Back to Journals » Advances in Medical Education and Practice » Volume 12
Factors Associated with Practicing Evidence-Based Medicine Among Medical Interns in Amhara Regional State Teaching Hospitals, Northwest Ethiopia: A Cross-Sectional Study
Authors Yehualashet DE ![]() , Yilma TM, Jemere AT, Gedlu NM
, Yilma TM, Jemere AT, Gedlu NM
Received 16 May 2021
Accepted for publication 19 July 2021
Published 30 July 2021 Volume 2021:12 Pages 843—852
DOI https://doi.org/10.2147/AMEP.S320425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Delelegn Emwodew Yehualashet,1 Tesfahun Melese Yilma,2 Adamu Takele Jemere,2 Nebiyu Mesfin Gedlu3
1Department of Health Informatics, School of Public Health, Dilla University, Dilla, Ethiopia; 2Department of Health Informatics, Institute of Public Health, University of Gondar, Gondar, Ethiopia; 3Department of Internal Medicine, School of Medicine, University of Gondar, Gondar, Ethiopia
Correspondence: Delelegn Emwodew Yehualashet
Health Informatics, Dilla University, Dilla, Ethiopia
Tel +251976061907
Email [email protected]
Background: Evidence-based medicine (EBM) is an important component of modern medicine and is essential for the provision of high-quality health services. Little is known about the level of EBM use among Ethiopian medical students. This study aimed to assess the factors associated with EBM practice among medical interns in teaching hospitals in northwestern Ethiopia.
Methods: A cross-sectional study was conducted using a random sample of medical interns in teaching hospitals of northwest Ethiopia. Binary logistic regression analysis was used to identify factors associated with EBM practice. The strength of the interaction between variables was calculated using the adjusted odds ratio (AOR) with a 95% confidence interval (CI).
Results: Completed questionnaire was obtained from 403 (95.3%) of 423 medical interns. About 48.4% of respondents had a good EBM practice. EBM knowledge (AOR = 1.86, 95% CI = 1.220– 2.835), attitude to EBM (AOR = 2.05, 95% CI = 1.318– 3.193), ability to appraise evidence (AOR = 2.35, 95% CI = 1.570– 3.517), and having sufficient time to search for evidence (AOR = 1.67, 95% CI = 1.065– 2.627) were factors significantly associated to EBM practice.
Conclusion: This study demonstrates that the main factors affecting medical intern’s practice of EBM were lack of critical appraisal skill, lack of knowledge needed to practice EBM, negative attitudes toward EBM, and insufficient time to search for evidence. Providing EBM training to the needs of medical interns would overcome the barriers identified in this study, as well as assist medical interns and other clinical staffs to ensure the correct application of EBM in to clinical practice.
Keywords: evidence-based medicine, medical, internship, barriers, Ethiopia
Introduction
Evidence-based medicine (EBM) is the systematic identification, evaluation, and use of the latest research results to inform clinical decision-making.1 The practice of EBM means integrating clinical expertise with the best evidence and the opinions, concerns, and expectations of individual patients.2,3 It consists of five steps: creating clinical questions, searching for relevant evidence, critically evaluating evidence, applying the evidence, and evaluating the performance.4
EBM is one of the strategies used in medicine these days to improve health, patient care, and medical services. It has a pronounced effect on medicine through enabling practitioners to deliver high quality care by basing decisions on both the patient wishes and the best available evidence found in the literature. Most medical schools in the world teach EBM as a major component of their medical curriculum.5–10 It helps physicians to go through different available research evidences and enable them to evaluate the clinical importance of these evidences and decide which one is best suited to support medical practice.11 In addition, practicing EBM should allow clinicians to excel and develop in clinical practice by enabling them to evaluate the clinical and cost effectiveness of treatments and services.12
Two decades have passed since the incorporation of EBM into the teaching and practice of medicine. During this period, medical students in preclinical and clinical training had a lower exposure for EBM.13–15 Now, in many countries, EBM is an important part of the undergraduate medical education curriculum that promotes lifelong learning and critical thinking. Unfortunately, this change has not yet taken place in most developing countries.8,10,16
Although the concepts of EBM are widely accepted in medical education, many medical learners and practicing physicians still do not have the knowledge and skills needed to incorporate EBM into their patient care.17 Lack of time, lack of skills and knowledge, inadequate access to resources, and expense are common barriers to learning and practicing EBM.18
Some studies have been conducted to assess the knowledge and practice of EBM in medical students;19–21 however, very little data is available about Ethiopian medical students. A study conducted in Iran shows that most medical students do not have enough knowledge of basic concepts and familiarity with the term EBM.20 Similarly, poor knowledge and practice of EBM among medical students was found in Saudi Arabia.19 Evidences have showed that incorporating EBM into medical education improved medical student’s skill to go through key steps of EBM practice such as formulating a clinical question, searching for evidence, appraising the evidence, and applying the evidence at the point of care.22–24 Also, medical students’ knowledge and attitudes toward EBM have improved after EBM training.23,25,26 Teaching EBM to medical students in setting where they could directly apply their knowledge and skills in daily practice might encourage them to think more critically about their medical decisions.27
At most medical universities in Ethiopia, the teaching of EBM is not yet part of the undergraduate medical curriculum. Therefore, it is necessary to understand the current EBM status to plan for long-term educational programs. Our study aimed to assess factors associated with EBM practice among medical interns at two teaching hospitals in north-western Ethiopia. This information helps to identify their shortcomings and programming practical training appropriate for this group.
Materials and Methods
Study Area and Period
The study was conducted in teaching hospitals in the Amhara region of the north-western province of Ethiopia, specifically at the University of Gondar and Tibebe Ghion teaching hospitals, from March to April 2020. The Amhara region is located in the north-western and northern parts of Ethiopia. According to the 2019 Amhara Regional Health Office, the region has two teaching hospitals, the University of Gondar and Tibebe-Ghion. These teaching hospitals are the training centers for undergraduate medical students, dentists, nurses, midwives, pharmacists, and others who are responsible for solving public health problems nationwide.
Study Design and Participants
An institution-based cross-sectional study design was employed. Medical interns studying at the University of Gondar and Tibebe Ghion hospitals were participants of the study. Medical interns are final year medical students in University of Gondar and Tibebe Ghion teaching hospitals. During this time, students do basic hospital works by rotating through surgical and clinical specialties while supervised by residents and staff.
Sample Size Determination and Sampling Technique
Sample size was determined using a single population proportion formula equal to n = (Zα/2)2 (p (1-p)/d2); where n = sample size required, confidence level taken as 95%, Zα/2 (1.96), margin of error 5% (d = 0.05), 50% of the proportion. The calculated sample size was 384 with a non-response rate of 10%; the final sample size was 423.
By taking a list of medical interns from each hospital, we determine the proportionate sample to be taken, to estimate the number of study participants per hospital, using the formula = (n) x (nf)/N where n = the number of medical interns at each hospital, nf = total sample size and N = total number of medical interns at two hospitals. After that, based on their population, a simple random sampling method was used. Finally, 311 medical interns were selected from University of Gondar and 112 from Tibebe-Ghion hospital.
Measurements and Data Collection Techniques
Data were collected using a 5 section self-administered questionnaire. Data was collected by a total of six health informatics students (BSc). The first section of the questionnaire contains socio-demographic information of respondents (6 items). The second section of the questionnaire focused on the participants knowledge of EBM (14 items). The third section was designed to determine the respondent’s attitudes toward EBM (11 items). The fourth section was developed to determine respondent’s level of EBM practice (10 items). The final section of the questionnaire was developed to investigate respondent’s perceived barriers to practice EBM.
The attitude of respondents was measured by 11 questions with a five-point Likert scale (“1 = strongly agree”, 2 = agree’, 3 = neutral’, 4 = disagree’ “5 = strongly disagree”). All individual answers to attitudinal questions were computed to obtain total scores; then, the mean score was calculated to categorize as having favorable attitude (if participants scored ≥ mean score) or unfavorable attitude (if participants scored < mean score). In addition, the respondent’s level of knowledge was measured by calculating the mean score of the 14 questions and categorized as good knowledge (if participants scored ≥ mean score of the correctly answered questions) or poor knowledge (if participants scored <mean score of the correctly answered questions). The respondent’s level of practice was measured by 10 questions with a five-point Likert scale (“1 = always’, 2 = frequently”, 3 = sometimes’, 4 = rarely’ “5 = never”). All individual answers to practice questions were computed to obtain total mean scores and categorized as good practice (if participants scored ≥ mean score) or poor practice (if participants scored < mean score).
Data Quality Assurance and Management
The data collectors and supervisors were trained before the actual data collection about the purpose of the study, sampling procedure, methods of data collection, and ethical issues. Continuous follow-up and supervision were done by the supervisors and principal investigator throughout the data collection period. The data were checked daily for completeness and consistency.
The questionnaire was pretested on 5% of the similar population at Tikur Anbessa hospital for consistency of response and validity of the questionnaire. Using the data obtained from the pre-test, the questionnaire was checked for reliability (internal consistency) using the Cronbach alpha test. The reliability for knowledge questions had a Cronbach’s alpha value of 0.839; attitude had a Cronbach’s alpha value of 0.764 and practice (Cronbach’s alpha 0.750). These values indicate that the questionnaire had a strong internal consistency.
Data Processing and Analysis
Data collected was edited, coded, and entered in Epi-Info 8.1, and exported to SPSS (Statistical Package for Social Sciences) version 20 for analysis. Descriptive statistics (frequency, percentage, and mean) were calculated to summarize the data. Binary logistic regression was used to determine the correlation between outcome variable and predictors. Initially bivariate logistic regression analysis was performed to determine the relationship between the outcome and each predictor, and the variables were selected with a P value of less than 0.25 to be considered for multivariable logistic regression analysis. Finally, variables with significant associations were identified based on Adjusted Odds Ratio (AOR), with a 95% confidence interval (CI) and a P-value ≤ 0.05.
Results
Socio-Demographic Characteristics
From a sample of 423 medical interns, 403 completed a questionnaire making a response rate of 95.3%. Of the 403 participants included in the study, 291 (72.2%) were male. The majority of 296 (73.4%) participants were from the University of Gondar teaching hospital and another 107 (26.6%) from Tibebe Ghion teaching hospital. Most of the respondents 324 (80.4%) had never received EBM-related training. Most of the 276 (68.5%) participants have their computer and 355 (88.1%) have internet access Table 1.
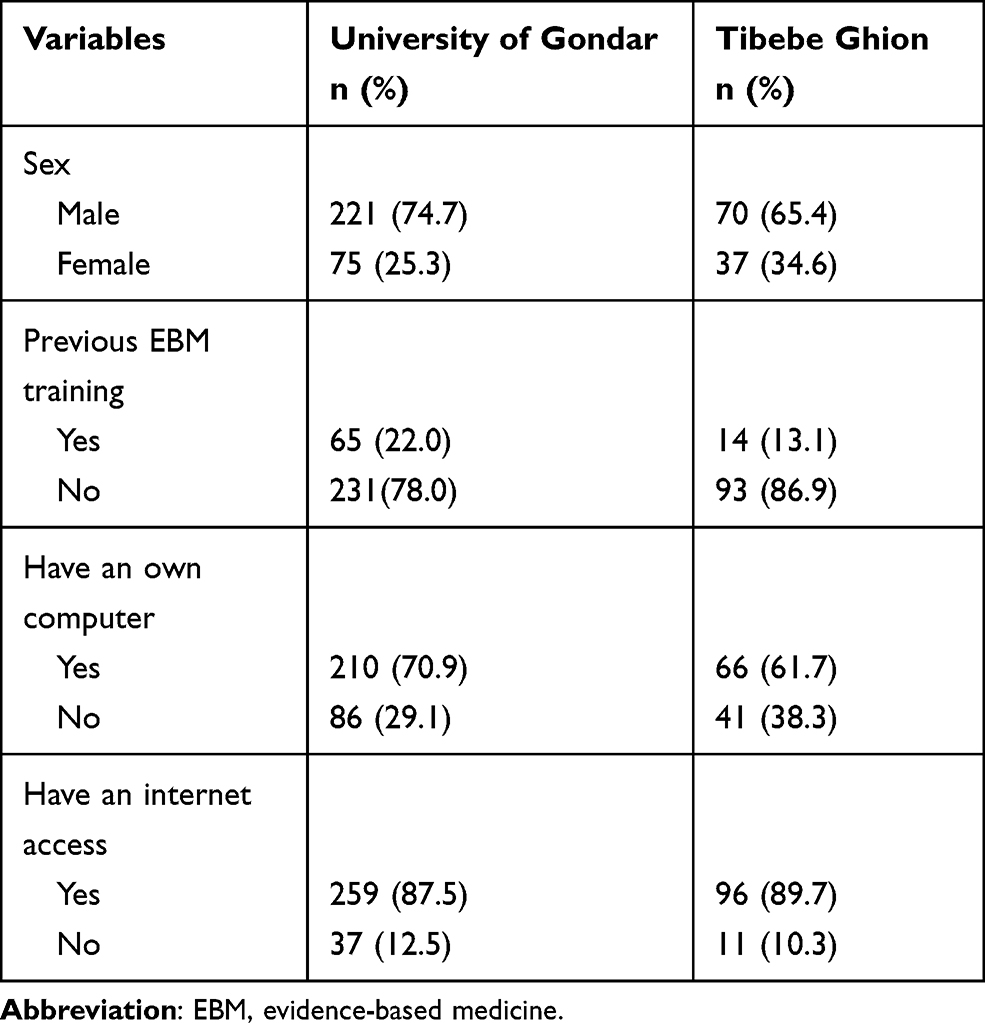 |
Table 1 Socio-Demographic Characteristics of Medical Interns in Northwest Ethiopia |
Knowledge About EBM
Of all participants, 230 (57.1%) had a good knowledge of EBM with a mean score of 6.6 ± 3.62 SD. Just over half, 226 (56.1%) participants responded correctly as EBM is a combination of good research evidence and clinical expertise. Similarly, 222 (55.1) were aware of the need for critical assessment skills to assess the quality of research papers and 212 (52.6) agreed that the EBM practice required proper identification and clinical questioning. However, only 108 (26.8%) responded correctly as a search of the literature on Medline using MeSH terms (medical subject headings) would reveal fewer articles than basic search using common keywords Table 2.
 |
Table 2 EBM Knowledge Among Medical Interns in Northwest Ethiopia |
Attitude Towards EBM
Among the total participants, 274 (68.0%) had a positive attitude to EBM with a mean score of 9.7 ± 1.65 SD. The majority, 380 (94.3%) of participants believe that the EBM practice is a useful tool for clinical decision making and 368 (91.3%) agreed that the EBM practice improves patient care Table 3.
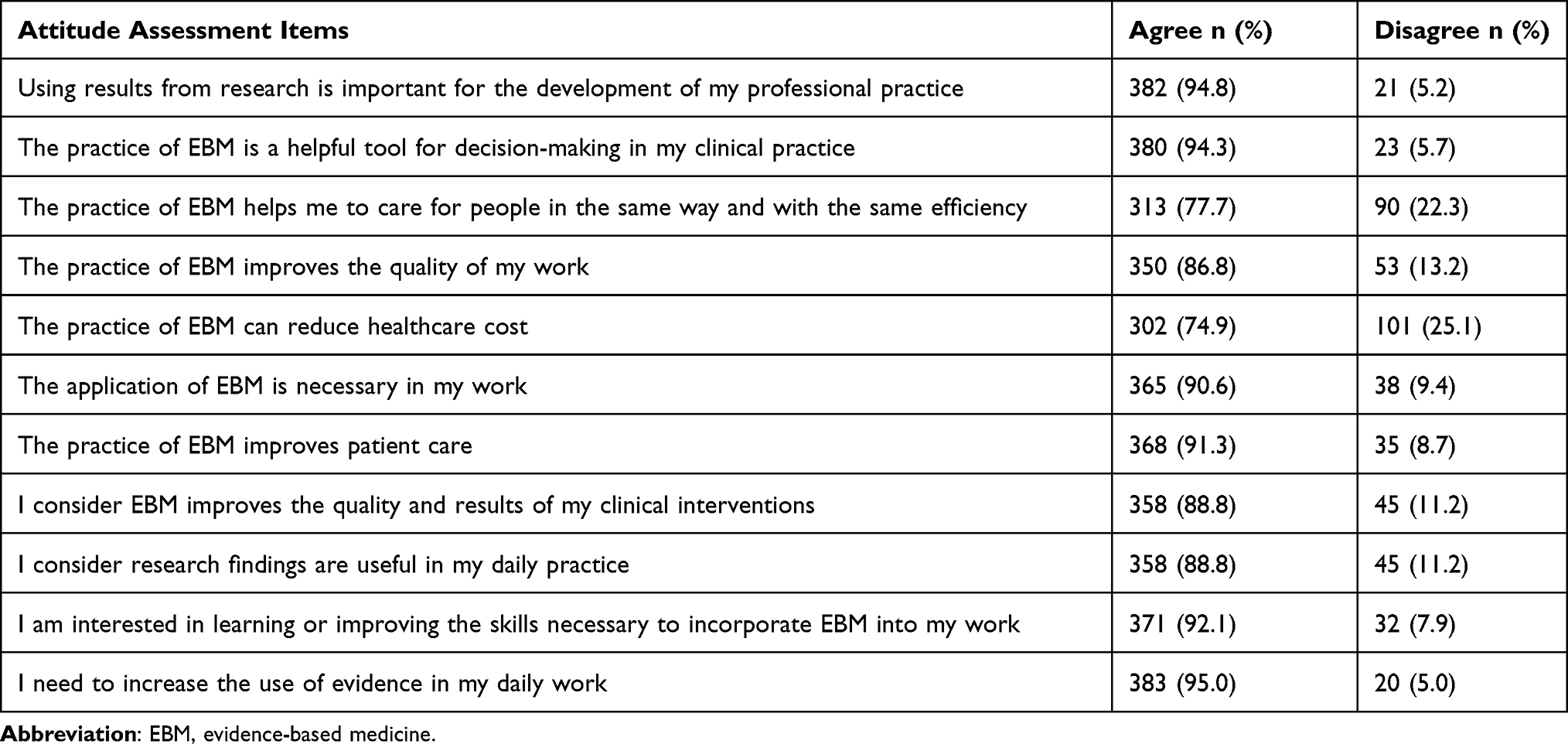 |
Table 3 Attitude Towards EBM Among Medical Interns in Northwest Ethiopia |
Practice of EBM
About 195 (48.4%) of the respondents had good practice of EBM with a practice mean score of 28.4 ± 7.69 SD. The majority, 338 (83.9%) of the respondents integrate the preference of patients in their clinical practice, and 322 (79.9%) formulated clinical questions. Despite this, 187 (46.4%) of the participants assess the validity of the research evidence Table 4.
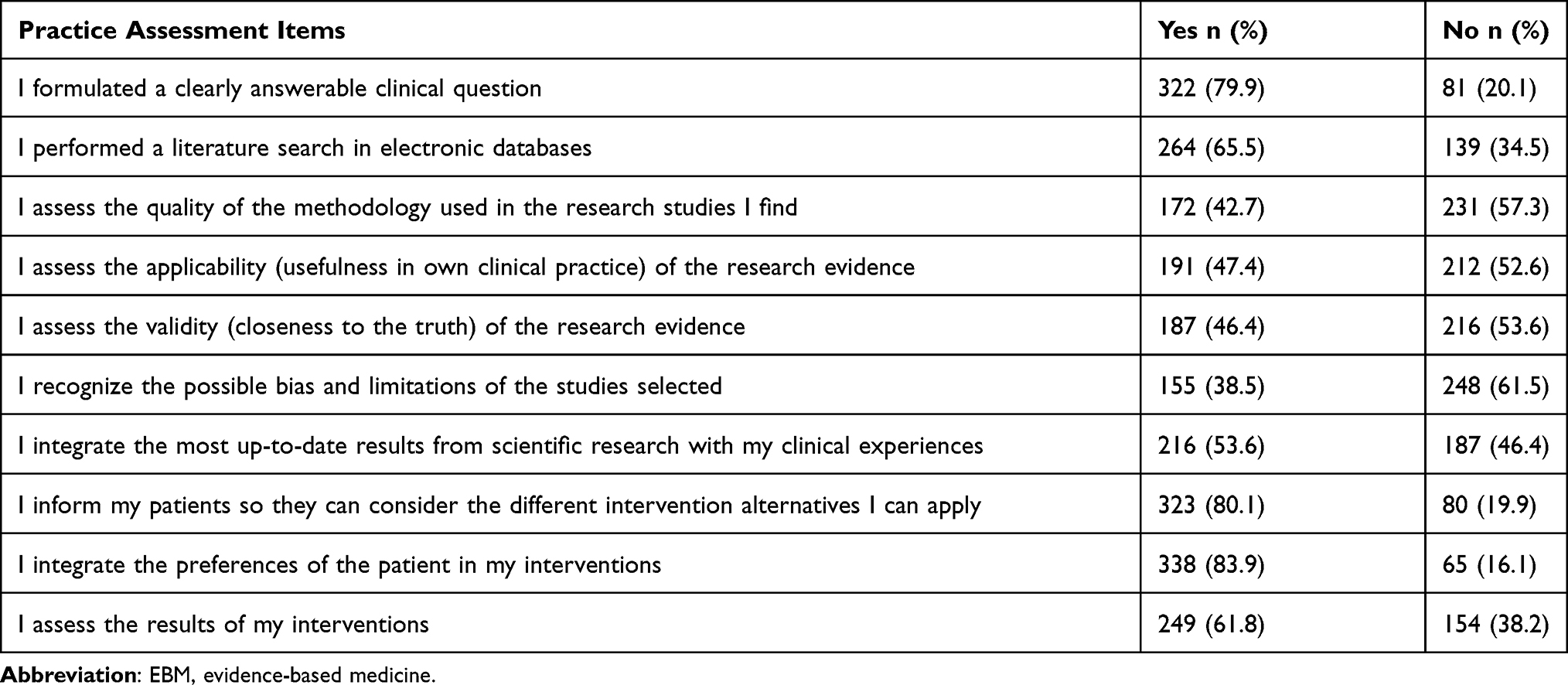 |
Table 4 The Practice of EBM Among Medical Interns in Northwest Ethiopia |
Perceived Barriers to Practice EBM
The most frequently reported barriers among medical interns were lack of access to electronic databases 241 (59.8%), lack of time to apply research evidence 288 (71.5%), lack of documents that guide the practice of EBM 262 (65.0%), and lack of institutional support for practicing EBM 320 (79.4%) Table 5.
 |
Table 5 Barriers to Practice EBM Among Medical Interns in Northwest Ethiopia |
Factors Associated with Practicing EBM
In the bivariate analysis, access to a research article in the workplace, access to an electronic database in the workplace, patient preference to EBM, patient belief in scientific evidence, having sufficient time to search for evidence, having sufficient time to read a research paper, reward for practicing EBM, supervisor support for practicing EBM, ability to access evidence, ability to critically appraise evidence, ability to apply evidence, EBM knowledge, and attitude towards EBM shows significant association with EBM practice at 0.01 level of significance.
In the multivariable analysis, the ability to critically appraise research evidence, EBM knowledge, attitude towards EBM, and having enough time to search for research evidence were factors significantly associated with the practice of EBM. The odds of practicing EBM were 2.3 times (AOR=2.35), 95% CI= (1.570, 3.517) higher for medical interns who can critically appraise research evidence when compared with those who did not have the ability. Medical interns who have good EBM knowledge were 1.9 times (AOR=1.86), 95% CI= (1.220, 2.835) more likely to practice EBM compared with those who have poor EBM knowledge. Medical interns who have a favorable attitude towards EBM were 2.1 times (AOR=2.05), 95% CI = (1.318, 3.193) more likely to practice EBM than those having an unfavorable attitude. Similarly, medical interns who have enough time to search for research evidence were 1.7 times (AOR=1.67), 95% CI= (1.065, 2.627) more likely to practice EBM compared to those who did not have sufficient time to search for research evidence Table 6.
 |
Table 6 Factors Associated with EBM Practice Among Medical Interns in Northwest Ethiopia |
Discussion
The result of this study indicated that medical interns have limited knowledge of key concepts of EBM, but a relatively positive attitude towards the concepts and limited practice of integrating scientific evidence into clinical practice. The majority of medical interns had never received any training related to EBM. The output from the multivariable analysis identifies EBM knowledge, attitude towards EBM, ability to critically appraise evidence, and having sufficient time to search for evidence as the factors positively associated with the practice of EBM.
In this study, 57.1% of participants had a good knowledge of EBM. Nearly half, (55.1%) respondents correctly answered as critical appraisal skills are necessary to ensure the quality of the research papers, and 52.6% were correctly answered as EBM practice requires proper identification and formation of clinical questions. This is consistent with a study of EBM in medical students in Switzerland.28 In contrast, a survey of knowledge, attitudes, and behaviors of medical students in Ireland showed that almost all (97%) participants were aware of the need for critical appraisal skills to ensure the quality of all research papers, and the majority (94%) was aware that the EBM practice required proper identification and clinical questioning.29 These differences may be due to the lack of formal EBM training in teaching hospitals included in the current study. Experimental evidence from Mexico suggested that the formal student training in EBM improved the knowledge and skills of medical students with EBM.25 Another reason for the discrepancy might be the difference in study setting and period.
The results of the current study revealed that about 68.0% of respondents had a positive attitude toward EBM. These findings were consistent with evidence from another study.30 This could be the first step in motivation and was a good sign to promote EBM teaching in the medical student curriculum. Similarly, a study conducted on knowledge and attitude of EBM among Jordanian physicians showed that 63.5% of participants had a positive attitude in EBM.31 In contrast, a study conducted among medical students reported unwelcome attitudes toward EBM.28 Moreover, 91.3% of medical interns agreed that practicing EBM improves patient care. Similarly, a study conducted on the knowledge and attitude of EBM in Iran has shown that 92.6% of physicians believe that practicing EBM improves patient management.32 The difference might be due to the difference in level of education and specialty of the participants included in the studies.
The current study also showed that 48.4% of participants had practicing EBM. A similar result was found in Jordan, in which 50% of participants were practicing EBM.31 Another study was done in Saudi Arabia also showed that 43.1% of the physicians are practicing EBM in their clinical practice.33 Only 1.1% of residence doctors practice EBM in their clinical practice in Sudan,34 which is lower than the current study. In contrast, 70% of physicians in Canada were applying EBM in their clinical practice.35 Evidence from China also revealed that 76.0% of physicians applied EBM in routine daily practice.36 The difference could be due to the level and experience of the respondents included in the studies. Professionals with a higher level of qualification are better equipped with knowledge and skills to retrieve, appraise and utilize the available evidence. Another possible explanation could be the difference in the institutional policy and training of medical students about methodological terms used in EBM.
In our study, 38.5% of respondents recognized methodological limitations of research evidences in their clinical practice. On the contrary, evidence from Saudi Arabia reported that 69.5% of medical students would evaluate the veracity of evidence when it contradicts clinical judgment.21 The first step toward translating EBM into clinical practice is determining what is meant by “best evidence.” Although the randomized controlled trial (RCT) is often touted as the be-all and end-all of clinical evidence, one can still practice EBM without such information. In fact, EBM involves using the best available evidence at the time, and what qualifies as “best evidence” differs by clinical question. Randomized controlled trials (RCTs), though desirable for clinical questions about therapy, may not be appropriate for all clinical questions. Therefore, various types of evidence can be used to develop the best treatment plan for a patient. Other than evidence from research, reliable clinical guidelines are also a useful source of recommended evidence that can be incorporated into clinical practice.37
In this study the most commonly identified barriers to the practice of EBM were lack of critical appraisal skill, lack of EBM knowledge, negative attitudes toward EBM, and insufficient time to search for evidence. Similarly, a study conducted in Gaza reported that the main factors affecting the practice of EBM were lack of knowledge needed to practice EBM and negative attitudes toward EBM.38 The results of this study are in agreement with previous study results38–42 and shows that lack of time were one of the top most common barriers to practice EBM. Even with the best guidelines for practicing EBM, there is not enough time in the day for the busy clinician to acquire and appraise research studies for every clinical question. One of the possible reasons for lack of time is health care provider’s high workload. To solve this problem, the staff workload is needed to be reduced or that more staff is employed. Another likely reason for the lack of time may be the clinician’s lack of ability in time management. To solve this problem, running time management workshops can be useful.
As future healthcare providers, medical students can be a receptive population to EBM concepts and it is important that they teach to offer the best possible care for their patients. Most Ethiopian physicians have unmet training needs concerning EBM and seek support for an improved education system to provide quality evidence-based health care. This will require a national policy for the EBM program in medical universities and need to be addressed at all levels of medical education in Ethiopia. It is in this context that the idea of this paper was developed to understand the current state of EBM in two teaching hospitals in Ethiopia, which could be very informative for planning long-term educational program. The early introduction of EBM in medical education increases the ability for logical and critical appraisal, better suited for the understanding of the disease process and subsequent management.25 It also gives an opportunity to the student to integrate basic and clinical sciences for developing skills as a future health professional.14
Conclusion
The result of this study shows that lack of time, inadequate critical appraisal skills, lack of knowledge needed to practice EBM, and negative attitudes toward EBM were found to be the most common barriers to practice EBM. Therefore, adapting EBM training to the needs of medical interns would reduce the barriers found in this study. We recommended that EBM teaching training be incorporated within both medical education and in clinical practice, which can help medical interns to overcome the barriers identified in this study. Further research in the area of EBM should focus on eliminating barriers to the practice of EBM and on educational solutions and interventions.
Abbreviations
EBM, evidence-based medicine; DARE, a database of reviews of abstracts of effectiveness; AOR, adjusted odds ratio; CI, confidence Interval; COR, crude odds ratio.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on a reasonable request.
Ethics Approval and Informed Consent
Ethical clearance and approval was obtained from the ethical review committee of the University of Gondar, Institute of Public Health and conducted following the guidelines of the Declaration of Helsinki. Subjects were informed about the purpose of the study and the benefits of participating in it. Written consent was obtained from each study subject to participate in the study. Confidentiality and privacy were guaranteed during the whole period of the study.
Acknowledgments
We would like to acknowledge the University of Gondar College of Medicine and Health Science, Institute of public health for financial support. Our heartily thanks also goes to supervisors and data collectors for their support in the data collection process. We also thank medical interns for their active participation in the study.
Author Contributions
All authors made a significant contribution to the conception, study design, execution, acquisition of data, analysis and interpretation of data, took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research has been financially supported by the University of Gondar for data collection and analysis. No fund was received for the publication of the article.
Disclosure
All authors declared that they have no conflicts of interest in this work.
References
1. Straus SE, McAlister FA. Evidence-based medicine: a commentary on common criticisms. CMAJ. 2000;163(7):837–841.
2. Maggio LA, Kung JY. How are medical students trained to locate biomedical information to practice evidence-based medicine? A review of the 2007–2012 literature. J Med Libr Assoc. 2014;102(3):184–191. doi:10.3163/1536-5050.102.3.008
3. Sackett DL, Rosenberg WM, Gray JM, Haynes RB, Richardson S. Evidence based medicine: what it is and what it isn’t. 1996. Clin Orthop Relat Res. 2007;455:3–5.
4. Dawes M, Summerskill W, Glasziou P, et al. Sicily statement on evidence-based practice. BMC Med Educ. 2005;5(1):1. doi:10.1186/1472-6920-5-1
5. West CP, McDonald FS. Evaluation of a longitudinal medical school evidence-based medicine curriculum: a pilot study. J Gen Intern Med. 2008;23(7):1057–1059. doi:10.1007/s11606-008-0625-x
6. Blake L, Ballance D. Teaching evidence-based practice in the hospital and the library: two different groups, one course. Med Ref Serv Q. 2013;32(1):100–110. doi:10.1080/02763869.2013.749143
7. Chakraborti C. Teaching evidence-based medicine using team-based learning in journal clubs. Med Educ. 2011;45(5):516–517. doi:10.1111/j.1365-2923.2011.03972.x
8. Gorgon EJ, Basco MD, Manuel AT. Teaching evidence based practice in physical therapy in a developing country: a national survey of Philippine schools. BMC Med Educ. 2013;13(1):154. doi:10.1186/1472-6920-13-154
9. Levin L, Hamama L. Teaching a systematic and evidence-based approach in an ambivalent context: a case example from Israel. Eval Program Plann. 2013;36(1):136–144. doi:10.1016/j.evalprogplan.2012.09.004
10. Prasad K. Teaching evidence-based medicine in resource-limited countries. JAMA. 2012;308(21):2248–2249. doi:10.1001/jama.2012.74124
11. Al Omari M, Khader Y, Jadallah K, et al. Awareness, attitude and practice of evidence-based medicine among primary health care doctors in Jordan. J Eval Clin Pract. 2009;15(6):1131–1136. doi:10.1111/j.1365-2753.2009.01223.x
12. Lewis SJ, Orland BI. The importance and impact of evidence-based medicine. J Manag Care Pharm. 2004;10(5 Suppl A):S3–S5. doi:10.18553/jmcp.2004.10.S5-A.S3
13. Ilic D, Tepper K, Misso M. Teaching evidence-based medicine literature searching skills to medical students during the clinical years: a randomized controlled trial. J Med Libr Assoc. 2012;100(3):190–196. doi:10.3163/1536-5050.100.3.009
14. Acharya Y, Raghavendra Rao MV, Arja S. Evidence-based medicine in pre-clinical years: a study of early introduction and usefulness. J Adv Med Educ Prof. 2017;5(3):95–100.
15. Ferwana M, Al Alwan I, Moamary MA, Magzoub ME, Tamim HM. Integration of evidence based medicine into the clinical years of a medical curriculum. J Fam Commun Med. 2012;19:136–140. doi:10.4103/2230-8229.98307
16. Kigali Declaration on Evidence Based Healthcare in Africa. Kigali, Rwanda. Final version; 2012. Available from: http://cebha.org/sites/default/files/Kigali%20Declaration.pdf.
17. Maggio LA, Tannery NH, Chen HC, Ten Cate O, O’Brien B. Evidencebased medicine training in undergraduate medical education: a review and critique of the literature published 2006–2011. Acad Med. 2013;88(7):1022–1028. doi:10.1097/ACM.0b013e3182951959
18. Sadeghi-Bazargani H, Tabrizi JS, Azami-Aghdash S. Barriers to evidence-based medicine: a systematic review. J Eval Clin Pract. 2014;20(6):793–802. doi:10.1111/jep.12222
19. Alahdab F, Firwana B, Hasan R, et al. Undergraduate medical students’ perceptions, attitudes, and competencies in evidence-based medicine (EBM), and their understanding of EBM reality in Syria. BMC Res Notes. 2012;5:431. doi:10.1186/1756-0500-5-431
20. Ghahremanfard F, Nassaji M, Mirmohammadkhani M, et al. Knowledge and attitude toward evidence-based medicine among medical students in Semnan, Iran. J Evid Based Med. 2014;7(1):32–37. doi:10.1111/jebm.12084
21. Aldugieman TZ, Alanezi RS, Alshammari WM, Al-Shamary YW, Alqahtani MM, Alreshidi FS. Knowledge, attitude and perception toward evidence-based medicine among medical students in Saudi Arabia: analytic cross-sectional study. J Fam Med Prim Care. 2018;7(5):1026–1031.
22. Ahmadi S, Baradaran HR, Ahmadi E. Effectiveness of teaching evidence-based medicine to undergraduate medical students: a BEME systematic review. Med Teach. 2015;37(1):21–30. doi:10.3109/0142159X.2014.971724
23. Dorsch JL, Aiyer MK, Meyer LE. Impact of an evidence-based medicine curriculum on medical students’ attitudes and skills. J Med Libr Assoc. 2004;92(4):397–406.
24. Sastre EA, Denny JC, McCoy JA, McCoy AB, Spickard A. Teaching evidence-based medicine: impact on students’ literature use and inpatient clinical documentation. Med Teach. 2011;33(6):e306–e312. doi:10.3109/0142159X.2011.565827
25. Sánchez-Mendiola M, Kieffer-Escobar LF, Marín-Beltrán S, et al. Teaching of evidence-based medicine to medical students in Mexico: a randomized controlled trial. BMC Med Educ. 2012;12:107. doi:10.1186/1472-6920-12-107
26. Khader YS, Batayha W, al-Omari M. The effect of evidence-based medicine (EBM) training seminars on the knowledge and attitude of medical students towards EBM. J Eval Clin Pract. 2011;17:640–643. doi:10.1111/j.1365-2753.2010.01604.x
27. Ilic D, Forbes K. Undergraduate medical student perceptions and use of evidence based medicine: a qualitative study. BMC Med Educ. 2010;10:58. doi:10.1186/1472-6920-10-58
28. Kaderli R, Carina LB, Hansali C, Businger A. Students’ view of evidence-based medicine: a survey in Switzerland. Archiv Clin Exp Surg. 2012;1(1):34–40. doi:10.5455/aces.20120217124737
29. Stronge M, Cahill M. Self-reported knowledge, attitudes and behaviour towards evidence-based practice of occupational therapy students in Ireland. Occup Ther Int. 2012;19(1):7–16. doi:10.1002/oti.328
30. Abeysena C, Jayawardana P, Wickremasinghe R, et al. Evidence-based medicine knowledge, attitudes, and practices among doctors in Sri Lanka. J Evid Based Med. 2010;3(2):83–87. doi:10.1111/j.1756-5391.2010.01077.x
31. Barghouti F, Halaseh L, Said T, Mousa AH, Dabdoub A. Evidence-based medicine among Jordanian family physicians: awareness, attitude, and knowledge. Can Fam Physician. 2009;55(7):e6–e13.
32. Rashidbeygi M, Sayehmiri K. Knowledge and attitudes of physicians towards evidence based medicine in ilam, iran. Iran Red Crescent Med J. 2013;15(9):798–803. doi:10.5812/ircmj.7204
33. Alshehri AA, Al-Khowailed MS, Alnuaymah FM, et al. Knowledge, attitude, and practice toward evidence-based medicine among hospital physicians in Qassim Region, Saudi Arabia. Int J Health Sci. 2018;12(2):9.
34. Zeidan AZ, Behairy MM. Knowledge, attitudes and practices of evidence based medicine among residence doctors in Sudan. Sudan JMS. 2010;5(3):207–212.
35. McAlister FA, Karr GW, Laupacis A, Laupacis A. Evidence-based medicine and the practicing clinician. J Gen Intern Med. 1999;14(4):236–242. doi:10.1046/j.1525-1497.1999.00323.x
36. Chen JH, Chen J. Clinical physicians’ attitudes towards Evidence-Based Medicine (EBM) and their Evidence-Based Practice (EBP) in Wuhan, China. Int J Environ Res Public Health. 2019;16:3758. doi:10.3390/ijerph16193758
37. Wallen GR, Mitchell SA, Melnyk B, et al. Implementing evidence-based practice: effectiveness of a structured multifaceted mentorship programme. J Adv Nurs. 2010;66:2761–2771. doi:10.1111/j.1365-2648.2010.05442.x
38. Albarqouni L, Elessi K. Awareness, attitudes and knowledge about evidencebased medicine among doctors in Gaza: a crosssectional survey. East Mediterr Health J. 2017;23(9):626–631.
39. Al Kubaisi NJ, Al Dahnaim LA, Salama RE. Knowledge, attitudes and practices of primary health care physicians towards evidence-based medicine in Doha, Qatar. East Mediterr Health J. 2010;16:1189–1197. doi:10.26719/2010.16.11.1189
40. Abd AL‐Magied DA, Abd El-Aziz KM. Knowledge, attitudes and practices of evidence‐based medicine among family physicians in Menoufia Governorate, Egypt. Thesis in family medicine submitted to Ain Shams Faculty of Medicine. 2013.
41. Adeodu A, Agius R, Madan I. Attitudes and barriers to evidence-based guidelines among UK occupational physicians. Occup Med (Chic Ill). 2009;59(8):586–592. doi:10.1093/occmed/kqp121
42. Al-Gelban KS, Al-Khaldi YM, Al-Wadei AM, Mostafa OA. Barriers against application of evidence-based medicine in general hospitals in Aseer region, Kingdom of Saudi Arabia. J Family Community Med. 2009;16(1):1–5.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.