Back to Journals » Infection and Drug Resistance » Volume 16
Factors Associated with Otitis Media Among Pediatrics in Two Government Hospitals in Arba Minch, Southern Ethiopia
Authors Araya EH, Manilal A ![]() , Oumer Y, Keyta G, Birru M, Desta Araya B
, Oumer Y, Keyta G, Birru M, Desta Araya B ![]() , Aklilu A
, Aklilu A ![]() , Alahmadi RM
, Alahmadi RM ![]() , Raman G, Idhayadhulla A
, Raman G, Idhayadhulla A ![]()
Received 8 July 2023
Accepted for publication 22 September 2023
Published 28 September 2023 Volume 2023:16 Pages 6405—6426
DOI https://doi.org/10.2147/IDR.S424927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Ephrem Henok Araya,1 Aseer Manilal,1 Yisiak Oumer,2 Gebre Keyta,1 Melkam Birru,1 Birhane Desta Araya,3 Addis Aklilu,1 Reham Mosleh Alahmadi,4 Gurusamy Raman,5 Akbar Idhayadhulla6
1Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 2Department of Medical Laboratory Science, College of Health Sciences, Arsi University, Asella, Ethiopia; 3School of Medicine, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 4Department of Botany and Microbiology, College of Science, King Saud University, Riyadh, 11451, Saudi Arabia; 5Department of Life Sciences, Yeungnam University, Gyeongsan, Gyeongbuk-Do, South Korea; 6Research Department of Chemistry, Nehru Memorial College (Affiliated to Bharathidasan University), Tiruchirappalli, Tamil Nadu, 621007, India
Correspondence: Aseer Manilal, Email [email protected]
Background: Bacterial otitis media (OM) is a common infection among the pediatric community worldwide and is the first reason for prescribing antibiotics in pediatric practices. However, if not promptly diagnosed and appropriately treated, it may persist and cause severe intra- and extra-cranial hard-to-cure complications. Hence, knowing the magnitude, etiology, and antibiotic susceptibility profile is very important for the proper management.
Methods: A cross-sectional study was carried out in 312 pediatrics (1 to 18 years) attending the Ear Nose Throat outpatient departments of the two title hospitals from 25 February to 30th August 2022. Patients were chosen through a systematic random sampling method. Data were obtained by means of a semi-structured questionnaire. Samples were collected to identify the causative bacteria as per microbiological guidelines. The antibiotic susceptibility test was done according to the Kirby–Bauer disc diffusion; SPSS version 25 was used for the analysis.
Results: The overall prevalence of otitis media was 67.3% (n=210); CSOM showed a slight preponderance (n=107) Gram-negative bacteria and Gram-positive bacteria were present in 59.8% (n=137) and 40.1% (n=92), respectively. Otitis media was predominantly caused by S. aureus (n=52, 56.5%), followed by Proteus spp. (n=33, 24%). Gram-negative bacteria were highly resistant to co-trimoxazole, amoxicillin-clavulanic acid, piperacillin, and tetracycline, whereas their positive counterparts were considerably penicillin and co-trimoxazole resistant. Overall, 61.5 and 19.2% of the isolates were MDR and XDR, respectively. MRSA, MR-CoNs, and VRE were 38.4% (n=20), 17.1% (n=5), and 58.3% (n=12), respectively; 19.7% (n=25) of Gram-negative bacteria produced ESBL, and 7% (n=9) were carbapenem-resistant. History of exposure to loud noise [AOR=3.4; CI=1.14– 10.23; P-value=0.028] and family history of smoking at home [AOR=2.9; CI=1.18– 7.25; P-value=0.020] have the greatest odds of otitis media.
Conclusion: Overall, the prevalence of otitis media is showing an upward trend, and MDR among bacterial isolates is increasing alarmingly.
Keywords: otitis media, prevalence, bacterial etiology, drug resistance, southern Ethiopia
Introduction
Otitis media (OM) may be considered a complication of upper respiratory tract infections that pave the way to hearing loss. It is common in both developed and developing countries, particularly among children.1 Approximately 1.2 billion are affected across the globe, and it is classified as the fifth one among the global burden of disease.2 Also, it is the second reason for hearing loss; the worst hit group is pediatrics, and is the most familiar disease that needs antibiotic treatments.2,3 Annual public health costs are estimated at around US 2.8 billion $ worldwide, overburdening the healthcare system.4
Otitis media can be chronic or recurrent and is often linked to complications involving loss of hearing and learning ability, with an inferior academic record.5 As per a global report, annually, 33 per 10 million meet with casualty due OM related intricacies.6 Countries with a prevalence rate between 1–2% and those with 3–6% or even higher are grouped separately, as per a WHO report. All developing countries, including Ethiopia, belong to the latter category, with a higher prevalence, even reaching 11%.7 The prevalence of OM varies geographically over time and is rising in developing countries.8 The demographic distribution and burden of this disease vary significantly among different regions. The prevalence and fatalities due to this disease are higher in countries of sub-Saharan Africa.9
OM can be viral, bacterial, or even a co-infection and bacteria account for majority of the cases. The most common bacterial otopathogens are S. pneumoniae, non-typeable H. influenzae, and M. catarrhalis. After the implementation of conjugate pneumococcal vaccines, the pneumococci has evolved into non-vaccine serotypes10 and still remains one of the most frequently diagnosed types in the childhood.
Otitis Media is subdivided into several categories: acute otitis media (ASOM), recurrent acute otitis media, otitis media with effusion and chronic supportive otitis media. Acute otitis media manifests with local and systemic signs and has a rapid onset,11 and is a prominent reason for antibiotic treatment among children in developed countries.12 Otitis media with effusion can occur during the resolution of ASOM once the acute inflammation has subsided, but with a persistence of bacteria. At the same time, CSOM manifest itself as continued middle ear inflammation leading to otorrhea persisting for at least two weeks and perforation of the tympanic membrane.13 The definition of CSOM varies depending on the duration and severity of symptoms, but it is generally believed that CSOM accompanies an unsuccessful or partially treated ASOM. Nevertheless, there is no clear distinction between otorrhea as a sign of ASOM and CSOM.14
The causative organisms ordinarily implicated in ASOM are S. pneumoniae (most common agent, 30%), followed by H. influenzae (20%) and M. catarrhalis (12%). Other organisms known to associate are S. pyogenes, S. aureus and rarely P. aeruginosa. Common aerobic bacteria associated with CSOM are P. aeruginosa, Proteus sp., E. coli and S. aureus, anaerobes and anaerobic streptococci.15
The burden of this disease in the pediatric population is massive in sub-Saharan African countries, including Ethiopia.16 Various reports from diverse regions of Ethiopia showed that the prevalence of OM remains high, ranging between 76.7% and 98.2%.7,17–20 The sobering report on the rising prevalence of OM in Ethiopian children suggests that OM is not well recognized in Ethiopia. An inaccurate diagnosis can lead to unnecessary antibiotic treatment contributing to the development of antibiotic resistance. Besides, the antimicrobial resistance patterns of otopathogens so far reported in other regions of Ethiopia are found to be weaker in terms of multidrug-resistant (MDR) (Methicillin Resistant S. aureus (MRSA), Extended-spectrum beta-lactamases (ESBL), and carbapenem-resistant Enterobacterales (CRE)).21 An overtime upsurge in the cases of upper respiratory tract infections such as rhinosinusitis, bronchitis, pneumonia, and OM among pediatric patients visiting the title hospitals had instigated us to perform this study to elucidate the exact magnitude of OM. Besides, recurrent episodes of OM are also common in the study area, making it a significant upper respiratory tract infection among the study population. The etiological agents may vary slightly from one region to another and in terms of their intensity too.
The treatment regimen usually opted for OM is usually empirical, based on topical antibiotics such as ciprofloxacin, ofloxacin, or rifampicin in combination with systemic drugs (ciprofloxacin, levofloxacin, amoxicillin/clavulanic acid, ceftazidime).22 Besides, most of the cases of OM in the title hospitals are managed by means of empirical therapy, and the antibiotics selected most often are amoxicillin and amoxicillin-clavulanic acid. This is not even facilitated by antimicrobial susceptibility testing, and therefore we anticipate the emergence of drug resistance necessitating much attention. Data on the OM-associated factors are also scanty in many reports published from the country, and Arba Minch is of no exception. Therefore, the present study is aimed to know the magnitude, bacterial profile and associated factors of OM among pediatrics of Arba Minch, Ethiopia.
Materials and Methods
Study Area
A facility-based cross-sectional bi-center study was designed and executed at two government hospitals in the Arba Minch borough. One of them is Arba Minch General Hospital (AMGH) which is the largest center providing medical care to Gamo Zone residents; the Ear Nose Throat (ENT) department of this hospital is staffed by senior otolaryngologists, general physicians, and nurses. Approximately 20 to 25 patients suspected of OM visit the outpatient wing (OPW) of this department every week. The second one is the Dill Fana Primary Hospital (DFPH). It serves a diverse spectrum of patients in the form of outpatient, inpatient, pharmacy, ART clinic, and laboratory services. The pediatric department of this hospital provides both outpatient and inpatient care.
Study Design and Study Period
An institution-based cross-sectional study was performed at AMGH and DFPH between 25th February and 30th August 2022, including both dates. All pediatric patients (1 to 18 years) who were treatment-naïve and clinically suspected of middle ear infections (acute and chronic OM) at the ENT OPWs of AMGH and DFPH were included. The inclusion criteria encompass subjects (of either sex) who visited the ENT OPWs with complaints of OM diagnosed by a physician, based upon the otoscopic examinations coupled with the patient’s history and clinical criteria (ie, patients with ear pain (fever and earache, aural discharge, erythematous and bulged ear drum and ear drum perforations and subsequent purulent discharge; infants may present with irritability and diarrhea too)) and provided pus swab from discharging ears. This is framed as per the clinical diagnostic criteria, covering both acute and chronic suppurative OM (ASOM and CSOM), set by concerned ENT physicians in the title hospitals and patients whose parents or caretakers volunteered to be part of the study; ASOM is an acute infection of the middle ear, usually lasting less than six weeks, whereas CSOM is defined as a perforated tympanic membrane with persistent drainage from the middle ear for more than six weeks.2 The exclusion criteria include subjects with aural abnormalities or who are on follow-up on any antibiotics, patients who were severely ill and were not in a position to give specimens, who were under antibiotic treatment during the previous week of sample collection, and also patients whose medical records are incomplete.
Sample Size and Sampling Technique
This parameter was arrived at by means of a formula based on a single population proportion, by fixing the rate of prevalence as 75.6%, opted from an earlier study done on pediatric patients in Hawassa, Ethiopia.18 After considering the confidence interval (CI) as 95% with a 5% margin of error, the calculated value of sample size became 283. The final consolidated sample size became 312 with an addition of a 10% non-response rate. The study participants were chosen through a systematic random sampling method. Dividing the total number of target patients by the sample size according to the latest annual report provided the sampling interval. The lottery method was adopted to fix each participant. A proportional allocation strategy was employed to choose the participants from both AMGH and the DFPH.
Independent Variables
Based on an extensive literature survey, 27 variables suspected to be linked to OM were incorporated into the work. It broadly comprised patient-related factors such as socio-demographic, behavioral, and clinical data; environmental factors were also added.
Outcome Variables
The primary outcome of this study provided a cumulative magnitude of OM in the two title hospitals based on the aerobic bacterial culture results. The secondary outcomes are the bacterial profile and antimicrobial susceptibility patterns, as well as the identification of independent factors that are suspected to influence the magnitude of OM.
Collection of Socio-Demographic and Clinical Data
It was conducted via a semi-structured questionnaire meant for the parents/juvenile patients and the assessment of records after a clinical examination. The consent and assent forms were filled and submitted on behalf of each participant before the collection of data and samples and then ENT specialists examined all the pediatrics. The socio-demographic, behavioral, clinical, and environmental details were also obtained for each subject. The questionnaire was divided into four subgroups. The patient-related factors (independent variables) documented were socio-demographic data such as age (years), sex, family size, residential status, level of education, occupation, and monthly income of parents. Details of behavioral factors, such as introducing foreign bodies in to the ears and ear-washing habits, were also collected. The clinical factors such as ear pain (unilateral and bilateral), its duration and frequency/year, ear discharge and its types (unilateral or bilateral), duration, the incidence of washing or cleaning the ear, history of upper respiratory tract infections (URTI) (whether treated and untreated), history of chronic ailments and hospitalization as well as the immunization status were abstracted from medical records. In addition, environmental factors such as the family history of OM, details of exposure to loud noise such as industrial, social, and gunfire, history of any trauma (in the external ear canal, ie, acute otitis externa), parental smoking, and indoor cooking were also gathered. These data were collected from the medical records of patients with the aid of senior nurses and through a face-to-face interview with parents/caretakers.
Collection, Transportation, and Handling of Clinical Specimens
The ear discharge (exudate) from the infected ear was aseptically collected using sterile cotton swabs by trained nurses and physicians after an otoscopy. Extreme care was taken to avoid touching the auricle or part of the ear with the swab. Each sample was adequately labeled, which showed the patient’s age, sex, and identity, along with the time and date of collection. Afterward, samples were transported in Amies transport media to the Medical Microbiology and Parasitology Laboratory within an hour and immediately processed.
Isolation and Identification of Bacteria
All the specimens were aseptically inoculated onto a series of culture media separately, which comprise 5% sheep blood agar, chocolate agar, McConkey agar, and mannitol salt agar. The last couple of agar plates were incubated aerobically at 37°C for 24 hours. The chocolate agar, as well as blood agar plates, were kept in a candle jar under a micro-aerophilic atmosphere (5–10% O2 and 10% CO2) and incubated at the same temperature for 48 hours. The identification of isolates was facilitated as per the published standard bacteriological procedures.23,24
Antibiotic Susceptibility Testing
The antimicrobial susceptibility tests were done by the Kirby-Bauer disc diffusion method as per the Clinical and Laboratory Standards Institute (CLSI) guidelines 2021.25 The antibiotics were selected based on standard treatment guidelines followed by hospitals and also as per the CLSI guidelines 2021.
Following antibiotic discs (Oxoid, Basingstoke, Hampshire, UK) were used for Gram-negative bacteria (GNB), such as ampicillin (AMP, 10μg), amoxicillin (AMX, 30μg), amoxicillin-clavulanic acid (AMC, 30μg), piperacillin (PIP, 100μg), ceftriaxone (CRO, 30μg), cefotaxime (CTX, 30μg), cefepime (FEP, 30μg), meropenem (MEM, 10μg), chloramphenicol (CHL, 30μg), gentamicin (GEN, 10μg), amikacin (AMK, 10μg), tetracycline (TET, 30μg), ciprofloxacin (CIP, 5μg), and sulfamethoxazole-trimethoprim or co-trimoxazole (SXT, 25μg).
In the case of Gram-positive bacteria (GPB), penicillin, amoxicillin-clavulanic acid, cefoxitin (FOX 30μg), vancomycin (VAN, 30μg), chloramphenicol, tetracycline, erythromycin (ERY, 15μg), ciprofloxacin, co-trimoxazole, and clindamycin (CLN, 300 μg) were used.25
To conduct the antimicrobial assay, standard inoculums of each bacterial isolate were prepared at 0.5 McFarland, and lawn cultures were performed on Mueller–Hinton agar plates. The antibiotic discs were placed and then incubated at 35–37°C for 24 hours. The diameters of zones of inhibition were measured with a ruler or caliper and categorized according to CLSI guidelines. The MRSA, ESBL producers, and CRE were detected as per standard procedures.25 An MDR is defined as acquired non-susceptibility to at least three antimicrobial classes. Extensively drug-resistant (XDR) bacteria were defined as non-susceptible to at least one antibiotic and two or fewer antimicrobial categories (ie, bacterial isolates remain susceptible to only one or two categories), and the term “pan-drug-resistant” refers to the non-susceptibility of a bacterial isolate to all the agents in all antimicrobial categories.26
Data Processing and Analysis
The analyses of data were carried out using SPSS (version 25.0; SPSS Inc., Chicago). Descriptive statistics, including frequency, mean and percentages, were articulated. To analyze the relationship between the dependent and independent variables, bivariable and multivariable logistic regression models were used. The variables with a P-value greater than 0.25 in the bivariable analysis were considered to be candidates for further analysis in the multivariable analysis. The Hosmer-Leme goodness fit test was used to determine the fitness of the model. P-values less than 0.05 were considered statistically significant. An adjusted odds ratio (AOR) and 95% confidence interval (CI) were calculated to assess the strength of the association.
Data Quality Control
We performed a pre-test on 5% of the samples at Wolaita Sodo University Otona Compressive and Specialized Hospital before the actual work to ensure the data quality. The principal investigator provided a one-day training session to data collectors. Quality control measures were implemented throughout the laboratory work to ensure the reliability of the results. A daily review of the data by the principal investigator was conducted to ensure its completeness, accuracy, clarity, and consistency. Strict adherence to Standard Operating Procedures was maintained for each operation. The expiry date of media and reagents and quality control parameters were checked as per CLSI guidelines. The culture media were prepared according to the manufacturer’s instructions, and their sterility was evaluated by incubating 5% of each batch overnight at 35–37°C. The culture plates and antibiotic disks were stored at the recommended temperature (2–8°C) following preparation. The type culture isolates of S. aureus (ATCC 25923), P. aeruginosa (ATCC 27853), and E. coli (ATCC 25922) were used as references. The type culture isolates such as S. aureus (ATCC 43300), E. coli (ATCC 35218), and K. pneumoniae (ATCC 700603) were used to validate the MRSA and ESBL isolates. These type culture isolates were obtained from Ethiopian Public Health Institute.
Ethical Considerations
This study was approved by the Institutional Review Board of Arba Minch University College of Medicine and Health Sciences and the Department of Medical Laboratory Science (IRB/13/2022). Before the collection of data and sample, informed consent (parents/guardian) and assent, in addition to the consent (elder pediatric patients), were obtained. The study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
During the study period between 25th February and 30th August 2022, a total of 312 eligible participants met the inclusion criteria and were incorporated into this research, with a 100% response rate. Of them, 180 (57.6%) were females and 132 (42.3%) were males; 102 (32.6%) were in the age group of 1–4; 187 (59.9%) hailed from rural areas, and the corresponding socio-demographic characteristics are described in Table 1.
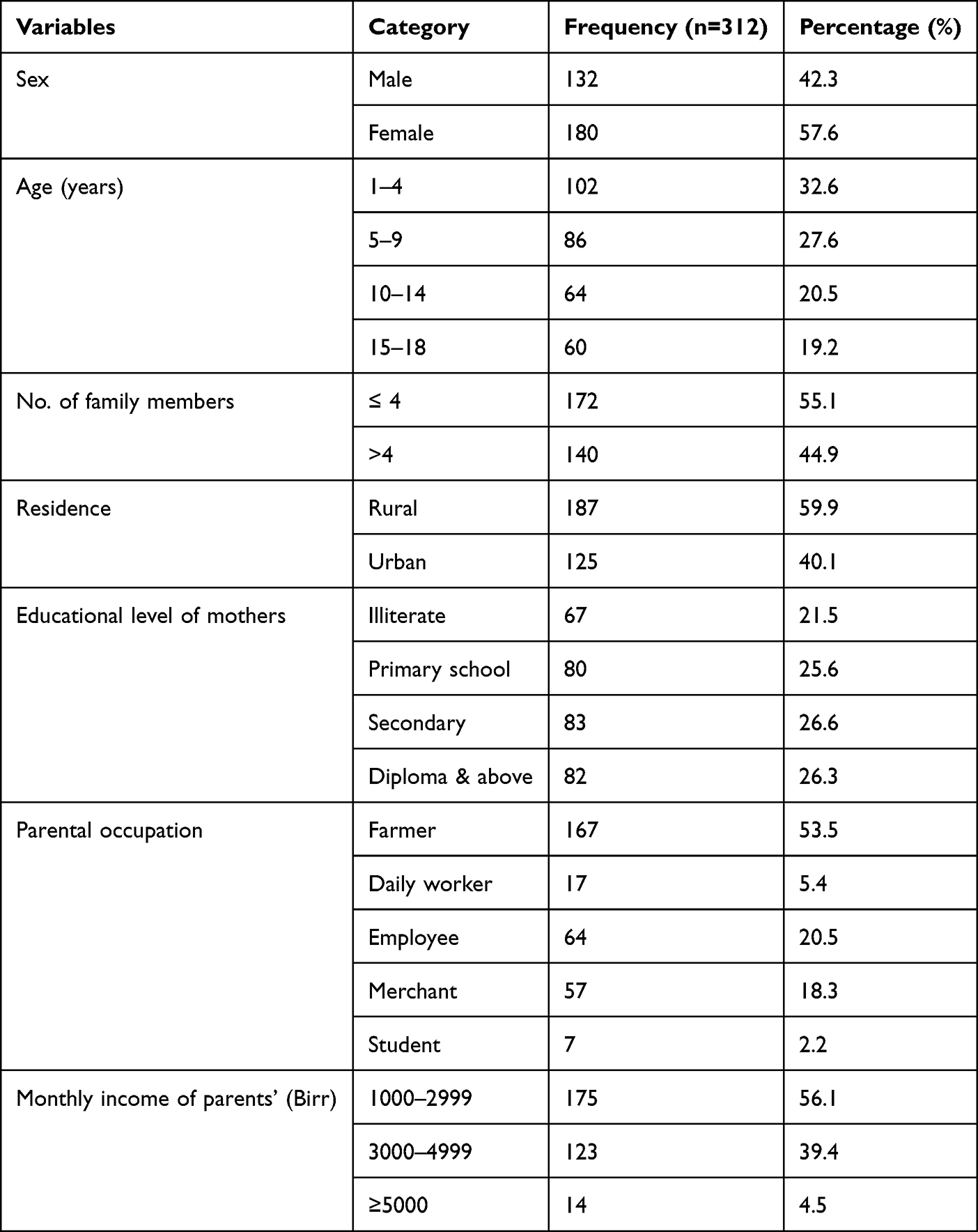 |
Table 1 Socio-Demographic Characteristics of Pediatric Patients with OM in Southern Ethiopia, 2022 |
Environmental and Behavioral Factors
It was found that a considerable proportion of the participants, ie, 74 (23.7%), had the habit of introducing foreign bodies into their ears. In contrast, only a tiny fraction of them, ie, 34 (10.8%), had a history of exposure to loud noises. Only 19 (6.0%) participants mentioned a history of head injury. A total of 63 (20.2%) had a family history of OM; 48 (15.4%) had a familial history of smoking. On the other hand, most of them, ie, 244 (78.2%), lack the routine habit of cleaning/washing their ears (Table 2).
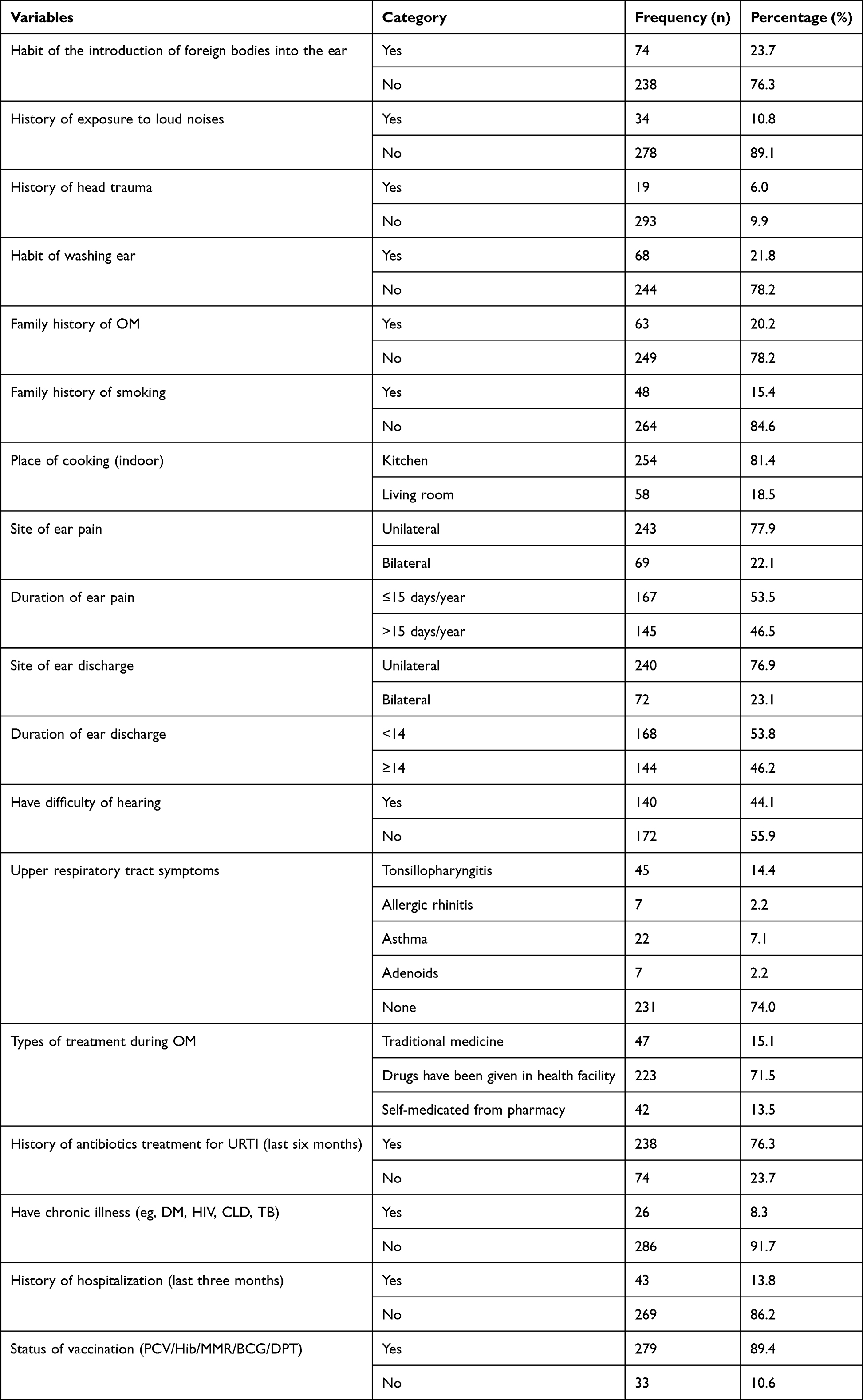 |
Table 2 Environmental, Behavioral, and Clinical Characteristics Among Pediatric Patients with OM in Southern Ethiopia, 2022 |
Clinical Characteristics
All the pediatric patients were clinically diagnosed with ear pain and discharge associated with OM. Nearly 50% (n=160) of the cases were clinically diagnosed as ASOM. Unilateral ear pain was observed in majority of participants, ie, 77.9% (n=243). It was observed that 46.5% (n=145) and 44.1% (n=140), respectively, had experienced ear pain more than 15 times per year along with hearing difficulties. Also, 25.9% (n=81) had experienced different types of signs and symptoms of URT infections. In addition, most of them, ie, 76.3% (n=238), had a history of consuming antibiotics for different clinical syndromes. Notably, 89.4% (n=279) were vaccinated with PCV/Hib/MMR/BCG/DPT (Table 2).
Magnitude and Bacterial Profile of OM
Among the participants enrolled, 210 cases were culture positive, making a cumulative magnitude of 67.3%. The total number of culture-positive cases of ASOM and CSOM were 103 and 107, respectively.
Altogether 229 otopathogens were obtained from 312 specimens; 83.4% (n=191) were mono-bacterial, and 16.5% (n=38) were bi-bacterial infections. Based on colony and biochemical characteristics, ten genera were identified; eight belong to GNB, while two were GPB (Table 3).
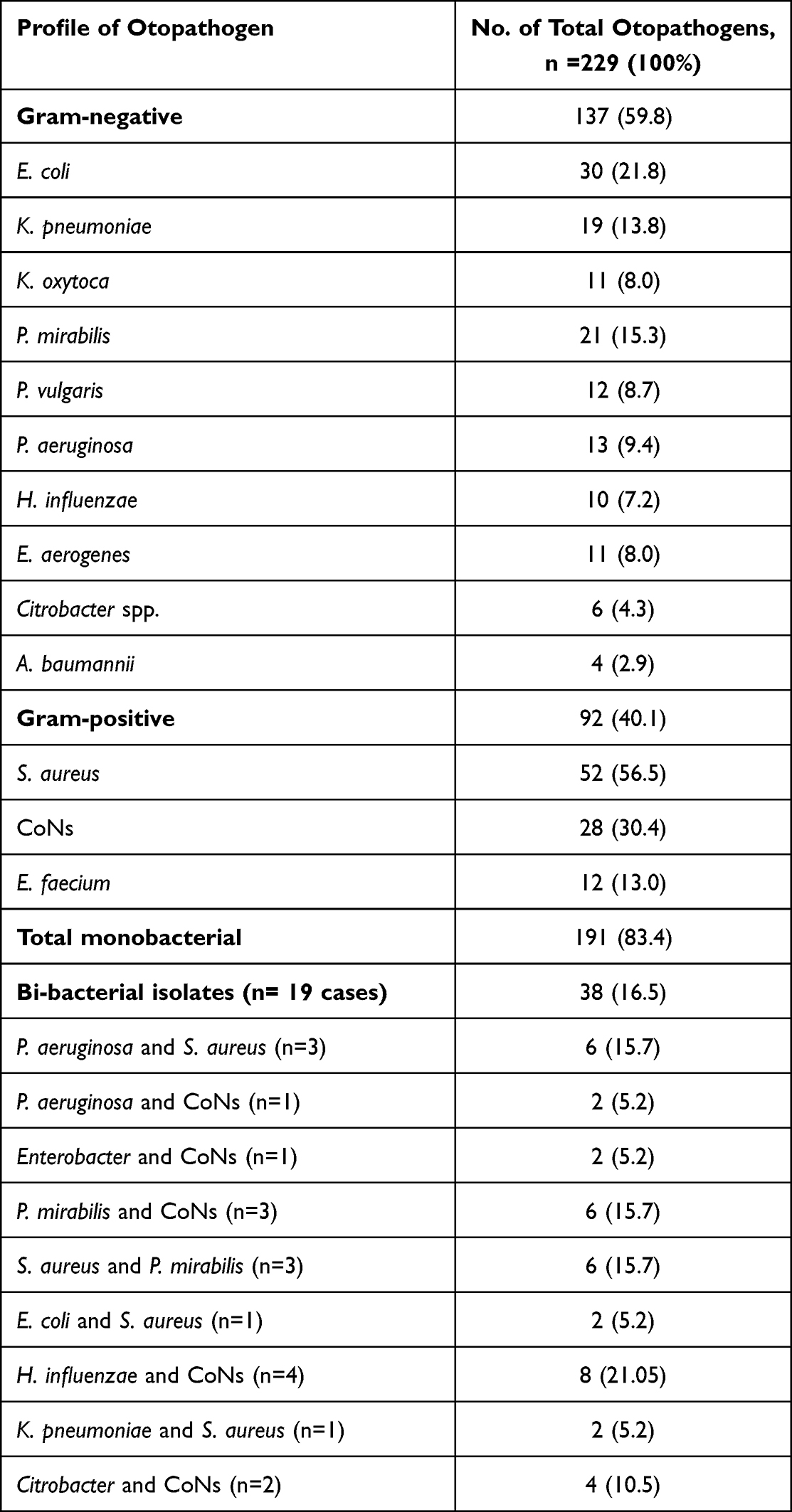 |
Table 3 Diversity and Percentage of Bacterial Otopathogens |
A total of 19 cases of bi-bacterial infections were detected. The prominent bi-bacterial infections correspond to four cases of H. influenzae and coagulase-negative staphylococci (CoNs). In this study, S. aureus (n=15), E. coli (n=12), and K. pneumoniae (n=10) are the most often found bacterial isolates associated with ASOM. On the other hand, in the case of CSOM, S. aureus (n=37), CoNs (n=21), and E. coli (n=18) were the most prevailing pathogens (Table 4).
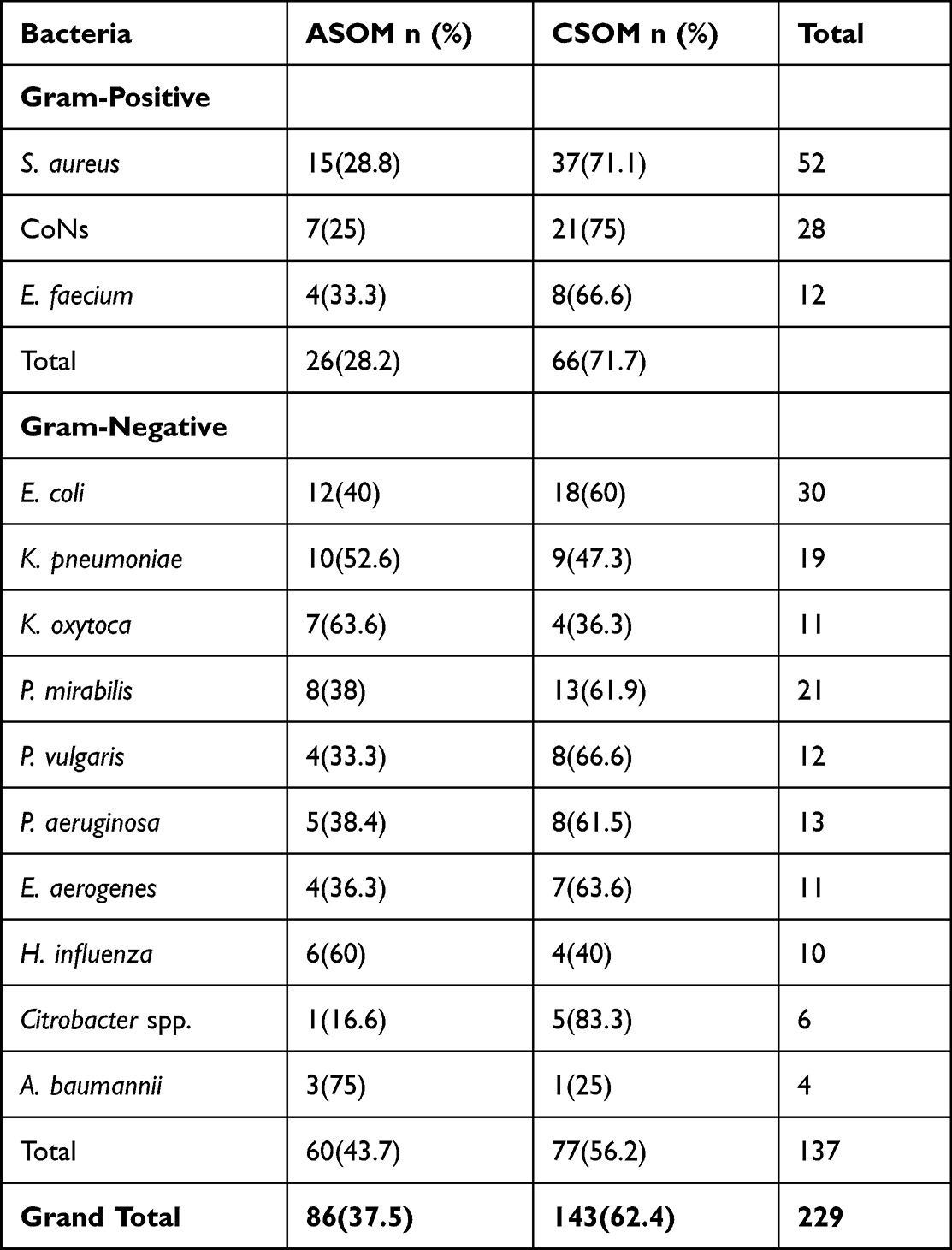 |
Table 4 Distribution of Bacterial Otopathogens |
Antibiotic Susceptibility Profile of Bacterial Otopathogens
Antibiotic Susceptibility Profile of GNB
The resistance/susceptibility profiles of GNB (n=137) are shown in Table 5; the intermediate results were also counted as resistant. Isolates of GNB exhibited considerable fluctuations in susceptibility/resistance patterns.
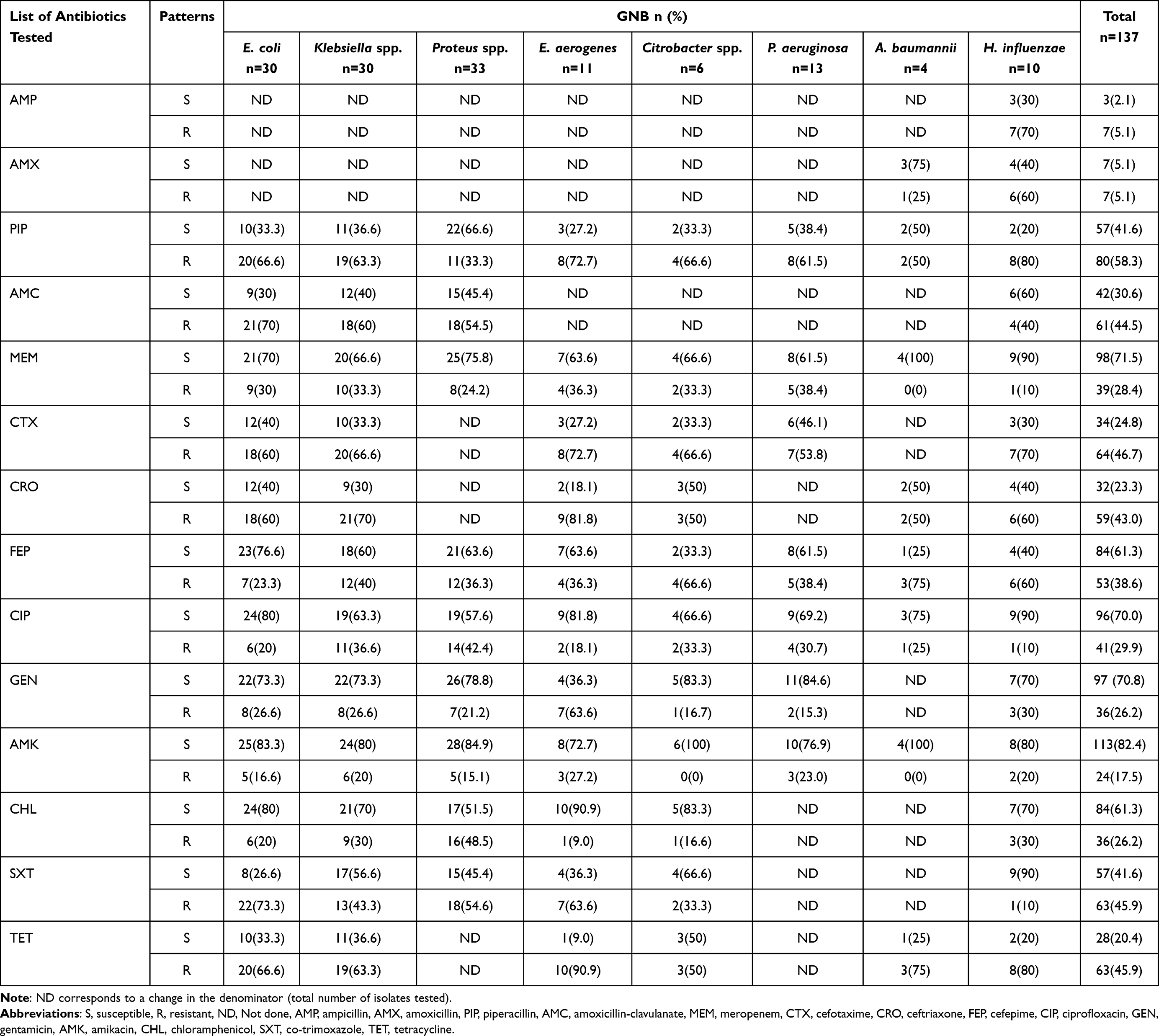 |
Table 5 Antimicrobial Susceptibility Profile of GNB Isolates |
The GNB showed resistance to piperacillin, 58.3% (80/137), cefotaxime 46.7% (64/137), tetracycline, co-trimoxazole, 45.9% (63/137) each, amoxicillin-clavulanic acid, 44.5% (61/137), ceftriaxone, 43% (59/137), and cefepime, 38.6% (53/137). However, most of the GNBs exhibited a relatively greater level of susceptibility to amikacin, as well as meropenem, ie, 82.4% (113/137) and 71.5% (98/137), respectively (Table 5). The predominant species of GNB, E. coli, showed 73.3% (22/30) resistance to co-trimoxazole, 70% (21/30) to amoxicillin-clavulanic acid, 66.6% each to piperacillin and tetracycline, and 60% each to cefotaxime and ceftriaxone; E. coli showed a higher level of susceptibility, ie, 83.3% (25/30) to amikacin and 80% (24/30) each to ciprofloxacin and chloramphenicol. Klebsiella isolates also showed higher resistance, ie, 66.6% (20/30) to cefotaxime, 63.3% (19/30) each to tetracycline and piperacillin and 60% (18/30) to amoxicillin-clavulanic acid (Table 5). Both the isolates of Proteus spp. showed augmented resistance to co-trimoxazole, 54.5% (18/33), amikacin, 54.6% (18/33), ciprofloxacin, 42.4% (14/33) and chloramphenicol, 48.5% (16/33).
Isolates of P. aeruginosa exhibited higher resistance to piperacillin, 61.5% (8/13), followed by cefotaxime, 53.8% (7/13); at the same time, these isolates were highly susceptible to gentamicin, 84.6% (11/13), and amikacin, 76.9% (10/13).
Antibiotic Susceptibility Profile of GPB
The susceptibility profiles of GPB (n=92) are shown in Table 6. As in the case of GNB, wide variations in resistance/susceptibility profiles were observed; Isolates of GPB were penicillin-resistant to a greater extent, 82.6% (76/92), and were also resistant to co-trimoxazole, 60.8% (56/92), however, were highly susceptible to clindamycin, 76% (70/92) and erythromycin, 70.6% (65/92). It can be noted that most of the S. aureus isolates were resistant to penicillin, 84.6% (44/52), and co-trimoxazole, 73% (38/52). On the other hand, 88.4% (46/52) and 69.2% (36/52) of S. aureus isolates were susceptible to clindamycin and chloramphenicol, respectively. The percentage of MRSA among S. aureus was 38.4% (20/52). Isolates of CoNs were resistant to penicillin, 85.7% (24/28), and co-trimoxazole, 64.2% (18/28); 17.8% (5/28) were found to be methicillin-resistant. However, isolates of CoNs were highly susceptible to erythromycin, 92.8% (26/28), clindamycin, 85.7% (24/28), and cefoxitin, 82.1% (23/28). The isolates of E. faecium were resistant to penicillin, 66.6% (8/12), chloramphenicol, 75% (9/12), and vancomycin, 58.3% (7/12).
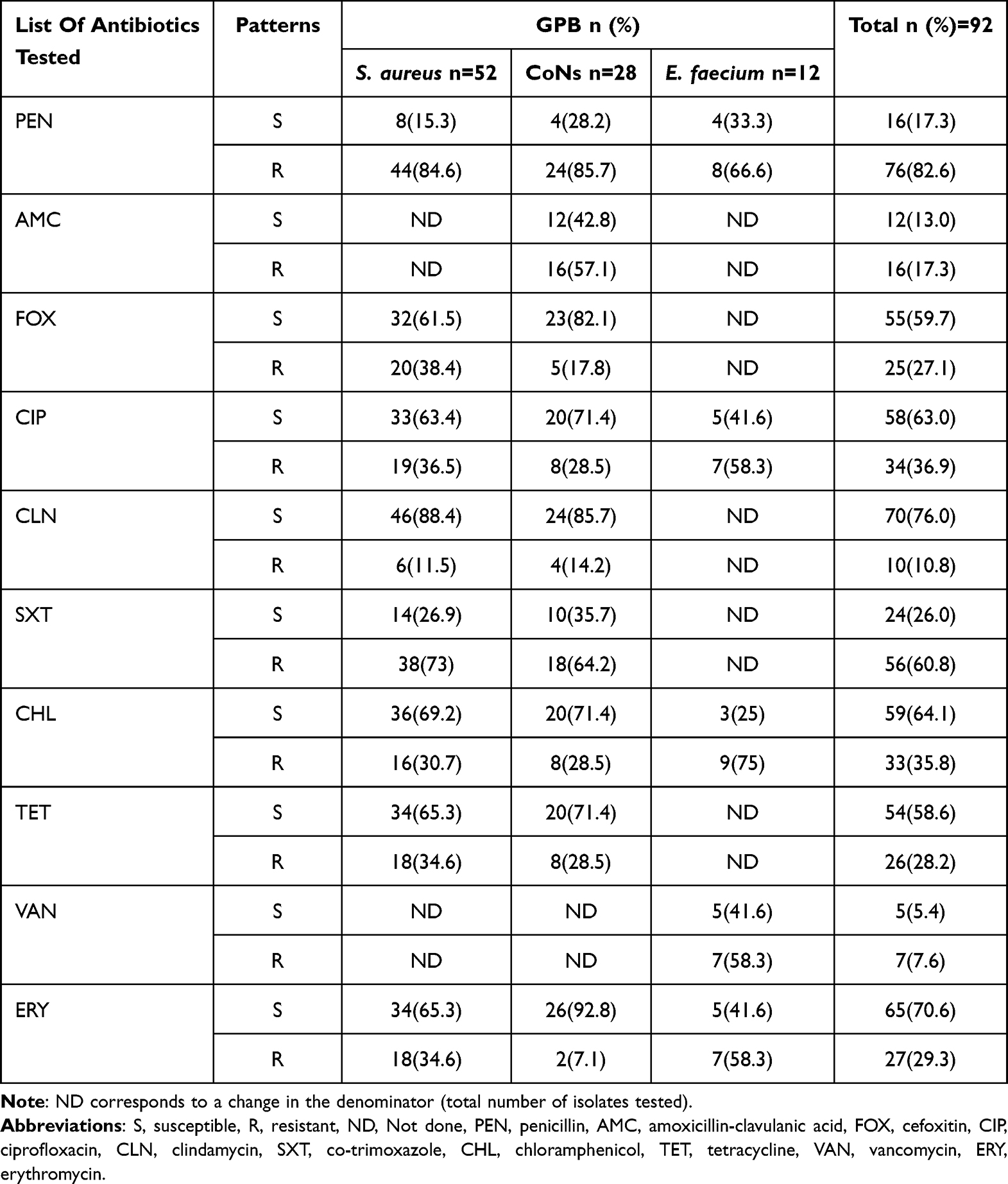 |
Table 6 Antimicrobial Susceptibility Patterns of GPB |
Multidrug Resistance Profile
Out of the 229 isolates, MDR was observed in 61.5% (n=141) of cases, of which 52.1% (n=48) belonged to GPB, and 67.8% (n=93) were GNB (Table 7). Among the GPB, 51.9% (n=27) of S. aureus, 57.1% (n=16) of CoNs, and 41.7% (n=5) of E. faecium were found to be MDR. Among the GNB, MDR was shown by P. aeruginosa (84.6%, n=11), E. aerogenes (81.8%, n=9), Proteus spp., (n=22), and E. coli (n=20) (66.6% each).
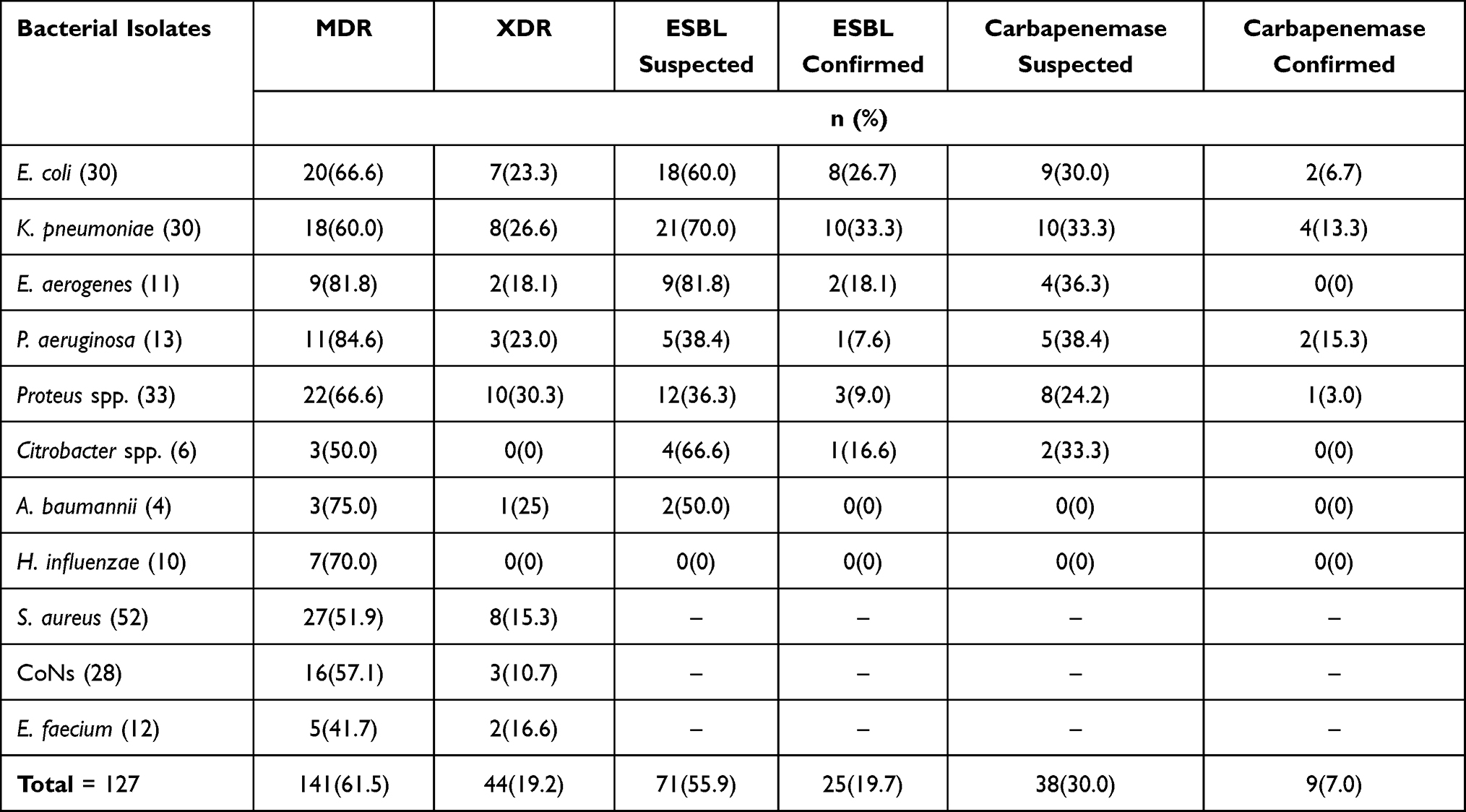 |
Table 7 MDR, XDR, ESBL, and CRE of Bacterial Isolates |
The observed extent of XDR was 19.2% (n=44); Proteus spp. was the main type, ie, 30.3% (n=10). Nevertheless, not even a single type of isolate tested was resistant to the entire classes of drugs, implying that pan-drug resistance was absent.
ESBL and Carbapenemase-Producing GNB
All isolates exhibiting resistance to the cephalosporins (cefotaxime or ceftriaxone and cefepime) were suspected to be ESBL producers. In contrast, meropenem-resistant bacteria were suspected to be producers of carbapenemase; 55.9% (n=71) and 30% (n=38) isolates were suspected ESBL and carbapenemase producers, respectively. Out of these isolates, 19.7 (n=25) and 7.0% (n=9) were phenotypically confirmed for ESBL and carbapenemase production, respectively. The most common ESBL producer was K. pneumoniae, 33.3% (n=10), followed by E. coli, 26.6% (n=8). Isolates of P. aeruginosa, 15.3% (n=2), and K. pneumoniae, 13.3% (n=4), were predominant organisms among the carbapenemase producers (Table 7).
Factors Associated with Bacterial OM
Association among socio-demographic and other chosen variables in connection with OM is described in Table 8. Sixteen variables were found to be statistically significant in bivariable logistic regression analysis. However, only two variables showed statistically significant association to OM in the multivariable logistic regression analysis; those patients with a history of exposure to noisy sounds acquired OM and were 3.4 times more prone than their counterparts [AOR=3.4; CI=1.14–10.23; P-value=0.028] and children with a family history of smoking also acquired, OM and they are 2.9 times more inclined than their counterparts hailing from the family of non-smokers [AOR=2.9; CI=1.18–7.25; P-value = 0.020].
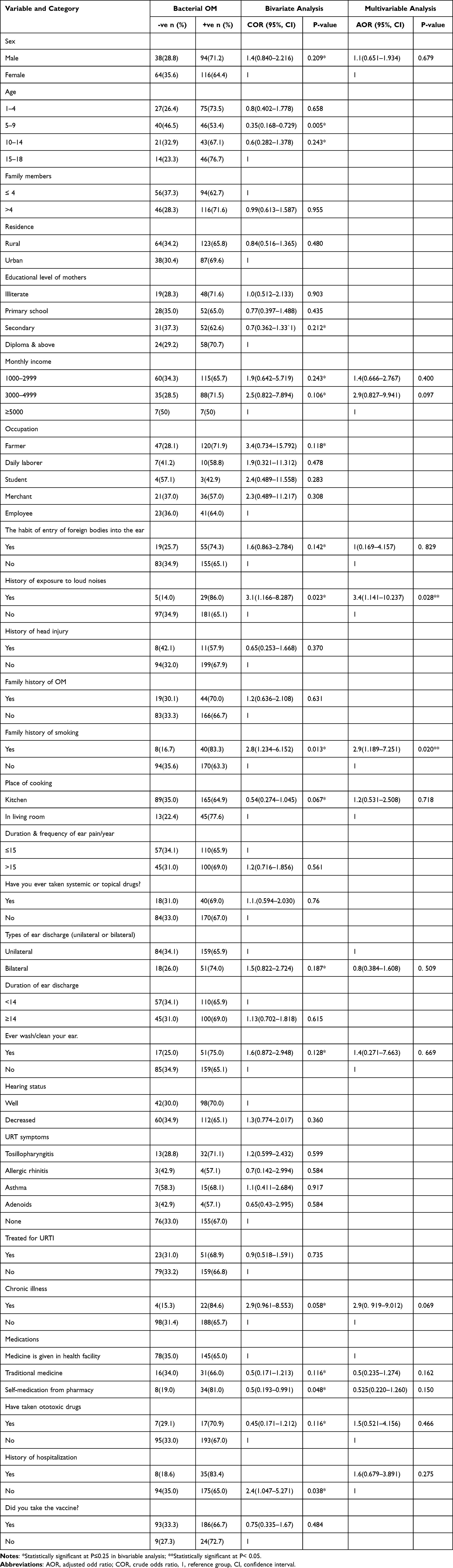 |
Table 8 Bivariable and Multivariable Logistic Regression Analyses of Different Factors with OM Among the Pediatric Patients in Southern Ethiopia, 2022 |
Discussion
Ethiopia has a higher incidence of OM, requiring immediate intervention. Despite the frequent incidence in clinical settings, diagnosis and treatment are still challenging for pediatricians due to the wide variation in clinical manifestations. Consequently, wrong regimens or inadequate treatment can result in irreparable damages and knowing the magnitude, etiological profile, and associated factors are crucial.
Otological complaints in pediatrics are one of the major causes of referrals to our study settings. It was found that OM was the most prevalent otorhinolaryngological disease among pediatrics visiting the title hospitals, with a cumulative magnitude of 67.3% (95% CI; 61.9–72.8), indicating that our study area is otitis-prone. Our results suggest that the prevalence of OM could be due to a common perception that it is a part of normalcy.
Nevertheless, the number of cases of ASOM and CSOM are more or less similar in our study, it is relevant to have a discussion on the latter due to the associated complications and consequences; CSOM is known to develop in infancy often as a result of poorly treated ASOM with the potential to progress into adulthood causing recurrent episodes of CSOM that can last of several years and end up in permanent hearing loss.27
The rate of culture-positive cases of CSOM (50.95%, 107/210) observed in our study was lower than that reported in a couple studies done in Ethiopia (75.6%)18 and Chad (86.1%).22 On the other hand, the rate was closely similar to that of an earlier study done in Ethiopia (48.5%).20
In sub-Saharan Africa, CSOM is a leading cause of preventable childhood hearing loss.28,29 CSOM rates can be higher in developing countries due to lower socioeconomic standards, poor nutrition, delayed consultation and lack of awareness that ASOM can eventually lead to chronic type.30 Likewise, diagnosing CSOM accurately remains a challenge since the exact instance at which ASOM becomes CSOM remains a controversy.31
The overall magnitude of our study is at par with the reports from Tanzania (62.1%)32 and Bangladesh (70.8%).33 It was found that the prevalence of OM was higher in our study and is in line with the report of the WHO expert committee. It can be noted that the current set of results shows a better trend (lower) than that reported from various locales in Ethiopia, such as Mekele (98.2%),17 Gondar (95.2%),19 Bahir Dar (80.4%),21 Dessie, 91.7%,34 Jimma (92.5%),35 Hawassa (75.7%)18 and also other African countries such as Cote d’Ivoire (91.7%),36 Malawi (98.2%)37 and Kenya (87%),38 however, is higher than that found in Addis Ababa, 48.5%.20 The reasons for these fluctuations could be due to varying situations in geographical locations, heterogeneity in socioeconomy, behavioral patterns (hygienic and the extent of awareness), environmental conditions, sample size, age, and nutritional status. Besides, different clinical criteria used for diagnosing OM, inadequate health care and laboratory facilities, and the type of infection-prevention control strategies followed by countries would also have contributed.
Most of the culture-positive specimens were mono-bacterial, ie, 83.4% (n=191), and this is in line with the outcome of an earlier work from Gondar (77.4%).19 On the other hand, the frequency of isolation of poly-bacterial pathogens was 16.9% (n=38) and is lower as compared to the results reported from Mekele (39.5%).17 A combination of CoNs with other GNBs was the most common profile observed in poly-microbial infections. The coexistence of GNB and GPB was only detected in our study, indicating that broad-spectrum antibiotics are required to deal with the situation. It is speculated that intense infections result in poly-microbial isolates, and less severe cases are mono-microbial. This can be linked to a condition that bacteria from the pinna migrate into the middle ear and multiply faster there in a favorable humid situation.
The eight most prevailing bacteria were E. coli (n=30, 21.9%), P. mirabilis (n=21, 15.3%), P. vulgaris (n=12, 8.8%), K. pneumoniae (n=19, 13.9%), K. oxytoca (n=11, 8%), P. aeruginosa (n=13, 9.4%), S. aureus (n=52, 56.5%), and CoNs (n=28, 30.4%), and this resembles the outcome of researches done in Nigeria (71.6% GNB and 27.6% GPB)1 and Nepal (45.9% GPB and 54.1% GNB).39
The GNB was the predominant and leading cause of OM, resulting in 59.8% (n=137) cases. The enhanced prevalence of GNB reveals that the nasopharynx is not the origin of the infection, as it is devoid of these bacteria. This observation is in parity with several reports from two cities in the country, Hawassa (48.0% GPB and 52.0% GNB)18 and Gondar (32.4% GPB and 67.6% GNB).19
Also, E. coli, 24.6% (n=29), was the often-found GN otopathogen, followed by K. pneumoniae, 13.8% (n=19), which is in agreement with a series of earlier work done in countries including Ethiopia (7.4% E. coli and 3.5% K. pneumoniae)20 and Kenya (7.2% E. coli and 3.5% K. pneumoniae).38 In contrast, P. aeruginosa was the dominant GNB detected in various cities of Ethiopia (such as Bahir Dar (29.7%)),21 Addis Ababa (10.9%),20 Mekele (16.7%),17 and Gondar (48.5%)7 and also in another African country, Cote d’Ivoire (31.8%).36 A higher incidence of GNB can be ascribed to the normal endogenous microflora of patients, which acts as a source.
In this study, species of the genus Proteus (n=33) have been isolated and are the most predominant bacterial pathogen. Of these, P. mirabilis (n=21, 15.3%) was often associated with OM, and this parallels the outcome of work done in Hawassa (n=19, 12.5%).18 On the other hand, the number of P. vulgaris (n=12, 8.8%) detected in our study was lower than that found in studies reported from Gondar (2.7%)19 and Mekele (4.5%).17
Specifically, P. aeruginosa gradually destroys the middle ear’s mastoid and structure due to its lethal virulence factors. This is another predominant bacterial pathogen found (n=13, 9.4%), as is the case of reports from Jimma, 10.61%35 and Addis Ababa, 10.9%;20 however, not as severe as found in research done in Mekele, Ethiopia, 27 (16.7%).17 Of interest, P. aeruginosa does typically not inhabit the URT, and its presence cannot be linked to a source in the Eustachian tube. Instead, it is mainly considered a secondary invader originating from the external auditory canal because of an acute OM.40
However, only a few numbers of H. influenzae (n=10, 7.2%) were isolated, and this is not at par with other studies done in Iraq (3.9% and 7.9%)41,42 and Ethiopia (11.1%).17 This discrepancy might be due to epidemiological differences (endemicity and seasonal variation) and the diversity of etiological agents circulating in the study population. It may also be associated with the gradation in the socio-economic status of the patients and hospital settings in respective countries.
The predominant GPB isolate was S. aureus, 56.5% (n=52), and the second most is CoNs, 30.4% (n=28), and is in accordance with the results obtained from Nepal,39 India,43 and Ethiopia.18,44 The source of S. aureus infection may be endogenous, ie, nasopharyngeal colonization.
The management of bacterial OM requires constant re-evaluation of the susceptibility to various antibiotics. If adequate treatment is not given, the infection can progress and culminate in irreversible sequelae and severe intracranial and extracranial complications, especially in the case of CSOM. Nearly half of the isolated GNB showed resistance to piperacillin, 58.4% (n=80), tetracycline, 63 (46%), co-trimoxazole, 63 (46%), cefotaxime, 64 (46.7%), ceftriaxone, 59 (43%), amoxicillin-clavulanic acid, 61 (44.5%), and cefepime, 53 (38.7%), questioning their empirical usage, which is unscientific, rendering the clinicians with limited choice of drugs.
An earlier study done among the general mass of Arba Minch revealed that respiratory tract infections are the main reason for treatment-seeking, and amoxicillin was the most commonly used antibiotic.45
A recent meta-analysis revealed a higher resistance by bacterial otopathogens against ampicillin, co-trimoxazole, amoxicillin, and amoxicillin-clavulanic acid.16 The current set of results is pretty similar to these reported from various regions in the country (Wollo and Jimma).35,46 On the other hand, the higher resistance level could be attributed to their indiscriminate usage in hospital settings across the country.
However, our result contradicts a report from Bahir Dar, Ethiopia, in that study, ceftazidime, piperacillin, ceftriaxone, and co-trimoxazole were effective against most of the GNB isolates.21 This might be due to the antibiotic exposure frequency, susceptibility test method, sample size, and clinical nature of the disease (chronic or acute). A reduced level of resistance was only produced against amikacin, 17.5% (n=23), ciprofloxacin, 30% (n=42), gentamicin, 26.5% (n=35), chloramphenicol, 26.2% (n=35), meropenem, 28.5% (n=39) and amoxicillin 5.1% (7) in our study. As per our findings, these antibiotics are still effective in treating OM in both study settings and therefore, must be meticulously used.
Among the isolates of E. coli, 73.3% are resistant to co-trimoxazole, 70% to amoxicillin-clavulanic acid, 66.7% each to piperacillin and cefepime, and 60% each to cefotaxime and ceftriaxone. The E. coli isolates were highly susceptible to amikacin (83.3%), ciprofloxacin, and chloramphenicol (80% each), and this resembles the results of earlier works reported from other parts of the country.18,46 Isolates of Klebsiella spp. also showed a growing trend in their resistance to cefotaxime (66.7%), tetracycline and piperacillin (each 63.3%), and amoxicillin-clavulanic acid (60%), which are comparable to the data obtained from other studies done in various cities of Ethiopia.17,18,21 Usually, the higher resistance can be correlated to the formation of beta-lactamase. Among the predominant GNB otopathogens, Proteus spp. showed resistance to co-trimoxazole (54.65%) and amoxicillin-clavulanic acid (54.5%). These results resemble a previous study done in Hawassa which indicated that 57.9% of the isolates were resistant to both co-trimoxazole and amoxicillin-clavulanic acid.18
The isolates of P. aeruginosa showed higher resistance to a pair of drugs, such as piperacillin (61.5%) and cefotaxime (53.9%). However, mustered increased susceptibility to gentamicin (83.3%), amikacin (77%), ciprofloxacin (69.2%), and meropenem (61.5%). These results are in line with that of a previous study conducted in Nepal (gentamicin (91.4%), amikacin (89.2%), ciprofloxacin (87.5%), and meropenem (92.9%)).39
Most of the isolates of GPB were resistant to penicillin (82.6%), co-trimoxazole (60.9%), and vancomycin (58.3%), and the resistance profile is similar to that described in a previous report from Mekele.17 On the other hand, GPB exhibited only a marginal resistance against clindamycin (10.9%), erythromycin (29.3%), tetracycline (28.2%), and ciprofloxacin (37.0%), which is in agreement with the researches conducted in Bangladesh,33 India,43 Cote d’Ivoire36 and Ethiopia17 itself.
Notably, the isolates of S. aureus demonstrated higher resistance against penicillin (84.5%), and the extent is more or less equal to those found in Jimma (87.5%).44 The isolates of S. aureus were highly resistant to co-trimoxazole (73%) as per the present study. This finding is exactly matching with the outcome of a study reported from Hawassa (73.2%).18 At the same time, isolates of S. aureus exhibited susceptibility to clindamycin (88.4%), chloramphenicol (69.2%), erythromycin (65.3%), and ciprofloxacin (63.4%). This pattern was also found in previous works reported from Gondar (75% susceptible to chloramphenicol and 66.7% to ciprofloxacin)19 and Bahir Dar (85.9% susceptible to erythromycin).21
The second most predominant GPB is CoNs, of which 85.7, 64.2, and 57.1% showed resistance to each antibiotic tested, such as penicillin, co-trimoxazole, and amoxicillin-clavulanic acid, respectively. This is identical to the results of previous research done in Mekelle, where the resistance to penicillin and amoxicillin-clavulanic acid was 76.5% each and 100% to co-trimoxazole.17
This study confirmed the cosmopolitan nature of heterogeneity in antimicrobial susceptibility profiles, and apparent differences in pattern could be due to the frequent and indiscriminate usage of several types of antibiotics for treating ear infections. In other words, it indicates that the drug-resistance genes of GPB are disseminated in Ethiopia, which needs a better understanding, and there must be a fight against drug resistance by all the stakeholders.
MDR was detected in 67.1% of isolates, and the results should be viewed with considerable caution. Our findings match with the results of a number of earlier studies done in different cities of the country (such as Mekele, 74.5%,17 Jimma, 67%35 and Hawassa, 69.9%)18 The current study hints at a higher percentage of MDR isolates compared to the reports from a couple of cities in Ethiopia (35% in Gonder19 and 50% in Wollo).46 It is to be mentioned that 19.2% (n=44) of the isolates were XDR which is not as high as found in an earlier study done in Iraq (31.7%).47
Isolates of ESBLs and CRE are of increasing clinical concern but have to be viewed from an angle of epidemiological and infection control. A staggering fact from our study is the detection of MRSA, ESBL, CRE, and VRE bacterial isolates, which are enlisted by WHO as priority pathogens; for instance, 38.4% of S. aureus were identified as MRSA, at par with the results of an earlier study conducted in Jimma (34.5%),35 but is higher than that reported from Hawassa, 17.0% (n=7).18 The higher rate of MRSA observed in the present study could be linked to the constant use of the third-generation cephalosporins. The coagulase-negative staphylococci, which are Methicillin-resistant (MRCoNs), were also detected in our study.
The overall percentage of VRE in our study was 58.3% and was consistent with the outcome of a study performed in Bahir Dar (41.7%).48 Of the isolated GNB, 71 (56.8%) were suspected to be ESBL producers, and precisely 25 (20.0%) were confirmed to be the actual ESBL producers.
Nine (7.2%) isolates were carbapenemase producers and can be connected to the indiscriminate use of carbapenem as a first-line drug, and this is more or less similar to the results related to the CRE isolates reported in other studies from different clinical samples obtained from Arba Minch itself (12.98% (17/131)),49 Addis Ababa, 12.12% (n=4/33),50 North Africa (2.3 to 67.7%), and sub-Saharan Africa (9 to 60%).51
Among the risk factors assessed, a couple of variables belonging to environmental factors were significantly associated (history of exposure to loud noises and a family history of smoking). It was found that patients with a history of exposure to loud noises are 3.4 times [(AOR=3.4; CI=1.141–10.237; P-value=0.028)] more prone to OM. It is envisaged that prolonged exposure to high-decibel noises may affect the eardrum, impair the respiratory and immune systems and make them vulnerable to infections. However, this factor was not significantly associated as per a previously published article52 and therefore, further in-depth clinical studies are required to bring out the fact involved. The patients with a family history of smoking have 2.9 times higher chance of acquiring OM than their peers [AOR=2.9; CI=1.189–7.251; p-value = 0.020]. Many previous studies have viewed the impact of a family history of smoking (passive smoking) on children and the incidence of OM.17 This finding is not unexpected since passive smoking can enhance bacterial adhesion to the respiratory epithelium, suppress local immune responses, and reduce mucociliary action.53 These results suggest that physicians/parents should consider developing interventions to discourage smoking in the family with pediatrics.
Limitations of the Study
Our current work has several shortcomings. For instance, it is a cross-sectional study design with a smaller sample size and a shorter duration.
It is based on institutions and may not represent the exact picture of the epidemiology of OM. Only aerobic bacterial cultures were performed. Serotyping and molecular characterizations of the bacterial isolates were not done. Audiological instrumental and API (Analytical Profile Index) 20E tests were not done. The significance of CSOM may be brought out in a future study with much larger sample size. The exact reason for the statistical association of OM with exposure to louder noises is to be further evaluated.
Conclusions
To the best of our knowledge, this is the first report on the magnitude of OM among the pediatric population in Arba Minch; the overall percentage of OM was extremely high, ie, 67.3%, and it has a certain association with environmental factors too.
From our results, we conclude that OM remains an ongoing challenge in the study area, causing significant morbidity in pediatric patients. Slightly above fifty percentage of the culture-positive cases were associated with CSOM and it is to be stressed that CSOM has far reaching consequences and specific sequelae. Isolates of Proteus spp., E. coli, and S. aureus were found to be the most prevalent otopathogens. It can be inferred that gentamicin, tetracycline, and ciprofloxacin are the options for managing OM in the study area. There exists a considerable augmentation in drug resistance (in the case of penicillin, ampicillin, amoxicillin-clavulanic acid, ceftriaxone, and co-trimoxazole). A startling finding of our study is that 67.1 and 19.2% of bacteria were MDR and XDR, respectively. The WHO prioritized superbugs such as ESBL, CRE, MRSA, and VRE were also detected. Significant predictors of OM in pediatrics in the study area are exposure to loud noises and a family history of smoking which are the most mentionable findings.
Acknowledgment
The authors would like to thank the College of Medicine and Health Sciences, Arba Minch University, and Arba Minch General Hospital. The authors extend their appreciation to the Researchers supporting project number (RSPD2023R543), King Saud University, Riyadh, Saudi Arabia. Thanks are extended to Dr. Sabu KR for critically reviewing the English.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Afolabi OA, Salaudeen AG, Ologe FE, Nwabuisi C, Nwawolo CC. Pattern of bacterial isolates in the middle ear discharge of patients with chronic suppurative otitis media in a tertiary hospital in North central Nigeria. Afr Health Sci. 2012;12(3):362–367. doi:10.4314/ahs.v12i3.18
2. Morris PS, Leach AJ. Acute and chronic otitis media. Pediatr Clin North Am. 2009;56(6):1383–1399. doi:10.1016/j.pcl.2009.09.007
3. Rovers MM, Schilder AG, Zielhuis GA, Rosenfeld RM. Otitis media. Lancet. 2004;363(9407):465–473. doi:10.1016/S0140-6736(04)15495-0
4. Grubb MS, Spaugh DC. Treatment failure, recurrence, and antibiotic prescription rates for different acute otitis media treatment methods. Clin Pediatr. 2010;49(10):970–975. doi:10.1177/0009922810370363
5. Taylor S, Marchisio P, Vergison A, Harriague J, Hausdorff WP, Haggard M. Impact of pneumococcal conjugate vaccination on otitis media: a systematic review. Clin Infect Dis. 2012;54(12):1765–1773. doi:10.1093/cid/cis292
6. Monasta L, Ronfani L, Marchetti F, et al. Burden of disease caused by otitis media: systematic review and global estimates. PLoS One. 2012;7(4):e36226. doi:10.1371/journal.pone.0036226
7. Muluye D, Wondimeneh Y, Ferede G, Moges F, Nega T. Bacterial isolates and drug susceptibility patterns of ear discharge from patients with ear infection at Gondar University Hospital, Northwest Ethiopia. BMC Ear Nose Throat Disord. 2013;13(1):10. doi:10.1186/1472-6815-13-10
8. Adoga AS, Ma’an EN, Malu D, Badung BP, Obiesie IV, Nwaorgu OG. Swab and aspiration specimen collection methods and antibiogram in chronic suppurative otitis media at Jos University Teaching Hospital: which is superior? Ann Afr Med. 2010;9(4):230–234. doi:10.4103/1596-3519.70961
9. Acuin J. Global Burden of Disease Due to Chronic Suppurative Otitis Media: Disease, Deafness, Deaths and DALYs Chronic Suppurative Otitis Media-Burden of Illness and Management Options. Geneva: World Health Organisation. 2004:9–23.
10. Danishyar A, Ashurst JV. Acute otitis media. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
11. Bluestone CD, Klein JO. Otitis Media in Infants and Children. PMPH-USA; 2007.
12. Atkinson H, Wallis S, Coatesworth AP. Otitis media with effusion. Postgrad Med. 2015;127(4):381–385. doi:10.1080/00325481.2015.1028317
13. Wallis S, Atkinson H, Coatesworth AP. Chronic otitis media. Postgrad Med. 2015;127(4):391–395. doi:10.1080/00325481.2015.1027133
14. Khairkar M, Deshmukh P, Maity H, et al. Chronic suppurative otitis media: a comprehensive review of epidemiology, pathogenesis, microbiology, and complications. Cureus. 2023;15(8):e43729. doi:10.7759/cureus.43729
15. Massa HM, Cripps AW, Lehmann D. Otitis media: viruses, bacteria, biofilms and vaccines. Med J Aust. 2009;191(S9):S44–S49. doi:10.5694/j.1326-5377.2009.tb02926.x
16. Tesfa T, Mitiku H, Sisay M, et al. Bacterial otitis media in sub-Saharan Africa: a systematic review and meta-analysis. BMC Infect Dis. 2020;20(1):225. doi:10.1186/s12879-020-4950-y
17. Wasihun AG, Zemene Y. Bacterial profile and antimicrobial susceptibility patterns of otitis media in Ayder Teaching and Referral Hospital, Mekelle University, Northern Ethiopia. Springerplus. 2015;4(1):701. doi:10.1186/s40064-015-1471-z
18. Tadesse B, Shimelis T, Worku M. Bacterial profile and antibacterial susceptibility of otitis media among pediatric patients in Hawassa, Southern Ethiopia: cross-sectional study. BMC Pediatr. 2019;19(1):398. doi:10.1186/s12887-019-1781-3
19. Molla R, Tiruneh M, Abebe W, Moges F. Bacterial profile and antimicrobial susceptibility patterns in chronic suppurative otitis media at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. BMC Res Notes. 2019;12(1):414. doi:10.1186/s13104-019-4452-4
20. Hailegiyorgis TT, Sarhie WD, Workie HM. Isolation and antimicrobial drug susceptibility pattern of bacterial pathogens from pediatric patients with otitis media in selected health institutions, Addis Ababa, Ethiopia: a prospective cross-sectional study. BMC Ear Nose Throat Disord. 2018;18(1):8. doi:10.1186/s12901-018-0056-1
21. Hailu D, Mekonnen D, Derbie A, Mulu W, Abera B. Pathogenic bacteria profile and antimicrobial susceptibility patterns of ear infection at Bahir Dar Regional Health Research Laboratory Center, Ethiopia. Springerplus. 2016;5(1):466. doi:10.1186/s40064-016-2123-7
22. Taoussi AA, Malloum MSM, Ali YA. Prevalence and clinico-bacteriological aspects of chronic suppurative otitis media at the Renaissance University Hospital in N’Djamena, Chad. Egypt J Otolaryngol. 2023;39(1):72. doi:10.1186/s43163-023-00437-9
23. Mama M, Manilal A. Laboratory Manual in Diagnostic Bacteriology. Lambert Publishers; 2019. ISBN 978-620-0-08182-7.
24. Collee JG, Marmion BP, Fraser AG, Simmons A, Mackie T. Mackie & McCartney Practical Medical Microbiology: Editors.
25. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. In: M100 Performance Standards for Antimicrobial [Internet].
26. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
27. Mittal R, Lisi CV, Gerring R, et al. Current concepts in the pathogenesis and treatment of chronic suppurative otitis media. J Med Microbiol. 2015;64(10):1103–1116. doi:10.1099/jmm.0.000155
28. World Health Organization. Chronic suppurative otitis media—burden of illness and management options [Internet]. WHO Library Cataloguing-in-Publication Data; 2004. doi:10.1016/j.amjoto.2007.09.002.
29. Mulwafu W, Kuper H, Ensink RJH. Prevalence and causes of hearing impairment in Africa. Trop Med Int Health. 2015;21(2):158–165. PMID:26584722. doi:10.1111/tmi.12640
30. Orji FT, Dike BO, Oji O. Oji O Determinants of non-healing ear discharge in chronic suppurative otitis media in a developing country. Eur Arch Otorhinolaryngol. 2015;272(10):2713–3278. doi:10.1007/s00405-014-3255-4
31. Li MG, Hotez PJ, Vrabec JT, Donovan DT, Pettigrew MM. Is chronic suppurative otitis media a neglected tropical disease? PLoS Negl Trop Dis. 2015;9(3):e0003485. doi:10.1371/journal.pntd.0003485
32. Mushi MF, Mwalutende AE, Gilyoma JM, et al. Predictors of disease complications and treatment outcome among patients with chronic suppurative otitis media attending a tertiary hospital, Mwanza Tanzania. BMC Ear Nose Throat Disord. 2016;16(1):1. doi:10.1186/s12901-015-0021-1
33. Khatun MR, Alam KMF, Naznin M, Salam MA. Microbiology of chronic suppurative otitis media: an update from a tertiary care hospital in Bangladesh. Pak J Med Sci. 2021;37(3):821–826. doi:10.12669/pjms.37.3.3942
34. Abera B, Kibret M. Bacteriology and antimicrobial susceptibility of otitis media at Dessie regional health research laboratory, Ethiopia. Ethiop J Health Dev. 2011;25(2):161–167.
35. Gorems K, Beyene G, Berhane M, Mekonnen Z. Antimicrobial susceptibility patterns of bacteria isolated from patients with ear discharge in Jimma Town, Southwest, Ethiopia. BMC Ear Nose Throat Disord. 2018;18(1):17. doi:10.1186/s12901-018-0065-0
36. Tanon-Anoh MJ, Kacou-Ndouba A, Yoda M, Ette-Akre E, Sanogo D, Kouassi B. Particularities of bacterial ecology of acute otitis media in an African subtropical country (Cote d’Ivoire). Int J Pediatr Otorhinolaryngol. 2006;70(5):817–822. doi:10.1016/j.ijporl.2005.09.009
37. Chirwa M, Mulwafu W, Aswani JM, Masinde PW, Mkakosya R, Soko D. Microbiology of chronic suppurative otitis media at Queen Elizabeth Central Hospital, Blantyre, Malawi: a cross-sectional descriptive study. Malawi Med J. 2015;27(4):120–124. doi:10.4314/mmj.v27i4.1
38. Aduda DS, Macharia IM, Mugwe P, et al. Bacteriology of chronic suppurative otitis media (CSOM) in children in Garissa district, Kenya: a point prevalence study. Int J Pediatr Otorhinolaryngol. 2013;77(7):1107–1111. doi:10.1016/j.ijporl.2013.04.011
39. Basnet R, Sharma S, Rana JC, Shah PK. Bacteriological study of otitis media and its antibiotic susceptibility pattern. J Nepal Health Res Counc. 2017;15(2):124–129. doi:10.3126/jnhrc.v15i2.18186
40. Flood LM. Scott-Brown’s Otorhinolaryngology and Head and Neck Surgery: Volume 1–3: Basic Sciences, Endocrine Surgery, Rhinology.
41. Al-Marzoqi AH, Al-Janabi HSO, Hussein HJ, Al Taee ZM, Yheea SK. Otitis media; etiology and antibiotics susceptibility among children under ten years old in Hillah city. Iraq J Nat Sci Res. 2013;3(3):2224–3186.
42. Alabbasi AM, Alsaimary IE, Najim JM. Prevalence and patterns of chronic suppurative otitis media and hearing impairment in Basrah city. J Med Med Sci. 2010;1(4):129–133.
43. Chandra Sahu M, Swain SK. Surveillance of antibiotic sensitivity pattern in chronic suppurative otitis media of an Indian teaching hospital. World J Otorhinolaryngol Head Neck Surg. 2019;5(2):88–94. doi:10.1016/j.wjorl.2018.05.008
44. Diriba M, Solomon G, Hailu N. Isolation and antimicrobial susceptibility pattern of bacterial pathogens causing otitis media in children in Jimma hospital, South Western Ethiopia. Ethiop J Health Sci. 2004;14(2):89–100.
45. Aklilu A, Agidew T, Manilal A, Woldemariam M. Antimicrobial use and awareness towards drug resistance among the community in Arba Minch Health and Demographic Surveillance site. In:
46. Argaw-Denboba A, Abejew AA, Mekonnen AG. Antibiotic-resistant bacteria are major threats of otitis media in Wollo Area, Northeastern Ethiopia: a Ten-year retrospective analysis. Int J Microbiol. 2016;2016:8724671. doi:10.1155/2016/8724671
47. Agha ZHM, Al-Delaimi MS. Prevalence of common bacterial etiology and antimicrobial susceptibility pattern in patients with otitis media in Duhok Province–Iraq. Zanco J Pure Appl Microbiol. 2021;33(4):11–25.
48. Ashagrie D, Genet C, Abera B, Karunasagar I. Vancomycin-resistant enterococci and coagulase-negative staphylococci prevalence among patients attending at Felege Hiwot Comprehensive Specialized Hospital, Bahir Dar, Ethiopia. PLoS One. 2021;16(4):e0249823. doi:10.1371/journal.pone.0249823
49. Mitiku A, Aklilu A, Tsalla T, Woldemariam M, Manilal A, Biru M. Magnitude and antimicrobial susceptibility profiles of Gram-Negative bacterial isolates among patients suspected of urinary tract infections in Arba Minch General Hospital, southern Ethiopia. PLoS One. 2022;17(12):e0279887. doi:10.1371/journal.pone.0279887
50. Legese MH, Weldearegay GM, Asrat D. Extended-spectrum beta-lactamase- and carbapenemase-producing Enterobacteriaceae among Ethiopian children. Infect Drug Resist. 2017;10:27–34. doi:10.2147/IDR.S127177
51. Manenzhe RI, Zar HJ, Nicol MP, Kaba M. The spread of carbapenemase-producing bacteria in Africa: a systematic review. J Antimicrob Chemother. 2015;70(1):23–40. doi:10.1093/jac/dku356
52. Zhang Y, Xu M, Zhang J, Zeng L, Wang Y, Zheng QY. Risk factors for chronic and recurrent otitis media–a meta-analysis. PLoS One. 2014;9(1):e86397. doi:10.1371/journal.pone.0086397
53. Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med. 2004;164(20):2206–2216. doi:10.1001/archinte.164.20.2206
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.