Back to Journals » Psychology Research and Behavior Management » Volume 17
Factors Influencing Occupational Stress Perceived by Emergency Nurses During Prehospital Care: A Systematic Review
Authors Montero-Tejero DJ, Jiménez-Picón N, Gómez-Salgado J ![]() , Vidal-Tejero E, Fagundo-Rivera J
, Vidal-Tejero E, Fagundo-Rivera J ![]()
Received 16 December 2023
Accepted for publication 29 January 2024
Published 13 February 2024 Volume 2024:17 Pages 501—528
DOI https://doi.org/10.2147/PRBM.S455224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Diego José Montero-Tejero,1 Nerea Jiménez-Picón,2 Juan Gómez-Salgado,3,4,* Elena Vidal-Tejero,5 Javier Fagundo-Rivera6,*
1Department of Emergency, Hospital Universitario Lucus Augusti, Galician Health Service, Lugo, Galicia, Spain; 2Department of Nursing, Faculty of Nursing, Physiotherapy and Podiatry, University of Seville, Seville, Andalusia, Spain; 3Department of Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Huelva, Andalusia, Spain; 4Safety and Health Postgraduate Programme, Universidad Espíritu Santo, Guayaquil, Ecuador; 5Department of Cardiology, Hospital Universitario Virgen Del Rocío, Andalusian Health Service, Sevilla, Andalusia, Spain; 6Centro Universitario de Enfermería Cruz Roja, University of Seville, Sevilla, Andalusia, Spain
*These authors contributed equally to this work
Correspondence: Juan Gómez-Salgado, Department of Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Avda. Tres de Marzo, S/N, Huelva, 21007, Spain, Tel +34 959219700, Email [email protected] Javier Fagundo-Rivera, Centro Universitario de Enfermería Cruz Roja, Sevilla, Spain, Avda, de la Cruz Roja, 1, duplicado, Sevilla, 41009, Spain, Tel +34 954350997, Email [email protected]
Objective: To assess personal and work-related factors influencing the stress levels of nurses during prehospital care. Specifically, to identify associations between the level of perceived stress, the degree of professional experience, and the level of knowledge. Secondly, to examine the relationship between stress levels and violence in the work environment. And third, to investigate the main protective factors against work-related stress during prehospital care.
Methods: Systematic review in PubMed, WOS, Enfispo, Cochrane, and LILACS databases following the PRISMA methodology (last search 08/Aug/2023). Following the PECO framework, studies on occupational stress factors in ambulance emergency nurses were investigated. Studies in English or Spanish, from 2013 to 2023, and only research articles were admitted, thus excluding reviews, dissertations, and grey literature. Possible bias and level evidence were assessed using critical appraisal tools and GRADE. This protocol was registered in PROSPERO with code CRD42023446080.
Results: Fourteen articles were selected, and n=855 prehospital nurses were identified. One study was a clinical trial, and the others were observational and qualitative. The level of evidence was very low (n=7), low (n=6), and moderate (n=1); any study was excluded due to methodological bias. Five categories of stressors were extracted: the management of the health service (ie, workload organisation, and resources), patient care (mainly paediatric care), interpersonal stressors (relationship with peers), environmental factors (exposure to injuries), and personal factors (training, experience, and coping strategies). Violence at work is frequent for prehospital nurses, implying both verbal and physical aggressions. Support from peers was associated with positive results against stress.
Conclusion: Managing workload and improving resources in the work environment are essential to reduce fatigue and allow emotional processes to be addressed. Providing workers with coping skills also imposes on them the responsibility to cope with stress. Collective awareness is the main element in reducing the incidence of stress.
Keywords: ambulance, prehospital, emergency care, nurses, stress, occupational health, management
Introduction
The term stress, developed by Hans Selye in 1936 and which gave rise to the general adaptation syndrome, has acquired an increasingly important role in the work environment and in the health of workers.1,2 It occurs as a harmful physical and emotional response when job requirements are not consistent with the competences and needs of the employees,3–6 and is now considered to be a major cause of the increasing incidence of infectious and cardiovascular diseases, as well as increased mental and physical disorders.2–6 Lazarus and Folkman, in 1986,7 went a step further and mentioned that stress refers to an existing relationship between the person and their environment, whose turning point is the personal evaluation of each situation. In this respect, these authors introduced two concepts, cognitive assessment and coping strategies. Coping was defined as the ability to make cognitive and behavioural efforts to respond to those external and/or internal demands that exceed the resources a person has. On the ability to make a personal cognitive assessment, Lazarus and Launier8 reasoned that an event can be analysed as loss (or damage), threat, or challenge, and it is the individual evaluation of the event what stimulates a particular set of coping reactions.7–9
Stress has been identified as one of the main reasons for turnover in the nursing field, also playing a very notable role in 50% of sick leaves as well as causing reduced performance, absenteeism, greater situations of violence in the work environment, and increased turnover among different professionals.4,6,10,11 Indeed, some work-related characteristics play a decisive role in the return-to-work process after a mental health sick leave. Aspects such as high job demands, low job control, limited opportunities for job promotion, and high job strain adversely affect return to work.11–13 In this sense, the Community Programme for Employment and Social Solidarity, PROGRESS (2007–2013), has financed studies and publications of documents in this regard to overcome the barriers that may be encountered by the worker who returns after a leave due to mental health problems.14
Currently, health workers suffering from stress exceed 28%, which causes an approximate health expenditure of between 150 and 372 million euros per year due to its consequences on health.10 In the particular case of nurses who work as ambulance staff for the prehospital emergency system, the special characteristics of the service facilitate the presence of a large number of potential stressors that increase the predisposition to suffer a high rate of work-related stress.3,4,10 Moreover, this problem could be aggravated when facing certain extraordinary situations such as, for example, terrorist attacks or health crises such as the COVID-19 pandemic.15,16
The main axiom of the prehospital emergency service is to be a rapid resource with a high degree of effectiveness, requiring coordinated interventions adapted to the specific characteristics of each situation, estimated after a previous assessment.4,17 The high specificity of this service, nonetheless, does not always correspond to regulated training of professionals, and it is still possible to access the emergency ambulance unit with just a university nursing degree in some locations. For instance, in Spain, the Emergency Nurse must have a university degree in Nursing, but the Master’s Degree in Emergency Nursing, or nursing specialties in community nursing or medical-surgical nursing are not mandatory requirements.17,18 Nevertheless, in other countries such as Sweden,19 Finland, Belgium, Thailand, Malaysia, Indonesia, or Brazil,20 nurses provide prehospital services and define a new field for the university nursing practice and training.21,22 Indeed, in Sweden, national regulations require an ambulance to be staffed with at least one registered nurse and, depending on local requirements, this nurse is often required to hold an additional one-year post-graduate specialist nursing diploma.23,24 In Croatia, Estonia, and Lithuania this training is ongoing, while in the Czech Republic, Germany, Ireland, Latvia, the Netherlands, and the United Kingdom nurses are required to attend courses on a yearly basis. In Belgium, skills are evaluated once in five years.25,26 However, in other countries such as Iran emergency medical technicians (EMTs) are the most common providers of prehospital emergency care27 and, due to the insufficient number of EMTs, nurses are included among prehospital care providers.21 The complexity of the practice and its prerequisites may explain why nursing professionals working in the ambulance service express the need for periodic renewal training based on the belief that the job requires a specialised level of education, including psycho-emotional competencies and tools.24
Inadequate training means that most ambulance nurses do not have the adequate knowledge to evaluate or initiate appropriate treatment, or to deal with situations where the patient is seriously affected and it is necessary to inform family members and, at the same time, offer emotional support.28 This has been associated with the idea that nurses with a longer career (greater experience) will experience lower levels of stress.29
Previous studies have also highlighted the influence of the paediatric patient as the most stressful factor, stating that such associated critical incidents account for up to 41% of the stress experienced by prehospital emergency professionals.30–32 Other notable aspects related to stress have been working overtime and the existence (or not) of a support network of co-workers and superiors.31,33 Regarding violence, as a stressor perceived by prehospital emergency nurses, a review carried out in 2018 included 25 studies that highlighted the frequent presence of this factor in daily work.34 A significant link has been found between exposure to violence, emotional exhaustion, depersonalisation, and lower personal accomplishment levels, noting that increased exposure to verbal abuse leads to staff fatigue, loss of productivity and, eventually, turnover.35 In this sense, cases of verbal and physical violence stand out,36 amounting to 34.5% of professionals who had been physically assaulted as evidenced by a study conducted in Spain.37 It has also been suggested that being female was a risk factor only for ambulance staff and emergency nurses,38 which increases the likelihood of suffering some form of violence, thus making the possibility of intimidation, sexual harassment, or sexual assault more relevant.34
Occupational health services play a major role in achieving the highest possible level of biopsychosocial well-being for workers.39–42 However, there is still a notable lack of knowledge about the multiple stress factors that nurses in the prehospital emergency service face on a daily basis. So, it is relevant to address this issue in order to achieve a favourable and optimal environment to work safely so as to offer higher quality of care.6,43 In this sense, the concept of coping with stress,7 defined as the effort to handle specific demands that require an effort, a challenge, or a price on the part of the person, is useful for ameliorating stressful situations.44,45
To our knowledge, there are no previous reviews on the stress levels of ambulance emergency nurses. Therefore, the general objective of this research was to assess the personal and work-related factors influencing the stress levels of nurses during prehospital care. As specific objectives, the first was to identify the association between the level of perceived stress, the degree of professional experience, and the level of knowledge. Secondly, it was to examine the relationship between stress levels and violence in the work environment. And third, to investigate the main protective factors against work-related stress during prehospital care.
Methods
Study Design
A systematic review of the available literature on prehospital nursing stressors and how they affect the work of nurses working in the ambulance service was carried out following the PRISMA methodology.46 A pre-established search and review protocol minimised the risk of selection and publication bias. This protocol was registered in PROSPERO with code CRD42023446080. First, the PECO question was formulated for an adequate literature review (Table 1). For this, the following research question was developed: What factors affect the stress levels of prehospital emergency nurses?
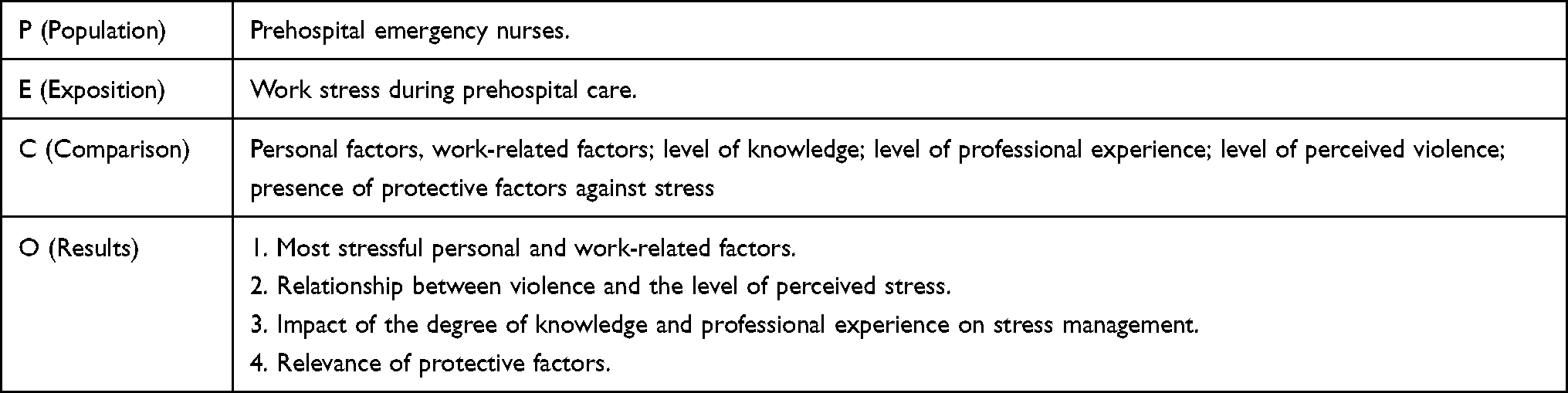 |
Table 1 PECO Question |
Databases and Search Strategy
The search was carried out in the PubMed, WOS, Enfispo, Cochrane, and LILACS databases during July and August, 2023. Last searched on 08/08/23. MeSH descriptors related to the topic were identified to define the search equation and were combined using parentheses and Boolean operators. The resulting search strategy was: “occupational stress” AND nurs* AND (“prehospital care” OR emergenc* OR ambulance OR “first aid” OR “work experience”) (Table 2). A reverse search was also conducted to collect suitable research studies from the reference lists of other pre-selected studies.
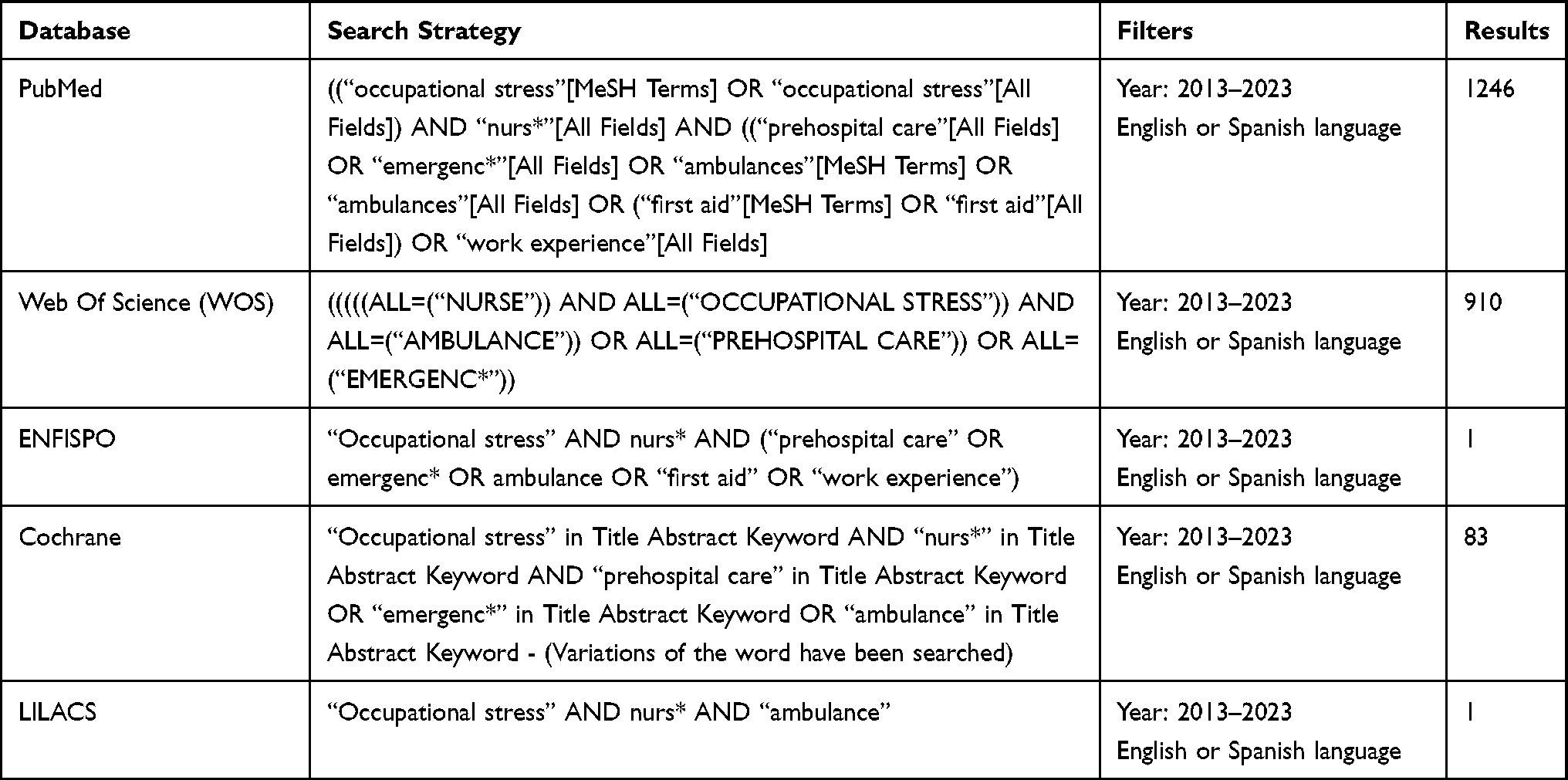 |
Table 2 Search Strategies |
Study Selection
The inclusion and exclusion criteria have been identified in Table 3. Two researchers performed the review using the aforementioned database search strategy, executing an initial screening of articles by title and abstract. After this, the same two researchers analysed the full text of the articles and agreed on those studies that were potentially suitable for inclusion in the review. Any discrepancies that arose were resolved by a third researcher.
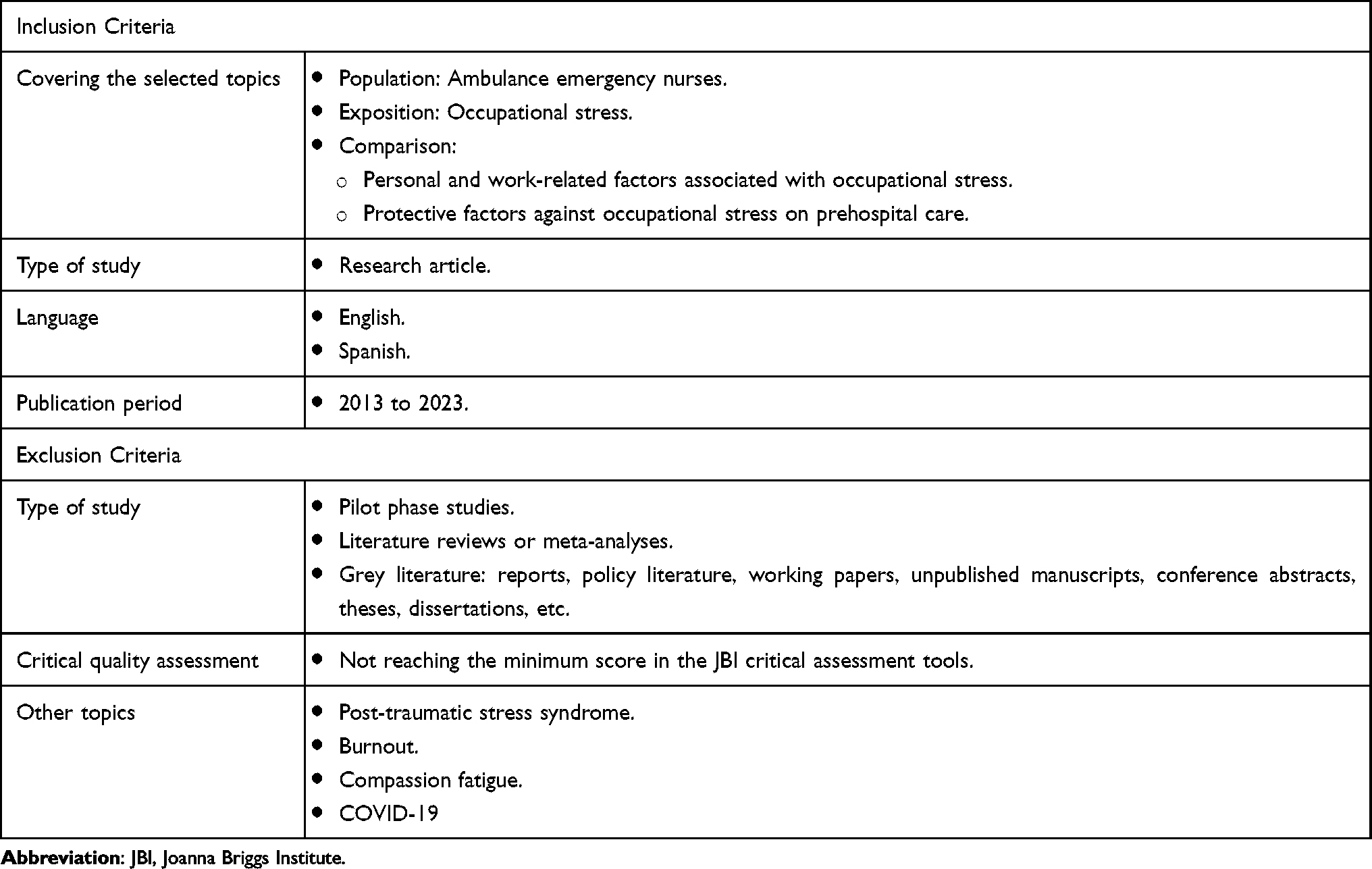 |
Table 3 Inclusion and Exclusion Criteria |
Initially, the search equation, once the criteria had been applied, yielded a total of 2241 articles of which n=1449 were assessed after removal of duplicates (n=756) and other records due to exclusion criteria (n=36). A first reading was performed by title and abstract of each study in order to obtain a first screening, eliminating those whose who did not met the expectations (n=1301). Next, the articles that had not been eliminated in the previous phase were sought for retrieval and read (n = 148). Finally, each study was full text reviewed to select those that could adequately meet the study objectives. Twenty-two studies were ruled out for analyzing PTSD, n=28 for treating compassion fatigue, and n=60 for treating burnout. Twenty-seven studies were excluded for not specifying that the sample consisted of nurses. A total of n=14 articles were finally selected, of which n=3 articles had been selected by reverse search (Figure 1).
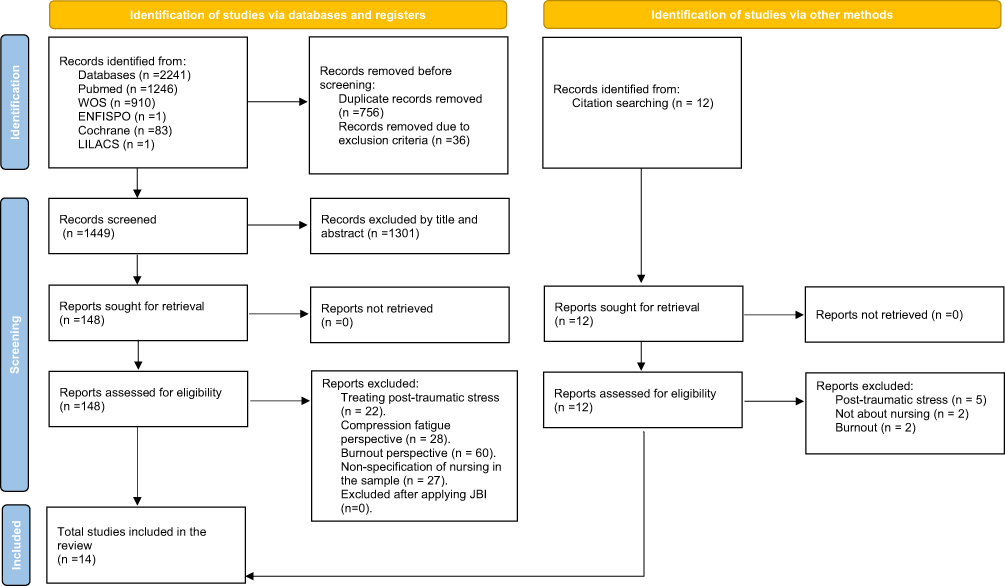 |
Figure 1 PRISMA flow chart. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.46 |
Data Collection and Extraction
For a peer-review purpose, a template was created to allow the researchers to review and collect the main characteristics of each study. All relevant data was synthesized and categorized according to the PECO framework and compared to resolve any possible discrepancies.
Risk of Study Bias and Methodological Quality Assessment
Once the articles on which this work would be based had been selected, a bias assessment was carried out on each of them in order to know the reliability and relevance of the studies and, therefore, their eligibility. For this, the critical appraisal tool of the Joanna Briggs Institute (JBI)47 was used, which allowed identifying the possible biases of each study in terms of design, conduct, and analysis, thus showing their methodological quality. The data obtained in this process were placed in tables according to the specific type of study.
The methodological quality assessment was performed independently by both reviewers. For the selected studies, a cut-off point was established for scores equal to or greater than half of their maximum value: analytical cross-sectional studies (Table S1) were measured through 8 items,48 and scores of 4/8 or higher were accepted; randomised controlled trials were measured through 13 items49 (Table S2), and scores of 7/13 or higher were accepted; for qualitative research, 10 items were assessed (Table S3),50 and scores of 5/10 or higher were accepted. In this study, no studies were ruled out by the investigators as all exceeded the minimum required scores.
Management of Data and Synthesis methods
Finally, both authors made a narrative synthesis of the data obtained and organized them into categories. This synthesis was aimed at explaining the results of the selected studies according to the objectives of this study. In addition to this, the quality of the evidence was evaluated using GRADE system for the assessment of quality of evidence and degree of recommendation.
Results
Descriptive Analysis of Study Characteristics
A total of 14 articles focusing on the factors that generate work-related stress in prehospital services were selected for this study.5,21,23,27,28,36,43,51–57 Half of these articles approached their research from a qualitative perspective (n = 7),21,23,28,36,43,51,52 and the others did so from a quantitative perspective (n = 7);5,27,53–57 the oldest articles selected were from 201436,56 and the most recent ones, from 2022.27 These studies were carried out in 8 different countries: 5 in Iran;21,27,43,54,55 2 in Sweden23,28 and Brazil;5,53 and 1 in Ireland,51 USA,52 Switzerland,56 Spain,36 and Poland.57 The total sample was n=2475 participants from various healthcare professions; in the specific case of nursing specialised in prehospital emergencies, n=855 (34.5%) were nurses. Table 4 shows the characteristics of each of the 14 final articles for this review. These characteristics were categorised by authors and year of publication, geographical context, objective, type of study, interventions, variables, measurement instrument(s), participants, and main findings.
 |
Table 4 Summary of the Selected Articles |
Results for the general objective: factors influencing the level of stress of nurses during prehospital emergencies.
In order to classify the results obtained in a homogeneous and practical format, the results were organised into 5 categories, based on the classification of 7 categories defined by Aisling et al51 in their study of mixed methods on prehospital nursing professionals. These categories were: 1) The management of the health service, comprising the personnel in charge of managing the material, economic, and human resources (also offering psychological support) within the prehospital emergency service, the aim of which is to offer an adequate service to meet the needs of the population; 2) Patient care, referring to the types of emergencies and interventions derived from prehospital clinical care; 3) Interpersonal stressors, including relationships with peers, both in the work team and in the work environment; 4) Environmental factors, related to the work context and risk scenes. 5) Personal factors, derived from personal experience, training, health status, or behavioural characteristics of nurses. A summary of the findings is shown in Table 5.
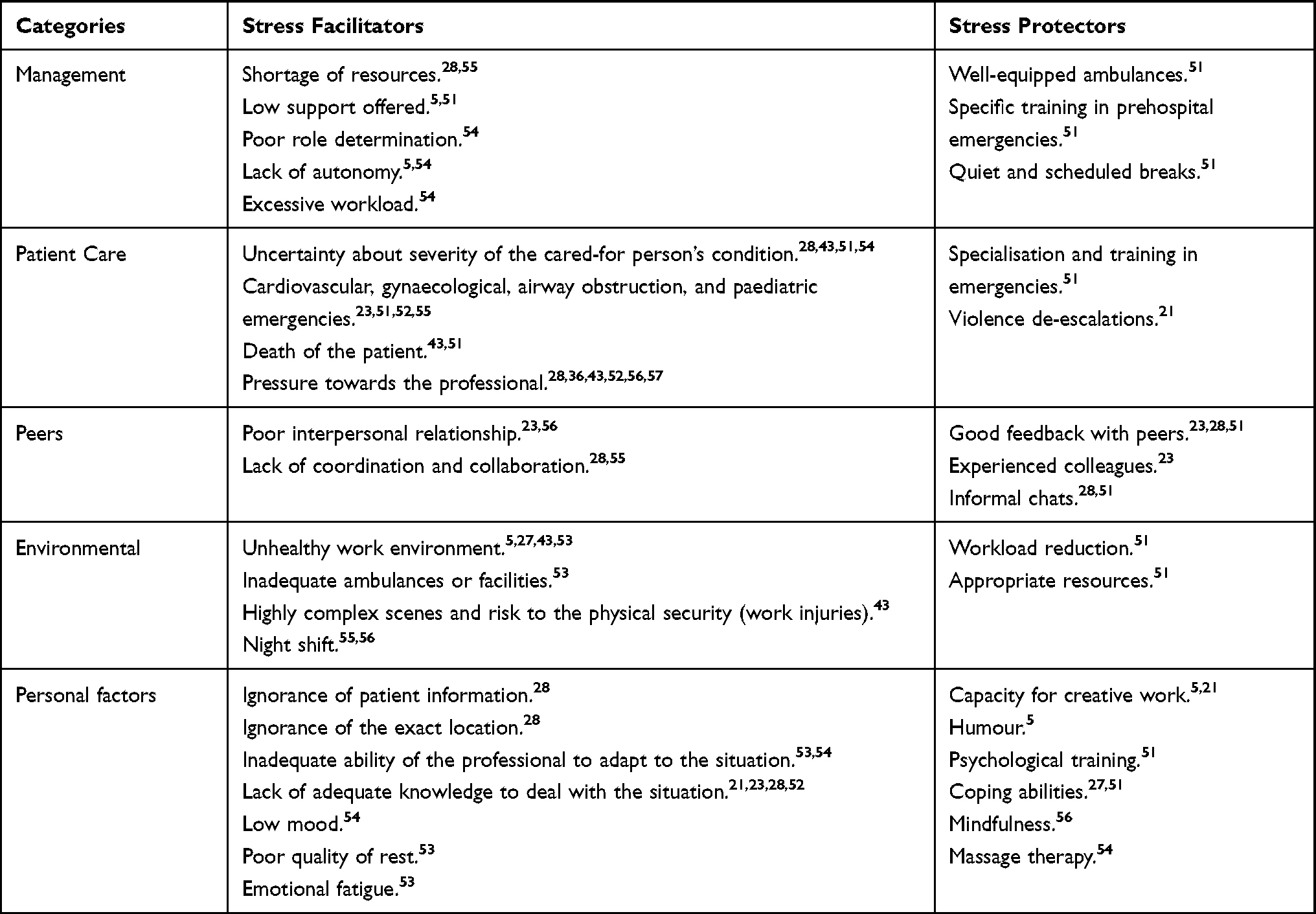 |
Table 5 Description of the Main Findings |
Management
The very nature of the service (ambulance and prehospital environment) is conducive to not having all the material resources (p=0.002; OR=2.88), nor the necessary personnel.53 This deficit is exacerbated in critical situations, where the demand for care is much higher, so managers must strive to equip ambulances with everything necessary to facilitate interventions and reduce the likelihood of developing stress among their staff members.28
In addition, the support received from those in charge is an aspect to highlight within this category. Several studies have reported on the low level of occupational care that nurses generally had, which also led to stress, cardiovascular problems, and both physical and emotional exhaustion.5,28 Managing bodies are also responsible for indicating the role of each of the team members who assist in any health emergency, which will allow for cooperation at all times, thus avoiding working in an unstructured team that can act as a stressor.27
On the other hand, as evidenced, the lack of autonomy in the nurses’ practice did significantly affect the level of perceived stress (p=0.001; OR=2.86).53 This fact seems to generate a passive profile in the worker who, due to the lack of a relevant role within the emergency team, was less involved, which resulted in decreased ability for problem solving.5,53
The workload has also been presented as a factor capable of generating work stress, and this is derived from the type and level of organisation of the work of health professionals. The authors Mirzaei et al27 found a higher level of occupational stress caused by workload (β=0.163, p = 0.012 β). However, Mahdizadeh et al classified this factor as being as stressful as the lack of autonomy (p < 0.05).54
Patient Care
Cardiovascular emergencies were classified as the most demanding and those that generated the need to act at a faster pace, thus limiting the possibility of fully using nurses’ competencies.23,55
Gynaecological emergencies (specifically if the nurse was a male), airway obstruction, and paediatric emergencies23,28,51,52,55 were also highly stressful, especially if the results obtained were considered negative.23,28,55 This feeling of stress is magnified if the patient eventually dies, and several studies have determined that this situation was the most stressful one faced by nursing professionals working in prehospital emergencies since, in addition to assimilating the death of the cared-for person, it is necessary to deal with the emotional responses of the relatives.51,54
Traumatology accidents, respiratory distress, and heart problems were revealed as the paediatric emergency situations that led to the highest level of occupational stress.52 In these cases, stress was associated with assuring patient safety at all times, the psychological trauma of seeing an injured child, lack of experience in these types of emergencies, responses from family members, as well as children’s reactions and knowing that the situation could worsen rapidly.52
The situations in which the behaviour, mainly of the patient or their companions, are out of control, thus becoming a danger for professionals, were described by the participants of the sample of M. Mahdizadeh et al54 and the research by A. Afshari et al43 as one of the most stressful factors. Bohström et al28 mentioned increased perceived danger by health professionals during prehospital emergencies, mainly due to violent or threatening behaviours from both patients and their companions who see their expectations unmet, both in priority and rapid care and as regards the results of the clinical assistance. This danger generates a high level of stress that continues to affect nurses even during holiday periods, due to memories of previously experienced incidents.
Interpersonal Stressors
Prehospital emergencies require multidisciplinary care, so it is essential, especially for nursing, to have a good working relationship with the staff who assist in the ambulance. This will make it possible to act in a coordinated manner seeking at all times the benefit of the patient and reducing the impact of stress on the work team.51
As assessed in the studies included, this adequate feedback with peers, especially among experienced professionals, led to a greater development of personal skills and safety in each intervention, while a poor interpersonal relationship with peers or a lack of trust between them was perceived by the professionals of three studies as one of the factors with the most significant impact on the generation of work stress.23,51,54
Environmental Stressors
Working in an unhealthy environment or inadequate facilities may increase the stress levels perceived by healthcare professionals.53 Likewise, highly complex scenes and high risk for the physical safety of the health team force nurses to be very attentive to the dangers, which generates a great feeling of stress and anxiety. The possibility of suffering a musculoskeletal injury when mobilising a patient, being involved in an accident inside the ambulance, or the possibility of exposure to different diseases transmitted by the patient have also been highlighted.43 As for work schedules, working the night shift also turned out to be an environmental factor that revealed a significant influence in the generation of stress.27 Despite this, environmental emergencies were recognised as one of the least stressful for prehospital care nurses,55 and the differences between hospital nurses and prehospital nursing teams were notable (t = −4.719; p=0.000).27
Personal Factors
Bohström et al focused their study on two main topics: inadequacy related to the ability to cope; and uncertainty about the context and final outcome of the health intervention.28 In this study in Sweden, it was reported that, since the emergency alert call is received, a series of stressors are activated, to which it is sometimes added the fact of not knowing all the patient’s information or the exact location of the incident.28 As shown in the study, when patient data were expanded, practitioners greatly relaxed. Other factors are related to the abilities of each professional to adapt to the situations they face. Many nurses claimed not to have the adequate knowledge for both evaluating the situation and initiating an adequate treatment, and above all they affirmed that situations where the patient was seriously affected and they had to inform their relatives and at the same time offer emotional support generated a great feeling of stress that was aggravated even more so when they were acquaintances of the patient they had to assist.28 Low personal mood, poor sleep quality, and emotional fatigue (an element that doubled the presence of stress in health workers) also obtained significant evidence as determinants of the generation of work stress perceived by ambulance emergency nurses in countries such as Ireland or Brazil.51,53
Results for the Specific Objective: Relationship Between Violence and Stress
Violence is a frequent problem for nurses during prehospital care due, mainly, to the false expectations of both the relatives and the patient, even in cases where there has been drug abuse. The emergency respondents’ perception of the most threatening situation would be, first, the interaction with patients who have taken designer drugs, followed by drunk patients and those with mental disorders.57
From the total selected research, it has been observed that prehospital nursing professionals do not define their profession as completely safe. For example, 572 health workers of the Polish emergency service indicated on a scale of 1 to 5 the level of perceived danger, obtaining a mean of 3.6, being valued by 40% as a high level of danger (level on the scale: 4/5). Multivariate regression has shown that staff with a career length > 5 years assessed the level of danger as 1.132 times higher (p < 0.001, R2 = 0.181).57
The above said contrasts with the results obtained in a Spanish study where it was found that 18.1% had never been exposed to any type of aggression. However, 47.6% had been exposed to verbal violence and 34.3% had also been physically assaulted.36 This study also mentions waiting times of both the patient and their environment as one of the most frequent reasons for aggression.36 In contrast, participants in an Iranian study were more likely to experience violence when they attended crowded scenes, with people with a high level of stress in high-severity incidents, which were aggravated if they had not arrived promptly at the scene.21 Also, feelings of anger are generated, mostly, in serious situations that can lead to the death of the patient.28,43
Results for the Specific Objective: Protective Factors Against Work-Related Stress
The importance of work experience and the level of knowledge of the nursing professionals has offered inconclusive results as regards the level of perceived stress. Some studies highlight that an optimal level of experience extends the stress-reducing capacity and point out statistically significant differences that confirm that younger professionals and with less prehospital experience are more vulnerable when facing complex situations such as, for example, those involving children (especially if the result of the intervention is not positive), so their perception of work stress rises, affecting their overall perception of health.23,57 Lack of experience is also a determining risk factor for numerous physical injuries caused by violent acts through direct confrontation with patients or relatives, resulting in obvious sources of stress.21,43 Being youth has been postulated as a facilitating factor for both physical and verbal violence that also increases the sense of danger.36
The professional experience of peers has been found to affect the level of stress of ambulance staff. It has been shown how nurses working in ambulances stated that the fact of working alongside an experienced peer allowed them, through feedback, to develop their own skills with a greater degree of confidence when performing the interventions, resulting in benefits on perceived stress. On the contrary, working with inexperienced peers or with whom one had a bad working relationship generated a high level of stress.23,28
On the other hand, there are some detractors who claim that the level of experience plays a relevant role as a stressor. The study by Mirzaei et al27 established a statistically significant relationship between both age and work experience and work-related stress. The results obtained suggest that, as the age and work experience of nurses increased, their ability to adapt and resistance to the stressful situations of the prehospital emergency service were minimised. Stress increased more significantly in those who had been working longer in the profession, since they had greater emotional exhaustion due to years of work and less physical capacity to perform activities. Afshari et al43 highlighted work injuries as the main source of stress, categorising them into physical injuries and psychological stress. Following this line, the results obtained by Carvalho et al showed a lower stress level among those who had worked less time in this service, being the time frame worked from 6 to 10 years as a prehospital nurse the most affected, with 35.2% of respondents declaring stress.53
The application of protective measures within the prehospital emergency service is mainly derived from the following two categories:
The Support Received from Colleagues
Prehospital nursing is a fundamentally collaborative profession, with the need for a fluid working relationship and an adequate level of trust in the rest of the colleagues, since this decreases the level of perception of stress, even when faced with a highly complex event.23,28 As shown by the results, the benefit of informal talks between peers should also be highlighted, which allowed to expose common experiences among the staff. This enabled regular feedback on healthcare outcomes, where professionals could maintain an open discussion about the stressful situations encountered during their practice in a self-evaluative and reflective way, sharing how they felt and coped with similar situations.23,28,51
Management
The role of the manager is also fundamental in reducing the feeling of stress on the part of health professionals, as among the functions of managing staff is to ensure the specific training of nurses in the field of prehospital emergency care, as well as to implement adequate and sufficient resources to allow the team to perform their tasks in an optimal way. In addition, as the person in charge of regulating working conditions and supporting professionals, the manager must address the perceived need for structured schedules and breaks.51 Other authors also highlighted increasing autonomy, creative work capacity, and humour as factors to be taken into account for protection against stress.5
Discussion
Occupational stress is a problem that professionals must cope with on a daily basis and, within the different professions that deal with prehospital emergencies, nursing is among the most affected by the level of perceived stress.51 The severity of this issue is made evident by the frequency with which this condition manifests itself in this professional group, with numerous studies declaring a prevalence of between 25% and 65%, the vast majority of which with stress in the resistance phase and with a high percentage in the exhaustion phase.27,51,53 To answer the first objective of this review, 14 studies were analysed and stressors felt by prehospital nurses were grouped into five categories: management, patient care, interpersonal stressors, environmental stressors, and personal factors. The violence perceived by professionals has also been a remarkable element in this review, being one of the factors that precipitates stress and the perception of danger. On the other hand, the main protective factors derive from peer support and provision from health service managers,23,28,51 although certain individual interventions have also been effective, such as mindfulness52,56 or positive coping therapies.27 The results from this review provide useful information for prehospital nurses and allow these factors to be mapped against other nursing specialties in the hospital setting.58
Regarding health services’ management, the shortage of resources outside a clinical centre has been considered one of the most relevant factors affecting stress, even having the capacity to double the stress levels.51,59 The incidence of psychological distress in ambulance personnel is not just a matter of exposure to traumatic incidents, but is also a result of the way in which the organisation responds, at managerial and organisational level.59 Likewise, a significant influence of the low level of support perceived by nurses from their superiors during the performance of their duties has also been observed.53 In this sense, it has been suggested that the effects of stress, especially those of a psychological nature, or cases of perceived violence, may have a relevant effect on the work engagement of nurses, and closer attention by occupational health services may help to reduce the negative consequences of these adverse events by favouring high levels of self-efficacy;38,60 for example, by facilitating access to formal paths of psychological attention, ambulance personnel could receive appropriate care against stress, lack of confidentiality, use of inappropriate therapies, poor return-to-work mechanisms, isolation, or stigmatisation of work.59
The personalised care of each patient, the patient’s state of health, and closeness to death are the patient-centred factors that most influence stress levels in nurses. In this sense, cardiovascular, gynaecological, and paediatric emergencies are the most demanding situations, highlighting musculoskeletal trauma, respiratory distress, and cardiac problems among the events involving children.23,51,55 The level of stress is also interrelated with decreased patient safety, mainly due to identification with the patient, lack of experience, responses from family members, and knowing that the situation could worsen at any time.55 Some studies already showed that ambulance nurses need more knowledge and education as regards the care of children.61,62
Similarly, dealing with special patients, suicide events, workplace violence, and other traumatic events have been pointed as the direct causes of stress in emergency nurses.63 Situations of violence are aggravated, according to some studies, when the patient and/or their companions are intoxicated or when the perception of the patient’s injuries differs between health workers and family members, and it is reinforced if the ambulance does not arrive promptly.21,54 In those situations, in which the patient gets out of control (becomes verbally and/or physically aggressive), professionals feel insecure, and there is debate about whether the age and experience of the professional can act as protective agents or censors in these situations.23,28,38 For example, problems with superiors have been positively associated with repeated confrontations, ie verbal aggression, being on guard, and/or any form of aggression, and could be seen as factors related to interpersonal conflict and inability to prevent violence escalations.26
The environmental factor comprises working in unhealthy environments, in inadequate physical facilities, or in scenes of high risk to the physical safety of the health provider, in addition to working the night shift.53,56 In a previous review,58 the work environment was pointed as a factor that contributes to increased stress levels, impacting on nurse retention rates in the emergency departments. These environmental stressors included inadequate staffing levels, very high responsibility, excessive workload, and overcrowding.64 On the other hand, the stressful role that night work plays in nursing has also been highlighted,64 being a possible cause of cancer65 and work-family conflicts.66
In terms of personal health, low mood and poor sleep quality stand out as stressors. Studies on the effects of long-term stress among nurses very often show sleep problems and insomnia.64 On the other hand, emotional fatigue, not knowing exactly the patient’s information, and not having adequate knowledge to evaluate a patient or perform the appropriate interventions aggravate the level of stress of prehospital nurses, especially in complex situations, thus increasing the probability of suffering both physical and psychological problems such as anxiety, physical pain, deterioration of personal relationships, or increased cardiovascular problems.28,53 In this sense, promoting ongoing training is essential, since nurses with less advanced training in the ambulance system may encounter greater complications during health care than those with a higher level of competence. A curriculum for a specialist nurse should reflect the actual knowledge, expertise, and skills required in the profession-specific environment.67 Treatment guidelines and working protocols, as well as contact with more competent colleagues, are workplace-based strategies that contribute to safe patient care and strengthen the ability to successfully deal with critical incidents.45
Finally, the main protective agents for stress reduction highlighted in this review are interventions carried out jointly with both managers and peers working in the service. However, these are not fully effective, so professionals suffering from stress should seek support in practices such as mindfulness, spiritual coping, massage, and psychological therapies.27,51,52,54,56,68
Psychological Therapies
Comprehensive psychiatric evaluations should include assessment of long working hours and high levels of strain and stress at work, in particular when there have been work-family conflicts, health issues, emotional problems, suicidal ideation, and previous psychological treatment. Marital status, perceived family and social support, and sense of coherence should also be assessed. Additionally, it is important to consider other factors such as age at the start of the profession, years of service, or rank.69 Similarly, a comprehensive psychiatric evaluation, including a clinical interview and administration of validated assessment measures, should be done on a regular basis to help the person to correctly perceive external threatening factors of stress.44,45 In this regard, the lack of accessibility described by nurses should be noted, since in very few cases this type of intervention is promoted by managers.51
Mindfulness
It has been proven that mindfulness therapies favourably affect the reduction of stress perceived by nurses, especially in cases of conflict with peers and with a great number of interventions during the workday. It is also worth noting the improvement obtained in the specific case of prehospital emergency care involving children.52,54,56
Positive spiritual coping was associated with decreased occupational stress (β = 0.373).27 This type of intervention has obtained significant statistical evidence as for reducing occupational stress in all its subscales, obtaining higher self-awareness and increasing the search for peace and internal harmony. It mainly consists of religious help, coping with difficult situations, and the use of cognitive and behavioural work through a positive attitude to overcome weaknesses.27
Massages
Although it has been mainly used in pain management, it has also been highlighted in the treatment of stress given its ability to promote patients’ relaxation as well as to increase the ability to concentrate and stabilise the immune system (p = 0.001).54 However, although massage was beneficial against some stressors (patient death and conflict with managers and peers), it did not obtain significant evidence when dealing with stress in general. Therefore, although this intervention should be considered when dealing with stress in prehospital care based the results obtained in various studies, where it was studied as a single intervention, it should be recommended as a complementary procedure, just like other means such as music therapy.54
The main limitation of the present study has been the low prevalence of previous studies that focus on work-related stress from the perspective of prehospital emergency nurses. Indeed, only one of the selected studies was a clinical trial, and the others were observational and qualitative studies. To this it must be added that some research was excluded because it did not offer data disaggregated by health professions, thus making it difficult to obtain a clear vision of the problem in the field of nursing. For future research it is convenient to analyse the stress factors exclusively from the nurses’ point of view, separating the nursing profession from the other professions that act within the ambulance service.
According to the selected studies, it should be mentioned that the information in this review has been extracted from a heterogeneous international context, so some variability in these factors may be found in each national health system. In this sense, a limitation of this study is that due to the low volume of articles, the variables analyzed, and the different measurement scales, the researchers did not consider it applicable to perform a meta-analysis as a synthesis of the evidence.
The investigators performed a review protocol to minimise bias during research and used the GRADE tool to assess the quality of the evidence to avoid potential publication bias, and consequent overestimation of the data. A selection bias must also be acknowledged, given that some studies in the research may not have been identified or were excluded as they did not fit the established criteria. Nonetheless, all identified research was retrieved, and any study was excluded due to methodological bias. Finally, note a possible researcher bias since expectations and opinions may have conditioned the conclusions.
The main contributions of this study are based on the description of the main factors that act in prehospital emergency systems that increase the stress perceived by nurses, with the aim of reducing these risks and acting to promote the mental health of healthcare professionals. The optimal strategy to follow parts from a collaborative effort between health services managers and the nurses who work in them, so as to correctly cope with these stressors, according to Lazarus’ theory.7,8 However, a review on this topic showed that most studies only measure some work stressors and some outcomes, without taking into account the perception of the stressor by the emergency nurse.70 According to Lazarus,71 coping strategies may be used to change the stressful situation for the better, either by modifying the person’s actions or by changing the environment. Seeking information or planning alternatives and direct actions are useful strategies for active coping.72 Nursing managers need to be aware of those situations when nurses’ usual strategies are no longer adequate for effective coping, and it is essential to understand that they might be key figures in helping them to cope.44,45
The organisation can assist through a number of strategies and processes that can be divided between cultural shifts and organisational re-design. Cultural action is required to remove the stigma associated to seeking help for work-related stress. This may mean that the service needs to organise staff to allow that fatigue and emotional processes can be addressed. Therefore, hospital and prehospital emergency managers can reduce their staff’s stress levels by reducing workplace demands and improving the work environment. By reducing stress, the health of staff members is maintained and improved, and the quality of care provided to patients increases.59,73
Conclusions
Due to the characteristics of the prehospital emergency, it is inevitable that nurses will be exposed to multiple potentially dangerous and stressful factors. Mainly, 5 categories have been highlighted based on personal characteristics of nurses, environmental stressors, management, interpersonal stressors, and patient characteristics. It was also possible to associate the increase in the perception of work-related stress with the violence received during the service. On the contrary, the level of experience and knowledge presented a diversity of opinions about their role in stress levels.
Against aggressions, there are multiple strategies to deal with it, being the control of the patient’s clinical situation and the control of their social environment the most effective, as well as implementing national strategies in order to minimise violence towards healthcare workers. To improve safety in the different interventions performed by the emergency team, the relationship of trust between colleagues is also relevant as well as working with professionals with a higher degree of experience and knowledge when nursing staff are poorly trained.
Finally, providing the necessary resources to ambulances and workers, so that professionals do not have a feeling of lack of control, especially when it comes to a complex intervention, is essential to control the environmental factor. To this can be added the establishment of adequate rest periods and the adequacy of the workload.
This study promotes that interventions for stress management in health workers could have a greater weight in health policies by managing resources and environmental factors that can influence stress levels among members of staff. In addition, providing workers with psychosocial skills to increase self-knowledge and self-care also places on them the responsibility of coping with stress. This allows collective awareness to be, finally, the main element that reduces the incidence of stress.
Funding
No funding was received for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nogareda S. Fisiología del estrés. NTP 355. Barcelona: centro Nacional de Condiciones de Trabajo. Instituto Nacional de Seguridad e Higiene en el Trabajo; 1994. Available from: https://www.insst.es/documents/94886/326853/ntp_355.pdf.
2. Pérez-Valdecantos D, Caballero-García A, Del Castillo-Sanz T, Bello HJ, Roche E, Córdova A. Stress salivary biomarkers variation during the work day in emergencies in healthcare professionals. Int J Environ Res Public Health. 2021;18(8):3937. doi:10.3390/ijerph18083937
3. Mirzaei A, Mozaffari N, Habibi Soola A. Corrigendum to «Occupational stress and its relationship with spiritual coping among emergency department nurses and emergency medical services staff» [Int. Emergency Nurs. 62 (2022) 101170]. Int Emerg Nurs. 2022;(64):101187. doi:10.1016/j.ienj.2022.101187
4. de Quirós-Aragón MB. Evaluación del estrés laboral y burnout en los servicios de urgencia extrahospitalaria. Int J Clin Health Psychol. 2007;7(2):323–335.
5. Araújo AF, Bampi LN, Cabral CC, Queiroz RS, Calasans LHB, Vaz TS. Occupational stress of nurses from the mobile emergency care service. Rev Bras Enferm. 2020;73:e20180898. doi:10.1590/0034-7167-2018-0898
6. Rajabi F, Jahangiri M, Molaeifar H, Honarbakhsh M, Farhadi P. Occupational stress among nurses and pre-hospital emergency staff: application of fuzzy analytic hierarchy process (FAHP) method. EXCLI J. 2018;17:808–824. doi:10.17179/excli2018-1505
7. Lazarus S, Folkman S. Estrés y procesos cognitivos. Biblioteca de Piscología, Psiquiatría y Salud. Universidad; 1986.
8. Lazarus RS, Launier R. Stress-related transactions between person and environment. In: Pervin LA, Lewis M, editors. Perspectives in Interactional Psychology. New York: Plenum; 1978:287–327. doi:10.1007/978-1-4613-3997-7_12
9. Rodríguez Campuzano ML, Ocampo-Juarez IY, Nava-Quiroz CN. Relación entre valoración de una situación y capacidad para enfrentarla. Summa Psicológica UST. 2009;6(1):25–41. doi:10.18774/448x.2009.6.50
10. Portero de la Cruz S, Cebrino J, Herruzo J, Vaquero-Abellán M. A multicenter study into burnout, perceived stress, job satisfaction, coping strategies, and general health among emergency department nursing staff. J Clin Med. 2020;9(4):1007. doi:10.3390/jcm9041007
11. González-Martínez A. Prevención de Riesgos Laborales en Servicios de Urgencias Prehospitalarias. Master project. Alicante, Spain: Universidad Miguel Hernández; 2016. Available from: http://dspace.umh.es/bitstream/11000/3276/1/Gonzalez%20Martinez%2C%20Ana%20TFM.pdf%20Hecho.pdf.
12. EU-OSHA. Return to Work after sick leave due to mental health problems; 2020. Available from: https://oshwiki.osha.europa.eu/en/themes/return-work-after-sick-leave-due-mental-health-problems.
13. Figueredo JM, García-Ael C, Gragnano A, Topa G. Well-Being at Work after Return to Work (RTW): a Systematic Review. Int J Environ Res Public Health. 2020;17(20):7490. doi:10.3390/ijerph17207490
14. Official Journal of the European Union. Decision No 1672/2006/EC of the European Parliament and of the Council of 24 October 2006 establishing a Community Programme for Employment and Social Solidarity — progress. Available from: https://eur-lex.europa.eu/eli/dec/2006/1672/oj.
15. García-Iglesias JJ, Gómez-Salgado J, Martín-Pereira J, et al. Impacto del SARS-CoV-2 (Covid-19) en la salud mental de los profesionales sanitarios: una revisión sistemática [Impact of SARS-CoV-2 (Covid-19) on the mental health of healthcare professionals: a systematic review.]. Rev Esp Salud Publica. 2020;94:e202007088. Spanish. PMID: 32699204.
16. Cano Vindel A. Repercusiones psicopatológicas de los atentados del 11.M en Madrid. Clínica y Salud. 2004;15(3):293–304.
17. Barroeta Urquiza J, Boada Bravo N Los servicios de emergencia y urgencias médicas extrahospitalarias en España. Mensor: Madrid; 2011. Available from: http://www.epes.es/wp-content/uploads/Los_SEM_en_Espana.pdf.
18. SUMMA 112. ¿Cómo trabajar en el SUMMA 112? SUMMA 112; 2019. Available from: https://www.comunidad.madrid/hospital/summa112/profesionales/trabajar-summa112.
19. Olsson M, Svensson A, Andersson H, et al. Educational intervention in triage with the Swedish triage scale RETTS©, with focus on specialist nurse students in ambulance and emergency care - A cross-sectional study. Int Emerg Nurs. 2022;63:101194. doi:10.1016/j.ienj.2022.101194
20. Ribeiro LB, Silveira CP, Castanheira CHC. Nurses’ roles in mobile prehospital care services in Brazil: integrative review. J Nurs UFPE Line. 2015;9(8):8882–8889. doi:10.5205/reuol.7696-67533-1-SP-1.0908201516
21. Dadashzadeh A, Rahmani A, Hassankhani H, Boyle M, Mohammadi E, Campbell S. Iranian pre-hospital emergency care nurses’ strategies to manage workplace violence: a descriptive qualitative study. J Nurs Manag. 2019;27(6):1190–1199. doi:10.1111/jonm.12791
22. Forsell L, Forsberg A, Kisch A, Rantala A. Specialist ambulance nurses’ perceptions of nursing: a phenomenographic study. Int J Environ Res Public Health. 2020;17(14):5018. doi:10.3390/ijerph17145018
23. Wihlborg J, Edgren G, Johansson A, Sivberg B. The desired competence of the Swedish ambulance nurse according to the professionals–a Delphi study. Int Emerg Nurs. 2014;22(3):127–133. doi:10.1016/j.ienj.2013.10.004
24. Hörberg A, Wälivaara BM, Wihlborg J. Taking or creating control: a qualitative study of uncertainty among novice nurses in ambulance care. Int Emerg Nurs. 2023;69:101308. doi:10.1016/j.ienj.2023.101308
25. Bos N, Krol M, Veenvliet C, Plass AM Ambulance care in Europe. Organization and practices of ambulance services in 14 European countries. Utrecht, The Netherlands: NIVEL; 2015. Available from: https://www.nivel.nl/sites/default/files/bestanden/Rapport_ambulance_care_europe.pdf.
26. van der Velden PG, Bosmans MW, van der Meulen E. Predictors of workplace violence among ambulance personnel: a longitudinal study. Nurs Open. 2015;3(2):90–98. doi:10.1002/nop2.38
27. Mirzaei A, Mozaffari N, Habibi Soola A. Occupational stress and its relationship with spiritual coping among emergency department nurses and emergency medical services staff. Int Emerg Nurs. 2022;62:101170. doi:10.1016/j.ienj.2022.101170
28. Bohström D, Carlström E, Sjöström N. Managing stress in prehospital care: strategies used by ambulance nurses. Int Emerg Nurs. 2017;32:28–33. doi:10.1016/j.ienj.2016.08.004
29. James A. Perceptions of stress in British ambulance personnel. Work Stress. 1988;2(4):319–326. doi:10.1080/02678378808257493
30. Sterud T, Hem E, Lau B, Ekeberg Ø. A comparison of general and ambulance specific stressors: predictors of job satisfaction and health problems in a nationwide 38 one-year follow-up study of Norwegian ambulance personnel. J Occup Med Toxicol Lond Engl. 2011;6:10. doi:10.1186/1745-6673-6-10
31. Sterud T, Hem E, Ekeberg Ø, Lau B. Occupational stressors and its organizational and individual correlates: a nationwide study of Norwegian ambulance personnel. BMC Emerg Med. 2008;8(1):16. doi:10.1186/1471-227X-8-
32. Boudreaux E, Mandry C. Sources of stress among emergency medical technicians (Part I): what does the research say? Prehospital Disaster Med. 1996;11(4):296–301. doi:10.1017/s1049023x00043168
33. Van der Ploeg E. Acute and chronic job stressors among ambulance personnel: predictors of health symptoms. Occup Environ Med. 2003;90001:40i–46. doi:10.1136/oem.60.suppl_1.i40
34. Maguire BJ, O’Meara P, O’Neill BJ, Brightwell R. Violence against emergency medical services personnel: a systematic review of the literature. Am J Ind Med. 2018;61(2):167–180. doi:10.1002/ajim.22797
35. Alameddine M, Kazzi A, El-Jardali F, Dimassi H, Maalouf S. Occupational violence at Lebanese emergency departments: prevalence, characteristics and associated factors. J Occupa Health. 2011;53:455–464. doi:10.1539/joh.11-0102-OA
36. Bernaldo-De-Quirós M, Piccini AT, Gómez MM, Cerdeira JC. Psychological consequences of aggression in pre-hospital emergency care: cross sectional survey. Int J Nurs Stud. 2015;52(1):260–270. doi:10.1016/j.ijnurstu.2014.05.011
37. Gómez-Gutiérrez MM, Bernaldo-de-Quirós M, Piccini AT, Cerdeira JC. Posttraumatic stress symptomatology in pre-hospital emergency care professionals assaulted by patients and/or relatives: importance of severity and experience of the aggression. J Interpers Violence. 2016;31(2):339–354. doi:10.1177/0886260514555370
38. Soravia LM, Schwab S, Walther S, Müller T. Rescuers at Risk: posttraumatic stress symptoms among police officers, fire fighters, ambulance personnel, and emergency and psychiatric nurses. Front Psychiatry. 2021;11:602064. doi:10.3389/fpsyt.2020.602064
39. Ministerio de Sanidad y Política Social. Orden SAS/1348/2009, de 6 de mayo, por la que se aprueba y publica el programa formativo de la especialidad de Enfermería del Trabajo; 2009. 44685–44696. Available from: https://www.boe.es/eli/es/o/2009/05/06/sas1348.
40. Corbelle Álvarez JM. La Enfermería del Trabajo, una especialidad reciente, una Profesión de siempre. Med Segur Trab. 2009;55(215):10–11.
41. Romero Saldaña M, Moreno Pimentel AG, Santos Posada A. Enfermería del Trabajo: competencia y experiencia para alcanzar la seguridad, la salud y el bienestar de la población laboral. Enferm Clín. 2019;29(6):376–380. doi:10.1016/j.enfcli.2019.09.012
42. Colegio de Enfermería de Alicante. Enfermería del Trabajo. Web del Colegio Oficial de Enfermería de Alicante; 2023. Available from: https://www.enferalicante.org/enfermeria_trabajo.php.
43. Afshari A, Borzou SR, Shamsaei F, Mohammadi E, Tapak L. Emergency medical service providers’ perception of health-threatening stressors in emergency missions: a qualitative study. Ethiop J Health Sci. 2021;31(3):517–524. doi:10.4314/ejhs.v31i3.8
44. Hendel T, Fish M, Aboudi S. Strategies used by hospital nurses to cope with a national crisis: a manager’s perspective. Int Nurs Rev. 2000;47(4):224–231. doi:10.1046/j.1466-7657.2000.0004
45. Vicente V, Jansson J, Wikström M, Danehorn E, Rubenson Wahlin R. Prehospital Emergency Nurses’ coping strategies associated to traumatic experiences. Int Emerg Nurs. 2021;59:101083. doi:10.1016/j.ienj.2021.101083
46. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
47. Jordan Z, Lockwood C, Munn Z, Aromataris E. The updated Joanna Briggs Institute model of evidence-based healthcare. Int J Evid Based Healthcare. 2019;17(1):58–71. doi:10.1097/XEB.0000000000000155
48. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI;2020. doi:10.46658/JBIMES-20-08
49. Barker TH, Stone JC, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
50. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. 2015;13(3):179–187. doi:10.1097/XEB.0000000000000062
51. Aisling M, Aisling D, David C. An assessment of psychological need in emergency medical staff in the northern health and social care trust area. Ulster Med J. 2016;85(2):92–98.
52. Guise JM, Hansen M, O’Brien K, et al. Emergency medical services responders’ perceptions of the effect of stress and anxiety on patient safety in the out-of-hospital emergency care of children: a qualitative study. BMJ Open. 2017;7(2):e014057. doi:10.1136/bmjopen-2016-014057
53. Carvalho AEL, Frazão I, Silva DMR, Andrade MS, Vasconcelos SC, Aquino JM. Stress of nursing professionals working in pre-hospital care. Rev Bras Enferm. 2020;73:e20180660. doi:10.1590/0034-7167-2018-0660
54. Mahdizadeh M, Jaberi AA, Bonabi TN. Massage therapy in management of occupational stress in emergency medical services staffs: a randomized controlled trial. Int J Ther Massage Bodyw. 2019;12(1):16–22.
55. Khazaei A, Esmaeili M, Navab E. The most and least stressful prehospital emergencies from emergency medical technicians’ view point; a cross-sectional study. Arch Acad Emerg Med. 2019;7(1):e20.
56. Westphal M, Bingisser MB, Feng T, et al. Protective benefits of mindfulness in emergency room personnel. J Affect Disord. 2015;175:79–85. doi:10.1016/j.jad.2014.12.038
57. Kłosiewicz T, Zalewski R, Dąbrowski M, et al. Emergency healthcare providers perception of workplace dangers in the Polish emergency medical service: a multi-centre survey study. Disaster Emerg Med J. 2019;4(4):166–172. doi:10.5603/DEMJ.a2019.0030
58. McDermid F, Peters K. Factors contributing to high turnover rates of emergency nurses: a review of the literature. Aust Crit Care. 2020;33(4):390–396. doi:10.1016/j.aucc.2019.09.002
59. Lawn S, Roberts L, Willis E, Couzner L, Mohammadi L, Goble E. The effects of emergency medical service work on the psychological, physical, and social well-being of ambulance personnel: a systematic review of qualitative research. BMC Psychiatry. 2020;20(1):348. doi:10.1186/s12888-020-02752-4
60. Navarro-Abal Y, Climent-Rodríguez JA, Vaca-Acosta RM, Fagundo-Rivera J, Gómez-Salgado J, García-Iglesias JJ. Workplace violence: impact on the commitment and involvement of nurses at work. J Nurs Manage. 2023;9987092. doi:10.1155/2023/9987092
61. Poljak A, Tveith J, Ragneskog H. Nursing in the prehospital emergency care – first link in the chain of caring. Nordic J Nurs Res. 2006;26(1):48–51. doi:10.1177/010740830602600110
62. Gentil RC, Ramos LH, Whitaker IY. Nurses’ training in prehospital care. Rev Lat Am Enfermagem. 2008;16(2):192–197. doi:10.1590/s0104-11692008000200004
63. Jiaru J, Yanxue Z, Wennv H. Incidence of stress among emergency nurses: a systematic review and meta-analysis. Medicine. 2023;102(4):e31963. doi:10.1097/MD.0000000000031963
64. Grochowska A, Gawron A, Bodys-Cupak I. Stress-inducing factors vs. the risk of occupational burnout in the work of nurses and paramedics. Int J Environ Res Public Health. 2022;19(9):5539. doi:10.3390/ijerph19095539
65. Gómez-Salgado J, Fagundo-Rivera J, Ortega-Moreno M, Allande-Cussó R, Ayuso-Murillo D, Ruiz-Frutos C. Night work and breast cancer risk in nurses: multifactorial risk analysis. Cancers. 2021;13(6):1470. doi:10.3390/cancers13061470
66. Fagundo-Rivera J, Gómez-Salgado J, García-Iglesias JJ, Allande-Cussó R, Ortega-Moreno M, Ruiz-Frutos C. Trabajo, familia y percepción de la propia salud en las enfermeras: relación con el cáncer de mama y el trabajo a turnos [Work, family and nurses perception about their own health: relationship with breast cancer and shift work.]. Rev Esp Salud Publica. 2021;95:e202106078.
67. Önnheim S, Johansson A, Ivarsson B, Hagström C. Self-perceived competence of ambulance nurses in the care of patients with mental illness: a questionnaire survey. Nurs Rep. 2022;12(1):226–234. doi:10.3390/nursrep12010023
68. Elder EG, Johnston A, Wallis M, Crilly J. Work-based strategies/interventions to ameliorate stressors and foster coping for clinical staff working in emergency departments: a scoping review of the literature. Australas Emerg Care. 2020;23(3):181–192. doi:10.1016/j.auec.2020.02.002
69. Jones S. Describing the Mental health profile of first responders: a systematic review. J Am Psychiatr Nurs Assoc. 2017;23(3):200–214. doi:10.1177/1078390317695266
70. Adriaenssens J, De Gucht V, Maes S. Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud. 2015;52(2):649–661. doi:10.1016/j.ijnurstu.2014.11.004
71. Lazarus RS. Stress and coping as factors in health and illness. In: Cohen J, Cullen SW, Martin LR, editors. Psychosocial Aspects of Cancer. New York: Raven Press; 1982.
72. Cohen F, Lazarus RS. Coping with Stresses of Illness. In: Stone GC, Cohen F, Adler NE, editors. Health Psychology: A Handbook. San Francisco: Jossy-Bass; 1979:217–254.
73. Organización Mundial de la Salud. Directrices de la OMS sobre salud mental en el trabajo: resumen ejecutivo. Organización Mundial de la Salud; 2022. Available from: https://apps.who.int/iris/handle/10665/363173.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Improving Nurses’ Knowledge on Sepsis Identification and Management at Mulago National Referral Hospital: A Quasi Experimental Study
Nakiganda C, Atukwatse J, Turyasingura J, Niyonzima V
Nursing: Research and Reviews 2022, 12:169-176
Published Date: 14 September 2022
Grip Strength Among Indian Nursing Students and Staff: A Cross-Sectional Study
Sadan V, Seetharaman B, Jesudoss I, Esther A, Roberts LR
Nursing: Research and Reviews 2023, 13:31-39
Published Date: 3 October 2023
Factors Influencing Occupational Stress of State Security Forces During the COVID-19 Pandemic: A Scoping Review
García-Iglesias JJ, Chirico F, Rizzo A, Szarpak L, Khabbache H, Yildirim M, Fagundo-Rivera J, Gómez-Salgado J
Risk Management and Healthcare Policy 2024, 17:2851-2868
Published Date: 20 November 2024
Paramedics Satisfaction with Simulation Experience for Career Development and Skills Maintenance
Alshibani A, Alburaidi AS, Alsukait MA, Albadr R, Alsubaie BK, Almutairi A, Almutairi S, AlHussaini Z
Advances in Medical Education and Practice 2025, 16:245-253
Published Date: 19 February 2025
Evaluating Quality of Care in Emergency Departments: Perspectives of Patients’ and Health Professionals in Saudi Arabia
Hobani MA, Almarashi AA, Dammas AH, Khusheim LH, Murshid GA, Alahmadi TG, Kattan WM, Alasmari KA
Open Access Emergency Medicine 2025, 17:313-321
Published Date: 26 October 2025