")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Family Members’ Experiences of Young-Onset Dementia: Becoming Responsible Yet Feeling Powerless
Authors Aspö M , Visser LNC , Kivipelto M, Boström AM , Seiger Cronfalk B
Received 27 May 2023
Accepted for publication 5 July 2023
Published 17 August 2023 Volume 2023:16 Pages 2379—2390
DOI https://doi.org/10.2147/JMDH.S418285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Malin Aspö,1,2 Leonie NC Visser,1,3,4 Miia Kivipelto,1,2,5,6 Anne-Marie Boström,2,6,7 Berit Seiger Cronfalk7
1Division of Clinical Geriatrics, Center for Alzheimer Research, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden; 2Theme Inflammation and Aging, Karolinska University Hospital, Stockholm, Sweden; 3Department of Medical Psychology, Amsterdam UMC Location AMC, University of Amsterdam, Amsterdam, the Netherlands; 4Amsterdam Public Health Research Institute, Quality of Care, Amsterdam, the Netherlands; 5Neuroepidemiology and Ageing Research Unit, School of Public Health, Imperial College London, London, UK; 6Stockholms Sjukhem, Research & Development Unit, Stockholm, Sweden; 7Department of Neurobiology, Care Sciences and Society, Division of Nursing, Karolinska Institutet, Stockholm, Sweden
Correspondence: Malin Aspö, Theme Inflammation and Aging, Karolinska University Hospital, Stockholm, 171 64, Sweden, Tel +4672-582 32 39, Email [email protected]
Purpose: Dementia is often associated with old age but can also occur in midlife. The latter is commonly referred to as young-onset dementia (YOD). The diagnosis not only has an impact on the persons with YOD but also on their family members. For family members, the diagnosis changes their lives, as responsibilities and roles alter when the care and wellbeing of the relative increasingly come into focus. The aim of this study was to explore family members’ experiences of sharing lives with a relative diagnosed with YOD – from onset of symptoms until the person relocated to a nursing home.
Patients and Methods: The study has a qualitative approach with in-depth interviews. In total, the study included 15 family members aged ≥ 18 years participated, all with a relative diagnosed with dementia before the age of 65. At the time of the interview, all had a relative living in a nursing home. The interviews were analyzed using thematic analysis.
Results: Two key themes were identified: Becoming responsible and Dealing with the situation. Family members found themselves increasingly responsible for many parts of their relatives’ lives and forced to make decisions on their behalf. This was experienced as being lonely, as family members wished to share their responsibility. Despite of their efforts to control and deal with their situation, family members reported a lack of power to influence certain factors, such as access to appropriate healthcare services, causing feelings of distress.
Conclusion: These findings emphasize the need of improved and tailored support and guidance for family members of persons with YOD. Further, the findings highlight the importance of increased knowledge and awareness among social workers and other healthcare professionals regarding support to family members of persons with YOD.
Keywords: YOD, relative, psychosocial support, qualitative, health care system
Introduction
Dementia is often associated with old age, but onset of symptoms can also occur in midlife, before the age of 65. The global prevalence of dementia before the age of 65 is estimated to be 119 per 100.0001 and is commonly referred to as persons living with early- or young-onset dementia (YOD). Young onset dementia affects whole families, and the impact is likely to be different from that of dementia in older persons. Family members of persons with YOD are often in midlife themselves and handle multiple roles and obligations, both professionally and socially.2 Their need to fulfill family obligations has been identified as a factor that could hinder acceptance of support.3 As the disease progresses, family members gradually take over roles and responsibilities otherwise handled by the person with YOD him/herself and become an informal caregiver;4 a situation they were not prepared for, as the multitude of responsibility is both challenging and burdensome.5
Previous research shows that a person with YOD stay in their private home for an average of nine years before being relocated to a nursing home.6,7 This is twice as long as older persons with dementia stay in their private homes, and this might also suggest that persons with YOD more often stay in private homes until the end of life.7 During the extended time, a person with YOD lives at home family members play an important role.8 Acting as primary caregivers is experienced to reduce quality of life compared to the general population, especially in domains of role limitations.9 In addition, family members also report increased burden and reduced sense of wellbeing compared to caregivers of persons with late onset dementia,10 even if the care need was less than the need of the older person with dementia.5 Bannon et al11 reported several psychosocial stressors that affected the family members’ sense of burden, including endless worries for the person’s well-being, shift in responsibilities (eg, family member taking full responsibility for household chores), and loss of meaningful relationship to the person with dementia. Caring for a person with dementia can consequently have negative psychological and physiological effects.12
Previous research characterized family members’ use of strategies to cope as adaptive strategies and dysfunctional strategies. The adaptive strategies involve problem focus, acceptance, and social-emotional support with positive effects on mental health and depression.12,13 Strategies associated with negative effects on family members' well-being are reported as denial, avoidance, and aspiring thoughts,11,12 self-blame and/or substance abuse,13 while others turn to work as a means to distract themselves.13 Gilhooly et al12 suggest that dysfunctional coping strategies are used as a means to maintain normality. In addition, family members applied strategies focusing on interpreting the relative’s problematic behavior as a consequence of the disease, and their need of relief as caregiver.11 Bannon et al11 argue that even though family members engage in adaptive coping strategies, the increased burden and distress suggest that these strategies are not sufficient. Furthermore, these strategies also act as a barrier to accept and receive support and to plan ahead11 but also, as suggested by Monteiro et al13 to avoid stress and burden. In addition, previous research also highlights that family members who care for a person with dementia need age-appropriate support and information concerning YOD.14–16
Family members’ needs might change as dementia progresses and depend on the type and closeness of the relationship the family member has to the person with YOD. Research often only includes family members who are the primary caregiver and are living with the person with YOD. However, there is a need to gain better understanding of the specific needs and challenges of all family members, including those who are not involved in the daily care and/or living together with the persons with YOD. As relocation to a nursing home often occurs in the later phases of dementia (if at all), interviewing family members with a relative who is currently living in a nursing home will provide insight in the experiences and needs regarding different phases of the disease. The aim of this study was therefore to explore the experiences of various close family members of a person diagnosed with YOD – from onset of symptoms until that person relocated to a nursing home.
Materials and Methods
Study Design
This study has a qualitative approach, using in-depth interviews and thematic analysis.17
Ethical Approval
The study was conducted in compliance with The Declaration of Helsinki18 and approved by the Regional Ethical Review Board in Stockholm, Sweden (Dnr: 2018/1179-31/1 and Dnr: 2020-00743). Written consent was obtained from all and included consent for publication of anonymized responses, such as quotes from the interviews.
Setting and Recruitment of Participants
The study was conducted in Sweden and applied a purposive sampling technique. Initially, participants from one specific nursing home were included followed by the inclusion from three other nursing homes and one support group. Inclusion criteria were family members ≥18 years of age, with a relative diagnosed with YOD living in a nursing home.
The recruitment was conducted as follows: At the sites (nursing homes) managers and the person in charge of the support group were contacted and informed about the study by the first author. They were then asked to identify and inform family members about the study if they met given inclusion criteria. Family members who were interested in the study contacted the first author by phone to receive further and more detailed information about the study. Twenty-eight family members expressed interest to participate, 13 family members did not participate after reviewing the detailed information. In total 15 family members were included in the study.
Data Collection
All participants were interviewed twice between May 2019 and December 2020 by the first author, who is a specialized nurse with extensive experience of dementia. Following acceptance to participate in the study, all family members signed the informed consent form, followed by arranging a date, time, and place for the first interview. During the first interview, a date and time for the second interview was decided. The second interview was conducted within two months from the first interview. The interviews were initially conducted face-to-face. However, due to the Covid-19 pandemic, interviews conducted between March 2020 and December 2020 were carried out by phone or video call. Interviews lasted between 42 and 99 minutes (mean = 66 minutes).
The first interview focused on identifying critical situations and experiences throughout the disease trajectory. Examples from the interview guide are provided in Table 1. The second interview provided an opportunity to follow-up on the first interview, ask additional questions, and confirm that information from the first interview was correctly perceived. By asking questions such as “Since we last spoke, is there something you have been thinking about, that you would like to share?” or “As I interpreted from our first interview you XX, is this correct?”
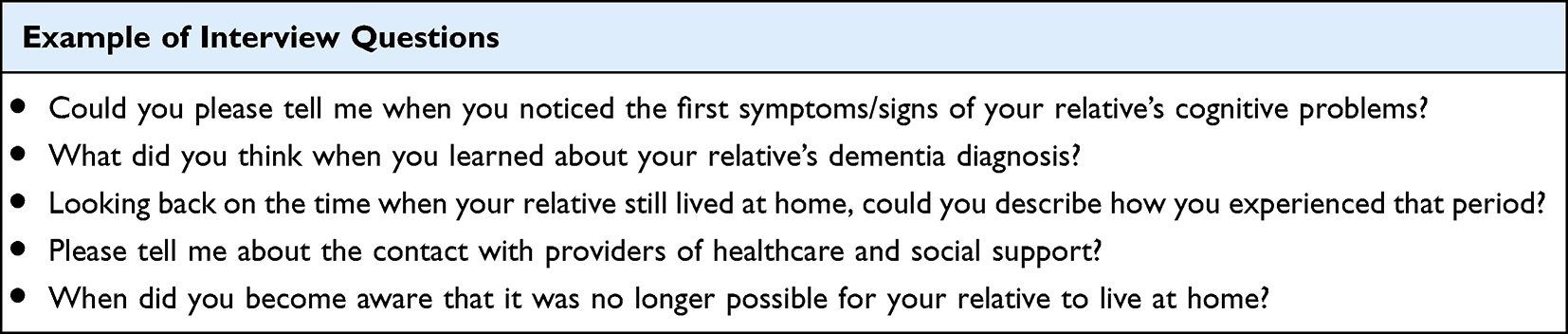 |
Table 1 Example of Interview Questions |
Analysis
A qualitative inductive thematic analysis was conducted to identify latent themes, following the six steps for thematic analysis (TA), as described by Braun & Clarke;17 1) Familiarization, 2) Coding, 3) Generating themes, 4) Reviewing themes, 5) defining themes, and 6) writing up. Most interviews were transcribed by the first author, who also conducted the interviews. The remaining interviews were transcribed by a research assistant not involved in the data collection, after which the transcriptions were checked by the first author. This was followed by familiarization of data, conducted individually by the first and last author, to get a deeper understanding of the content and to identify patterns and potential themes. An example of the coding process is provided in Table 2. The coding was performed in the software program MaxQDA. The codes were grouped to initial themes, and these were reviewed and discussed by the first and last author until consensus was reached. The analysis procedure also included workshops, with the second author, to refine and further develop themes and sub-themes. All co-authors participated in the analytic process until consensus was reached. During the analysis, the researchers needed to reflect on their own understanding. Therefore, all were consciously reflecting on how their previous experiences and knowledge may influence the analytic process, to lessen its influence and risk of selection bias, as all have extensive experiences and knowledge of persons with dementia and their family members (in the field of nursing, psychology, and medicine). Three participants were family members of the same person with YOD, and the interviews with these participants were independently analyzed, since they reflected different/unique perspectives.
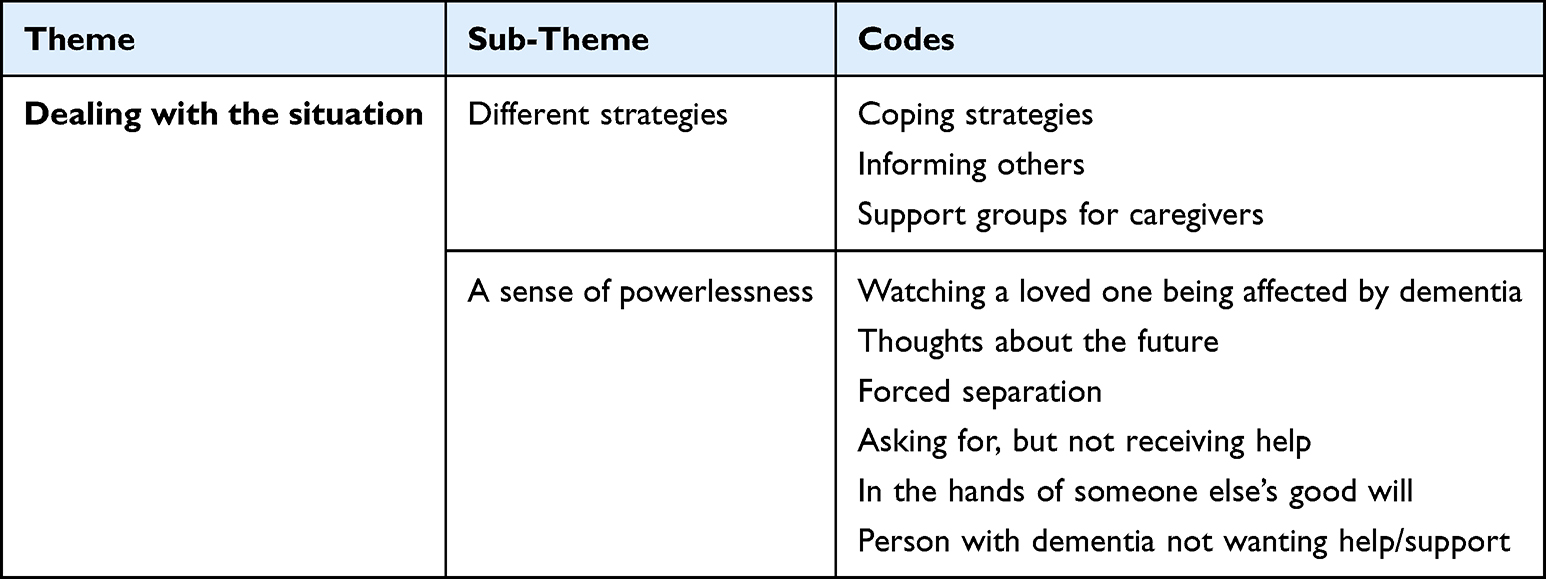 |
Table 2 Example of Coding |
Results
In total, 15 family members of 13 persons with dementia were included: nine women and six men with an average age of 52 at the time of their relative’s diagnosis. The family members’ relationships with their relative varied: nine partners, three children and three siblings. All participants, except one sibling, were considered responsible for making decisions and looking after the wellbeing of the person with YOD, on behalf of the person with YOD. Eight of the partners lived together with the person with YOD prior to that person relocating to the nursing home, and one partner and the person with YOD had been living in separate homes for several years (already prior to onset of symptoms). None of the adult children and siblings that were interviewed were living together with the person with YOD before onset of symptoms or at time of the move to the nursing home. The relatives were diagnosed with dementia: Alzheimer’s disease (AD), frontotemporal dementia (FTD) and dementia due to Wernicke-Korsakoff’s syndrome (WKS). Table 3 displays sample characteristics.
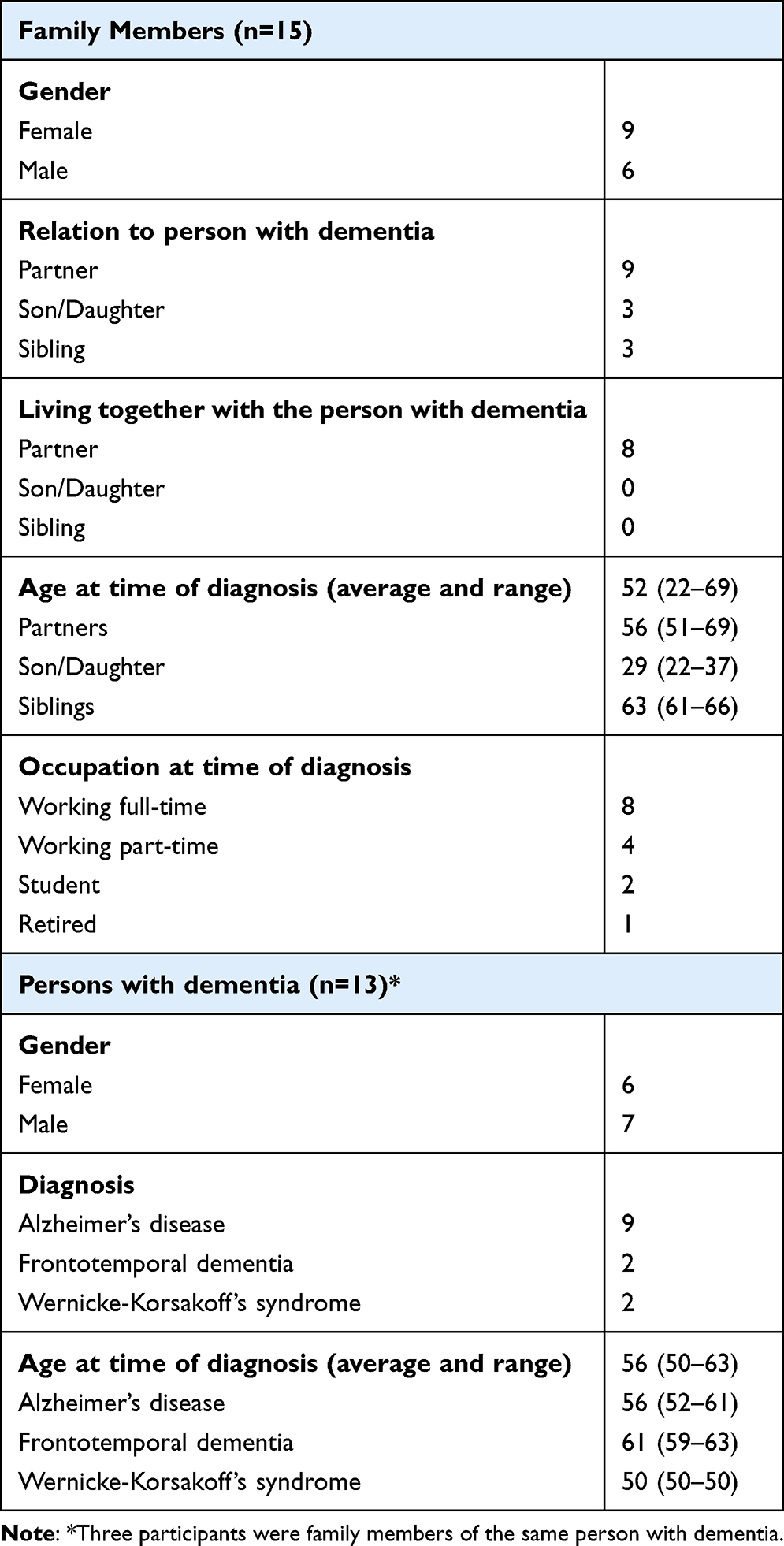 |
Table 3 Sample Characteristics |
The findings are presented in two themes: “Becoming responsible” and “Dealing with the situation” and five sub-themes (Table 4).
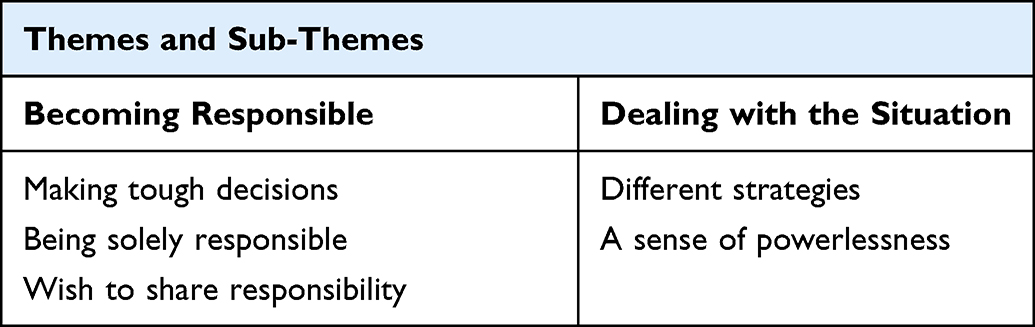 |
Table 4 Overview of the Themes |
Becoming Responsible
During onset of dementia, family members gradually found themselves responsible for their relative. This responsibility forced them to make several tough decisions. Most experienced being solely responsible for the decision making, although this varied depending on the relationship with their relative and other family members.
Making Tough Decisions
Family members described how they often had to make decisions on behalf of the relative with YOD, sometimes violating their autonomy. Undoubtedly, the toughest decision was being responsible for the relocation of the relative to a nursing home. It was often a decision made against the relative’s own will. This caused feelings of guilt and betrayal and was often experienced as a failure to protect and care for the relative. Family members portrayed that they often felt alone in making this crucial decision. This made them question if they had made the correct decision.
I felt that I did not do enough, I did not fight hard enough. I put all the blame on myself. I should have done more…. [1: Wife, AD]
Making decisions that violated the will and autonomy of the relative with dementia was difficult for all. However, those with previous experience of dementia were better able to justify their decisions. Family members described the importance of someone else, preferably a professional, confirming they had made the right decisions.
When she was offered to relocate to a nursing home, I made several phone calls to the day care center to ask their opinion. And they told me that it most likely was time for her to move. [2: Partner, AD]
After the decision to relocate the relative to a nursing home was made, handing over responsibility to others was described in two ways: both as a relief and as a cause of anxiety. As time passed and family members established a relationship with the nursing staff, worries and anxiety decreased. The staff’s competence and readiness to share responsibility for the relative’s wellbeing meant that some family members could reverse.
I cannot describe the relief it is that he is living here (nursing home), and to see that he is in good hands. [3: Sister, FTD]
Still, some found it difficult to hand over responsibility and control. They described it as their role to protect the relative and feared that their relative’s needs would not get the attention needed. Which sometimes also seemed to be the case, as illustrated in the quote below.
They (nursing staff) would not let him take walks, so he stopped. His balance became worse and his ability to walk got worse. Exactly what I was afraid would happen. So, it was not long before he was in a wheelchair. [14: Wife, AD]
Being Solely Responsible
Family members described how they carried multiple responsibilities alone. They described how their daily lives were drastically affected as they no longer were able to share the responsibilities with their partner and found themselves trapped with responsibilities they previously had shared.
And during it all we had three children … And at the same time a husband with a brain that was not working as it should. And on top of that a dog that he should take for walks but was not able to, so the children and I had to do it. [14: Wife, AD]
Partners also experienced social isolation to a greater extent than other family members. Lack of energy and not being able to leave the partner alone were described as the main reasons for withdrawing from social activities. It was also evident for some that they no longer were included in social activities, as friends withdrew from contact and stopped including them as couple in social engagements.
What I miss… This disease put an end to everything, friends disappeared as they did not feel comfortable seeing us. And all leisure activities and other things I have done, I had to stop. [5: Wife, AD]
Being the partner with sole responsibility was lonely and overwhelming at times. This became evident in contact with administrative and health care organizations regarding different aspects of support. Some partners were forced to continue their employment as the financial situation was hard to deal because the relative could no longer contribute financially. Besides being solely responsible for the current financial situation, partners also needed to focus on their own future financial stability.
I had to work full time to be able to finance all of this. Pay the bills and buy food, the cost of food is massive when you feed five persons and we live in a house with mortgages. [14: Wife, WKS]
In contrast to the partners, adult children and siblings explained that they had no or sparse experience of sharing everyday life with their relative prior to the diagnosis. Even though it was described as challenging to suddenly take on the responsibility, some also experienced the relationship to improve throughout the care-taking process.
And then suddenly it was I who should be responsible for his life. It was strange. I was thinking “Do I really know him?” and “What do I feel about this?” Our distance and lack of relationship for so many years made it more complicated. [7: Sister, AD]
Wish to Share Responsibility
The process of sharing responsibility between family members was often described as challenging. The three participants who were relatives of the same person with YOD described that the responsibility for making decisions was shared between the two adult children. This was described to lessen the burden when forced to make tough decisions. For some family members, it became clear that persons not included in the immediate family sometimes found it difficult to comprehend the situation and because of that withdrew from contact.
It was difficult because I believed that it might be too early (for her to move), on the other hand her children did not support me as much as I had hoped for… One daughter told me that I could not decide when they should meet their mother. Of course not, but I just tried to share the burden. [2: Partner, AD]
Social welfare services were described as an organization lacking knowledge about the specific needs of families to persons with YOD. It became evident as family members described a lack of interest from the social welfare offices to support them in difficult times.
I expected to get help from the social welfare agency, but it was not at all what I expected. I had to know myself what support to apply for and that was the problem. How could I know? What I needed to know was what decisions to make so that I could make the right ones. [13: Husband, AD]
Not all family members were disillusioned as some portrayed themselves as fortunate as they were in contact with experienced social welfare managers and physicians at the memory clinic, who had knowledge of and experience with YOD. These professionals acted in line with what the family members expected and evaluated their needs when planning care and support services.
She (the social welfare officer) was great as she was able to fix things I myself did not understand or know. Thinking back, I realize that she knew what we had to expect (in the future). And she did all she could without me having to ask her. I just explained to her “help!” and “what shall I do?” [4: Wife, AD]
Sometimes one need a hand to hold on to. And in my case the physician was the one who realized my needs. She was straight forward and told me what I needed to do rather than asking if I wanted. [10: Husband, AD]
Dealing with the Situation
Family members described how they had to manage the situation and how they tried to remain in control by using different strategies. Despite their efforts to cope, family members reported not being able to or have the power to influence certain factors, such as the progression of the dementia, their own emotional responses, and support and care received by the health care organizations.
Different Strategies
Family members described different strategies, to manage their own feelings and burden. One strategy was to turn off their own emotions and focus on solving problems or the needs of the other.
My way of handling most of this has been to turn off my feelings because it was hard to handle otherwise. [4: Wife, AD]
Another strategy was to inform others about the relatives’ diagnosis, hoping that people would be understanding and accept the changed or deviant behavior. However, not all relatives allowed their family member to tell others about their diagnosis. Family members that were forced by the demented relative to cover up their cognitive symptoms described that as stressful.
I believe it’s important, to inform them so that they understand that there is a reason for his behaviour. Why he does certain things. I have noticed that the neighbours help him for example if he can’t remember the code to the door, helping him to get in. Or when he has left the keys in the door lock, which happens quite often. The neighbours are observant, to me that is positive. [12: Wife, AD]
Seeking further knowledge about dementia and dementia care was described as a means to try to comprehend the situation and prepare for the future. Online searches and participation in support groups were described as important resources of information. Sharing experiences, receiving guidance and support from others in the same situation were described to reduce the experience of being isolated. Still, a criticism regarding the support groups was that they focused on Alzheimer’s disease and/or older persons with dementia and therefore not fully providing support for family members of persons with YOD or non-Alzheimer related dementias.
We had so much in common and it was nice to hear that I am not a lunatic. no I have quite normal reactions. It was really a relief to meet the group and talk about my response and my situation [3: Sister, FTD]
Another strategy was to continue work, and this was described as positive for some family members. Especially partners experienced working as an opportunity to spend time in a social environment and in a context away from a chaotic home situation. Others described work as a place to keep them busy, focusing on something else than their relative. Still, being away from home could also be stressful, unless the relative was engaged in daily care activities, since being at work or occupied with other engagements meant that they had no control of what happened at home.
At home during this period it was chaos all the time. I don’t know what I would have done without work. I had not managed. To be with him all the time I don’t think I would have managed it. My job was my haven…. [1: Wife, AD]
A Sense of Powerlessness
Despite applying different strategies to deal with the situation, sharing lives with a relative with YOD was related to a sense of being powerless. Especially partners expressed loss and grief as the relative no longer was able to be an active part of their lives. Not being able to influence disease progression was experienced as unbearable, especially in the early phases of the disease. However, family members to a relative with a progressive type of dementia experienced that the relative’s conscious suffering decreased as the disease advanced, while their own level of suffering was difficult to endure throughout the entire trajectory.
It is especially when I am with my children and grandchildren that I think of what we could have done together. It is difficult but it is really my own grief as he is not capable to grieve or miss our life at all. [4: Wife, AD]
In contrast, having a relative with dementia due to Wernicke-Korsakoff’s syndrome was related to another type of powerlessness. Family members described that the relative’s cognitive status had improved after they had stopped abusing alcohol. This made them reflect on their relative’s health perspectives rather than when the relative would pass away.
It depends on how much she will improve. I would imagine that there is a limit, but I don’t know. I cannot see into the future or so. I find it hard to believe that she one day suddenly wakes up and is independent, I don’t think so. But you never know, maybe. She is still young, that’s the thing. The brain is healing. [6: Son, WKS]
In the earlier phases of dementia, family members described frustration and anger that they were unable to influence important decisions, as the responsibility to make decisions was left to the relative himself/herself. From the family members’ perspective, accepting care or support was considered pivotal to the relative’s standard of living. Yet, the relative often declined support which meant that family members remained solely responsible for his/her safety and wellbeing.
He refused home care, shut the door in their faces. He did not want, opened the door again and said, “No thank you I am okey”. [3: Sister, FTD]
Family members described not being able to influence care services and experienced that support was mostly approved based on predefined standards and financial aspects, and not based on the individual’s needs. Some described that they were in the hands of care manager’s good will.
She (social care officer) told me that “Your application is at the bottom of this pile of papers now and I don´t know when I get the time to consider it”. When you find yourself in a desperate situation it is not what you want to hear. [4: Wife, FTD]
Still, contact with professionals at the memory clinics was described as important even if these professionals had no power to influence the social welfare services.
They have different approaches. The doctor has one way to look at it, focusing on the need of care and support. While the others (social welfare organization) sit and count money. [10: Husband, AD]
The lack of support from health care organisations and authorities was described as critical and generated feelings of powerlessness. In some cases, affecting their psychological and physical wellbeing negatively.
Later my whole body crashed, everything crashed, I could not walk. My body was in a state of emergency associated with stress. It still is sometimes. [9: Son, FTD]
Some family members described a sense of relief and freedom as they had relocated the relative to a nursing home. The relocation meant that they re-gained some influence over their own lives. Still, some reported that they could not move on in life before their relative had passed.
Now I am feeling great. I have met a woman a couple of years ago, so I am living in a new relationship. But I have decided not to divorce my wife, because it does not change anything…I still bring her home for a weekend every month. [8: Husband, WKS]
All family members reported a drastic change in life due to a relative being diagnosed with YOD. During the onset of symptoms leading up to the diagnosis, most family members described that they had no previous experience of dementia. Initially, the thought and insight of taking on responsibility for the relatives’ care and wellbeing was experienced as challenging. To handle the responsibilities, while also managing other obligations and roles, was described as difficult. This at a time when they also had to deal with the grief of seeing the cognitive functioning and health of a loved one deteriorate, as well as with feelings related to a drastically changed life situation.
Discussion
Family members of persons with YOD described their situation as life-changing. Our findings highlight the importance of better attending to the specific needs of family members of persons with YOD. Becoming responsible for a relative with YOD is difficult, and most experience a strong sense of powerlessness and distress, despite their best efforts to deal with the situation.
Our findings suggest that family members had different strategies and tried to manage their situation. This is in line with previous research11–13 as family members have been described to use both adaptive and dysfunctional strategies as means to cope. In our study, adaptive strategies were used such as seeking information, revealing the diagnosis to others, and preparing for the future. Monteiro et al13 showed that such strategies had a positive impact, as they reduced depression, anxiety, and stress. Planning for the future was a beneficial strategy, even if it was difficult to plan ahead due to uncertainty of disease progression and lack of support, thereby contributing to feelings of powerlessness and distress. Our findings are in line with Bannon et al,11 indicating the need for psychosocial interventions which could help facilitate family members and relatives with dementia to cope with their situation. We also argue that family members need information about financial and legal aspects, as well as professional support that can help to increase the family members’ awareness of their own needs, in line with previous research of Contreras et al.3 Based on the above, it is essential to increase the awareness of family members adaptive coping strategies during different phases of YOD.
According to Contreras et al,3 family members experience caring for persons with dementia as stressful, burdensome, and isolating. This is in accordance with our findings as family members in our study described powerlessness as they were unable to influence various decisions and disease progression. Another aspect was the relative’s gradual inability to share responsibilities with the family member, adding to the burden especially among persons feeling isolated due to their relative’s diagnosis. It became clear that family members needed guidance throughout the disease trajectory and someone to share the responsibility with.
Previous research also shows that as the disease progresses, family members are faced with new challenges and are compelled to make decisions, despite feeling insecure.19 Based on our findings, we also argue that taking over responsibility from the relative and becoming the main decision-maker was experienced as overwhelming. Shanley et al20 suggest that family members are not prepared to make decisions on behalf of the relative and emphasize the importance of support/interventions early during the disease trajectory. They also point out the need of care professionals to be active in guiding family members throughout the disease trajectory and help plan and prepare for the future. Consistent with previous research,2 the decision to relocate the relative to a nursing home was described as the toughest decision the family members had to make. In the interviews, the family members described that they constantly had to make decisions on behalf of their relative; however, the decision to relocate was clearly defined as the most difficult decision by all. One reason for this might be that this was a decision closely related to a great level of guilt and feelings of having abandoned the relative. Contreras et al3 report that lack of sufficient support at the beginning of the disease trajectory causes unmet needs that may lead to difficulties later. Our findings emphasize the need of educational interventions that would increase awareness about YOD among social care workers and other healthcare professionals outside of specialized memory clinics.
The findings show that being responsible for a relative with YOD, differed depending on the relationship, as did daily life for family members who were cohabitants compared to adult children or siblings. Still, adult children and siblings also described a drastic impact and a change in roles when they were forced to take on responsibilities such as care and wellbeing of their relative. None of the adult children in our study had been living together with their parent at onset of symptoms, nevertheless it is important to acknowledge that children of a person with YOD may put off moving out/away due to the parent’s need of support. However, previous research shows that family members who are not considered to be the primary caregiver often experience that healthcare professionals do not address their specific needs.21 All family members described pushing their own needs aside as they needed to constantly focus on the needs of the relative. Our findings are in line with Clemmensen et al,19 as they reported that family caregivers, regardless of relation to the relative focused on the needs of the person with dementia, suggesting that family members were only able to recognize their own needs in retrospect. This emphasizes the importance of further education and research on how to support family members to persons with YOD throughout the entire disease trajectory.
Strengths, Limitations, and Future Directions
A strength in the present study design is that different family members were included and not only family members as primary caregivers. In addition, the cause of YOD differed: Alzheimer’s disease, frontotemporal dementia and Wernicke-Korsakoff’s syndrome. Combined this provided a possibility for a holistic description of family members’ experiences of living close to a person with YOD. Another strength was the design to follow-up with a second interview, as it made it possible to ask additional questions and clarify uncertainties from the first interview.
Family members of persons with YOD have specific needs. Still, our findings may be transferable to other settings and groups, such as family caregivers of persons with late-onset dementia (LOD). The experiences of social consequences may also be transferable to younger family members of persons with other types of neurodegenerative disorders.
One limitation was the heterogeneity in our sample. Only three siblings and adult children participated. This may affect the trustworthiness of the results regarding potential differences between partners, siblings, and adult children. Previous research shows that there is a difference between the level of strain, distress, and perceived control, when comparing family caregivers of persons with Alzheimer’s disease and frontotemporal dementia.22 There are some studies focusing on the experiences of spouses/caregivers of persons with young-onset frontotemporal dementia23 and Alzheimer’s disease.24 However, there is a need of further research focusing on the needs of specific groups of family members and how their needs vary, for example depending on their relationship and type of dementia. In addition, social care workers and health care professionals outside the memory clinic settings play an important role in providing care and support for family members throughout the disease trajectory. Because of this, research should also focus on increased level of awareness and responsiveness to specific needs in YOD.
Conclusion
Our findings emphasize the need to increase education, understanding and awareness of family members' specific needs when living close to a relative with YOD. In order to support and empower family members, it is necessary to provide guidance throughout the disease trajectory. Such guidance and support have to be tailored to individual needs and provided by professionals with knowledge about YOD. Healthcare professionals need to understand what mechanisms family members use as strategies to cope. Therefore, educational interventions are of importance as it increases the understanding of what these family members need.
Abbreviations
YOD, young-onset dementia; AD, Alzheimer’s disease; FTD, Frontotemporal dementia; WKS, Wernicke-Korsakoff’s syndrome; LOD, Late-onset dementia.
Acknowledgments
The authors would like to thank all family members for sharing their personal experiences. Further, the authors wish to thank professor Åke Seiger for providing comments on the manuscript.
Funding
Funding for this study was received from Swedish Research Council, Alzheimerfonden, Center for Innovative Medicine (CIMED) at Karolinska Institutet South Campus, Stiftelsen Stockholms Sjukhem (Sweden), Hjärnfonden, Region Stockholm (ALF), Swedish Research Council for Health, Working Life and Welfare (FORTE).
Disclosure
The authors declare no conflicts of interest with respect to the research, authorship and/or publication of this article.
References
1. Hendriks S, Peetoom K, Bakker C, et al. Global prevalence of young-onset dementia: a systematic review and meta-analysis. JAMA Neurol. 2021;78(9):1080–1090. doi:10.1001/jamaneurol.2021.2161
2. Cabote CJ, Bramble M, McCann D. Family caregivers’ experiences of caring for a relative with younger onset dementia: a qualitative systematic review. J Fam Nurs. 2015;21(3):443–468. doi:10.1177/1074840715573870
3. Contreras M, Mioshi E, Kishita N. What are the educational and support needs of family carers looking after someone in the early stages of Alzheimer’s disease? A qualitative retrospective approach. Health Soc Care Community. 2022;30(5):1726–1734. doi:10.1111/hsc.13552
4. Bakker C, de Vugt ME, van Vliet D, et al. The use of formal and informal care in early onset dementia: results from the NeedYD study. Am J Geriatr Psychiatry. 2013;21(1):37–45. doi:10.1016/j.jagp.2012.10.004
5. Arai A, Matsumoto T, Ikeda M, Arai Y. Do family caregivers perceive more difficulty when they look after patients with early onset dementia compared to those with late onset dementia? Int J Geriatr Psychiatry. 2007;22(12):1255–1261. doi:10.1002/gps.1935
6. Bakker C, de Vugt ME, van Vliet D, et al. Predictors of the time to institutionalization in young- versus late-onset dementia: results from the Needs in Young Onset Dementia (NeedYD) study. J Am Med Dir Assoc. 2013;14(4):248–253. doi:10.1016/j.jamda.2012.09.011
7. Koopmans RTCM, van der Steen JT, Bakker C. Palliative care in people with Young-Onset Dementia (YOD): an Undiscovered Area! J Am Med Dir Assoc. 2015;16(12):1008–1009. doi:10.1016/j.jamda.2015.07.001
8. Gibson AK, Anderson KA, Acocks S. Exploring the service and support needs of families with early-onset Alzheimer’s disease. Am J Alzheimers Dis Other Demen. 2014;29(7):596–600. doi:10.1177/1533317514558160
9. Bakker C, de Vugt ME, van Vliet D, et al. Unmet needs and health-related quality of life in young-onset dementia. Am J Geriatr Psychiatry. 2014;22(11):1121–1130. doi:10.1016/j.jagp.2013.02.006
10. van Vliet D, de Vugt ME, Bakker C, Koopmans RTCM, Verhey FRJ. Impact of early onset dementia on caregivers: a review. Int J Geriatr Psychiatry. 2010;25(11):1091–1100. doi:10.1002/gps.2439
11. Bannon S, Reichman M, Popok P, et al. In it together: a qualitative meta-synthesis of common and unique psychosocial stressors and adaptive coping strategies of persons with young-onset dementia and their caregivers. Gerontologist. 2022;62(2):123–139. doi:10.1093/geront/gnaa169
12. Gilhooly KJ, Gilhooly ML, Sullivan MP, et al. A meta-review of stress, coping and interventions in dementia and dementia caregiving. BMC Geriatr. 2016;16(1):1–8. doi:10.1186/s12877-016-0280-8
13. Monteiro AMF, Santos RL, Kimura N, Baptista MAT, Dourado MCN. Coping strategies among caregivers of people with Alzheimer disease: a systematic review. Trends Psychiatry Psychother. 2018;40(3):258–268. doi:10.1590/2237-6089-2017-0065
14. Flynn R, Mulcahy H. Early-onset dementia: the impact on family care-givers. Br J Community Nurs. 2013;18(12):598–606. doi:10.12968/bjcn.2013.18.12.598
15. Millenaar JK, Bakker C, Koopmans RT, Verhey FR, Kurz A, de Vugt ME. The care needs and experiences with the use of services of people with young-onset dementia and their caregivers: a systematic review. Int J Geriatr Psychiatry. 2016;31(12):1261–1276. doi:10.1002/gps.4502
16. Sansoni J, Duncan C, Grootemaat P, Capell J, Samsa P, Westera A. Younger onset dementia: a review of the literature to inform service development. Am J Alzheimers Dis Other Demen. 2016;31(8):693–705. doi:10.1177/1533317515619481
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
19. Clemmensen TH, Lauridsen HH, Andersen‐Ranberg K, Kristensen HK. ‘I know his needs better than my own’ – carers’ support needs when caring for a person with dementia. Scand J Caring Sci. 2021;35(2):586–599. doi:10.1111/scs.12875
20. Shanley C, Fetherstonhaugh D, McAuliffe L, Bauer M, Beattie E. Providing support to surrogate decision-makers for people living with dementia: healthcare professional, organisational and community responsibilities. Health Soc Care Community. 2017;25(5):1563–1570. doi:10.1111/hsc.12456
21. Wiggins M, McEwen A, Sexton A. Young-onset dementia: a systematic review of the psychological and social impact on relatives. Patient Educ Couns. 2023;107:107585. doi:10.1016/j.pec.2022.107585
22. Wong C, Merrilees J, Ketelle R, Barton C, Wallhagen M, Miller B. The experience of caregiving: differences between behavioral variant of frontotemporal dementia and Alzheimer disease. Am J Geriatr Psychiatry. 2012;20(8):724–728. doi:10.1097/JGP.0b013e318233154d
23. Johannessen A, Helvik AS, Engedal K, Thorsen K. Experiences and needs of spouses of persons with young-onset frontotemporal lobe dementia during the progression of the disease. Scand J Caring Sci. 2017;31(4):779–788. doi:10.1111/scs.12397
24. Bergman M, Graff C, Eriksdotter M, Fugl-Meyer KS, Schuster M. The meaning of living close to a person with Alzheimer disease. Med Health Care Philos. 2016;19(3):341–349. doi:10.1007/s11019-016-9696-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.