Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Feasibility Study of an Early, Interdisciplinary, Non-Pharmacological Intervention for Patients at Risk of Developing Persistent Post-Traumatic Headache: The PTHEENOT intervention
Authors Baatz SRG ![]() , Simonÿ C
, Simonÿ C ![]() , Sejbæk T
, Sejbæk T ![]() , Rytter HM, Mose LS
, Rytter HM, Mose LS ![]()
Received 4 March 2026
Accepted for publication 4 June 2026
Published 12 June 2026 Volume 2026:19 606760
DOI https://doi.org/10.2147/JMDH.S606760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Sasha Revelius Gaj Baatz,1,2 Charlotte Simonÿ,2,3 Tobias Sejbæk,1,2 Hana Malá Rytter,4– 6 Louise Schlosser Mose1,2
1Department of Neurology, University Hospital of Southern Denmark, Esbjerg, Denmark; 2Department of Regional Health Research, University of Southern Denmark, Odense, Denmark; 3The Research and Implementation Unit Progrez, Central and West Zealand Hospital, Slagelse, Denmark; 4Department of Psychology, University of Copenhagen, Copenhagen, Denmark; 5Department of Neurology, University Hospital Bispebjerg-Frederiksberg, Copenhagen, Denmark; 6Danish Concussion Center, Copenhagen, Denmark
Correspondence: Sasha Revelius Gaj Baatz, Department of Neurology, University hospital of Southern Denmark, Finsensgade 35, Esbjerg, 6700, Denmark, Email [email protected]
Purpose: Persistent post-traumatic headache (PTH) is a disabling consequence of mild head injury, leading to functional impairment, reduced quality of life, and adverse vocational outcomes. Evidence-based treatments are limited, and early, interdisciplinary, non-pharmacological interventions have been proposed to prevent symptom persistence. This study assessed the feasibility and acceptability of PTHEENOT (Post-traumatic Headache - Early Engagement in Non-pharmacological Treatment), combining nurse-led Acceptance and Commitment Therapy-based psychoeducation with physiotherapy-guided activity and gradual return to daily life for patients at risk of persistent PTH.
Patients and Methods: A convergent parallel mixed-methods design was used. Adults with acute PTH following mild head injury were recruited between June and October 2024. Quantitative feasibility outcomes included recruitment, retention, adherence, and questionnaire usability rather than intervention effectiveness. Six participants (mean age 40.8 years) completed a five-week intervention at a specialized headache clinic, and self-reported questionnaire data were analyzed descriptively. Qualitative data were obtained through a focus group interview, analyzed using a phenomenological-hermeneutic approach inspired by Ricoeur.
Results: Recruitment was feasible following adjustments, though early symptom improvement and work commitments limited retention. Adherence among completers was high, and questionnaires were manageable. Participants reported perceived improvements in headache management, functional engagement, sleep quality, and self-efficacy. Four themes emerged: 1. Balancing meaningful engagement and program intensity, 2. Gradual improvement and mastery, 3. Peer support is of great value in the recovery process, and 4. Experiences a lack of support and guidance during illness. Peer interactions were important for validation, motivation, and coping, while participants suggested extended session time and follow-up.
Conclusion: The PTHEENOT intervention was acceptable, feasible, and perceived as meaningful by participants, supporting early, interdisciplinary approaches to PTH management. Findings provide guidance for refining intervention structure, delivery, and recruitment strategies prior to a randomized controlled trial aimed at preventing persistent PTH and improving quality of life.
Keywords: mild head injury, mixed-method, cognitive behavioral therapy, graded physical exercise, psychoeducation
Introduction
Persistent post-traumatic headache (PTH) is a frequent and disabling consequence of mild head injury that is associated with substantial functional impairment, reduced quality of life, and adverse vocational outcomes.1–3 The terms mild head injury, concussion and mild traumatic brain injury (mTBI) are often used interchangeably4,5 as they all refer to an injury caused by an external traumatic force that results in physiological disruption of brain function, manifested through clinical signs and symptoms. This convention is also adopted in this paper. Despite the high prevalence and clinical impact of PTH, evidence-based treatment options remain limited.6–8 Estimates suggest that up to two-thirds of patients continue to experience headache one year post-injury,9,10 although reported prevalence varies due to different diagnostic criteria and classification methods.11,12
Approximately 20,000–25,000 individuals in Denmark are diagnosed with mild head injury every year, but the true incidence is likely higher due to underreporting.13 Most patients recover within weeks. However, 30–40% experience persistent post-traumatic symptoms beyond one month, and a subset continues to report headache symptoms up to one year post-injury.2,9,14
According to the International Classification of Headache Disorders (ICHD), PTH is defined as a secondary headache that occurs within seven days of head or neck trauma. During the first three months it is classified as acute and thereafter categorized as persistent.15 The underlying mechanisms of PTH are not fully understood but are considered multifactorial, involving interactions between neurobiological alterations, central sensitization, cervical musculoskeletal dysfunction, and psychological factors.16,17
Once PTH becomes persistent, treatment is challenging. No pharmacological therapies have yet been specifically approved, and management typically relies on migraine and tension-type headache protocols, including simple analgesics, triptans, antidepressants, and anticonvulsants.8,18 However, these approaches have demonstrated limited efficacy in this population.6 A recent systematic review of treatment options for PTH similarly concluded that the current evidence base remains limited, with few high-quality studies and no clear consensus regarding optimal management strategies.19 Similarly, multidisciplinary non-pharmacological interventions initiated at later stages, appear to provide limited effectiveness in patients with established persistent PTH.20
These limitations have prompted growing interest in early, non-pharmacological interventions, initiated during the subacute phase (approximately 2–4 months post-injury), where there may be a window of opportunity to prevent symptom persistence.6,21,22
Persistent post-traumatic symptoms are influenced by multiple interacting factors, including psychological distress and musculoskeletal pain. Neck pain is commonly reported after mild head injury and may contribute to headache persistence, although cervicogenic headache is generally regarded as a distinct diagnostic entity rather than a subtype of PTH.23–25 This multifactorial symptom profile supports the rationale for interdisciplinary treatment approaches that address both physical and psychological components.22,26,27 Physiotherapeutic and psychological interventions have therefore been proposed as promising early treatment strategies,23,26,27 with cognitive-behavioral approaches delivered within an interdisciplinary framework appearing to offer the greatest potential benefit.22
Acceptance and Commitment Therapy (ACT), a third-wave cognitive-behavioral approach, has demonstrated effectiveness in persistent pain populations by enhancing psychological flexibility and promoting value-driven behavior change,28–30 making it a relevant component in early PTH management.
Despite growing consensus regarding the potential of early interdisciplinary, non-pharmacological interventions, the current evidence base remains limited. Large-scale randomized controlled trials are lacking, and critical uncertainties persist regarding acceptability, feasibility, and implementation in routine clinical settings.6,21,31 According to current guidance on complex intervention development, feasibility studies are a necessary step prior to effectiveness testing.32 Therefore, as part of the development of a complex intervention, this feasibility study evaluates an early interdisciplinary, non-pharmacological intervention-PTHEENOT (Posttraumatic Headache – Early Engagement in Non-pharmacological Treatment). The study focuses on acceptability, fidelity of delivery, and overall practicality, and identifies contextual barriers and facilitators relevant to future implementation. Findings will inform refinement of the intervention and guide the design of a subsequent randomized controlled trial aimed at reducing the occurrence and severity of persistent PTH and improving patients’ quality of life.
Methods
Study Design
This feasibility study was designed using a convergent parallel mixed-methods approach.33 Quantitative and qualitative data were collected concurrently. The quantitative component focused on feasibility outcomes, including clarity and usability of questionnaires, functionality of the automated scheduling system, and timely delivery of follow-up questionnaires.34,35 The qualitative component consisted of a focus group interview (FGI), guided by a semi-structured interview protocol,36 to explore participants’ experiences with the interdisciplinary PTHEENOT intervention.
The two datasets were analyzed separately using descriptive summaries for quantitative feasibility checks and a Ricoeur-inspired phenomenological-hermeneutic approach for qualitative analysis,37,38 and subsequently integrated during interpretation.33
Intervention
The PTHEENOT intervention was specifically designed for patients at risk of persistent PTH to support early symptom management and facilitate a gradual return to daily activities. It draws on a humanistic approach, which supports patients in mastering life with illness by actively understanding and managing their health challenges.39 Based on ACT principles, the intervention combined psychoeducation with individualized physical exercise to address both psychological and physical aspects of recovery.28,30 Psychoeducational sessions included exercises, group discussions, therapeutic metaphors,40,41 and mindfulness techniques to foster knowledge, behavior change, and internalization of therapeutic concepts.29,42,43 This design acknowledges that participants bring prior experiences and knowledge, and it encourages experiential, practice-focused learning, prompting reflection and application of ACT principles in real-life contexts such as work, social interactions, and daily routines.28
The physiotherapeutic component complemented this approach by translating ACT principles, such as values and committed action, into guided physical activity, encouraging patients to gradually re-engage in meaningful movement and daily activities.1 The interdisciplinary structure, delivered by experienced nurses and physiotherapists trained in ACT, further supported a holistic, person-centered approach.44 This ensured a consistent therapeutic message across sessions and facilitated the integration of psychological and physical rehabilitation.1,28,29
The Intervention Setting and Structure
The PTHEENOT intervention was developed and implemented following the MRC framework for complex interventions.45 In line with the framework, intervention components were designed based on existing evidence and theoretical principles. This feasibility study corresponds to the development phase and assesses acceptability, fidelity, and practical implementation before a full-scale RCT.
Sessions were delivered at the specialized Headache Clinic at the University Hospital of Southern Denmark in Esbjerg. The program consisted of five weekly sessions, each comprising a 90-minute nurse-led educational segment, followed by a break and a 90-minute physiotherapy session. The decision to structure the intervention as five weekly sessions was informed by previous similar intervention studies. In addition, the timeframe was designed to support early symptom management following mild head injury while remaining clinically implementable within a hospital setting.31,46
The nurse-led sessions covered topics such as ACT principles, psychoeducation, occupational rehabilitation, and strategies for gradually resuming daily activities, including both cognitive and social tasks such as reading, computer work, household chores, and social interaction.47–49 Physiotherapy sessions included strength training, relaxation techniques, and cardiovascular exercises like walking, running, or cycling. Participants also received home exercise materials to support ongoing activity between sessions. An overview of the core elements of the five-week intervention is shown in Table 1. A more detailed description of nurse-led cognitive and educational components, and physiotherapy exercises is provided in Supplementary Table 1.
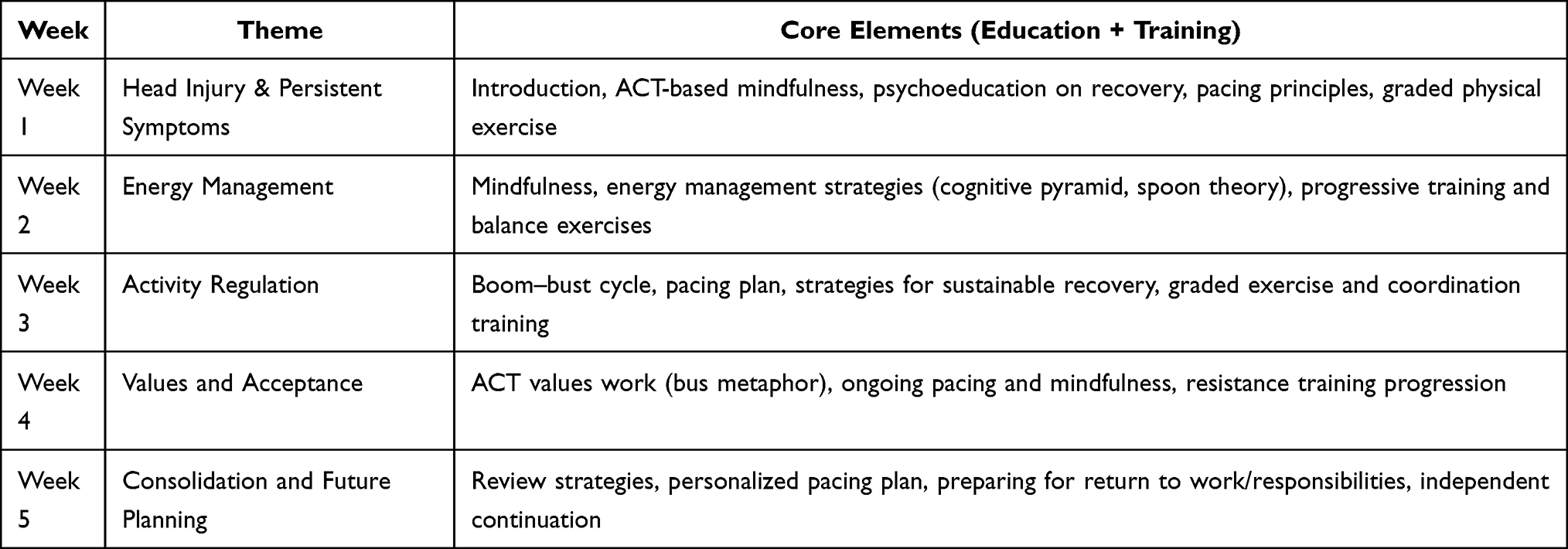 |
Table 1 Overview of the Core Elements of the Five-Week PTHEENOT Intervention |
During the intervention period, the first author maintained ongoing dialogue with the healthcare professionals through scheduled weekly meetings and ad hoc consultations to discuss the progress of the intervention. This approach ensured consistent implementation, adherence to ACT principles, and fidelity to the planned procedures.45 Following completion of the intervention, the healthcare professionals participated in a structured evaluation to inform potential refinements of the upcoming RCT.
Study Population and Recruitment
Participants with mild head injury were recruited between June and October 2024, with the intervention administered from November to December 2024. Eligible participants were recruited from the Medical Helpline in the Region of Southern Denmark. From June to September 2024, potential participants with head injury were provided with a contact phone number if symptoms persisted beyond six weeks. Internal Emergency Department records in Esbjerg indicate that approximately 54 patients with head injury are diagnosed monthly (unpublished departmental data). However, recruitment proceeded slowly. Seven potential participants contacted the provided number, and six reported symptom improvements before inclusion.
As a result, recruitment strategies were expanded to include general practitioner (GP) referrals and social media outreach. All GPs in the Region of Southern Denmark were informed about the study through meetings, emails, and newsletters. Recruitment posters were created and placed in GP waiting rooms, on social media, and in public spaces such as pharmacies, libraries, and sports facilities, encouraging eligible participants to contact the research team (the poster is available in Supplementary File 1). A visual overview of the recruitment process and subsequent strategy adjustment is provided in Figure 1.
 |
Figure 1 Recruitment flow, strategy adjustments, and inclusion outcomes. Initial recruitment via the Medical Helpline was slow, leading to an expanded strategy, including general practice referrals and social media promotion, which improved recruitment and enabled a timely intervention start. Vertical arrows indicate progression through the recruitment process, while horizontal arrows indicate participant flow between eligibility, withdrawal, and enrolment. |
Participants were recruited according to the following inclusion criteria:
- Age 18 to 60 years.
- Head injury within the past 2–6 months following a reported traumatic event (eg., fall, assault, contact sport engagement), either confirmed by a physician or clinically suspected based on the presence of ongoing posttraumatic symptoms (eg., headache, dizziness, cognitive difficulties), consistent with mild head injury.
- Self-reported headache lasting more than 15 days per month in accordance with the ICHD criteria for persistent post-traumatic headache.15
- Proficiency in both written and spoken Danish.
Participants were excluded if:
- History of head injury with persistent residual effects.
- Continued use of analgesic medications for more than 14 days per month during the last month, consistent with thresholds associated with medication overuse headache as defined by the ICHD.15
- A history of headaches occurring on average more than 10 days per month during the three months before the head injury.
- Presence of severe dementia or comorbid neurological or psychiatric disorders of significant severity.
- Inability to actively participate or engage in the intervention.
The upper age limit of 60 years was chosen because older adults may present with different comorbidities, recovery trajectories, or medication use, which could confound the feasibility outcomes. This carefully defined study population was selected to ensure that the feasibility study addressed the relevant target group for the PTHEENOT intervention, enabling a focused evaluation of recruitment strategies, intervention acceptability, and procedural practicality in preparation for an RCT.
Data Collection
Quantitative data were collected at baseline and after the five-week intervention using standardized questionnaires. All six participants completed baseline questionnaires, and four completed follow-up questionnaires. Responses were summarized descriptively to assess feasibility of administering standardized questionnaires and inform refinements for the upcoming RCT. Qualitative data were collected through a FGI conducted six weeks after the intervention. Hereby, we explored participants’ experiences with the intervention and the study procedures.
This convergent parallel design combined descriptive quantitative data with in-depth qualitative insights to assess the usability of study procedures and participants’ experiences with the intervention, PTHEENOT.
Questionnaires
All participants received online questionnaires at baseline and after the intervention to assess the feasibility of: 1) the overall survey setup, 2) the clarity of the questionnaire items, and 3) the functionality of the automated delivery system, including whether the follow-up questionnaire was sent as scheduled after the intervention. The questionnaires were completed electronically and stored in compliance with national approval (24/36139) and EU legislation using REDCap, a secure web-based application designed for building and managing online surveys and databases.50
The Headache Impact Test (HIT-6)
The severity and impact of headaches were assessed using the Headache Impact Test (HIT-6), a widely used and psychometrically validated instrument for measuring headache-related disability in various populations and languages.51 It assesses how headaches affect patients’ ability to function at work, school, home, and in social settings. The questionnaire includes six items rated on a five-point scale (never = 6, rarely = 8, sometimes = 10, very often = 11, always = 13), with individual item scores summed to create a total score ranging from 36 to 78. Higher scores indicate a greater negative impact of headaches on overall functioning.52 A Danish translation was used in this study; however, a formal psychometric evaluation has not yet been published in a Danish population.
Coping Strategy Questionnaire (CSQ)
Coping strategies were assessed using the Coping Strategy Questionnaire (CSQ), a widely used instrument that evaluates cognitive and behavioral pain-coping strategies. It includes six cognitive coping subscales: Ignoring pain, reinterpretation of pain, diverting attention, coping self-statements, catastrophizing, praying/hoping; as well as two behavioral subscales: increasing activity levels and rising pain behaviors.53,54 Each subscale contains six items rated on a numerical scale from 0 (I never do that) to 6 (I always do that), reflecting how often participants use each coping strategy to manage headache pain. Subscale scores range from 0 to 36, with higher scores indicating greater use of the corresponding coping strategy.53 A Danish translation was used in this study; however, to our knowledge, a full psychometric validation of the CSQ has not yet been published in a Danish population.
The 36-Item Short Form Survey (SF-36)
Health-related quality of life, including mental, physical, emotional, and social functioning, was assessed using the 36-item Short Form Survey (SF-36), a reliable and validated instrument frequently used across diverse patient groups.55 The SF-36 consists of 36 items organized into eight scales that measure different health domains: physical functioning, role limitations due to physical health, role limitations due to emotional problems, social functioning, bodily pain, mental health, vitality, and general health perceptions. These scales each contribute differently to the overall physical and mental health summary scores. The raw scores for each scale are coded and linearly transformed to a 0–100 scale, where higher scores indicate better health status.32,55,56 The SF-36 has been translated and extensively validated in the Danish population, demonstrating good psychometric properties.57
Headache Features
Additionally, participants responded to four customized items designed to capture headache-related burden: number of sick leave days during the past month, and headache intensity rated on a 0–10 numeric rating scale for the past week, the past month (overall), and the past 24 hours.
Focus Group Interview (FGI)
The qualitative component consisted of an FGI conducted in a meeting room at the University Hospital of Southern Denmark. After completing the program, participants were invited by email. A semi-structured interview guide was developed, drawing on a phenomenological-hermeneutic approach inspired by the French philosopher Paul Ricoeur.38,58 This approach emphasizes creating an open dialogue that allows participants to reflect on their lived experiences and articulate the meanings attached to them.
During the FGI, participants were encouraged to share their thoughts and reflections on their lived experiences of the PTHEENOT intervention, including the interdisciplinary sessions and any perceived changes in headache symptoms or daily functioning. Topics covered included the setup of the intervention, perceptions of the weekly schedule, and the perceived sufficiency of the weekly 90-minute nurse-led and physiotherapy sessions. Participants also disclosed experiences with persistent headache symptoms before and after the intervention, the resources they gained from the program, and any perceived effects from their participation. Of the six participants, who completed the program, four attended the FGI. The two-hour session was facilitated by the first author, audio-recorded and subsequently transcribed verbatim with minor editing into 30 pages of text using Amberscript. The transcriptions were reviewed for accuracy.37
Analyses
Questionnaires
Data from the questionnaires were examined descriptively, as the study was not powered to detect statistical differences. Questionnaire responses were not interpreted as indicators of intervention effectiveness but rather as part of a feasibility evaluation to inform the design of the upcoming RCT.
Focus Group Interview
The data from the FGI were analyzed through a three-level interpretive process, inspired by Ricoeur’s theory on narratives and interpretation.37,38,58,59 As illustrated in Figure 2, the process included: A naïve reading in which we read and re-read the text to grasp an initial overall understanding of participants’ lived experiences. A structural analysis leading to the identification of themes that reflect participants’ experiences of participating in PHEENOT. By a critical interpretation, we obtained the last and sophisticated level of understanding by discussing the findings with other research to bring them from the individual to the general level. The themes identified in the structural analysis are presented with selected quotes in the Results section. The critical interpretation informs the Discussion section, providing a nuanced understanding of the data.
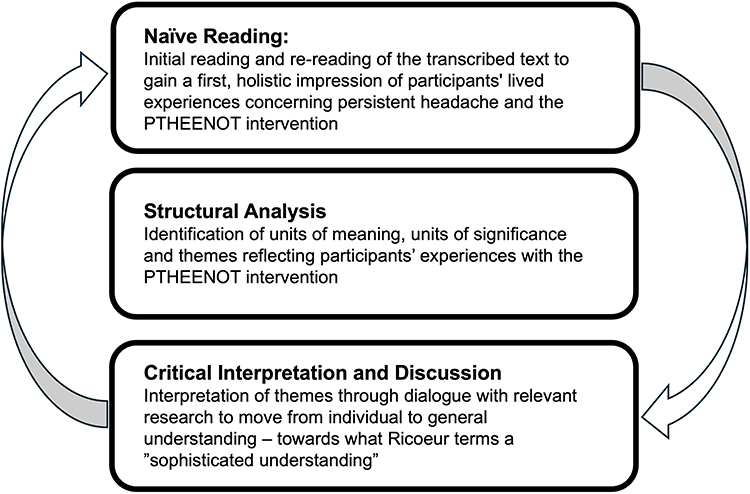 |
Figure 2 Three-level Interpretive Analysis Inspired by Paul Ricoeur. The overall interpretation involves a dialectical movement between naive reading, structural analysis, and critical interpretation and discussion. It encompasses moving understandings between explanation and comprehension, wherein lies an internal validation of initial preconceptions and presumptions.60 This leads to what Ricoeur names a sophisticated understanding of the world that the text reveals.58 |
The analysis was conducted manually, using reflective memos made during transcription and interpretive notes generated throughout the analytic process, both of which supported reflexivity and depth. To ensure rigour and consistency, the first and last authors maintained ongoing dialogue throughout the analytic process.61 The interview was conducted in Danish and later translated into English for reporting. Quotations included in the article have been translated by the authors, with efforts made to preserve meaning and tone. Participant anonymity was maintained by using ID numbers (eg., P1, P2). An example of the analytic process is shown in Table 2.
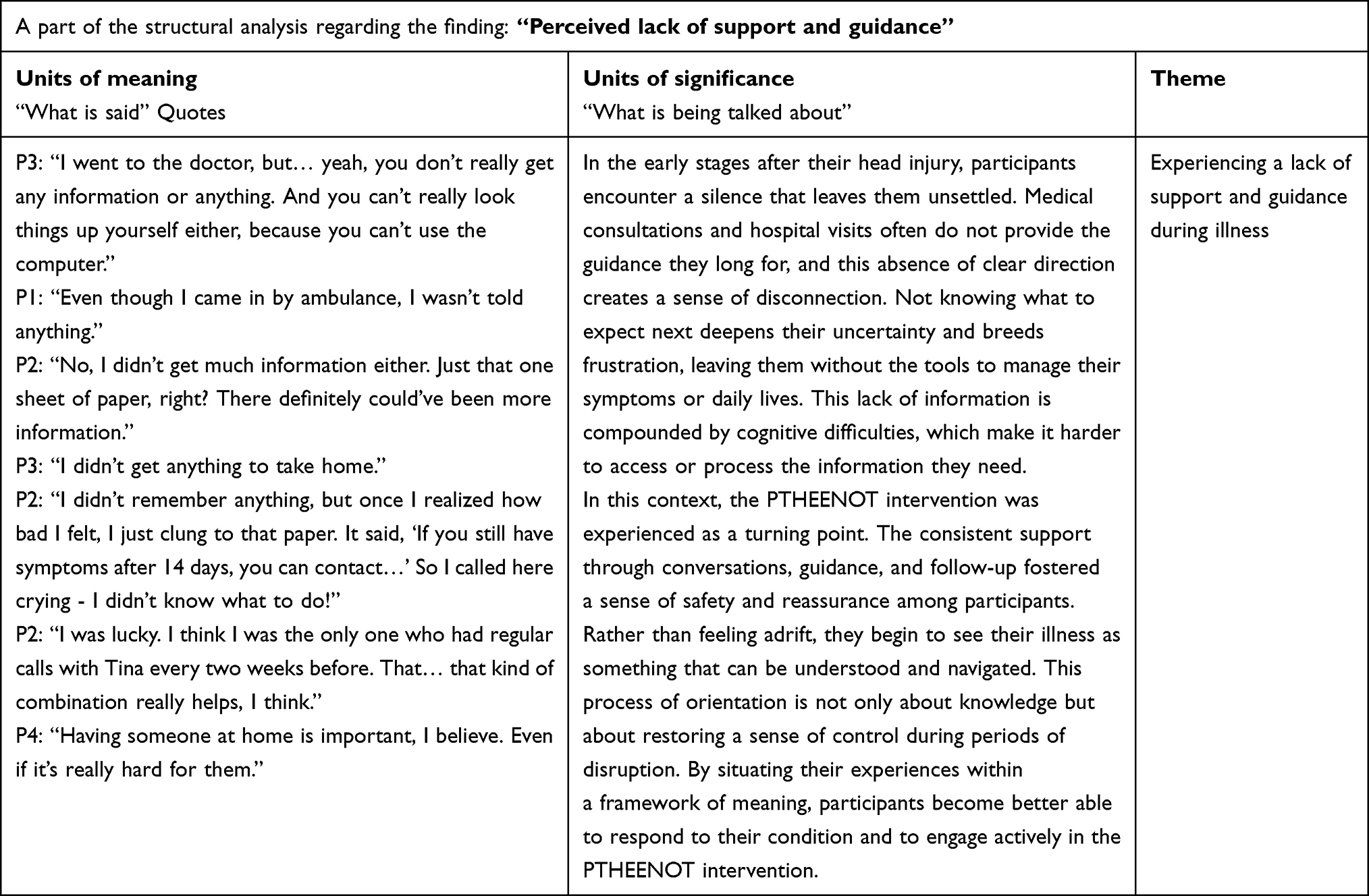 |
Table 2 An Example of the Structural Analysis, from the PTHEENOT Study |
The final themes presented below illustrate the balancing act between explanation and understanding, which is central to Ricoeur’s theory of interpretation.37,38
Results
In line with the convergent mixed-methods design, quantitative and qualitative findings were considered parallel and integrated during interpretation. Due to the exploratory nature of this feasibility study, greater interpretive weight was placed on qualitative findings, while quantitative measures were used to contextualize participant experiences and assess procedural feasibility. This triangulation revealed that perceived improvements in symptom manageability, functional engagement, and self-efficacy were more clearly articulated in participants’ narratives than reflected in standardized questionnaire scores.
Recruitment and Adherence Outcomes
A total of twenty-three potential participants expressed interest in the study. Eleven were excluded after the initial phone call, leaving twelve who met the inclusion criteria and were invited to participate in the intervention program. Of these, four withdrew before the intervention began, three due to work commitments, and one because of symptom remission.
In November 2024, the intervention started with a group of eight participants. Two dropped out after the first session due to illness, leaving six who completed the program. Three participants attended all five sessions, while three participated in four sessions.
These findings indicate that recruitment was feasible following adjustments within the designated timeframe, although work commitments and early symptom improvement limited retention. Adherence among completers was high, with half attending all sessions, and the rest missing only one.
The six participants who completed the intervention were all female, with a mean age of 44 years (range 31–58). The duration of persistent headache symptoms before inclusion ranged from 9 to 26 weeks. Baseline clinical characteristics, including headache frequency and intensity, are summarized in Table 3.
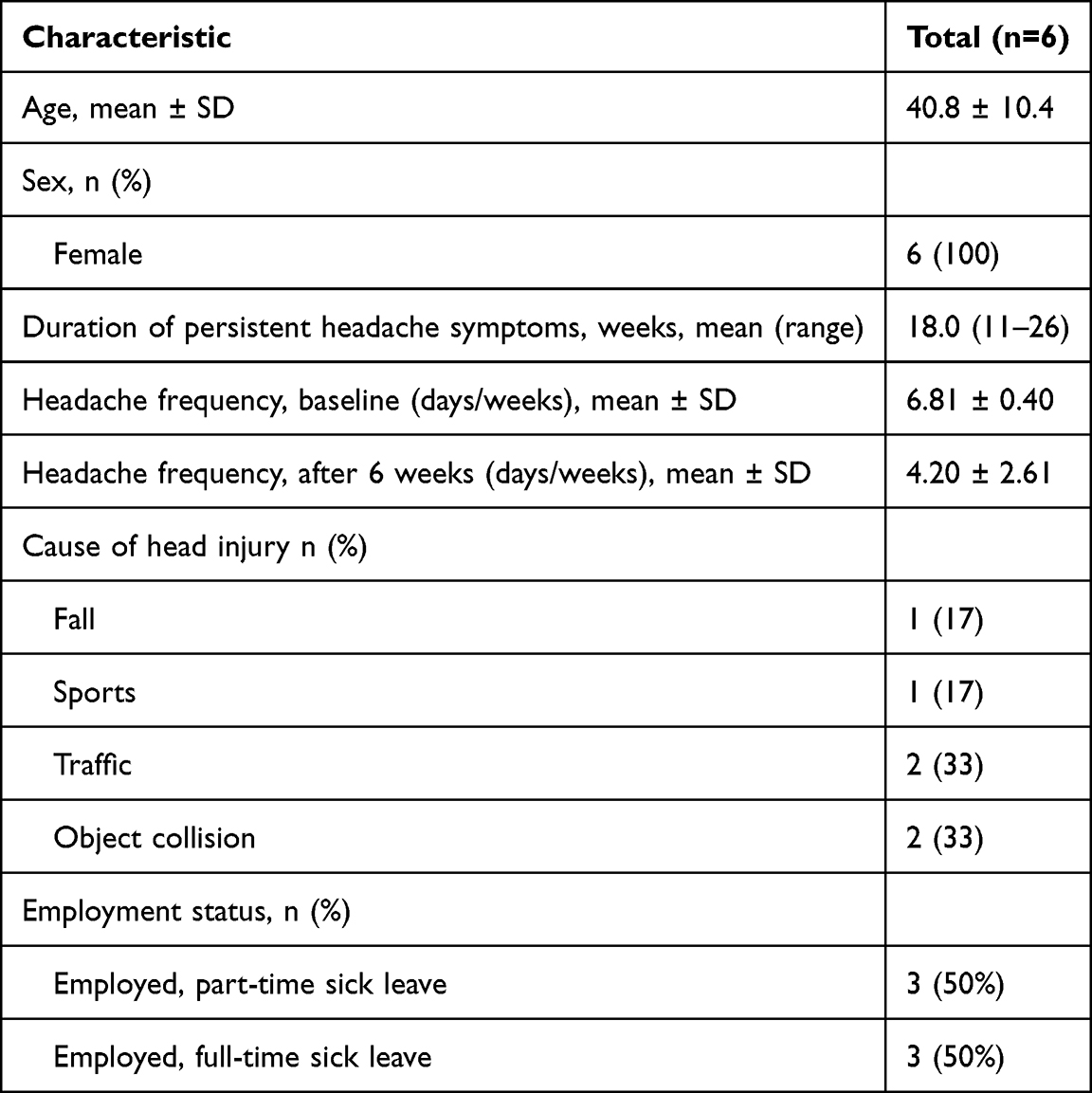 |
Table 3 Characteristics of Participants Completing the PTHEENOT Intervention |
Questionnaires
Questionnaire responses demonstrated the feasibility of the study measures. All participants completed the baseline questionnaires, and four completed the follow-up questionnaires after five weeks. Descriptive reviews indicated that the questionnaires were generally understandable and feasible for participants to complete. Descriptive results for all administered questionnaires are presented in Table 4.
 |
Table 4 Descriptive Results From the Questionnaires |
Symptom Burden
At baseline, all participants self-reported multiple symptoms in addition to persistent headache, indicating a high overall symptom burden. Commonly reported symptoms included photophobia and phonophobia, concentration problems, sleep difficulties, and fatigue, each reported by all six participants. Neck pain, dizziness, and mood disturbances were reported by some participants, reflecting individual variation in symptom presentation as summarized in Table 5.
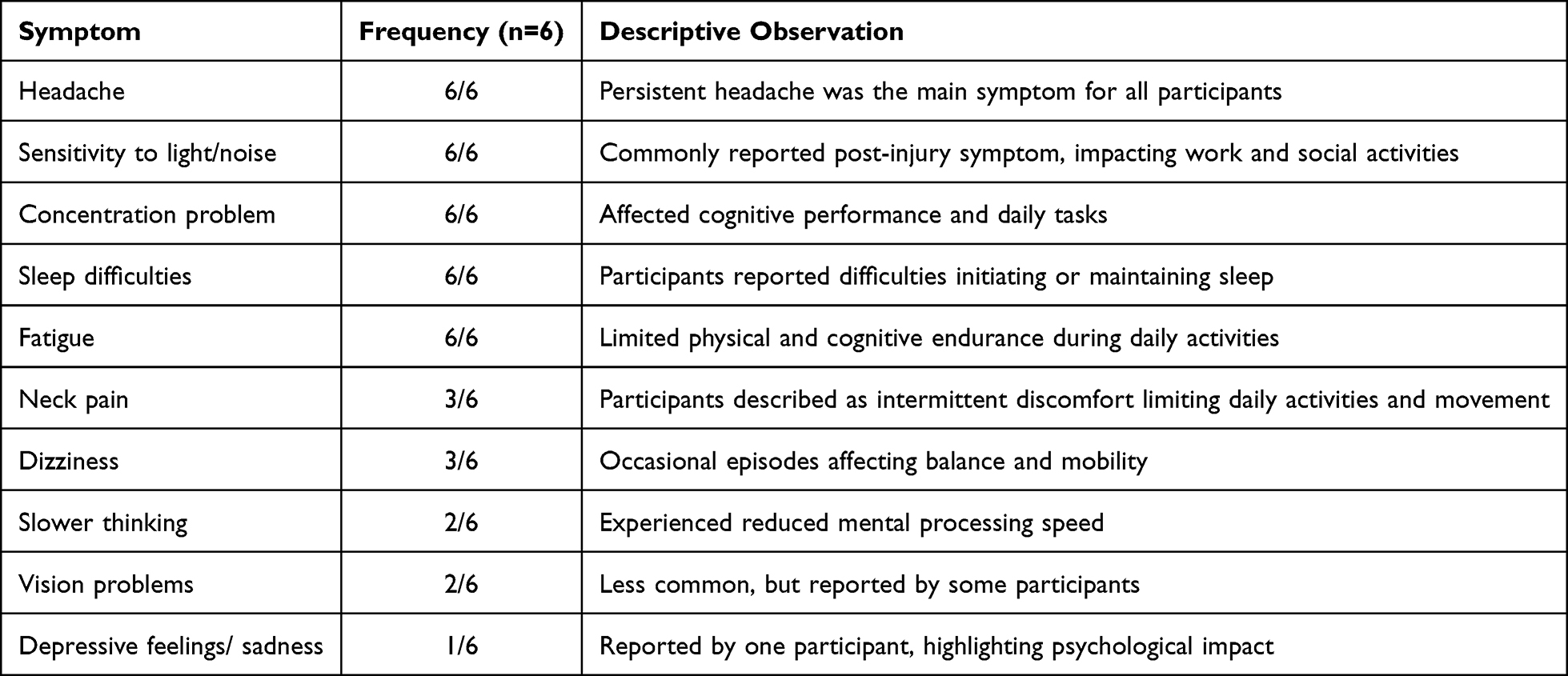 |
Table 5 Baseline Symptom Burden |
Outcome Measures
Based on the FGI, no technical difficulties were reported in connection with the questionnaires. Participants found the questions presented in a logical order, clearly communicated, and easy to understand. There were no reports of confusion, missing items, or challenges in completing the questionnaires. Completion rates were 100% at baseline and 67% at follow-up.
Overall, descriptive patterns suggested reduced headache-related disability (HIT-6) and lower headache intensity from baseline to follow-up. Health-related quality of life (SF-36) was characterized by generally low baseline scores across physical and mental domains, with only minor changes observed at follow-up. Coping strategies (CSQ) remained largely stable, although small shifts toward more adaptive coping strategies and increased perceived pain control were noted. Sick leave data suggested a possible reduction in work absence for some participants, as summarized in Table 4. Given the small sample size, these quantitative findings should be interpreted cautiously and primarily in conjunction with the qualitative results.
Focus Group Interview
The three-level Interpretive Analysis revealed four key themes reflecting participants’ experiences and perceptions of the intervention. Figure 3 illustrates these themes and provides an integrative visual synthesis summarizing the main insights. This visual summary highlights the interconnected nature of participants’ experiences with PTHEENOT, and the findings inform acceptability, perceived value, implementation challenges, and contextual considerations relevant to the intervention’s feasibility and future scalability.
 |
Figure 3 An Illustration of participants’ experiences with the PTHEENOT intervention. |
Theme 1. Balancing Meaningful Engagement and Program Intensity
Participants described widespread appreciation for the PTHEENOT intervention, which they experienced as meaningful and supportive, emphasizing that its variety and professional quality had an impact on both body and mind. As one participant noted: “I felt it made a difference—it’s the walks and training that truly helped me recover” (P1). This sentiment was echoed by others, who highlighted how their emotions were acknowledged and taken seriously by both nurses and physiotherapists. Another participant shared, with visible appreciation: “I found the teaching sessions to be really good and more important than I had expected” (P2). These reflections convey an experience of being genuinely met and supported, where PTHEENOT was not merely a program but a source of recognition and renewed self-awareness in the recovery process.
Although the overall evaluation was positive, participants pointed out structural challenges. They perceived time pressure, which limited opportunities for rest and reflection, as one participant, with a skeptical tone, explained: “There were times when we had, what, 12 minutes from finishing here to being over there. And in that time, we had to eat, go to the restroom, everything” (P4). Others nodded in agreement, and another added with emphasis: “I think we could have used 15 more minutes. It wasn’t just small talk; we were having important conversations” (P3). This shared response underlined a sense of being hurried, where meaningful dialogue risked being cut short. The atmosphere in the group suggested that these interruptions were not only practical inconveniences but also barriers to deeper reflection and connection.
Despite these structural challenges, participants consistently described the intervention as both demanding yet transformative. One participant expressed: “Getting started with physical activity is really beneficial, and taking mental breaks is also important; mindfulness proved to be very helpful” (P2). Another, recalling her initial despair, noted: “I was hopeless at the beginning, thinking it would never go away. But that changed. We discussed a lot about mindfulness and how the mind works—and that helped me” (P2).
PTHEENOT was experienced as an unfolding path, one that participants did not initially recognize, yet which slowly opened new horizons of hope and recovery. These reflections show how the intervention supported not only coping, but also a re-interpretation of what it meant to live with and move beyond illness.
Taken together, the group reflections illustrate a tension between the program’s therapeutic depth and its rigid time frames. While participants valued the meaningful content and professional guidance, the limited opportunities for rest and shared reflection sometimes left them with a sense of incompleteness. The narratives make visible a movement between being recognized and being constrained, between support and pressure. In this way, PTHEENOT was lived not simply as an intervention, but as a meaningful passage into new ways of inhabiting recovery.
Theme 2. Gradual Improvement and Mastery
Participants described gradual and meaningful improvements in functioning, symptom relief, and a growing sense of control over their lives. Although progress was often fragile and non-linear, it was experienced as motivating and significant. One participant reflected on the changing presence of headaches, which had once dominated daily life: “I used to wake up with a headache every day. Now I can go for days without even thinking about it. Then suddenly I realize, hey, I have not had a headache in a while” (P2). As this was shared, others nodded in agreement, some smiling quietly in recognition, and one added: “You can actually get used to not having headaches every day” (P4). These observations convey not only how participants gradually reclaimed a sense of bodily predictability and relief, but also the shared understanding that came from hearing similar experiences reflected in the group.
Participants also observed improvements in cognitive performance and physical endurance, making previously impossible tasks achievable, though still challenging. One participant explained with a tone of pride: “I can do it now. A few months ago, I couldn’t. Now I can, but it still tires me” (P1). Another described how bodily awareness guided adaptation: “I’ve started my physical training. Once I felt really unwell, so I just stopped and rested, and then it was gone” (P2). These accounts highlight a process of learning to listen to the body, balancing activity and rest.
Adaptive coping and self-regulation emerged as central elements of this journey. One participant shared, with determination: “It’s much better now. I keep telling myself that—there’s no stagnation. I’m still moving forward” (P4). Another reflected with quiet satisfaction: “It’s important to reflect on where I was a month ago. I was doing worse. So, I remind myself: it’s getting better” (P2). These reflections suggest that participants actively structured their experiences into a narrative of progress, finding reassurance in small, incremental achievements.
Sleep quality was another domain of noticeable improvement. One participant recalled: “I used to sleep terribly in the beginning, but pretty early in the program, I began sleeping really well” (P1). Another added with relief: “This morning I thought I’d sleep just one more hour. I ended up getting three and a half hours of deep sleep - that hasn’t happened in a month” (P4). These experiences illustrate how recovery was tangibly felt in daily rhythms, shaping energy and well-being.
Alongside symptom relief, participants described a growing sense of mastery and self-efficacy. Tasks that had once required extensive rest became manageable, allowing for renewed engagement in social and physical life. One participant said, with evident satisfaction: “I used to have to rest after work before I could do anything. Now I just go out right after” (P3). Another reflected: “Now I do more on weekends—before, I’d just walk the dog and collapse on the sofa” (P4). These stories convey an expanding sense of self-efficacy and the possibility of inhabiting life more fully.
Recovery was experienced as an unfolding, ongoing journey. Participants described becoming more active and making deliberate choices about energy, pacing, and priorities: ”I used to have headaches and dizziness. But now, I have only experienced a headache twice since January. That’s it” (P2). Another participant leaned forward and began speaking eagerly, clearly wanting to share her experience: “I started looking at things week by week—what I can manage now and what I couldn’t do last week. Small steps and managing my energy. Deciding when to do something for myself and when to do something for others” (P1).
Taken together, these reflections illustrate how participants began to re-narrate their illness experience as a process of gradual mastery and regained control. Their language signals a movement from chaos toward coherence, where the challenges of recovery were transformed into meaning and personal growth. In inhabiting this journey, participants actively reconfigured their relationship to both their bodies and their daily lives, discovering renewed possibilities for engagement, autonomy, and self-understanding.
Theme 3. Peer Support Is of Great Value in the Recovery Process
A key part of participants’ recovery experience was the sense of mutual recognition and understanding developed within the group. Unlike the early stages of their illness, often characterized by uncertainty and a lack of information, participants described the group as a place where their experiences were validated and shared. One participant reflected with a mixture of relief, as she looked back on her experiences: “So many shocks I had—you’ve all had them too… Getting an explanation for that, I think that was important” (P1), recognizing that others had faced similar challenges. As this was shared, other participants nodded and exchanged brief glances, silently acknowledging the commonality of their experiences.
The group setting provided both emotional support and practical insight. Participants discussed treatment strategies, asked questions, and reflected on their own progress in relation to others. These exchanges offered reassurance that challenges were not uncommon and that coping was possible. One participant described the motivating effect of this shared accountability: “It motivated me to walk and do the physical exercises because I had to be prepared for Tuesday” (P1). Smiles and occasional laughter punctuated these moments, revealing a sense of connection and lightness amid the ongoing challenges of recovery.
However, some participants also noted a sense of abruptness at the program’s conclusion. One participant expressed with hesitation: “There could have been some kind of follow-up… I don’t know if that’s a phone call or something like that” (P2). A few others murmured in agreement, suggesting that while the group offered meaningful support, continuity beyond the program remained a concern. These reflections highlight the importance of sustained opportunities for peer interaction to reinforce both motivation and emotional well-being.
Overall, participants’ experiences underscore the value of group-based recovery settings where individuals can share experiences, compare progress, and exchange coping strategies. These interactions foster not only inspiration but also a deeper sense of being seen and understood by others facing similar challenges. In inhabiting this shared space, participants were able to reframe their own experiences, transforming isolation and uncertainty into mutual recognition and solidarity. The attentive gestures, nods, and subtle smiles throughout the discussions further reinforced a sense of collective understanding. This social connectedness appeared to be a vital component in supporting engagement, resilience, and the ongoing journey of recovery.
Theme 4. Experiencing a Lack of Support and Guidance During Illness
Participants described feeling unsupported both during the early stages of their illness and after completing the structured five-week program. A common concern was the lack of clear information, proper follow-up, and continuity, especially at times when they felt vulnerable and uncertain. In the acute phase, participants recalled confusion and distress due to the lack of guidance from healthcare providers. One participant reflected, with a tense in her voice: “Even though I came in by ambulance, I wasn’t told anything” (P1).
Another added, expressing frustration over the isolation this created: “You don’t really get any information or anything. And you can’t really look things up yourself either, because you can’t use a computer” (P2).
For some, even a single sheet of paper became a crucial anchor in an otherwise disorienting experience. One participant remembered, with visible unease: “I didn’t remember anything, but once I realized how bad I felt, I just clung to that paper. It said, ‘if you still have symptoms after 14 days, contact...’ So, I called here crying, I didn’t know what to do!” (P1).
The group responded with quiet acknowledgment, nodding and murmuring softly, signaling a shared understanding of the vulnerability and fear described.
This lack of early support often carried over into the rehabilitation phase. Participants expressed concern that the program ended too soon, before new habits were fully established, leaving them unsure how to sustain progress. One participant said, with a note of frustration: “If you’re trying to build a new habit, it takes about three months. And this was a five-week program. So, it’s easy to fall back into the same old routine” (P3).
Another stated firmly, with clear frustration: “I felt like I was let go too early” (P1). Small gestures of follow-up were described as potentially transformative: “I found it very hard to overcome that obstacle—what if I don’t recover? That’s why I believe some follow-up might have helped” (P1). The group voiced agreement, showing a collective understanding of the gap in support.
Participants also highlighted the importance of understanding and support, at home and in the workplace. Several spoke of the need to actively involve family members to foster comprehension of their challenges. One participant reflected with relief, recognizing the support she had at home, knowing not everyone was as fortunate: “I believe it’s important to have someone at home, I think. Even if it’s hard on them” (P3).
Overall, these reflections underscore the critical need for ongoing, structured support that continues beyond the end of the intervention program. Participants emphasized the importance of clear information and guidance soon after their head injury, as well as continuous contact to support new routines, offer reassurance, and help them feel less isolated in their recovery process. In sharing these experiences within the group, participants were able to articulate the gaps in support and treatment and envision what might help them navigate recovery more securely. Their narratives reveal how meaningful support, both timely and sustained, can transform vulnerability into a pathway toward agency and confidence in managing daily life after illness.
Discussion
This feasibility study provides insights into how six patients at risk of persistent PTH experience the PTHEENOT intervention. Overall, participants described the intervention as meaningful, supportive, and feasible, valuing the tailored content, interdisciplinary professional guidance, and peer interaction. At the same time, they emphasized a need for adjustments related to pacing and extended follow-up to support sustained engagement and integration of strategies.
Feasibility and Acceptability
Overall feasibility outcomes indicate that the PTHEENOT intervention can be delivered with acceptable adherence and procedural fidelity in a clinical setting. While recruitment and retention posed challenges, adherence among participants who completed the program was high, and online questionnaires were perceived as clear and manageable. Together, these findings support the acceptability of the intervention format and study procedures while underscoring the importance of refined recruitment strategies and scheduling flexibility in future trials.
Reconstruction and Agency
The study reflects how participants actively reconstruct meaning from their recovery experiences, gradually transforming vulnerability into agency and confidence.59 Viewed through the lens of Bury’s concept of biographical disruption,62 it becomes clear how post-traumatic headache disrupted participants’ everyday lives and roles, while PTHEENOT facilitated the reconstruction of new forms of continuity and meaning. Moreover, Charmaz’s work on loss and reconstruction of self63 further supports this interpretation, emphasizing how chronic illness can challenge identity and self-perception. According to Charmaz, recognition, validation, and peer support are essential for regaining a sense of agency. In this light, PTHEENOT appeared to provide a meaningful and supportive context in which participants´ experiences were acknowledged and shared, thereby supporting the intervention’s acceptability and feasibility.
These findings are consistent with a recent qualitative study, which examined work identity among individuals living with persistent post-concussion symptoms.64 In this study, participants articulated a profound sense of loss associated with their professional roles, frequently describing how ongoing symptoms threatened their sense of self, competence, and future orientation. It is argued that prolonged symptoms may progressively undermine identity and personal agency, thereby highlighting the need for rehabilitation approaches that offer recognition, sustained support, and interdisciplinary care throughout the recovery process.64
Within this framework, PTHEENOT may be conceptualized as an example of the type of supportive, interdisciplinary intervention. By integrating symptom management with ACT principles, peer support, and physical activity, the intervention appears to provide participants with opportunities to redefine their identities, re-establish a sense of agency, and reconstruct meaning in the context of persistent symptoms.
Raised Illness Mastery
Participants also reported gradual improvement in areas such as headache frequency, physical endurance, sleep quality, and self-efficacy. These experiences are consistent with existing evidence suggesting that early non-pharmacological interventions based on ACT principles, emphasizing psychological flexibility and value-driven action, may positively influence recovery.28,30 In addition, the integration of physiotherapy aligns with prior research indicating that graded physical activity can be safe and beneficial in reducing PTH symptom burden.1,6 Moreover, participants described co-occurring symptoms, such as cognitive difficulties, fatigue, sleep disturbances, and sensory hypersensitivity. This underscores the multidimensional nature of persistent PTH and supports the relevance of an interdisciplinary intervention addressing a broad spectrum of post-injury symptoms.16 Taken together, these findings suggest that PTHEENOT may support gradual recovery, illness mastery, and self-efficacy, even when progress is experienced as non-linear.
Valuable Peer Support
Peer support proved to be a central and highly valued component of the intervention. Participants described experiences of mutual recognition, validation, and motivation through interactions with peers who shared similar challenges. These findings align with previous research demonstrating that group-based interventions can reduce social isolation, enhance coping strategies, and improve adherence in rehabilitation settings.65,66 From a theoretical perspective, peer interactions may function as a key mechanism for reconstructing selfhood, as described by Charmaz,63 by enabling participants to move from experiences of loss and isolation toward recognition, agency, and renewed identity. In this study, peer support contributed to participants’ motivation and sense of belonging, reinforcing engagement in the intervention.
Need for Follow-Up and Program Intensity
Despite overall positive experiences, participants identified challenges related to program intensity and limited follow-up. Several described a sense of time pressure during nurse-led sessions, which constrained opportunities for reflection and dialogue. This finding is particularly relevant given that patients with persistent PTH symptoms frequently experience cognitive impairments, including reduced attention span, mental fatigue, and concentration difficulties.6,8,22
The original structure of the intervention, with 90-minute nurse-led sessions, was deliberately designed to accommodate these cognitive vulnerabilities by limiting session duration and information load. However, participant feedback indicated that the density of content within this timeframe created a sense of rushing, which interfered with reflective processes central to ACT principles.30,67 From a theoretical perspective, learning under conditions of cognitive load is optimized when sufficient time is provided for processing, reflection, and integration of new knowledge. For patients with acquired cognitive impairments, excessive time pressure may increase cognitive load, thereby reducing engagement and learning efficiency.68
In response to these findings, the nurse-led sessions in the upcoming RCT have been extended from 90 to 120 minutes. This adjustment allows for a slower pace, structured pauses, and deeper reflection without increasing overall cognitive burden. Furthermore, the intervention has been modified to include a structured follow-up phone call 2–4 months after program completion, aimed at supporting continued application of intervention strategies. Together, these refinements illustrate how participants’ experiences informed optimization of the intervention and delivery prior to an RCT. In addition, participants found the online questionnaires clear and manageable, with no technical issues reported, which is why they were considered appropriate to retain for the subsequent RCT.
Recruitment Feasibility
Recruitment emerged as a central feasibility challenge. Initial recruitment through the medical helpline alone proved insufficient, resulting in slower-than-anticipated enrollment. Although this pathway was selected to facilitate early identification and timely consent, reliance on a single access point limited reach to the target population. Patients at risk of persistent PTH are often managed in primary care or community settings, with limited contact with specialized healthcare services in the subacute phase.69 This makes recruitment through hospital-based pathways alone challenging. Recruitment feasibility improved after expanding pathways to include GP referrals, posters in community settings, and social media outreach. This multi-channel approach aligns with previous feasibility literature demonstrating that diversified recruitment strategies are often necessary to reach non-hospitalized populations.70,71 Based on these findings, recruitment strategies for the upcoming RCT have been refined to include multiple access points across both healthcare and community settings, improving the practicality of enrolling a representative sample.
Strengths and Limitations
A key strength of this feasibility study is its focus on assessing the practicality, acceptability, and implementation of the PTHEENOT intervention using a convergent mixed-methods design. Quantitative data were used to examine procedural aspects such as recruitment, retention, adherence, questionnaire usability, and follow-up procedures, while qualitative data from a focus group interview provided insight into participants’ experiences of participating in the intervention and study procedures. This approach aligns with the MRC framework for complex interventions, which emphasizes the importance of understanding how interventions are delivered and experienced before proceeding to effectiveness testing.
The qualitative component, analyzed using a phenomenological-hermeneutic approach inspired by Ricoeur, enabled an in-depth exploration of how participants made sense of their illness and the intervention. Collaborative interpretation among authors enhanced reflexivity and supported a transparent analytic process, contributing to the trustworthiness of the findings.
Several limitations should be considered. The study included a small sample size, and recruitment and retention proved challenging, with participant withdrawal occurring both before and during the intervention. These challenges reflect known difficulties in engaging individuals with mild head injury and persistent symptoms and underline the importance of refining recruitment strategies and intervention logistics before a full-scale RCT. As the study was not designed or powered to assess effectiveness, quantitative outcome data were interpreted solely as indicators of feasibility and participant burden. An additional limitation is that all participants included in this feasibility study were female. Although eligibility was not restricted by sex, no male participants volunteered during the recruitment period. This limits the transferability of the findings across sexes, as feasibility and acceptability of the intervention may differ in male participants, and highlights the need for broader recruitment strategies in future studies to ensure more representative participant inclusion.
Some discrepancies were observed between participants’ subjective experiences described in the qualitative interviews and the changes captured in standardized questionnaires. Rather than representing inconsistency, this highlights the complementary role of qualitative methods in feasibility research, where experiential insights can inform refinement of outcome selection, timing, and follow-up procedures in future trials.
In summary, despite limitations related to sample size and recruitment, this study provides valuable feasibility data regarding intervention acceptability, procedural challenges, and contextual factors influencing participation. These findings offer clear guidance for refining both the PTHEENOT intervention and the research design prior to conducting an RCT.
Conclusion
This convergent mixed-methods feasibility study suggests that the interdisciplinary PTHEENOT intervention is acceptable, feasible, and meaningful for patients at risk of persistent PTH following mild head injury. Although the sample was small and involved only female participants, the mixed-method design provided rich insights into both participants’ experiences and intervention feasibility, which can inform refinements for a future RCT. Participants valued the combination of ACT-based psychoeducation, physiotherapy, and peer support, which supported gradual recovery, illness mastery, and self-efficacy, while highlighting the importance of pacing and structured follow-up to sustain gains.
Clear recruitment pathways, schedule transparency, and the combination of online measures with FGI proved feasible and manageable. Peer interactions emerged as a key mechanism for validation, motivation, and coping, reinforcing the value of group-based approaches within interdisciplinary interventions. Aligned with the MRC framework, these findings support progression to an RCT, incorporating refinements such as expanded recruitment pathways and structured follow-up.
Trial Registration
The trial was registered at ClinicalTrials.gov (NCT06466499). Ethical approval was obtained from the Regional Committee on Health Research Ethics for Southern Denmark (S-20240057) and the Region of Southern Denmark (24/34801).
Abbreviations
PTH, Persistent Posttraumatic Headache; ICHD - International Classification of Headache Disorders; ACT, Acceptance and Commitment Therapy; MRC, Medical Research Council; RCT, Randomized Controlled Trial; FGI, Focus Group Interview; GP, General Practitioners; SF-36, The 36-item Short Form Survey; CSQ, Coping Strategy Questionnaire; HIT6, Headache Impact Test.
Data Sharing Statement
The datasets generated and/or analyzed during the current study include transcribed FGI and responses to questionnaires administered via REDcap. Due to the sensitive and confidential nature of the data, these materials are not publicly available but may be made available by the corresponding author on reasonable request and with appropriate ethical approval.
Ethics Approval and Informed Consent
All participants were informed about the voluntary nature of the study and provided written consent for their participation and the use of their data. Participant confidentiality and anonymity were maintained throughout the study, including data collection, storage, and analysis. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Concent for Publication
The authors confirm that any images, figures, or other materials included in this manuscript can be published, and all participants have provided consent for their use.
Acknowledgment
The authors would like to thank OPEN (Open Patient Data Explorative Network) at the University of Southern Denmark and Odense University Hospital for facilitating access to the REDCap database, as well as the staff of The Headache Clinic at the University Hospital of Southern Denmark, for delivering the interdisciplinary treatment program to the participating patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was financially supported by a PhD scholarship from the Faculty of Health Sciences at the University of Southern Denmark, a research grant from the Regional Research Fund of Southern Denmark, and grants from the Karola Jørgensen Foundation and the Danish patient organization Migræne og Hovedpineforegningen. The funders had no role in the study design; collection, analysis, or interpretation of data, nor in the writing of the manuscript or the decision to submit the paper for publication.
Disclosure
LSM has received travel and speaker honoraria from Lundbeck A/S. These activities are unrelated to the present work. The remaining authors declare no competing interests in this work.
References
1. Heslot C, Cogné M, Guillouët E, et al. Management of unfavorable outcome after mild traumatic brain injury: review of physical and cognitive rehabilitation and of psychological care in post-concussive syndrome. Neurochirurgie. 2021;67(3):283–20. doi:10.1016/j.neuchi.2020.09.001
2. Cancelliere C, Verville L, Stubbs JL, et al. Post-concussion symptoms and disability in adults with mild traumatic brain injury: a systematic review and meta-analysis. J Neurotrauma. 2023;40(11–12):1045–1059. doi:10.1089/neu.2022.0185
3. Graff HJ, Siersma V, Møller A, et al. Labour market attachment dynamics in patients with concussion: a Danish nationwide register-based cohort study. BMC Public Health. 2023;23(1):2493. doi:10.1186/s12889-023-17364-2
4. Silverberg ND, Iverson GL, Cogan A, et al. The American congress of rehabilitation medicine diagnostic criteria for mild traumatic brain injury. Arch Phys Med Rehabil. 2023;104(8):1343–1355. doi:10.1016/j.apmr.2023.03.036
5. Davis GA, Patricios J, Schneider KJ, et al. Definition of sport-related concussion: the 6th international conference on concussion in sport. Br J Sports Med. 2023;57(11):617–618. doi:10.1136/bjsports-2022-106650
6. Rytter HM, Graff HJ, Henriksen HK, et al. Nonpharmacological treatment of persistent postconcussion symptoms in adults: a systematic review and meta-analysis and guideline recommendation. JAMA Network Open. 2021;4(11):e2132221. doi:10.1001/jamanetworkopen.2021.32221
7. Bergersen K, Halvorsen J, Tryti EA, et al. A systematic literature review of psychotherapeutic treatment of prolonged symptoms after mild traumatic brain injury. Brain Inj. 2017;31(3):279–289. doi:10.1080/02699052.2016.1255779
8. Heslot C, Azouvi P, Perdrieau V, et al. A systematic review of treatments of post-concussion symptoms. J Clin Med. 2022;11(20):6224. doi:10.3390/jcm11206224
9. Schwedt TJ. Post-traumatic headache due to mild traumatic brain injury: current knowledge and future directions. Cephalalgia. 2021;41(4):464–471. doi:10.1177/0333102420970188
10. Lucas S, Hoffman JM, Bell KR, et al. A prospective study of prevalence and characterization of headache following mild traumatic brain injury. Cephalalgia. 2014;34(2):93–102. doi:10.1177/0333102413499645
11. DCFH. Posttraumatisk hovedpine, 2025. Available from: https://dcfh.dk/viden-om-hjernerystelse/behandling-af-senfoelger/posttraumatisk-hovedpine-efter-hjernerystelse/.
12. Voormolen DC, Cnossen MC, Polinder S, et al. Divergent classification methods of post-concussion syndrome after mild traumatic brain injury: prevalence rates, risk factors, and functional outcome. J Neurotrauma. 2018;35(11):1233–1241. doi:10.1089/neu.2017.5257
13. Eggertsen PP, Cordsen P, Lauritsen J, et al. Incidence and prevalence of concussion in denmark from 1999 to 2018: a nationwide cohort study. J Neurotrauma. 2025;42(11–12):994–1007. doi:10.1089/neu.2024.0217
14. Ashina H, Iljazi A, Al-Khazali HM, et al. Persistent post-traumatic headache attributed to mild traumatic brain injury: deep phenotyping and treatment patterns. Cephalalgia. 2020;40(6):554–564. doi:10.1177/0333102420909865
15. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38:1–211. doi:10.1177/0333102417738202
16. Sørensen AN, Rytter HM. Vidensrapport om let hovedtraume, herunder hjernerystelse – Voksne. København: Dansk Center for Hjernerystelse; 2024.
17. Silverberg ND. Behavioral treatment for post-traumatic headache after mild traumatic brain injury: rationale and case series. NeuroRehabilitation. 2019;44(4):523–530. doi:10.3233/nre-192708
18. Bendtsen L, Birk S, Kasch H, et al. Reference programme: diagnosis and treatment of headache disorders and facial pain. Danish headache society, 2nd Edition, 2012. J Headache Pain. 2012;13(Suppl S1):S1–29. doi:10.1007/s10194-011-0402-9
19. Minen MT, Mahmood N, Khan F, et al. Treatment options for posttraumatic headache: a current review of the literature. Curr Pain Headache Rep. 2024;28(4):205–210. doi:10.1007/s11916-023-01199-y
20. Abd-Albaqi SW. The effect of multidisciplinary open-label treatment in patients with persistent post-traumatic headache at two tertiary headache centers. Pain Manag. 2026;16(5):. 471–478 doi:10.1080/17581869.2026.2638405
21. Lee MJ, Zhou Y, Greenwald BD. Update on non-pharmacological interventions for treatment of post-traumatic headache. Brain Sci. 2022;12(10):1357. doi:10.3390/brainsci12101357
22. Sanford EM, Sramek KN, McGeary DD, et al. Behavioral, non-pharmacological intervention modalities to alleviate persistent headache attributable to traumatic brain injury: a systematic review of patient pain outcomes in the context of the mutual maintenance model. Cephalalgia. 2025;45(5):3331024251341237. doi:10.1177/03331024251341237
23. Mavroudis I, Ciobica A, Luca AC, et al. Post-traumatic headache: a review of prevalence, clinical features, risk factors, and treatment strategies. J Clin Med. 2023;12(13):4233. doi:10.3390/jcm12134233
24. Coffeng SM, Jacobs B, de Koning ME, et al. Patients with mild traumatic brain injury and acute neck pain at the emergency department are a distinct category within the mTBI spectrum: a prospective multicentre cohort study. BMC Neurol. 2020;20(1):315. doi:10.1186/s12883-020-01887-x
25. Bogduk N. Cervicogenic headache: anatomic basis and pathophysiologic mechanisms. Curr Pain Headache Rep. 2001;5(4):382–386. doi:10.1007/s11916-001-0029-7
26. Register-Mihalik JK, DeFreese JD, Callahan CE, et al. Utilizing the biopsychosocial model in concussion treatment: post-traumatic headache and beyond. Curr Pain Headache Rep. 2020;24(8):44. doi:10.1007/s11916-020-00870-y
27. Dansk Center for hjernerystelse. National Klinisk Retningslinje for non-farmakologisk behanling af længerevarende symptomer efter hjernerystelse. København; 2021.
28. Martinez-Calderon J, García-Muñoz C, Rufo-Barbero C, et al. Acceptance and commitment therapy for chronic pain: an overview of systematic reviews with meta-analysis of randomized clinical trials. J Pain. 2024;25(3):595–617. doi:10.1016/j.jpain.2023.09.013
29. Vasiliou VS, Karademas EC, Christou Y, et al. Acceptance and commitment therapy for primary headache sufferers: a randomized controlled trial of efficacy. J Pain. 2021;22(2):143–160. doi:10.1016/j.jpain.2020.06.006
30. Feliu Soler A, Montesinos F, Gutiérrez-Martínez O, et al. Current status of acceptance and commitment therapy for chronic pain: a narrative review. J Pain Res. 2018;11:2145–2159. doi:10.2147/jpr.S144631
31. Argyriou AA, Mitsikostas -D-D, Mantovani E, et al. An updated brief overview on post-traumatic headache and a systematic review of the non-pharmacological interventions for its management. Expert Rev Neurother. 2021;21(4):475–490. doi:10.1080/14737175.2021.1900734
32. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239. doi:10.1136/bmj.i5239
33. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches.
34. Bowen DJ, Kreuter M, Spring B, et al. How we design feasibility studies. Am J Prev Med. 2009;36(5):452–457. doi:10.1016/j.amepre.2009.02.002
35. Leon AC, Davis LL, Kraemer HC. The role and interpretation of pilot studies in clinical research. J Psychiatr Res. 2011;45(5):626–629. doi:10.1016/j.jpsychires.2010.10.008
36. Patton M. Qualitative Research and Evaluation Methods.
37. Simonÿ C, Specht K, Andersen IC, et al. A ricoeur-inspired approach to interpret participant observations and interviews. Glob Qual Nurs Res. 2018;5:2333393618807395. doi:10.1177/2333393618807395
38. Simonÿ C, Damsgaard JB, Johansen K, et al. The power of a ricoeur-inspired phenomenological-hermeneutic approach to focus group interviews. J Adv Nurs. 2026;82(5):5457–5466. doi:10.1111/jan.70133
39. Simonÿ C, Andersen IC, Bodtger U, et al. Raised illness mastering – a phenomenological hermeneutic study of chronic obstructive pulmonary disease patients’ experiences while participating in a long-term telerehabilitation programme. Disabil Rehabil Assist Technol. 2022;17(5):594–601. doi:10.1080/17483107.2020.1804630
40. Tilahun B. What Is the Spoon Theory? 2021. Available from: https://health.clevelandclinic.org/spoon-theory-chronic-illness.
41. Miserandino C. The Spoon Theory. 2003. Available from: https://cdn.totalcomputersusa.com/butyoudontlooksick.com/uploads/2010/02/BYDLS-TheSpoonTheory.pdf.
42. Vesterskov B, Mose LS. Recognizing, accepting, and belonging: patient learning and experiences in a structured headache education program. J Multidiscip Healthc. 2025;18:8053–8066. doi:10.2147/jmdh.S564841
43. Cathcart S, Galatis N, Immink M, et al. Brief mindfulness-based therapy for chronic tension-type headache: a randomized controlled pilot study. Behavioural and Cognitive Psychotherapy. 2014;42(1):1–15. doi:10.1017/s1352465813000234
44. Kitson A, Marshall A, Bassett K, et al. What are the core elements of patient-centred care? A narrative review and synthesis of the literature from health policy, medicine and nursing. J Adv Nurs. 2013;69(1):4–15. doi:10.1111/j.1365-2648.2012.06064.x
45. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. Int J Nurs Stud. 2024;154:104705. doi:10.1016/j.ijnurstu.2024.104705
46. Thastum MM, Rask CU, Naess-Schmidt ET, et al. Design of an early intervention for persistent post-concussion symptoms in adolescents and young adults: a feasibility study. NeuroRehabilitation. 2018;43(2):155–167. doi:10.3233/nre-172391
47. Ettenhofer ML, Remigio-Baker RA, Bailie JM, et al. Best practices for progressive return to activity after concussion: lessons learned from a prospective study of U.S. military service members. Neurotrauma Reports. 2020;1(1):137–145. doi:10.1089/neur.2020.0023
48. Antcliff D, Keeley P, Campbell M, et al. Activity pacing: moving beyond taking breaks and slowing down. Qual Life Res. 2018;27(7):1933–1935. doi:10.1007/s11136-018-1794-7
49. Innovation AfC. Pacing - learning to do a little bit often. 2024. Available from: https://aci.health.nsw.gov.au/chronic-pain/brain-injury/physical-activity/pacing?utm.
50. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
51. Kothari SF, Eggertsen PP, Frederiksen OV, et al. Characterization of persistent post-traumatic headache and management strategies in adolescents and young adults following mild traumatic brain injury. Sci Rep. 2022;12(1):2209. doi:10.1038/s41598-022-05187-x
52. Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6™. Qual Life Res. 2003;12(8):963–974. doi:10.1023/a:1026119331193
53. Abbott A. The coping strategy questionnaire. J Physiother. 2010;56(1):63. doi:10.1016/s1836-9553(10)70061-8
54. Keefe FJ, Crisson J, Urban BJ, et al. Analyzing chronic low back pain: the relative contribution of pain coping strategies. Pain. 1990;40(3):293–301. doi:10.1016/0304-3959(90)91126-4
55. Ware JE Jr, Kosinski M, Bayliss MS, et al. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the medical outcomes study. Med Care. 1995;33(4 Suppl):As264–279.
56. Ware JE, Kosinski M. Interpreting SF&-36 summary health measures: a response. Qual Life Res. 2001;10(5):405–420. doi:10.1023/a:1012588218728
57. Bjorner JB, Thunedborg K, Kristensen TS, et al. The Danish SF-36 health survey: translation and preliminary validity studies. J Clin Epidemiol. 1998;51(11):991–999. doi:10.1016/s0895-4356(98)00091-2
58. Ricoeur P. Interpretation Theory: Discourse and the Surplus of Meaning. Fort Worth, Texas: Texas Christian University Press; 1976.
59. Ricoeur P. Time and Narrative (Translated). University of Chicago Press; 1984.
60. Dreyer PS, Pedersen BD. Distanciation in Ricoeur’s theory of interpretation: narrations in a study of life experiences of living with chronic illness and home mechanical ventilation. Nurs Inq. 2009;16(1):64–73. doi:10.1111/j.1440-1800.2009.00433.x
61. Karwacka W. Quality assurance in medical translation. J Specialised Translation. 2014;(21):19–34. doi:10.26034/cm.jostrans.2014.382
62. Bury M. Chronic illness as biographical disruption. Sociol Health Illness. 1982;4(2):167–182. doi:10.1111/1467-9566.ep11339939
63. Charmaz K. Good days, Bad Days: The Self in Chronic Illness and Time. New Brunswick, NJ: Rutgers University Press; 1991.
64. Rytter HM, Attauabi S, Hansen LS, et al. “It feels like a loss of one’s own identity” - Work identity in persons suffering persisting post-concussion symptoms: a qualitative study. Disabil Rehabil. 2025:1–16. doi:10.1080/09638288.2025.2578994
65. Shalaby RAH, Agyapong VIO. Peer support in mental health: literature review. JMIR Ment Health. 2020;7(6):e15572. doi:10.2196/15572
66. Wellecke C, Douglas J, Winkler D, et al. Peer support needs, preferences and experiences of adults with acquired neurological disability: a scoping review protocol. BMJ Open. 2024;14(10):e088237. doi:10.1136/bmjopen-2024-088237
67. Rauwenhoff JC, Bol Y, van Heugten CM, et al. Acceptance and commitment therapy for people with acquired brain injury: rationale and description of the BrainACT treatment. Clin Rehabil. 2023;37(8):1011–1025. doi:10.1177/02692155231154124
68. Sweller J, Ayres P, Kalyuga S. Cognitive Load Theory. New York: Springer; 2011.
69. Galili SF, Bech BH, Vestergaard C, et al. Use of general practice before and after mild traumatic brain injury: a nationwide population-based cohort study in Denmark. BMJ Open. 2017;7(12):e017735. doi:10.1136/bmjopen-2017-017735
70. Helm A, Kaufman M, Glassy N, et al. Strategies for recruiting participants underrepresented in clinical research: a scoping review. Soc Sci Med. 2025;385:118603. doi:10.1016/j.socscimed.2025.118603
71. Hoffmann SH, Paldam Folker A, Buskbjerg M, et al. Potential of online recruitment among 15-25-year olds: feasibility randomized controlled trial. JMIR Form Res. 2022;6(5):e35874. doi:10.2196/35874
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.