Back to Journals » Journal of Pain Research » Volume 18
Fire Needle Therapy for Nocturnal Leg Cramps in Older Adults: A Randomized Sham-Controlled Pilot Trial Protocol
Authors Wang X ![]() , You W, Li Y
, You W, Li Y ![]() , Li B, Tian W, Sun J
, Li B, Tian W, Sun J
Received 4 July 2025
Accepted for publication 30 September 2025
Published 17 October 2025 Volume 2025:18 Pages 5467—5480
DOI https://doi.org/10.2147/JPR.S551660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Xiyun Wang,1,2 Wei You,1 Yanpi Li,2 Bin Li,1 Wei Tian,1 Jingqing Sun1
1Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Key Laboratory of Acupuncture Neuromodulation, Beijing, People’s Republic of China; 2Beijing University of Chinese Medicine, Beijing, People’s Republic of China
Correspondence: Wei You, Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Key Laboratory of Acupuncture Neuromodulation, 23 Meishuguanhou Street Dongcheng District, Beijing, 100010, People’s Republic of China, Email [email protected] Jingqing Sun, Department of Acupuncture and Moxibustion, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing Key Laboratory of Acupuncture Neuromodulation, 23 Meishuguanhou Street Dongcheng District, Beijing, 100010, People’s Republic of China, Email [email protected]
Background: Nocturnal Leg Cramps (NLC) are prevalent in older adults, yet safe and effective non-pharmacological treatments are lacking. Fire Needle Therapy (FNT), a Traditional Chinese Medicine (TCM) technique combining thermal and mechanical stimulation, may address this gap.
Methods: This prospective, randomized, participant-and assessor-blind pilot trial will enroll 68 participants (aged 50– 75 years) experiencing ≥ 8 days of NLC monthly. Participants will receive FNT targeting the Ashi points (APs) as treatment or Sham Fire Needle Therapy (SFNT) targeting the non-Ashi points (NAPs) as control twice a week for 4 weeks (1:1 randomization). The primary outcome is the change in the number of days with NLC from baseline (week − 4– 0) to follow-up (weeks 5– 8 and weeks 13– 16). Secondary outcomes include pain severity, cramp duration, sleep quality, quality of life, and muscle stiffness assessed via ultrasound Shear Wave Elastography (SWE). Safety and compliance will be systematically monitored, with analysis following the Intention-to-Treat (ITT) principle.
Discussion: This trial is the first to evaluate the efficacy of manualized FNT protocols for NLC with innovative blinding design and objective biomechanical assessments.
Ethics and Trial Registration: The Research Ethics Committee of the Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University Ethics Committee has approved the study protocol (Approval No. 2024BL02-073-02). This trial was registered at the International Traditional Medicine Clinical Trial Registry (ITMCTR, http://itmctr.ccebtcm.org.cn/). Trial number: ITMCTR2024000325. Registered on August 29, 2024.
Keywords: nocturnal leg cramps, fire needle therapy, randomized controlled trial, sham fire needle therapy, innovative design
Introduction
Nocturnal Leg Cramps (NLC) are sudden, painful, and involuntary contractions of the lower limb muscles that occur during sleep,1 affecting approximately 38–50% of adults over the age of 50.2,3 Its frequency and severity rise with age, often causing moderate-to-severe pain,4 sleep disruption, impaired daytime function, and quality-of-life decline.5 Chronic or recurrent cases are further associated with complications including insomnia,6 cardiovascular risk,7 mood disturbance, and cognitive impairment.8–10
Despite the high prevalence and clinical burden of NLC, treatment options remain limited.11 Pharmacological agents remain suboptimal: quinine provides modest relief12 but with safety concerns;13,14 magnesium supplementation yields inconsistent effects;15,16 and other agents such as vitamin K2 or gabapentin lack rigorous trial support.17,18 Non-pharmacological strategies such as stretching, physical therapy, and myofascial trigger point (MTrP)-based interventions show promise19,20 but systematic reviews emphasize the absence of high-quality randomized controlled trials (RCTs).21
Fire Needle Therapy (FNT), a traditional Chinese medicine modality,22 combines needle insertion with controlled thermal stimulation.23,24 In contrast to conventional acupuncture, which primarily induces mechanical effects, and thermal therapies like cupping, which provide superficial heating, FNT integrates both approaches to achieve a more comprehensive therapeutic effect. Based on Traditional Chinese Medicine (TCM) principles and supported by preliminary clinical evidence, FNT has demonstrated particular effectiveness in the treatment of Neuritis-Linked Conditions (NLC), for which other therapeutic modalities have shown limited success. FNT targets Ashi points (APs), which are non-fixed, tenderness-based sites identified through palpation.25 These dynamic points are associated with localized dysfunction and may overlap with myofascial trigger points (MTrPs). APs are typically found at myotendinous junctions or fascial planes along muscle-tendon meridians.26 Stimulation of these points is thought to restore neuromuscular balance,27 aligning with the TCM principle of Warming Yang and Relaxing Tendons.28 Conceptually, APs are akin to Western-defined MTrPs,29 which are characterized by localized tenderness and referred pain.
Although the pathophysiology of NLC remains incompletely understood, emerging evidence suggests that neuromuscular junction instability and MTrPs, particularly within the gastrocnemius–soleus complex, may contribute to the condition’s development.30 The therapeutic potential of mechanical stimulation in MTrP therapy was first reported in a seminal study published in The Lancet in 198031 and has since been supported by a more recent RCT in 2021.32 Together, these findings provide a rationale for investigating FNT as a potential intervention for NLC.
Preliminary clinical observations indicate that FNT may reduce the frequency and severity of NLC, but its efficacy and safety remain untested in rigorous trials. Given the limitations of current therapies and the absence of validated non-pharmacological alternatives, high-quality evidence is urgently needed. This pilot randomized controlled trial is designed to evaluate the efficacy and safety of FNT for NLC while providing exploratory insights into its potential mechanisms.
Methods
Study Design
This prospective, single-center, randomized, participant- and assessor-blind, sham-controlled pilot trial with concealed allocation will enroll 68 older individuals aged 50–75 years with 8 or more documented days of NLC during 4 weeks of screening. Participants will be randomized to receive FNT as treatment or Sham Fire Needle Therapy (SFNT) as control (n=34/group) twice a week for 4 weeks at a 1:1 ratio, followed by a 12-week follow-up period, which was chosen to allow sufficient time to evaluate the persistence of therapeutic effects and potential recurrence of NLC, in line with previous non-pharmacological intervention studies.21 The primary outcome is the average number of days with NLC per week in the treatment group compared to the control group. Secondary outcomes include pain Visual Analog Scale (VAS), cramp duration, sleep quality (PSQI), quality of life (SF-36), and muscle stiffness (SWE). The flow diagram of the study procedure is presented in Figure 1. The entire protocol of the present study will be performed at the Acupuncture & Moxibustion Center outpatient of Beijing Hospital of Traditional Chinese Medicine (Beijing, China), affiliated with the Beijing Municipal Health Commission, a research center specializing in the fire needle, which also serves as the chairing unit of the Fire Needle Committee of the China Association for Acupuncture and Moxibustion (CAAM). The trail was registered at http://itmctr.ccebtcm.org.cn/ (Code: ITMCTR2024000325), following the Standard Protocol Items: Recommendation for Interventional Trials (SPIRIT),33 the Consolidated Standards of Reporting Trials (CONSORT),34 and the Template for Intervention Description and Replication checklist.35 A completed copy of the SPIRIT checklist is included in the consolidated Supplementary Material (Section 1). This study aims to investigate the efficacy of Fire Needle Therapy (FNT) in treating NLC and also to introduce a specially designed sham procedure as a negative control. The design of using SFNT as a control measure is based on established principles from previous sham acupuncture studies,36 with adjustments tailored to the unique characteristics of FNT to minimize specific physiological effects while preserving only non-specific placebo responses.37
 |
Figure 1 Study flow diagram. |
Sample Size
This study is an exploratory clinical trial. According to the Pilot Trial Sample Size Calculation Guidelines,38 the sample size is calculated using G*Power 3.1 with ANOVA repeated measures (within–between interaction). A moderate effect size (f = 0.25) is assumed, with α = 0.05, power = 80%, correlation = 0.5 among repeated measures, and a 20% attrition rate, resulting in a required sample size of 34 participants per group (total N = 68). The effect size assumption is informed by prior studies and clinical experience, where a moderate effect size (Cohen’s d ≈ 0.5) is commonly adopted in exploratory research.39 Based on this assumption and using a conventional power analysis approach, a sample size of 30 per group is considered adequate for detecting clinically meaningful trends.40 To account for potential attrition—including loss to follow-up, exclusion, and dropout—an additional 10% is incorporated, consistent with dropout rates of 5–15% reported in comparable clinical studies.41 Accordingly, the final sample size is set at 34 participants per group, yielding a total of 68 cases. As this is a pilot study, the assumed effect size is regarded as provisional, and the calculated sample size is intended primarily to establish feasibility and provide preliminary effect estimates rather than a definitive powered calculation.
Participants
Randomization and Blinding
Randomization will be conducted through a centralized web-based system using block randomization with a block size of 4, maintaining allocation concealment until intervention assignment. Participants will be allocated in a 1:1 ratio using the Research Electronic Data Capture (REDCap) platform. REDCap, developed by Paul Harris’ team at Vanderbilt University (2004),42 is a secure web application for clinical research data management,43 supported by the Clinical Epidemiology Research Center of Peking University Third Hospital.
Given the inherent challenges in blinding fire needle therapy (FNT), this trial adopts a single-blind design, ensuring participants remain unaware of treatment allocation. To maintain methodological rigor, intervention operators, outcome assessors, and statistical analysts will remain independent throughout the study. All biological samples and datasets will be anonymized prior to analysis. During treatment, participants will be positioned prone, which naturally prevents them from observing the procedure. In addition, interventions will be conducted behind curtains or in separate rooms to avoid cross-contamination of blinding. Only individuals without prior exposure to FNT will be recruited, reducing the likelihood of distinguishing between interventions based on treatment sensation.
In the FNT group, the procedure involves igniting an alcohol-soaked cotton ball, heating the fire needle until red-hot, and then rapidly inserting it into Ashi points (APs) without retention. To enhance treatment credibility, patients receive a standardized verbal prompt immediately before insertion (eg, “You are now receiving fire needle treatment; you may feel a slight pain”), thereby establishing consistent expectations.
In the Sham Fire Needle Therapy (SFNT) group, the same specialized fire needle instruments and procedural sequence are used to maximize similarity.44 An alcohol-soaked cotton ball is ignited near the skin to generate thermal sensation, but the fire needle itself is not heated. Instead, the operator applies a rapid superficial prick (≤1 mm depth) at predefined non-acupoint sites (NAPs), which are standardized across participants and confirmed to lack nodules or tenderness. This approach aims to simulate the tactile and procedural features of FNT while minimizing its three critical therapeutic components: (1) stimulation of therapeutic acupoints, (2) penetration at sufficient depth, and (3) heat delivery via the needle. Patients receive the same standardized verbal prompt as in the FNT group, reinforcing expectancy.45
By comparing outcomes between the FNT and SFNT groups, the trial seeks to isolate the specific therapeutic effects of FNT beyond placebo and contextual influences, thereby strengthening internal validity. To further evaluate the success of blinding, participants will be asked at the end of treatment identify their allocation as “real FNT”, “sham FNT”, or “uncertain”, following established practice in sham-controlled acupuncture trials.46
Recruitment
Participant recruitment adheres to CONSORT equity guidelines47 through three primary channels, from September 2024 to December 2025:
- Posted recruitment advertisements in hospital public areas
- Physician-initiated oral dissemination during clinical consultations
- Digital enrollment notices via the hospital’s official WeChat platform
All recruitment materials received prior ethics committee approval (No. 2024BL02-073-02). Eligible candidates will receive standardized written documentation detailing:
- Study objectives and procedures
- Potential risks/benefits
- Data confidentiality protocols
- Voluntary withdrawal mechanisms
Written informed consent will be obtained during baseline visits, with copies containing investigator contact information provided to participants. The Nocturnal Cramps Sleep Diary (NCSD) will be administered to monitor sleep parameters and Adverse Events (AEs). Participant confidentiality will be maintained through anonymized data coding, with personal information stored in password-protected hospital servers. Intention-to-Treat (ITT) analysis will address withdrawal cases and missing data per predefined statistical plans.
Eligibility Criteria
Eligible participants should meet NLC diagnostic criteria, based on the diagnostic criteria in the International Classification of Sleep Disorders, Third Edition (ICSD-3), published in 2014, which includes the following three mains: (1) A painful sensation in the leg or foot accompanied by sudden, involuntary muscle stiffness or tightness and other strong muscle contractions; (2) Painful muscle contractions occurring in bed during wakefulness or sleep; (3) Pain can be relieved and muscle contractions slowed by stretching the affected muscles with force.
An overview of all inclusion and exclusion criteria is provided in Table 1, each participant must meet all inclusion criteria and meet none of the exclusion criteria.
 |
Table 1 Eligibility Criteria According to PICOS Framework |
Intervention Conditions
This study will adhere to the SPIRIT-TCM Extension 2018 guidelines48 to ensure standardized protocols for Fire Needle Therapy (FNT). It will also fully comply with the ethical principles of the revised Declaration of Helsinki (2013). Key adaptations include: All participants will receive the allocated intervention twice a week for 4 weeks. All participants will go through a standardized interview and be provided with details of the study. The acupuncturists who perform treatments for both groups are registered with the Ministry of Health of the People’s Republic of China as Chinese medicine practitioners and have more than 20 years of clinical experience. Before the trial begins, all acupuncturists will receive special training regarding the purpose and standard operating procedure of the trial, treatment strategies, and quality control. The treatment details will be fully documented in accordance with the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA)49 and Good Clinical Practice guidelines.
Operator Training Protocol
Standard Operating Procedure (SOP)
Operators completed a 40-hour training program (Fire Needle SOP v.FNT-2024), including:
- 8-hour theoretical training (mechanisms, contraindications, safety zones);
- 20-hour simulation practice (needle heating, 90° vertical insertion on silicone models);
- 12-hour supervised clinical practice (≥30 cases).
Competency Assessment
Passed Objective Structured Clinical Examination (OSCE) with ≤1 mm depth error and ≤0.5-second timing deviation; all procedures were video-recorded and reviewed by two independent evaluators.
Experimental Group
In this group, FNT will be used to insert the APs. Before acupuncturing, APs will be identified through palpation of both lower legs, guided by the commonly accepted locations of the Foot Taiyang meridian sinew as described in Meridian Sinew Theory and Clinical Diagnosis & Treatment of Pain Disorders.50 Identify areas with significant tenderness accompanied by cord-like structures or local tissue swelling and thickening as APs. Mark these points sequentially, with 3–5 points on each side being sufficient. The common APs’ locations in meridian sinew theory are shown in Figure 2, Weizhongci: Located at the center of the popliteal crease. Weiyangci: Located at the lateral end of the popliteal crease, on the medial border of the biceps femoris muscle. Heyangci: Located on the posterior aspect of the calf, inferior to the midpoint of the inferior border of the popliteal fossa, at the level corresponding to the inferior border of the fibular head. Chengjinci: Located on the posterior aspect of the calf, in the depression at the center of the gastrocnemius muscle belly. Chengshanci: Located on the posterior aspect of the calf, at the junction between the muscle bundles of the triceps surae and the Achilles tendon. Chengshannei: Located on the posterior aspect of the calf, at the junction between the medial belly of the gastrocnemius muscle and the Achilles tendon. Chengshanwai: Located on the posterior aspect of the calf, at the junction between the lateral belly of the gastrocnemius muscle and the Achilles tendon.
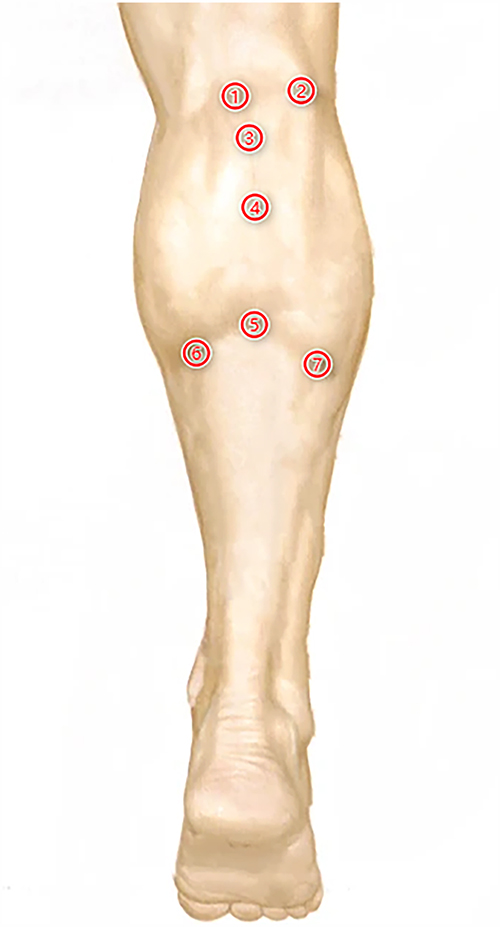 |
Figure 2 Common locations of APs in patients with NLC: ① Weizhongci; ② Weiyangci; ③ Heyangci; ④ Chengjinci; ⑤ Chengshanci; ⑥ Chengshannei; ⑦ Chengshanwai. |
Procedure
The Fire Needle protocol followed STRICTA guidelines:51 The patient assumes a prone position with both lower legs fully exposed. After disinfection with 75% rubbing alcohol, ignite a 95% alcohol cotton ball. Use a fire needle (specification: a heat-resistant tungsten-manganese alloy, Diameter: 0.5 mm × Length: 40 mm; manufactured by Beijing ZhongyanTaihe Medical Instrument Co., Ltd., Beijing, China). Heat the front part of the needle by the external flame until achieving red-heat phase (~800°C). Single-hand swift insertion-withdrawal motion (Cycle duration: ≤0.1 second per AP, Immediate post-withdrawal compression with sterile cotton ball: 1–2 seconds). The typical insertion depth is 10–15 mm, adjusted according to anatomical layer (Superficial muscle layer: 10–12 mm, Deep fascia layer: 12–15 mm), to avoid damage to adjacent blood vessels, nerves, or tendons (maintaining≥3 mm from superficial vessels, parallel insertion relative to nerve pathways and pre-procedure anatomical palpation ensures accurate APs).
Post-Treatment Instructions
Post-procedure monitoring requires a 15-minute observation for immediate AEs, and the emergency protocol specifies the use of a cold compress kit to manage accidental thermal injury. Advise the patients to keep the acupunctured area clean and avoid scratching or touching the site. Do not apply oils, ointments, or topical medications to the area. Prevent the inserted area from contact with water on the day of treatment to minimize infection risk (24-hour post-treatment hygiene protocol; 24/7 emergency hotline provided for AEs).
Total Treatment Duration
10 minutes per session (including disinfection, positioning, and post-treatment care).
Control Group
Sham Fire Needle Therapy (SFNT) is performed using the same fire needle to prick the non-Ashi points (NAPs).
Procedure
In the SFNT group, patients are positioned prone and APs are identified by palpation as in the FNT group. For each AP, a corresponding NAP is selected at least 2 cm lateral to the AP, explicitly outside recognized meridians,45 and confirmed by palpation to lack nodules, induration, or tenderness; sites overlying bony prominences, tendon pathways, or visible superficial vessels are avoided. Once validated, NAPs are marked with a sterile skin marker to ensure reproducibility. Following routine skin disinfection with 75% alcohol, a 95% alcohol–soaked cotton ball is ignited and held near the AP’s surface to generate thermal sense. The fire needle is not heated and applied at the predefined NAPs with a swift, single-handed superficial prick (cycle duration ≤0.1 second, insertion depth ≤1 mm), without retention. Immediately after withdrawal, the puncture site is compressed with a sterile dry cotton ball for 1–2 seconds to achieve hemostasis. Patients are expected to experience a brief needle-pricking sensation and perceptible warmth from the burning cotton ball, mimicking the sensory characteristics of authentic fire needle therapy without delivering specific thermal or mechanical stimulation. All procedures are repeated bilaterally for procedural symmetry, with post-treatment care kept identical to that of the experimental group, and expectancy reinforced through the same standardized verbal cue as in the FNT group to ensure the integrity of participant blinding.
Follow-up
After the 4-week treatment, follow-up will be conducted among all participants for 12 weeks. FNT and NLC-related treatment are not permitted during follow-up.
Specific Notes
Emergency Management
If the participant experiences symptom exacerbation or is unable to tolerate the treatment due to lack of response, they should be informed that stretching the calf can help alleviate pain and terminate cramps during nighttime episodes. If the pain becomes unbearable and prevents the participant from falling back asleep, oral administration of nonsteroidal anti-inflammatory drugs (eg, Paracetamol 500 mg PRN (max 4 g/day)) or short-acting sedatives (eg, zolpidem tartrate) is allowed. However, the use of quinine, verapamil, magnesium supplements, or other medications that may directly affect NLC treatment is prohibited. Patients should be reminded to record their medication usage in detail in their diary after each dose.
Measurements and Procedures
The outcomes and measurement timepoints are presented in Table 2. A demographic questionnaire, which consists of participants’ characteristics (sex, age, medical history, height, weight, important signs, systematic checks, and so on) and previous treatment and medication history of NLC, will be completed before the intervention.
 |
Table 2 | Time Schedule |
Primary Outcome
The Change in the Number of days with NLC
To quantify the primary outcome, we employ the Nocturnal Cramps Sleep Diary (NCSD), a validated patient-reported instrument used in previous studies52 and provided in Supplementary Material (Section 2). The NCSD captures key parameters of NLC, including frequency (number of days with NLC per week), pain severity (rated using a Visual Analogue Scale), and duration of each cramp. To improve the reliability of data, the NCSD includes both evening (pre-sleep) and morning (post-sleep) entries. Participants are instructed to complete the evening section before bedtime to record factors that may influence sleep or cramp susceptibility (eg, physical activity, caffeine or alcohol intake, emotional stress) and the morning section upon waking to document NLC events during the night. The number of days with NLC over a 4-week interval is calculated based on morning reports and will serve as the primary outcome. To comprehensively evaluate both immediate and sustained treatment effects, data will be collected during three distinct periods: Baseline period (weeks – 4 to 0) to establish pre-treatment cramp frequency and sleep disturbance. Follow-up period 1 (weeks 5 to 8) to assess short-term efficacy following intervention. Follow-up period 2 (weeks 13 to 16) to evaluate longer-term effects and symptom recurrence. In addition to the paper-based NCSD, participants will also be offered the option of completing an electronic version of the NCSD (eNCSD) via a secure digital platform.
Secondary Outcomes
Secondary outcomes involve pain intensity, duration of cramps, sleep quality, quality of life, and gastrocnemius muscle stiffness measured by SWE.
Severity of Pain
Pain severity during NLC is documented in NCSD and evaluated using the Visual Analog Scale (VAS), a 0–10 scale where 0 indicates no pain and 10 represents unbearable pain. The evaluation time points are the same as the primary outcome indicator: baseline period (weeks −4 to 0), follow-up period 1 (week 5 to 8), and follow-up period 2 (weeks 13 to 16).
Duration of Cramps
The duration of each NLC episode is recorded in NCSD so that the average duration of NLC episodes for each participant could be calculated. The evaluation time points are the same as the primary outcome indicator: baseline period (weeks −4 to 0), follow-up period 1 (week 5 to 8), and follow-up period 2 (weeks 13 to 16).
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) is used to measure sleep quality. The PSQI is a standardized self-administered questionnaire designed to assess subjective sleep quality during the study period. It consists of 19 self-rated questions, divided into 7 component scores. Each component score is weighted from 0 to 3 points. The sum of the 7 component scores provides an overall PSQI score, with a total score range from 0 to 21. A score of 5 or higher indicates poor sleep quality, with higher scores reflecting worse sleep quality. Evaluation time points: at enrollment, immediately after the end of treatment, and at the 8th week after treatment.
Quality of Life
The Medical Outcomes Study 36-Item Short Form 36 Health Survey (SF-36) is used to assess the quality of life in NLC patients, including aspects such as physical, mental, and social functioning. Evaluation time points: at enrollment, immediately after the end of treatment, and at the 8th week after treatment.
Muscle Stiffness Assessment
We use ultrasonic Shear Wave Elastography (SWE) to measure the stiffness of the gastrocnemius fascia.53 Device: French Shear-wave elastography Aixplorer® ultrasound (L4-15 probe; 10×10 mm ROI; triplicate measurements) and SuperSonic Imagine The AixPlorer real-time Shear Wave Elastography ultrasonic diagnostic system will be used, employing an L4-15 model linear array probe with a frequency range of 4–15 MHz and parameters selected for musculoskeletal conditions, following WFUMB guidelines.54 Method: The patient is placed in a prone position. The ultrasound physician identifies the probe position and the area of interest, instructing the patient to relax completely. A routine two-dimensional ultrasound examination is first performed, with a transverse view of the gastrocnemius muscle belly. The probe is then rotated 90° to examine the longitudinal section along the direction of the muscle bundle, checking the muscle echo and fiber alignment. The elastography mode (SWE) is selected, and a square sampling box of 10mm × 10mm is set for the region of interest (ROI), located 1–2 cm below the skin surface. The Q-BOX function is activated, and the system automatically calculates the average Young’s modulus value (in kPa) for the muscle tissue within the Q-BOX area. Images are collected and measured three times, with the average value taken as the result. Evaluation Time Points: At enrollment, immediately after the end of treatment.
Safety Assessments
Safety assessment consists of Adverse Events (AEs) and acupuncture-related adverse reactions. AEs occurring during the course of the study will be assessed by a professional physician after each weekly treatment session and during the follow-up period. These events will be thoroughly documented. Serious AEs will be reported and handled in accordance with relevant regulations. Adverse reactions related to acupuncture, including but not limited to pain, bleeding, local hematoma, itching, infection, nerve injury, severe skin allergies, fainting, needle retention, and needle breakage, will be closely monitored and recorded. Each symptom will be documented in detail, including the severity and duration. AEs will be recorded, and participants will be monitored for any signs of infection, bleeding, or other complications related to needling. The intervention will be stopped if there are any severe AEs or participants request to withdraw. Discontinuation of the trial means that treatment with the trial intervention is stopped, but safety or post-treatment visits may continue.
Data Management and Analysis
Data Collection
After recruitment, the researchers will replace the participants’ names with numerical codes in order to protect their privacy. Their data will be collected at baseline and weeks 4, 8, and 12 respectively. Two professional data workers are responsible for entering their paper files into the same database and crosschecking them for data’s accuracy. Participants will use a secure mobile application to document daily episodes of NLC, including frequency, duration, and pain severity, as measured by the Visual Analog Scale (VAS). Data entry is automatically timestamped and uploaded to a centralized server for secure storage and analysis. To enhance compliance, participants will receive reminders through app notifications and weekly follow-up calls to ensure adherence to the data collection process. Participants will also complete a paper-based Case Report Form (CRF), which includes the Pittsburgh Sleep Quality Index (PSQI), Short Form 36 (SF-36), and reports of any AEs. For those who prefer a digital format, an electronic CRF will be made available via a web-based platform, REDCap, which replicates the paper CRF. Data entered through the digital platform will be encrypted and stored securely to maintain confidentiality and integrity. Eventually, all paper files and encrypted electronic files will be kept and backed up by the researcher leader. These files will be maintained in storage for 3 years after completion of the study.
Data Management and Monitoring
Researchers who manage data will be trained prior to enrollment. Assessors will be in charge of the acquisition of participant information and outcome assessment during the study. Data collectors will transfer the data from the case reports to electronic form. All paper and electronic data will be kept safely in the office of the Department of Acupuncture and Moxibustion. Only investigators of our study team can have access to the final trial data. Others getting written requests from the project administration can be allowed. The study will be regularly monitored and audited by the Data Management and Monitoring Committee of the Good Clinical Practice Department of Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, China. The committee is independent of the study researchers and has no competing interests; it will examine original case report forms, monitor the quality and completeness of the data, verify the recording of AEs, and ensure that the study complies with the principles of the protocol. The periodic review is done every 3 months. Paper CRFs will be entered twice by independent staff to minimize errors. Discrepancies resolved by a third reviewer. Electronic entries (eNCSD and eCRF) include range checks and logic validation (eg, VAS scores 0–10). All electronic data changes are logged with user ID, timestamp, and reason. Incomplete forms will be addressed during weekly follow-ups.
Data Analysis
The statistical analysis will adhere to both Intention-to-Treat (ITT) and Per-Protocol (PP) principles. The ITT analysis will include all randomized participants who received at least one intervention, irrespective of protocol adherence, while the PP analysis will be restricted to participants who completed all study procedures, demonstrated full protocol compliance, avoided prohibited medications, and achieved satisfactory follow-up rates. Consistency between ITT and PP results will be systematically evaluated.
Analyses will be performed using SPSS 25.0 (IBM Corp). Continuous variables will be assessed for normality (Shapiro–Wilk test) and homogeneity of variance (Levene’s test). If normality assumptions are violated, non-parametric alternatives will be employed where appropriate. Parametric data will be analyzed using ANOVA with significance defined as P < 0.05, supplemented by post-hoc pairwise comparisons. Non-parametric data will be analyzed using Mann–Whitney U-tests (independent groups) or Wilcoxon signed-rank tests (paired groups). Categorical variables will be analyzed via chi-square or Fisher’s exact tests. Correlation between ultrasound Shear Wave Elastography parameters and subjective symptom scores of NLC will be quantified using Pearson’s coefficient.
Blinding Assessment
Blinding effectiveness will be evaluated using Bang’s Blinding Index (BI).55 Following consensus-based cutoffs (±0.2) proposed in systematic reviews of acupuncture RCTs,56 BI values within this range are interpreted as successful blinding. If these thresholds are not met, study findings will not be invalidated but will be interpreted with caution, with unblinding acknowledged as a potential limitation.
Predefined Statistical Plan:
- Primary analysis: Linear mixed-effects models incorporating time×group interaction terms
- Missing data handling: Multiple imputation via chained equations (MICE package, R v4.3.1)
- Sensitivity analyses:
- Comparative evaluation of ITT vs PP outcomes
- Subgroup stratification by age cohorts and baseline severity levels
- Robustness verification: Bootstrapping for critical endpoints
Trial Status
This article reports only the study protocol. No results are available at this stage. Participant recruitment is ongoing at the time of manuscript submission.
Discussion
This trial systematically evaluates FNT for NLC and incorporates key methodological innovations to enhance internal validity and feasibility. Specifically, (1) a standardized sham fire needle protocol with defined recruitment criteria and treatment positioning enables a rigorously controlled single-blind design, (2) Shear Wave Elastography (SWE) is applied for the first time in this context to objectively quantify gastrocnemius muscle stiffness alongside symptom outcomes, and (3) a dual-track digital data collection system—including an electronic NCSD with automated reminders and paper-based alternatives—improves compliance, inclusivity, and data completeness across diverse participant groups.
Despite these strengths, several limitations should be noted. First, as a single-center pilot trial with a modest sample size (n = 68) and a three-month follow-up, the results will be exploratory and should not be directly generalized to clinical practice. Future studies should adopt multicenter designs, larger and more diverse cohorts, and extended follow-up periods to improve external validity and assess long-term outcomes. Second, the inclusion criterion of ≥8 cramps/months is deliberately chosen to ensure compliance, and a more homogeneous study population. Patients with lower cramp frequency may lack sufficient motivation or tolerance for intensive interventions such as FNT, potentially increasing dropout rates. However, this threshold may limit the applicability of findings to individuals with milder symptoms. Future trials should therefore broaden inclusion criteria and incorporate stratified analyses by symptom severity. Third, cultural context may influence treatment responsiveness. As FNT is rooted in Traditional Chinese Medicine (TCM), its acceptance and patient expectations in China may not translate directly to regions where TCM is less familiar. To address this, subsequent research should evaluate FNT across multiple cultural and healthcare settings, allowing assessment of cross-cultural generalizability. Finally, current technical constraints prevent blinding of the operator during FNT. To overcome this limitation, our team is developing a standardized fire needle device designed to facilitate double-blind protocols in future studies.
In conclusion, this protocol demonstrates the feasibility of evaluating a traditional therapy within a modern clinical framework. The findings obtained in this study will provide preliminary information on the efficacy, safety, and possible mechanisms of FNT in NLC, offering essential reference for future research.
Abbreviations
AEs, Adverse Events; APs, Ashi points; CAAM, China Association for Acupuncture and Moxibustion; FNT, Fire Needle Therapy; ITT, Intention-to-Treat; MTrPs, Myofascial Trigger Points; NAPs, non-Ashi points; NLC, Nocturnal Leg Cramps; NCSD, Nocturnal Cramps Sleep Diary; RCT, Randomized Controlled Trial; SF-36, Short Form 36 Health Survey; SFNT, Sham Fire Needle Therapy; SPIRIT, Standard Protocol Items: Recommendations for Interventional Trials; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; SWE, Shear Wave Elastography; TCM, Traditional Chinese Medicine; VAS, Visual Analogue Scale.
Ethics Approval and Consent to Participate
This study protocol has received ethical approval from the Beijing Hospital of Traditional Chinese Medicine Affiliated to Capital Medical University Ethics Committee (Approval No. 2024BL02-073-02). Written informed consent will be obtained from all participants prior to enrollment, with additional consent specifically acquired for the publication of identifiable images or clinical data. Trial conduct will be supervised by an independent Data Safety Monitoring Board (DSMB) to ensure participant safety and data integrity.
This trial was prospectively registered at the International Traditional Medicine Clinical Trial Registry (ITMCTR, http://itmctr.ccebtcm.org.cn/) under registration number ITMCTR202400032. Date of first registration: August 29, 2024.
Funding
Supported by the Beijing Municipal Administration of Hospitals Incubating Program (PZ2023013) and the Beijing Hospital Management Center “peak” talent training plan team (DFL20241001). The funder has no role in the design of the study, collection, analysis, and interpretation of data, writing of the manuscript, or decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests. None of the authors have received any sponsorship, funding, or in-kind support related to Fire Needle Therapy, including training or equipment provision. All the research activities were independently conducted, with no external influence on the study design, data collection, analysis, or interpretation of the results.
References
1. Monderer RS, Wu WP, Thorpy MJ. Nocturnal leg cramps. Curr Neurol Neurosci Rep. 2010;10(1):53–59. doi:10.1007/s11910-009-0079-5
2. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
3. Sateia MJ. International classification of sleep disorders—third edition. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
4. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet Lond Engl. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
5. Fitzcharles M-A, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet Lond Engl. 2021;397:2098–2110.
6. Perlis ML, Posner D, Riemann D, Bastien CH, Teel J, Thase M. Insomnia. Lancet. 2022;400(10357):1047–1060. doi:10.1016/S0140-6736(22)00879-0
7. Fogacci F, Ray KK, Nicholls SJ, Cicero AFG. Reducing the global prevalence of cardiometabolic risk factors: a bet worth winning. Metabolism. 2025;163.
8. Lee SY, Pearce EN. Hyperthyroidism: a review. JAMA. 2023;330(15):1472–1483. doi:10.1001/jama.2023.19052
9. Yuan Q, Yue X, Wang M, et al. Association between pain, sleep and intrinsic capacity in Chinese older adults: evidence from CHARLS. J Nutr Health Aging. 2024;29(3):100466. doi:10.1016/j.jnha.2024.100466
10. Weiner IH, Weiner HL. Nocturnal leg muscle cramps. JAMA. 1980;244(20):2332–2333. doi:10.1001/jama.1980.03310200066033
11. Guay DR. Are there alternatives to the use of quinine to treat nocturnal leg cramps? Consult Pharm J Am Soc Consult Pharm. 2008;23:141–156.
12. Wise J. Long term quinine for muscle cramps may increase death risk. BMJ. 2017;j2236. doi:10.1136/bmj.j2236
13. Brinker AD, Beitz J. Spontaneous reports of thrombocytopenia in association with quinine: clinical attributes and timing related to regulatory action. Am J Hematol. 2002;70(4):313–317. doi:10.1002/ajh.10148
14. Man-Son-Hing M, Wells G. Meta-analysis of efficacy of quinine for treatment of nocturnal leg cramps in elderly people. BMJ. 1995;310(6971):13–17. doi:10.1136/bmj.310.6971.13
15. Barna O, Lohoida P, Holovchenko Y, et al. A randomized, double-blind, placebo-controlled, multicenter study assessing the efficacy of magnesium oxide monohydrate in the treatment of nocturnal leg cramps. Nutr J. 2021;20(1):90. doi:10.1186/s12937-021-00747-9
16. Garrison SR, Korownyk CS, Kolber MR, et al. Magnesium for skeletal muscle cramps. Cochrane Database Syst Rev. 2020;9:CD009402.
17. Tan J, Zhu R, Li Y, et al. Vitamin K 2 in managing nocturnal leg cramps. JAMA Intern Med. 2024;184(12):1443–1447. doi:10.1001/jamainternmed.2024.5726
18. Kim HJ, Yoon KB, Kang M, Lee HW, Kim SH. Use of baclofen as a treatment for nocturnal calf cramps in individuals with lumbar spinal stenosis: a prospective randomized study. Am J Phys Med Rehabil. 2024;103(5):384. doi:10.1097/PHM.0000000000002364
19. Hallegraeff JM, Van Der Schans CP, De Ruiter R, De Greef MHG. Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in older adults: a randomised trial. J Physiother. 2012;58(1):17–22. doi:10.1016/S1836-9553(12)70068-1
20. Ge H-Y, Arendt-Nielsen L. Latent myofascial trigger points. Curr Pain Headache Rep. 2011;15(5):386–392. doi:10.1007/s11916-011-0210-6
21. Hawke F, Sadler SG, Katzberg HD, Pourkazemi F, Chuter V, Burns J. Non-drug therapies for the secondary prevention of lower limb muscle cramps. Cochrane Database Syst Rev. 2021;5(5):CD008496. doi:10.1002/14651858.CD008496.pub3
22. Kaptchuk TJ. Acupuncture: theory, efficacy, and practice. Ann Intern Med. 2002;136(5):374–383. doi:10.7326/0003-4819-136-5-200203050-00010
23. Xu Y-L, Sun G-M, Zhang J-M, et al. Regulating the Wnt/ β -catenin signaling pathway promotes repigmentation in vitiligo using fire needle therapy. Dermatol Ther. 2024;2024(1):8522969. doi:10.1155/2024/8522969
24. Lin LJ, Xu JS, Zhu XX, et al. Development on research on of acupuncture effects on microcirculation. Chin Acupunc Moxibust. 2015;35(02):203–208. doi:10.13703/j.0255-2930.2015.02.030
25. Shao Y. Meta-analysis comparing traditional acupuncture points and ashi-points: delayed onset muscle soreness. Med Sci Sports Exerc. 2024;56(10S):75. doi:10.1249/01.mss.0001053136.16367.73
26. Gao F, Shao B, Li B, et al. The curative effect of fire needling combined with filiform needling on tension-type headache and its effect on the tenderness of pericranial muscles. Zhenci Yanjiu. 2023;48(11):1151–1158. doi:10.13702/j.1000-0607.20230189
27. Yue X, Feng Z, Yu X, Hu J, He X, Shu S. Fire-needle acupuncture for upper limb spastic paralysis after stroke: study protocol for a randomized controlled trial. J Integr Med-Jim. 2019;17(3):167–172. doi:10.1016/j.joim.2019.03.002
28. Qiu X, Gao Y, Zhang Z, Cheng S, Zhang S. Fire acupuncture versus conventional acupuncture to treat spasticity after stroke: a systematic review and meta-analysis. PLoS One. 2021;16:e0249313.
29. Shah JP, Thaker N, Heimur J, Aredo JV, Sikdar S, Gerber L. Myofascial trigger points then and now: a historical and scientific perspective. Pm&r. 2015;7(7):746–761. doi:10.1016/j.pmrj.2015.01.024
30. Kim D-H, Yoon DM, Yoon KB. The effects of myofascial trigger point injections on nocturnal calf cramps. J Am Board Fam Med. 2015;28(1):21–27. doi:10.3122/jabfm.2015.01.140151
31. Frost FA, Jessen B, Siggaard-Andersen J. A control, double-blind comparison of mepivacaine injection versus saline injection for myofascial pain. Lancet Lond Engl. 1980;1(8167):499–500. doi:10.1016/S0140-6736(80)92761-0
32. Jiménez-Sánchez C, Gómez-Soriano J, Bravo-Esteban E, et al. Effects of dry needling on biomechanical properties of the myofascial trigger points measured by myotonometry: a randomized controlled trial. J Manipulative Physiol Ther. 2021;44(6):467–474. doi:10.1016/j.jmpt.2021.06.002
33. Chan A-W, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomised trials. BMJ. 2025;389:e081477.
34. Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet. 2001;357(9263):1191–1194. doi:10.1016/S0140-6736(00)04337-3
35. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348(mar07 3):g1687. doi:10.1136/bmj.g1687
36. Goddard G, Shen Y, Steele B, Springer N. A controlled trial of placebo versus real acupuncture. J Pain. 2005;6(4):237–242. doi:10.1016/j.jpain.2004.12.009
37. Chae Y, Lee Y-S, Enck P. How placebo needles differ from placebo pills? Front Psychiatry. 2018;9:243. doi:10.3389/fpsyt.2018.00243
38. Johanson GA, Brooks GP. Initial scale development: sample size for pilot studies. Educ Psychol Meas. 2010;70(3):394–400. doi:10.1177/0013164409355692
39. Cocks K, Torgerson DJ. Sample size calculations for pilot randomized trials: a confidence interval approach. J Clin Epidemiol. 2013;66(2):197–201. doi:10.1016/j.jclinepi.2012.09.002
40. Arain M, Campbell MJ, Cooper CL, Lancaster GA. What is a pilot or feasibility study? A review of current practice and editorial policy. BMC Med Res Methodol. 2010;10(1):67. doi:10.1186/1471-2288-10-67
41. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. 2010;10(1):1. doi:10.1186/1471-2288-10-1
42. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
43. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
44. Liu T, Jiang L, Li S, et al. The blinding status and characteristics in acupuncture clinical trials: a systematic reviews and meta-analysis. Syst Rev. 2024;13(1):302. doi:10.1186/s13643-024-02692-0
45. Chae Y, Lee J-H, Lee MS. Using the right design controls for acupuncture trials: methodological rigor and validity in research. Integr Med Res. 2024;13(1):101026. doi:10.1016/j.imr.2024.101026
46. Yang J, Liu J, Luo X, et al. Blinding assessment in randomised sham-controlled trials of acupuncture:protocol for a systematic survey. BMJ Open. 2025;15:e090238.
47. Welch VA, Norheim OF, Jull J, et al. CONSORT-equity 2017 extension and elaboration for better reporting of health equity in randomised trials. BMJ. 2017;359:j5085.
48. Dai L, Cheng C-W, Tian R, et al. Standard protocol items for clinical trials with traditional Chinese medicine 2018: recommendations, explanation and elaboration (SPIRIT-TCM extension 2018). Chin J Integr Med. 2019;25(1):71–79. doi:10.1007/s11655-018-2999-x
49. MacPherson H, Altman DG, Hammerschlag R, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. Acupunct Relat Ther. 2015;3(4):35–46. doi:10.1016/j.arthe.2016.03.001
50. Xue LG, Zhang HR. Meridian Sinew Theory and Clinical Diagnosis & Treatment of Pain Disorders, in Chinese.
51. Liu L, Skinner M, McDonough SM, Kannan P, Baxter GD. STRICTA: is it time to do more? BMC Complement Altern Med. 2015;15(1):190. doi:10.1186/s12906-015-0714-4
52. Roguin Maor N, Alperin M, Shturman E, et al. Effect of magnesium oxide supplementation on nocturnal leg cramps: a randomized clinical trial. JAMA Intern Med. 2017;177(5):617. doi:10.1001/jamainternmed.2016.9261
53. Haueise A, Le Sant G, Eisele-Metzger A, Dieterich AV. Is musculoskeletal pain associated with increased muscle stiffness? Evidence map and critical appraisal of muscle measurements using shear wave elastography. Clin Physiol Funct Imaging. 2024;44(3):187–204. doi:10.1111/cpf.12870
54. Wang X, Zhu J, Gao J, et al. Assessment of ultrasound shear wave elastography within muscles using different region of interest sizes, manufacturers, probes and acquisition angles: an ex vivo study. Quant Imaging Med Surg. 2022;12(6):3227–3237. doi:10.21037/qims-21-1072
55. Zeng D, Yan X, Deng H, et al. Placebo response varies between different types of sham acupuncture: a randomized double-blind trial in neck pain patients. Eur J Pain. 2022;26(5):1006–1020. doi:10.1002/ejp.1924
56. Moroz A, Freed B, Tiedemann L, Bang H, Howell M, Park JJ. Blinding measured: a systematic review of randomized controlled trials of acupuncture. Evid Based Complement Alternat Med. 2013;2013:708251. doi:10.1155/2013/708251
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.