")
Back to Journals » International Journal of Women's Health » Volume 12
Factors Associated with Treatment Uptake Among Women with Acetic Acid/Lugol’s Iodine Positive Lesions of the Cervix in Cameroon
Authors Manga SM , Shi L , Welty TK , DeMarco RF , Aronowitz T
Received 13 February 2020
Accepted for publication 9 June 2020
Published 25 June 2020 Volume 2020:12 Pages 495—504
DOI https://doi.org/10.2147/IJWH.S249607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Simon M Manga,1– 3 Ling Shi,1 Thomas K Welty,2 Rosanna F DeMarco,1 Teri Aronowitz1
1College of Nursing and Health Sciences, University of Massachusetts Boston, Boston, MA, USA; 2Cameroon Baptist Convention Health Services, Bamenda, Cameroon; 3Center for Women’s Reproductive Health, Department of Obstetrics and Gynecology, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Simon M Manga Tel +237 671863768
Email [email protected]
Purpose: Treatment of cervical precancer is the primary aim in secondary prevention of cervical cancer. The purpose of this study was to examine factors associated with treatment uptake among women with acetic acid/Lugol’s iodine positive lesions identified by digital cervicography (DC) in a cervical cancer prevention program in Cameroon.
Patients and Methods: We conducted a cross-sectional survey of medical records from 2013 to 2018 of 755 women in Cameroon who screened positive with acetic acid/Lugol’s iodine in 2013.
Results: Of the 755 women, 422 (55.9%) had treatment/biopsy on the same day or followed up later, but only 344 (45.6%) received treatment/biopsy and 333 (44.1%) were lost to follow-up. Overall, 180 (52.3%) of the 344 women were treated/biopsied the same day they were screened, and 164 (47.7%) were treated/biopsied after the initial visit. Women aged 30– 49 and HIV-positive women were significantly more likely to have received treatment or returned for treatment than women less than 30 and HIV-negative women. Of the 266 women who followed up at a later date, the lesions of 78 (29.3%) women regressed spontaneously without treatment. Women with low-grade lesions, HIV-negative women and women who had follow-up more than a year after the initial exam were significantly more likely to have spontaneous regression with regression rates of 30.6%, 32.1% and 62.2%, respectively (p< 0.001). Age was not a significant determinant of spontaneous regression (p=0.149).
Conclusion: Efforts to increase treatment uptake are needed in this population, including adherence to same day “See and treat” policies.
Keywords: cervical precancer, treatment uptake, cameroon, cryotherapy, thermal ablation, loop electrosurgical excision procedure
Introduction
Cervical precancer can usually be diagnosed through screening1 and can be effectively treated by cryotherapy/thermal ablation or Loop Electrosurgical Excision Procedure (LEEP) with a cure rate of almost 100%.2,3 Women who screen positive for cervical precancer and are not treated are at risk of developing invasive cervical cancer (ICC). In sub-Saharan Africa (SSA) and other developing settings, it is difficult to get women back for treatment after screening positive for cervical precancer.4 Understanding the factors that contribute to the lack of treatment uptake is a significant factor in cervical cancer secondary prevention and policy development.
A literature search was performed through PubMed to identify the variables that are likely to be associated with treatment uptake. For this study, we defined treatment uptake to include women with visual inspection with acetic acid (VIA) or visual inspection with Lugol’s iodine (VILI) positive cervical lesions detected by digital cervicography (DC) who received same day treatment or treatment during a follow-up visit or who returned for a follow-up visit and were found to have spontaneous regression of their cervical lesions. The variables that emerged were classified using a systems model where personal, environmental, and clinical factors were identified.5 The personal factors that were explored included age, level of education, marital status, employment status, income, and health status, including human immunodeficiency virus (HIV) status and severity of the precancer. Lower education levels have been shown to be associated with lower rates of treatment uptake.6 Individuals who are HIV positive have a higher incidence rate of cervical precancer and have a treatment failure rate of 51% for low-grade lesions and 55% for high-grade lesions.7 The major environmental factor examined in this study was the distance from home to the clinic. It has been found that the farther women live from the clinic, the lower the treatment uptake rates.6 Specific factors related to clinic characteristics include location and type of clinic.
The largest cervical cancer prevention program in Cameroon is administered by the Women’s Health Program (WHP) of the Cameroon Baptist Convention Health Services (CBCHS). The CBCHS is a large faith-based health organization that has a network of 82 health facilities in eight of the 10 regions of Cameroon. The WHP has screened over 100,000 women for cervical cancer and has treated over 5000 for cervical precancer. The WHP has a documented 9% prevalence for cervical precancer and 613 per 100,000 prevalence rates for ICC among women screened by VIA and VILI enhanced by digital cervicography (DC).4 For comparison, the Cervical Cancer Prevention Program in Zambia had similar detection rates for ICC (690 per 100,000 women screened).8 Consequently, it is reasonable to assume that cervical cancer screening programs in SSA will likely detect one ICC for every 150 women who are screened. Since appropriate treatment for ICC is often not available nor affordable in Cameroon,9 screening programs should intensify diagnoses, treatment, and follow-up women wish positive cervical lesions as timely and efficiently as possible in a manner acceptable, affordable, and accessible to this population.
The type of treatment offered depends on the characteristics of the lesion. Lesions that are small and meet criteria for treatment with cryotherapy are called cryotherapy-eligible lesions, while bigger lesions that meet criteria for treatment by LEEP are called LEEP-eligible lesions.2 The WHP has adopted the “see-and-treat” approach where women who screen positive for cryotherapy-eligible lesions are treated on the same day of diagnoses with cryotherapy or thermal ablation.3,4 Women with LEEP-eligible lesions are scheduled for treatment by appointment at facilities where surgical intervention can be done to control bleeding, if necessary. Lesions suspicious for cancer are biopsied for histopathological confirmation. This descriptive study aimed to examine the determinants associated with treatment uptake among women diagnosed with VIA/VILI cervical lesions in Cameroon.
Patients and Methods
Ethical Consideration
This secondary analysis of clinical data from the WHP received Institutional Review Board (IRB) approval from University of Massachusetts Boston (UMB), United States (US) and the CBCHS IRB, which constituted ethical approval of the study. Thus, the data accessed complied with relevant patient data protection rules and guidelines.
Study Population and Procedure
A descriptive cross-sectional design was used to examine five years of data from 2013 through 2018 of 755 women diagnosed with VIA/VILI cervical lesions in 2013 in Cameroon. The data analyzed were collected from electronic and paper medical records. The WHP designed its database to provide ongoing access to clinically useful data, as well as for program monitoring and evaluation.
A checklist and data codebook were developed using the factors from the systems model that pertain and were sent to the WHP data manager, and she was instructed to develop a dataset with these variables. Clinic registers were consulted in cases where variables were missing in the database. The dataset was deidentified for analyses.
WHP performs cervical cancer screening with a technique known as digital cervicography (DC), which is an adjunct to VIA and VILI. In DC, a digital camera with a macro-conversion lens or a Samsung Galaxy S4, or S6, or J8 cell phone is utilized to take highly magnified real-time images of the cervix, which are projected onto a television screen, so that both the woman and the provider see the cervix live on the screen at the same time; mimicking video colposcopy.10 In WHP, the nurses perform a biopsy on VIA/VILI lesions when they are uncertain about the diagnosis or optimal treatment. The WHP followed the World Health Organization (WHO) guidelines for the “see-and-treat” approach for treatment and follow-up.3
All women who screened positive by VIA/VILI from January 1st to December 31st 2013 were included in the study irrespective of age. However, in Cameroon, eligibility age for screening with VIA/VILI is 25 to 65. Though WHP is now performing human papillomavirus (HPV) testing, HPV testing was not done in the 2013 cohort. Their medical records were reviewed for five years to assess treatment uptake. Women with HIV unknown status were excluded, because we were interested in the comparison between HIV positive and negative women. Women with lesions suspicious for ICC were also excluded from the study, because the recommendations for treatment and follow-up differ from those for precancers.
Measures
The independent variables were classified into personal, environmental, and clinic variables. The following is a list of the personal variables and how they were coded: age (<30, 30 to 39, 40–49, and ≥50); educational level (0–7yrs, 8–12yrs, 13–14yrs, 15–17yrs, and ≥18yrs); marital status (single, married/cohabiting, widowed, separated, and divorce); employment (employed versus unemployed); health status which included the characteristics of the VIA/VILI lesion (high-grade versus low-grade), and HIV status (positive versus negative). Women with unknown HIV status were excluded from the study. The environmental variable of distance from the clinic was coded with respect to whether the woman lived in the city where the clinic was located or not. The clinic variables that were available in the dataset included the location of the clinic (rural versus urban) and type of clinic (stationary versus mobile).
The dependent variables for this study were treatment uptake and spontaneous lesion regression. Treatment uptake included women who received same-day treatment or who returned for treatment at a later date irrespective of whether or not they were treated. Some of the women were not treated because their lesions were found to have regressed spontaneously, but they were still counted under treatment uptake because of the fact that they showed up.
Data Analysis
Chi-square tests were used to compare participants’ characteristics by treatment status. Variables with p<0.05 in the bivariate analysis were included in the multivariable analyses. The proportion of women who received treatment in the first year and between the second year and the end of five years were calculated. Proportions of women with cryotherapy-eligible lesions who received same-day treatment and proportions of women with LEEP-eligible lesions who received treatment within the first two months were also calculated. A binary logistic regression model was used to model the log odds for treatment uptake. Firstly, simple logistic regression analysis with just one predictor at a time was performed with treatment uptake as the dependent variable. Secondly, the predictors in the simple logistic regression model that had statistical significance were entered into a multivariable logistic model with treatment uptake and spontaneous lesion regression as the dependent variables. The predictors were those collected at enrollment. The data were summarized using odds ratios (ORs) with p-values and 95% confidence interval (CI). All underlying assumptions regarding multivariable regression models were met. The data were normally distributed, and the variables added to the multivariable model had significant relationships. A backward stepwise selection was completed, using p-value >0.2 as removal criterion. All statistical analyses were performed using Stata version 15 (Stata Corp, College Station, TX, USA).
Results
Sample
In 2013, WHP screened a total of 8283 women for cervical cancer. There were 127 women who reported they did not know their HIV status and were excluded. Seven hundred and fifty-five women met the inclusion criteria for the study. The mean age of the women in the sample was 34.8 years (standard error[SE 0.3]). The majority of the women were between 30 and 39 years of age (44.5%), were married 493 (65.7%), and had less than eight years of education 372 (51.5%). There were 141 (18.7%) women who reported living with HIV.
Types of Lesions and Treatment
Of the 8283, 926 (11.2%) had a positive screen, that is either lesions suspicious for ICC or VIA/VILI lesions. Of those, 882 (95.3%) had VIA/VILI lesions. Of the 755 women included in the study, 602 (79.7%) had cryo-eligible lesions and 153 (20.2%) had LEEP-eligible lesions. A total of 344 (45.6%) women included in the study received treatment/biopsy. Among those who followed up for treatment, 180 (42.7%) had same-day treatment/biopsy. Of the 344 women who received treatment, 28 (8%) were treated with LEEP and the other 316 (92%) were treated by cryotherapy, thermal ablation, or had a biopsy. A total of 28 biopsies were performed (Table 1).
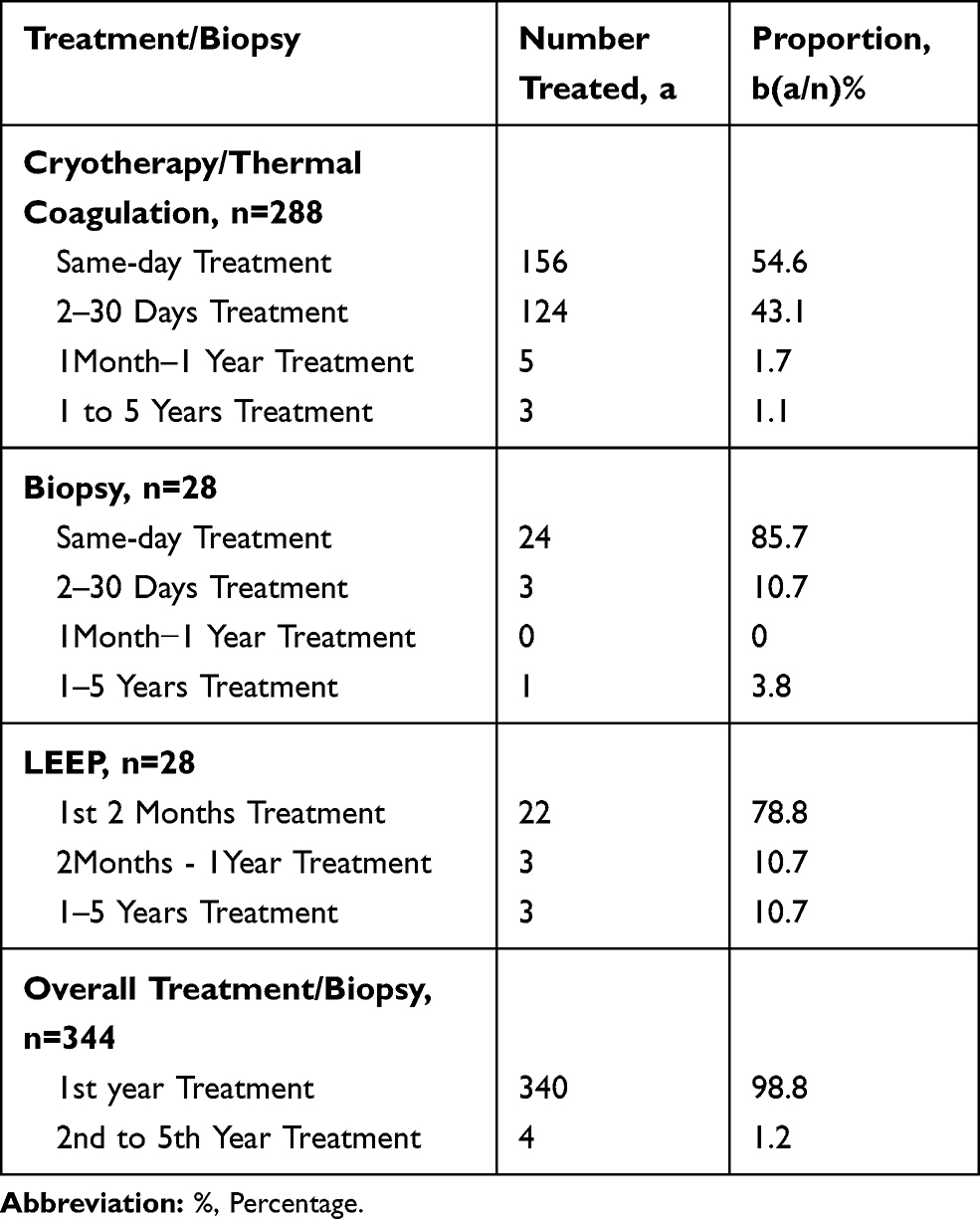 |
Table 1 Treatment/Biopsy Proportions |
Age
Women younger than age 30 were the least likely to return for treatment, whereas women aged 40–49 were the most likely to follow-up for treatment (Table 2). In the logistic regression with treatment uptake as the dependent variable, age was the most significant predictor (Table 3). In the multivariate model, 83% of women 30–39 had treatment uptake compared to 61% of women less than 30 [adjusted odds ratio (AOR=1.61, p=0.006, 95% CI 1.14–2.26)] (Table 4).
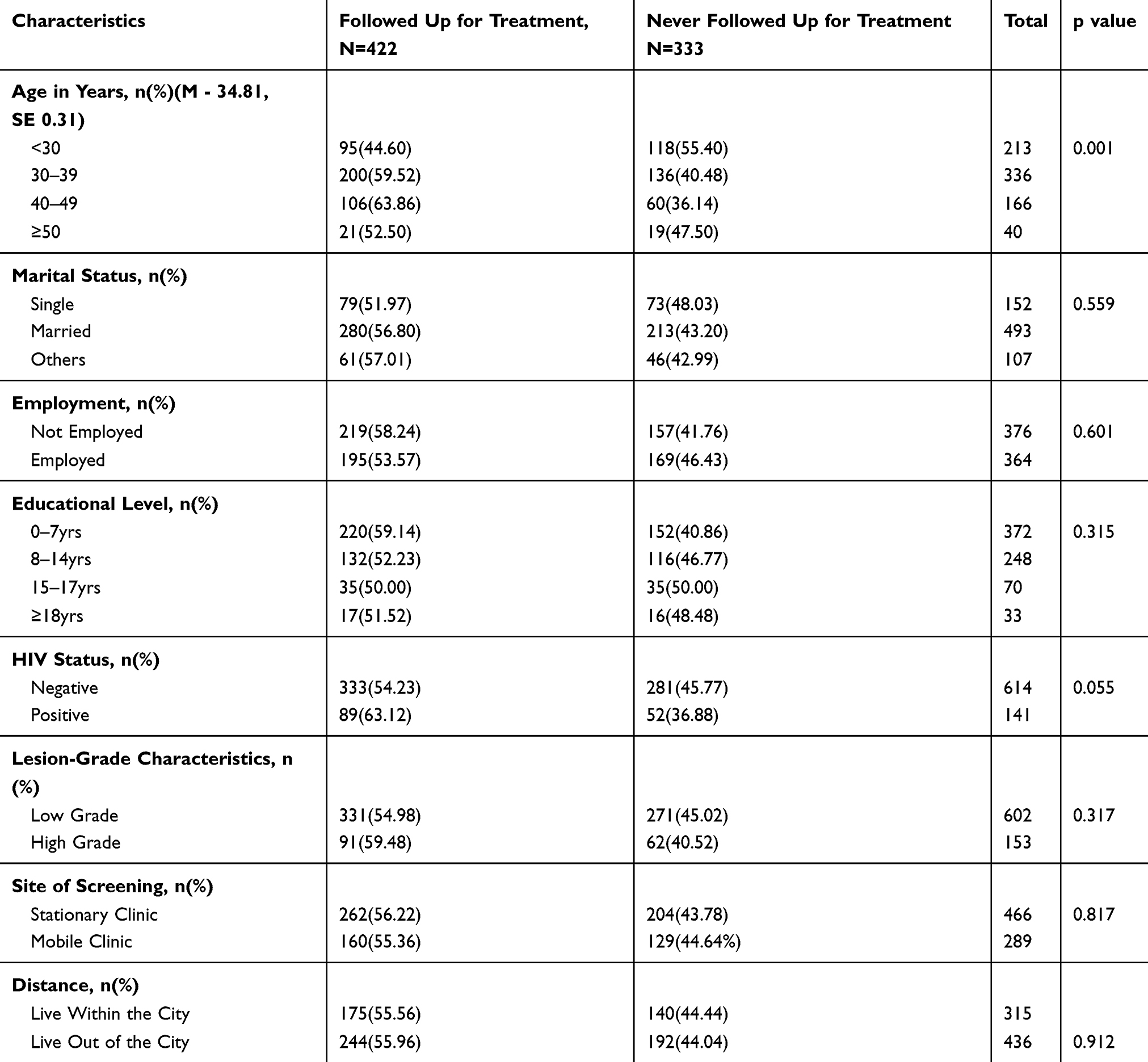 |
Table 2 Participants Characteristics at Enrollment According to Treatment Follow-Up (N=755) |
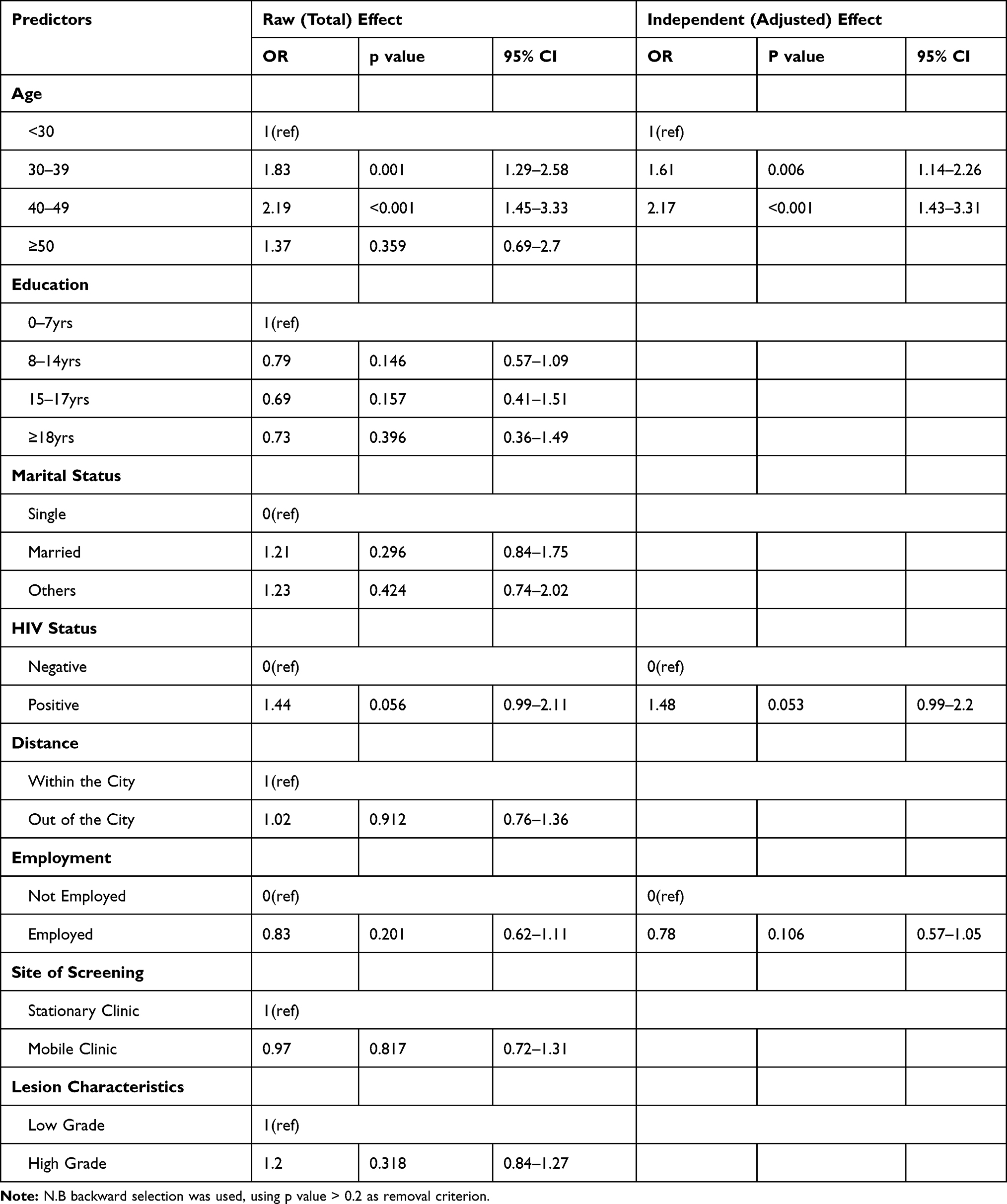 |
Table 3 Logistic Regression of Predictors for Treatment Follow-Up |
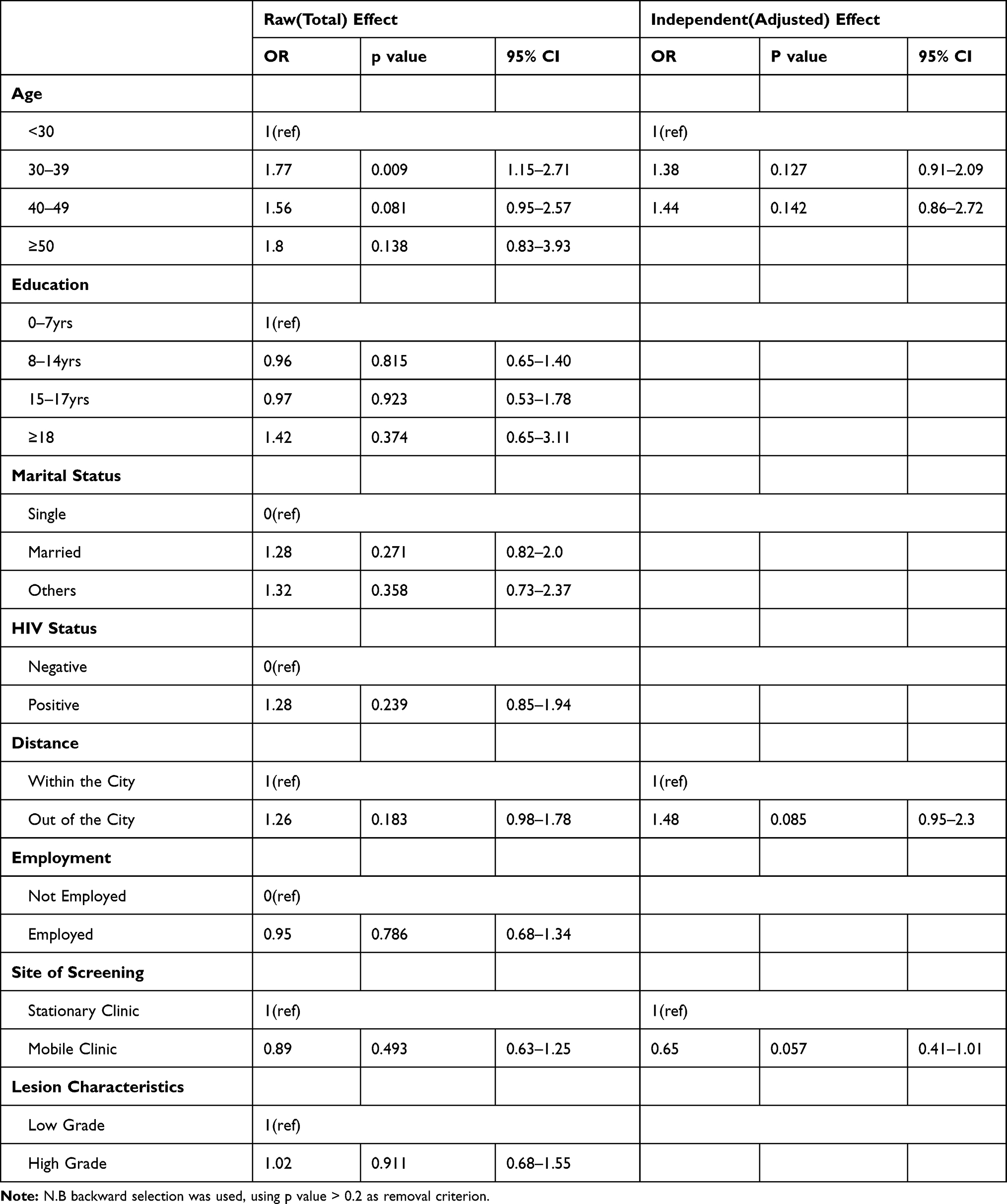 |
Table 4 Logistic Regression of Predictors for Same-Day Treatment |
Lesion Regression
Of the 266 women who returned for treatment at a later date, interestingly, the lesions of 78 (29.3%) (Table 5) had regressed. Of those, 39 (50%) were still treated despite lesion regression. Spontaneous lesion regression was a serendipitous finding of this study. Spontaneous lesion regression represents the cervixes that had VIA/VILI positive lesions at the initial visit and who screened negative with VIA/VILI at the follow-up visit. Women who had low-grade lesions at the initial exam, those who had follow-up more than a year after the initial exam, and those who were HIV negative (p < 0.001), were significantly more likely to have spontaneous regression. Age was not a significant determinant of spontaneous regression (p=0.149).
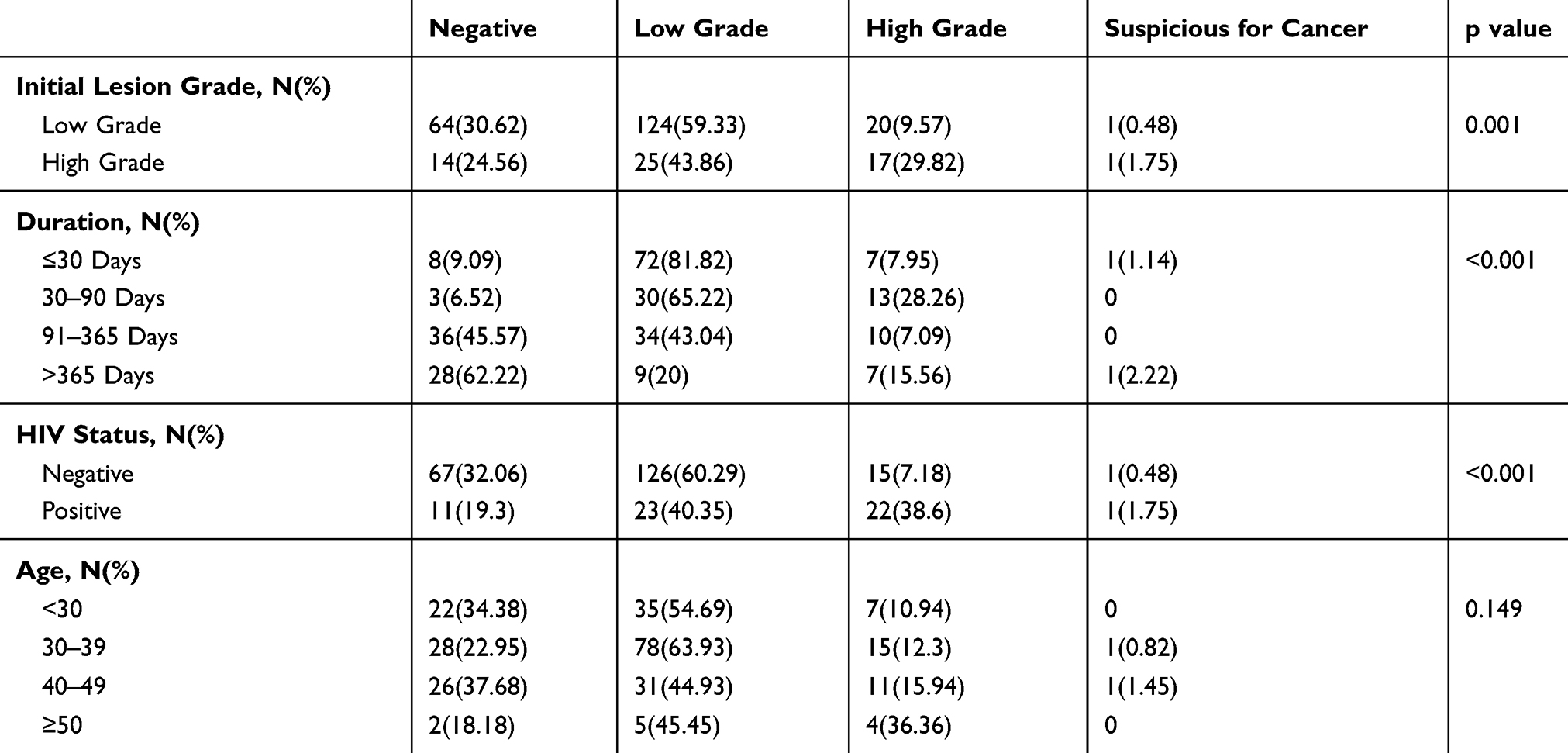 |
Table 5 Results of Treatment Follow-Up Visit Showing Spontaneous Lesion Regression n=266 |
Discussion
The total percentage of women that did not follow-up for treatment in this sample was 44.1%, which is similar to the 47.2% of no treatment in Nigeria,6 but higher than the 36.5% in Cote d’Ivoire.11 Even though the rate is also similar to 40.8% in Zambia, we cannot directly compare because the Zambian rate applies only to women with LEEP-eligible lesions.12 Usually, LEEP is not provided on the day of diagnosis in a “see and treat” program. Older women were more likely to be treated than younger women. Contrary to this finding, a Nigerian study did not find any association between age and treatment uptake.6 In the Nigerian study, a significant proportion of the women who did not follow-up for treatment had less than secondary school education (OR: 2.9, 95% CI: 1.1–7.7). Whereas, educational level had no effect on treatment uptake in our study. Both the Nigerian study and this study did not find significant associations between marital or employment status with treatment uptake.
Even though WHP has implemented a “see and treat” cervical cancer prevention program, the rate of women who received same-day treatment/biopsy (180/755, 23.8%) was relatively low. In an earlier cross-sectional study analyzing data among women screened at WHP from 2007 to 2014, the rate of same-day treatment was 31.1%,4 higher than what we found for 2013 alone. “See and treat” programs are likely to work better in funded projects where treatment is offered at no charge. WHP has minimal external funding and thus relies on patients’ fees to sustain the program.13 Thus, women are expected to pay for their treatment. Cryotherapy and thermal ablation are offered at $20 to $60 while LEEP is offered at $60 to $150. In a recent qualitative study conducted among WHP nurses and clients, payment for treatment was identified as one of the major barriers to same-day treatment and post-treatment follow-up.14 In a “see and treat” program in Thailand, 98.5% (609/618) of the women with precancer received same-day treatment.15 However, in this Thailand study, it is not clear whether the treatment was provided at no charge or the women had to pay for it.
Regression of cervical precancer has been well documented.3 There is evidence that about 40% of CIN2 lesions will regress spontaneously over two years. In a recent US study where 356 HIV-negative women with cervical precancers were followed for three years, the researchers reported spontaneous lesion regression rate at 25.3%,16 lower than the regression rate in our study, which increased to 62.2% in women who came back more than a year after their initial exam. In a retrospective study among HIV-positive women with cervical precancer in the US, the spontaneous lesion regression rate within two years of follow-up was 31%,17 which is higher than the regression we found among women living with HIV (19.3%).
We found that HIV-negative women had a significantly higher regression rate (32.1%) than women living with HIV, which is consistent with other studies that documented a lower rate of lesion regression in women living with HIV than those who are HIV negative.16,17 Among various racial groups in the US, the black race was found to have the slowest expected times for lesion regression (49 months; 95% CI, 29.1–86.2).18 The highest regression rate (62%) in our study was among women whose follow-up exam was more than one year after their initial exam, most of whom were followed up within two years. Our data indicate that less than 10% of VIA/VILI lesions regress within 90 days of examination. Regression increases to 45% in the first year and then to 62% with two years (Table 5). However, 44% of women with VIA/VILI lesions in this study were not treated or followed up and even if most of the lesions in those women had regressed, many will persist and progress to ICC. Thus, same day treatment is still justified whenever possible to reduce the risk of progression to ICC, because ablative treatment with cryotherapy or thermal ablation have minimal side effects.
Although age was not significantly associated with spontaneous lesion regression in our study, young age was associated with lesion regression in other studies. In a retrospective study in Western Australia among women aged 18–24, the regression rates for CIN2 in two years was as high as 59.5% (95% CI 0.5–0.6).19 In a three-year follow-up study among 95 women aged 24 and younger with CIN2, 38% regressed within one year, 63% within two years, and 68% within three years.20 Although spontaneous lesion regression was a serendipitous finding in this study, it is not clear why there was no association between age and lesion regression. Nevertheless, in a study with an priori hypothesis on age and spontaneous lesion regression, the researchers did not find any such association.17
Interestingly, among the 78 women with spontaneous lesion regression, half (39) were still treated. So far, there is no protocol on how to manage women whose lesions regressed spontaneously in a “see and treat” program. It could have been an oversight of policymakers regarding the management of such women, because of the assumption that almost all women attending a “see and treat” program will receive treatment shortly after diagnosis. Considering that women successfully treated for precancer still carries a risk of up to 30% of developing ICC compared to women in the general population,21,22 it can also be inferred that the women whose lesions regressed spontaneously carry a similar risk, even though women with spontaneous lesion regression have not been sufficiently studied.
The progression from HPV infection to ICC begins with a precancer and the overall purpose of cervical cancer screening is to identify and treat the precancers.3 With the advent of HPV DNA tests, there has been a paradigm shift in cervical cancer prevention strategy from identifying just the precancer to identifying the presence of high-risk HPV on the cervix. When a woman is diagnosed with high-risk HPV and she has clearly defined precancer, the management is simple. Treat the lesion according to its presenting characteristics.3 On the other hand, if the woman is positive for high-risk HPV, but has no apparent lesion on examination with VIA, WHO has a dichotomous strategy for managing such cases depending on the likelihood of follow-up. First, if follow-up is uncertain, women with a positive high-risk HPV test should be treated with cryotherapy/thermal ablation, even if they have no apparent lesion with VIA. The second option is indicated for settings where follow-up is good, so that women who test positive for high-risk HPV and have no apparent lesion can be reliably followed up and treated if the lesion develops.23 In the case of the women in the present study with spontaneous lesion regression, in the absence of the capacity to provide HPV testing, it may be prudent to assume that the women are positive with high-risk HPV and provide them with treatment as per the WHO protocol for HPV “screen and treat” approach, especially, since we have documented that follow-up is not optimal.
Had WHP implemented a strict “see and treat” program, almost all 422 women who showed up for treatment would have been treated at the first visit and the issue on how to handle those with spontaneous lesion regression would not have arisen. However, this raises concerns for overtreatment. Over-treatment remains one of the main challenges of the “see and treat” approach.3 There is a burden on financial, material, and human resources when treating every VIA/VILI lesion, of which about 30% would regress spontaneously over time. Not only can the precancer regress, but even infection with high-risk HPV can resolve spontaneously. In another earlier study that was conducted in WHP, 44% of women with high-risk HPV infection had spontaneous clearance at one year.24
The major strength of this study is that it evaluates treatment uptake of a cohort of women with VIA/VILI lesions for up to five years in a LMIC.
Limitations
This study had some limitations. First, it is a review of medical records with data that was originally collected for clinical work and program evaluation, not for research. The HIV status in our cohort was self-reported. For reasons associated with sigma, some HIV-positive women might have reported their status as negative. As such, there could have been potential bias towards the null. Additionally, the dataset did not have other aspects of the systems model that could be affecting “see and treat” rates, as well as treatment uptake.
Conclusion
Treatment uptake is low among women with acetic VIA/VILI lesions in Cameroon. The main significant factors associated with treatment uptake are age and HIV status. Longitudinal prospective studies are needed to examine predictors for cervical precancer regression and same-day treatment uptake among women with VIA/VILI cervical lesions in Cameroon and sub-Saharan Africa. Secondary to the unanswered questions about the low treatment uptake rates, future studies should include issues such as financial barriers to treatment uptake. Spontaneous regression of cervical lesions needs to be considered in decisions related to optimal treatment.
Acknowledgments
The authors thank Ms. Nulah Kathleen and Ms. Ketu Comfort who assembled and deidentified the data that were used for the study. Dr. Edith Welty provided input into the study design, and Dr. Joel Fokom provided editorial assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wright TC, Cox TJ. Cervical cancer: epidemiology and etiology. In: Mayeaux EJ, Cox JT, editors. Modern Colposcopy: Textbook and Atlas.
2. Cox JT, Chelmow DP, Moscicki AB. Management of abnormal cervical cancer screening. In: Mayeaux EJ, Cox JT, editors. Modern Colposcopy: Textbook and Atlas.
3. World Health Organization (WHO). Comprehensive Cervical Cancer Control. December 2014. 2014;364. Available from: http://www.who.int/reproductivehealth/publications/cancers/cervical-cancer-guide/en/%5Cnwww.who.int.
4. DeGregorio GA, Bradford LS, Manga S, et al. Prevalence, predictors, and same day treatment of positive VIA enhanced by digital cervicography and histopathology results in a cervical cancer prevention program in Cameroon. PLoS One. 2016;11(6):e0157319. doi:10.1371/journal.pone.0157319
5. Neuman B. The Neuman systems model. In: Neuman B, Fawcett J, editors. The Neuman Systems Model.
6. Ezechi OC, Petterson KO, Gabajabiamila TA, et al. Predictors of default from follow-up care in a cervical cancer screening program using direct visual inspection in south-western Nigeria. BMC Health Serv Res. 2014;14(1). doi:10.1186/1472-6963-14-143
7. Reimers LL, Sotardi S, Daniel D, et al. Outcomes after an excisional procedure for cervical intraepithelial neoplasia in HIV-infected women. Gynecol Oncol. 2010;119(1):92–97. doi:10.1016/j.ygyno.2010.06.012
8. Parham GP, Mwanahamuntu MH, Kapambwe S, et al. Population-level scale-up of cervical cancer prevention services in a low-resource setting: development, implementation, and evaluation of the cervical cancer prevention program in Zambia. PLoS One. 2015;10(4):e0122169. doi:10.1371/journal.pone.0122169
9. Manga S, Kanjo M, Ngwa W. Challenges with cervical cancer treatment in Cameroon. Obstetrics Gynaecol Cases Rev. 2017;4(2):1–5. doi:10.23937/2377-9004/1410104
10. Manga S, Parham G, Nkoum B, et al. Cervical cancer screening in cameroon. J Low Genit Tract Dis. 2015;19(4):288–294. doi:10.1097/LGT.0000000000000133
11. Horo A, Jaquet A, Ekouevi D, et al. Cervical cancer screening by visual inspection in Cote d’Ivoire, operational and clinical aspects according to HIV status. BMC Public Health. 2012;12(1):237. doi:10.1186/1471-2458-12-237
12. Pfaendler KS, Mwanahamuntu MH, Sahasrabuddhe VV, et al. Management of cryotherapy-ineligible women in a “screen-and-treat” cervical cancer prevention program targeting HIV-infected women in Zambia: lessons from the field. Gynecol Oncol. 2008;110:402–407. doi:10.1016/j.ygyno.2008.04.031
13. Degregorio G, Manga S, Kiyang E, et al. Implementing a fee-for-service cervical cancer screening and treatment program in Cameroon: challenges and opportunities. Oncologist. 2017;22(7):850–859. doi:10.1634/theoncologist.2016-0383
14. Manga S, Kiyang E, Demarco RF. Barriers and facilitators of follow-up among women with precancerous lesions of the cervix in Cameroon: a qualitative pilot study. Int J Women’s Health. 2019;Volume 11:229–239. doi:10.2147/IJWH.S196112
15. Gaffikin L, Blumenthal PD, Emerson M, et al. Feasibility of a single visit approach to cervical cancer prevention: results from a demonstration project in rural Thailand. Lancet. 2003;361:814–820. doi:10.1016/s0140-6736(03)12707-9
16. Mark K, Frost A, Hussey H, et al. Rates of regression of cervical dysplasia between initial biopsy and excisional procedure in routine clinical practice. Arch Gynecol Obstet. 2019;299(3):841–846. doi:10.1007/s00404-018-5026-8
17. Lofgren SM, Tadros T, Herring-Bailey G, et al. Progression and regression of cervical Pap test lesions in an urban AIDS clinic in the combined antiretroviral therapy era: a longitudinal, retrospective study. AIDS Res Hum Retroviruses. 2015;31(5):508–513. doi:10.1089/aid.2014.0254
18. Martingano D, Renson A, Martingano AJ, et al. Variations in progression and regression of precancerous lesions of the uterine cervix on cytology testing among women of different races. J Am Osteopathic Assoc. 2018;8(1):8–18. doi:10.7556/jaoa.2018.003
19. Munro A, Spilsbury KA, Cohen P, et al. Spontaneous regression of CIN2 in women aged 18-24 years: a retrospective study of a state-wide population in Western Australia. Acta Obstet Gynecol Scand. 2015;95(3):291–298. doi:10.1111/aogs.12835
20. Moscicki AB, Ma Y, Wibbelsman C, et al. Rate of and risks for regression of CIN-2 in adolescents and young women. Obstet Gynecol. 2011;116(6):1373–1380. doi:10.1097/AOG.0b013e3181fe777f
21. Aerssens A, Claeys P, Garcia A, et al. Natural history and clearance of HPV after treatment of precancerous cervical lesions. Histopathology. 2008;52(3):381–386. doi:10.1111/j.1365-2559.2007.02956.x
22. Bae JH, Kim CJ, Park TC, et al. Persistence of human papillomavirus as a predictor for treatment failure after loop electrosurgical excision procedure. Int J Gynecol Cancer. 2007;17:1271–1277. doi:10.1111/j.1525-1438.2007.00945.x
23. Santeso N, Reem AM, Holger JS, et al. World Health Organization guidelines for treatment of cervical intraepithelial neoplasia 2-3 and screen-and-treat strategies to prevent cervical cancer. Int J Gynecol Obstet. 2016;132(3):252–258. doi:10.1016/j.ijgo.2015.07.038
24. Cholli P, Bradford L, Manga S, et al. Screening for cervical cancer among HIV-positive and HIV-negative women in Cameroon using simultaneous co-testing with careHPV DNA testing and visual inspection enhanced by digital cervicography: findings of initial screening and one-year follow-up. Gynecol Oncol. 2017. doi:10.1016/j.ygyno.2017.11.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.