Back to Journals » Clinical Ophthalmology » Volume 16
Faricimab for Treatment-Resistant Diabetic Macular Edema
Received 7 July 2022
Accepted for publication 10 August 2022
Published 24 August 2022 Volume 2022:16 Pages 2797—2801
DOI https://doi.org/10.2147/OPTH.S381503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ryan B Rush,1– 3 Sloan W Rush1,2
1Panhandle Eye Group, Amarillo, TX, USA; 2Department of Surgery, Texas Tech University Health Science Center, Amarillo, TX, USA; 3Southwest Retina Specialists, Amarillo, TX, USA
Correspondence: Ryan B Rush, Southwest Retina Specialists, 7411 Wallace Blvd, Amarillo, TX, 79106, USA, Tel +1 806 351-1870, Email [email protected]
Purpose: To assess the short-term outcomes in treatment-resistant diabetic macular edema (DME) patients changed from intravitreal aflibercept (IVA) to intravitreal faricimab (IVF).
Methods: A retrospective review was undertaken on DME subjects receiving IVA therapy at a single private practice. Patients were separated into study and control cohorts. Both study and control patients had received more than or equal to six IVA injections during the preceding 12 months, more than or equal to four IVA injections during the preceding 6 months, had a central macular thickness (CMT) on optical coherence tomography (OCT) of ≥ 300 μm, and had retinal fluid on OCT before cohort assignment. Study patients were switched to IVF and underwent three injections within 4 months, whereas control patients stayed on IVA during the same period and received three injections within 4 months.
Results: There were 51 patients analyzed. There were 37.5% (9/24) in the study group and 3.7% (1/27) in the control group who achieved a CMT of less than 300 μm without retinal fluid on OCT at the end of the 4-month study (p=0.001). There were 41.7% (10/24) in the study group and 11.1% (3/27) in the control group who had gained two or more lines of visual acuity at the end of the 4-month study (p=0.01).
Conclusion: For a significant minority, IVF can improve the short-term visual and anatomic outcomes in treatment-resistant DME patients formerly managed with IVA. Longer follow-up is needed to determine if such improvements can be preserved.
Keywords: faricimab, treatment-resistant, diabetic macular edema, recalcitrance
Introduction
Intravitreal injections targeting VEGF have revolutionized treatment of diabetic macular edema (DME).1,2 However, there are a number of limitations to anti-VEGF treatment, including the constraint of repetitive injections and insufficient response in a subset of patients. Despite monthly anti-VEGF treatments over 36 months, approximately 20% of patients with DME may have persistent retinal fluid on optical coherence tomography (OCT) with worse visual acuity than patients with fluid-free maculae.3 As a result, new delivery systems and therapies have been developed to target other corresponding mediators implicated in angiogenesis and vascular leakage.
Faricimab (Roche/Genentech, Basel, Switzerland) was developed as a bispecific antibody to bind VEGFA and Ang2. Based on the outcomes of two multi-center phase III clinical trials, YOSEMITE and RHINE,4 faricimab was granted approval by the US Food and Drug Administration for the management of DME in January 2022. In these key studies,4 patients who underwent intravitreal faricimab (IVF) treatment at an interval of 8 weeks or according to a personalized treatment interval had noninferior best-corrected visual acuity (BCVA) outcomes compared to patients who underwent intravitreal aflibercept (IVA; Eylea/Regeneron, NY, USA) treatment at a fixed interval of 8 weeks. Although the outcomes in the personalized treatment cohort of YOSEMITE and RHINE imply that IVF may be more effective than IVA in regard to permitting longer intervals of treatment when using an OCT-guided protocol, a noteworthy limitation in these studies rests in the design, which did not allocate patients in the IVA cohort to a personalized treatment protocol. Therefore, one may only speculate how a personalized treatment protocol with IVA might have compared to the personalized treatment protocol administered to subjects receiving IVF. In this case-controlled study, the authors assessed the short-term effects of switching patients with DME from IVA to IVF when recalcitrance was encountered in a real-world setting using a personalized OCT-guided treatment protocol.
Methods
This study was conducted as a retrospective, case-controlled series of patients with DME treated from February to May 2022 at a single private practice specializing in vitreoretinal diseases in Amarillo, TX. It was authorized by the Panhandle Eye Group Institutional Review Board (IORG0009239; IRB00011013-07), and all components of research followed the tenets of the Declaration of Helsinki. Informed consent from study participants was waived because this was a retrospective study and all patient data were protected and kept confidential by the researchers. Research subjects were allocated into study and control groups according to whether or not the patient had been switched from IVA to IVF during the selected study period.
Inclusion criteria common to both study and control cohorts were as follows: 1) the patient had actively been receiving IVA injections for DME leading up to the beginning of the study period in February 2022, 2) an OCT-guided treat-and-extend management protocol was being employed, 3) the patient had received more than or equal to six IVA injections during the preceding 12 months (370 days), 4) the patient had received more than or equal to four IVA injections during the preceding 6 months (180 days), and 5) the patient was documented to have a central macular thickness (CMT) on OCT of ≥300 µm with identifiable DME prior to the study initiation period.
Patients allocated to the study group were changed from IVA to IVF between February and March 2022 and received three IVF injections within 4 months (120 days) following the switch with subsequent follow-up during the research interval. Patients allocated to the control group stayed on IVA between February and May 2022 and received three IVA treatments within 4 months (120 days) with subsequent follow-up during the research period.
Exclusion criteria common to both study and control cohorts were as follows: 1) the baseline Snellen BCVA of the patient was worse than 20/200, 2) an ocular treatment other than anti-VEGF therapy was performed within 6 months (180 days) of the initiation of the study interval (eg, cataract surgery, vitrectomy, retinal laser), and/or 3) a condition apart from DME was considered to be responsible for a decrease in Snellen visual acuity to the tune of more than or equal to two lines (eg, glaucoma, cataract, stroke-related vision loss).
An OCT-guided treat-and-extend management protocol was used during this study, similar in design to what has been widely adopted in the real world.5,6 In short, patients underwent monthly (28–34 days) anti-VEGF treatments until all identifiable retinal edema had resolved on OCT. Once the retinal edema had resolved, patients were extended out to 1–2 week increments until recurrence of the retinal edema was observed, and the interval of treatment was then adjusted to maintain a macula that was fluid-free. For the purpose of this study, patients were considered treatment-resistant whenever a fluid-free macula on OCT could not be accomplished in spite of more than or equal to six anti-VEGF treatments over a 12-month period. Whenever both eyes of study and control patients met the inclusion/exclusion criteria, a coin toss–simulating program (simple randomization) selected which eye would be included. The baseline examination for the purpose of this study was the evaluation directly preceding the study’s start (February 2022). OCT examination employed the Heidelberg Spectralis system (Heidelberg Engineering, Heidelberg, Germany). OCT scans at baseline and final follow-up were assessed for the presence of retinal edema by two masked fellowship-trained retina specialists. Whenever discordance between the two assessing specialists arose, a third masked specialist made the prevailing determination.
Outcomes and Statistical Analysis
The primary outcome of this study was the percentage of subjects who attained a CMT <300 µm without identifiable retinal edema on OCT at the end of the 4-month study. The secondary outcome of this study was the percentage of subjects who had improved by two or more lines of BCVA at the end of the 4-month study. Snellen visual acuity was converted into logMAR for analysis of the data. Likelihood ratios and one-way analyses of variance were used to assess for statistical significance at the α<0.05 level. The JMP 11 (SAS Institute, USA) statistical program performed the analysis of the data.
Results
There were a total of 51 patients included in the analysis, of which 24 were in the study group and 27 in the control group. The research population’s baseline characteristics and demographics are shown in Table 1. No significant differences between cohorts at baseline were found. The agreement rate between the two masked OCT reviewers was 94.1% (48/51).
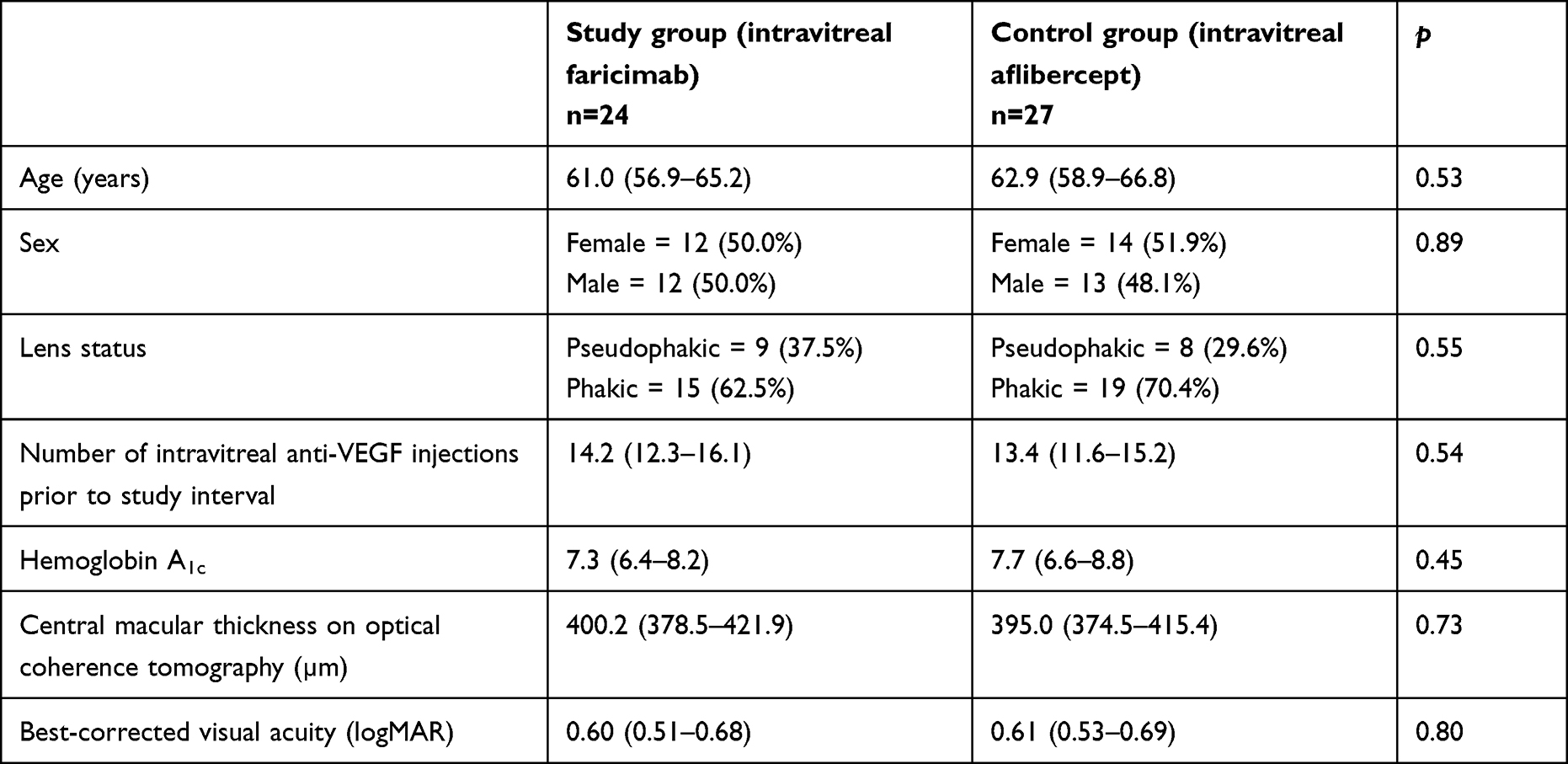 |
Table 1 Faricimab for treatment-resistant diabetic macular edema. baseline demographics, and characteristics of the study population (means with 95% CIs) |
There were 37.5% (9/24) patients in the study group and 3.7% (1/27) patients in the control group who had attained a CMT of less than 300 µm without identifiable retinal edema on OCT at the end of the 4-month study (p=0.001). CMT on OCT had changed from 400.2 (377.5–422.9) µm at baseline to 340.3 (317.6–363.0) µm at the end of the 4-month study in the study group (p<0.001). CMT on OCT had changed from 395.0 (373.2–416.7) µm at baseline to 374.7 (353.0–396.5) µm at the end of the 4-month study in the control group (p=0.19).
There were 41.7% (10/24) subjects in the study group and 11.1% subjects (3/27) in the control group who had improved by two or more lines of BCVA at the end of the 4-month study (p=0.01). Visual acuity had changed from 0.60 (0.50–0.69) logMAR (Snellen 20/80) at baseline to 0.50 (0.40–0.59) logMAR (Snellen 20/63) at the end of the 4-month study in the study group (p=0.12). Visual acuity had changed from 0.61 (0.53–0.69) logMAR (Snellen 20/81) at baseline to 0.59 (0.51–0.68) logMAR (Snellen 20/78) at the end of the 4-month study in the control group (p=0.75). Figure 1 demonstrates an example of a study subject who was successfully switched from IVA to IVF.
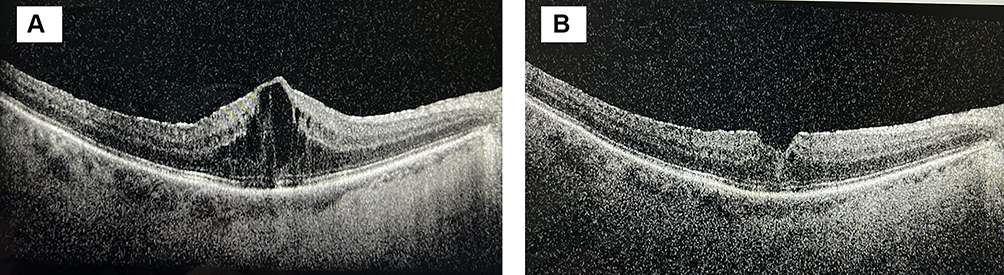 |
Figure 1 A 66-yearold male with severe nonproliferative diabetic retinopathy and persistent macular edema following ten intravitreal aflibercept injections over 12 months. (A) The baseline optical coherence tomography image demonstrates substantial diabetic macular edema. The central macular thickness was 570 µm and the Snellen visual acuity was 20/70. (B) The optical coherence tomography image of the same patient after being switched to faricimab and undergoing three faricimab treatments. The central macular thickness had decreased to 359 µm and the Snellen visual acuity improved to 20/40. |
Discussion
The benefits of switching from bevacizumab or ranibizumab to aflibercept in recalcitrant cases of DME has been well established.7–9 However, the authors were unable to identify any studies in the literature reporting treatment alternatives when recalcitrance to aflibercept was encountered in this patient population. The incidence of patients with DME experiencing persistent retinal fluid on OCT despite monthly injections with aflibercept was 32% at 24 weeks, and 44% of those same subjects remaining on aflibercept therapy had persistent retinal fluid on OCT at 2 years (24 months).10 To our knowledge, this study is the first to report outcomes in patients with DME switched from aflibercept to faricimab secondary to treatment resistance to aflibercept. Both visual and anatomic outcomes were noted in a clinically significant minority when switched to faricimab from aflibercept. This suggests that faricimab may offer the potential for fewer intravitreal injections without compromising visual outcomes in this difficult-to-treat subgroup of DME subjects resistant to aflibercept therapy when a treat-and-extend protocol is employed. Since the negative effect that chronic fluid on OCT has on long-term visual outcomes in subjects with DME has been documented,11 faricimab’s ability to resolve DME in a significant minority of subjects recalcitrant to aflibercept therapy is indeed a welcome addition to the retina specialist’s armamentarium of anti-VEGF treatment options.
Intravitreal faricimab has hypothetical advantages over aflibercept, including a greater affinity for VEGFA as well as neutralizing Ang2, which research has implicated in the pathophysiology of angiogenesis.12–14 However, as mentioned in the Introduction, the pivotal trials YOSEMITE and RHINE did not allow subjects randomized to aflibercept to receive a personalized treatment plan, regardless of the subject’s clinical course.4 The authors would have favored an identical treatment protocol among subjects receiving IVA and IVF in order to better evaluate comparative effectiveness between treatments. In this study, the authors made it a point to provide a robust comparison by case controlling subjects included. Since no significant differences were found between study and control cohorts at baseline and both cohorts underwent the same treat-and-extend protocol, the authors believe that our study population received an adequate comparison. However, our study consisted only of treatment-resistant DME subjects and thus may not be applicable to a general population of subjects consisting of treatment-naïve, treatment-responsive, and treatment-resistant DME.
Our study’s strengths include its case-controlled design with well-matched subjects allocated to study and control cohorts at baseline, the reasonably large sample analyzed considering the novelty of faricimab, and its setting in the real world using a characteristic treat-and-extend protocol familiar to most specialists, thereby allowing for sensible application by other specialists treating a recalcitrant DME population. Our study’s weaknesses comprise its retrospective design, the use of logMAR visual acuity rather than ETDRS letter scoring, and its rather short duration. Greater follow-up is required to establish long-term outcomes once treatments are extended using the treat-and-extend protocol employed in this study.
To conclude, switching DME patients resistant to treatment with aflibercept to faricimab may lead to better visual and anatomic outcomes in a statistically significant minority of patients, thereby potentially allowing longer periods between treatments when a real-world treat-and-extend regimen is employed. Further investigations into this topic are warranted in order to confirm our study’s results, especially with a greater follow-up interval.
Abbreviations
OCT, optical coherence tomography; BCVA, best-corrected visual acuity; DME, diabetic macular edema; VEGF, vascular endothelial growth factor; CMT, central macular thickness.
Data Sharing
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics and Consent
The study was approved by the Panhandle Eye Group Institutional Review Board (IORG0009239; IRB00011013-07) in accordance with the ethical standards laid down in the Declaration of Helsinki. Informed consent from study participants was waived because this was a retrospective study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval to the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wells JA, Glassman AR, Ayala AR, et al.; Diabetic Retinopathy Clinical Research Network. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N Engl J Med. 2015;372(13):1193–1203.
2. Elman MJ, Aiello LP, Beck RW, et al.; Diabetic Retinopathy Clinical Research Network. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology. 2010;117(6):1064–1077 e35. doi:10.1016/j.ophtha.2010.02.031
3. Bressler SB, Ayala AR, Bressler NM, et al. Persistent macular thickening after ranibizumab treatment for diabetic macular edema with vision impairment. JAMA Ophthalmol. 2016;134(3):278–285. doi:10.1001/jamaophthalmol.2015.5346
4. Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, Phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/S0140-6736(22)00018-6
5. Sarohia GS, Nanji K, Khan M, et al. Treat-and-extend versus alternate dosing strategies with anti-vascular endothelial growth factor agents to treat center involving diabetic macular edema: a systematic review and meta-analysis of 2346 eyes. Surv Ophthalmol. 2022;(22). doi:10.1016/j.survophthal.2022.04.003
6. Chujo S, Sugimoto M, Sasaki T, et al. Comparison of 2-year outcomes between intravitreal ranibizumab and intravitreal aflibercept for diabetic macular edema with “treat-and-extend” regimen-its usefulness and problems. J Clin Med. 2020;9(9):2848. doi:10.3390/jcm9092848
7. Laiginhas R, Silva MI, Rosas V, et al. Aflibercept in diabetic macular edema refractory to previous bevacizumab: outcomes and predictors of success. Graefes Arch Clin Exp Ophthalmol. 2018;256(1):83–89. doi:10.1007/s00417-017-3836-1
8. Bahrami B, Hong T, Schlub TE, Chang AA. Aflibercept for persistent diabetic macular edema: forty-eight-week outcomes. Retina. 2019;39(1):61–68. doi:10.1097/IAE.0000000000002253
9. Ashraf M, Souka AA, ElKayal H. Short-term effects of early switching to ranibizumab or aflibercept in diabetic macular edema cases with non-response to bevacizumab. Ophthalmic Surg Lasers Imaging Retina. 2017;48:230–236. doi:10.3928/23258160-20170301-06
10. Bressler NM, Beaulieu WT, Glassman AR, et al. Persistent macular thickening following intravitreous aflibercept, bevacizumab, or ranibizumab for central-involved diabetic macular edema with vision impairment: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2018;136(3):257–269. doi:10.1001/jamaophthalmol.2017.6565
11. Sadda SR, Campbell J, Dugel PU, et al. Relationship between duration and extent of oedema and visual acuity outcome with ranibizumab in diabetic macular oedema: a post hoc analysis of Protocol I data. Eye. 2020;34(3):480–490. doi:10.1038/s41433-019-0522-z
12. Hussain RM, Neiweem AE, Kansara V, et al. Tie-2/Angiopoietin pathway modulation as a therapeutic strategy for retinal disease. Expert Opin Investig Drugs. 2019;28(10):861–869. doi:10.1080/13543784.2019.1667333
13. Ferro Desideri L, Traverso CE, Nicolò M. The emerging role of the Angiopoietin-Tie pathway as therapeutic target for treating retinal diseases. Expert Opin Ther Targets. 2022;26(2):145–154. doi:10.1080/14728222.2022.2036121
14. Sahni J, Dugel PU, Patel SS, et al. Safety and efficacy of different doses and regimens of faricimab vs ranibizumab in neovascular age-related macular degeneration: the AVENUE phase 2 randomized clinical trial. JAMA Ophthalmol. 2020;138(9):955–963. doi:10.1001/jamaophthalmol.2020.2685
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intravitreal Faricimab for Aflibercept-Resistant Neovascular Age-Related Macular Degeneration
Rush RB, Rush SW
Clinical Ophthalmology 2022, 16:4041-4046
Published Date: 9 December 2022
One-Year Outcomes of Faricimab Treatment for Aflibercept-Resistant Neovascular Age-Related Macular Degeneration
Rush RB
Clinical Ophthalmology 2023, 17:2201-2208
Published Date: 1 August 2023
One Year Results of Faricimab for Aflibercept-Resistant Diabetic Macular Edema
Rush RB
Clinical Ophthalmology 2023, 17:2397-2403
Published Date: 16 August 2023
Clinical Evaluation of Faricimab in Real-World Diabetic Macular Edema in India- A Multicenter Observational Study
Chakraborty D, Das S, Maiti A, Sinha TK, Das A, Sheth J, Boral SK, Mondal S, Nandi K
Clinical Ophthalmology 2025, 19:269-277
Published Date: 25 January 2025
Faricimab Outcomes in Chorioretinal Disorders: Indian Real-World Analysis (FOCUS Study)
Agrawal V, Gupta A, Agrawal V, Sheth JU
Clinical Ophthalmology 2025, 19:1855-1862
Published Date: 12 June 2025