Back to Journals » Infection and Drug Resistance » Volume 17
Factors Associated with Mortality Among Severe Omicron Patients for COVID-19
Authors Wu S, Liao G, Mao J, Yan H ![]() , Chen J, Peng J
, Chen J, Peng J
Received 17 December 2023
Accepted for publication 13 March 2024
Published 3 April 2024 Volume 2024:17 Pages 1309—1319
DOI https://doi.org/10.2147/IDR.S450504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Shuting Wu, Guichan Liao, Jingchun Mao, Haiming Yan, Juanjuan Chen, Jie Peng
Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, People’s Republic of China
Correspondence: Jie Peng, Department of Infectious Diseases, Nanfang Hospital, Southern Medical University, Guangzhou, 510515, People’s Republic of China, Tel +8613802515784, Fax +86 20 87719653, Email [email protected]
Purpose: The purpose of the study was to explore the potential risk factors of mortality in patients with severe pneumonia during the omicron pandemic in South China in 2022.
Methods: Clinical data was collected from patients hospitalized with omicron COVID-19. Then, patients were categorized into the non-survival and survival groups. A comprehensive analysis was conducted to analyze the factors associated with negative outcome in individuals suffering from severe omicron COVID-19.
Results: In this study, 155 severe COVID-19 patients were included, comprising 55 non-survivors and 100 survivors. Non-survivors, in comparison to survivors, exhibited elevated levels of various biomarkers including neutrophil count, hypersensitive troponin T, urea, creatinine, C-reactive protein, procalcitonin, interleukin-6, plasma D-dimer, and derived neutrophil-to-lymphocyte ratio (dNLR) (P < 0.05). They also displayed reduced lymphocyte count, platelet count, and albumin levels (P < 0.05) and were more prone to developing comorbidities, including shock, acute cardiac and renal injury, acute respiratory distress syndrome, coagulation disorders, and secondary infections. Platelet count (PLT) < 100 × 10^/L, interleukin-6 (IL-6) > 100 pg/mL, and dNLR > 5.0 independently contributed to the risk of death in patients suffering from severe COVID-19.
Conclusion: PLT, IL-6, and dNRL independently contributed to the risk of mortality in patients with severe pneumonia during the 2022 omicron pandemic in South China.
Keywords: COVID-19, omicron, severe infection, dNLR, risk factors
Introduction
Throughout the COVID-19 pandemic, a multitude of SARS-CoV-2 variants have surfaced, exhibiting variances in both transmissibility and clinical impact. Initially detected in Botswana on November 11, 2021, the omicron (B.1.1.529) variant was first reported in South Africa on November 24, 2021.1,2 On November 26, 2021, the World Health Organization (WHO) formally classified omicron as a variant of significant concern.1 The initial case of omicron within mainland China was officially reported on December 9, 2021, which subsequently precipitated a widespread outbreak in southern China in December 2022.3 To date, the omicron variant has been identified in 215 countries.4
Various studies have shown that the clinical manifestations of infection for omicron were comparatively milder than those for delta.5–10 Estimates of vaccine efficacy reveal a reduced level of protection against symptomatic omicron infection compared to delta, which is mild after the primary vaccination series. However, this protection improves to a moderate degree against symptomatic infection and demonstrates a high efficacy in preventing hospitalization after the administration of a booster dose.11 It is crucial to note that China’s vaccination rates for booster shots remain low. Consequently, a significant number of patients were admitted with severe pneumonia during the omicron wave in southern China in 2022, and death is a serious adverse outcome for these severe patients. A detailed understanding is needed of the characteristics and related factors that influence mortality in patients suffering from severe COVID-19.
Previous studies have observed a decrease in the immune response in patients with COVID-19, resulting in laboratory parameter changes (particularly those that are related to complete blood count and inflammation).12 In addition, the relationship between laboratory parameters and the severity, but not the mortality of COVID-19 had also been studied.13 Still, the severity of the disease was primarily determined by its clinical symptoms. Therefore, analyzing early laboratory indicators is important to predict the progression of severe diseases and thus prevent adverse outcomes. A novel biomarker of systemic inflammation, the derived neutrophil-to-lymphocyte ratio (dNLR), defined as the absolute neutrophil count/[white cell count—absolute neutrophil count], has exhibited prognostic implications in various cancer categories.14,15 International studies have underscored its association with inflammation severity in COVID-19 patients.16 Notably, comprehensive national data concerning its association with death in severe omicron COVID-19 cases are presently lacking.
In this research, we aimed to analyze the characteristics and risk factors associated with mortality in patients with severe omicron COVID-19.
Methods
Ethics
The research was a retrospective design. Our research had been verified and authorized by the Institutional Ethics Committee of Nanfang Hospital (study identifier NFEC-2023-446) and conducted following the principles of the Helsinki Declaration of 1964 and its subsequent revisions. Every patient has given written informed consent, agreed to adhere to the protocol, and allowed the publication of their medical record details in an anonymous manner.
Study Population
The minimum sample size was calculated, and 155 patients with severe omicron COVID-19 who were hospitalized in the department of infectious diseases and intensive care units in Nanfang Hospital of Southern Medical University in Guangzhou, China, between December 1, 2022, and February 5, 2023, were selected to participate in the study as subjects. Inclusion criteria: (1) ≥18 years old; (2) laboratory confirmed omicron SARS-CoV-2 infection; (3) clinical classification consistent with severe or critical type; (4) all patients and their families had been informed and signed informed consent forms. Exclusion criteria: (1) incomplete medical records; (2) patients who were unwilling to participate in this study.
Operational Definition
Severe is defined as meeting any of the following criteria: ①Experiencing respiratory distress with a respiratory rate of ≥30 breaths/min; ②Having finger oxygen saturation ≤93% while inhaling air at rest; ③Partial pressure of oxygen in the arterial blood (PaO2)/oxygen concentration at the time of inspiration (FiO2) ≤300 mmHg; ④Increasing severity of clinical signs, and imaging of the lungs showing a lesion that had progressed >50% within 24–48 h. Critical is defined as respiratory failure requiring mechanical ventilation, shock, and other organ failure requiring ICU care. The above diagnoses and clinical classification were made according to the NIH COVID-19 Treatment Guidelines.17 The criteria for defining sepsis and septic shock were established using the 2016 Third International Consensus Definition.10 The diagnosis of secondary infection was established upon the manifestation of clinical signs or symptoms of pneumonia or bacteremia in patients, coupled with the identification of a new pathogen through positive cultures derived from specimens taken from lower respiratory tract or blood samples after admission.18 Acute kidney injury diagnosis followed the clinical practice guidelines of the Kidney Disease Improving Global Outcomes (KDIGO) organization,19 while the diagnosis of acute respiratory distress syndrome (ARDS) was made based on the criteria outlined in the Berlin Definition.20 An acute cardiac injury was diagnosed by serum levels above 99th percentiles of upper reference limits, or by new abnormalities on ECG and echocardiography. Coagulopathy was operationally defined as a 3-second prolongation of prothrombin time or a 5-second prolongation of the activated partial thromboplastin time.18
Data Collection
Baseline clinical data of all enrolled inpatients were collected, including age, gender, vital signs, duration of hospitalization, smoking history, pre-existing chronic conditions, and associated complications. Laboratory metrics included blood cell count, albumin, total bilirubin, urea, creatinine, C-reactive protein, procalcitonin, IL-6, hypersensitive troponin T, plasma fibrinogen, and D-dimer. Additionally, we introduced dNLR, defined by the absolute neutrophil count/[white cell count-absolute neutrophil count], into the analysis to investigate its association with adverse outcomes in severe omicron COVID-19 cases.
Statistical Analysis
In this study, G*Power 3.1.9.7 (https://g-power.apponic.com/) was used to perform a power calculation. For 80% power with α set at 0.05, a total sample size of 128 participants was needed. Categorical variables and continuous variables were reported as frequency with percentage and the median with interquartile range (IQR), respectively. Chi-square tests and Wilcoxon rank-sum test were used to determine the differences between groups. Restricted cubic spline (RCS) was utilized to show the non-linear relationship among neutrophil count, lymphocyte count, platelet count, interleukin-6, hypersensitive troponin t, dNLR and mortality in patients with severe omicron COVID-19. Based on their clinical significance, we stratified the above six indicators. After that, we performed univariate and multivariate logistic regression to analyze what factors are associated with a poor prognosis for patients with severe COVID-19. The correlation between dNLR and relevant clinical and biochemical factors was examined using the Spearman correlation coefficient. It was considered statistically significant if the significance level was less than 0.05. The statistical analysis was performed in strict adherence to the prescribed statistical methods utilizing GraphPad Prism (v8.0, GraphPad software), SPSS (v26.0), and R v4.2.2.
Results
Demographic Characteristics and Clinical Symptoms in Patients with Severe Omicron COVID-19
A total of 203 adult patients were hospitalized in the department of infectious diseases and the intensive care units, at Nanfang Hospital in Guangzhou and tested positive for SARS-CoV-2 RNA from December 1, 2022 to February 5, 2023. Final analysis included 155 inpatients after excluding 36 non-severe patients and 12 inpatients whose medical records did not have critical information. Figure 1 depicts the selection process of the study. Fifty-five patients died, of which 41 died during hospitalization, and the other 14 died during follow-up after discharge; 100 patients were cured and discharged. There was a significant difference between survival and non-survival groups in respiratory rate (P < 0.001), dyspnea (P < 0.001), white blood cell (P = 0.022), lymphocyte (P = 0.001), neutrophil (P = 0.003), platelet (P < 0.001), albumin (P = 0.049), total bilirubin (P = 0.049), urea (P < 0.001), creatinine (P < 0.001), C-reactive protein (P = 0.008), procalcitonin (P < 0.001), IL-6 (P < 0.001), hypersensitive troponin T (P < 0.001), D-dimer (P = 0.005), shock (P < 0.001), acute cardiac injury (P < 0.001), acute kidney injury (P < 0.001), acute respiratory distress syndrome (P < 0.001), coagulopathy (P < 0.001), secondary infection (P < 0.001), and dNLR (P < 0.001), a new serological biomarker. Patients’ detailed characteristics are shown in Table 1.
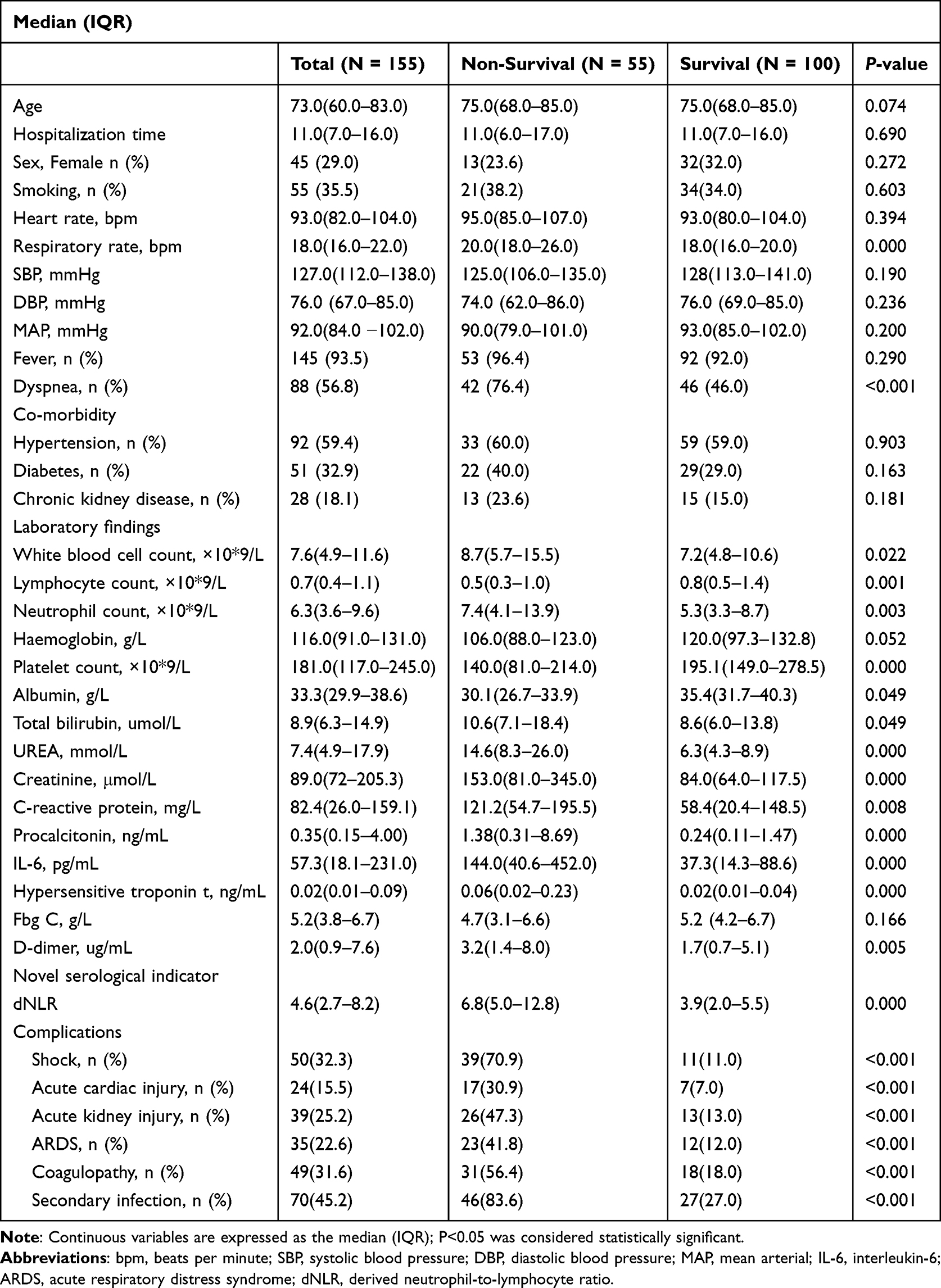 |
Table 1 The Demographics and Clinical Characteristics of Patients Enrolled |
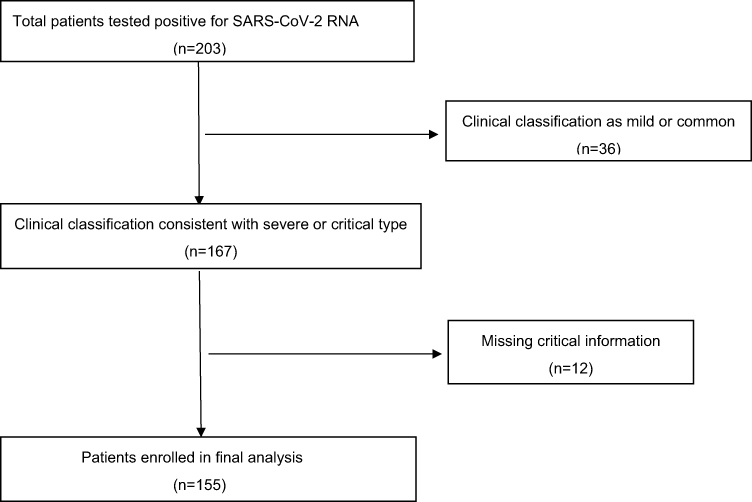 |
Figure 1 Flow chart for patient selection. |
Analysis of Factors Associated with Death in Severe Omicron COVID-19 Patients
Restricted cubic spline suggested the relationship among neutrophil count, lymphocyte count, platelet count, interleukin-6, hypersensitive troponin t, dNLR, and mortality was no-linear (all p for non-linearity <0.05; Figure 2). In univariate logistic regression analysis, age (OR = 1.026, 95% CI 1.003–1.049; P = 0.025), neutrophil count >6.5×10^9/L (OR = 2.737, 95% CI 1.386–5.406; P = 0.004), lymphocyte count <0.74 × 10*9/L (OR = 4.000, 95% CI1.955–8.182; P < 0.001), platelets count <100×10^9/L (OR = 5.778, 95% CI 2.401–13.902, P < 0.001), interleukin-6 >100pg/mL (OR = 4.580, 95% CI 2.246–9.339; P < 0.001), dNLR >5.0 (OR = 8.735,95% CI 4.074 −18.730; P < 0.001), hypersensitive-troponin-t >0.02ng/mL (OR = 7.788, 95% CI 3.336 −18.179, P < 0.001), procalcitonin (OR = 1.040, 95% CI 1.009 −1.072, P = 0.012), C-reactive protein (OR = 1.004, 95% CI 1.001–1.008, P = 0.022), D-dimer (OR = 1.051, 95% CI 1.000 −1.104, P = 0.048), acute cardiac injury (OR = 5.944, 95% CI 2.281–15.487, P < 0.001), acute kidney injury (OR = 6.000, 95% CI2.730–13.185, P < 0.001), acute respiratory distress syndrome (OR =5.271,95% CI2.352–11.810, P < 0.001), coagulopathy (OR = 5.884, 95% CI 2.814–12.305, P < 0.001), secondary infection (OR = 16.185, 95% CI 6.924–37.833, P < 0.001) were associated with death (Table 2). The final multivariate logistic regression analysis (Table 2) showed that platelets count <100 × 10^9/L (OR = 11.038,95% CI 3.165–38.495, P < 0.001), interleukin-6 >100pg/mL (OR = 2.558, 95% CI 1.072–6.106, P = 0.034) and dNLR >5.0 (OR = 6.555, 95% CI 2.572–16.705; P < 0.001) were significantly correlated with poor prognosis, suggesting that platelets count <100 × 10^9/L, interleukin-6 >100 pg/mL, and dNLR >5.0 were the independent risk factors of death in severe omicron COVID-19.
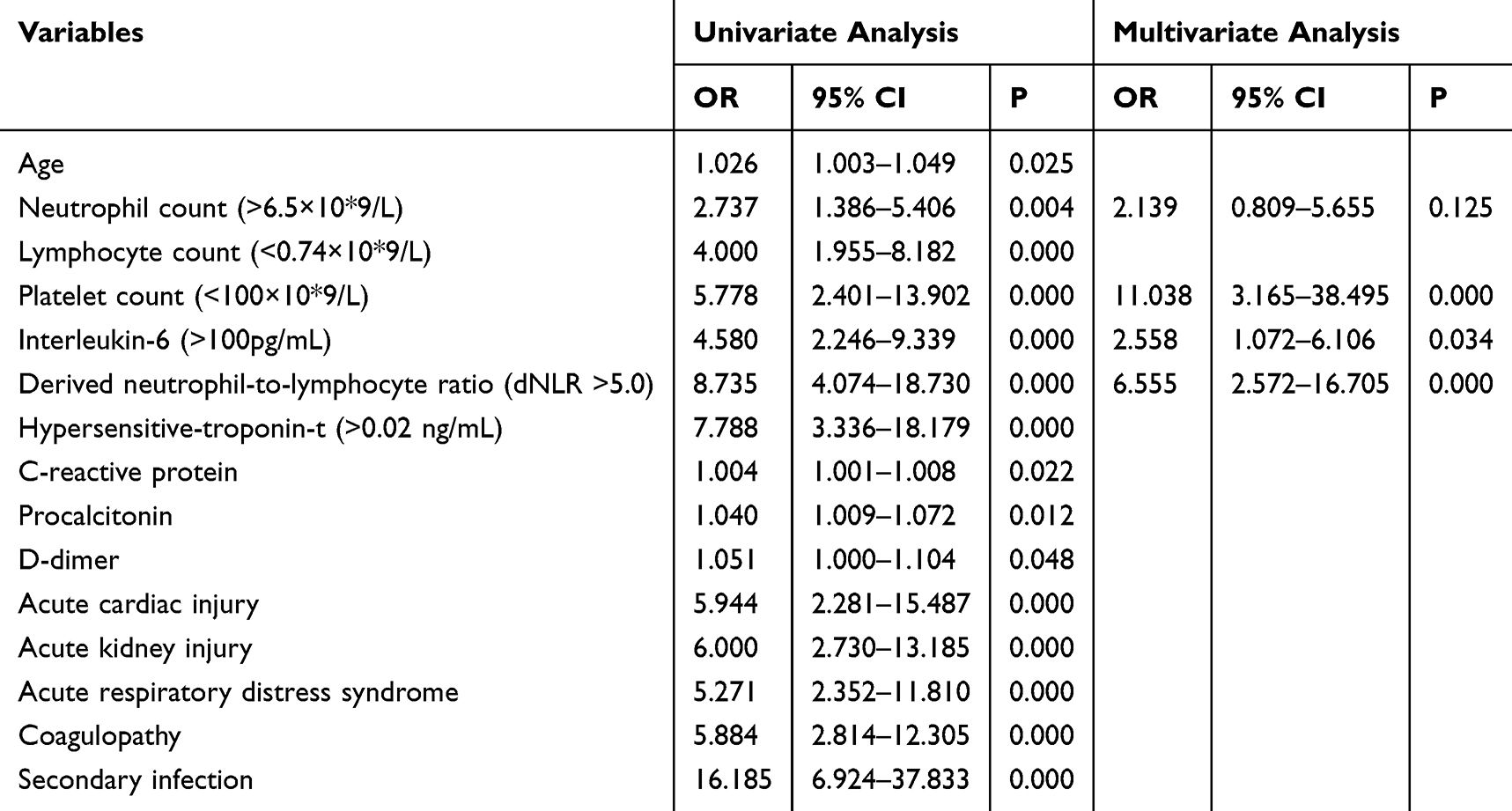 |
Table 2 Logistic Regression Analysis on the Risk Factors of Death in Severe COVID-19 Patients |
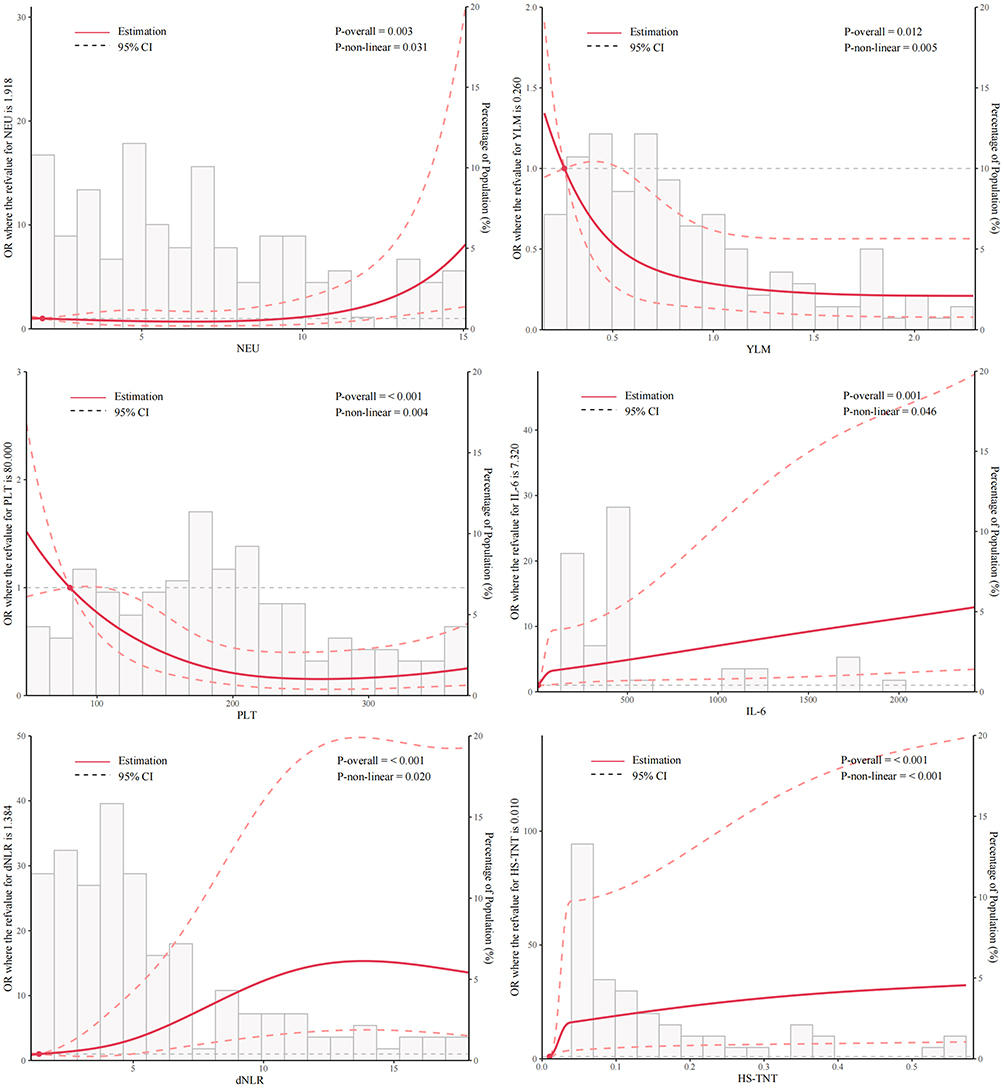 |
Figure 2 Non-linear relationship among neutrophil count, lymphocyte count, platelet count, interleukin-6, hypersensitive troponin t, dNLR and mortality in severe patients using restricted cubic spline. |
Correlation Analysis of Potential Marker of dNLR with Other Indicators
The dNLR significantly correlated with age (r = 0.160, P = 0.047), monocyte (r = 0.226, P = 0.004), albumin (r = 0.342, P < 0.001), urea (r = 0.353, P < 0.001), fibrinogen C (r = 0.168, P = 0.036), procalcitonin (r = 0.198, P = 0.013), and C-reactive protein (r = 0.392, P < 0.001). dNLR was independently associated with death in severe omicron patients. The findings are illustrated in Figure 3.
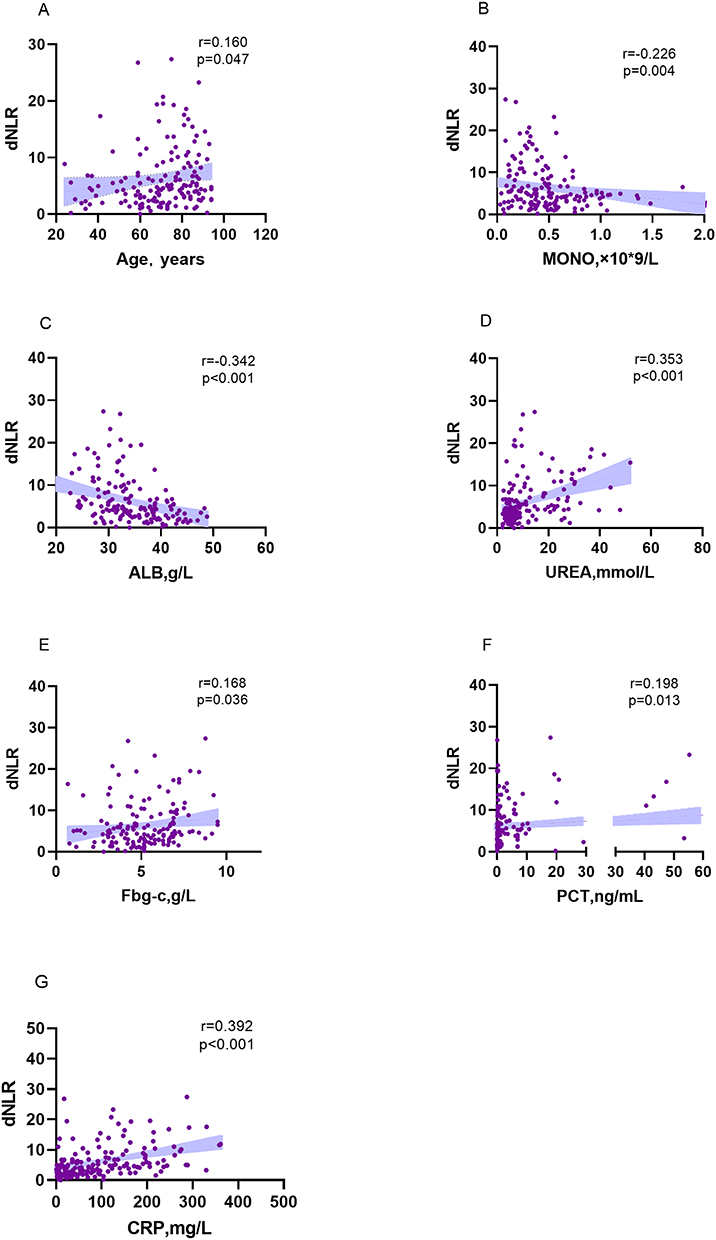 |
Figure 3 Correlation of dNLR with other clinical variables. dNLR level by age (A), MONO (B), ALB(C), UREA(D), Fbg-c(E), PCT(F), and CRP(G). Abbreviations: MONO, monocyte count; ALB, albumin; Fbg-c, plasma fibrinogen; PCT, Procalcitonin; CRP, C-reactive protein. |
Discussion
In this retrospective study, several risk factors for death were identified among adults hospitalized with severe COVID-19. Particularly, when platelets count <100 × 10^9/L, interleukin-6 >100pg/mL, and dNLR >5.0 were present on admission, the odds of death were higher. In non-survivors, elevated levels of neutrophil count, blood infection indicators such as interleukin-6, C-reactive protein, procalcitonin, high-sensitivity cardiac troponin T, and plasma D-dimer were observed. Additionally, decreased levels of lymphocyte count and albumin were more commonly seen, consistent with findings from prior studies.21–23
The derived neutrophil-to-lymphocyte ratio (dNLR) exhibits a correlation with systemic inflammatory status and disease activity. Higher dNLR has been reported associated with the development of death in various cancer types.15,24 Additionally, dNLR is a variable in risk-scoring models which associate with critical illness in COVID-19 patients.25 Several studies have recognized its independent significance in affecting mortality.16,26 Similarly, our study confirmed that dNLR >5.0 was associated with death in patients with severe omicron infection. The dNLR was derived from the following equation: absolute neutrophil count/[white cell count—absolute neutrophil count], and the assumption that the white blood cell count is primarily composed of lymphocytes and neutrophils. Subtracting the neutrophil count from the white blood cell count yields a value that approximates the lymphocyte count. Sun et al showed that patients with COVID-19 have the lowest lymphocyte count and the highest neutrophil count during the severe phase of the disease.27 Additionally, during the severe phase, Wang et al reported rising neutrophils and declining lymphocytes in several COVID-19 patients.28 According to Barnes et al, COVID-19 patients have extensive neutrophil infiltration in their pulmonary capillaries.29
Neutrophils are major components among the leukocyte population that migrate from the venous system to the immune system. As a result, they release reactive oxygen to damage DNA and release viruses. Therefore, antibody-dependent cell-mediated cytotoxicity (ADCC) has the ability to directly eliminate viruses, reveal viral antigens, and activate both humoral and cellular immunity.30 Furthermore, in addition to interacting with diverse cellular communities, NEU also produces cytokines and other effector substances, like circulating vascular endothelial growth factor (VEGF). In turn, angiogenesis, growth, and metastasis of tumors are facilitated by VEGF.31 Notably, COVID-19 patients exhibit significantly elevated expressions of VEGF-A and VEGF-C compared to those observed in healthy tissues,32 and a decrease in VEGF and VEGFR expression significantly inhibits organ and tissue damage. In addition, the initiation of NEU can be prompted by viral-associated inflammatory mediators, including IL-8, TNF-alpha, and G-CSF, along with interferon-gamma factors produced in endothelial and lymphocyte cells.33–35
Immune response in humans, when triggered by a viral infection, primarily depends on lymphocytes,36 while systemic inflammation has a notable suppressive effect on cellular immunity, leading to a significant decrease in CD4+ T lymphocytes and an increase in CD8+ suppressor T lymphocytes.37 Consequently, virus-induced inflammation leads to an increased dNLR. This elevated dNLR may, in turn, facilitate the progression of COVID-19 and contribute to an unfavorable prognosis.
Previously, thrombocytopenia has been identified as a potential cause of death in cases of SARS and MERS.38,39 In the study, we found that thrombocytopenia was also considered a risk factor of poor prognosis. In patients with COVID-19, reduced TPO production, increased platelet clearance, a dysfunctional BM microenvironment, lung damage, and antiviral drugs may contribute to thrombocytopenia, leading to DIC.40
IL-6, also known as Interleukin-6, has a vital function in immune and inflammatory reactions.41 In this study, an increased level of IL-6 has been identified as an independent risk factor of poor prognosis. This finding is supported by several previous studies.42,43 IL-6 typically helps maintain immune homeostasis and combats infections by regulating the immune response, promoting inflammation, and modulating platelet function.44 However, in severe COVID-19 cases, excessively elevated IL-6 levels can trigger a cytokine storm, resulting in ARDS and thrombosis. This excessive inflammation affects pulmonary responses and viral replication, potentially resulting in multi-organ failure and, in some cases, death.45,46 In summary, while IL-6 is essential for the immune response, its overexpression in severe COVID-19 can have detrimental effects on the patient’s health, leading to a poorer prognosis.
The study found that age was related to death in univariate logistic regression, but a multivariate logistic regression showed age was not an independent risk factor. Despite prior research indicating a substantial association between disease severity and age,21,26,47 When compared with the general population of positive cases of COVID-19, an Italian study found no age disparities among those admitted to ICU with the disease.48 Consequently, this discovery implies that age, when considered independently, does not act as a solitary risk factor for ICU admission.
Certainly, there are some limitations to our study. First, the sample size might limit the interpretation of our findings. Future studies with larger samples size and rigorous design are needed to further elucidate the related factors of mortality in severe COVID-19 patients. Second, due to the nature of the retrospective study, certain laboratory tests such as lactate dehydrogenase and serum ferritin assessments were not conducted in all patients. Consequently, their role in influencing adverse prognosis may be underestimated. Third, our study aimed to examine severe inpatients infected with omicron in southern China at the end of 2022. Due to limited antiviral drug supply, critical patients were prioritized for treatment, our analysis did not encompass a comprehensive evaluation of therapeutic interventions. Fourth, due to this study’s single-center design and lack of comprehensive coverage of all hospitalized patients. Our case fatality ratio observed in our research may not accurately reflect severe omicron COVID-19 mortality.
Conclusion
In summary, in this retrospective study, for patients with platelets count <100 × 10^9/L, interleukin-6 >100 pg/mL, and dNLR >5.0 measured at admission, they may have higher risks for the development of death, prevention and early warning should be taken to reduce mortality.
Data Sharing Statement
Without undue reservation, the corresponding authors will make available raw data for this article upon request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research for this study was supported by the National Key Research and Development Program of China (No. 2022YFC2304800), the National Natural Science Foundation of China (81572000), the Clinical Research Program of Nanfang Hospital, Southern Medical University (No. 2018CR026), the Natural Science Foundation of Guangdong Province (No. 2023A1515030252), and the Municipal and University (Hospital) joint funding project of Guangzhou Municipal Science and Technology Bureau (No. 202201020253, 202201020250, and 2023A03J0796).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. World Health Organization. Classification of omicron (B.1.1.529): SARS-CoV-2 variant of concern; 2021. Available from: https://www.who.int/news/item/26-11-2021classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern.
2. Centers for Disease Control and Prevention. Science brief: omicron (B.1.1.529) variant. Available from: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/scientific-brief-omicron-variant.html.
3. Chinese center for disease control and prevention; 2023. Available from: https://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/jszl_13141/202307/t20230705_267605.html.
4. GISAID. Tracking of variants. Available from: https://www.gisaid.org/hcov19variants/.
5. Wolter N, Jassat W, Walaza S, et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet. 2022;399(10323):437–446. doi:10.1016/S0140-6736(22)00017-4
6. Ferguson N, Ghani A, Hinsley W, Volz E Report 50: hospitalisation risk for omicron cases in England; 2021. Available from: https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-19/report-50severity-omicron/.
7. Ulloa AC, Buchan SA, Daneman N, Brown KA. Estimates of SARS-CoV-2 omicron variant severity in Ontario, Canada. JAMA. 2022;327(13):1286–1288. doi:10.1001/jama.2022.2274
8. Lewnard JA, Hong VX, Patel MM, Kahn R, Lipsitch M, Tartof SY. Clinical outcomes among patients infected with omicron (B.1.1.529) SARS-CoV-2 variant in southern California. Nat Med. 2022;28(9):1933–1943. doi:10.1038/s41591-022-01887-z
9. Abdullah F, Myers J, Basu D, et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in Tshwane, South Africa. Int J Infect Dis. 2022;116:38–42. doi:10.1016/j.ijid.2021.12.357
10. Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):775–787. doi:10.1001/jama.2016.0289
11. Andrews N, Stowe J, Kiresbom F, et al. Effectiveness of COVID-19 vaccines against the omicron (B.1.1.529) variant of concern. NEJM. 2022;399:1303–1312.
12. Mertoglu C, Huyut MT, Olmez H, et al. COVID-19 is more dangerous for older people and its severity is increasing: a case-control study. Med Gas Res. 2022;12(2):51–54. doi:10.4103/2045-9912.325992
13. Kosidlo JW, Wolszczak-Biedrzycka B, Dymicka-Piekarska V, et al. Clinical significance and diagnostic utility of NLR, LMR, PLR and SII in the Course of COVID-19: a literature review. J Inflamm Res. 2023;16:539–562. doi:10.2147/JIR.S395331
14. Proctor MJ, McMillan DC, Morrison DS, et al. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br J Cancer. 2012;107(4):695–699. doi:10.1038/bjc.2012.292
15. Yang T, Hao L, Yang X, et al. Prognostic value of derived neutrophil-to-lymphocyte ratio (dNLR) in patients with non-small cell lung cancer receiving immune checkpoint inhibitors: a meta-analysis. BMJ open. 2021;11(9):e049123. doi:10.1136/bmjopen-2021-049123
16. Citu C, Gorun F, Motoc A, et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics. 2022;12(1):122. doi:10.3390/diagnostics12010122
17. Information on COVID-19 Treatment, Prevention and Research. COVID-19 Treatment Guidelines; 2023, Available from: https://www.covid19treatmentguidelines.nih.gov/.
18. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
19. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–184. doi:10.1159/000339789
20. Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. doi:10.1001/jama.2012.5669
21. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
22. Hh Z, Xj H, Huang X-J. Abnormal indexes of liver and kidney injury markers predict severity in COVID-19 patients. Infec Drug Resist. 2021;14:3029–3040. doi:10.2147/IDR.S321915
23. Gong J, Ou J, Qiu X, et al. A tool for early prediction of severe coronavirus disease 2019 (COVID-19): a multicenter study using the risk nomogram in Wuhan and Guangdong, China. Clin Infect Dis. 2020;71(15):833–840. doi:10.1093/cid/ciaa443
24. Grenader T, Nash S, Adams R, et al. Derived neutrophil lymphocyte ratio is predictive of survival from intermittent therapy in advanced colorectal cancer: a post hoc analysis of the MRC COIN study. Br J Cancer. 2016;114(6):612–615. doi:10.1038/bjc.2016.23
25. Dymicka-Piekarska V, Dorf J, Milewska A, et al. Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – risk of Death Inflammatory Biomarkers in Patients with COVID-19. J Inflamm Res. 2023;16(16):2209–2222. doi:10.2147/JIR.S409871
26. Fois AG, Paliogiannis P, Scano V, et al. The Systemic Inflammation Index on Admission Predicts In-Hospital Mortality in COVID-19 Patients. Molecules. 2020;25(23):5725. doi:10.3390/molecules25235725
27. Sun S, Cai X, Wang H, et al. Abnormalities of peripheral blood system in patients with COVID-19 in Wenzhou, China. Clin Chim Acta. 2020;507:174–180. doi:10.1016/j.cca.2020.04.024
28. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
29. Barnes BJ, Adrover JM, Baxter-Stoltzfus A, et al. Targeting potential drivers of COVID-19: neutrophil extracellular traps. J Exp Med. 2020;217(6):doi:10.1084/jem.20200652
30. Kusumanto YH, Dam WA, Hospers GAP, et al. Platelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular-endothelial growth factor. Angiogenesis. 2003;6(4):283–287. doi:10.1023/B:AGEN.0000029415.62384.ba
31. Hanrahan V, Currie MJ, Gunningham SP, et al. The angiogenic switch for vascular endothelial growth factor (VEGF)-A, VEGF-B, VEGF-C, and VEGF-D in the adenoma-carcinoma sequence during colorectal cancer progression. J Pathol. 2003;200(2):183–194. doi:10.1002/path.1339
32. Kim SL, Lee ST, Trang KTT, et al. Parthenolide exerts inhibitory effects on angiogenesis through the downregulation of VEGF/VEGFRs in colorectal cancer. Int J Mol Med. 2014;33(5):1261–1267. doi:10.3892/ijmm.2014.1669
33. Kuper H, Adami H-O, Trichopoulos D. Infections as a major preventable cause of human cancer. J Intern Med. 2000;248(3):171–183. doi:10.1046/j.1365-2796.2000.00742.x
34. Blaser MJ, Chyou PH, Nomura A. Age at establishment of Helicobacter pylori infection and gastric carcinoma, gastric ulcer, and duodenal ulcer risk. Cancer Res. 1995;55(3):562–565.
35. Zhao X, Zhou L, Kou Y, Kou J. Activated neutrophils in the initiation and progression of COVID-19: hyperinflammation and immunothrombosis in COVID-19. Am J Transl Res. 2022;14(3):1454–1468.
36. Rabinowich H, Cohen R, Bruderman I, Steiner Z, Klajman A. Functional analysis of mononuclear cells infiltrating into tumors: lysis of autologous human tumor cells by cultured infiltrating lymphocytes. Cancer Res. 1987;47(1):173–177.
37. Menges T, Engel J, Welters I, et al. Changes in blood lymphocyte populations after multiple trauma: association with posttraumatic complications. Crit Care Med. 1999;27(4):733–740. doi:10.1097/00003246-199904000-00026
38. Choi KW, Chau TN, Tsang O, et al. Outcomes and prognostic factors in 267 patients with severe acute respiratory syndrome in Hong Kong. Ann Intern Med. 2003;139(9):715–723. doi:10.7326/0003-4819-139-9-200311040-00005
39. Saad M, Omrani AS, Baig K, et al. Clinical aspects and outcomes of 70 patients with Middle East respiratory syndrome coronavirus infection: a single-center experience in Saudi Arabia. Int J Infect Dis. 2014;29:301–306. doi:10.1016/j.ijid.2014.09.003
40. Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020;18(4):844–847. doi:10.1111/jth.14768
41. Hunter CA, Jones SA. IL-6 as a keystone cytokine in health and disease. Nat Immunol. 2015;16(5):448–457. doi:10.1038/ni.3153
42. Ramasamy S, Subbian S. Critical determinants of cytokine storm and type i interferon response in COVID-19 pathogenesis. Clin Microbiol Rev. 2021;34(3):e00299–20. doi:10.1128/CMR.00299-20
43. Wolszczak-Biedrzycka B, Dorf J, Milewska A, et al. The Diagnostic Value of Inflammatory Markers (CRP, IL6, CRP/IL6, CRP/L, LCR) for Assessing the Severity of COVID-19 Symptoms Based on the MEWS and Predicting the Risk of Mortality. J Inflamm Res. 2023;(16):2173–2188. doi:10.2147/JIR.S406658
44. Kishimoto T, Kang S IL-6 revisited: from rheumatoid arthritis to CAR T Cell Therapy and COVID-19. Annu Rev Immunol. 2022;40:323–348. doi:10.1146/annurev-immunol-101220-023458
45. Xu X, Han M, Li T, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci U S A. 2020;117(20):10970–10975. doi:10.1073/pnas.2005615117
46. Ye Q, Wang B, Mao J. The pathogenesis and treatment of the `Cytokine Storm’ in COVID-19. J Infect. 2020;80(6):607–613. doi:10.1016/j.jinf.2020.03.037
47. Chen L, Yu J, He W, et al. Risk factors for death in 1859 subjects with COVID-19. Leukemia. 2020;34(8):2173–2183. doi:10.1038/s41375-020-0911-0
48. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.