")
Back to Journals » International Journal of General Medicine » Volume 16
Fibrinogen-to-Albumin Ratio in Neonatal Sepsis
Authors Dong G, Ma T, Xu Z, Zhang M, Hu Y, Yang J, Li T
Received 12 August 2023
Accepted for publication 23 October 2023
Published 31 October 2023 Volume 2023:16 Pages 4965—4972
DOI https://doi.org/10.2147/IJGM.S432903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Geng Dong,1 Tingting Ma,2 Zhe Xu,1 Min Zhang,1 Yidi Hu,1 Junmei Yang,1 Tiewei Li1
1Zhengzhou Key Laboratory of Children’s Infection and Immunity, Children’s Hospital Affiliated to Zhengzhou University, Henan Children’s Hospital, Zhengzhou Children’s Hospital, Zhengzhou, People’s Republic of China; 2Department of Neurology, Children’s Hospital Affiliated to Zhengzhou University, Henan Children’s Hospital, Zhengzhou Children’s Hospital, Zhengzhou, People’s Republic of China
Correspondence: Tiewei Li, Email [email protected]
Background: Previous studies have established an association between fibrinogen-to-albumin ratio (FAR) and cancer, cardiovascular disease, and coronavirus disease 2019. However, no studies have investigated the relationship between FAR and neonatal sepsis. This study aims to evaluate the association of fibrinogen-to-albumin ratio with the presence and severity of sepsis in neonates.
Methods: A total of 1292 neonates with suspected sepsis were enrolled in this study. Clinical and laboratory data were collected from electronic medical records. Neonates with final diagnosis with sepsis were divided into the sepsis group, The remaining neonates were divided into the control group. Neonates with sepsis were further categorized into mild (n = 312) and severe (n = 425) groups based on the severity of their condition. FAR was determined by dividing the plasma fibrinogen concentration (g/L) by the serum albumin concentration (g/L). The statistical analyses were conducted using the SPSS 26.0 statistical software package, as deemed appropriate.
Results: FAR levels were significantly higher in neonates with sepsis compared to the control group. Additionally, a significant gradual increase in FAR was observed in the control, mild sepsis, and severe sepsis groups (P < 0.001). Correlation analysis showed that FAR had a positive correlation with PCT, CRP, and the length of hospital stay. Multiple logistic regression analysis showed that FAR was independently associated with the presence and severity of neonatal sepsis. Specifically, FAR was identified as an independent risk factor for both the presence of sepsis (OR = 8.641, 95% CI 5.708– 13.080, P < 0.001) and severe sepsis (OR = 2.817, 95% CI 1.701– 4.666, P < 0.001).
Conclusion: FAR is significantly increased in neonates with sepsis and had a correlation with the severity of sepsis. Increased FAR was an independent predictor for the presence and severity of neonatal sepsis.
Keywords: fibrinogen-to-albumin ratio, neonatal sepsis, severe sepsis, predictor
Introduction
Sepsis is one of the leading causes of neonatal morbidity and global mortality and the recent WHO’s Resolution on sepsis suggests that addressing sepsis may also become a critical healthcare priority in the upcoming decade.1 Sepsis is a complex clinical syndrome consisting of a severe infection caused by pathogens. The current gold standard for the diagnosis of neonatal sepsis is blood culture. However, blood cultures have several obvious disadvantages, such as a long wait to get a test report and low positive rates (mainly due to small blood volumes, contaminated blood samples, or intrapartum antimicrobial administration).2–4 The accurate and timely diagnosis of neonatal sepsis is valuable in early intervention and treatment, which can further improve the prognosis of neonates with sepsis. Circulating blood biomarkers that may be useful in the early diagnosis of neonatal sepsis have been processed.5
Previous studies have shown that plasma fibrinogen (FIB), as an acute phase reactant protein, exhibits an increase during the early stages of inflammation and a rapid decrease during the recovery stage.6 Although the relationship between FIB and sepsis has been reported previously, current published research pertains predominantly to adults, and few studies have focused on the relationship between FIB and neonatal sepsis. Albumin (ALB) is a protein synthesized by hepatocytes, accounting for 40–60% of the total protein of the human body.7 ALB serves not only as a crucial protein for maintaining plasma colloidal osmotic pressure, but also as an important nutritional indicator.8 Studies have indicated a close association between ALB and inflammation, with hypoproteinemia being prevalent in patients suffering from inflammatory ailments. Additionally, Qian and Liu9 discovered that hypoalbuminemia rates were high among children diagnosed with sepsis, while serum albumin levels exhibited an inverse correlation with prognosis.
The fibrinogen-to-albumin ratio (FAR) was determined by dividing the plasma FIB concentration (g/L) by the serum albumin concentration (g/L). The FAR, as the ratio of FIB to ALB, reflects inflammatory changes in the body during inflammation. FAR has garnered significant attention as an emerging biomarker for inflammation. Studies have shown that FAR is a predictor of the ascending aorta aneurysm and predicts mortality-related cancer patients, patients with sepsis caused by Peritonitis, and COVID-19 patients in intensive care unit.10,11 However, there is limited literature on the association of FAR with the presence and severity of sepsis in neonates. Therefore, this study aims to investigate the potential clinical value of FAR in predicting the presence and severity of sepsis in neonates.
Materials and Methods
Study Population
This retrospective study was conducted at the Children’s Hospital of Zhengzhou University (Henan Children’s Hospital) from January 2017 to December 2022. We consecutively enrolled neonates with suspected sepsis, and a total of 1292 newborns with suspected neonatal sepsis were collected. Clinical and laboratory data were extracted from patient database, and all laboratory parameters were collected from the first sampling of patients who had not been treated after admission. The exclusion criteria for this study were: (1) Missing fibrinogen, albumin, or other clinical data, (2) Other diseases, such as hematological disorders, major congenital malformations, cancer, congenital liver disease, acute kidney injury, inherited metabolic disorders, infants of drug-dependent mothers and cyanotic congenital heart diseases, and (3) Prematurity with a gestational age of less than 34 weeks, or a birth weight of less than 2.0 kg.
Our research protocol complied with the Declaration of Helsinki and was approved by the hospital’s ethics committee. As it was a retrospective study, informed consent was not required, and this was approved and authorized by the hospital ethics review committee of Henan Children’s Hospital (2021-K-054). We can confirm that all data collected was anonymized and no information pertaining to privacy was gathered.
Clinical Definition
In this study, the control group consisted of neonates admitted to the hospital with suspected sepsis but did not meet the diagnostic criteria after a comprehensive examination and instead presented with mild infections neonatal pneumonia or neonatal hyperbilirubinemia. According to the International Consensus on Pediatric Sepsis, our definition of neonatal sepsis has been constantly evolving and improving based on current experience and current available research.12 There was a consensus on the definition of neonatal sepsis, which was further defined by Goldstein Brahm et al in 2005.13 Infection is defined as a suspected or confirmed infection caused by any pathogen or clinical syndrome associated with a high likelihood of infection, including clinical, imaging, or laboratory tests.13 Neonatal sepsis is characterized by the presence of a systemic inflammatory response syndrome or suspected/proven infection. Severe sepsis is defined as sepsis accompanied by cardiovascular organ dysfunction, acute respiratory distress syndrome, or two or more instances of other organ dysfunction (respiratory, renal, neurologic, hematologic, or hepatic), per the International Consensus on Pediatric Sepsis.13,14 In clinical practice, the differential diagnosis between neonatal infection and sepsis should be conducted by two physicians following the international pediatric sepsis consensus.13,14 If a case fulfills the criteria for sepsis but does not meet the criteria for severe sepsis, it is classified as mild sepsis.
Data Collection
The laboratory test results in this study were obtained from the initial sample collection upon admission prior to any clinical intervention. The information from the admissions were collected for the patient’s electronic medical records, including the following domains: 1) demographic and admission status data, including age, gender, weight, body temperature, respiratory rate, and heart rate; and 2) laboratory data at admission. The detection methods of those laboratory indexes were described in our previous published study.15 To facilitate statistics, CRP levels < 0.8 mg/L were assigned a value of 0.7 mg/L. PCT levels > 100 ng/mL or < 0.02 ng/mL were assigned, 101 ng/mL and 0.01 ng/mL, respectively.
Statistical Analysis
The normality of all variables was checked before performing a statistical analysis using SPSS 26.0. Variables, following the normal distribution, were represented by the mean ± standard deviation (SD) and analyzed by independent t-test or one-way ANOVA. Non-normally distributed variables were represented by the median (interquartile range) and analyzed with a Mann–Whitney U-test. Categorical variables were presented as numbers and percentages (n, %) and evaluated them through a chi-square test or Fisher’s exact test. Spearman correlation test was conducted to analyze the correlation between two variables. Multivariate logistic regression analysis was applied to determine the independent risk factors of neonatal sepsis. The variables were predetermined according to a univariate p-value lower than 0.05 and previously published literature. A two-sided P value below 0.05 was considered statistically significant.
Results
Baseline Clinical Data of the Study Population
A total of 1292 neonates (with a median age of 8.0 (5.0, 15.0) days, including 59.67% of males) were divided into two groups: the control group (non-septic infections) and the sepsis group. According to the severity of sepsis, neonates with sepsis were further divided into mild sepsis and severe sepsis groups. There were 312 neonates in the mild sepsis group and 425 neonates in the severe sepsis group. Characteristics of the study population are indicated in Table 1. Neonates in the sepsis group were older than the neonates in the control group (P < 0.05). Compared with the control group, newborns with sepsis had lower body weight, higher body temperature, higher respiratory rate, and faster heart rate (P < 0.05). Biochemical analysis revealed that neonates with sepsis had higher levels of FAR, procalcitonin (PCT), C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), urea nitrogen (UREA), uric acid (UA), and a longer length of hospital stay (P < 0.05), and lower levels of total bilirubin (TBIL), total protein (TP), and albumin (ALB) (P < 0.05). Among those variables, FAR, PCT, CRP, ALT, AST, UA, and the length of hospital stay showed a gradual increase or decrease in the control, mild sepsis, and severe sepsis groups.
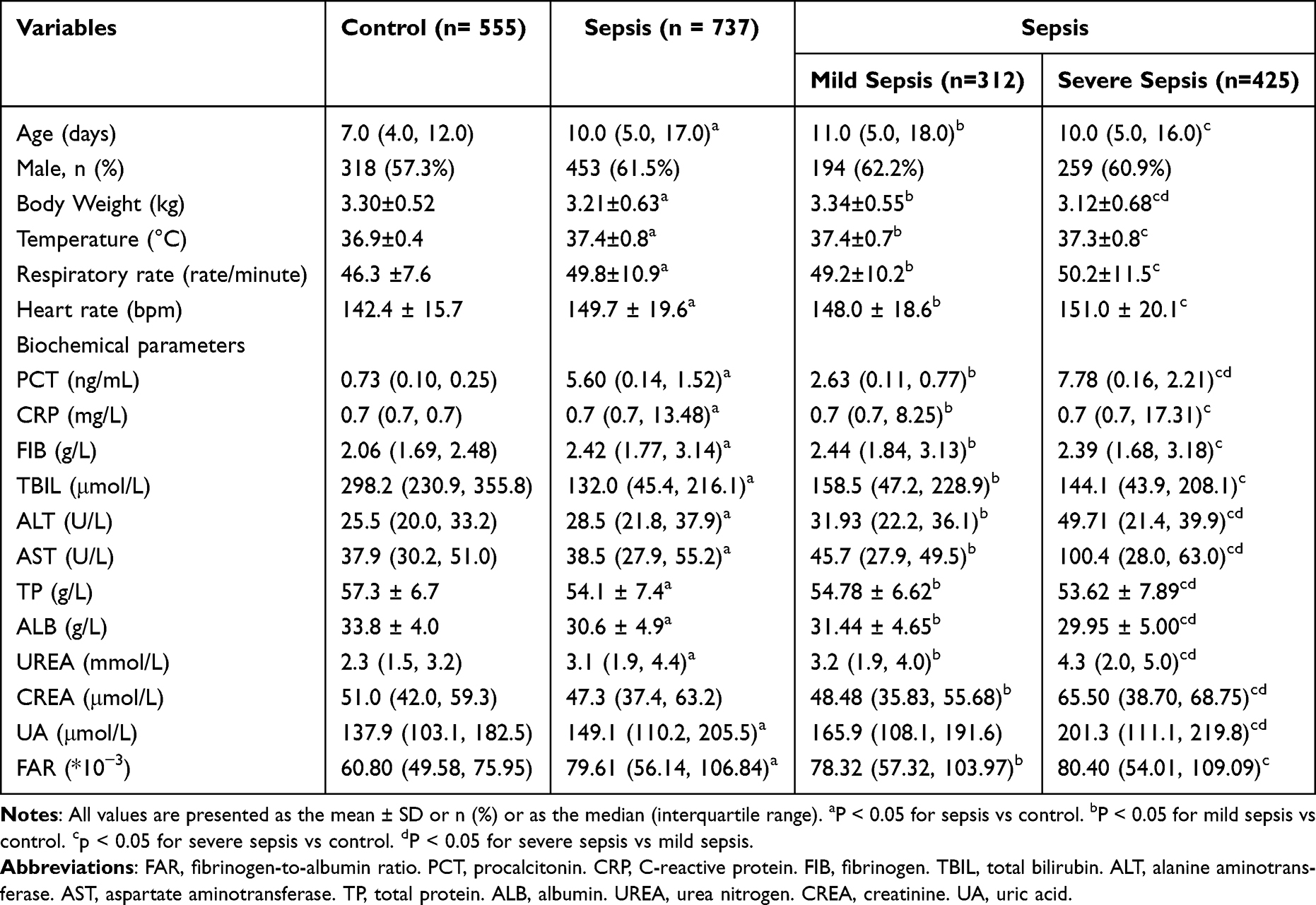 |
Table 1 Basic Characteristics of Study Subjects |
Associations Between FAR and the Presence and Severity of Neonatal Sepsis
To further investigate the relationship between the FAR and severity of neonatal sepsis, the subjects were classified into three groups according to the FAR tertile: low FAR group (< 57.06), intermediate FAR group (57.06–83.98), and high FAR group (> 83.98). The clinical and laboratory data of the neonates are presented in Table 2. Neonates in the high FAR group were older. Further analysis showed that the prevalence of overall sepsis, mild sepsis, and severe sepsis in the high FAR group was significantly higher than in the low FAR and intermediate FAR groups (p < 0.001). In comparison, the prevalence of control was significantly lower in in the high FAR group.
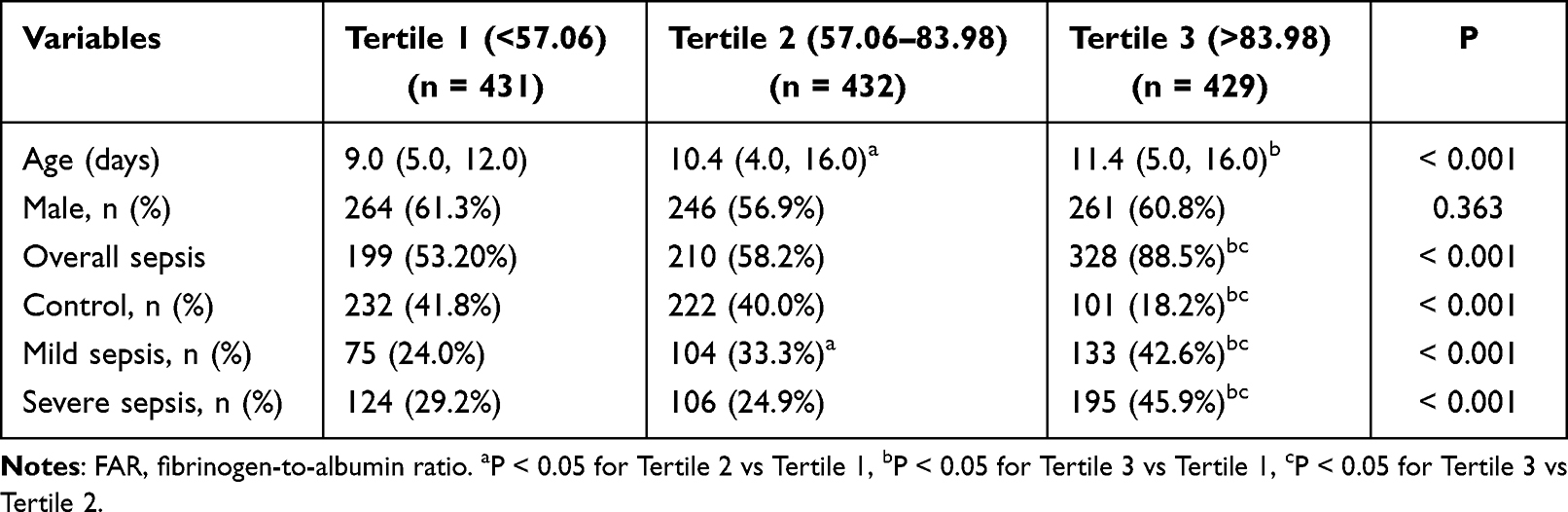 |
Table 2 The Presence and Severity of Neonatal Sepsis According to FAR Tertiles |
Correlation Between FAR and Clinical Parameters
To study the relationship between FAR and neonatal sepsis, we performed a Spearman correlation analysis. In the overall population, FAR was positively correlated with age (r = 0.160, P < 0.001), temperature (r = 0.229, P < 0.001), respiratory rate (r = 0.174, P < 0.001), heart rate (r = 0.218, P < 0.001), PCT (r = 0.283, P < 0.001), CRP (r = 0.257, P < 0.001) and length of hospital stay (r = 0.375, P < 0.001), and negatively correlated with weight (r = - 0.086, P = 0.002) and TP (r = - 0.111, P < 0.001) (As shown in Table 3). In addition, we found no significant correlations were identified between ALT (r = 0.106, P = 0.680) and AST (r = 0.025, P = 0.376) (P > 0.05). However, in the neonates with sepsis group, FAR was only positively correlated with weight (r = 0.119, P = 0.001), PCT (r = 0.109, p = 0.003) and length of hospital stay (r = 0.103, P = 0.005).
 |
Table 3 Correlations Between FAR and Clinical Parameters |
Predictive Value of FAR for the Presence and Severity of Neonatal Sepsis
As presented in Table 4, after adjusting age, temperature, respiratory rate, weight, PCT, CRP, ALT, and TP, multivariate analysis showed that FAR (OR = 2.817, 95% CI 1.701–4.666, P < 0.001) is an independent predictor of neonatal sepsis. Further multivariate analysis showed that FAR were also an independent risk factor for neonatal severe sepsis. Meanwhile, data also showed that high FAR is independently associated with the presence and severity of neonatal sepsis.
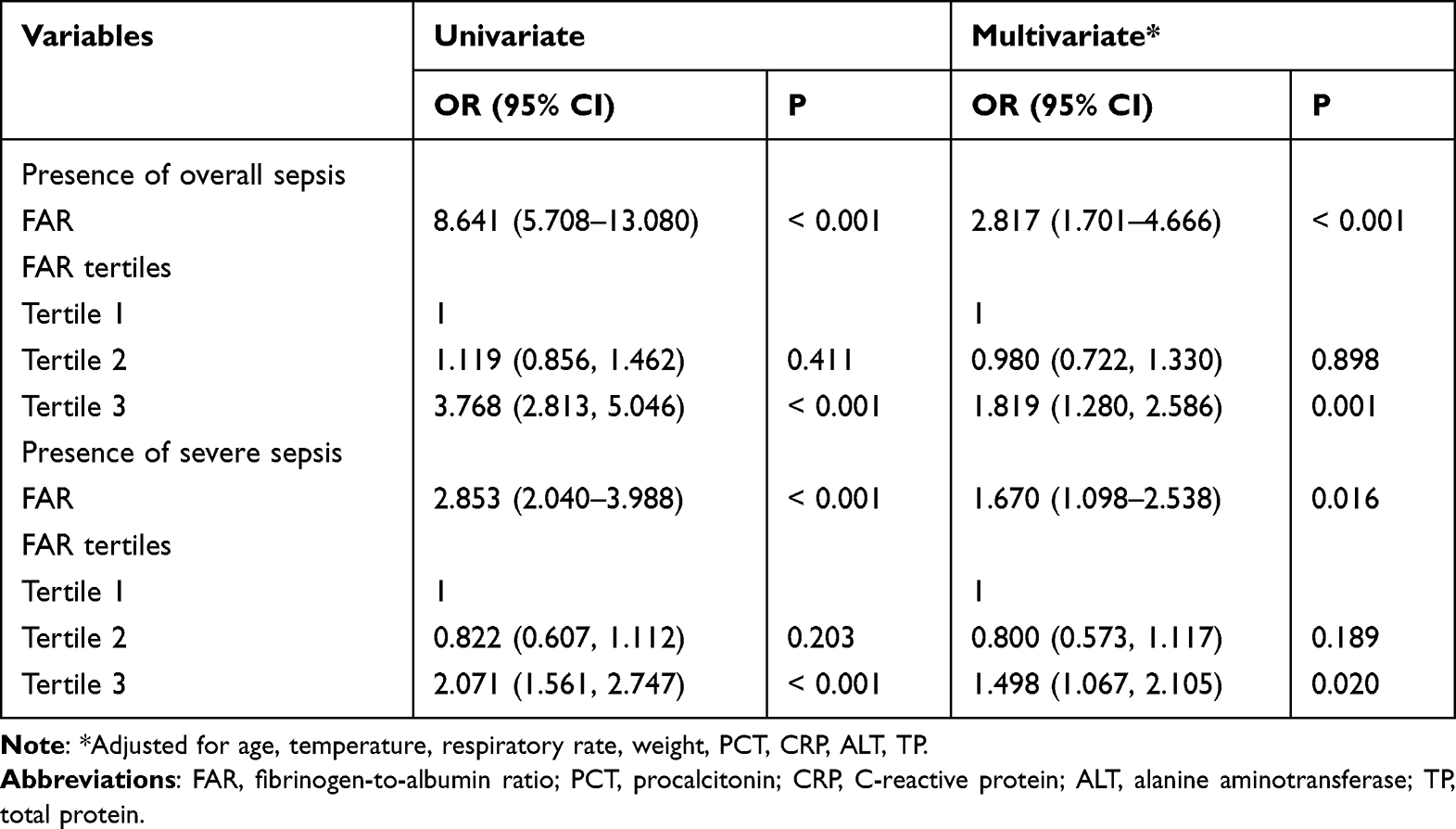 |
Table 4 Regression Analysis to Assess the Presence of Neonatal Sepsis and Severe Sepsis According to FAR Tertiles |
Discussion
Sepsis is defined as a life-threatening organ dysfunction caused by a dysregulated host response to infection,16 and remains one of the leading causes of death in children (most of that were neonatal) globally.17 Therefore, the early diagnosis of neonatal sepsis is of great significance in treating neonatal sepsis and improving neonatal survival rate. Although positive blood culture is considered the gold standard for diagnosing neonatal sepsis due to its prolonged reporting period and low positivity rate, it can be easily influenced by factors such as early antibiotic administration, posing a challenge in clinical diagnosis. The identification of appropriate markers or their combinations is thus crucial for the accurate diagnosis of neonatal sepsis.
FIB, a glycoprotein synthesized and secreted by the liver, is stable and abundant in peripheral blood. The conversion of FIB to fibrin by thrombin is essential for its physiological hemostatic function. FIB is an acute response protein, which makes it a pro-inflammatory factor, a pro-inflammatory regulator and a potential therapeutic target. During inflammation in the body, FIB exhibits a ligand-receptor mode of binding to various immune cells. It engages in direct or indirect interactions with vascular endothelial cells, smooth muscle cells, and inflammatory cells, thereby actively participating in the process inflammatory response.18 Increasing evidence suggests significant crosstalk between the coagulation system and pathways related to inflammation.19 Inflammation promotes coagulation through crosstalk, while coagulation significantly impacts inflammatory activity. In recent years, FIB has gathered significant attention and has been recognized as a viable diagnostic tool for sepsis.20
ALB is another protein produced by the liver. In addition to maintaining plasma osmotic pressure, albumin is a multifunctional transport protein capable of binding with various small molecules within the body for transportation purposes, including amino acids, drugs, hormones, and fatty acids. Studies have demonstrated a strong correlation between ALB and inflammation.21 When inflammation occurs in the body, it impairs hepatic function, leading to reduced synthesis of albumin and subsequently levels. This phenomenon was also observed and confirmed in this study across the control group, mild sepsis group, and severe sepsis group. Furthermore, there was an inverse correlation between the level of ALB and disease severity.22 Sepsis is a pathological condition that can result in multi-organ dysfunction syndrome. Studies have demonstrated the frequent occurrence of hypoalbuminemia in neonatal sepsis patients, and clinical evidence suggests a positive correlation between low ALB levels and inflammation severity as well as poor prognosis.23,24 Studies have shown that ALB level can be used as an independent predictor of sepsis.25,26
As an emerging index, FAR has attracted substantial attention in recent years. During inflammation, the increasing trend of FIB and the decreasing trend of ALB in the body enable FAR to detect inflammatory changes more accurately. Multiple studies have demonstrated that there was a close correlation between FAR and cardiovascular disease, hemorrhagic transformation in acute ischemic stroke patients, and other diseases.27–30 Cetin et al have confirmed that the FAR ratio is an independent predictor of long-term major cardiovascular adverse events in patients with acute coronary syndrome who undergo percutaneous coronary intervention.31 The study conducted by Ruan et al demonstrated that FAR was linked to hemorrhagic transformation following acute ischemic stroke. However, it is not optimal to discriminate the severity of such transformation. Nevertheless, it can still assist clinicians in conducting an initial assessment of bleeding risk.32 Furthermore, FAR can be a potent tool for tracking morning blood pressure surges in newly diagnosed and untreated hypertensive individuals.33 Besides, FAR can serve not only as an independent influencing factor for SLE, but also as a reliable indicator of the severity and poor prognosis of SLE, while possessing diagnostic value in determining the activity status of SLE.34 Moreover, high FAR with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention.35 Additionally, studies have validated the utility of FAR as a novel biomarker for diagnosing diabetic kidney disease and monitoring its progression.36 However, no research has been conducted to investigate the correlation between FAR and neonatal sepsis.
In this study, we first explore the association between FAR and sepsis in a relatively large neonatal population and found that FAR was higher in neonates with sepsis and showed a gradual increase among the control group, mild sepsis group, and severe sepsis group. Although there were no significant differences in FAR between the mild and severe sepsis groups, it should be emphasized that the test results we gathered were obtained post-admission and pre-treatment of the patient. It should also be noted that FIB levels tend to increase significantly during the early stages of inflammation. In cases of critical patient admission, there is a heightened probability of coagulation dysfunction, specifically Disseminated Intravascular Coagulation (DIC). Throughout this period, the FIB level may have surpassed the stage of elevation and instead decreased. Moreover, neonates with severe sepsis may not exhibit significant elevations in FAR levels relative to those with mild sepsis. According to FAR tertiles, neonates were divided into three groups, and our data showed that the prevalence of overall sepsis increased significantly from 53.2% in FAR tertile 1 to 88.5% in FAR tertile 3 (P < 0.001). Meanwhile, multivariate analysis showed that FAR was an independent predictor of neonatal sepsis and severe sepsis.
However, as a retrospective study, our research has some limitations. First of all, although we have 1292 cases, it is a single-center study, and we may obtain more authoritative results if we had recruited multiple centers in the study. Secondly, the diagnostic criteria that was chosen based on clinical as opposed to definitive positive blood culture results, which may lead to errors. Ultimately, we solely utilize the initial admission FAR as the analytical indicator. FAR can be used as a monitoring marker, and may be more significant.
Conclusions
Our research has demonstrated a significant correlation between the FAR and neonatal sepsis. FAR was an independent predictor of both the presence and severity of neonatal sepsis, with higher ratios positively associated with increased prevalence of this condition.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Hospital Ethics Review Board of Henan Children’s Hospital. We confirmed that all the data were anonymized and maintained with confidentiality; therefore, the requirement for informed consent has been waived because of the retrospective nature of the current study.
Acknowledgement
We thank Bullet Edits Limited for the language editing and proofreading of the manuscript.
Funding
This work was supported by the Key Research, Development, and Promotion Projects of Henan Province (222102310067, 232102310234), and Medical Science and Technology Project of Henan Province (LHGJ20210665, LHGJ20210672, and LHGJ20210681).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 2018;6(3):223–230. doi:10.1016/S2213-2600(18)30063-8
2. Iroh Tam PY, Bendel CM. Diagnostics for neonatal sepsis: current approaches and future directions. Pediatr Res. 2017;82(4):574–583. doi:10.1038/pr.2017.134
3. Lamy B, Dargere S, Arendrup MC, Parienti JJ, Tattevin P. How to optimize the use of blood cultures for the diagnosis of bloodstream infections? A State-of-the Art. Front Microbiol. 2016;7:697. doi:10.3389/fmicb.2016.00697
4. Fernandez-Hidalgo N, Ribera A, Larrosa MN, et al. Impact of Staphylococcus aureus phenotype and genotype on the clinical characteristics and outcome of infective endocarditis. A multicentre, longitudinal, prospective, observational study. Clin Microbiol Infect. 2018;24(9):985–991. doi:10.1016/j.cmi.2017.12.002
5. Sharma D, Farahbakhsh N, Shastri S, Sharma P. Biomarkers for diagnosis of neonatal sepsis: a literature review. J Matern Fetal Neonatal Med. 2018;31(12):1646–1659. doi:10.1080/14767058.2017.1322060
6. Mitra P, Guha D, Nag SS, Mondal BC, Dasgupta S. Role of plasma fibrinogen in diagnosis and prediction of short term outcome in neonatal sepsis. Indian J Hematol Blood Transfus. 2017;33(2):195–199. doi:10.1007/s12288-016-0683-x
7. Fanali G, Di Masi A, Trezza V, Marino M, Fasano M, Ascenzi P. Human serum albumin: from bench to bedside. Mol Aspects Med. 2012;33(3):209–290. doi:10.1016/j.mam.2011.12.002
8. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
9. Qian SY, Liu J. 脓毒症/严重脓毒症/脓毒性休克患儿血清白蛋白水平与预后关系的研究 [Relationship between serum albumin level and prognosis in children with sepsis, severe sepsis or septic shock]. Zhonghua Er Ke Za Zhi. 2012;50(3):184–187. Chinese.
10. Afsin A, Tibilli H, Hosoglu Y, et al. Fibrinogen-to-albumin ratio predicts mortality in COVID-19 patients admitted to the intensive care unit. Adv Respir Med. 2021. doi:10.5603/ARM.a2021.0098
11. Wen Y, Yang J, Han X. Fibrinogen-to-Albumin ratio is associated with all-cause mortality in cancer patients. Int J Gen Med. 2021;14:4867–4875. doi:10.2147/IJGM.S322735
12. Wynn JL. Defining neonatal sepsis. Curr Opin Pediatr. 2016;28(2):135–140. doi:10.1097/MOP.0000000000000315
13. Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric S. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
14. Li T, Li X, Liu X, et al. Association of procalcitonin to albumin ratio with the presence and severity of sepsis in neonates. J Inflamm Res. 2022;15:2313–2321. doi:10.2147/JIR.S358067
15. Li T, Dong G, Zhang M, et al. Association of neutrophil-lymphocyte ratio and the presence of neonatal sepsis. J Immunol Res. 2020;2020:7650713. doi:10.1155/2020/7650713
16. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
17. Kissoon N, Reinhart K, Daniels R, Machado MFR, Schachter RD, Finfer S. Sepsis in children: global implications of the world health assembly resolution on sepsis. Pediatr Crit Care Med. 2017;18(12):e625–e627. doi:10.1097/PCC.0000000000001340
18. Hsieh JY, Smith TD, Meli VS, Tran TN, Botvinick EL, Liu WF. Differential regulation of macrophage inflammatory activation by fibrin and fibrinogen. Acta Biomater. 2017;47:14–24. doi:10.1016/j.actbio.2016.09.024
19. Karer M, Kussmann M, Ratzinger F, et al. Different types of coagulase are associated with 28-day mortality in patients with staphylococcus aureus bloodstream infections. Front Cell Infect Microbiol. 2020;10:236. doi:10.3389/fcimb.2020.00236
20. Faix JD. Biomarkers of sepsis. Crit Rev Clin Lab Sci. 2013;50(1):23–36. doi:10.3109/10408363.2013.764490
21. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722 e717. doi:10.1016/j.amjmed.2019.10.031
22. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. JPEN J Parenter Enteral Nutr. 2019;43(2):181–193. doi:10.1002/jpen.1451
23. Nesseler N, Launey Y, Aninat C, Morel F, Malledant Y, Seguin P. Clinical review: the liver in sepsis. Crit Care. 2012;16(5):235. doi:10.1186/cc11381
24. Yang C, Liu Z, Tian M, et al. Relationship between serum albumin levels and infections in newborn late preterm infants. Med Sci Monit. 2016;22:92–98. doi:10.12659/MSM.895435
25. Sheng S, Zhang YH, Ma HK, Huang Y. Albumin levels predict mortality in sepsis patients with acute kidney injury undergoing continuous renal replacement therapy: a secondary analysis based on a retrospective cohort study. BMC Nephrol. 2022;23(1):52. doi:10.1186/s12882-021-02629-y
26. Godinez-Vidal AR, Correa-Montoya A, Enriquez-Santos D, Perez-Escobedo SU, Lopez-Romero SC, Gracida-Mancilla NI. Is albumin a predictor of severity and mortality in patients with abdominal sepsis? Cir Cir. 2019;87(5):485–489. doi:10.24875/CIRU.180003903
27. Li Z, Zhou C, Peng Q, et al. Fibrinogen-albumin ratio index exhibits predictive value of neoadjuvant chemotherapy in osteosarcoma. Cancer Manag Res. 2022;14:1671–1682. doi:10.2147/CMAR.S358310
28. Scheuer K, Helbing C, Firkowska-Boden I, Jandt KD. Self-assembled fibrinogen-fibronectin hybrid protein nanofibers with medium-sensitive stability. RSC Adv. 2021;11(23):14113–14120. doi:10.1039/D0RA10749B
29. Ying HQ, Chen W, Xiong CF, Wang Y, Li XJ, Cheng XX. Quantification of fibrinogen-to-pre-albumin ratio provides an integrating parameter for differential diagnosis and risk stratification of early-stage colorectal cancer. Cancer Cell Int. 2022;22(1):137. doi:10.1186/s12935-022-02532-y
30. Lee LE, Pyo JY, Ahn SS, Song JJ, Park YB, Lee SW. Fibrinogen to albumin ratio reflects the activity of antineutrophil cytoplasmic antibody-associated vasculitis. J Clin Lab Anal. 2021;35(4):e23731. doi:10.1002/jcla.23731
31. Cetin M, Erdogan T, Kiris T, et al. Predictive value of fibrinogen-to-albumin ratio in acute coronary syndrome. Herz. 2020;45(Suppl 1):145–151. doi:10.1007/s00059-019-4840-5
32. Ruan Y, Yuan C, Liu Y, et al. High fibrinogen-to-albumin ratio is associated with hemorrhagic transformation in acute ischemic stroke patients. Brain Behav. 2021;11(1):e01855. doi:10.1002/brb3.1855
33. Ozdemir M, Yurtdas M, Asoglu R, Yildirim T, Aladag N, Asoglu E. Fibrinogen to albumin ratio as a powerful predictor of the exaggerated morning blood pressure surge in newly diagnosed treatment-naive hypertensive patients. Clin Exp Hypertens. 2020;42(8):692–699. doi:10.1080/10641963.2020.1779282
34. Dai LL, Chen C, Wu J, Cheng JF, He F. The predictive value of fibrinogen-to-albumin ratio in the active, severe active, and poor prognosis of systemic lupus erythematosus: a single-center retrospective study. J Clin Lab Anal. 2022;36(9):e24621. doi:10.1002/jcla.24621
35. Wang P, Yuan D, Zhang C, et al. High fibrinogen-to-albumin ratio with type 2 diabetes mellitus is associated with poor prognosis in patients undergoing percutaneous coronary intervention: 5-year findings from a large cohort. Cardiovasc Diabetol. 2022;21(1):46. doi:10.1186/s12933-022-01477-w
36. Wang K, Xu W, Zha B, Shi J, Wu G, Ding H. Fibrinogen to albumin ratio as an independent risk factor for type 2 diabetic kidney disease. Diabetes Metab Syndr Obes. 2021;14:4557–4567. doi:10.2147/DMSO.S337986
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.