Back to Journals » Journal of Pain Research » Volume 16
Fear-Avoidance Beliefs for Physical Activity Among Chronic Low Back Pain: A Multicenter Cross-Sectional Study
Authors Yihunie M, Abich Y ![]() , Demissie SF
, Demissie SF ![]() , Kassa T
, Kassa T ![]() , Ranganathan P, Janakiraman B
, Ranganathan P, Janakiraman B ![]()
Received 1 November 2022
Accepted for publication 17 January 2023
Published 26 January 2023 Volume 2023:16 Pages 233—243
DOI https://doi.org/10.2147/JPR.S388002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Mulualem Yihunie1 ,† Yohannes Abich,1 Solomon Fasika Demissie,1 Tesfa Kassa,1 Parthasarathy Ranganathan,2 Balamurugan Janakiraman3
1Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Faculty of Physiotherapy, Meenakshi Academy of Higher Education and Research (MAHER), Chennai, India; 3Department of Research and Faculty of Physiotherapy, Meenakshi Academy of Higher Education and Research (MAHER), Chennai, India
†Mulualem Yihunie passed away in May 2022
Correspondence: Yohannes Abich, Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, PO Box: 196, Gondar, Ethiopia, Email [email protected]
Background: Among different psychological predictors of outcome in low back pain (LBP) adults, the negative influence of fear-avoidance beliefs in physical activity is an area of research attention. However, there is a lack of evidence on the burden of fear avoidance about physical activity among chronic LBP adults in Ethiopia.
Objective: To describe fear-avoidance beliefs about physical activity and explore its association with socio-demographic and clinical factors among low back pain patients attending physiotherapy treatment in 3 Amhara regional comprehensive hospitals.
Methods: A multi-center cross-sectional study was conducted and adults with chronic LBP (n = 263) participated. Data were collected by face-to-face interview using the modified Fear-Avoidance Belief Questionnaire about Physical Activity (mFABQ-PA) tool. Multivariable logistic regression at a p-value < 0.05 significance level was used to identify predictors of fear-avoidance beliefs about physical activity.
Results: Among the 263 participants, 113 subjects (43%, 95% CI (36.9– 49.0)) reported a higher cut-off (> 15) mFABQ-PA. The logistic regression model demonstrated that LBP adults with a higher mFABQ-PA score were more likely to be urban residents (AOR 2.75, 95% CI (1.32, 5.88)), and ADL-related LBP (AOR 1.97 95% CI (1.18, 3.29)). The clinical-specific factor indicative of a higher cut-off score of mFABQ-PA was using analgesic medications (AOR 2.00, 95% CI (1.19, 3.37)). The model fit was 0.21 and 0.11 (R2 = Nagelkerke’s, Cox & snell respectively).
Conclusion: High fear avoidance beliefs about physical activity in adults with low back pain were found and associated with residence, work, and medication intake. These findings might urge the researchers to explore further associations and assist clinicians in choosing subgroups to use behavioral therapy and graded exposure to physical activity.
Keywords: avoidance behavior, fear-avoidance beliefs, low back pain, physical activity
Background
LBP is rated as the number one cause of years lived with disability compared with all health conditions. In the past 3 decades, Disability-adjusted Life Years (DALYs) caused by LBP have increased by 53% globally, with the greater fraction observed from low and middle-income countries.1,2 Even though most patients heal quickly, 10% of patients are at risk of acquiring chronic LBP and evidence suggests that LBP poses a considerable challenge, particularly in the chronic phase to the clinical and research agenda of LMICs.3 Hence, chronic LBP has become a major medical, social, and economic problem with frequent use of health services and long-term disability.4 Likewise, it has a negative impact on the relationships, job loss, depression, reduced quality of life, and reduced physical activity (PA) levels.5
Several factors like socio-demographic, psychological, clinical characteristics, and other risk factors are associated with the transition of Acute LBP to Chronic LBP in some individuals.6,7 Beyond biomedical factors, sometimes LBP is non-specific and cannot be attributed to recognizable pathology.8 Conversely, psychosocial factors are increasingly recognized to be frequently involved in the development of chronicity. Among the multi-facet psychosocial factors, fear-avoidance beliefs have received substantial research and clinical attention.9,10
The fear-avoidance model proposes that the experience of pain can negatively influence pain-related fear to produce an avoidance attitude leading to a decrease in physical activity, and then followed by disuse, disability, and chronification of pain.11 Studies report that the development of chronicity and disability after the incidence of LBP is strongly predicted by the presence of higher fear-avoidance beliefs,12,13 suggesting early identification of the levels of fear-avoidance beliefs which could direct appropriate management approach to reduce the risk of chronicity.
In a country with a larger proportion of economically productive age groups, where largely people work in informal employments with no or very limited job modification possibilities, low access work insurance, and a compensation system, it is worrisome that conditions like LBP are a common diagnosis and overburden to the healthcare system in Ethiopia.14,15 Based on the studies in the western liberal society, there is enough evidence to argue that the fear-avoidance model cannot be generalized to other cultures with different socio-cultural environments.16,17 Ethiopia is a low-income country, which has a diversity of cultures, low literacy rates, substandard occupational health structures, a unique social setting, and fast economic growth. The current health expenditure of Ethiopia as reported by 2019 World Bank data was estimated at 3.24% of the GDP.18,19 Western industrialized countries incur an enormous medical cost for musculoskeletal disorders and at the same time, the problem of highly prevalent chronic LBP in developing countries is not well understood.2 The fear avoidance beliefs questionnaire is an important screening tool in clinical practice for assessing the risk of disability due to fear-avoidance behavior. Conversely, there is compelling evidence that the fear-avoidance model should be utilized within the approach of biopsychosocial pain interventions in LBP.20,21 However, the magnitude of fear-avoidance beliefs among adults with chronic LBP and factors contributing to the avoidance attitude toward physical activity remains unexplored in the study area and in the country.
Due to the difference in cultural contexts, health-care systems, informal employment, lack of insurance coverage or health finance, and social structures, extrapolating the results of studies of this type from other nations to Ethiopia is challenging. Therefore, there is a definite need for context-specific data and unceasing research to understand the fear-avoidance beliefs in different musculoskeletal conditions in Ethiopia. Therefore, this study was set out to describe the fear-avoidance beliefs about physical activity (FABQ-PA) among patients with LBP attending the physiotherapy out-patient unit at the three governmental regional comprehensive hospitals in the Amhara region.
Methods and Materials
Study Design, Settings, and Population
This study was reported in compliance with the Strengthening the Reporting of Observational studies in Epidemiology22 and conducted in accordance with the declaration of Helsinki. A multi-institutional-based cross-sectional study was carried out in the three physiotherapy centers at the University of Gondar comprehensive specialized hospital (UGCSH) which is the first teaching center for physiotherapy in Ethiopia, and Felege-Hiwot comprehensive specialized Hospital (FHCSH) and Tebebe Ghion comprehensive specialized hospital (TGCSH) from 1st March to 30th June 2021. The three big tertiary referral hospitals have equipped Physiotherapy centers with trained physical therapists. The teaching hospitals serve about 10 million people in their catchment area, and provide free diagnosis, consultation, medications, and physical rehabilitation for the needy patients. The city of Gondar is situated in Northwest Ethiopia at 724 km from Addis Ababa, about 175 km from the nearby Felege-Hiwot comprehensive specialized hospital in the city of Bahir Dar. The department of Physiotherapy in the study centers provides physical rehabilitation to a wide spectrum of conditions and age groups, for both in-patients, and out-patients. The outpatient units at the UOGCSH, Felege Hiwot hospital, and Tsebe Ghion deliver physical therapy services to 150, 110, and 50 patients, respectively, per month on average. Based on the previous year’s registry, an estimated 700 low back patients are expected to visit the OPD of the 3 centers during the study period.
Study Population and Eligibility Criteria
Ethiopian citizens over 18 to 65 years, with LBP lasting more than 3 months duration attending physiotherapy out-patient unit. The subjects were informed about the study at their first appointment and subsequently screened for inclusion. Exclusion criteria were: cauda equina lesion, malignancy, infection, history of spinal surgeries, pregnancy, pain related to mensuration, and mental illness. All participants provided written informed consent before enrollment.
Sample Size and Sampling Technique
The sample size was determined based on the following assumptions using the single population proportion formula;23 since there were no similar regional studies a proportion of 50% was taken, a confidence level of 95% (Zα/2 = 1.96), precision of 5%, and 10% contingencies and non-response.
So, the derived power calculated sample for an estimated population of 700 during the study period was n = 273. A systematic random sampling method was employed to recruit subjects with chronic low back pain from the outpatient units of the three tertiary referral hospitals. To improve sample representativeness, the participants were proportionally allocated from each study area, UGCSH 132, FHCSH 97, and TGCSH 44 subjects. Based on the number of patients expected to visit each of the centers during the study period the Kth number was calculated and the first subject of the day was selected by the clinician using the lottery method.
Operational Definition
Adult participants who had experienced and self-reported pain localized between the costal margin and the inferior gluteal line or folds lasting for at least 3 months that may be associated with leg pain or numbness is defined as LBP. In addition, a flashcard with a shaded area illustrating the area of pain was included in the questionnaire. Fear-avoidance beliefs were measured by the modified version of the FABQ (mFABQ). If the mFABQ-PA subscale score is >15 out of 24 (based on the median score of the population studied)24 it is considered a high or elevated score or elevated fear avoidance belief about physical activity.
Data Collection Tool and Procedure
The data was collected using a face-to-face interview by 3 physiotherapists. The data collectors were trained for one day on the background knowledge of the study, questionnaire, and subject approach by the principal investigator. A structured face-to-face interviewer-administered questionnaire was used to collect data. The questionnaire contained three parts: socio-demographic (sex, age, marital status, education status, residence, religion, occupation), clinical factors (radiating pain, duration of low back pain, analgesic use, work-related low back pain, sport-related low back pain, regular exercise, advised resting, and sickness absence) and Fear-Avoidance Belief Questionnaire about Physical Activity (FABQ-PA) tool to measure the avoidance behavior or attitudes, and reduced physical activity in patients with LBP. The Fear-Avoidance Beliefs Questionnaire, developed by Waddell and colleagues, consists of two subscales; FABQ related to work and FABQ related to physical activity. This study used the four-item fear avoidance beliefs about physical activity subscale, score ranging from 0 to 24. Participants rated their beliefs about the activity from 0 (completely disagree) to 6 (completely agree). Higher scores represent higher levels of fear-avoidance beliefs. High FABQ-PA was defined as scores ≥15.25,26 The questionnaire was translated from the original English version to the regional language (Amharic) and checked for discrepancies and completeness.
Data Analyses
Descriptive statistics such as frequencies, percentages, means, and standard deviation were calculated and the variables associated with reporting of higher fear avoidance belief on physical activity were identified. The association between high mFABQ-PA (mFABQ-PA score ≥15) and experiencing LBP at least for 3 months was determined using the logistic regression model. Bivariate logistic regression analysis was done to identify factors associated with high fear-avoidance beliefs on physical activity (mFABQ-PA ≥15 vs, <15) with different independent variables. The independent variables included in the regression model were; age in years (categorized: 18–30, 31–40, above 40), gender, education (categorized: no formal schooling, primary, secondary, college and above), employment status (employed, unemployed, housewife, student), residence (categorized: urban, rural), chronicity of LBP (categorized: >3 months, 6 to 12 months, and >1 year), radiating pain (categorized: yes or no), regular exercise (yes, no), sick leave (yes, no), and advised to take rest (yes, no). Variables that were significant at a p-value of <0.25 in the bivariate (crude model) were entered for the final multivariate regression (adjusted) model to control the possible confounders and examine the association between different independent variables. In multivariate analysis, variables with 95% confidence intervals, p-value of <0.05 were considered statistically significant and factors that were associated with the outcome variables were included to control the potential confounders. The results of the final model were expressed in terms of adjusted odds ratio (AOR). Model fitness was checked by the Hosmer-Lemeshow goodness-of-fit test.27 Analyses were conducted using the IBM Statistical Package for Social Sciences (SPSS) software version 25.0 for Windows (IBM Corp, Armonk, NY, USA).
Results
Socio-Demographic, and Clinical Characteristics of Participants
From the 273 eligible adults who were approached for consent, 263 consented to participate in this study. The response rate was 96.33 and this is more than the power-calculated sample. The most common reason for non-response were lack of interest and time. Both male (52.5%) and female (47.5%) participants almost had equal representation and about 70% of the participants had attained secondary level and higher education. The mean age (±SD) for the participants was 39.8 (± 10.8) and 45.6% of the participants were aged above 40 years. Nearly 3/4th of the participants were employed and most of the participants (85.9%) were urban residents. Only 76 (28.9%) and 8 (3%) participants were overweight and obese, respectively. The mean BMI was almost similar for both males (24.1 ±2.8) and females (23.5 ±3.1). Almost 25% of the participants were home-makers, unemployed, and students. Among the participants, 173 (75.3%) reported being married, and 27.8%, 2.7%, and 3.8% were single, divorced, and separated or widowed, respectively (Table 1).
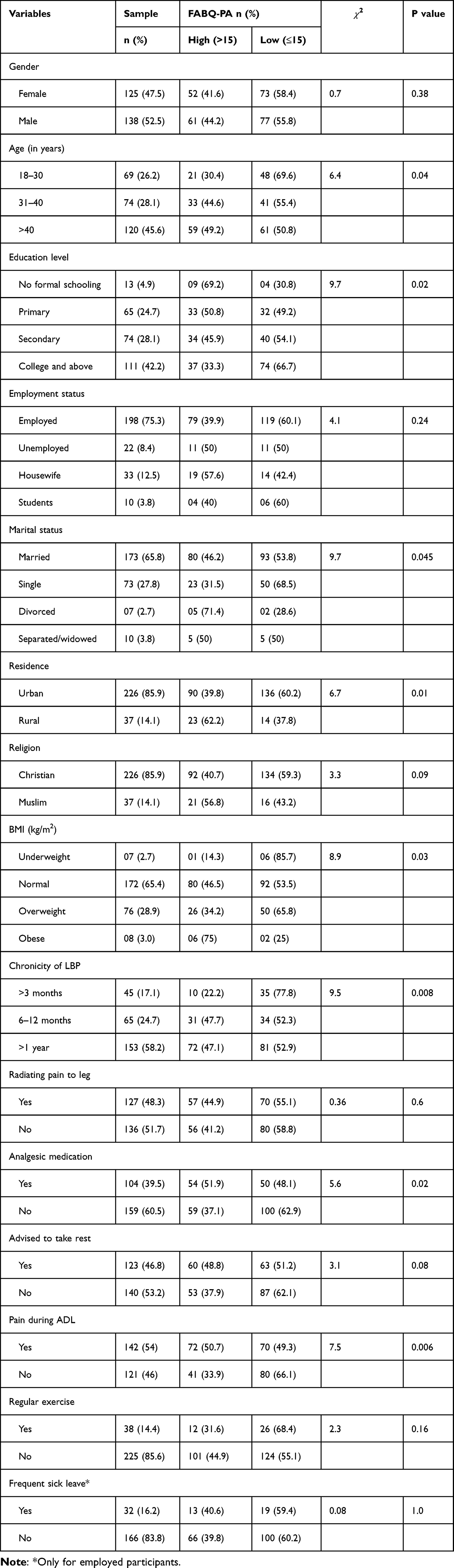 |
Table 1 Socio-Demographic, Physical Measurements, Clinical Characteristics and Distribution of FABQ-PA (>15 Score) in the Study Population (n = 263) |
The chronicity of pain symptoms reported by the participants was more than 3 months (17.1%), 6 to 12 months duration (24.7%), and majority of them (58.2%) were observed to have LBP beyond one year. The prevalence of radiating pain in the leg or sciatica was 48.3% (n = 127). Nearly, 40% of the participants were under analgesics medication during the study. More than half of the participants (54%) self-reported of pain symptom while performing activities of daily living (ADL) and only 14.4% reported having indulged in regular exercises. About 16% reported that frequent sick leave was availed due to LBP in the past 1 year.
Distribution of Elevated Scores of mFABQ-PA
Among the 263 participants, 113 subjects (43%, 95% CI (36.9–49.0)) were classified as having elevated or higher scores on mFABQ-PA based on the cut-off (>15). A statistically significant difference was observed in the proportion of elevated mFABQ-PA between the age categories (Above 40 years 49.2%, 31–40 years 28.1%, and 18–30 years 26.2%;  22 (2, n = 263) = 6.4, p < 0.05, phi = 0.15). The majority of homemakers (57.6%) were observed to have elevated mFABQ-PA followed by unemployed (50%), students (40%) versus employed (39.9%). The chronicity of the pain symptom was significantly associated with elevated mFABQ-PA (>3 months 17.1% versus 47% each for 6–12 months and >1 year;
22 (2, n = 263) = 6.4, p < 0.05, phi = 0.15). The majority of homemakers (57.6%) were observed to have elevated mFABQ-PA followed by unemployed (50%), students (40%) versus employed (39.9%). The chronicity of the pain symptom was significantly associated with elevated mFABQ-PA (>3 months 17.1% versus 47% each for 6–12 months and >1 year;  2 (2, n = 263) = 9.5, p < 0.05, phi = 0.19). The observed fear avoidance beliefs were significantly different between categories of pain during ADL (yes 50.7% versus 33.9%;
2 (2, n = 263) = 9.5, p < 0.05, phi = 0.19). The observed fear avoidance beliefs were significantly different between categories of pain during ADL (yes 50.7% versus 33.9%;  2 (1, n = 263) = 7.54, p < 0.05, phi = 0.16), advised to take rest (yes 48.8% versus no 37.9%), and intake of analgesics (yes 51.9% versus no 37.1%;
2 (1, n = 263) = 7.54, p < 0.05, phi = 0.16), advised to take rest (yes 48.8% versus no 37.9%), and intake of analgesics (yes 51.9% versus no 37.1%;  2 (1, n = 263) = 5.6, p < 0.05, phi = 0.14) Table 1.
2 (1, n = 263) = 5.6, p < 0.05, phi = 0.14) Table 1.
Regression Analysis
The results of the logistics regression analysis are displayed in Table 2. High mFABQ-PA score (≥15) was significantly associated with urban residence (OR 2.75 [1.32–5.88], p = 0.007), chronic LBP participants taking analgesics (OR 2.0 [1.19–3.37], p = 0.009) were twice more likely to report higher FABQ-PA, and participant who experienced pain during ADL (OR 1.97 [1.18–3.29], p = 0.009) are almost twice more likely to report high scores Table 2. Overall, the logistic model correctly classified 61.3% of the cases as high or low fear-avoidance (Nagelkerke’s R2 0.29).
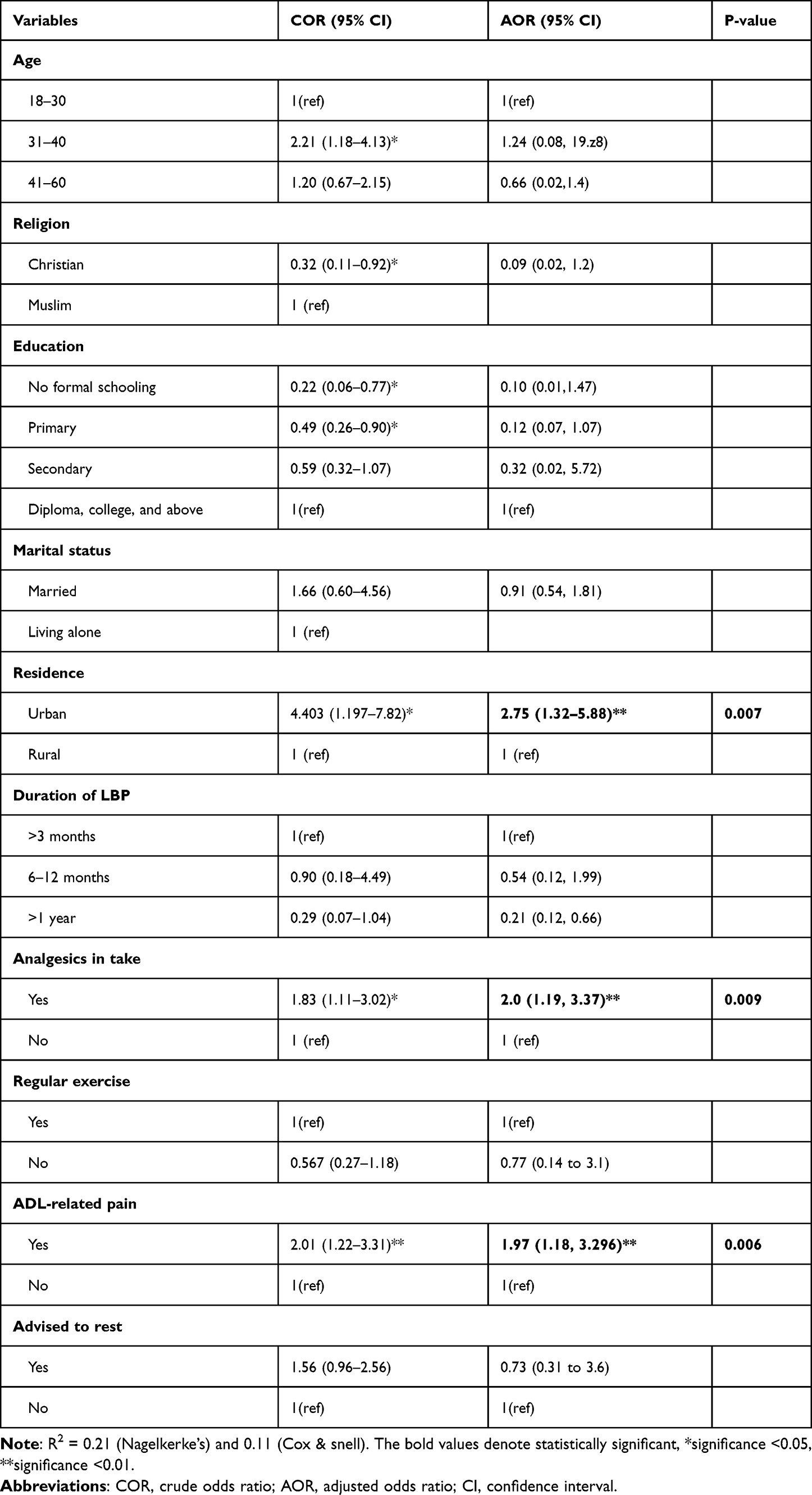 |
Table 2 Factors Associated with High Fear-Avoidance Beliefs About Physical Activities (Cut-off Score of >15) Among Adult Chronic LBP Patients (n = 263) |
Discussion
The key findings of this study were that higher fear avoidance beliefs about physical activity were significantly associated with urban residence, taking analgesics, and pain during ADL among chronic LBP subjects. Literature28–30 has identified that an elevated FAB as a critical prognostic indicator for individuals with LBP, especially after the emergence of the bio-psycho-social model of pain and recognition of the importance of psychosocial factors in LBP chronicity and disability.9 This study found that fear avoidance beliefs about physical activity were relatively common (43%) among the sample of LBP subjects at the three Amhara regional comprehensive hospitals. The findings of this study are supportive of previous research for the association and possible mediating relationship between fear-avoidance and physical activity. For instance, a cross-sectional study of 218 Australian adults with chronic LBP reported the indirect effect of FAB on activity with pain and disability.31,32 Further, fear-avoidance beliefs about physical activity can be addressed as negative bodily attention, patient with chronic pain commonly believe that their ability to control pain is limited, which can further reinforce inactivity.33 Our results are comparable to the studies done in the USA (41.8%)34 and (37.5%).35 However, studies conducted involving adults with LBP from specific occupational strata reported significantly higher fear avoidance beliefs. For example, studies conducted in the USA (69.4%)36 and Japan (61.8%),37 respectively. The USA study36 by George et al included patients from Military health-care clinic; this sample deviation from the average population of the current study could explain the difference in the finding, and the Japan study included health professionals (Nurses) with LBP from multi-hospitals. This study used only the FAB-physical activity sub scale part of the FABQ tool, and the fear avoidance beliefs about work is not considered in our study which could also be the possible reasons for a higher fear-avoidance beliefs in these studies in addition to the difference in cultural, socioeconomic, and occupational health system.
In contrast, a Norwegian study38 reported a comparatively lower FABQ-PA of 32.1% using a cut-off score of >14 for the FABQ-PA subscale. Further, the study included only 115 acute low back pain patients with chronicity of fewer than 3 months duration. Most of the participants in the Norwegian study were on sick leave, which is paid and worker compensation benefits to go with it. In addition, the higher level of education of the Norwegian research could have been the reason for the lower observation of FABs. The differences in the observed magnitude of FABQ-PA score between countries and populations can also be explained by the present view and approach on LBP in the countries, educational status, cultural context, employer and family supports, personal insurance, and worker’s compensation. For instance, in this study, we observed that about half (46.8%) of the participants reported of being advised to take rest. But, the approach to LBP in the developed countries is more in the direction of confronting the pain than on the rest.36,39 Further, the occupational health system and negative psychological characteristics like somatic hypervigilance, financial insecurity, and misinterpretation of people who are fearful and ambiguous about physical sensations as threatening or painful may have increased the likelihood of higher FABQ-PA scores.40
In our study, factors such as residency, analgesic use, and ADL-related low back pain were significantly associated with fear-avoidance beliefs about physical activities among LBP patients. Participants who lived in rural areas were 64% times less likely to report higher fear-avoidance beliefs about physical activity than urban residents. The possible reason might be rural residents are unique in culture, lifestyle, values, pain tolerance, behaviors relating to the clinical course of LBP and health care. Another possible reason could be that features of the physical environment directly impact participation in physical activity.41
Analgesic users are significantly associated with high fear-avoidance beliefs about physical activity in our study. The risk of reporting higher fear-avoidance beliefs about physical activity among the chronic LBP patients who were under analgesics medication was twice higher than their counterpart. Though, with the cross-sectional design, it is difficult to explain if pain medication came after the high fear avoidance beliefs manifest or the higher fear avoidance beliefs were led by pain medication. The association of analgesic medication with higher fear avoidance beliefs is supported by the study done in Norwegian adults with acute LBP.39 The possible explanation could be predicting pain based on internal or external stimuli is a fundamental and highly adaptable self-protective process. This reaction is created through associative and instrumental learning processes, and pain-related fear is an important component of it. Pain-related fear can become maladaptive in chronic pain, leading to avoidance strategies and symptom persistence.42 Stress may affect pain processing, impair perceptual discrimination, favor overgeneralization, and may lead to the re-activation of maladaptive pain-related anxiety. Stress is likely to occur in the everyday life of chronic pain sufferers.43 More importantly, the Norwegian study included patients with acute LBP where there is high possibility of larger proportion being under medications particularly during episode of acute pain.
On the other hand, the risk of reporting higher fear-avoidance beliefs was 1.97 times greater in ADL-related LBP patients than in work-related LBP patients. The possible explanation might be people who are engaged in work are physically active and have a lower risk for the development of chronic LBP. It is also well-recognized that being active is an effective clinical treatment to reduce pain and improve function in a variety of pain conditions.44
Strengths and Limitations
To the best of our knowledge, this study is one of the few studies that determined the fear-avoidance beliefs among LBP in Ethiopia, and the findings are important in the cultural context considering the increasing burden of LBP in the country. The findings of this study with a sufficiently powered analysis to detect the significance of relationship between variable are most likely to have good generalizability for clinical practice. However, there are some limitations that are to be counted while interpreting the results. The study design did not allow the analysis of the ROC curve and thereby the possibilities to determine a cut-off for the sample and the cross-sectional nature of this study is limited to observed prevalence, distribution, and inter-relations of variables within the population studied, thus the temporal causality between the variables studied cannot be established. Finally, this was conducted on participants presenting to the hospital for healthcare, which might have exaggerated our values and the use of self-reported questionnaires did not allow us to exclude the possible recall bias. Future studies shall consider community-based design and cohort design to obtain a detailed association of factors with fear-avoidance belief within the community.
Conclusion
In this study, 43% had a higher score on FABQ-PA (>15). The fear-avoidance belief was higher among the urban residents, patients under analgesic medications, and those who reported pain during the performance of ADL. These findings might urge the researchers to prospectively explore the causal relationship within the fear-avoidance model and assist clinicians in choosing subgroups to use behavioral therapy and graded exposure to physical activity.
Abbreviations
BMI, body mass index; AOR, adjusted odds ratio; CI, confidence interval; CLBP, chronic low back pain; COR, crude odds ratio; ETB, Ethiopian birr; mFABQ-PA, Modified fear-avoidance belief for physical activity; LBP, low back pain; OR, odds ratio; SD, standard deviation; PA, physical activity; SPSS, Statistical package for social sciences.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy issues. However, data will be available upon reasonable request from the corresponding author.
Ethical Approval and Consent to Participate
This study was approved by the Institutional Review Committee of the College of Medicine and Health Sciences, the University of Gondar, Ethiopia (Ref. No. 453/2021). Official letters from the administrators of the University of Gondar and Bahir Dar specialized hospitals were obtained before contacting study participants. The purposes and the importance of the study have been clarified to each participant. They were also told that until they gave their formal approval, they were free to refuse to participate or answer any of the questions. To ensure data confidentiality at all levels of the study, the names of participants and any personal identifiers were not included.
Acknowledgment
The authors would like to thank the University of Gondar and Bahir Dar specialized hospital coordinators and staff members. Our thanks also go to the data collectors and the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, data, analysis and interpretation. MY, YA, SFD and TK trained the data collectors, supervised data collection, and approved completed questionnaires. All the authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was fully funded by the University of Gondar, scientific research grant number (19/453/13 CMHS, UOG) after defending the study proposal. The funder has no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen S, Chen M, Wu X., et al. Global, regional and national burden of low back pain 1990–2019: a systematic analysis of the Global Burden of Disease study 2019. J Orthopaedic Translation. 2022;32:49–58. doi:10.1016/j.jot.2021.07.005
2. Lee H, Hübscher M, Moseley GL, et al. How does pain lead to disability? A systematic review and meta-analysis of mediation studies in people with back and neck pain. Pain. 2015;156:988–997. doi:10.1097/j.pain.0000000000000146
3. Freburger JK, Holmes GM, Agans RP, et al. The rising prevalence of chronic low back pain. Arch Intern Med. 2009;169:251–258. doi:10.1001/archinternmed.2008.543
4. Coudeyre E, Tubach F, Rannou F, et al. Fear-avoidance beliefs about back pain in patients with acute LBP. Clin J Pain. 2007;23:720–725. doi:10.1097/AJP.0b013e31814da407
5. Nelson N, Churilla JR. Physical activity, fear avoidance, and chronic non-specific pain: a narrative review. J Bodyw Mov Ther. 2015;19:494–499. doi:10.1016/j.jbmt.2015.02.001
6. Nieminen LK, Pyysalo LM, Kankaanpää MJ. Prognostic factors for pain chronicity in low back pain: a systematic review. Pain Rep. 2021;6. doi:10.1097/PR9.0000000000000919
7. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391:2356–2367. doi:10.1016/S0140-6736(18)30480-X
8. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482–491. doi:10.1016/S0140-6736(11)60610-7
9. Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine. 2002;27:E109–20. doi:10.1097/00007632-200203010-00017
10. Ramond A, Bouton C, Richard I, et al. Psychosocial risk factors for chronic low back pain in primary care—a systematic review. Fam Pract. 2011;28:12–21. doi:10.1093/fampra/cmq072
11. Vlaeyen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85:317–332. doi:10.1016/S0304-3959(99)00242-0
12. Beneciuk JM, Bishop MD, Fritz JM, et al. The STarT back screening tool and individual psychological measures: evaluation of prognostic capabilities for low back pain clinical outcomes in outpatient physical therapy settings. Phys Ther. 2013;93:321–333. doi:10.2522/ptj.20120207
13. Karstens S, Lang S, Saunders B. Patients’ views on the implementation potential of a stratified treatment approach for low back pain in Germany: a qualitative study. Health Services Insights. 2020;13:1178632920977894. doi:10.1177/1178632920977894
14. Cedraschi C, Nordin M, Haldeman S, et al. The Global Spine Care Initiative: a narrative review of psychological and social issues in back pain in low-and middle-income communities. Eur Spine J. 2018;27:828–837. doi:10.1007/s00586-017-5434-7
15. Sikiru L, Shmaila H, Wang’ombe JK, Griffiths JK. Prevalence and risk factors of low back pain among nurses in Africa: Nigerian and Ethiopian specialized hospitals survey study. East Afr J Public Health. 2009;6(1):6. doi:10.4314/eajph.v6i1.45734
16. Chapman JR, Norvell DC, Hermsmeyer JT, et al. Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine. 2011;36:S54–68. doi:10.1097/BRS.0b013e31822ef74d
17. Terho H, Haapea M, Paananen M, Korniloff K, Häkkinen A, Karppinen J. Translation and validation of the Finnish version of the Fear-Avoidance Beliefs Questionnaire (FABQ). Scandinavian J Pain. 2016;10:113–118. doi:10.1016/j.sjpain.2015.09.003
18. Global Health Expenditure Database [Internet]. Available from: https://apps.who.int/nha/database/ViewData/Indicators/en.
19. Current health expenditure (% of GDP) - Ethiopia | data [Internet]. Available from: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=ET.
20. Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7:261–271. doi:10.1016/j.jpain.2005.10.011
21. Kovacs F, Abraira V, Cano A, et al. Fear avoidance beliefs do not influence disability and quality of life in Spanish elderly subjects with low back pain. Spine. 2007;32:2133–2138. doi:10.1097/BRS.0b013e318145a74b
22. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147:573–577. doi:10.7326/0003-4819-147-8-200710160-00010
23. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35:121–126. doi:10.4103/0253-7176.116232
24. Williamson E. Fear avoidance beliefs questionnaire (FABQ). Aust J Physiother. 2006;52:149. doi:10.1016/S0004-9514(06)70052-6
25. Aasdahl L, Marchand GH, Gismervik SØ, Myhre K, Fimland MS, Røe C. The fear avoidance beliefs questionnaire (FABQ) does it really measure fear beliefs? Spine. LWW. 2020;45:134–140.
26. Waddell G, Newton M, Henderson I, Somerville D, Main CJ, Fear-Avoidance Beliefs A. Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain. 1993;52:157–168. doi:10.1016/0304-3959(93)90127-B
27. Evans S, Li L. A comparison of goodness of fit tests for the logistic GEE model. Stat Med. 2005;24:1245–1261. doi:10.1002/sim.2023
28. Boersma K, Linton SJ. Screening to identify patients at risk: profiles of psychological risk factors for early intervention. Clin J Pain. 2005;21:38–43. doi:10.1097/00002508-200501000-00005
29. Buer N, Linton SJ. Fear-avoidance beliefs and catastrophizing: occurrence and risk factor in back pain and ADL in the general population. Pain. 2002;99:485–491. doi:10.1016/S0304-3959(02)00265-8
30. George SZ. Fear: a factor to consider in musculoskeletal rehabilitation. J Orthopaedic Sports Phys Therapy. 2006;36:264–266. doi:10.2519/jospt.2006.0106
31. Tan B-KB, Smith A, O’Sullivan P, Chen G, Burnett A. Low back pain beliefs and their relationships with low back pain-related disability in nurses working in mainland China and in Australia. J Cult Divers. 2015;22:71.
32. Feyer A-M, Herbison P, Williamson AM, et al. The role of physical and psychological factors in occupational low back pain: a prospective cohort study. Occup Environ Med. 2000;57:116–120. doi:10.1136/oem.57.2.116
33. Geertzen J, Van Wilgen C, Schrier E, Dijkstra P. Chronic pain in rehabilitation medicine. Disabil Rehabil. 2006;28:363–367. doi:10.1080/09638280500287437
34. George SZ, Stryker SE. Fear-avoidance beliefs and clinical outcomes for patients seeking outpatient physical therapy for musculoskeletal pain conditions. J Orthopaedic Sports Phys Therapy. 2011;41:249–259. doi:10.2519/jospt.2011.3488
35. Calley DQ, Jackson S, Collins H, George SZ. Identifying patient fear-avoidance beliefs by physical therapists managing patients with low back pain. J Orthopaedic Sports Phys Therapy. 2010;40:774–783. doi:10.2519/jospt.2010.3381
36. George SZ, Fritz JM, Childs JD. Investigation of elevated fear-avoidance beliefs for patients with low back pain: a secondary analysis involving patients enrolled in physical therapy clinical trials. J Orthopaedic Sports Phys Therapy. 2008;38:50–58. doi:10.2519/jospt.2008.2647
37. Fujii T, Oka H, Takano K, et al. Association between high fear-avoidance beliefs about physical activity and chronic disabling low back pain in nurses in Japan. BMC Musculoskelet Disord. 2019;20:1–10. doi:10.1186/s12891-019-2965-6
38. Grotle M, Vøllestad NK, Veierød MB, Brox JI. Fear-avoidance beliefs and distress in relation to disability in acute and chronic low back pain. Pain. 2004;112:343–352. doi:10.1016/j.pain.2004.09.020
39. Svensen AR, Ringvold ML, Bergland A. Acute Low Back Pain–a Cross Sectional Study: Fear-Avoidance Beliefs and Associated Characteristics. Norsk Fysioterapeutforbund (NFF); 2011.
40. Meyer K, Tschopp A, Sprott H, Mannion AF. Association between catastrophizing and self-rated pain and disability in patients with chronic low back pain. J Rehabilitation Med. 2009;41:620–625. doi:10.2340/16501977-0395
41. Hoehner CM, Ramirez LKB, Elliott MB, Handy SL, Brownson RC. Perceived and objective environmental measures and physical activity among urban adults. Am J Prev Med. 2005;28:105–116. doi:10.1016/j.amepre.2004.10.023
42. Nees F, Becker S. Psychological processes in chronic pain: influences of reward and fear learning as key mechanisms–behavioral evidence, neural circuits, and maladaptive changes. Neuroscience. 2018;387:72–84. doi:10.1016/j.neuroscience.2017.08.051
43. Elsenbruch S, Wolf OT. Could stress contribute to pain-related fear in chronic pain? Frontiers in behavioral neuroscience. Front Media SA. 2015;9:340.
44. Shraim MA, Massé-Alarie H, Hall LM, Hodges PW. Systematic review and synthesis of mechanism-based classification systems for pain experienced in the musculoskeletal system. Clin J Pain. 2020;36:793–812. doi:10.1097/AJP.0000000000000860
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.