Back to Archived Journals » Research and Reviews in Parkinsonism » Volume 12
Fear of Falling Avoidance Behavior Assessment and Intervention in Parkinson’s Disease: A Scoping Review
Authors Rider JV ![]() , Longhurst JK
, Longhurst JK ![]() , Lekhak N, Young DL
, Lekhak N, Young DL ![]() , Landers MR
, Landers MR
Received 1 December 2021
Accepted for publication 31 January 2022
Published 16 March 2022 Volume 2022:12 Pages 1—17
DOI https://doi.org/10.2147/JPRLS.S350890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Peter Hedera
John V Rider,1,2 Jason K Longhurst,3 Nirmala Lekhak,4 Daniel L Young,2 Merrill R Landers2
1School of Occupational Therapy, Touro University Nevada, Henderson, NV, USA; 2Department of Physical Therapy, School of Integrated Health Sciences, University of Nevada, Las Vegas, Las Vegas, NV, USA; 3Department of Physical Therapy and Athletic Training, Saint Louis University, St. Louis, MO, USA; 4Department of Nursing, University of Nevada, Las Vegas, Las Vegas, NV, USA
Correspondence: John V Rider, School of Occupational Therapy, Touro University Nevada, 874 American Pacific Dr, Henderson, NV, 89014, USA, Tel +1 801 717 6445, Fax +1 702 777 4837, Email [email protected]
Abstract: Falling and fear of falling (FOF) are significant concerns for people with Parkinson’s disease (PD). FOF can lead to activity avoidance behavior, a risk factor for increased falls and further functional decline. The significant implications of fear of falling avoidance behavior (FFAB) among PD warrant a literature review. The objective of this review was to explore existing literature on FFAB and identify what is known about this phenomenon in people with PD. This scoping review considered studies including adults 18 years and older diagnosed with PD experiencing FFAB. Using Joanna Briggs Institute methodology and the PRISMA extension for scoping reviews, we performed a scoping review searching MEDLINE, Embase, Scopus, APA PsycInfo, CINAHL, Papers First, and ProQuest Dissertations and Theses for studies examining FFAB among people with PD with no limit on publication date. A three-step search strategy was followed and data extraction was performed by two independent reviewers. A total of 9 articles met eligibility criteria. Seven studies were quantitative and two were qualitative. The results identified that FFAB has a significant impact on daily life and is associated with downstream consequences of physical and psychological decline. The symptoms and severity of PD uniquely influence FFAB. Multiple assessments were utilized, but only two measured the impact of FOF and how this fear translates into avoidance behavior. There is a paucity of literature on interventions targeting FFAB among PD. In summary, this review demonstrated that FFAB is complex, multifactorial, and significantly impacts everyday life for people with PD. Evaluation and treatment should begin in the early stages of the disease. PD adds disease-specific symptoms and progression that directly impact FFAB, possibly in a bidirectional or cyclical manner. Further research is required to explore assessment and interventions for FFAB among people with PD.
Keywords: anxiety, activity restriction, catastrophizing, rehabilitation, sedentary behavior, participation
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder with motor and non-motor symptoms which significantly impact safety and independence with daily activities.1,2 PD is the most common movement disorder and the second most common neurodegenerative disorder.3 Falling is a significant concern for persons with PD,4–6 with 60.5% of individuals reporting at least one fall each year, and approximately 39% reporting multiple falls each year.6 Recurrent falling substantially increases the likelihood of injury and long-term disability.7 Factors contributing to falls are typically characterized as either extrinsic (outside the individual, such as the environment) or intrinsic (arising from within the individual, such as impaired cognition or emotional status) in nature.8 One significant intrinsic variable associated with falling is fear of falling (FOF).9–11
FOF may develop as a direct consequence of a fall; however, it may also emerge without any history of falls.4,12 Among individuals with PD, FOF and its consequences have been found to be a more important determinant of health-related quality of life than falling and one of the strongest predictors of falls.13,14 FOF has also been found to have a more significant influence than other aspects of gait disorders on quality of life in persons with PD.15 In an attempt to decrease the fear and anxiety of falling, persons with PD may begin to avoid activities that they perceive as putting them at risk for a fall. Up to three-quarters of all adults, 65 years and older, avoid at least one daily activity due to FOF, with 15% of them reporting severe activity restrictions.16 In persons with PD, this FOF and subsequent activity avoidance behavior are also common and referred to as fear of falling avoidance behavior (FFAB).17 Further, individuals with PD have a greater FOF than similarly aged healthy adults, which may lead to greater FFAB.18
Some degree of FOF may be considered protective and beneficial, especially in those with poor balance and a high physiological risk for falls.19,20 However, when activity avoidance is excessive and not balanced with functional abilities, it may promote sedentary behavior and social isolation, eventually leading to deconditioning and functional decline.21–23 Fear, anxiety, and catastrophizing about future falling have all been shown to contribute to FOF and avoidance behavior, leading to an increased need for assistance with daily activities.24–27 FOF is generally characterized by high levels of anxiety related to walking or engaging in an activity with the fear that it might cause a fall.28–30 FOF was first recognized as an internal phenomenon or anxiety, often, but not always associated with actual falling, or the significant impact on purposeful activity and independence that may lead to deconditioning and functional loss.8 Other terms commonly associated with FOF are balance confidence (operationalizing FOF as an individual’s confidence in performing various activities without falling) or falls efficacy (operationalizing FOF as low perceived self-efficacy at avoiding falls during essential, nonhazardous activities of daily living).31–33 Due to the interrelated nature of these concepts in the literature, both terms were included in our search strategy in addition to FOF.
Activity avoidance behavior can be described as any restriction of one’s activities or foregoing participation in any daily activity.20 For the purposes of this review, avoidance behavior was considered only when it resulted from FOF. Participants actively avoiding activities may or may not have valid balance concerns and may avoid activities that do or do not pose an increased fall risk. Adopting sedentary and isolated lifestyles of activity avoidance behavior from increased fear and anxiety often leads to functional decline and even institutionalization.12,34,35 Moreover, avoidance behavior has been shown to be a strong risk factor for further falls.30 The significant implications of FFAB among people with PD warrant a literature review.
A preliminary search of PROSPERO, MEDLINE, the Cochrane Database of Systematic Reviews, and JBI Evidence Synthesis was conducted, and no current or in-progress scoping reviews or systematic reviews on the topic were identified. The objective of this scoping review was to explore the existing literature for (1) themes related to FFAB, (2) assessments used to measure FFAB, and (3) interventions used to treat this phenomenon among people with PD.
Review Questions
The following questions were used to frame this study.
1. What literature exists on FFAB in people with PD?
2. What assessments are used to measure FOF and its impact on daily activities among people with PD?
3. What interventions are being used to address FFAB among people with PD?
Inclusion Criteria
Participants
This review considered studies that included adults 18 years and older who were diagnosed with PD experiencing FFAB. Studies with mixed populations were considered for inclusion if the data could be extracted specifically for PD. PD was categorized as a physician’s clinical diagnosis based on contemporary diagnostic criteria.36
Concept
This review considered studies that explored the downstream consequences of activity avoidance or participation restriction that FOF has on individuals with PD. We aimed to examine existing evidence highlighting whether FOF, balance confidence, or falls self-efficacy translate into avoidance behavior and any unique characteristics of this behavior among the PD population. For this reason, studies were excluded if they only addressed FOF without discussing the behavioral impact of activity restriction or avoidance. We also aimed to understand what assessments accurately identified the effect, if any, of FOF on activity avoidance behavior. Additionally, we aimed to determine what, if any, interventions were being used to mitigate FFAB and what factors of FFAB (eg, psychological, physical, environmental, etc.) the identified interventions were designed to address.
Context
This review considered studies that were conducted in the context of any setting (eg, hospitals, outpatient and inpatient rehabilitation settings, home, community, etc.) or geographical location.
Types of Sources
This scoping review considered quantitative, qualitative, mixed-method studies, systematic reviews, experimental and quasi-experimental study designs, analytical observational studies, descriptive observational study designs, and qualitative designs for inclusion. In addition, text and opinion papers were also considered for inclusion in this scoping review.
Methods
This scoping review was conducted in accordance with JBI methodology for scoping reviews.37 The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) was also followed.38 This review was conducted in accordance with an a priori protocol.39
Search Strategy
The search strategy aimed to locate both published and unpublished primary studies, reviews, and text and opinion papers. This scoping review used a three-step search strategy. First, an initial limited search of MEDLINE (PubMed) and CINAHL (EBSCO) was undertaken to inform our primary search strategy. In this preliminary search, we sought to identify articles on the topic, followed by an analysis of the text words in the title and abstract and the index terms used to describe the articles. Second, our primary search using all identified keywords and index terms was undertaken across all included databases on August 1, 2020. Finally, we used the reference lists of all included articles to search for additional studies. A research librarian was consulted at each stage of the search strategy. Studies published in English from any date to the present were considered for inclusion. The complete search strategy for PubMed is presented in Appendix 1.
The databases searched included: MEDLINE (PubMed), Embase (Elsevier), Scopus (Elsevier), APA PsycINFO (EBSCO), and CINAHL (EBSCO). The search for unpublished studies and gray literature included the following: Papers First (OCLC) and ProQuest Dissertations and Theses (ProQuest). The literature search was performed on 8-1-2020.
Study Selection
Following the search, all identified citations were collated and uploaded into RefWorks (Legacy Version) (ProQuest, MI, USA). Two independent reviewers removed duplicates with double validation. Two independent reviewers screened the titles and abstracts for assessment against the inclusion criteria. Potentially relevant studies were retrieved in full, and their citation details were imported into the Joanna Briggs Institute System for the Unified Management, Assessment, and Review of Information (JBI SUMARI; JBI, Adelaide, Australia).40 The full texts of selected citations were analyzed in detail against the inclusion criteria by two independent reviewers. Studies that did not meet the inclusion criteria were excluded (Appendix 1). Disagreements between the two reviewers were resolved through discussion until a consensus was reached.
Data Extraction
Data were extracted from papers by two independent reviewers using the data extraction tool developed by the reviewers based on the standardized tool from JBI SUMARI.37 The extracted data included specific details about the population, concept, context, study methods, and key findings relevant to the review objectives (Appendix 1). Modification of the JBI data extraction tool consisted of adding the following items: details about measurements/assessments used for FFAB and details about intervention methods used to address FFAB.39
Data Analysis and Presentation
The results of the study selection and inclusion process are illustrated with a PRISMA flow diagram (Figure 1).38 The data were organized using a Microsoft Excel (Redmond, Washington, USA) worksheet. This instrument was developed in accordance with the preliminary search and review questions. Two authors independently reviewed the data. The study findings were tabulated according to the research questions and reported narratively by theme.41 The methodological quality of the included studies was not assessed as this is not customary for scoping reviews.
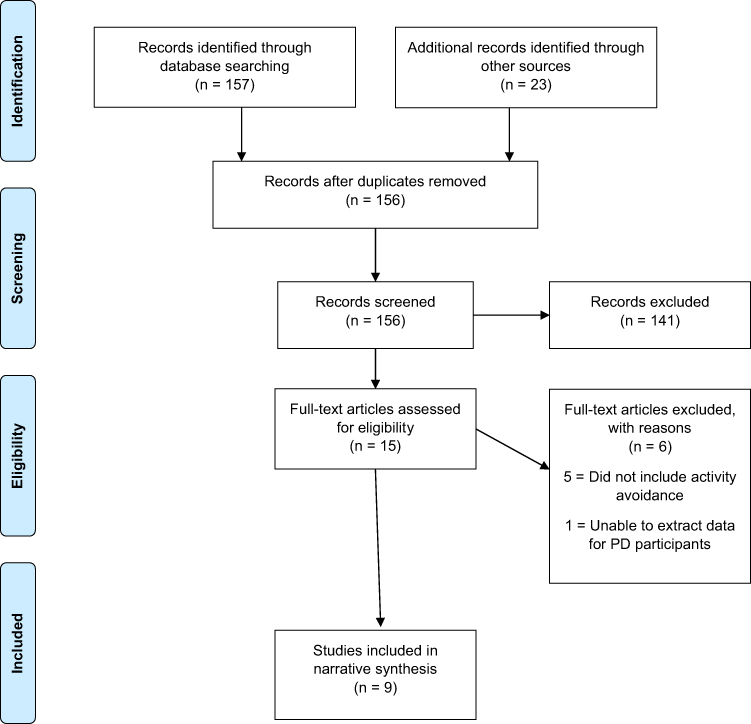 |
Figure 1 Search results, study selection, and inclusion process reported using the PRISMA Flow Diagram. Notes: Adapted from: Tricco AC, Lillie E, Zarin W et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850.38 Creative Commons. |
Results
Study Inclusion
The primary search resulted in a total of 180 citations across all databases. After duplicate removal (n = 24), 156 titles and abstracts remained based on the inclusion criteria. At this stage, 141 references were excluded because they did not meet the inclusion criteria, leaving 15 articles that were retrieved in full text for analysis (Figure 1). Six articles were excluded after the full-text review (Appendix 1), leaving nine articles for final inclusion (Figure 1).
Characteristics of Included Studies
All articles selected in this scoping review were published in peer-reviewed journals between 2010 and 2020. The included articles were both qualitative (n = 2) and quantitative (n = 7) in nature. The quantitative studies were cross-sectional (n = 5) or cohort studies (n = 2). Regarding the origin of the included articles, Sweden was the most represented country (n = 6), followed by the United States of America (n = 2) and the United Kingdom (n = 1). The main characteristics of the included articles are reported in Table 1.
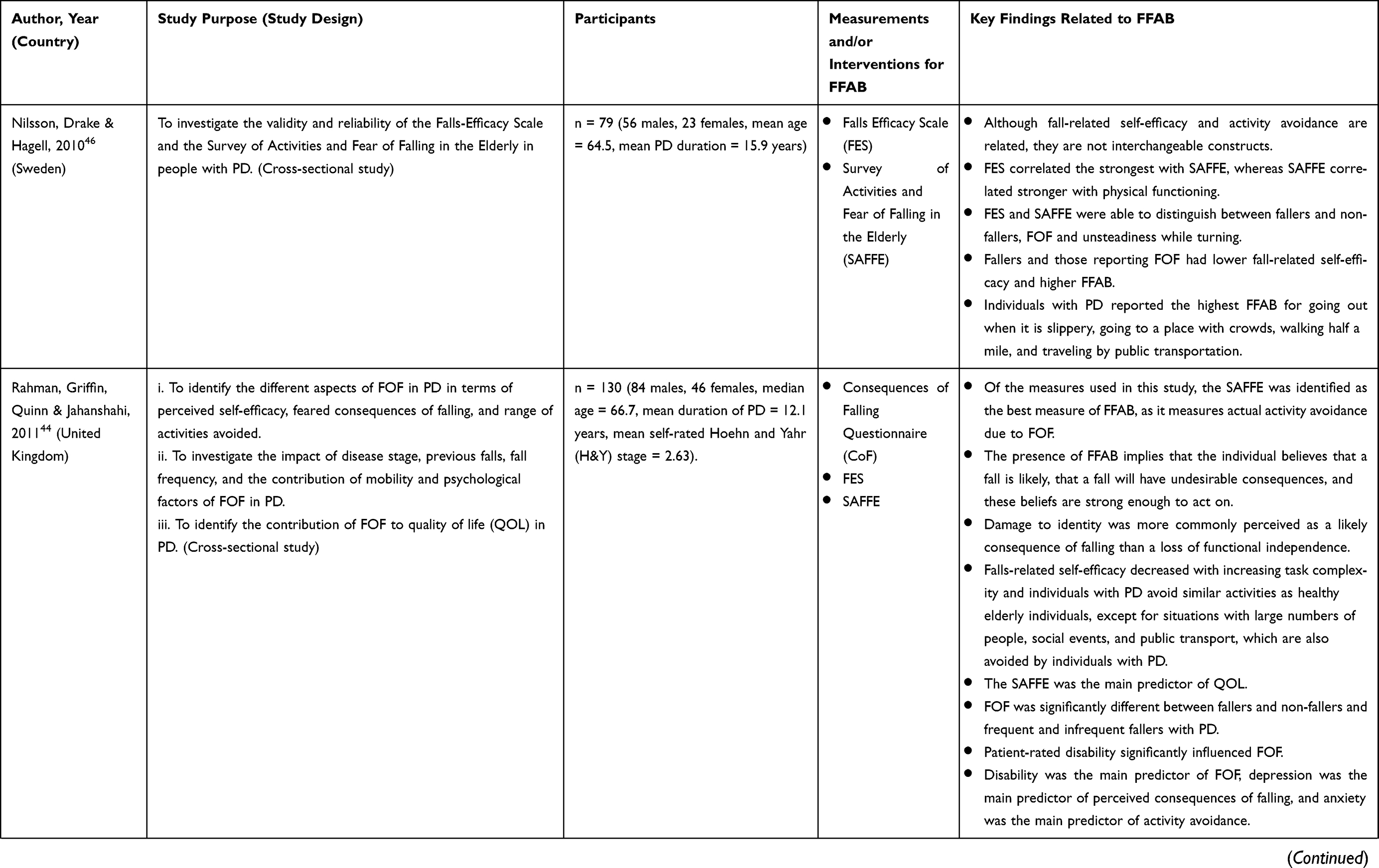 |  | 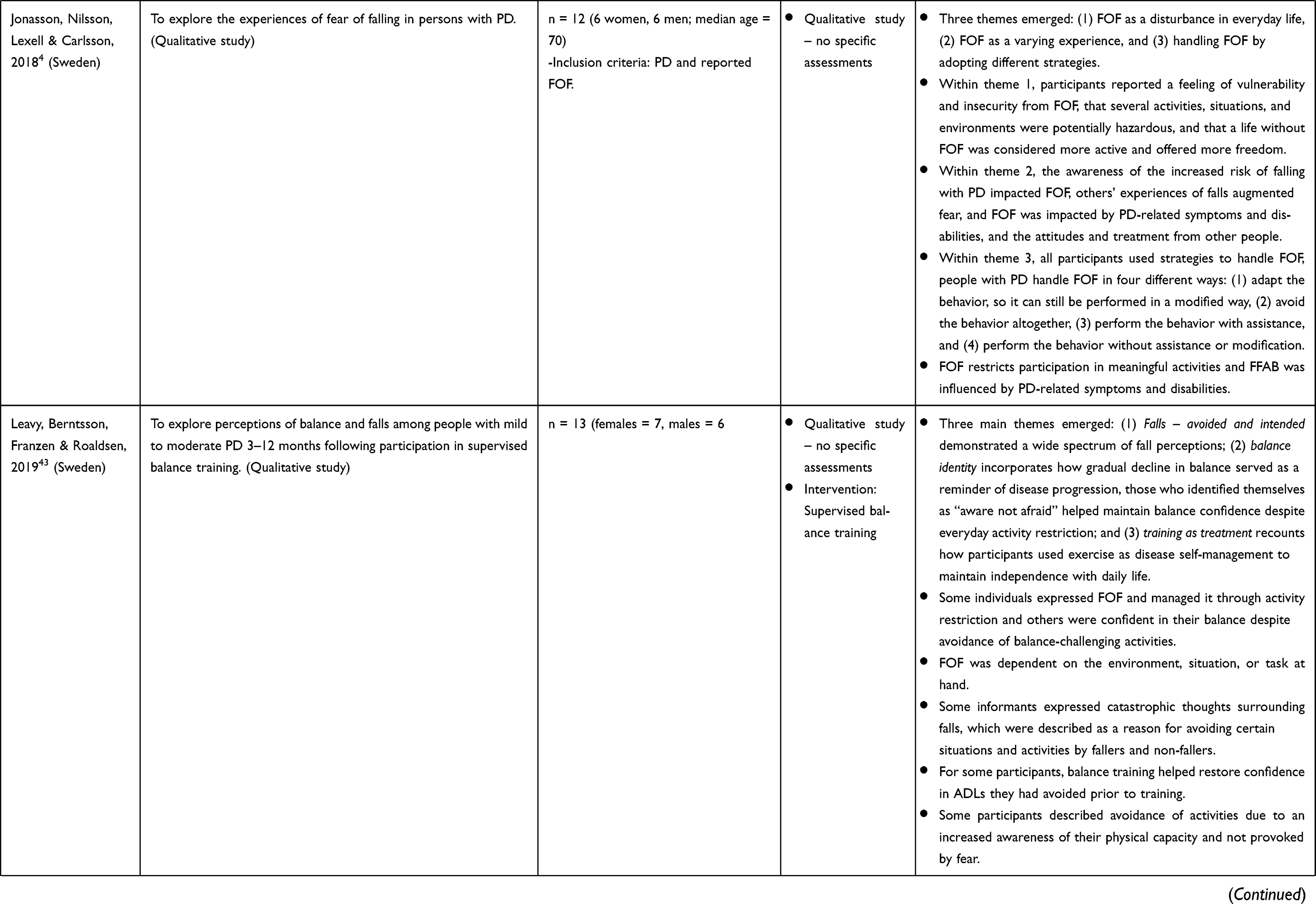 | 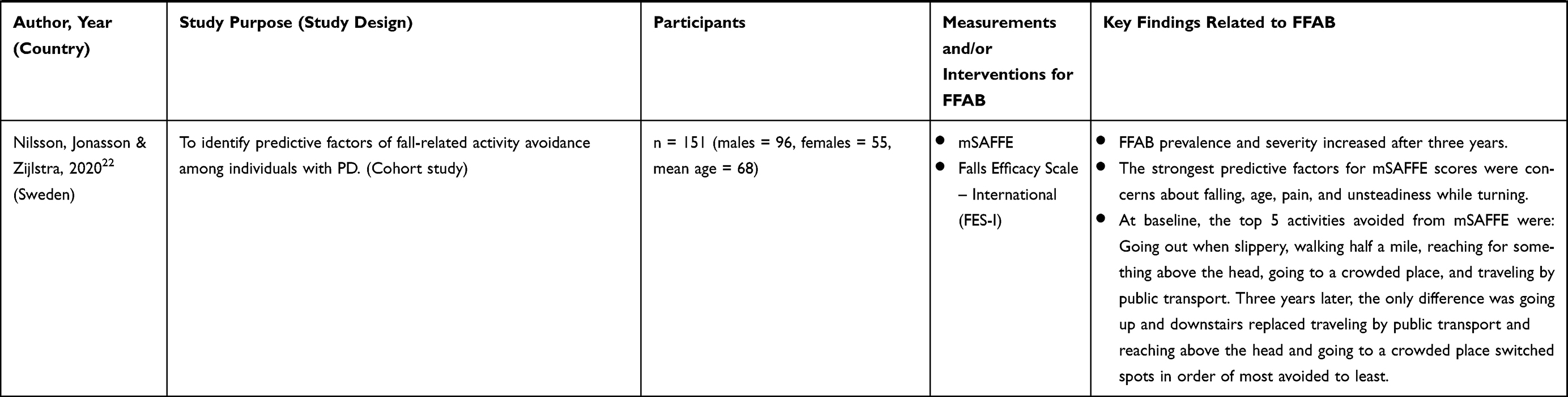 |
Table 1 Main Characteristics of Included Studies |
Review Findings
Regarding question 1 (What literature exists on FFAB in people with PD?), multiple themes emerged from the literature. The most prominent theme highlighted the significant impact of FFAB on daily life for individuals with PD, including subthemes characterizing how PD-specific symptoms may influence FFAB and the psychological influence and effect on FFAB.4,21,22,42–44 FFAB was reported as an everyday disturbance that significantly impacted the quality of life for individuals with PD.4,43 Participants reported being cautious in all mobility-related activities, having to be more attentive at all times, especially in new environments, and adapting through compensatory patterns of movement due to their FOF.4,43 Activities and environments perceived as unsafe, whether they had the mobility and capabilities to engage safely, were often avoided.4,43 FOF was associated with limitations in the performance of activities of daily living and physical inactivity.45 Reported experiences of FOF varied throughout the day because of the impact of PD-related symptoms and the attitudes and treatment of other people.4 Individuals with PD reported that PD-specific symptoms and disabilities influenced FFAB, such that FFAB was aggravated as PD progressed due to increased walking difficulties, hyperkinesia, rigidity, wearing-off episodes, freezing of gait, and impaired balance.4,42 Multiple studies found higher levels of FFAB correlated with PD disease severity or symptoms and that FFAB increased over time.4,22,42,43 The psychological burden of PD and declining functional status were evident in both qualitative studies.4,43 Greater depression was found to predict perceived consequences of falling, and greater anxiety predicted activity avoidance behavior.44 Catastrophizing was also a predictor of FFAB.21,43 FOF was reported to increase when individuals with PD were feeling low, tired, or stressed; however, they reported less or no FOF when they were in good spirits.4 Similarly, FOF increased when alone and was expressed in negative terms and associated with feelings of vulnerability.4 Furthermore, valued activities were shown to counteract the avoidance impact of FOF.4
While most studies described the negative consequences of FFAB within the impact of FFAB on daily life, a separate theme noting the potential benefits of FFAB was also discussed in three studies.21,22,43 Among the reviewed studies, activity restriction was not always reported as fear-related. Three of the included studies indicated that FFAB might be a sound strategy in hazardous circumstances when it appropriately matches the individuals’ capabilities.21,22,43 Leavy et al identified multiple potential benefits through qualitative inquiry and found that for some individuals with PD, restricted engagement in activities was an expression of increased awareness of their own abilities and involved careful mental planning.43 When discussing activity avoidance, some participants described themselves as being analytical and observant of their physical capacity instead of afraid.43 While two additional studies mentioned that FFAB might be a sound strategy, these statements were not directly related to the results of the respective studies.21,22 Lastly, assessments used to measure FFAB and intervention approaches were found throughout the included studies and will be addressed in more detail with review questions 2 and 3.
Regarding question 2 (What assessments are used to measure FOF and its impact on daily activities among people with PD?), multiple standardized assessments were identified in the included studies. For this review, FOF and FFAB assessments were categorized as either including the behavioral impact of FOF on activity participation (ie, FFAB) or not. Those that did not include the behavioral impact measured balance confidence, fall-related self-efficacy, or consequences of falling (eg, Activities-Balance Confidence Scale (ABC), Falls Efficacy Scale (FES), and Consequences of Falling Scale (CoF)).21,44–47 While these assessments have been used extensively in PD research, they do not include the behavioral impact of activity avoidance, restriction, or curtailment. Two assessments identified in this review included the behavioral impact of FOF on activity participation (The Survey of Activities and Fear of Falling in the Elderly (SAFFE) and the Fear of Falling Avoidance Behavior Questionnaire (FFABQ)).21,22,42,44,46,47 The SAFFE specifically asks participants if they do not do specific activities because they are worried about falling and if so, how worried they are about falling.20 Additionally, the SAFFE asks open-ended questions regarding other reasons that they may avoid activities besides FOF.20 The FFABQ provides the following prompt, “Due to my fear of falling, I avoid … ” and asks participants to rate their agreement (completely disagree, disagree, unsure, agree, completely agree) for 14 items describing different activities.17 Both assessments were created to uniquely assess the role of FOF in activity restriction, providing a distinct measure of FFAB.17,20 Outside of FFAB measures, every study included one or more PD-specific assessments used to characterize the severity of PD symptoms and their impact on daily life (eg, Unified Parkinson’s Disease Rating Scale (UPDRS), Hoehn & Yahr (H&Y), Schwab & England Activities of Daily Living Scale (SE-ADL), Parkinson’s Disease Questionnaire (PDQ-39), and the Parkinson’s Disease Activities of Daily Living Scale (PADLS)). While some of the PD-specific assessments were completed by licensed healthcare professionals, such as the UPDRS and the H&Y, others were completed by individuals with PD, such as the SE-ADL, PDQ-39, and PADLS. The severity of PD symptoms as measured by both objective and subjective assessments was found to be associated with FFAB.4,21,22,42–44 Lastly, one study included the Physical Activity Scale for the Elderly,48 to capture the frequency and duration of various activities.45
Regarding question 3 (What interventions are being used to address FFAB among people with PD?), we found that few studies have investigated interventions to address FFAB among people with PD. One study prospectively investigated the effects of subthalamic deep brain stimulation on FFAB among people with PD.47 Findings indicated that subthalamic deep brain stimulation increased fall-related self-efficacy and decreased FFAB and near fall rates; however, no changes in fall rates were observed.47 Another study interviewed participants about their FOF and FFAB after completing a balance training intervention.43 Using a qualitative approach, they found that participants perceived multiple benefits from the supervised balance training, including improved physical balance, increased confidence in self-managing their disease using physical activity, and decreased fear and avoidance.43 None of the other studies included in this review examined the effects of interventions on FFAB. However, several authors have suggested potential intervention approaches based on the results of their respective descriptive studies or by referencing evidence from non-PD studies addressing FFAB in the general population.4,21,22,43,44 The following areas have been suggested as potential targets to mitigate FFAB: physical and psychological functioning, motor symptoms of PD, approaches to self-management of symptoms, environmental modifications, and support for engagement in meaningful activities. Overall, there is a lack of research on interventions addressing FFAB among people with PD.
Discussion
The experiences of FOF and FFAB reported by individuals with PD are complex, contextual, multifaceted, and vary significantly in relation to activities, environments, time, and PD symptoms. This scoping review provides additional insight for researchers and clinicians working with persons with PD who experience FFAB.
Operationalization of FFAB
Conceptually, the construct of FOF varies widely and has been described as ongoing concern about falling, a loss of balance confidence, a low fall-related self-efficacy, or activity avoidance.20,31,33,46 These differences are reflected in the available assessment tools identified in this review (eg, FES, ABC scale, CoF, SAFFE, and FFABQ). Moreover, research has indicated that falls-efficacy or balance confidence and FFAB are separate constructs, and the activity avoidance behavior due to FOF is an important construct when evaluating people with PD.21,44,46 The construct of FFAB includes FOF and the downstream consequence of activity avoidance behavior.21 Activity avoidance behavior can be described as a restriction of one’s activities, and within FFAB, the avoidance behavior is viewed as a result of FOF. FFAB may or may not be due to balance concerns and may be present in individuals with or without a fall history or an increased fall risk.4,21,43 An underlying assumption of FFAB is that fear itself (ie, FOF) is not typically damaging (ie, adaptive or protective) unless it leads to excessive sedentary behavior or restriction of activities (ie, maladaptive or problematic) that are not inherently dangerous.20,49 Furthermore, individuals with PD have also described avoidance of activities due to an increased awareness of their physical capacity and not provoked by FOF.43 While further research is needed to identify the separation between adaptive and maladaptive levels of FFAB, the distinction between FOF and FFAB is necessary as evaluation and treatment may differ depending on which construct is present among individuals with PD.
Impact of FFAB on Daily Life
FFAB significantly affects performance and participation in daily activities among individuals with PD. Among the included studies, individuals with PD reported that FFAB was an everyday disturbance that greatly impacted their quality of life.4,43 The qualitative studies included in this review provided detailed insight into how FOF caused feelings of insecurity and vulnerability and influenced activity engagement by restricting individuals from fully participating in meaningful activities.4,43 Participants reported being cautious in all mobility-related activities, indicating a significant impact on activities inside and outside the home.4,43 Furthermore, FFAB caused individuals with PD to be more attentive throughout the day, especially in new environments, leading to compensatory movement patterns.4,43 This need for increased attention and compensatory movement patterns may be a significant factor for evaluation and intervention as individuals with PD have been known to have more difficulties with dual-tasking (eg, walking and cognitively attending to new and ever-changing environments).50–52 The perception of activities and environments being unsafe was more influential when it came to FFAB than the individual’s mobility capabilities, indicating a potential disparity between perceived and actual fall risk.4,43 These disparities between perceived fall risk and physiological fall risk may play an important role in identifying maladaptive versus adaptive FFAB and individuals needing intervention.19 Interestingly, people (eg, caregivers, family, friends, healthcare professionals, etc.) were identified as stressors that increased FOF based on their attitudes and treatment of the individual with PD when trying to provide assistance.4 For example, FOF increased when people tried to help but did it in the “wrong way” or when people had expectations for activity engagement that was different than the individual with PD, leading to avoidance behavior.4 This information may prove beneficial when training caregivers and healthcare professionals assisting individuals with PD. The distinct construct of activity avoidance was highlighted in the included literature as it can result in excessive sedentary behavior and functional decline, owing to the importance of evaluating FFAB, not just FOF.4,21,22,45 Relative to normative data from the general population, individuals with PD demonstrated greater fear of the consequences of falling and lower perceived self-efficacy, providing additional support for why persons with PD experience higher levels of FFAB.44
PD and Its Impact on FFAB
PD-specific symptoms uniquely influence FFAB. Individuals with PD reported that PD-specific symptoms and disabilities influenced FFAB, such that FFAB was aggravated as PD progressed due to increased walking difficulties, hyperkinesia, rigidity, wearing-off episodes, freezing of gait, and impaired balance.4,42 Due to the impact of PD-related symptoms and their fluctuations, FFAB also varied throughout the day in response to PD symptom severity.4 Participants reported that as they realized that falls are often part of the PD profile, FOF and FFAB increased as they became more afraid of the consequences of falls.4 Multiple studies found higher levels of FFAB correlated with PD disease severity or symptoms and that FFAB increased over time.4,22,42,43 However, it is noteworthy that FFAB was reported even among those who did not have a history of falls and were in early or mild disease stages, indicating a need to address FFAB early among all individuals with PD, whether they have fallen or not.42 FFAB among individuals with PD often leads to more sedentary behavior and can influence quality of life and the progression of PD negatively.4,21,22,42,43,45 The potential bidirectional or cyclical relationship of PD progression influencing FFAB and FFAB influencing PD progression and disability indicates the need for clinicians and researchers to evaluate this relationship further. Kader et al found that the most avoided activities among individuals with PD were, in order from most to least avoided: Going out when it is slippery, reaching for something above the head, walking a kilometer, going to a place with crowds, and bending down to get something.42 Freezing of gait, a common symptom of PD, was found to be associated with higher levels of FOF.44 Two of the studies we reviewed highlighted that crowded situations and activities requiring turning or maneuvering around obstacles may be avoided because they increase the likelihood of falling due to freezing of gait.22,44 While this information may prove useful for clinicians designing interventions for persons with PD, more research is needed to understand if persons with PD avoid different activities than the general population and how PD symptoms impact activity selection. Moreover, additional research is needed on how pharmacological factors, such as “on/off” periods for PD medications, may influence FFAB. Although FOF and FFAB have been explored in other populations and older adults, it is unlikely that these findings are transferable to those with PD due to disease-specific motor, non-motor, and neuropsychiatric symptoms.
Psychological Influence and Impact
The psychological influence and the impact of FOF emerged with a strong association with avoidance behavior, above physical abilities, and fall frequency.4,21,22,44,45 Psychological constructs associated with FFAB, such as depression, anxiety, and catastrophizing, were evident throughout the included studies. Depression, anxiety, and catastrophizing were reported in addition to fear and worries about falling.4,21,43,44 FOF was associated with limitations in performance of activities of daily living more strongly than fall frequency and physical activity after adjusting for physical impairments, demonstrating the influence of fear-related thoughts on falling.45 Both qualitative studies highlighted the psychological burden of PD and declining functional status.4,43 Greater depression was found to predict perceived consequences of falling, and greater anxiety predicted activity avoidance behavior, providing insight into factors possibly related to the progression of FOF to FFAB.44 Catastrophizing was also found to be a predictor of FFAB and may play a role in identifying potential avoiders with maladaptive FFAB as well as a target for treatment.21,43 FOF was reported to increase at times when individuals with PD were feeling low, tired, or stressed; however, they reported less or no FOF at times when they were in good spirits.4 Furthermore, FOF increased when alone and was expressed in negative terms and associated with feelings of vulnerability.4 These findings highlight the significant influence of mood on FOF and potential targets for intervention. In some cases, participants endeavored to lead a normal daily life as much as possible, despite FOF and FFAB, and were able to develop coping strategies.4 Their desire to engage in a particular activity was sometimes prioritized above FOF, indicating the power of valued activities.4 Valued activities were shown to counteract the avoidance impact of FOF, allowing some individuals with PD to overcome FFAB and engage in meaningful activities.4 This evidence supports the benefit of identifying meaningful activities for individuals with PD, exploring coping strategies, and providing appropriate support to engage in these activities safely despite reported FOF or FFAB. Further research is needed to determine which psychological factors and coping strategies are necessary for individuals to prioritize valued activities above the FOF.
Benefits of FFAB
Among reviewed studies, activity restriction was not always reported as fear-related. While the negative implications of FFAB have been widely discussed and may indicate an implicit bias within the current literature, there was an indication that FFAB may be a sound strategy in hazardous circumstances when it appropriately matches the individuals’ capabilities.21,22,43 For some individuals with PD, restricted engagement in activities was an expression of increased awareness of their own abilities and involved careful mental planning.43 When discussing activity avoidance, some participants described themselves as being analytical and observant of their physical capacity, as opposed to being afraid.43 Some avoidance behavior in an individual with postural stability, a common concern of individuals with PD, may be appropriate if it matches their actual balance capability.21 From a clinical perspective, these findings indicate the importance of identifying an individual’s rationale behind activity avoidance, to ascertain if it is protective and due to increased awareness and understanding of physiological risks, or if it is excessive and due to a disparity between physiological risk and perceived risk.19 The concept of an adaptive or appropriate level of FFAB, which requires further evidence to define, may serve as a protective factor for individuals with PD and decrease fall risk.21,22,43 The possible benefits of FFAB may be overlooked among this population as only three of the nine studies provided a discussion for both positive and negative consequences of FFAB. These findings demonstrate the importance of investigating FOF, FFAB, physiological fall risk, perceived fall risk, and individual reasons for avoiding certain activities in clinical assessment and ensuring that future research further examines the constructs of adaptive and maladaptive FFAB.
Assessing FFAB in PD
Multiple assessments utilized in the reviewed studies sought to quantify an individual’s balance confidence or self-efficacy related to falls. For example, the Activities-Balance Confidence (ABC) scale asks respondents to indicate their level of confidence in doing activities without losing balance (eg, “How confident are you that you will not lose your balance or become unsteady when you … Walk around the house?”).33 The FES evaluates how confident respondents are in performing particular activities without falling (eg, “Please circle the opinion closest to your own to show how concerned you are that you might fall if you did this activity”).31 The CoF scale asks respondents to rate their agreement with statements of concern regarding potential consequences of falls (eg, “I think that if I fall over … I will be embarrassed”).53 While these assessments have been used with the PD population to measure FOF, they fail to capture the downstream implications of activity avoidance behavior and participation restriction that a lack of confidence, decreased self-efficacy or concern for consequences have on performing functional tasks and engaging in daily activities.17 Moreover, research has indicated that these assessments are often used beyond the scope of their original design to measure FOF.54
In this scoping review, we identified two assessments that aim to evaluate both FOF and the behavioral consequences of fear on activity participation, adhering to the construct of FFAB. The SAFFE and the FFABQ measure FOF and how it translates into avoidance behavior among daily activities.17,20 The SAFFE asks respondents to report their current activity levels, FOF, and the impact FOF has on activity participation (for example, ”Do you currently go to the store? Do you not go to the store because you are very/somewhat/a little/not at all worried that you might fall? Are there other reasons that you do not go to the store?”).20 The FFABQ, including its new modified version, asks respondents to rate how often they avoid activities due to their FOF (eg, “Due to my fear of falling, I never/rarely/sometimes/often/always avoid walking on different surfaces?”).17 The FFABQ has also been used to dichotomize avoiders vs non-avoiders to provide a more comprehensive picture of the impact of avoidance behavior due to FOF.21 Based on the outcome of these assessments, clinicians can then utilize further ecological evaluation and intervention methods for the identified situations or activities that are avoided due to FOF.
Importantly, FOF and FFAB are associated with the disease-related characteristics of PD. In addition to measures specific to FOF and FFAB, the included studies also outlined PD-specific assessments used to assess the impact of PD symptoms. The UPDRS, H&Y, SE-ADL, PDQ-39, and PADLs were identified in the included studies. The UPDRS assesses a broad range of functioning with contributions from the investigator, patient, and caregiver and contains four parts: non-motor experiences of daily living, motor experiences of daily living, motor examination, and motor complications.55,56 The H&Y assesses how the patient and caregiver view their health and describes the progression of PD.57 The SE-ADL assesses how the patient and caregiver view their present overall activity levels.58 The PDQ-39 is a self-report questionnaire assessing PD-specific health-related quality over the last month.59 The PADLS allows patients to report the impact that PD has on daily activities subjectively.60 These PD-specific assessments are commonly used in clinical practice and research among the PD population to quantify disease severity, functioning, and health-related quality of life.61,62 Although these assessments contribute information about activity participation among individuals with PD, none of these assessments measure FFAB. The use of PD-specific assessments adds to the understanding of how PD-specific symptoms and severity influence or are influenced by FFAB and the overall impact on daily activities and quality of life.
Intervention Approaches
There is limited research on interventions to mitigate FOF or FFAB among persons with PD. Only one of the nine included studies investigated an intervention to treat FFAB.47 In that study, deep brain stimulation at the subthalamic nucleus was found to have no impact on the rate of falls after surgery; however, fewer activities were avoided owing to the risk of falling, and fall-related self-efficacy improved during complex activities, providing initial support for subthalamic deep brain stimulation as a potential intervention approach.47 While positive effects were found not only on activities but also on participation one year after surgery, the lack of control group warrants caution when interpreting the results.47 However, further research is necessary to explore the role of the subthalamic nucleus in FFAB and fall-related self-efficacy. Balance training was found to increase confidence, which helped individuals with PD engage in more activities.43 With regards to physical activity and balance training, participants reported that they wished providers discussed the importance of physical activity, alongside medications, in the early stages of PD to manage disease symptoms better actively.43 While a significant limitation was the lack of evidence on interventions, many included studies made recommendations for potential interventions based on the predictors and associated variables of FOF and FFAB identified in their respective studies. The recommended intervention approaches are summarized below. Physical interventions to address motor symptoms of PD, such as freezing of gait, balance impairments, functional mobility concerns, turning deficits, fall recovery techniques, and overall physical activity.4,22,43,45,46 Psychological interventions and coping strategies to address anxiety, catastrophizing, depression, balance confidence, concerns about falling, and executive functioning.4,21,43,44 Self-management and support interventions to address pain management, PD symptoms, comorbid disabilities, engagement in activities of daily living, adapting and compensating, caregiver training, home exercise programs, self-monitoring, planning, and problem-solving.4,21,43,45 Environmental modifications to address the use of proper durable medical equipment, training for assistive mobility devices, and safety in the home, specifically with stairs and common fall hazards.4,43,45 Supporting and encouraging engagement in meaningful activities through modifications and adaptations, problem-based strategies, exposure Therapy, sound avoidance strategies, caregiver training, and addressing socio-economic considerations such as transportation, accessibility, and in-home support.4,21,43,45 Lastly, due to the limited evidence for treating FFAB among persons with PD, generalizing evidence from non-PD studies was a common occurrence in the included literature. It is important to note that based on the literature included in this review, the above recommendations have not been tested within the PD population, and further research is needed to assess their efficacy within this population. While many of the reported findings indicate that FFAB has intrinsic and extrinsic, as well as physical and psychological dimensions, a cause-to-effect relationship cannot be determined because the majority of included studies utilized a cross-sectional research design, lacking the temporality and control needed to support evidence of causation. Although the recommendations indicate that the intrinsic, extrinsic, psychological (eg, fear itself), and physical (eg, balance and postural concerns) dimensions of FFAB should all be addressed in treatment, further research is needed to confirm these recommendations. While limited evidence exists for interventions targeting FFAB among individuals with PD, based on the unique impact of PD-related symptoms and the varied experiences of FFAB, clinicians may benefit from a battery of assessments to understand what specific impairments impact FFAB. This knowledge may allow clinicians to identify appropriate interventions and assist individuals with PD in making informed decisions regarding their particular risk of falling for any given task or environment. Lastly, given the multiple dimensions of FFAB, a multidisciplinary treatment team (eg, Occupational therapy, physical therapy, psychology, etc.) may be necessary to assess and treat FFAB effectively.49
Limitations
Despite following a structured framework and utilizing a search strategy that was designed to be comprehensive and broad, with no limit on publication date, there is a possibility that some relevant literature was not captured, thus impacting our findings. Additionally, we did not assess individual studies on their methodological quality. Although this is not a requirement for scoping reviews, as the aim is to map the extent of the literature, assessing the risk of bias may have impacted the presentation of these results.37 While the exclusion criteria were designed to ensure that our literature search provided only studies characterizing FFAB, the exclusion of studies related to FOF, balance confidence, or self-efficacy that do not report on associated activity avoidance behavior is a limitation that must be recognized. Subsequently, additional factors contributing to FOF and FFAB and the maladaptive or adaptive value of activity avoidance behavior may not be included in the reviewed studies. For example, the role of cognitive impairment was not addressed in the included studies, limiting the generalizability of the findings to individuals with PD and cognitive impairment. Lastly, there was a bias towards the negative consequences of FFAB among the included studies. Only three of the nine studies addressed the possibility that FFAB may be appropriate according to the physiological fall risk, environment, and the task being undertaken by the individual, indicating a limitation of current research and a need for further exploration into both adaptive and maladaptive types of FFAB.
Further Research
Further research is needed to describe the impact of PD-specific symptoms and severity on FFAB and how FFAB may contribute to the progression of PD. The complexity of FFAB and the misuse of FOF constructs indicate a need for further research that provides evidence for the validity and reliability of standardized assessments. While deep brain stimulation and balance training were found to have some efficacy in reducing FFAB among persons with PD, most articles made recommendations for intervention approaches based on evidence from the older adult population or hypothesized based on factors associated with FFAB. Interventions for FFAB among the general population emphasize cognitive behavioral approaches; however, further research is needed to understand the effect of cognitive behavioral approaches among individuals with PD. This review highlighted that FFAB is associated with psychological, physical, and environmental factors. Future research should consider these domains along with PD-specific symptoms when examining potential interventions to mitigate FFAB. Additionally, further research is necessary to ascertain the causal relationships, if any, between the predictors of FOF and FFAB. Furthermore, it needs to be determined whether treatment targeting these predictors can effectively mitigate FFAB and its downstream consequences. Lastly, further research is needed to identify at what level FFAB no longer provides a protective benefit and begins to contribute to unnecessary sedentary behavior, social isolation, deconditioning, and further decline.
Conclusions
This review sought to describe the available evidence for FFAB among persons with PD, with attention to assessments and intervention approaches. FFAB is complex, multifaceted, contextual, unique to the individual, and is significantly impacted by PD-specific symptoms. FOF is prevalent among the PD population, and the downstream consequences of activity restriction can lead to sedentary behavior and further disability. However, it is important to note that there are potential benefits of FFAB when it is appropriately matched with fall risk. The need for early identification and intervention for FOF and FFAB was also highlighted in the literature as FFAB was found in the early stages of PD and among those without a history of falls. The SAFFE and the FFABQ were the only assessments identified in this review that measured the construct of FFAB. Additionally, this review found limited evidence for interventions targeting FFAB among individuals with PD. Clinicians should seek to recognize the difference between FOF and FFAB and adaptive and maladaptive levels of FFAB to best select and initiate appropriate treatment. The majority of available evidence was cross-sectional and aimed at understanding associated factors and potential predictors of FFAB. Although these associated factors provide insight into FFAB, a causal relationship cannot be assumed. Clinicians should recognize that the severity and symptoms of PD influence FFAB, possibly in a bidirectional manner, and should consider psychological, physical, and environmental factors and utilize a multidisciplinary team when evaluating and treating FFAB among individuals with PD.
Acknowledgment
Jason Fetty, MLIS, AHIP, for assistance in the development of search strategies of database systems.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no disclosures or conflicts of interest in this work. No specific funding was received for this scoping review. This review was conducted in accordance with an a priori protocol published in JBI Evidence Synthesis.39 An abstract of this paper was presented at the 2021 American Congress of Rehabilitation Medicine Annual Conference as a poster presentation with interim findings. The poster’s abstract was published in “Systematic/Meta-Analytic Review Posters” in the Archives of Physical Medicine and Rehabilitation: https://doi.org/10.1016/j.apmr.2021.07.485.
References
1. Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79(4):368–376.
2. Rao G, Fisch L, Srinivasan S, et al. Does this patient have Parkinson disease? JAMA. 2003;289(3):347–353.
3. Mhyre TR, Boyd JT, Hamill RW, Maguire-Zeiss KA. Parkinson’s disease. Subcell Biochem. 2012;65:389–455.
4. Jonasson SB, Nilsson MH, Lexell J, Carlsson G. Experiences of fear of falling in persons with Parkinson’s disease - A qualitative study. BMC Geriatr. 2018;18(1):44.
5. Bryant MS, Rintala DH, Hou J-G, Protas EJ. Influence of fear of falling on gait and balance in Parkinson’s disease. Disabil Rehabil. 2014;36(9):744–748.
6. Allen NE, Schwarzel AK, Canning CG. Recurrent Falls in Parkinson’s Disease: a Systematic Review. Parkinson’s Dis. 2013;2013:906274.
7. Pickering RM, Grimbergen YAM, Rigney U, et al. A meta-analysis of six prospective studies of falling in Parkinson’s disease. Mov Disord. 2007;22(13):1892–1900.
8. Harding S, Gardner A. Fear of Falling. Aust J Adv Nurs. 2009;27(1):94–100.
9. Landers M, Oscar S, Sasaoka J, Vaughn K. Balance confidence and fear of falling avoidance behavior are most predictive of falling in older adults: prospective analysis. Phys Ther. 2015;96(4):433–442.
10. Lindholm B, Hagell P, Hansson O, Nilsson MH. Factors associated with fear of falling in people with Parkinson’s disease. BMC Neurol. 2014;14(1):19.
11. Dennison AC, Noorigian JV, Robinson KM, et al. Falling in Parkinson disease: identifying and prioritizing risk factors in recurrent fallers. Am J Phys Med Rehabil. 2007;86(8):621–632.
12. Howland J, Peterson EW, Levin WC, Fried L, Pordon D, Bak S. Fear of falling among the community-dwelling elderly. J Aging Health. 1993;5(2):229–243.
13. Lindholm B, Hagell P, Hansson O, Nilsson MH. Prediction of falls and/or near falls in people with mild Parkinson’s disease. PLoS One. 2015;10(1):e0117018.
14. Grimbergen YA, Schrag A, Mazibrada G, Borm GF, Bloem BR. Impact of falls and fear of falling on health-related quality of life in patients with Parkinson’s disease. J Parkinsons Dis. 2013;3(3):409–413.
15. Brozova H, Stochl J, Roth J, Ruzicka E. Fear of falling has greater influence than other aspects of gait disorders on quality of life in patients with Parkinson’s disease. Neuro Endocrinol Lett. 2009;30(4):453–457.
16. Deshpande N, Metter EJ, Lauretani F, Bandinelli S, Guralnik J, Ferrucci L. Activity restriction induced by fear of falling and objective and subjective measures of physical function: a prospective cohort study. J Am Geriatr Soc. 2008;56(4):615–620.
17. Landers MR, Durand C, Powell DS, Dibble LE, Young DL. Development of a scale to assess avoidance behavior due to a fear of falling: the Fear of Falling Avoidance Behavior Questionnaire. Phys Ther. 2011;91(8):1253–1265.
18. Adkin AL, Frank JS, Jog MS. Fear of falling and postural control in Parkinson’s disease. Mov Disord. 2003;18(5):496–502.
19. Delbaere K, Close JCT, Brodaty H, Sachdev P, Lord SR. Determinants of disparities between perceived and physiological risk of falling among elderly people: cohort study. BMJ. 2010;341:CD007146–c4165.
20. Lachman ME, Howland J, Tennstedt S, Jette A, Assmann S, Peterson EW. Fear of falling and activity restriction: the survey of activities and fear of falling in the elderly (SAFE). J Gerontol B Psychol Sci Soc Sci. 1998;53(1):P43–50.
21. Landers MR, Lopker M, Newman M, Gourlie R, Sorensen S, Vong R. A cross-sectional analysis of the characteristics of individuals with Parkinson disease who avoid activities and participation due to fear of falling. J Neurol Phys Ther. 2017;41(1):31–42.
22. Nilsson MH, Jonasson SB, Zijlstra GAR. Predictive factors of fall-related activity avoidance in people with Parkinson disease-A longitudinal study with a 3-year follow-up. J Neurol Phys Ther. 2020;44(3):188–194.
23. Landers MR, Jacobson KM, Matsunami NE, McCarl HE, Regis MT, Longhurst JK. A vicious cycle of fear of falling avoidance behavior in Parkinson’s disease: a path analysis. Clin Park Relat Disord. 2021;4:100089.
24. Delbaere K, Crombez G, van Haastregt JC, Vlaeyen JW. Falls and catastrophic thoughts about falls predict mobility restriction in community-dwelling older people: a structural equation modelling approach. Aging Ment Health. 2009;13(4):587–592.
25. van Haastregt JC, Zijlstra GA, van Rossum E, van Eijk JT, Kempen GI. Feelings of anxiety and symptoms of depression in community-living older persons who avoid activity for fear of falling. Am J Geriatr Psychiatry. 2008;16(3):186–193.
26. Painter JA, Allison L, Dhingra P, Daughtery J, Cogdill K, Trujillo LG. Fear of falling and its relationship with anxiety, depression, and activity engagement among community-dwelling older adults. Am J Occup Ther. 2012;66(2):169–176.
27. Deshpande N, Metter EJ, Bandinelli S, Lauretani F, Windham BG, Ferrucci L. Psychological, physical, and sensory correlates of fear of falling and consequent activity restriction in the elderly: the InCHIANTI study. Am J Phys Med Rehabil. 2008;87(5):354–362.
28. Murphy SL, Williams CS, Gill TM. Characteristics associated with fear of falling and activity restriction in community-living older persons. J Am Geriatr Soc. 2002;50(3):516–520.
29. Arfken CL, Lach HW, Birge SJ, Miller JP. The prevalence and correlates of fear of falling in elderly persons living in the community. Am J Public Health. 1994;84(4):565–570.
30. Vellas BJ, Wayne SJ, Romero LJ, Baumgartner RN, Garry PJ. Fear of falling and restriction of mobility in elderly fallers. Age Ageing. 1997;26(3):189–193.
31. Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. J Gerontol. 1990;45(6):P239–P243.
32. Yardley L, Beyer N, Hauer K, Kempen G, Piot-Ziegler C, Todd C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing. 2005;34(6):614–619.
33. Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A-Biol. 1995;50A(1):M28–M34.
34. Cumming RG, Salkeld G, Thomas M, Szonyi G. Prospective study of the impact of fear of falling on activities of daily living, SF-36 scores, and nursing home admission. J Gerontol A-Biol. 2000;55(5):M299–M305.
35. Scheffer AC, Schuurmans MJ, van Dijk N, van der Hooft T, de Rooij SE. Fear of falling: measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing. 2008;37(1):19–24.
36. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease - A clinicopathological study of 100 cases. J Neurol Neurosur PS. 1992;55(3):181–184.
37. Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: scoping Reviews. In: Aromataris E, Munn Z, editors JBI Manual for Evidence Synthesis. 2020.
38. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. ANN INTERN MED. 2018;169(7):467–473. doi:10.7326/M18-0850
39. Rider JV, Longhurst JK. Fear-of-falling activity-avoidance behavior in people with Parkinson’s disease: a scoping review protocol. JBI Evidence Synthesis. 2021;19:7.
40. Munn Z. Software to support the systematic review process: the Joanna Briggs institute system for the unified management, assessment and review of information (JBI-SUMARI). JBI Database System Rev Implement Rep. 2016;14(10):1.
41. Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis. 2020;18:10.
42. Kader M, Iwarsson S, Odin P, Nilsson MH. Fall-related activity avoidance in relation to a history of falls or near falls, fear of falling and disease severity in people with Parkinson’s disease. BMC Neurol. 2016;16:84.
43. Leavy B, Berntsson J, Franzén E, Skavberg Roaldsen K. Perceptions of balance and falls following a supervised training intervention - A qualitative study of people with Parkinson’s disease. Disabil Rehabil. 2019;41(8):934–940.
44. Rahman S, Griffin HJ, Quinn NP, Jahanshahi M. On the nature of fear of falling in Parkinson’s disease. Behav Neurol. 2011;24(3):219–228.
45. Bryant MS, Rintala DH, Hou J-G, Protas EJ. Relationship of falls and fear of falling to activity limitations and physical inactivity in Parkinson’s disease. J Aging Phys Act. 2015;23(2):187.
46. Nilsson MH, Drake A-M HP. Assessment of fall-related self-efficacy and activity avoidance in people with Parkinson’s disease. BMC Geriatr. 2010;10(1):78.
47. Nilsson MH, Rehncrona S, Jarnlo GB. Fear of falling and falls in people with Parkinson’s disease treated with deep brain stimulation in the subthalamic nuclei. Acta Neurol Scand. 2011;123(6):424–429.
48. Washburn RA, Smith KW, Jette AM, Janney CA. The physical activity scale for the elderly (PASE): development and evaluation. J Clin Epidemiol. 1993;46(2):153–162.
49. Landers MR, Nilsson MH. A theoretical framework for addressing fear of falling avoidance behavior in Parkinson’s disease. Physiother Theory Pract. 2022;2:896.
50. Giladi N, Simon ES, Springer S, Peretz C, Hausdorff JM, Yogev-Seligmann G. Dual tasking, gait rhythmicity, and Parkinson’s disease: which aspects of gait are attention demanding? Eur J Neurosci. 2005;22(5):1248–1256.
51. Kelly VE, Eusterbrock AJ, Shumway-Cook A. A review of dual-task walking deficits in people with Parkinson’s disease: motor and cognitive contributions, mechanisms, and clinical implications. Parkinsons Dis. 2012;2012:918719.
52. Rochester L, Galna B, Lord S, Burn D. The nature of dual-task interference during gait in incident Parkinson’s disease. Neuroscience. 2014;265:83–94.
53. Yardley L, Smith H. A prospective study of the relationship between feared consequences of falling and avoidance of activity in community-living older people. Gerontologist. 2002;42(1):17–23.
54. Moore DS, Ellis R. Measurement of fall-related psychological constructs among independent-living older adults: a review of the research literature. Aging Ment Health. 2008;12(6):684–699.
55. Goetz CG, Tilley BC, Shaftman SR, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–2170.
56. Schwab ZJ, England AC, Schwab RS. The Unified Parkinson’s Disease Rating Scale (UPDRS): status and Recommendations. Mov Disord. 2003;18(7):738–750.
57. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology. 1967;17(5):427–442.
58. Schwab RS, England AC. Projection technique for evaluating surgery in Parkinson’s disease. Int J Med. 1969;152–157.
59. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The Parkinson’s Disease Questionnaire (PDQ-39): development and validation of a Parkinson’s disease summary index score. Age Ageing. 1997;26(5):353–357.
60. Hobson JP, Edwards NI, Meara RJ. The Parkinson’s Disease Activities of Daily Living Scale: a new simple and brief subjective measure of disability in Parkinson’s disease. Clin Rehabil. 2001;15(3):241–246.
61. Perlmutter JS. Assessment of Parkinson disease manifestations. Curr Protoc Neurosci. 2009;1:654.
62. Marinus J, Ramaker C, van Hilten JJ, Stiggelbout AM. Health related quality of life in Parkinson’s disease: a systematic review of disease specific instruments. J Neurol Neurosurg Psychiatry. 2002;72(2):241–248.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.