")
Back to Journals » Cancer Management and Research » Volume 15
Family Wellbeing and Sexual Health of Patients Receiving Treatment for Prostate Cancer
Authors Rio CJ , Goto T, Hsiao CP , Ross ALR , Saligan LN
Received 24 May 2023
Accepted for publication 9 September 2023
Published 31 October 2023 Volume 2023:15 Pages 1197—1206
DOI https://doi.org/10.2147/CMAR.S421951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Carielle Joy Rio,1 Taichi Goto,1 Chao-Pin Hsiao,2 Alexander LR Ross,1 Leorey N Saligan2
1National Institute of Nursing Research, Division of Intramural Research, National Institutes of Health, Bethesda, MD, USA; 2Case Western Reserve University School of Nursing, Cleveland, OH, USA
Correspondence: Leorey N Saligan, National Institute of Nursing Research, Division of Intramural Research, National Institutes of Health, Building 3, Room 5E14, 3 Center Drive, Bethesda, MD, 20892, USA, Tel/Fax +1 301-451-1685, Email [email protected]
Purpose: Prostate cancer and its treatment may affect patients’ sexual function and social wellbeing. This study investigated the relationship between social/family wellbeing and sexual health in patients with prostate cancer. Additionally, the moderating effect of clinical characteristics on this relationship was also explored.
Patients and Methods: This is a descriptive correlational study using baseline data of a longitudinal study enrolling 137 patients with prostate cancer. Sexual Function (SF) and Sexual Function Distress (SFD) data were collected using the Symptom Index questionnaire. Demographic data were obtained during study intake and clinical data were obtained from chart review. Bivariate correlation determined the correlations among continuous demographic/clinical data, social/family wellbeing, and sexual health. Moderated regression analysis determined the moderating effects of clinical characteristics on the relationship of social/family wellbeing and sexual health.
Results: Moderate positive correlation was found between social/family wellbeing and SF, whereas a weak negative correlation was noted between social/family wellbeing and SFD. Depression was significantly correlated with social/family wellbeing and SFD. Both sexual health domains were significantly correlated with Gleason score. A significant difference was noted in the social/family wellbeing and both SF and SFD in participants receiving androgen deprivation therapy (ADT) compared to those not receiving ADT. Concomitant ADT use was the only clinical characteristic found to be a significant moderator of the relationship between social/family wellbeing and SFD, but none of the clinical characteristics was found to have a moderating effect on the relationship of social/family wellbeing and SF. Among patients who were not receiving ADT, high social/family wellbeing was associated with low SFD. Patients who were receiving ADT reported slightly higher SFD despite having higher social/family wellbeing.
Conclusion: Ensuring sexual health in patients with prostate cancer requires a comprehensive approach to address factors contributing to sexual health such as side effects of treatment and family wellbeing.
Keywords: sexual function, sexual function distress, family health, male reproductive health
Corrigendum for this paper has been published.
A Letter to the Editor has been published for this article.
Introduction
In 2020, there was an estimated 1.41 million new cases of prostate cancer worldwide.1 Prostate cancer is a global concern and is the second most common cancer in males.2 The five-year relative survival rate of prostate cancer is 98%. Although the prevalence of prostate cancer is high, the risk of dying from prostate cancer is low. Advances in treatment and the growing trend of early diagnosis contributed to the decline in prostate cancer mortality.3 An estimated 3.1 million Americans alive today have been diagnosed with prostate cancer at some point in their lives.4 The high survival rate of prostate cancer means that there is a high number of long-term prostate cancer survivors who may be suffering from the side effects of prostate cancer and its treatment.
Patients undergoing treatment for prostate cancer experience a wide range of physical and psychological side effects. Physiologically, prostate cancer treatment may affect hormone levels, cardiovascular function, hemodynamics, and nerve function.5 Other side effects such as fatigue, changes in bladder and bowel functions, and change in physical appearance may affect a person’s self-esteem, body image, sexual function, and subsequently sexual health and overall wellbeing.6 Patients and doctors tend to focus more on ensuring survival and perceive sexual health as a low-priority aspect of cancer care.7 However, earlier studies found that sexual health affects a person’s quality of life and general health.8,9 Thus, sexual health as an underexplored aspect of prostate cancer treatment may have negative consequences on patients’ overall wellbeing.6
This paper focuses on a common concern, sexual dysfunction, reported by individuals treated for prostate cancer.10 Physical needs often receive more attention in prostate cancer care, but sexual care remains a significant unmet need in patients undergoing prostate cancer treatment.11 Earlier studies show that a high percentage (70–90%) of men with prostate cancer experience sexual dysfunction, regardless of their treatment status. Erectile dysfunction was identified as the most common cause of sexual dysfunction.5,12 In addition, problems with orgasm and overall sexual function were also identified as factors that contribute to changes in sexual health among patients with prostate cancer.12
Although it is well established that prostate cancer treatment causes sexual function and sexual health changes, there is limited literature that discusses the influence of sociodemographic variables and social wellbeing on sexual health. In understanding sexual health in patients with prostate cancer, it is important to note that social factors include a wider sphere outside of the patient and his partner. Demands from family responsibilities, home dynamics, and work responsibilities may contribute to sexual health problems.13 An individual’s perception that there are significant others who are available to offer support affects their emotional and mental health.14 A study found that in patients with prostate cancer, better social support was associated with lesser depressive symptoms.14 In another study, it was found that positive social relationships is linked with lower perceived stress and better quality of life in patients with prostate cancer.15
This study was conducted to primarily investigate whether social/family wellbeing is significantly correlated with sexual health, specifically focusing on two domains: sexual function and sexual function distress, in patients with prostate cancer. In addition, the study explored whether there is a significant difference in social/family wellbeing and the two sexual health domains when participants are grouped according to age, marital status, race, and highest level of education completed. This study also determined whether clinical characteristics such as use of androgen deprivation therapy (ADT), clinical stage of cancer, Gleason score, body mass index (BMI), and depression were correlated with social/family wellbeing, perceived sexual function and perceived sexual function distress. Clinical characteristics were additionally assessed to determine potential moderating effects on the relationship between family/social wellbeing and the two domains of sexual health.
Materials and Methods
Participants
This is a descriptive correlational study from the baseline data of a longitudinal study approved by the Institutional Review Board of the National Institutes of Health (NIH, NCT00852111). This study enrolled 137 patients aged 18 years or older, diagnosed with non-metastatic prostate cancer with or without prior prostatectomy, and scheduled to receive external beam radiation therapy (EBRT). Baseline data were obtained from the participants before they started EBRT. Participant recruitment was done from April 2009 to January 2019 at the NIH Magnuson Clinical Research Center. Signed written informed consent was obtained prior to study participation. This study excluded patients with prostate cancer who have progressive diseases causing significant fatigue, psychiatric disease within the past five years, uncorrected hypothyroidism, anemia, or a second malignancy. Individuals who used sedatives, steroids, or non-steroidal anti-inflammatory agents were also excluded. All stages of this study were conducted in accordance with the ethical standards stipulated in the Declaration of Helsinki.
Variables and Instruments
Demographic data (ie, age, marital status, race, education) were obtained during study intake and clinical data (ie, ADT use, clinical stage of cancer, Gleason score, body mass index) were obtained from chart review. Social/family wellbeing was assessed using the Social/Family Wellbeing subscale of the Functional Assessment of Cancer Therapy-Prostate (FACT-P) questionnaire. The Social/Family Wellbeing subscale consists of 7 items which can be scored from 0 to 4. The total Social/Family Wellbeing subscale score ranges from 0 to 28. Higher scores indicate better social/family wellbeing.
The Symptom Index (SI) questionnaire has two subscales that measure sexual health: Sexual Function (SF) subscale and Sexual Function Distress (SFD) subscale. The SF subscale contains five questions that asked the participants to rank the severity of their symptoms on a five-point Likert scale. Negative statements were reverse coded, and a total SF subscale score was obtained. Higher total SF subscale scores indicate better sexual functioning. The items in the SF subscale questionnaire were based on the participants’ perception of their sexual function during the past week or the past four weeks. Only 47 of the 137 participants indicated that they had sexual activity in the past week or the past four weeks. This limitation is discussed in the discussion section of this paper. The SFD subscale of the SI questionnaire also utilized a five-point Likert scale where participants indicate “how big a problem” the different sexual health symptoms are to them. A higher SFD score indicates higher distress or a stronger perception of the symptom as a burden. Depression scores were measured using the 24-item version of the Hamilton Depression Rating Scale (HAM-D). Total scores may range between 0–54, with higher scores indicating more severe depressive symptoms. Using this scale, depressive symptoms are categorized based on published guidelines: 0–7 indicate no depression, 8–16 indicate mild depression, and a score of ≥ 17 indicate moderate to severe depression.16
Statistical Analysis
Frequency distribution was calculated to describe the sociodemographic and clinical characteristics of the sample. Correlations between sexual health, age and social/family wellbeing were determined using bivariate correlation (Spearman’s rho). Mann–Whitney U-test was used to determine whether there is a significant difference in social/family wellbeing, sexual function distress and sexual function when age (≤ 65 versus > 65), marital status (married versus non-married), race (Whites versus non-Whites), and highest education level (completed at least college versus completed less than college) were controlled.
Bivariate correlation using Spearman’s rho was calculated to determine correlations between continuous clinical data such as body mass index (BMI), Gleason score and depression score on social/family wellbeing, sexual function distress and sexual function scores. Moderated regression analysis was conducted to determine the moderating effects of clinical characteristics (ADT, clinical stage, BMI, Gleason score and depression) on the relationship between social/family wellbeing and the two sexual health domains. In conducting the moderated regression analyses, the absence of interaction between the predictor variable and the moderator variable was not assumed or avoided, as it does not imply a causal sequence between the predictor and outcome variables.17–20 Threshold α values were 0.05 for all statistical tests. Statistical analyses were performed with SPSS statistics software version 23 (IBM SPSS, Purchase, NY). The Hayes Process Macro extension in SPSS was used to perform moderated regression analysis.
Results
Sociodemographic Characteristics, Social/Family Wellbeing, and Sexual Function Distress
Table 1 presents the distribution of the participants according to their sociodemographic characteristics, social/family wellbeing, and sexual function distress scores. Bivariate correlation analysis showed that age was not significantly correlated with social/family wellbeing and perceived sexual function distress. Using the Mann–Whitney U-test, a significant difference in social/family wellbeing scores was found between participants who are married versus those who are not married (p=0.011). Married participants had higher median social wellbeing scores compared to those who are not married. No significant difference was noted in social/family wellbeing when age, race, and level of education were controlled. Table 1 further shows that there is no significant difference in sexual function distress scores across all sociodemographic groups. These results suggest that sexual function distress is not better or worse when groups were compared according to their sociodemographic characteristics. However, married participants displayed better social/family wellbeing compared to those who were not married.
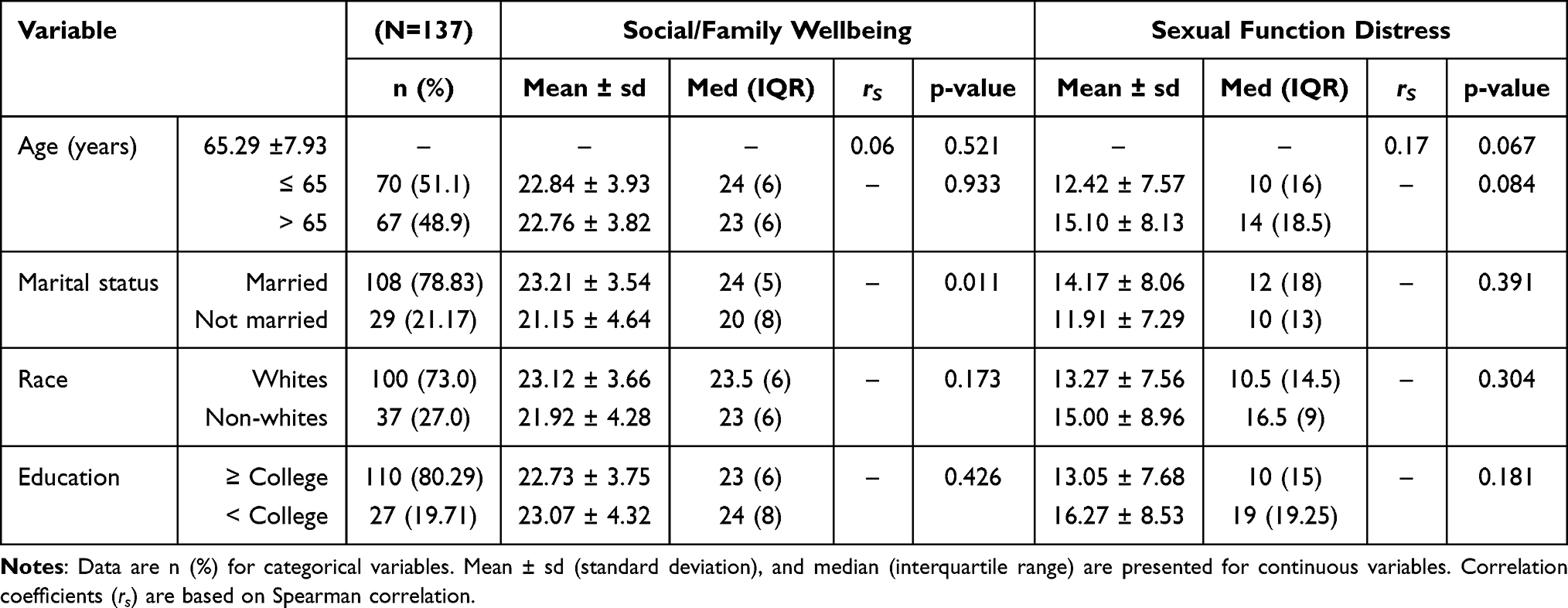 |
Table 1 Sociodemographic Characteristics, Social/Family Wellbeing, and Sexual Function Distress |
Clinical Characteristics, Social/Family Wellbeing, and Sexual Function Distress
The direct correlation between clinical characteristics, social/family wellbeing and perceived sexual function distress were also explored (see Table 2). A weak negative correlation (rs= −0.23, p= 0.009) was noted between depression and social/family wellbeing. This suggests that participants with lower depression scores tend to have higher social/family wellbeing scores. The results further show that participants with higher Gleason and depression scores were likely to have higher sexual function distress scores as shown by the positive correlation between Gleason (rs= 0.29, p= 0.002) and depression scores (rs= 0.25, p= 0.009) and sexual function distress scores. When clinical characteristics were controlled, a significant difference in the social/family wellbeing (p= 0.028) and sexual function distress scores (p= <0.001) were noted between participants who were receiving ADT and those who did not. Participants who are not treated with ADT have higher median social/family wellbeing scores (24.5 vs 23) and lower median sexual function distress scores compared to those on ADT (7 vs 18.5).
 |
Table 2 Clinical Characteristics, Social/Family Wellbeing, and Sexual Function Distress |
Sub-Group Analysis of Sexual Function
All participants were asked to recall their sexual health-related symptom experience in the past week or within the past four weeks. The majority of the participants (66%) indicated that they have not had sexual intercourse within the past week or within the past four weeks. Only 47 of the 137 participants provided information regarding their perceived sexual function. Sub-analysis for this group found no significant correlation between age and social/family wellbeing and sexual function scores. No significant difference was noted in both social/family wellbeing and sexual function scores when age, marital status, and race were controlled (see Table 3).
 |
Table 3 Sociodemographic Characteristics, Social Wellbeing, and Sexual Function |
Table 4 presents the results for tests of correlation and difference in social/family wellbeing and sexual function when clinical characteristics were controlled. A significant difference (p= <0.001) was noted in sexual function scores when participants were grouped based on ADT use (taking ADT versus not taking ADT). Participants who were not taking ADT had higher median sexual function scores compared to those on ADT (19 vs 11). Analysis of the direct correlations between clinical characteristics with social/family wellbeing and sexual function revealed that only Gleason score was significantly correlated with sexual function (rS = −0.44, p = 0.002), suggesting that perceived sexual function tended to decrease with an increase in Gleason score. Table 4 further shows that participants with lower Gleason scores (≤ 7) rated their sexual function higher compared to those with higher Gleason scores (> 7).
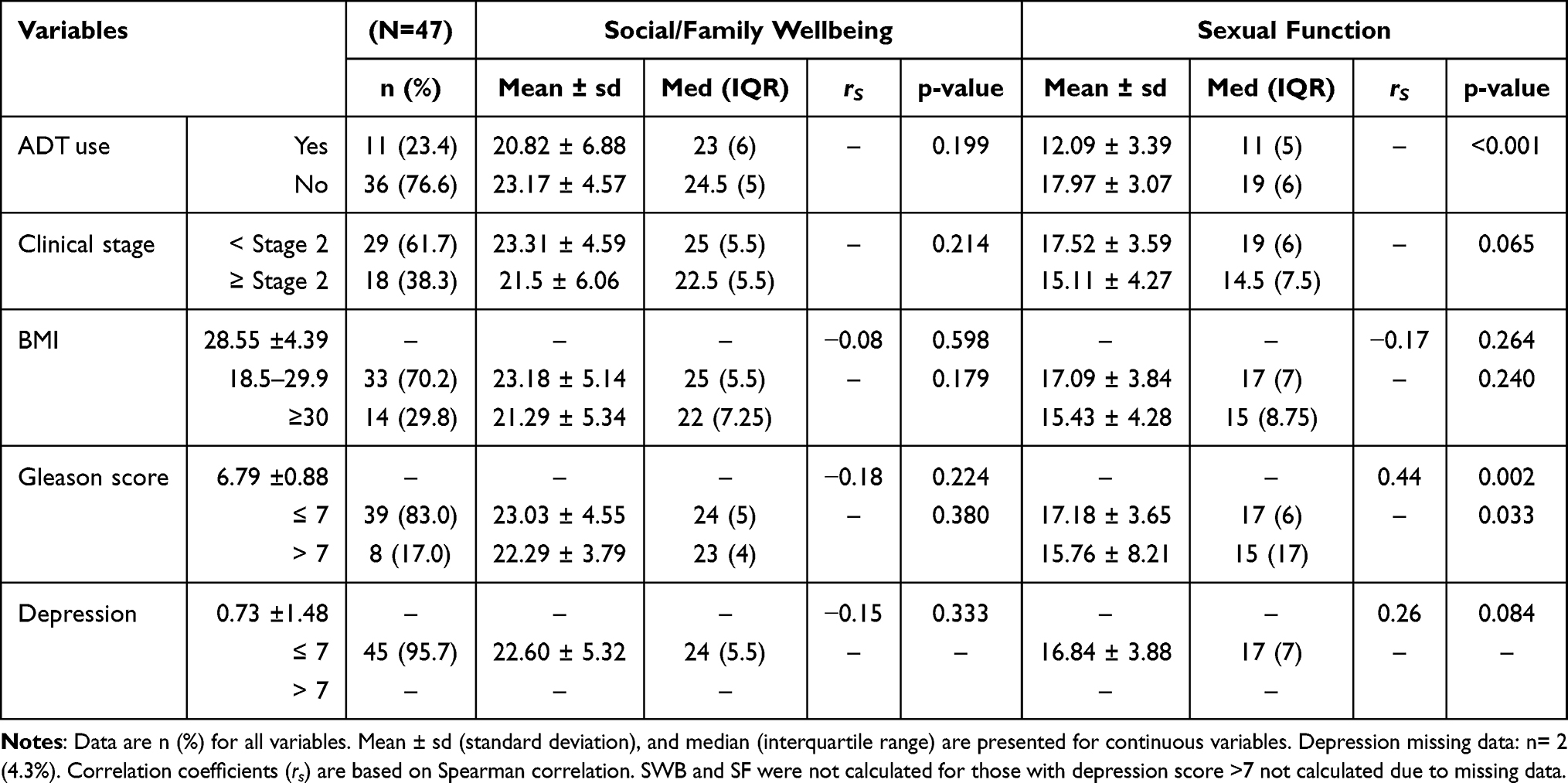 |
Table 4 Clinical Characteristics, Social/Family Wellbeing, and Sexual Function (Sub-Group Analysis) |
Social/Family Wellbeing, Sexual Function Distress and Sexual Function
There is a significant but weak negative correlation between social/family wellbeing and sexual function distress (rs= −0.386, p ≤ 0.001). A moderate positive correlation was noted between social/family wellbeing and sexual function (rs= 0.505, p < 0.001) in the subgroup analysis, suggesting that higher (better) social/family wellbeing scores is linked with lower sexual function distress and higher sexual function scores. When sociodemographic factors were controlled, a significant correlation between social/family wellbeing and sexual function distress was observed regardless of marital status, race, age, and education. However, a significant correlation between social/family wellbeing and sexual function was only observed in participants who were married (rs=0.52 p=0.002 vs rs=0.48 p=0.099), aged 65 years old or younger (rs=0.56 p=0.001 vs rs=0.48 p=0.052), identify as White (rs=0.50 p=0.001 vs rs=0.69 p=0.086), and have completed at least college-level education (rs=0.48 p=0.001 vs rs=0.50 p=0.667). Given the limitations in sample size, the results for the sub-group analysis may not be generalizable. For example, the number of participants who have completed less than college education in the sub-group analysis is only 3 out of 47 and 7 of the 47 identified as non-Whites.
In Table 5, it can be gleaned that only ADT use was found to be a significant moderator on the relationship between social/family wellbeing and sexual function distress. Without ADT use, every point increase in social/family wellbeing score results in a decrease in sexual function distress score by 0.78 (B= −0.78 p= <0.001). With ADT use (B=0.80 p= 0.008), every point increase in social/family wellbeing results in an increase of 0.02 in sexual function distress score. The results suggest that improving social/family wellbeing potentially decreases sexual function distress. However, patients receiving ADT may experience a slight increase in sexual function distress despite a higher or healthier social/family wellbeing. In the sub-group analysis, none of the clinical characteristics was found to have a moderating effect on the relationship between social/family wellbeing and sexual function, meaning participants who rated their social/family wellbeing higher also tended to rate their sexual function higher regardless of ADT use, Gleason score, cancer stage and level of patient-reported depression.
 |
Table 5 Moderating Effects of Clinical Characteristics on the Relationship Between Social/Family Wellbeing and Perceived Sexual Function Distress |
In summary, there were significant correlations between social/family wellbeing and the two domains of sexual health (sexual function and sexual function distress). Gleason and depression scores were found to be significantly correlated with social/family wellbeing and sexual function distress. Concomitant ADT use was the clinical characteristics found to be a significant moderator in the relationship between social/family wellbeing and sexual function distress. However, the results of this study only considered perceptions of sexual function and sexual function distress based on genitalia-focused sexual expressions and therefore cannot be used to generalize the state of sexual health of patients with prostate cancer.
Discussion
In this study, we observed a positive correlation between social/family wellbeing and sexual function and a negative correlation between social/family wellbeing and sexual function distress. This finding indicates that participants who rated their social/family wellbeing higher tend to report better sexual function. Consequently, those who rated their social/family wellbeing lower tend to have higher sexual function distress. Social/family support has been reported to help patients manage their cancer and cancer treatment-related symptoms. A prior study involving patients with bladder cancer showed a positive correlation between social/family support with decrease in cancer-related cognitive distress.19 Expressions of social support for cancer patients may be in the form of emotional support or tangible support such as helping them with transportation needs or assisting patients in gaining access to information.20
Among the clinical characteristics explored in this study, only ADT use was found to exert a moderating effect on the relationship between social/family wellbeing and sexual function distress. None of the clinical characteristics was noted to have a moderating effect on the relationship between social/family wellbeing and sexual function. ADT use is known to cause decrease in sexual desire and erectile dysfunction.21 Psychological changes such as emotional lability, low self-esteem, and depression have also been linked with ADT use.22–24 The physiologic and psychological changes that patients may experience during ADT use also affect marital relationships, communication, intimacy, and role perception.24 The lack of sexual intimacy may lead to negative emotions such as disappointment, guilt, feeling of premature aging, and low self-esteem.23 It is important to recognize that improving sexual health, particularly in patients receiving ADT, requires clinicians to discuss the effects not only related to the patient’s sexual function but also on how the side effects of this treatment may affect the patient’s role perception and relationships with others.
Disruptions in sexual relationships, especially in married or partnered patients with prostate cancer can be a distressing experience for both the patients and their partners. However, the perception of ADT side effects as an androcentric, meaning male-focused issue remains prevalent in both patients and clinicians.25 Past studies have shown that men with prostate cancer who are in a sexual relationship perceived sexual dysfunction as more bothersome.21 Married men may be concerned with fulfilling their partner’s sexual needs, in addition to their own thus increasing the feeling of burden caused by the limitations in their sexual function.13 Our findings showed that, statistically, there is no significant difference in the sexual function distress and sexual function scores of married and unmarried participants. However, there is significant difference in the social/family wellbeing when marital status is controlled. It is also noteworthy that when marital status is controlled, no significant relationship was found between social/family wellbeing and sexual function in unmarried participants, but a significant relationship between social/family wellbeing and sexual function distress was noted regardless of marital status.
De Vocht et al caution clinicians against assumptions about patient’s sexual health needs based on their age, relationship status or religion and culture.26 Thus, a comprehensive sexual health-related assessment and interventions should be part of care planning regardless of the patient’s marital or relationship status. This includes the development of inclusive, population-appropriate evaluation tools and interventions for all patients, even for patients from gender minorities. In addition, the concept of sexual intimacy should not solely be focused on the physical aspects of a person because sexual intimacy also encompasses affective and even cognitive components.27 The Global Advisory Board (GAB) for Sexual Health and Wellbeing defines sexual pleasure as “the physical and/or psychological satisfaction and enjoyment derived from solitary or shared erotic experiences, including thoughts, dreams and autoeroticism”. The GAB for Sexual Health and Wellbeing further asserts that the experience of sexual pleasure is a diverse human experience, and the rights of all people to have a positive sexual experience should be upheld.28 Even in its early conception, the definition of sexual health encompassed aspects beyond the physical view of sexuality. The first definition of sexual health formulated by the WHO in 1975 included emotional, intellectual, and social aspects of a person as a sexual being. The aim of sexual health according to WHO’s first definition includes the enhancement of personality, communication, and love.29
Evaluation of sexual health in patients with prostate cancer should consider other comorbidities such as cardiovascular diseases, diabetes and clinical depression that may also contribute to changes in sexual function.30 It is important to note that the overall health of the patient’s sexual partner also plays a role. For example, women with diabetes tend to be less sexually active than women without diabetes.31 In addition, changes in sexual response associated with aging affect both men and women.32 Additional factors such as the age and the presence of medical conditions in the partners of patients with prostate cancer should be considered. When patients report a decline or absence of sexual activity, the reason for this should be explored so that patients or their partners could be given appropriate interventions.
In this study, the majority of the participants were White (73%), married (78.8%), and have completed a college degree or higher (80.3%). Future studies involving a more diverse pool of participants that can be more representative of the general population would be beneficial in building more generalizable conclusions when comparing groups based on demographic characteristics such as race, marital status, or the highest education received.
Another aspect that needs to be revisited in this study is the use of more inclusive categories to indicate sexual relationships. In this study, categories for marital status only included married, single, widowed, or divorced. These categories do not necessarily reflect whether the participant is engaged in any form of sexual relationship. For example, Lindau et al used the category “spousal or other intimate relationships” when participants indicated that they have “romantic, intimate or sexual partners”.31 In addition, questions related to sexual health in this study were exclusive to aspects of sexual intercourse (eg, erection, penetration, and ejaculation). Thus, limiting the possibility of exploring participants’ perspectives on other forms of sexual expressions such as non-genitally focused sexual activities such as kissing, hugging, and touching, as well as solitary sexual activities such as masturbation.32
Practice guidelines should ensure that a holistic approach in understanding and addressing sexual health are observed. Assessment tools and algorithms that allow a more comprehensive evaluation of sexual needs and sexual health could help clinicians provide more person-centered holistic interventions that will create a positive experience for patients. Clinicians should be aware of the influence of culture on how patients express their sexual needs or how they respond to questions related to sexuality. A study found that perceived language appropriateness in describing data related to sexual health is a source of discomfort in some patients or their partners. In addition, the setting and context in which the discussion on sexual health takes place affect patients’ responses with patients likely to be more open when the discussion is conducted in a home setting.33 These findings underscore the value of having dynamic sexual health programs to accommodate the sexual health needs of individuals from culturally, linguistically, and gender diverse backgrounds. It is also important to consider the unique needs of individuals who are engaged in non-monogamous sexual relationships. Studies that would compare the effectiveness of clinic-based versus community-based sexual health programs, as well as patients’ responses to professionals (eg, physicians or nurses) versus trained community navigators would also be valuable.
Conclusion
The effects of prostate cancer and its treatment, such as ADT, on sexual function are well-documented. There are also published evidence that highlight the role of social support in the emotional and mental wellbeing, as well as the quality of life of people with prostate cancer. However, to our knowledge, there are no studies that explored the association between social/family wellbeing and specific domains of sexual health (sexual function and sexual function distress). The result of this study, as well as published literature, suggest that prostate cancer diagnosis and treatment affect patients and their intimate partners. Thus, it is essential to employ a holistic approach to addressing the sexual health needs of patients with prostate cancer. This may include an evaluation of the patient’s family or social wellbeing and sexual health in planning prostate cancer treatment. Options to mitigate side effects of cancer treatment, such as erectile dysfunction or a decrease in sexual desire, must be thoroughly discussed with patients and their partners prior to the treatment. Particular attention should be given to patients whose treatment regimen includes ADT as this does not only have a direct association with sexual health but can also affect the relationship between social/family wellbeing and sexual health.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author and will be shared according to the institutionally approved data sharing plan.
Acknowledgments
The authors acknowledge the contribution of Mr. Michael Steele who managed and prepared the data needed for this study, Dr. Xiaobai Li for providing statistical support for this study and the NIH Fellows Editorial Board for their technical assistance in the preparation of this manuscript. This study is supported by the Division of Intramural Research in the National Institute of Nursing Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health and the National Institute of Nursing Research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Smith DP, Calopedos R, Bang A, et al. Increased risk of suicide in New South Wales men with prostate cancer: analysis of linked population-wide data. PLoS One. 2018;13(6):e0198679. doi:10.1371/journal.pone.0198679
3. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
4. cancer.org [homepage on the internet]. Key statistics for prostate cancer. American Cancer Society; [cited January 16, 2023]. Available from: https://www.cancer.org/cancer/prostate-cancer/about/key-statistics.html.
5. Vear NK, Coombes JS, Bailey TG, Skinner TL. The interplay between vascular function and sexual health in prostate cancer: the potential benefits of exercise training. Med Sci. 2020;8(1):11.
6. Watson E, Shinkins B, Frith E, et al. Symptoms, unmet needs, psychological well-being and health status in survivors of prostate cancer: implications for redesigning follow-up. BJU Int. 2016;117(6B):E10–E19. doi:10.1111/bju.13122
7. Brautigam E, Schratter-Sehn A, Kottmel A, Bitzer J, Teleky B, Ucsnike L. Do radiation oncologists talk about sexual health and dysfunction with their cancer patients? Results of the igls-Vienna-sexmed-survey. Clin Transl Radiat Oncol. 2020;21:120–126. doi:10.1016/j.ctro.2020.01.005
8. Mollaioli D, Ciocca G, Limoncin E, et al. Lifestyles and sexuality in men and women: the gender perspective in sexual medicine. Reprod Biol Endocrinol. 2020;18(1):10. doi:10.1186/s12958-019-0557-9
9. Zhou ES, Nekhlyudov L, Bober SL. The primary health care physician and the cancer patient: tips and strategies for managing sexual health. Transl Androl Urol. 2015;4(2):218–231. doi:10.3978/j.issn.2223-4683.2014.11.07
10. Hyun JS. Prostate cancer and sexual function. World J Mens Health. 2012;30(2):99–107. doi:10.5534/wjmh.2012.30.2.99
11. Palacios LAG, Krouwel EM, den Oudsten BL, et al. Suitable sexual health care according to men with prostate cancer and their partners. Support Care Cancer. 2018;26(12):4169–4176. doi:10.1007/s00520-018-4290-2
12. Hald GM, Pind MD, Borre M, Lange T. Scandinavian prostate cancer patients’ sexual problems and satisfaction with their sex life following anti-cancer treatment. Sex Med. 2018;6(3):210–216. doi:10.1016/j.esxm.2018.06.002
13. Smith AB, Wittmann D, Saint Arnault D. The ecology of patients’ sexual health adjustment after prostate cancer treatment: the influence of the social and healthcare environment. Oncol Nurs Forum. 2020;47(4):469–478. doi:10.1188/20.ONF.469-478
14. Scandurra C, Muzii B, La Rocca R, et al. Social support mediates the relationship between body image distress and depressive symptoms in prostate cancer patients. Int J Environ Res Public Health. 2022;19(8):4825. doi:10.3390/ijerph19084825
15. Zhou ES, Penedo FJ, Lewis JE, et al. Perceived stress mediates the effects of social support on health-related quality of life among men treated for localized prostate cancer. J Psychosom Res. 2010;69(6):587–590. doi:10.1016/j.jpsychores.2010.04.019
16. Zimmerman M, Martinez JH, Young D, Chelminski I, Dalrymple K. Severity classification on the Hamilton Depression Rating Scale. J Affect Disord. 2013;150(2):384–388. doi:10.1016/j.jad.2013.04.028
17. Leppink J. Analysis of covariance (ANCOVA) vs. Moderated Regression (MODREG): why the interaction matters. Health Professions Education. 2018;4(3):225–232.
18. Mackinnon DP. Integrating mediators and moderators in research design. Res Soc Work Pract. 2011;21(6):675–681.
19. Heyes SM, Bond MJ. Pathways to psychological wellbeing for patients with bladder cancer and their partners-in-care. Eur J Oncol Nurs. 2020;46:101757.
20. Parthipan M, Feng G, Toledano N, et al. Symptom experiences of older adults during treatment for metastatic prostate cancer: a qualitative investigation. J Geriatr Oncol. 2022;14(1). doi:10.1016/j.jgo.2022.10.012
21. Schover LR. Sexual healing in patients with prostate cancer on hormone therapy. Am Soc Clin Oncol Educ Book. 2015;35(1):e562–e566. doi:10.14694/EdBook_AM.2015.35.e562
22. Donovan KA, Walker LM, Wassersug RJ, Thompson LMA, Robinson JW. Psychological effects of androgen-deprivation therapy on men with prostate cancer and their partners. Cancer. 2015;121(24):4286–4299. doi:10.1002/cncr.29672
23. Shahinian VB, Kuo YF, Freeman JL, Goodwin JS. Risk of the “androgen deprivation syndrome” in men receiving androgen deprivation for prostate cancer. Arch Intern Med. 2006;166(4):465–471. doi:10.1001/archinte.166.4.465
24. Walker LM, Robinson JW. The unique needs of couples experiencing androgen deprivation therapy for prostate cancer. J Sex Marital Ther. 2010;36(2):154–165. doi:10.1080/00926230903554552
25. Wassersug RJ. Maintaining intimacy for prostate cancer patients on androgen deprivation therapy. Curr Opin Support Palliat Care. 2016;10(1):55–65. doi:10.1097/SPC.0000000000000190
26. de Vocht H, Hordern A, Notter J, van de Wiel H. Stepped Skills: a team approach towards communication about sexuality and intimacy in cancer and palliative care. Australas Med J. 2011;4(11):610–619. doi:10.4066/AMJ.2011.1047
27. Aykutoglu B, Uysal A, Wu H. The relationship between intimacy change and passion: a dyadic diary study. Front Psychol. 2017;8:8. doi:10.3389/fpsyg.2017.00008
28. gab-shw.org [homepage on the internet]. Working definition of sexual pleasure 2016. Global Advisory Board for Sexual Health and Wellbeing: c2006–c2018; [cited January 16, 2023]. Available from: https://www.gab-shw.org/our-work/working-definition-of-sexual-pleasure/.
29. Gruskin S, Yadav V, Castellanos-Usigli A, Khizanishvili G, Kismodi E. Sexual health, sexual rights and sexual pleasure: meaningfully engaging the perfect triangle. Sex Reprod Health Matters. 2019;27(1):1593787. doi:10.1080/26410397.2019.1593787
30. Nicolosi A, Moreira ED, Shirai M, Bin Mohd Tambi MI, Glasser DB. Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Urology. 2003;61(1):201–206. doi:10.1016/S0090-4295(02)02102-7
31. Lindau ST, Schumm LP, Laumann EO, Levinson W, O’Muircheartaigh CA, Waite LJ. A study of sexuality and health among older adults in the United States. New Engl J Med. 2007;357(8):762–774. doi:10.1056/NEJMoa067423
32. Srinivasan S, Glover J, Tampi RR, Tampi DJ, Sewell DD. Sexuality and the Older Adult. Curr Psychiatry Rep. 2019;21(10):97. doi:10.1007/s11920-019-1090-4
33. Kelly D, Forbat L, Marshall-Lucette S, White I. Co-constructing sexual recovery after prostate cancer: a qualitative study with couples. Transl Androl Urol. 2015;4(2):131–138. doi:10.3978/j.issn.2223-4683.2015.04.05
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.