Back to Journals » Patient Preference and Adherence » Volume 20
Family Function and Self-Management in Glaucoma Patients: Chain Mediation of Psychological Capital and Coping Style
Authors Liu Y, Zhang J, Zhang Q, Sa R ![]() , Xu H
, Xu H
Received 14 January 2026
Accepted for publication 29 April 2026
Published 25 May 2026 Volume 2026:20 591763
DOI https://doi.org/10.2147/PPA.S591763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Yu Liu,1 Jingjing Zhang,1 Qian Zhang,2 Rina Sa,1 Haiyang Xu3
1Department of Ophthalmology, The First Hospital of Jilin University, Changchun, People’s Republic of China; 2Ward 3 of Neurosurgery, The First Affiliated Hospital of Military Medical University, Xi’an, People’s Republic of China; 3Department of Anesthesia, The First Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Haiyang Xu, Department of Anesthesia, The First Hospital of Jilin University, Xinmin Dajie, Chaoyang District, Changchun, Jilin, People’s Republic of China, Tel +8615804303312, Fax +0431-81875567, Email [email protected]
Purpose: Glaucoma is an irreversible blinding disease, and patients’ self-management ability directly influences both disease progression and quality of life. We aimed to study the relationship between family functioning and patient self-management behaviors, and mediating roles of psychological capital and coping styles.
Patients and Methods: Drawing from the theory of personal and family self-management, the present cross-sectional study proposed a conceptual model to assess the influence of family functioning on self-management behaviors in patients with glaucoma. The mediating effects of psychological capital and coping styles were also explored. We recruited 336 patients to participate in this study. A relational model was constructed using structural equation modeling, and bootstrap analyses were conducted to assess the mediation effects.
Results: A strong positive link was identified between family functioning and self-management behaviors (r = 0.506, P < 0.01). Psychological capital and positive coping styles showed significant mediating effects, with effect sizes of 0.198 and 0.151, which represented 35.04% and 26.73% of the total effect, respectively. Furthermore, the combined chain mediating effect of these two variables was 0.049, representing 8.67% of the total effect.
Conclusion: Family functioning not only has a direct impact on self-management but also indirectly enhances the self-management capacity of glaucoma patients through psychological capital and positive coping styles. The findings implicated that a family-centered approach should be adopted to place family functioning in a central role to improve the psychological resources and promote adoption of positive coping mechanisms, ultimately leading to better self-management outcomes in glaucoma patients.
Keywords: family functioning, psychological capital, coping style, self-management
Introduction
Glaucoma is a chronic eye disease characterized by progressive deterioration of the optic nerve, which ultimately results in irreversible loss of visual fields.1 As the second leading cause of irreversible blindness globally, glaucoma threatens individual autonomy and presents a substantial burden to the public healthcare systems.2,3 Effective self-management, including medication adherence, routine follow-ups, symptom monitoring, and adaptation to the psychosocial challenges of chronic disease, is essential to delay disease progression and preserve visual function and quality of life in these patients.4–6 However, many glaucoma patients demonstrate poor self-management due to insufficient disease knowledge, complex medical treatment, low self-efficacy, difficulties associated with adapting to visual impairments, and misbelief regarding unavoidable vision loss.7–11 Despite increasing recognition of these challenges, the psychosocial mechanisms underlying self-management in glaucoma remain insufficiently understood.
Research Gap
While the importance of self-management is well-documented, a significant gap remains in understanding the psychosocial mechanisms that drive these behaviors in glaucoma patients. Existing literatures have established that family support is beneficial and effective family functioning, the collective ability of a family to mobilize material resources and provide emotional and informational support, can affect patient emotional state and behavioral responses, facilitating adaptive psychological outcomes and health-related behaviors in patients.12–16 However, there were significant gaps in understanding the impact of family functioning on self-management efficacy in glaucoma patients, especially the potential mediators linking family functioning to patient self-management. All of these warrant further investigations.
Application of Personal and Family Self-Management Theory
The personal and family self-management theory (PFSMT) is a theoretical structure that integrates and builds upon earlier studies concerning self-management at both individual and family levels, emphasizing the practices of individuals, dyadic relationships, and family systems.12 The theory is structured around three fundamental components, namely context, process, and outcome, and illustrates how individual, contextual, and environmental factors contribute to the formation of self-management abilities, which subsequently affect health behaviors and long-term outcomes.
Glaucoma management could be particularly suitable for application of PFSMT since its control depends not only on individual motivation but also on family support and sustained behavioral regulation. Within the PFSMT framework, family functioning represents a contextual resource; psychological capital (hope, resilience, optimism, self-efficacy) and coping styles function as process-level mechanisms;17 and self-management constitutes the behavioral outcomes. Application of PFSMT could enable a structured and theory-driven examination of how family-level influences translate into individual behavioral outcomes in glaucoma management.
Psychological Capital and Coping Styles in Chain Mediation Pathway
Psychological capital has been consistently associated with improved health behaviors in chronic disease management.18–20 Families with high levels of functioning can foster psychological capital among their members through sustained emotional support and effective communication. This enhanced psychological capital contributes to reduced psychological distress, improved mental well-being, and ultimately, strengthened self-management capacity.21–24
Coping styles represent concrete behavioral and cognitive response to illness-related stress. Adaptive coping facilitates treatment adherence and emotional adjustment, whereas maladaptive coping undermines self-management efforts.25 Empirical evidence indicates a strong association between coping styles and patients’ self-management capacity.26,27
Family functioning may shape self-management by enhancing psychological capital, which in turn impact coping styles.28 Psychological capital and coping styles are key internal resources for management illness-related stress. Psychological capital may influence the selection and effectiveness of coping styles.29 Patients with stronger psychological resources are more likely to adopt active and problem-focused coping behaviors,19 ultimately enhancing their capacity for effective self-management.30 Coping style may represent a downstream behavioral manifestation of psychological capital. Understanding this chain mediation pathway allows for a more comprehensive understanding than merely examining each mediator separately.
Conceptual Framework Development
Drawing upon the proven efficacy of PFSMT in chronic disease management, this study adopted the framework by defining family functioning as the contextual factor, psychological capital and coping styles as the process variables, and self-management as the resulting outcome. We investigated how family functioning, psychological capital, and coping styles affect self-management in glaucoma patients using structural equation modeling. Our hypotheses were:
H1: Family functioning directly and positively influences self-management. H2: Psychological capital is an independent mediator in the correlation between family functioning and self-management. H3: Coping style independently mediates the link between family functioning and self-management. H4: Psychological capital and coping style collectively serve as sequential mediators in the link between family functioning and self-management.
Building on these hypotheses, a preliminary theoretical framework has been developed (Figure 1).
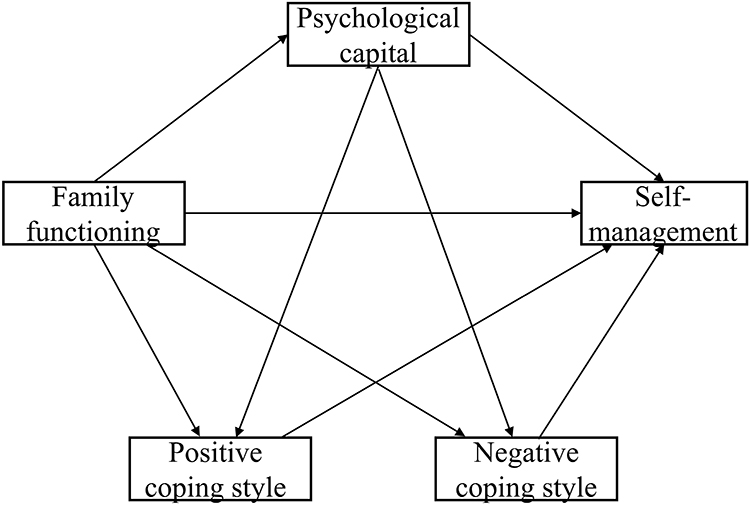 |
Figure 1 Assumed structural equation model. |
Materials and Methods
Data Origins
Glaucoma patients participated in a cross-sectional study at the Department of Ophthalmology, First Hospital of Jilin University, China, using convenience sampling. The inclusion criteria were as follows: (1) patients diagnosed with glaucoma; (2) those who had undergone medical, surgical, or laser interventions; (3) those aged ≥18 years; and (4) those with adequate comprehension and communication skills. The exclusion criteria were as follows: (1) patients with other acute or chronic ocular conditions; (2) those with coexisting severe physical illnesses; and (3) those diagnosed with additional mental health disorders. The survey was administered via an online platform with all scale items set as mandatory. Participants could not submit the questionnaire unless every item was answered. Consequently, no item-level missing data were present in the collected questionnaires. Of the 355 initial questionnaires, 19 (5.35%) were excluded due to straight-lining responses (n = 7), logical contradictions (n = 6), or completion time < 1 minute (n = 6). The final valid sample consisted of 336 responses (effective response rate = 94.65%). Since there was no missing value in the valid cases, no imputation was performed. The subsequent principal component analysis was conducted on the complete dataset (N=336). In line with Kendall’s guidelines,31 the recommended participant count is typically calculated as 5–10 participants for each independent variable. This study incorporated 21 independent variables in total, consisting of 7 participant characteristics, 5 dimensions of family functioning, 4 dimensions of psychological capital, 3 dimensions of self-management, and both positive and negative coping styles. Based on this calculation, the estimated required sample size is 105 to 210 participants. Considering a potential 20% invalid response rate, the required number of participants becomes 126 to 252. Therefore, our sample size fulfills the study’s criteria.
Investigation Instruments
The study participants were glaucoma patients. Most of whom had varying degrees of visual impairment. To ensure data quality and response authenticity, we adopted the following measures, including 1) all scale items were kept in their original format without any adaptation; 2) patients with mild visual impairment were allowed to use the device’s built-in zoom function or screen reader to complete the questionnaire independently; 3) for patients with severe visual impairment or those unable to read the screen, family members, caregivers, or research assistants would assist them, including operating the electronic device and reading the items aloud line by line. The patients responded orally. The family members, caregivers, and research assistants were instructed not to interfere with patient’s independent response but only selected the answers based on patient responses. This approach respected the patients’ autonomous responses while minimizing the impact of visual impairment on data collection.
Family Function Scale
The Family Care Index Scale, created by Smilkstein,32 was used to evaluate the family functioning of participants. The scale comprised five key aspects: adaptation, partnership, growth, affection, and resolve. Each dimension is assessed through a single item, measured using a 3-point Likert scale from 0 to 2, with higher scores suggesting increased degrees of family functioning. The scale is simple to administer and offers a consistent measure reflecting a person’s view of their family functioning. The scale showed a Cronbach’s α value of 0.884 in this study, indicating a high level of internal consistency. This suggests that the items within the scale reliably measure aspects of family function in the study population.
Psychological Capital Scale
Psychological capital was assessed using the Chinese Psychological Capital Questionnaire.33 This questionnaire comprises four core elements: self-efficacy, hope, resilience, and optimism. It uses a 7-point Likert scale, with 1 indicating “not at all” and 7 representing “totally.” Items with negative wording were reverse scored, and the average score across all responses was subsequently computed. Elevated scores indicate greater psychological capital. In the present research, the Cronbach’s α coefficients for both the whole questionnaire and its individual dimensions ranged from 0.905 to 0.976, indicating excellent internal consistency. These high values suggest that the questionnaire and its subscales reliably assess psychological capital among the participants.
Coping Style Scale
The Simple Coping Style Questionnaire, designed by Xie34 based on the characteristics of Chinese individuals, was used to measure coping styles. The scale includes two categories of coping styles: 12 styles for positive coping and 8 styles for negative coping. Each item is measured using a 4-point Likert scale from 1 (never used) to 4 (frequently used). Higher scores on the positive coping dimension suggest a more adaptive approach to coping, whereas higher scores on the negative dimension imply a less effective, maladaptive style. In the present study, the overall Cronbach’s α coefficient was 0.830, with values of 0.882 and 0.765 for the positive and negative coping subscales, respectively. These results indicate good internal consistency for the total scale, with particularly strong reliability for the positive coping dimension and acceptable reliability for the negative coping dimension.
Self-Management Scale
The Glaucoma Patient Self-Management Behavior Questionnaire, designed by Wu,35 was used to assess the self-management skills of participants. This tool evaluates three critical aspects: life adjustment, promotion of physical function, and medical management of glaucoma. Each item is evaluated using a 4-point Likert scale, extending from 1 (not at all) to 4 (completely achievable), where elevated scores represent a greater ability of self-management. In this research, the Cronbach’s α for the scale was 0.918, showing strong internal consistency. This suggests that the items within the scale reliably measure self-management behaviors among glaucoma patients.
Statistical Analysis
Data were analyzed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and Amos 26.0 (IBM Corp.), with the significance threshold set at 0.05. Initial examination involved descriptive statistics (percentages, means, and standard deviations) to evaluate participants’ demographics and their performance across variables like family functioning, psychological capital, coping styles, and self-management. Then, Pearson correlation analysis was performed to investigate the interactions among these variables. Thereafter, structural equation modeling using Amos was performed to analyze the mediating roles of psychological capital and coping styles, including the investigation of their chain mediation effect within the model. The Bootstrap method was used to evaluate the significance of the mediating effects, with 5000 resamples used for validation. A 95% confidence interval (CI) excluding zero was considered to indicate a statistically significant mediating effect. Common method bias was assessed using Harman’s single-factor test based on an unrotated principal component analysis. To evaluate the measurement model, confirmatory factor analysis (CFA) was conducted for the latent constructs, including family functioning, psychological capital, and self-management. Internal consistency was assessed using Cronbach’s α and composite reliability (CR). Convergent validity was evaluated based on the average variance extracted (AVE), and discriminant validity was examined using the Fornell–Larcker criterion. Positive coping was treated as an observed variable using the total score of the corresponding subscale, rather than as a latent construct, to maintain model parsimony. Therefore, item-level CFA indices (eg, factor loadings, CR, and AVE) were not estimated for this variable.
Results
Patient Demographics
The research comprised 336 glaucoma patients, including 154 males (45.83%) and 182 females (54.17%). Among them, 160 (47.62%) were aged below 60 years, 213 (63.39%) had attained a college-level education or lower, and 223 (66.37%) had a personal monthly income of less than 5000 yuan. In addition, 217 (64.58%) of the respondents lived with their families. Notably, 132 (39.29%) were classified as having moderate-stage glaucoma, with 138 (41.07%) having a disease duration of 1–5 years. Table 1 summarizes demographic and clinical characteristics in detail.
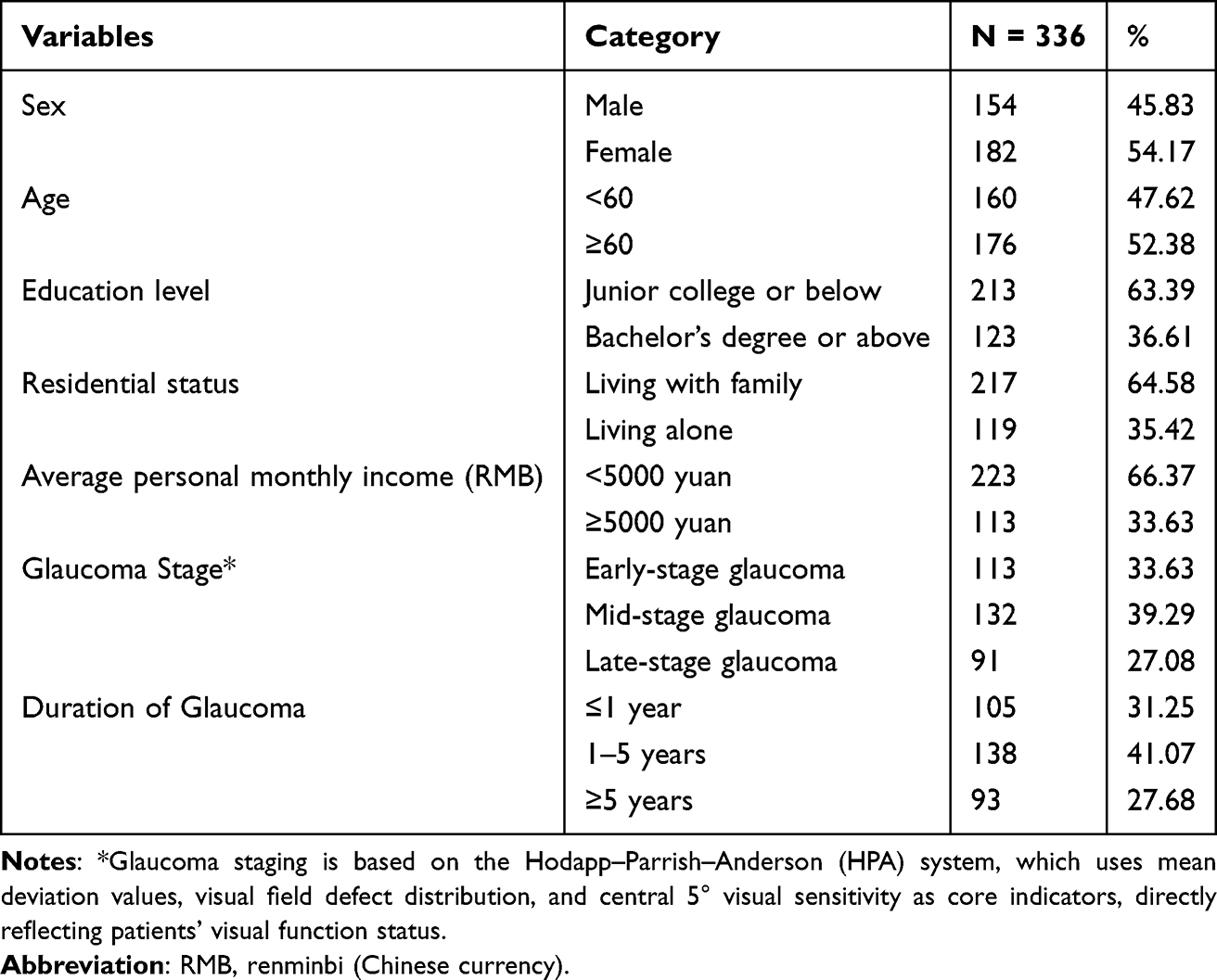 |
Table 1 Demographics of Glaucoma Patients (N=336) |
To assess potential common method bias, Harman’s single-factor test was conducted. The results indicated that multiple factors with eigenvalues greater than 1 were extracted, and the first factor accounted for 34.42% of the total variance, below the commonly accepted threshold of 40% (Table 2). These findings suggested that common method bias was unlikely to be a serious concern in this study, although it could not be completely ruled out.
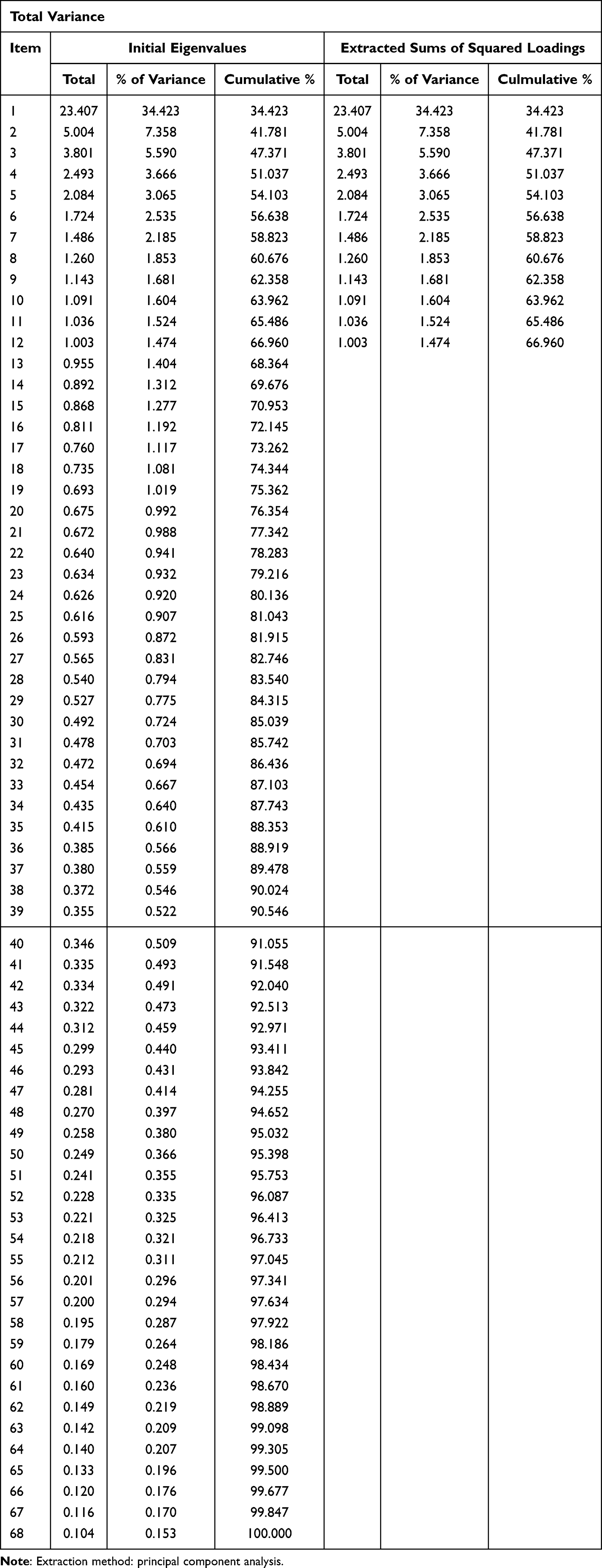 |
Table 2 Harman’s Single-Factor Test to Assess Potential Common Method Bias |
Measurement Model Evaluation
The measurement model demonstrated satisfactory reliability and validity (Table 3). All standardized factor loadings ranged from 0.724 to 0.929, exceeding the recommended threshold of 0.70.
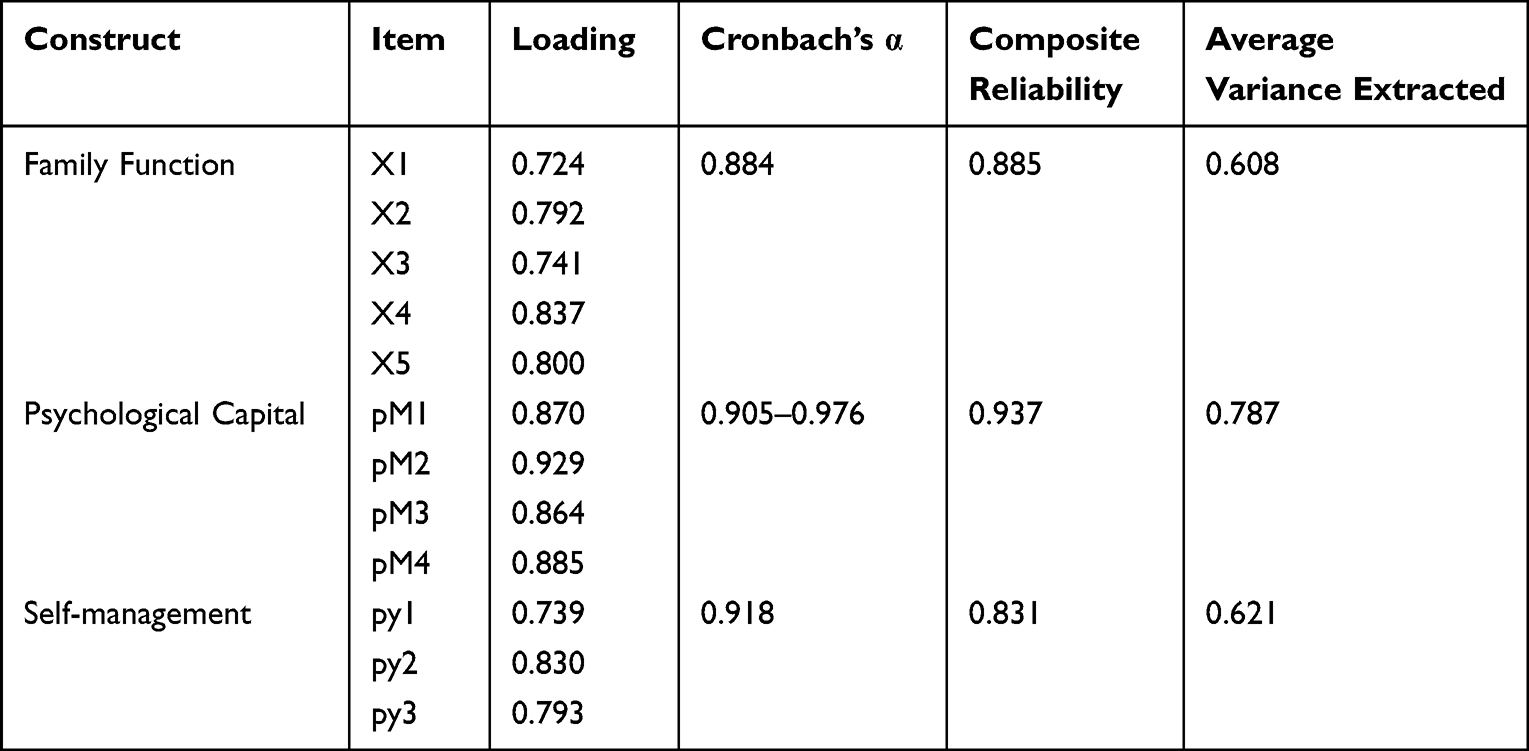 |
Table 3 Measurement Model Results |
Cronbach’s α values for all constructs were above 0.80, indicating good internal consistency. CR values ranged from 0.831 to 0.937, exceeding the recommended threshold of 0.70. The AVE values ranged from 0.608 to 0.787, all above the recommended threshold of 0.50, indicating satisfactory convergent validity. The square roots of AVE for each construct were greater than the corresponding inter-construct correlations, suggesting adequate discriminant validity (Table 4). Positive coping was entered into the structural model as an observed composite variable. Therefore, CFA-based indices (eg, factor loadings, CR, and AVE) were not estimated for this construct.
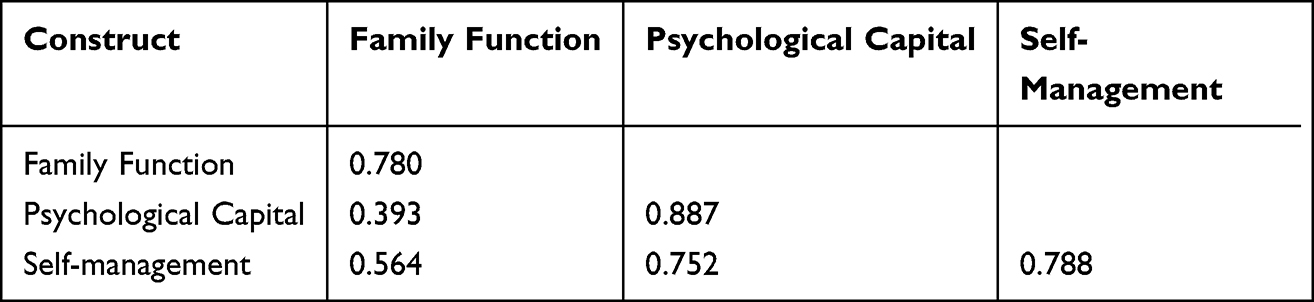 |
Table 4 Discriminant Validity Assessed Using the Fornell–Larcker Criterion |
Correlation Analysis
Descriptive statistics and Pearson correlation coefficients for all key investigated factors are shown in Table 5. Self-management showed significant positive correlations with family functioning (r = 0.506, P < 0.01), psychological capital (r = 0.681, P < 0.01), and positive coping styles (r = 0.656, P < 0.01) and a strong inverse relationship with negative coping styles (r = –0.169, P < 0.01). Family functioning was strongly positively linked to psychological capital (r = 0.359, P < 0.01) and positive coping styles (r = 0.563, P < 0.01) and significantly negatively associated with negative coping styles (r = –0.157, P < 0.01). Psychological capital showed a significant positive correlation with positive coping styles (r = 0.527, P < 0.01) but a reverse correlation with negative coping styles (r = –0.116, P < 0.05).
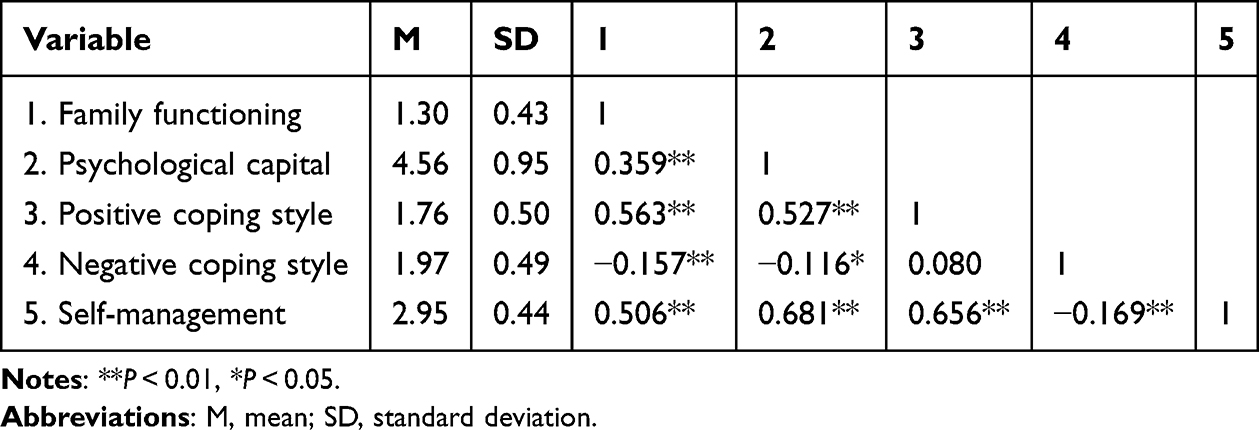 |
Table 5 Descriptive Statistics and Correlations of the Main Variables |
Structural Equation Modeling
An initial structural equation model was specified according to the proposed theoretical framework. To control for the confounding effects of visual function on core variables, this study incorporated Hodapp-Parrish-Anderson (HPA) glaucoma classification as a control variable into the structural equation model, correcting for differences in visual function among patients with early, moderate, and severe glaucoma. Positive coping was included in the structural model as an observed variable. The confirmatory factor analysis results showed that the model fit appropriately, as evidenced by the following fit indices: GFI = 0.90, NFI = 0.92, IFI = 0.94, TLI = 0.92, CFI = 0.94, RMSEA = 0.09, and SRMR = 0.044. However, the path coefficients from family functioning to negative coping styles (P = 0.06) and from psychological capital to negative coping styles (P = 0.32) did not reach statistical significance and were subsequently excluded from the final model. The revised model, as shown in Figure 2, showed strengthened fit indices (GFI = 0.903, NFI = 0.93, IFI = 0.94, TLI = 0.93, CFI = 0.94, and RMSEA = 0.09), indicating an acceptable overall model fit. All retained factor loadings and path coefficients reached statistical significance, confirming the adequacy of the final model specification.
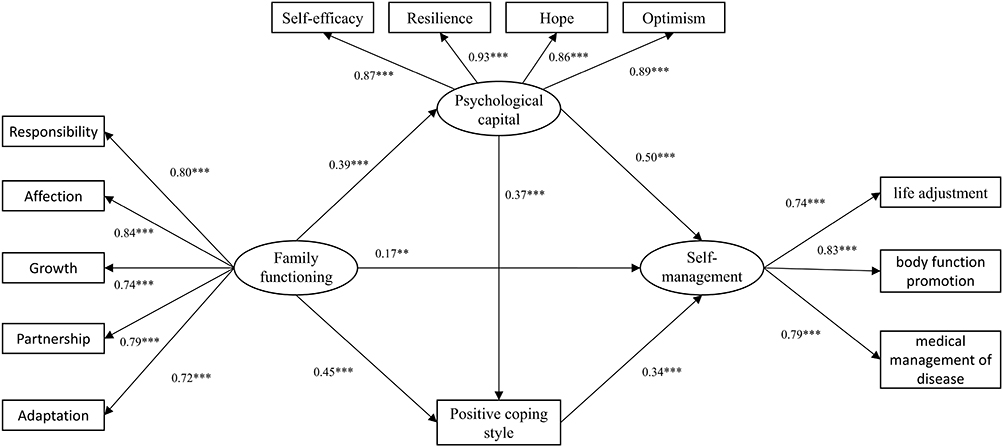 |
Figure 2 Final model with standardized path coefficients and statistical significance indicators. |
As shown in Table 6, the final structural model (SRMR = 0.041) revealed notably positive associations between self-management and family functioning (standardized β = 0.167, P < 0.01), psychological capital (β = 0.502, P < 0.001), and positive coping styles (β = 0.335, P < 0.001). Furthermore, family functioning was positively associated with psychological capital (β = 0.393, P < 0.001) and positive coping styles (β = 0.450, P < 0.001). Furthermore, psychological capital was markedly and positively associated with positive coping styles (β = 0.372, P < 0.001).
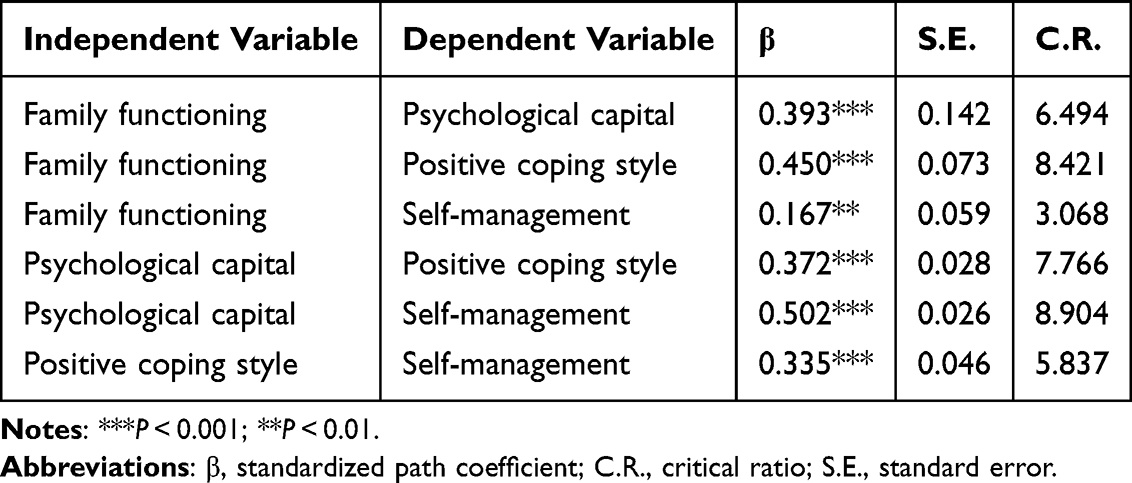 |
Table 6 Path Coefficient Test for the Final SEM Model |
The mediating effects were evaluated using the bias-corrected percentile bootstrap approach with 5000 resamples. Table 7 shows that the direct effect of family functioning on self-management was statistically significant [β = 0.167, 95% CI (0.042, 0.293), P < 0.01], constituting 29.56% of the total effect. Both psychological capital [indirect effect = 0.198, 95% CI (0.123, 0.293), P < 0.001] and positive coping styles [indirect effect = 0.151, 95% CI (0.080, 0.235), P < 0.001] emerged as significant mediators in the connection between family functioning and self-management, representing 35.04% and 26.73% of the total effect, respectively. Moreover, a significant sequential mediating effect through psychological capital and positive coping styles was detected [indirect effect = 0.049, 95% CI (0.025, 0.087), P < 0.001], explaining 8.67% of the total effect.
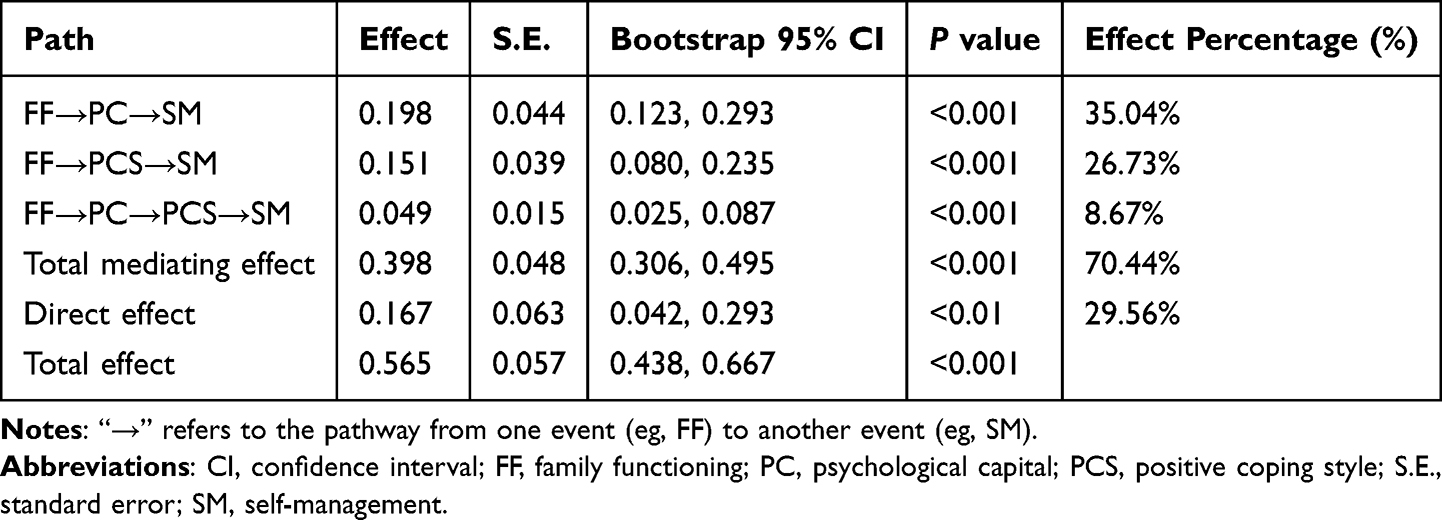 |
Table 7 Mediator Effect and Magnitude of Effect |
Discussion
Anchored in the personal and family self-management theory, this study investigates the multifaceted mechanisms influencing self-management among glaucoma patients by developing a theoretical model that integrates contextual factors (family functioning), process variables (psychological capital and coping styles), and outcome measures (self-management). The results show that family functioning, psychological capital, and positive coping styles are significant positive predictors of self-management, whereas adverse coping styles are inversely associated with self-management. Furthermore, the association between family functioning and self-management is mediated by psychological capital and positive coping styles, which also operate as sequential mediators within this relational pathway. These findings highlight the critical role of strengthening family functioning, cultivating psychological capital, and enhancing positive coping styles in effectively promoting self-management in individuals with glaucoma.
First, consistent with prior empirical evidence, glaucoma patients reporting higher levels of family functioning showed significantly enhanced self-management behaviors, thus providing support for Hypothesis 1.8 The ecological systems theory offers a theoretical foundation for this finding; it posits that individual behavior is influenced by multiple nested environmental contexts, including the microsystem (eg, family), mesosystem, exosystem, and macrosystem.36 As a fundamental element of the microsystem, the family may play a pivotal role in promoting self-management through two key pathways: by providing emotional support, which alleviates disease-related stress and strengthens coping capacity, and by assisting in the formulation of problem-solving styles, which enhance the efficacy of daily disease management practices. Therefore, by establishing a model of collaborative management between the individual and the family, families with high levels of functioning can transform individualized disease management into a collective practice within the family health community, ultimately achieving effective glaucoma control.
The study showed that psychological capital mediates the connection between family functioning and self-management, validating the accuracy of Hypothesis 2. This relationship can be interpreted through the framework of social cognitive theory, which posits that an individual’s external environment (eg, family functioning), internal psychological resources (eg, psychological capital), and behaviors (eg, self-management) mutually influence one another.37 High-functioning families are characterized by strong emotional connections and open communication among members, which create a supportive environment conducive to psychological well-being and consequently facilitate the development of psychological capital in family members. People with higher psychological capital often show increased optimism and hope for the future, along with a strong sense of self-efficacy. They show greater confidence in their ability to regulate intraocular pressure and adhere to treatment regimens; furthermore, they exhibit greater motivation and determination in managing their condition. These findings further reinforce prior evidence indicating that well-functioning families contribute to the enhancement of individuals’ psychological capital, which in turn facilitates more effective self-management.19
This study also identified that coping styles mediate the connection between family functioning and self-management, thus supporting Hypothesis 3. Notably, family functioning was found to be strongly linked to the adoption of positive coping approaches; however, its relationship with negative coping styles did not reach statistical significance. Members of well-functioning families are more inclined to provide emotional and instrumental support, which facilitates glaucoma patients’ comprehension of their health condition and enhances their awareness of effective health management styles. This supportive environment fosters a positive outlook, encouraging patients to adopt constructive coping styles when facing challenges associated with their condition.8 This positive coping style facilitates the enhancement of self-management capabilities by strengthening patients’ emotional regulation and behavioral control, ultimately contributing to improved well-being and long-lasting medical benefits in glaucoma patients.38 Accordingly, the use of positive coping styles further reinforces the positive impact of family functioning on self-management in individuals with glaucoma. The negative coping style refers to maladaptive strategies, such as skipping appointment, ignoring symptoms, or substance use, used by patients and family members to manage stress and pressure from illness. Our current analysis did not show a statistically significant correlation between family functioning and negative coping styles. However, the small P value (0.06) could still suggest that further investigations are required, such as in a large sample of patients or stratified analysis in each item of these 8 negative coping styles.
We further identified psychological capital and positive coping styles as sequential mediators in the pathway linking family functioning to self-management, thus offering empirical support for Hypothesis 4. A plausible explanatory mechanism is that in families exhibiting high levels of functional cohesion, harmonious interpersonal dynamics and effective collaborative problem-solving significantly contribute to the development and reinforcement of the patient’s psychological capital.39 Subsequently, the enhanced psychological capital endows patients with greater psychological resilience to confront illness-related challenges. Psychological capital not only strengthens patients’ capacity to navigate adversity but also encourages a cognitive reappraisal of difficulties as opportunities for personal development, thus facilitating the adoption of positive coping styles. Components of psychological capital, including hope, self-efficacy, resilience, and optimism, can facilitate positive coping by providing patients with the motivation, confidence, and emotional resource to manage health challenges. Hope enables goal-directed planning and creative problems-solving ability. Self-efficacy fosters confidence in performing health behaviors. Resilience helps patients recover from illness. Optimism encourages proactive actions in patients. Positive coping behaviors further contribute to the strengthening of patients’ self-management capacities through positive feedback mechanisms, ultimately fostering a virtuous cycle of “family support → psychological resources → behavioral adaptation → health benefits.”
The findings of this study offer strong theoretical backing for enhancing self-management skills in glaucoma patients. First, the research emphasizes the role of family functioning in patients’ self-management behaviors, revealing that family support delivers both emotional encouragement and hands-on help, which boosts the patient’s disease management in daily routines. This finding further confirms the important role of the family as an external resource in health behavior decision-making, helping to improve the application framework of social support theory in chronic disease management. Second, this study highlights the contribution of psychological capital to self-management. Psychological capital enhances patients’ self-efficacy and intrinsic motivation, while also helping them develop more positive disease cognition and attitudes. This enables patients to be more resilient and adaptive when faced with disease recurrence or treatment challenges. This finding provides a theoretical basis for further exploration of how internal psychological resources affect health behaviors and underscores the unique value of the “positive psychology” perspective in chronic disease management research. In addition, the study points out the significance of positive coping approaches in facilitating psychological stability and behavioral discipline, suggesting that emotional and behavioral management abilities are key to achieving efficient self-management. This provides new empirical support for the construction of the “cognitive–emotional–behavioral” chain in the health behavior theory, enriching the understanding of individual self-regulation mechanisms in the management of persistent medical conditions. In conclusion, this research not only deepens the theoretical understanding of how the family, psychological factors, and behavioral factors interact to influence patients’ self-management behaviors but also provides an important foundation for future exploration of multi-factorial mechanisms and the development of integrated intervention models.
Notwithstanding its contributions, there are a few noteworthy limitations of this study that warrant attention. First, glaucoma patients were selected solely from a single hospital in the Jilin Province, which introduces a strong regional limitation. This may prevent the findings from fully reflecting the overall characteristics and behavioral patterns of glaucoma patients throughout the nation. Therefore, future studies should consider incorporating a more comprehensive, multi-center sampling approach that includes various regions and medical institutions to confirm that the findings are applicable across a wider demographic. Second, the research implemented a cross-sectional methodology, capturing data at a single moment. Such a design hinders in-depth analysis of cause-and-effect relationships and variable progression over time. For a clearer view of the cause-and-effect pathways among variables, future investigations should implement longitudinal designs to monitor variable progression and relationships. Third, our structural equation model showed an appropriate acceptable fit. However, the RMSEA = 0.09 suggested a marginally or mediocrely fit, requiring further refinement by including additional paths, removing misfitting items in future large-scale studies. Finally, in the analysis using structural equation modeling, the limitations of sample size and study design made it difficult to conduct detailed subgroup analyses based on different age groups or other demographic characteristics. Therefore, future studies should aim for larger sample sizes and design more targeted research plans that allow for independent modeling and comparative analysis of different subgroups. This would provide a theoretical foundation and practical guidance for developing more precise intervention strategies tailored to different patient groups with varying characteristics. Finally, current study used HPA staging as an indicator of visual status to effectively reflect glaucoma-related visual field damage. However, we did not measure best-corrected visual acuity. Central visual acuity might independently influence certain self-management behaviors (eg, reading small text on medication labels). Future research is recommended to include both visual field staging and visual acuity as covariates.
Clinical Practice Relevance
From a clinical practice perspective, this study provides scientific and practical guidance for developing and implementing approaches to foster self-management in patients with glaucoma, with significant real-world applicability. First, the research underscores the essential role of assistance from the family in disease management. Family members not only provide important emotional support to patients but also play the roles of health behavior supervisors and behavior guides during treatment. Based on these findings, clinical healthcare providers should actively involve families in the treatment process, encouraging their participation in supporting patients’ treatment and daily life management. By establishing a collaborative mechanism involving healthcare providers, clinical pharmacists, nurses, patients, and families, patients’ treatment adherence and long-term self-management outcomes can be improved. Clinical pharmacists and nurses can play a critical role in ensuring treatment adherence in glaucoma patients. They can provide clear treatment explanations and education to patients in plain language and write down important instructions to patients. Pharmacists can monitor the side effects from the medications and address any structural barriers to medication and treatment access. Nurses can also connect patients and families with the social workers if social support is required. In addition, close follow-ups can be made with phone calls or instant messages to ensure treatment adherence. Second, we identified psychological capital as an intrinsic driving force for effective self-management, providing clear direction for clinical psychological interventions. In clinical practice, psychological capital can be fostered by administering mental health education courses, forming patient support groups, and using other methods to systematically enhance patients’ self-efficacy, hope, optimism, and resilience. This fosters patients’ capacity for psychological adjustment and flexibility when dealing with disease uncertainty and treatment challenges, allowing them to maintain long-term positive health behaviors. In addition, our findings also uphold the importance of emotional and behavioral management strategies in clinical interventions. Healthcare institutions should provide personalized health guidance services for patients, utilizing psychotherapeutic approaches along with cognitive–behavioral therapy to support patients with precisely identifying and modifying negative emotions and harmful behaviors. This will help them develop positive emotional expression and healthy coping styles.
Conclusion
This research explored the association between family functioning and self-management, with particular attention to the intermediary roles of psychological capital and coping styles. The outcomes indicate that family functioning exerts not only a significant direct influence on self-management in individuals with glaucoma but also an indirect influence via the successive mediation of psychological capital and positive coping styles. These results underscore the essential role of promoting self-management behaviors in this group through the enhancement of family functioning, growth of psychological capital, and promotion of adaptive coping styles.
Ethics Approval and Consent to Participate
Ethical clearance for the study was provided by the Research Ethics Committee of Jilin University First Hospital (reference number: 2024-1279). All patients provided informed consent in accordance with the principles of the Helsinki Declaration.
Acknowledgments
We would like to thank all of the involved physicians, nurses for dedicating their time and skill to complete this study. We would also like to thank all participants for their dedication and cooperation with data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. The corresponding author, Haiyang Xu, took the full responsibility for conduction of study, administrative duties, ethical compliance, integrity of the work as whole, and serves as the primary contact for communications.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002;86(2):238–14. doi:10.1136/bjo.86.2.238
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090.
3. Zhang X, Olson DJ, Le P, Lin FC, Fleischman D, Davis RM. The association between glaucoma, anxiety, and depression in a large population. Am J Ophthalmol. 2017;183:37–41. doi:10.1016/j.ajo.2017.07.021
4. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. doi:10.1016/S0738-3991(02)00032-0
5. Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annu Rev Public Health. 2019;40:127–146. doi:10.1146/annurev-publhealth-040218-044008
6. Hua Y, Lu H, Dai J, et al. Self-management challenges and support needs among patients with primary glaucoma: a qualitative study. BMC Nurs. 2023;22(1):426. doi:10.1186/s12912-023-01527-y
7. Wu P, Xi S, Xia H, Lu H, Guo W. Survey on vision-related quality of life and self-management among patients with glaucoma. J Glaucoma. 2014;23(2):75–80. doi:10.1097/IJG.0b013e318265bbf3
8. Tripathi RK, Shah A, Jalgaonkar SV, Kerkar S. Evaluation of antiglaucoma drug treatment awareness and patient-reported medication adherence: determinants of glaucoma management. J Postgrad Med. 2023;69(3):146–152. doi:10.4103/jpgm.jpgm_905_22
9. Sleath BL, Blalock SJ, Muir KW, et al. Determinants of self-reported barriers to glaucoma medicine administration and adherence: a multisite study. Ann Pharmacother. 2014;48(7):856–862. doi:10.1177/1060028014529413
10. Rathinavelu JK, Muir KW, Majette NT, et al. Qualitative analysis of barriers and facilitators to glaucoma medication adherence in a randomized controlled trial intervention. Ophthalmol Glaucoma. 2023;6(6):626–635. doi:10.1016/j.ogla.2023.06.002
11. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122(7):1308–1316. doi:10.1016/j.ophtha.2015.03.026
12. Ryan P, Sawin KJ. The individual and family self-management theory: background and perspectives on context, process, and outcomes. Nurs Outlook. 2009;57(4):217–225.e216. doi:10.1016/j.outlook.2008.10.004
13. Miller IW, Ryan CE, Keitner GI, Bishop DS, Epstein NB. The McMaster Approach to Families: theory, assessment, treatment and research. J Fam Ther. 2000;22(2):168–189. doi:10.1111/1467-6427.00145
14. Whitehead L, Jacob E, Towell A, Abu-Qamar M, Cole-Heath A. The role of the family in supporting the self-management of chronic conditions: a qualitative systematic review. J Clin Nurs. 2018;27(1–2):22–30. doi:10.1111/jocn.13775
15. Chang YS, Beake S, Kam J, Lok KY, Bick D. Views and experiences of women, peer supporters and healthcare professionals on breastfeeding peer support: a systematic review of qualitative studies. Midwifery. 2022;108:103299. doi:10.1016/j.midw.2022.103299
16. Mohanan P, Kamath A. Family support for reducing morbidity and mortality in people with HIV/AIDS. Cochrane Database Syst Rev. 2009;2009(3):Cd006046. doi:10.1002/14651858.CD006046.pub2
17. Luthans F, Youssef CM, Avolio BJ. Psychological Capital: Developing the Human Competitive Edge. Oxford university press; 2006.
18. Zhang Q, Sun J, Bian H, et al. The relationship between hope level and self-management behaviors in Chinese patients with type 2 diabetes mellitus: a chain-mediated role of social support and disease perception. BMC Psychol. 2024;12(1):446. doi:10.1186/s40359-024-01939-8
19. Ren LL. Correlation between psychological resilience and negative emotions as well as visual-related quality of life in glaucoma patients. Chin J Health Psychol. 2018;26(10):1469–1472.
20. Kong XM, Xu H, Zhang Q, Zhang HY. Investigation on the psychological status and vision-related quality of life of glaucoma patients and analysis of its influencing factors. Chin J Ophthalmol Otolaryngol. 2015;15(2):84–89.
21. Sahin Z, Nalbone D, Wetchler J, Bercik J. The relationship of differentiation, family coping skills, and family functioning with optimism in college-age students. Contemp Fam Ther. 2010;32:238–256. doi:10.1007/s10591-010-9116-4
22. Connelly TW. Family functioning and hope in children with juvenile rheumatoid arthritis. MCN Am J Matern Child Nurs. 2005;30(4):245–250. doi:10.1097/00005721-200507000-00008
23. Mathiesen KS, Prior M. The impact of temperament factors and family functioning on resilience processes from infancy to school age. Eur J Dev Psychol. 2006;3(4):357–387. doi:10.1080/17405620600557797
24. Reitz AK, Motti-Stefanidi F, Asendorpf JB. Mastering developmental transitions in immigrant adolescents: the longitudinal interplay of family functioning, developmental and acculturative tasks. Dev Psychol. 2014;50(3):754–765. doi:10.1037/a0033889
25. Peng Z, Fu N, Zhang X. The relationship between interparental conflict and middle school students’ coping style: the chain mediating effect of parental rearing style and emotional security. Psychol Dev Educ. 2020;36(6):668–676.
26. Peng PP, Zhang FF. Research on the correlation between psychological resilience, self-efficacy and social support in glaucoma patients. Int J Nurs. 2019;38(7):896–898.
27. Huang K, Xu Q, Jiang M, Wang B. A study on the correlation between psychological resilience and anxiety and depression in patients undergoing postoperative chemotherapy for breast cancer. J Nurs. 2013;28(2):89.
28. Zhang L. The impact of family and peer support care on improving self-efficacy and psychological resilience of glaucoma patients. Nurs Pract Res. 2022;19(3):452–455.
29. Duan Y, He J, Zheng R, Feng X, Xiao H. The relationship between disaster preparedness, psychological capital, and coping style among nurses: a cross-sectional study from China. Perspect Psychiatr Care. 2022;58(4):2577–2584. doi:10.1111/ppc.13097
30. Dreer LE, Owsley C, Campbell L, Gao L, Wood A, Girkin CA. Feasibility, patient acceptability, and preliminary efficacy of a culturally informed, health promotion program to improve glaucoma medication adherence among African Americans: “Glaucoma Management Optimism for African Americans Living with Glaucoma” (GOAL). Curr Eye Res. 2016;41(1):50–58. doi:10.3109/02713683.2014.1002045
31. Chow SC, Shao J, Wang H, Lokhnygina Y. Sample Size Calculations in Clinical Research. Chapman and Hall/CRC; 2017.
32. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978;6(6):1231–1239.
33. Zhang K. Positive psychological capital: measurement and relationship with mental health. Stud Psychol Behav. 2010;8:58.
34. Xie Y. A preliminary study of the reliability and validity of the brief coping styles scale. Chin J Clin Psychol. 1998;2(02):53–54.
35. Wu PX, Xi SX, Guo WY, Xia HO, Lu HJ. Development of the questionnaire on self-management Behaviors of glaucoma patients and evaluation of its reliability and validity. J Nurs People’s Lib Army. 2013;30(17):4.
36. Bronfenbrenner U. The Ecology of Human Development: Experiments by Nature and Design. Harvard university press; 1979.
37. Bandura A. Social foundations of thought and action: a social cognitive theory/Albert Bandura. 1986.
38. Wu JF, Deng JJ, Shen Y. Correlation analysis of quality of life and self-efficacy, coping styles in glaucoma patients. Qilu Nurs J. 2021;27(03):116–118.
39. Epstein NB, Bishop DS, Levin S. The McMaster model of family functioning. J Marital Fam Ther. 1978;4(4):19–31. doi:10.1111/j.1752-0606.1978.tb00537.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations of Psychological Capital, Coping Style and Emotional Intelligence with Self-Rated Health Status of College Students in China During COVID-19 Pandemic
Jing X, Meng H, Li Y, Lu L, Yao Y
Psychology Research and Behavior Management 2022, 15:2587-2597
Published Date: 14 September 2022
A Psychometric Network Analysis of Fear of Progression, Coping Styles, and Self-Management Among Patients Undergoing Continuous Ambulatory Peritoneal Dialysis
Fu S, Cao X, Liu X, Zhang L, Yang Y
Psychology Research and Behavior Management 2026, 19:620815
Published Date: 21 July 2026