Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Female is Associated with Left Ventricular Diastolic Dysfunction in Patients with Type 2 Diabetes
Authors Wang Y ![]() , Zhou Y, Zhang Y, Ren Q, Wang Y, Su H
, Zhou Y, Zhang Y, Ren Q, Wang Y, Su H
Received 17 May 2023
Accepted for publication 27 July 2023
Published 7 August 2023 Volume 2023:16 Pages 2355—2364
DOI https://doi.org/10.2147/DMSO.S421761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Yiting Wang,1,* Yikun Zhou,1,* Yonghong Zhang,1 Qiuting Ren,2 Yan Wang,1 Heng Su1
1Department of Endocrinology and Metabolism, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China; 2Echocardiogram Laboratory, Department of Cardiology, The First People’s Hospital of Yunnan Province, The Affiliated Hospital of Kunming University of Science and Technology, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Wang; Heng Su, Email [email protected]; [email protected]
Aim: Diabetic cardiomyopathy is a subset of heart disease that is directly associated with diabetes, and left ventricular diastolic dysfunction is the earliest sign. We aimed to investigate the association between sex differences and left ventricular diastolic function in patients with type 2 diabetes.
Methods: This was a cross-sectional study included patients with type 2 diabetes who visit the National Metabolic Management Center (MMC) at the First People’s Hospital of Yunnan from 2018 to 2021. Patients with hypertension, history of heart disease or ejection fraction < 50% were excluded from the study. Logistic regression was used to analyze their associations.
Results: A total of 1778 patients were included in the study. The study included 1205 (70%) males and 573 (30%) females. Compared with males, females had higher total cholesterol and LDL cholesterol levels but lower diastolic pressure, body mass index (BMI), visceral fat area, HbA1c, blood urea nitrogen (BUN), serum creatinine and triglyceride. Females had a relatively higher ejection fraction than males (68.17 ± 6.055 vs 67.5 ± 6.096, P < 0.05). More female patients than male patients in the age group of 45– 60 years old had left ventricular diastolic dysfunction (female vs male, 54.5% vs 46.9%, P < 0.05). We also found that females were independently associated with left ventricular diastolic dysfunction, after adjusting for important clinical factors.
Conclusion: Left ventricular diastolic function might be worse in female patients with type 2 diabetes. Further study is needed to verify the underlying mechanism.
Keywords: type 2 diabetes, sex differences, left ventricular diastolic dysfunction
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ponath Sukumaran has been published for this article.
Introduction
According to the International Diabetes Federation (IDF) Diabetes Atlas in 2021, there are 537 million adults living with diabetes, and the number is predicted to rise to 643 million by 2030. Despite the control of glycemia, hypertension and/or hyperlipidemia, one person dies of diabetes every five seconds. Diabetes and its complications come with a huge burden.
Cardiovascular disease associated with diabetes confers the primary cause of death in patients with type 2 diabetes. Hopefully, the EMPA-Heart randomized clinical trial has proven that sodium-glucose cotransporter 2 (SGLT2) inhibitors with empagliflozin lower cardiovascular events in type 2 diabetes.1 Glucagon-like peptide-1 receptor agonists (GLP-1 RA) have also been shown to reduce stroke risk in type 2 diabetes.2 The early detection of high-risk groups for cardiovascular disease gives us opportunity to initiate medications that are beneficial to the heart.
Physiologically, female sex hormones could be beneficial in cardiovascular diseases,3 however, the benefit would disappear in patients with diabetes. Studies have shown that diabetic females were with more advanced carotid atherosclerosis4 and higher rate of heart failure5 than diabetic males when they were compared with their respective non-diabetic cohorts. Another study also confirmed that females with diabetes have higher hospital admission rates for acute myocardial incident compared with males.6 A recent nationwide study observed that the relative rate of first-time cardiovascular complications related to diabetes was higher in females than in males.7
Diabetic cardiomyopathy refers to a unique subset of heart diseases associated with diabetes. It is characterized by diastolic and systolic dysfunction, which is gradually unrelated to hypertension or primary heart diseases.8 Left ventricular diastolic dysfunction is usually considered to be the earliest manifestation of diabetic cardiomyopathy. However, no study has focused on sex differences of diabetic cardiomyopathy, and whether female is a risk factor for the diabetic cardiomyopathy in the early stage remains unclear.
Therefore, in the current study, we aimed to investigate the association between sex difference and left ventricular diastolic function in patients with type 2 diabetes.
Method
Study Population
We performed a cross-sectional study. The study included patients with type 2 diabetes who visited the National Metabolic Management Center (MMC) at the First People’s Hospital of Yunnan from 2018 to 2021. The diagnostic criteria for diabetes were based on the 1999 World Health Organization criteria and 2012 American Diabetes Association standards. Patients with (1) type 1 diabetes and other types of diabetes, (2) aged <18 and >80 years, (3) pregnancy, (4) a lack of echocardiography results, (5) a diagnosis of hypertension, (6) a history of heart disease and (6) an EF <50% were excluded from the study (Figure 1).
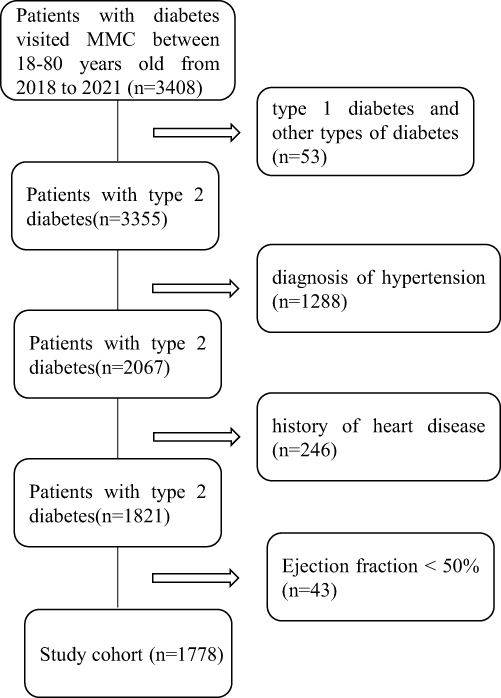 |
Figure 1 Flowchart of study participants. Abbreviation: MMC, Metabolic Management Center. |
This study protocol conformed with the Declaration of Helsinki and was approved by the Ethics Committee of the First People’s Hospital of Yunnan Province. The approval ID number is KHLL2021-KY012.
All the participants have provided informed consent.
Clinical Parameters and Evaluation of Left Ventricular Diastolic Function
Clinical parameters including age, sex, hypertension, duration of diabetes, liver and kidney function, etc., were collected from the electronic records of our hospital.
Evaluation of left ventricular diastolic function with normal ejection fraction was accomplished by professional cardiac sonographers in our hospital according to Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography in 2016.9 Briefly, we diagnosed left ventricular diastolic function if the following four conditions satisfy greater than two: (1) average E/e’ >14; (2) septal e’ velocity <7 cm/s or lateral e’ velocity <10 cm/s; (3) tricuspid regurgitation velocity >2.8 m/s; (4) left atrium volume index >34mL/m2.
Statistical Analysis
Data are presented as mean ± standard deviation (normal distribution) or median and interquartile range (skewed distribution). Differences between groups were analyzed using the Student’s t-test, the Mann–Whitney test, the rank sum test or the chi-square test, as appropriate. Univariable and multivariable logistic regressions were employed to assess the association between clinical parameters and left ventricular diastolic dysfunction.
Results
Clinical Characteristics of the Study Cohort
A total of 1778 patients were included in the study, and baseline clinical characteristics are presented in Table 1. Briefly, the mean age of patients was 50.0 ± 10.89 years old, the mean diabetic duration was 87.7 ± 72.2 months, and the mean HbA1c was 10.0 ± 2.68%. The mean serum albumin was 40 ± 4.33 g/L, the mean serum creatinine was 64 ± 15.8 μmol/L, and the median of albumin-to-creatinine ratio (ACR) was 12 (2.7, 69.4) mg/g. There were 1205 (70%) male and 573 (30%) female in the cohort. Compared with male, female was older, had the higher total cholesterol, high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol, but female had lower diastolic pressure, body mass index (BMI), visceral fat area, HbA1c, blood urea nitrogen (BUN), alanine aminotransferase (ALT), serum creatinine and triglyceride. More males were smokers and drinkers, but more females have a family history of diabetes. There was no difference of systolic pressure, subcutaneous fat area, diabetic duration, aspartate transaminase (AST) and ACR between male and female.
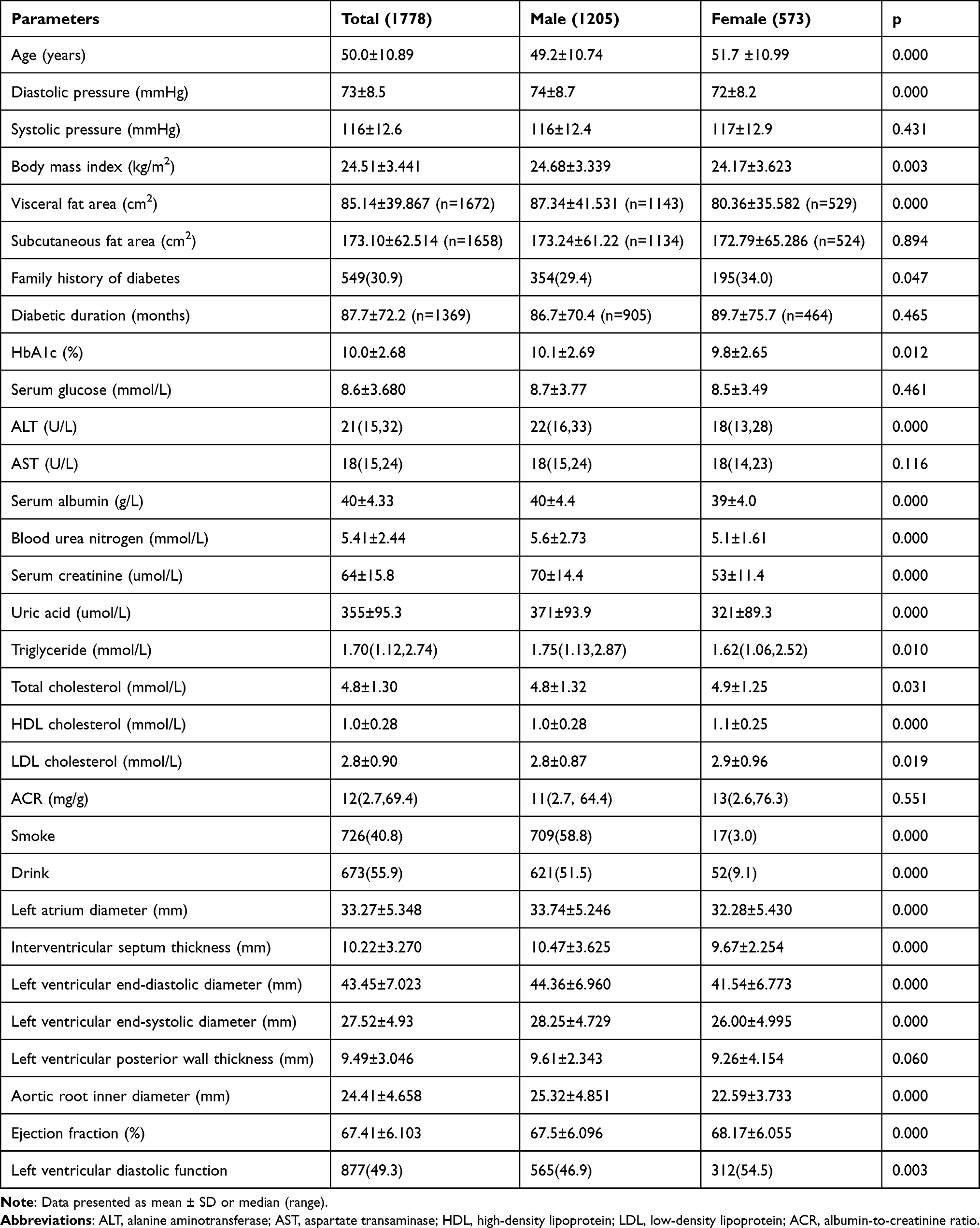 |
Table 1 Baseline Characteristics |
In terms of cardiac characteristics, females had significantly shorter left atrium diameter, ventricular septal thickness, left ventricular end-diastolic and systolic diameter, and aortic root inner diameter compared with males. The differences might contribute to physiological differences. Females had relatively higher ejection fraction than males (68.17 ± 6.055 vs 67.5 ± 6.096, P < 0.05), but there was no difference of left ventricle posterior wall thickness between male and female.
The Association Between Clinical Factors and Left Ventricular Diastolic Dysfunction
First, we used the univariable logistic regression to analyze important clinical factors which might be associated with left ventricular diastolic dysfunction (Table 2). We found that female, the older, higher blood pressure, higher visceral/subcutaneous fat area, family history of diabetes, longer diabetic duration, lower HbA1c, higher BUN, and serum creatinine were all associated with left ventricular diastolic dysfunction.
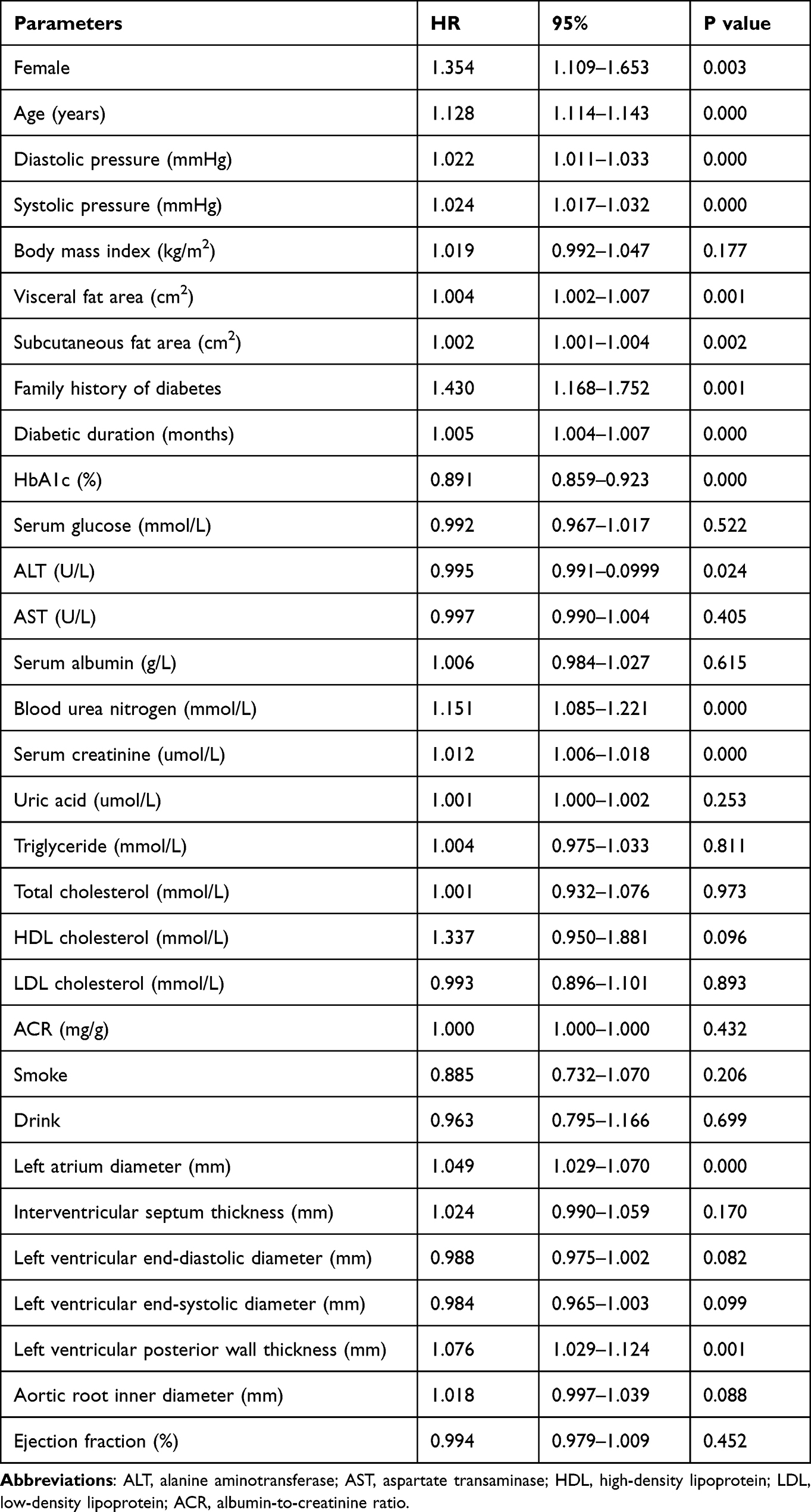 |
Table 2 Univariate Logistic Regression |
Then, we used multivariable logistic regression to adjusted confounding factors (Table 3). We found that females were still associated with left ventricular diastolic dysfunction when adjusted age, diastolic/systolic pressure, BMI, visceral/subcutaneous fat area, diabetic duration, HbA1c, family history of diabetes, smoking, drinking, serum albumin, ALT, AST, BUN, serum creatinine, ACR, uric acid, triglyceride, total cholesterol and HDL/LDL cholesterol (Figure 2).
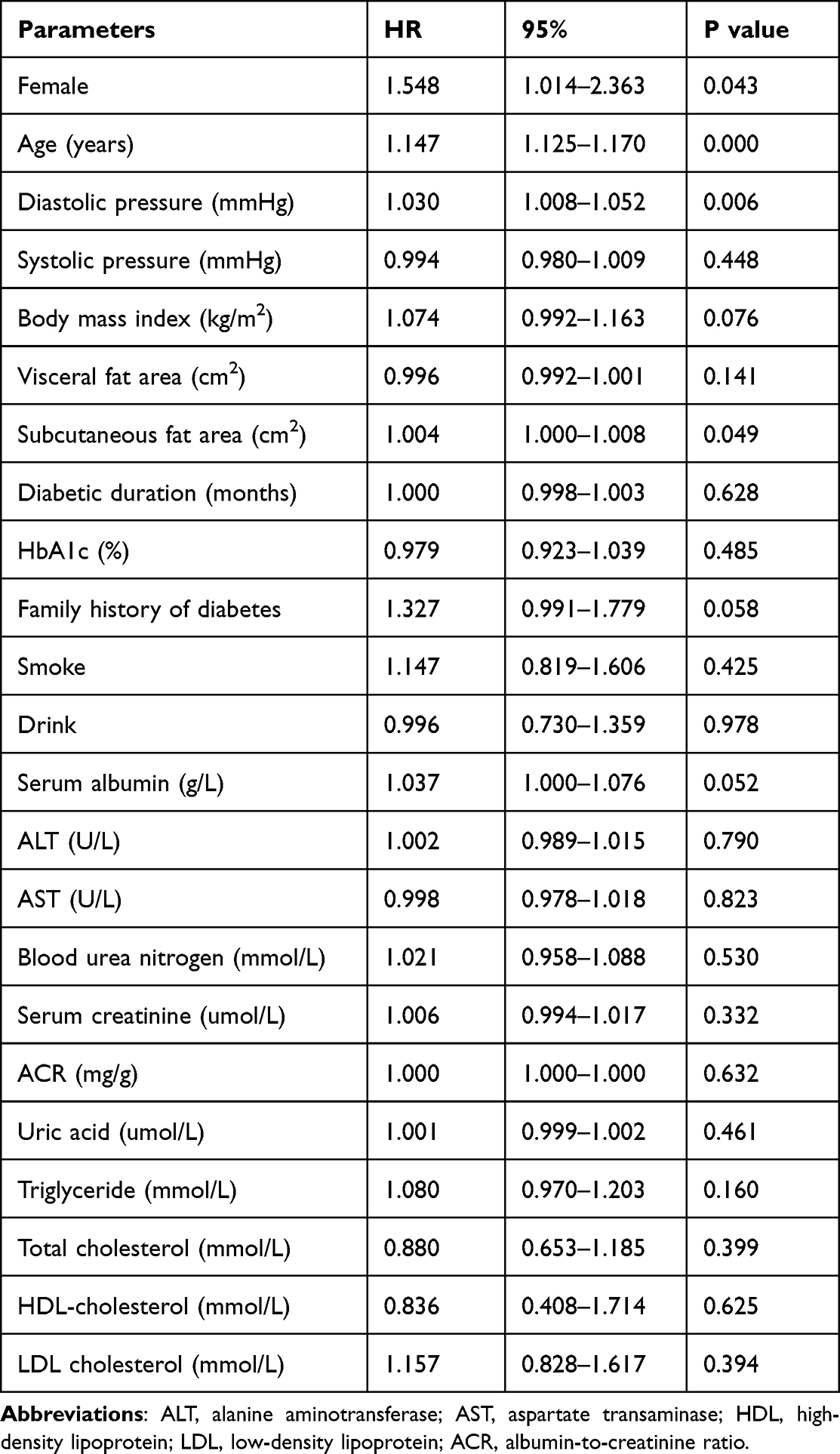 |
Table 3 Multivariate Logistic Regression |
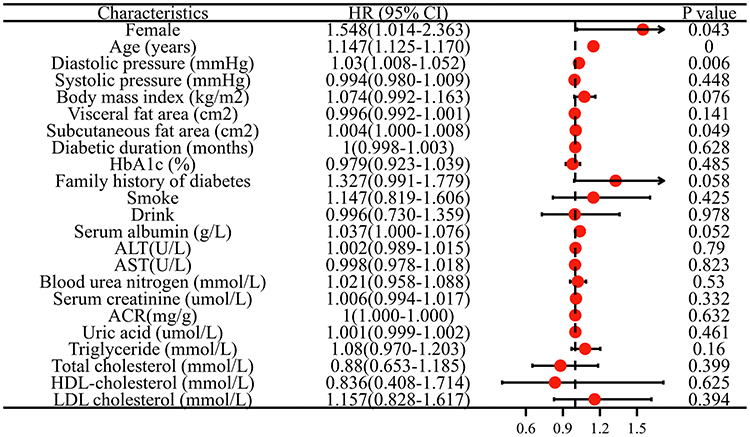 |
Figure 2 The association between clinical factors and left ventricular diastolic dysfunction determined by multivariate logistic analysis. Abbreviations: ALT, alanine aminotransferase; AST, aspartate transaminase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ACR, albumin-to-creatinine ratio; HR, hazard ratio; CI, confidence interval. |
Sex Difference of Left Ventricular Diastolic Dysfunction in Different Age Groups
In the above analysis, we found age was an important factor associated with left ventricular diastolic dysfunction; thus, we analyzed the incidence of it in different age groups. The incidence of left ventricular diastolic dysfunction had no difference between male and female (female vs male, 16.5% vs 13.8%, P > 0.05) in patients less than 45 years old or more than 60 years old (female vs male, 80.2% vs 80.0%,P > 0.05). However, more females were with the left ventricular diastolic dysfunction than males in patients in age group of 45–60 years old (female vs male, 54.5% vs 46.9%, P < 0.05) (Figure 3).
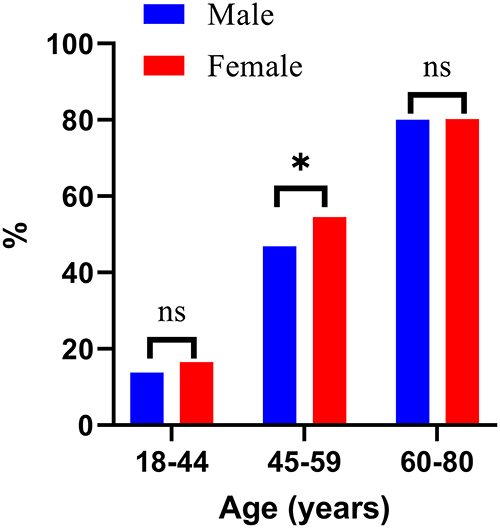 |
Figure 3 The sex difference of left ventricular diastolic dysfunction in different age groups. Abbreviation: ns, not statistically significant. Note: *P < 0.05. |
Discussion
In the current study, we found that females were independently associated with left ventricular diastolic dysfunction in our cohort with type 2 diabetes, even after adjusting for important clinical confounding factors. More females were with the left ventricular diastolic dysfunction than males in patients in age group of 45–60 years old.
Lifestyle changes and obesity increase the susceptibility to diabetes. The incidence of diabetes has increased dramatically, with one in ten people living with diabetes worldwide (https://diabetesatlas.org/). Cardiovascular disease is one of the serious macrovascular complications that causes high mortality of patients with type 2 diabetes. Well-controlled lipid and glycemic levels have decreased the prevalence of cardiovascular disease. However, the incidence of heart failure remains high even after adjusting for common risk factors such as age, hypertension, and hypercholesterolemia in diabetes.10 The estimated prevalence of heart failure in type 2 diabetic reached 22%.11 Recent decades, diabetic cardiomyopathy has been considered as a significant mediating mechanism in the development of heart failure. Diabetic cardiomyopathy is defined as left ventricular dysfunction and cardiac structural maladaptation associated with diabetes independent of established risk factors such as coronary artery disease, hypertension, or valvular heart disease.12 It is characterized by gradual diastolic and systolic dysfunctions. A recent study from the UK Biobank involving 3984 patients also indicated diabetic cardiomyopathy affected the heart globally.13 It is important to slow down the progression of diabetic cardiomyopathy at the beginning. The EMPA-HEART cardioLink-6 randomized clinical trial1 and DAPA-LVH trial14 have both found that empagliflozin and dapagliflozin were able to be beneficial for left ventricular function. Moreover, DELIVER and EMPEROR-preserved studies recently found dapagliflozin and empagliflozin reduced composite cardiovascular death or first hospitalization for heart failure.15 Therefore, identifying patients at high risk of diabetic cardiomyopathy, especially in left ventricular diastolic dysfunction and preserved ejection fraction stage, and giving them appropriate therapy timely are significant.
There are many risk factors associating with diabetic cardiomyopathy, such as BMI,16 diabetic duration,17 and insulin resistance states18 in patients with type 1 diabetes. Obesity women with gestational diabetes mellitus have lower biventricular even in post-partum.19 In our current study, based on type 2 diabetes, we just included patients with normal left ventricular systolic function and found that the higher level of BMI is independently associated with left ventricular diastolic dysfunction. Besides, we found that the older, higher diastolic pressure, and larger subcutaneous fat area also increase the risk for it. Mounting evidence suggests that females have the higher risk for cardiovascular disease.8,20 The Framingham Heart Study indicated that diabetes independently increases the risk of heart failure in men by 2-fold and in women by of 5-fold, comparison with age-matched non-diabetic groups.5 However, there is no study focus on a gender discrepancy of left ventricular diastolic dysfunction in type 2 diabetes. In our study, we found that females were independently associated with the left ventricular diastolic dysfunction, which is regarded as the early stage of diabetic cardiomyopathy.
In addition, we generally believe that the risk of heart disease in pre-menopausal females is lower than in males of the same age because the protective effect of estrogen. However, this protective effect is lost in patients with type 2 diabetes. When we stratified patients by age groups, we found the incidence of left ventricular diastolic dysfunction was same in patients with 18–44 years old and 61–80 years old groups, but the incidence was significantly higher in female with 45–60 years old than male. We speculated it might be associated with hormone fluctuations in perimenopause or menopause. The results remind us to screen the diabetic cardiomyopathy for this group of patients more carefully at an early stage and give them the most appropriate therapy in a timely manner.
The underlying mechanisms of sex differences in diabetic cardiomyopathy are complex and have not yet been studied thoroughly. There are several factors that may contribute to it. First and foremost is the role of sex steroid hormones. It is well documented that estrogen and progesterone have protective effect on glucose homeostasis and metabolic disorder.21 Estrogen and its receptors are also could inhibit vascular injury and22 have effect on endothelial cell growth and smooth muscle differentiation,23 which are beneficial on cardiovascular.24 The most direct evidence is hormone replacement therapy (HRT) of estrogens which protect cardiovascular disease in study.25 However, these protective effects might disappear during the perimenopause and menopause periods and even would play a harmful role. Clarifying the issue can provide evidence of the HRT for females with diabetes who are perimenopause and menopause. There are other contributors of sex differences such as lifestyle. A study showed that testosterone and exercise can promote neoangiogenesis in rats with diabetes, which is associated with the increased expression of VEGF-A and SDF-1a to protect heart.26
In the current cross-sectional study (even in MMC at the First People’s Hospital of Yunnan), we also found that the number of males was almost as twice as females, and males have significantly the higher BMI, triglyceride, and larger visceral fat area. In recent years, sex differences in diabetes have been addressed in many studies. However, it has not been fully understood and reached a consensus. Most epidemiological evidence shows that diabetes is more prevalent in males. According to a national cross-sectional study of China, the prevalence was also higher in males than females.27 The underlying mechanisms are complicated, lifestyle including smoking or drinking, sex steroid hormones, energy expenditure, response for medications, and metabolic features all play important roles in the susceptibility of diabetes. In males, the main metabolic characteristics include the higher skeletal muscle mass, visceral adiposity, and ectopic fat, but females are usually characterized with the higher total fat mass, subcutaneous adiposity, and higher peripheral insulin sensitivity.28
There are several limitations of the study. First, cause and effect cannot be well illustrated in a cross-sectional study, and prospective study is needed in future. Second, we decided to use real-world data to diminish the selective bias, but there are much more males than females in our cohort. This may relate to sex difference of incidence of type 2 diabetes or influenced by behavioral and environmental factors. Third, cardiovascular magnetic resonance is the most advanced way to evaluate cardiac function; however, there are few patients who would accept the examination because of it is expensive, and we would continue to collect results of the examination. Last, in order to study the diabetic cardiomyopathy, we excluded patients with hypertension and cardiovascular disease history. Therefore, the study sample is small.
Conclusion
Left ventricular diastolic function might be worse in female patients with type 2 diabetes. Further study is needed to verify the underlying mechanism.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers 82200815).
Disclosure
Yiting Wang and Yikun Zhou are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Verma S, Mazer CD, Yan AT, et al. Effect of empagliflozin on left ventricular mass in patients with type 2 diabetes mellitus and coronary artery disease: the EMPA-HEART CardioLink-6 randomized clinical trial. Circulation. 2019;140(21):1693–1702. doi:10.1161/CIRCULATIONAHA.119.042375
2. Kanie T, Mizuno A, Takaoka Y, et al. Dipeptidyl peptidase-4 inhibitors, glucagon-like peptide 1 receptor agonists and sodium-glucose co-transporter-2 inhibitors for people with cardiovascular disease: a network meta-analysis. Cochrane Database Syst Rev. 2021;10:Cd013650. doi:10.1002/14651858.CD013650.pub2
3. Mendelsohn ME, Karas RH. Molecular and cellular basis of cardiovascular gender differences. Science. 2005;308:1583–1587. doi:10.1126/science.1112062
4. Catalan M, Herreras Z, Pinyol M, et al. Prevalence by sex of preclinical carotid atherosclerosis in newly diagnosed type 2 diabetes. Nutr Metab Cardiovasc Dis. 2015;25(8):742–748. doi:10.1016/j.numecd.2015.04.009
5. Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34(1):29–34. doi:10.1016/0002-9149(74)90089-7
6. Laverty AA, Bottle A, Kim SH, et al. Gender differences in hospital admissions for major cardiovascular events and procedures in people with and without diabetes in England: a nationwide study 2004–2014. Cardiovasc Diabetol. 2017;16:100. doi:10.1186/s12933-017-0580-0
7. Malmborg M, Schmiegelow MDS, Nørgaard CH, et al. Does type 2 diabetes confer higher relative rates of cardiovascular events in women compared with men? Eur Heart J. 2020;41:1346–1353. doi:10.1093/eurheartj/ehz913
8. Murtaza G, Virk HUH, Khalid M, et al. Diabetic cardiomyopathy - a comprehensive updated review. Prog Cardiovasc Dis. 2019;62:315–326. doi:10.1016/j.pcad.2019.03.003
9. Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American society of echocardiography and the European Association of cardiovascular imaging. J Am Soc Echocardiogr. 2016;29:277–314. doi:10.1016/j.echo.2016.01.011
10. Kenny HC, Abel ED. Heart failure in type 2 diabetes mellitus. Circ Res. 2019;124(1):121–141. doi:10.1161/CIRCRESAHA.118.311371
11. Roberts AW, Clark AL, Witte KK. Review article: left ventricular dysfunction and heart failure in metabolic syndrome and diabetes without overt coronary artery disease — do we need to screen our patients? Diab Vasc Dis Res. 2009;6(3):153–163. doi:10.1177/1479164109338774
12. Dillmann WH. Diabetic cardiomyopathy. Circ Res. 2019;124(8):1160–1162. doi:10.1161/CIRCRESAHA.118.314665
13. Jensen MT, Fung K, Aung N, et al. Changes in cardiac morphology and function in individuals with diabetes mellitus: the UK biobank cardiovascular magnetic resonance substudy. Circ Cardiovasc Imaging. 2019;12(9):e009476. doi:10.1161/CIRCIMAGING.119.009476
14. Brown AJM, Gandy S, McCrimmon R, Houston JG, Struthers AD, Lang CC. A randomized controlled trial of dapagliflozin on left ventricular hypertrophy in people with type two diabetes: the DAPA-LVH trial. Eur Heart J. 2020;41(36):3421–3432. doi:10.1093/eurheartj/ehaa419
15. Vaduganathan M, Docherty KF, Claggett BL, et al. SGLT-2 inhibitors in patients with heart failure: a comprehensive meta-analysis of five randomised controlled trials. Lancet. 2022;400(10354):757–767. doi:10.1016/S0140-6736(22)01429-5
16. Šuran D, Kanič V, Naji F, et al. Predictors of early cardiac changes in patients with type 1 diabetes mellitus: an echocardiography-based study. Bosn J Basic Med Sci. 2019;19:384–391. doi:10.17305/bjbms.2019.4250
17. Jensen MT, Sogaard P, Andersen HU, et al. Prevalence of systolic and diastolic dysfunction in patients with type 1 diabetes without known heart disease: the Thousand and 1 Study. Diabetologia. 2014;57:672–680. doi:10.1007/s00125-014-3164-5
18. Jia G, DeMarco VG, Sowers JR. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat Rev Endocrinol. 2016;12:144–153. doi:10.1038/nrendo.2015.216
19. Sonaglioni A, Barlocci E, Adda G, et al. The impact of short-term hyperglycemia and obesity on biventricular and biatrial. Nutrition, Metabolism and Cardiovascular Diseases. 2022;32(2):456–468.
20. Toedebusch R, Belenchia A, Pulakat L. Diabetic cardiomyopathy: impact of biological sex on disease development and molecular signatures. Front Physiol. 2018;9:453. doi:10.3389/fphys.2018.00453
21. Mauvais-Jarvis F, Clegg DJ, Hevener AL. The role of estrogens in control of energy balance and glucose homeostasis. Endocr Rev. 2013;34:309–338. doi:10.1210/er.2012-1055
22. Karas RH, Schulten H, Pare G, et al. Effects of estrogen on the vascular injury response in estrogen receptor alpha, beta (double) knockout mice. Circ Res. 2001;89:534–539. doi:10.1161/hh1801.097239
23. Knowlton AA, Lee AR. Estrogen and the cardiovascular system. Pharmacol Ther. 2012;135:54–70. doi:10.1016/j.pharmthera.2012.03.007
24. Wu Y, Shen Y, Kang K, et al. Effects of estrogen on growth and smooth muscle differentiation of vascular wall-resident CD34(+) stem/progenitor cells. Atherosclerosis. 2015;240:453–461. doi:10.1016/j.atherosclerosis.2015.04.008
25. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ. 2017;8:33. doi:10.1186/s13293-017-0152-8
26. Chodari L, Mohammadi M, Ghorbanzadeh V, Dariushnejad H, Mohaddes G. Testosterone and voluntary exercise promote angiogenesis in hearts of rats with diabetes by enhancing expression of VEGF-A and SDF-1a. Can J Diabetes. 2016;40:436–441. doi:10.1016/j.jcjd.2016.03.004
27. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
28. Kautzky-Willer A, Harreiter J, Pacini G. Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev. 2016;37:278–316. doi:10.1210/er.2015-1137
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.