers was unavailable and, thus, possible confounding factors that we were unable to account for. The large sample size and multicenter design of this study are important strengths of our study and increase the generalizability of our findings. Additionally, there was standardized data collection across the study sites using the same EMR system that enforced complete and accurate capture of intraoperative complications. Large prospective studies assessing risk of IOL dislocation would provide additional clinically useful information for cataract surgeons while avoiding biases inherent to retrospective studies.
In summary, this multicenter study defined several risk factors for developing an IOL dislocation necessitating second surgery after initial phacoemulsification cataract surgery. Risk factors included younger age, male sex, pseudoexfoliation, zonular dialysis, combined phaco-vitrectomy, and YAG capsulotomy, with PCR constituting the highest risk. Cataract surgeons should take these risk factors into account to conduct appropriate preoperative risk stratification and adopt preventative strategies to reduce morbidity from IOL dislocation. Use of capsular support devices and conservative YAG capsulotomy in high-risk patients, particularly those with pseudoexfoliation of intraoperative complications, such as PCR or zonular dialysis, may reduce the risk of IOL dislocation after cataract surgery.
Data Sharing Statement
Data will be made available upon reasonable request to the corresponding author, Dr. Ahmed Sallam.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no conflict of interest.
References
1. Lee CM, Afshari NA. The global state of cataract blindness. Curr Opin Ophthalmol. 2017;28(1):98–10. doi:10.1097/ICU.0000000000000340
2. Ascaso FJ, Huerva V, Grzybowski A. Epidemiology, etiology, and prevention of late IOL-capsular bag complex dislocation: review of the literature. J Ophthalmol. 2015;2015:1–7. doi:10.1155/2015/805706
3. Subasi S, Yuksel N, Karabas VL, Yilmaz Tugan B. Late in-the-bag spontaneous IOL dislocation: risk factors and surgical outcomes. Int J Ophthalmol. 2019;12(6):954–960. doi:10.18240/ijo.2019.06.12
4. Lee GI, Lim DH, Chi SA, Kim SW, Shin DW, Chung TY. Risk factors for intraocular lens dislocation after phacoemulsification: a nationwide population-based cohort study. Am J Ophthalmol. 2020;214:86–96. doi:10.1016/j.ajo.2020.03.012
5. Pueringer SL, Hodge DO, Erie JC. Risk of late intraocular lens dislocation after cataract surgery, 1980–2009: a population-based study. Am J Ophthalmol. 2011;152(4):618–623. doi:10.1016/j.ajo.2011.03.009
6. Dabrowska-Kloda K, Kloda T, Boudiaf S, Jakobsson G, Stenevi U. Incidence and risk factors of late in-the-bag intraocular lens dislocation: evaluation of 140 eyes between 1992 and 2012. J Cataract Refract Surg. 2015;41(7):1376–1382. doi:10.1016/j.jcrs.2014.10.040
7. Shakarchi AF, Soliman MK, Yang YC, Sallam AB. Risk of pseudophakic cystoid macular edema in fellow-eye cataract surgeries: a multicenter database study. Ophthalmology. 2023;130(6):640–645. doi:10.1016/j.ophtha.2023.01.019
8. Chu CJ, Johnston RL, Buscombe C, et al. Risk factors and incidence of macular edema after cataract surgery: a database study of 81984 eyes. Ophthalmology. 2016;123(2):316–323. doi:10.1016/j.ophtha.2015.10.001
9. Davis D, Brubaker J, Espandar L, et al. Late in-the-bag spontaneous intraocular lens dislocation. Ophthalmology. 2009;116(4):664–670. doi:10.1016/j.ophtha.2008.11.018
10. Gimbel HV, Condon GP, Kohnen T, Olson RJ, Halkiadakis I. Late in-the-bag intraocular lens dislocation: incidence, prevention, and management. J Cataract Refract Surg. 2005;31(11):2193–2204. doi:10.1016/j.jcrs.2005.06.053
11. Østern AE, Sandvik GF, Drolsum L. Late in‐the‐bag intraocular lens dislocation in eyes with pseudoexfoliation syndrome. Acta Ophthalmol. 2014;92(2):184–191. doi:10.1111/aos.12024
12. Petersen AM, Bluth LL, Campion M. Delayed posterior dislocation of silicone plate-haptic lenses after neodymium:yag capsulotomy. J Cataract Refract Surg. 2000;26(12):1827–1829. doi:10.1016/s0886-3350(00)00500-9
13. Shingleton BJ, Marvin AC, Heier JS, et al. Pseudoexfoliation: high risk factors for zonule weakness and concurrent vitrectomy during phacoemulsification. J Cataract Refract Surg. 2010;36(8):1261–1269. doi:10.1016/j.jcrs.2010.02.014
14. Kim SS, Smiddy WE, Feuer W, Shi W. Management of dislocated intraocular lenses. Ophthalmology. 2008;115(10):1699–1704. doi:10.1016/j.ophtha.2008.04.016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Flutter Sign – An Indicator of Intact Anterior Hyaloid Face After Posterior Capsule Rupture During Phacoemulsification

Om Parkash R, Om Parkash T, Sharma T, Vajpayee RB, Megur D, Patwardhan SD, Desai A, Tassignon MJ
Clinical Ophthalmology 2025, 19:4313-4321
Published Date: 26 November 2025