")
Back to Journals » Infection and Drug Resistance » Volume 16
Fire Needle Combined Topical Mupirocin for the Treatment of Simple Skin Abscesses in Pediatric Patients: A Case Series
Authors Li M , Zhu X, Cao Z , Du L , Wei J , Zhang C
Received 2 May 2023
Accepted for publication 8 June 2023
Published 12 June 2023 Volume 2023:16 Pages 3683—3692
DOI https://doi.org/10.2147/IDR.S416917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Mingming Li, Xia Zhu, Zhiqiang Cao, Lingyun Du, Jingjing Wei, Chunhong Zhang
Department of Dermato-Venereology, the Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China
Correspondence: Chunhong Zhang, Department of Dermato-Venereology, the Second Hospital, Cheeloo College of Medicine, Shandong University, 247 Beiyuan Street, Jinan, Shandong, 250033, People’s Republic of China, Fax +86-531-88962544, Email [email protected]
Background: Skin abscesses are a common skin condition usually caused by bacterial infections and their incidence is increasing in children. Its current management strategy is still mainly incision and drainage, sometimes with antibiotics. In pediatric patients, surgical incision and drainage of skin abscesses is challenging compared to in adults because of their specific age and psychological characteristics and high aesthetic requirements. Therefore, it is important to seek better treatment options.
Patients and methods: We reported 17 cases of skin abscesses in pediatric patients aged 1 to 9 years. Ten cases had lesions on the face and neck and 7 cases on the trunk and limbs. They all received treatment based on fire needle combined with topical mupirocin.
Results: The lesions of all 17 pediatric patients healed within 4 to 14 days, with a median time of 6 days, and all achieved satisfactory results with no scarring left behind. No adverse events were observed in all patients, and no recurrence occurred within 4 weeks.
Conclusion: For skin abscesses in pediatric patients, early application of a combination therapy based on fire needle is convenient, aesthetic, economical, safe and clinically important as an alternative to incision and drainage, and deserves further clinical promotion.
Keywords: fire needle combined therapy, simple skin abscesses, pediatric patients, mupirocin
Introduction
Skin abscesses are a common skin disease in which pus accumulates in the dermis or subcutaneous tissue, usually caused by a bacterial infection, and their incidence is increasing in children.1–3 Clinical signs of skin abscesses include erythema, swelling, pain, fluctuating lumps and pus oozing.4 Skin abscesses are usually 1–3 cm long in diameter and can sometimes be larger. Single abscesses up to 5 cm in diameter (3 cm in patients aged 6–11 months, 4 cm in patients aged 1–8 years) are classified as simple skin abscesses.5,6 The incision and drainage procedure is the main treatment option for skin abscesses, and antibiotics such as clindamycin and mupirocin have been shown to improve outcomes.7,8 However, antibiotics alone can sometimes be ineffective due to the worldwide spread of antimicrobial resistance, and the disease continues to progress.9,10 For skin abscesses that do not drain independently, the mainstay of treatment remains incision and drainage (I&D).6 But incision and drainage can be relatively more challenging for pediatric patients. Children are in a critical period of growth and psychological development and are extremely demanding in aesthetics,11 they are more reluctant to undergo incision and drainage procedures than adults.12 Surgery is particularly problematic for pediatric patients who may require sedation, and post-operative care is more difficult than for adults.13 Furthermore, the surgical incision and stuffing with gauze is extremely painful for children and the tamponade may be removed, making a second operation more likely.14 Although Ladde JG, Rencher L et al advocated the use of the new minimally invasive LOOP technique as an alternative to standard incision and drainage and tamponade treatment, it still carried some risk of leaving a surgical scar and requiring a second incision if treatment fails.15,16 According to Ladde JG, the treatment failure rate of the I&D and LOOP methods in treating skin abscesses of children was 16.5% and 3.9% respectively.15 Rencher L reported that the treatment failure rates of LOOP and I&D were 7.3% and 7.5%, with the parental dissatisfaction rates of on day 14 after surgery 13.9% and 11.8% respectively.16 Therefore, searching for better treatments is the key to solving such problems.
Fire needle is one of the three main types of acupuncture in Chinese medicine and has a history of thousands of years. According to the literature reports, fire needle therapy is widely used in surgery, gynecology, orthopedics and internal medicine.17 It is also considered an effective treatment for skin diseases such as psoriasis, vitiligo, and acne.18–20 According to the literature review, fire needle therapy can accelerate local blood circulation and reduce pathological changes in local tissue such as edema, congestion, and exudation.21 Furthermore, the fire needle directly stimulates the lesion and raises the skin temperature around the lesion, thus accelerating metabolism and promoting the repair of damaged tissue.22 Clinical trials and animal studies have shown that the specific mechanisms of fire needle therapy include the following aspects: regulating the secretion of cytokines such as reducing IL-6, TNF-α, IL-1β and increasing IL-10, promoting the release of growth factors such as VEGF, and regulating the proportion of immune cells such as increasing the number of CD4+ T cells and type 2 helper T cells.20,23,24 In recent years, fire needle therapy has also been reported to treat bacterial infectious skin diseases, including perifolliculitis capitis abscedens et suffodiens, carbuncle of neck.25,26 But there is little evidence from clinical studies on treating skin abscesses with fire needle. Most of the patients in the previous clinical studies on fire needle therapy were adults, and the clinical efficacy of fire needle in the treatment of children with skin abscesses is still unclear.
In this paper, we report our experience in treating 17 cases of pediatric patients with skin abscesses successfully by using fire needle combined therapy. It avoided further disease progression, surgical incision and drainage, and brought about satisfactory clinical effect and fantastic cosmetic results.
Methods
The study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice Guidelines. Ethical approval has been confirmed by the Research Ethics Committee of the Second Hospital of Shandong University (No. KYLL-2023LW010). We confirmed that all guardians of the pediatric patients gave informed consent, signed the informed consent form and agreed to be published in this study.
Inclusion Criteria
We included children aged 1 to 12 years diagnosed with uncomplicated simple skin abscesses at the Second Hospital of Shandong University with two or more of the following signs or symptoms for at least 24 hours: erythema, swelling or hard nodules, localized fever, purulent drainage, pain or pressure to touch; refusal of incision and drainage or contraindication to incision and drainage.
Exclusion Criteria
This included superficial skin infections, multiple abscesses, abscesses < 1cm or > 5cm, history of dizziness from acupuncture, coagulation disorders, liver and kidney disease and other disorders that possibly affect the results.
Treatment Options
The lesion was routinely disinfected with iodophor and prepared for fire needle treatment. A disposable sterile stainless-steel needle (0.30 × 25 mm, China Wujiang Yunlong Medical Instrument Co Ltd) was selected. (Figure 1A) The lower part of the needle was heated with an alcohol lamp until the tip and front burned red. (Figure 1B) The needle was then rapidly and accurately inserted into the skin abscess lesion (approximately at a depth of the skin abscess capsule wall) at a 90° angle for about 0.5 s and then rapidly removed. We selected the appropriate number of needles during the treatment according to the patient’s tolerance. The distance between needles on the lesion was about 0.5 cm. After puncturing the skin with the fire needle, the blood and pus was gently squeezed and cleaned with a cotton swab. During the treatment, for skin lesions on the face, especially on the upper lip and the dangerous triangle of the nose, the pus should be squeezed gently so that it flows out as naturally as possible to avoid the infection spreading caused by forced extrusion and discharge of pus. Finally, using a sterile cotton swab, we applied a 0.5 mm thick layer of mupirocin ointment to the affected area. After treatment, patients were asked to apply the same thickness of mupirocin ointment to the lesion twice daily. The lesion was not to be exposed to water or skin care products within 24 hours.
 |
Figure 1 Needle used in fire needle therapy in this study (A). Fire needle therapy (B). |
Observation Indicators
Pain Level
The pain level was assessed using the Face, Legs, Activity, Cry, and Consolability (FLACC), with higher values indicating greater pain.27,28 1 to 3 were classified as mild pain, 4 to 6 as moderate pain and 7 to 10 as severe pain. The scores were 0, 1, 2 and 3 on a scale of no, mild, moderate and severe pain.
Skin Lesion Level
Erythema or mild pigmentation, nodules, pustules and purulent discharge are scored 0, 1, 2 and 3 in that order.
Efficacy Index and Efficacy Rating
Total score = pain level score + skin lesion level score. The Efficacy Index is calculated based on the total score before and after 7 days of treatment [(total score before treatment - total score after 7 days of treatment)/total score before treatment × 100%]. There were four levels of efficacy: complete remission (CR): Efficacy Index of 100%; significant remission (SR): 60% ≤ Efficacy Index ≤ 99%; partial remission (PR): 30% ≤ Efficacy Index ≤ 59%; no remission (NR): Efficacy Index < 30% or worsening of symptoms (Table 1).
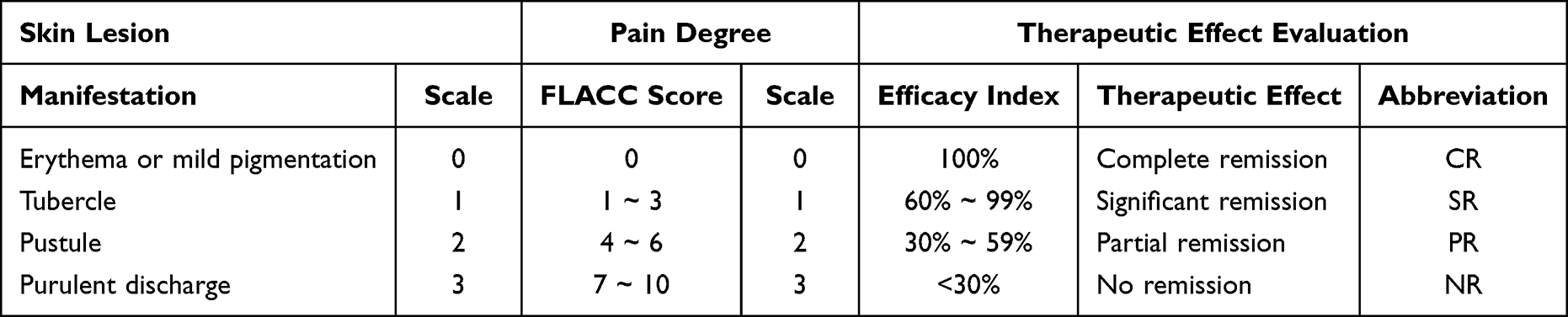 |
Table 1 Quantitative Criteria for Grading of Disease |
Basic Healing Time
Basic healing meant that the pain and the redness, nodules and pustules of the lesions had subsided, there was no flow of pus or exudate and only slight erythema or pigmentation of the skin remained. “Days” were used as the unit of measurement for basic healing time.
Adverse Reactions
Patients were observed for adverse reactions such as scarring, poor mobility and infection during the treatment.
Data Collection
Demographic data and clinical information were recorded. For all patients, images of skin lesions in normal ambient light were obtained before the start of treatment and during each treatment and follow-up, and the above observations were recorded. The clinical characteristics of all cases were analyzed. The data collected were subjected to descriptive statistics using SPSS 25.0 software.
The follow-up period was 3 days, 1 week, 2 weeks and 4 weeks after the initial fire needle treatment. Follow-up was terminated when recurrence was observed.
Results
A total of 17 pediatric patients, 10 females and 7 males, aged 1 to 9 years, were included in this study. The duration of the disease ranged from 3 to 12 days, with a median duration of 6 days. Lesions were located on the face in 9 patients, on the neck in 1 patient, on the limbs in 4 patients, and on the trunk in 3 patients (Table 2). All the above patients received the characteristic Chinese medicine treatment of fire needle combined with topical mupirocin (twice a day until basic healing). After receiving fire needle combined therapy, 11 cases achieved complete remission (CR) with an efficacy index of 100% at 1 week after treatment; 6 cases achieved significant remission (SR) with an efficacy index of 60% - 99% at 1 week after treatment and 100% within 2 weeks after treatment. (Table 3) Before treatment, the median Skin Lesion Scale and Pain Degree Scale of patients were both 2, which decreased to 0 after treatment. The degrees of skin lesion and pain were significantly reduced in all patients after treatment (P<0.001), and the overall efficacy index after seven days of treatment was 100%. The basic healing time was as fast as 4 days and as slow as 14 days, with a median of 7 days. (Table 4 and Table 5) Representative images are shown in Figures 2 and 3. At the follow-up of 3 days, 1 week, 2 weeks and 4 weeks after the treatment, there was no scar growth or other cosmetic problems, which did not affect the aesthetics; simultaneously, the muscles moved freely without nerve damage. All patients had no recurrence within 4 weeks of treatment.
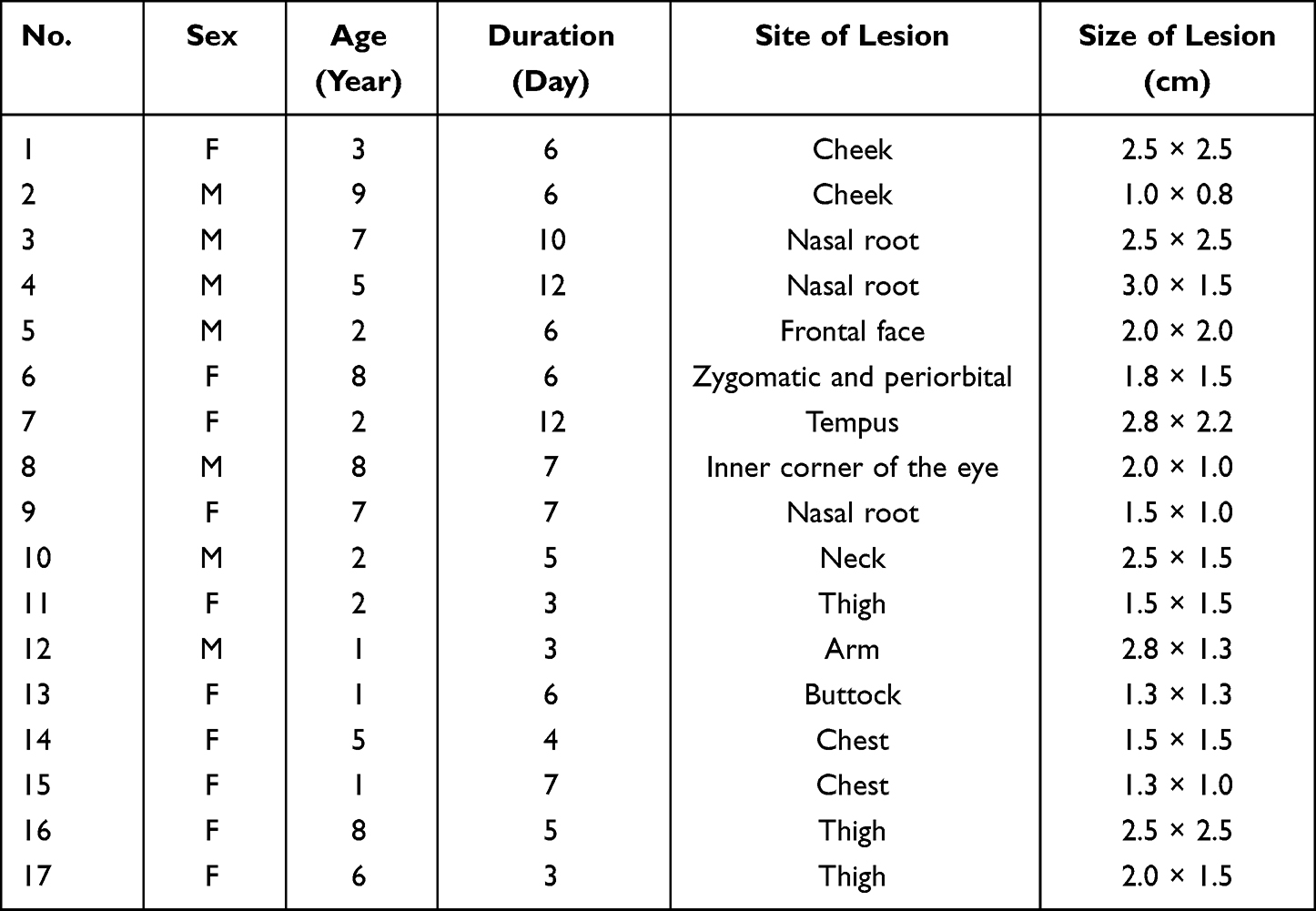 |
Table 2 Demographic and Clinical Characteristics of Patients |
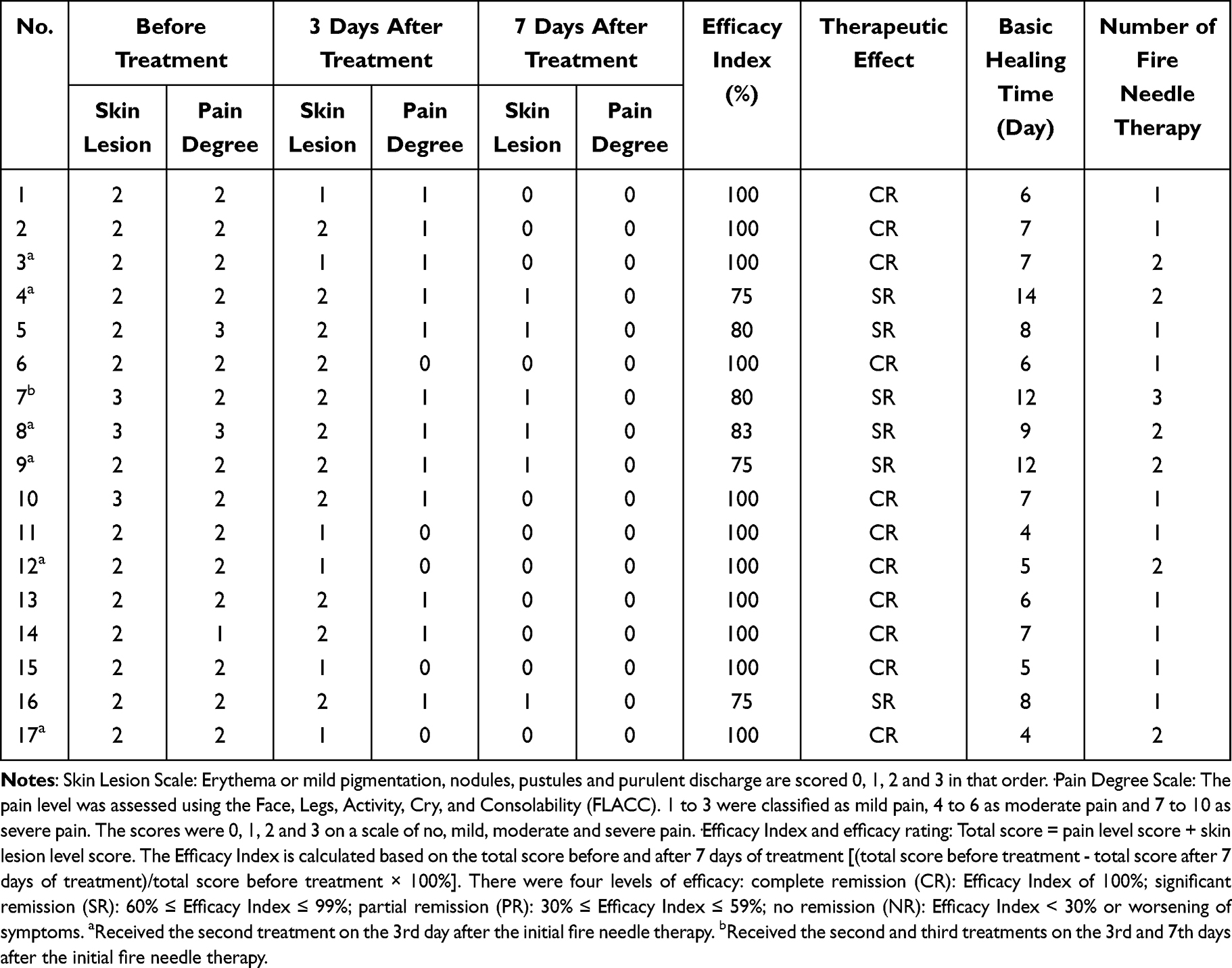 |
Table 3 Efficacy and Follow-Up of Patients |
 |
Table 4 Summary of 17 Cases of Simple Skin Abscesses in Pediatric Patients |
 |
Table 5 Comparison of Skin Lesion and Pain Degree Before and After Treatment |
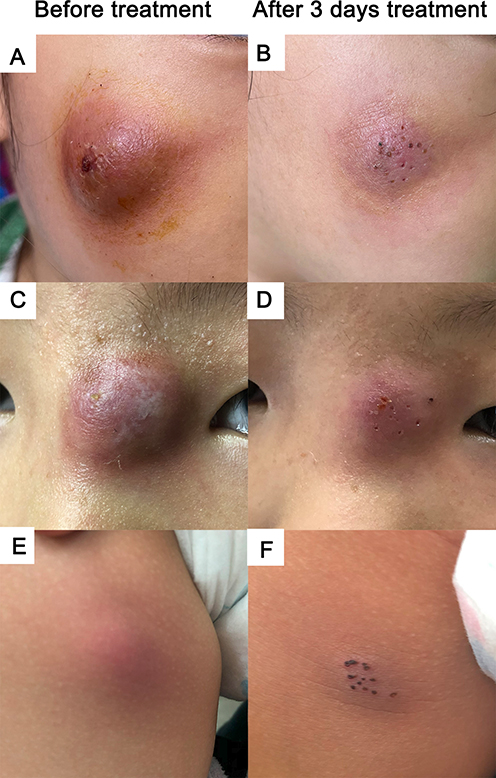 |
Figure 2 Case1: A skin abscess on the face of a 3-year-old child before (A) and after (B) 3 days of fire needle combined therapy. Case 3: A skin abscess on the nasal root of a 7-year-old child before (C) and after (D) 3 days of fire needle combined therapy. Case 13: A skin abscess on the buttock of a 1-year-old child before (E) and after (F) 3 days of fire needle combined therapy. |
 |
Figure 3 Case 4: A skin abscess on the nasal root of a 5-year-old child before (A) and after (B) 7 days of fire needle combined therapy. Case 8: A skin abscess on the inner corner of the eye of an 8-year-old child before (C) and after (D) 7 days of fire needle combined therapy. Case 12: A skin abscess on the arm of a 1-year-old child before (E) and after (F) 7 days of fire needle combined therapy. (All three patients received two needle treatments, with a 3-day interval between the second treatment and the first). |
All treatments were well tolerated. The pain caused by fire needle was mild to moderate and tolerable, and subsided quickly after the treatment. No other adverse effects such as infection or scarring were found in this study.
Discussion
We reported 17 cases of simple skin abscesses in children who used fire needle combined therapy. The lesions of 10 patients were located on the face and neck, and the other 7 cases were located in important functional areas of the trunk and extremities. After 7 days of treatment with fire needle combined therapy, all patients’ pain degrees were reduced to 0, and 65% of patients had only erythema or mild pigmentation left in their skin lesions. The overall treatment efficiency was 100%, with 65% of patients achieving complete remission on the Efficacy Index. Overall, all patients achieved satisfactory clinical and cosmetic effects with rapid pain reduction and significant reduction of redness and swelling after treatment.
Currently, topical antibiotics are used in the treatment of skin abscesses in addition to the main incision and drainage therapy, but antibiotic use alone is sometimes ineffective due to bacterial resistance and skin barriers to the drug.9,10 In this case series, all patients treated with fire needle combined with topical medication achieved satisfactory clinical outcomes. The high temperature of fire needle can kill pathogenic microorganisms and strengthen the antibacterial and anti-inflammatory effects. At the same time, the tiny holes left by the fire needles can weaken the skin barrier against the penetration of topical drugs, facilitate the transdermal absorption of antibiotic ointments and help to reduce antibiotic resistance.29 Liu Z et al reported the successful treatment of three cases of carbuncle on the neck in adult patients using a therapy based on fire needle combined with antibiotics. Early and timely treatment with fire needle combined therapy was considered beneficial in controlling the further progression of the disease and minimally invasive treatment.25 In our study, patients 11, 12 and 17 applied fire needle therapy at an early stage and had a shorter basic healing time, demonstrating the effectiveness of fire needle in the early stage of skin abscesses in children as well. Therefore, early application of combined treatment with fire needle combined therapy can prevent further aggravation of the skin abscess and avoid the impact of surgical incision and drainage on the patient’s quality of life.
Among the 10 pediatric patients with lesions on the face and neck, 6 cases were extremely challenging because their lesions were located in areas such as the periocular and nasal regions, where surgical incision was inconvenient and could lead to the risk of infection. For facial skin abscesses, early incision, wound enlargement or improper treatment can result in the spread of infection, especially in areas such as the dangerous triangle of the face, prone to suppurative cavernous vein sinusitis, eye and surrounding tissue inflammation. Pannu AK reported a case of a furuncle on the tip of the nose that developed into a septic cavernous sinus thrombosis.30 However, pediatric patients do not accept conventional surgical incision and drainage easily as surgery tends to affect appearance.31,32 In addition, post-operative scarring can be a problematic issue as the expressions and movements of children are not easily managed.33 The above pediatric patients were treated with fire needle combined therapy and the painful symptoms disappeared quickly and the lesions healed satisfactorily, stopping the progression of the disease and avoiding surgical incisions. Compared to surgical incision and drainage, the fire needle has the function of sterilizing and hemostatic effect at high temperatures, allowing for less bleeding by burning the small local blood vessels. Moreover, the fire needle is a substitute for a scalpel, which also facilitates the unobstructed drainage of pus through a small wound, resulting in faster healing with a smaller opening and avoiding the aesthetic and psychological impact of post-operative scarring.34
At post-treatment follow-up, all pediatric patients had no significant cosmetic problems, muscle and nerve dysfunction, and no recurrences within 4 weeks. During our literature collection, we found that literature relating to fire needle therapy overwhelmingly demonstrates the safety and effectiveness of this treatment, only Huang M reported two patients with hyperplastic scars after fire needle therapy that resolved after multiple injections of tretinoin.18 Therefore, we advocate that fire needle therapy should be applied to patients with non-cicatricial constitution and performed by professionals whenever possible.
Although this case series fills a gap in the outcome evidence for the treatment of skin abscesses in children with fire needle therapy, the data are limited by the relatively small sample size. High-quality studies such as randomized controlled studies on more diverse samples are needed to assess further the value of fire needling in the treatment of skin abscesses.
Conclusion
Pediatric patients, especially those with skin abscesses in areas with high cosmetic or functional requirements such as the face and neck, have a relatively large aesthetic demand and incision and drainage is highly challenging. Fire needle combined therapy can significantly improve skin lesions and relieve pain and may be a more preferred treatment option in appropriate circumstances. This therapy has the advantages of less bleeding, no cosmetic impact, simple operation, and reliable curative effect, which is worthy of further research and promotion.
Ethics Approval and Informed Consent
The research was conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice guidelines. Our research has been approved by the Research Ethics Committee of the Second Hospital of Shandong University, with the number KYLL-2023LW010. The guardians of 17 patients provided written informed consent for publication of this study and accompanying images.
Acknowledgments
All authors thank the operator of cases, Changyu Han. We also thank all patients and their guardians for their consent to the publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81973856).
Disclosure
All authors report no conflicts of interest in this work.
References
1. L GF-B, Borrull Senra AM, Pérez Velasco C, et al. Rate of methicillin-resistant Staphylococcus aureus in pediatric emergency departments in Spain. An Pediatr. 2022;97(2):95–102. doi:10.1016/j.anpede.2021.06.015
2. Qualls ML, Mooney MM, Camargo CA, Zucconi T, Hooper DC, Pallin DJ. Emergency department visit rates for abscess versus other skin infections during the emergence of community-associated methicillin-resistant Staphylococcus aureus, 1997-2007. Clin Infect Dis. 2012;55(1):103–105. doi:10.1093/cid/cis342
3. Hsiao CB, Dryja D, Abbatessa L, Patel PH. Staphylococcus aureus antimicrobial susceptibility of abscess samples from adults and children from the Kaleida Health System in western New York State, 2003 to 2006. J Clin Microbiol. 2010;48(5):1753–1757. doi:10.1128/jcm.01065-08
4. Gorwitz RJ. A review of community-associated methicillin-resistant Staphylococcus aureus skin and soft tissue infections. Pediatr Infect Dis J. 2008;27(1):1–7. doi:10.1097/INF.0b013e31815819bb
5. Singer AJ, Talan DA. Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. N Engl J Med. 2014;370(11):1039–1047. doi:10.1056/NEJMra1212788
6. Galli L, Venturini E, Bassi A, et al. Common Community-acquired Bacterial Skin and Soft-tissue Infections in Children: an Intersociety Consensus on Impetigo, Abscess, and Cellulitis Treatment. Clin Ther. 2019;41(3):532–551.e517. doi:10.1016/j.clinthera.2019.01.010
7. Alhasso B, Ghori MU, Conway BR. Development of Nanoemulsions for Topical Application of Mupirocin. Pharmaceutics. 2023;15(2). doi:10.3390/pharmaceutics15020378
8. Murray H, Leifso K. Just the Facts: methicillin-resistant Staphylococcus aureus and soft tissue abscess in the emergency department. CJEM. 2020;22(2):149–151. doi:10.1017/cem.2019.452
9. Moore SJ, O’Leary ST, Caldwell B, et al. Clinical characteristics and antibiotic utilization in pediatric patients hospitalized with acute bacterial skin and skin structure infection. Pediatr Infect Dis J. 2014;33(8):825–828. doi:10.1097/inf.0000000000000304
10. Chen M, Zhou J, Ran P, et al. Photoactivated Release of Nitric Oxide and Antimicrobial Peptide Derivatives for Synergistic Therapy of Bacterial Skin Abscesses. Adv Healthc Mater. 2022;11(12):e2200199. doi:10.1002/adhm.202200199
11. Marshall CD, Hu MS, Leavitt T, Barnes LA, Lorenz HP, Longaker MT. Cutaneous Scarring: basic Science, Current Treatments, and Future Directions. Adv Wound Care. 2018;7(2):29–45. doi:10.1089/wound.2016.0696
12. Volpicelli L, Venditti M, Oliva A. Acute bacterial skin and skin structure infections in pediatric patients: potential role of dalbavancin. Expert Rev Anti Infect Ther. 2023;21(4):329–341. doi:10.1080/14787210.2023.2182769
13. Baumann BM, Russo CJ, Pavlik D, et al. Management of pediatric skin abscesses in pediatric, general academic and community emergency departments. West J Emerg Med. 2011;12(2):159–167.
14. Brody AM, Gallien J, Murphy D, Marogil J. A Novel Silicon Device for the Packing of Cutaneous Abscesses. J Emerg Med. 2019;56(3):298–300. doi:10.1016/j.jemermed.2018.12.009
15. Ladde JG, Baker S, Rodgers CN, Papa L. The LOOP technique: a novel incision and drainage technique in the treatment of skin abscesses in a pediatric ED. Am J Emerg Med. 2015;33(2):271–276. doi:10.1016/j.ajem.2014.10.014
16. Rencher L, Whitaker W, Schechter-Perkins E, Wilkinson M. Comparison of Minimally Invasive Loop Drainage and Standard Incision and Drainage of Cutaneous Abscesses in Children Presenting to a Pediatric Emergency Department: a Prospective, Randomized, Noninferiority Trial. Pediatr Emerg Care. 2021;37(10):e615–e620. doi:10.1097/pec.0000000000001732
17. Ifrim Chen F, Antochi AD, Barbilian AG. Acupuncture and the retrospect of its modern research. Rom J Morphol Embryol. 2019;60(2):411–418.
18. Huang M, Tang L, Li X, et al. Clinical observation on therapeutic effect of filiform fire needle for vitiligo: a retrospective study. Dermatol Ther. 2020;33(6):e14415. doi:10.1111/dth.14415
19. Shi L, Yang Y, Zhang L, et al. Efficacy and therapeutic reactions of tri-needle-pretreatment combined with painless ALA-PDT for the treatment of moderate-to-severe acne vulgaris: a randomized controlled trial. Photodiagnosis Photodyn Ther. 2022;37:102680. doi:10.1016/j.pdpdt.2021.102680
20. Liu L, Sun XY, Lu Y, et al. Fire Needle Therapy for the Treatment of Psoriasis: a Quantitative Evidence Synthesis. J Altern Complement Med. 2021;27(1):24–37. doi:10.1089/acm.2019.0409
21. Lin JG, Kotha P, Chen YH. Understandings of acupuncture application and mechanisms. Am J Transl Res. 2022;14(3):1469–1481.
22. Wang H, Gu Y, Huang L, et al. Effectiveness of fire needle combining with moist healing dressing to promote the growth of granulation tissue in chronic wounds: a case report. Int J Nurs Sci. 2020;7(3):386–390. doi:10.1016/j.ijnss.2020.05.008
23. Pan HD, Qi XL, Wang L, et al. Whether Fire-needle Therapy Benefits Plaque Psoriasis: a Multicenter, Randomized, and Controlled Trial. Chin J Integr Med. 2019;25(4):259–263. doi:10.1007/s11655-018-2940-8
24. Li ZJ, Wang X, Sun JQ, et al. Effect of fire-needle intervention on joint function, cartilage impairment and inflammatory response in knee osteoarthritis rats. Zhen Ci Yan Jiu. 2020;45(3):220–226. doi:10.13702/j.1000-0607.190963
25. Liu Z, Wei J, Cao Z, Zhu X, Zhang C. Fire Needle Combined Therapy or Surgery Therapy for Carbuncle of Neck? A Case Series. Infect Drug Resist. 2022;15:7293–7299. doi:10.2147/idr.S391381
26. Su Y, Xu Q, Zhang C, Zhang C. Photodynamic therapy pre-treated by fire needle combined with isotretinoin in the treatment of refractory perifolliculitis capitis abscedens et suffodiens: case report. Photodiagnosis Photodyn Ther. 2021;33:102103. doi:10.1016/j.pdpdt.2020.102103
27. Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23(3):293–297.
28. Crellin DJ, Harrison D, Santamaria N, Huque H, Babl FE. The Psychometric Properties of the FLACC Scale Used to Assess Procedural Pain. J Pain. 2018;19(8):862–872. doi:10.1016/j.jpain.2018.02.013
29. Jo HR, Choi SK, Sung WS, Lee SD, Lee BW, Kim EJ. Thermal Properties of Warm- versus Heated-Needle Acupuncture. Evid Based Complement Alternat Med. 2022;2022:4159172. doi:10.1155/2022/4159172
30. Pannu AK, Saroch A, Sharma N. Danger Triangle of Face and Septic Cavernous Sinus Thrombosis. J Emerg Med. 2017;53(1):137–138. doi:10.1016/j.jemermed.2017.03.016
31. Hom DB. Facial Scar Management. Facial Plast Surg Clin North Am. 2017;25(1):ix–x. doi:10.1016/j.fsc.2016.10.001
32. McNamara WF, Hartin CW, Escobar MA, Yamout SZ, Lau ST, Lee YH. An alternative to open incision and drainage for community-acquired soft tissue abscesses in children. J Pediatr Surg. 2011;46(3):502–506. doi:10.1016/j.jpedsurg.2010.08.019
33. Mobley SR, Sjogren PP. Soft tissue trauma and scar revision. Facial Plast Surg Clin North Am. 2014;22(4):639–651. doi:10.1016/j.fsc.2014.07.007
34. Zhang HH, Zhang CM, Xu QQ, Zhang CH. Effective Treatment of Small Uncomplicated Skin Abscesses with Fire Needle: a Case Series. Infect Drug Resist. 2021;14:4085–4090. doi:10.2147/idr.S327089
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.