Back to Journals » Patient Preference and Adherence » Volume 15
Factors Associated with Heart Failure Knowledge and Adherence to Self-Care Behaviors in Hospitalized Patients with Acute Decompensated Heart Failure Based on Data from “the Weak Heart” Educational Program
Authors Kolasa J, Lisiak M ![]() , Grabowski M, Jankowska EA
, Grabowski M, Jankowska EA ![]() , Lelonek M
, Lelonek M ![]() , Nessler J, Pawlak A, Uchmanowicz I
, Nessler J, Pawlak A, Uchmanowicz I ![]()
Received 16 December 2020
Accepted for publication 6 May 2021
Published 15 June 2021 Volume 2021:15 Pages 1289—1300
DOI https://doi.org/10.2147/PPA.S297665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jolanta Kolasa,1 Magdalena Lisiak,2 Marcin Grabowski,3 Ewa A Jankowska,4 Malgorzata Lelonek,5 Jadwiga Nessler,6 Agnieszka Pawlak,7 Izabella Uchmanowicz2
1Medical Unit Cardiology, Novartis Poland Sp. z o.o, Warsaw, Poland; 2Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland, and Centre for Heart Diseases, University Hospital, Wroclaw, Poland; 3 1st Department of Cardiology, Medical University of Warsaw, Warsaw, Poland; 4Centre for Heart Diseases, University Hospital, Wroclaw, Poland, and Department of Heart Diseases, Wroclaw Medical University, Wroclaw, Poland; 5Department of Noninvasive Cardiology, Medical University of Lodz, Lodz, Poland; 6Department of Coronary Disease and Heart Failure, Jagiellonian University Medical College, John Paul II Hospital, Krakow, Poland; 7Department of Invasive Cardiology, Centre of Postgraduate Medical Education, Central Clinical Hospital of the Ministry of the Interior and Administration, Warsaw, Poland, and Department of Applied Physiology, Mossakowski Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland
Correspondence: Jolanta Kolasa
Medical Unit Cardiology, Novartis Poland Sp. z o.o, Marynarska 15, Warsaw, 02-674, Poland
Tel +48 22 375 48 88
Email [email protected]
Purpose: As insufficient adherence to recommendations is a major cause of poor health outcomes in patients with heart failure (HF), it is important to identify the factors that improve disease knowledge and self-care behaviors. We aimed to identify factors associated with HF knowledge and self-care behaviors in patients hospitalized due to acute decompensated heart failure (ADHF) in Poland.
Patients and Methods: This was a secondary analysis of data from a multi-center, prospective, non-randomized educational program named “The Weak Heart”, which was conducted in 14 cardiology centers in Poland. The level of HF knowledge was assessed using a questionnaire developed by the research team, and self-care behaviors were evaluated using the European Heart Failure Self-care Behaviour Scale (9-EHFScBS) questionnaire.
Results: The study included 259 patients admitted to the hospital with ADHF. The mean HF knowledge and 9-EHFScBS questionnaire scores were 8.25± 4.34 and 25.2± 9.5, respectively. The patients’ level of education (P = 0.002), number of prior HF hospitalizations (P = 0.008), and previous disease education (P < 0.001) were independently associated with better HF knowledge. Age (P = 0.03) and disease education (P = 0.02) were independently associated with self-care behaviors.
Conclusion: The adherence to self-care recommendations among patients with ADHF is insufficient. Disease education positively influenced both HF knowledge and self-care abilities. To improve patients’ adherence to HF recommendations, well-designed models of education based on HF management guidelines should be implemented.
Keywords: adherence, heart failure, health education, self-care behaviors
Introduction
Heart failure (HF) is a progressive clinical syndrome characterized by increased mortality, frequent hospitalizations, and a complex therapeutic regimen.1,2 It has one of the worst prognoses among all chronic diseases and places a reasonable burden on patients, caregivers, and the healthcare system.3,4 Recent studies demonstrated that 25% of hospitalized patients with HF are readmitted within 30 days of discharge and 50% are readmitted within 6 months.5 According to the analysis of data from the HF Pilot Survey (ESC-HF Pilot), which included Polish patients with HF, 57% of patients were previously hospitalized due to ADHF.6 Patients discharged after hospitalization for HF also remained at high risk of death and hospital readmission.7 Although the “transition phase” is the most vulnerable period after hospital discharge, 75% of readmissions in this time may be preventable.8,9 There is evidence that discharge education improves outcomes in patients with HF,10 which is why “The Weak Heart” program was developed for patients hospitalized for ADHF.
Medical education, self-care management, and other related long-term activities are important non-pharmacological treatments for chronic diseases, including HF.11,12 These activities can reduce morbidity and mortality, as well as improve patients’ quality of life.11,12 Indeed, the 2016 European Society of Cardiology guidelines and practical recommendations for HF (ESC-HF) specify several non-pharmacological methods that are relevant for patients with HF, emphasizing the importance of multispecialty teams, monitoring, physical activity, self-care, and education.2 Despite this, many studies suggest that the level of disease knowledge and self-care abilities are insufficient among patients with HF.13–20
A low level of adherence to non-pharmacological recommendations increases the occurrence of adverse outcomes and may impact HF prognosis.11,21 Hospital readmissions are also known to contribute to poor prognosis.22 Moreover, a lack of disease knowledge and incorrect recognition of symptoms among patients with HF can result in poor patients’ compliance as the disease progresses.23 Therefore, increasing disease knowledge and self-management skills among patients with HF should improve patient outcomes.24,25
Data concerning disease education among patients with HF in Poland is scarce. To the best of our knowledge, this is the first comprehensive study revealing the level of HF knowledge and self-care behaviors among Polish patients with ADHF. The purpose of this study was to identify factors associated with HF knowledge and self-care behaviors in patients hospitalized due to ADHF in Poland and to examine the current level of HF knowledge and self-care behaviors within this cohort.
Materials and Methods
Design, Settings, and Participants
“The Weak Heart” was a nurse-led educational model for patients hospitalized due to ADHF. It was conducted between February 2019 and October 2019 in 14 cardiology centers in Poland. This study was a prospective, multi-center, non-randomized, quasi-experimental program to evaluate the impact of the abovementioned model on enhancing the level of patients’ knowledge of HF and their adherence to self-care recommendations in the three-month follow-up period. Trained and certified HF nurses educated patients based on online content (www.slabeserce.pl). The program consisted of two one-hour long educational sessions conducted at the hospital. Following patient discharge, the HF nurses performed three 30-minute monitoring telephone calls according to the established schedule (ie, at the end of the first week, the first and the third month). The knowledge and health-promoting behaviors among patients were evaluated before starting any educational activities (visit 1), immediately after completing in-hospital education (visit 2 – only HF knowledge), and three months later (visit 5 – the end of the program). A detailed description of the “The Weak Heart” program has been published elsewhere.26
Consecutive patients admitted to the cardiology centers with ADHF as the principal reason for hospitalization were screened for eligibility for the program. Patients who met the following inclusion criteria were recruited to the program: ejection fraction below 40% (EF < 40% documented by echocardiography), cognitive function enabling participation in the program (as subjectively assessed by a recruited physician) and declaration of a patient’s active involvement in the treatment following the signing of the Informed Consent Form.
Data Collection: Sociodemographic and Clinical Questionnaires
A checklist was developed by the research team to measure the following sociodemographic and clinical variables: age, gender, education, place of residence, professional activity, marital status, comorbidities, prior HF hospitalizations, time to HF diagnosis, and prior disease education (Supplementary material, Figure S1). The initial level of HF knowledge was assessed by the HF knowledge questionnaire, which was created by the research team and based on the 2016 ESC-HF guidelines.2 The survey includes 10 questions about patients’ perceptions of the disease. The questionnaire assessed knowledge of the definition and symptoms of HF, as well as recommendations related to nutrition, physical activity, pharmacotherapy, and outpatient care. Questions to the patient were posed verbally and the HF nurse scored the patient’s response on a scale of 0 to 2 based on predetermined key words (0 – incorrect response, 1 – partially correct response, 2 – correct response). The maximal score was 20 points. A higher score corresponded to better disease knowledge. Since a non-standardized test of knowledge was used, we performed reliability analysis of the test based on the calculation of Cronbach’s alpha coefficients for each of the three measurements, stratified according to disease duration, number of hospitalizations, and prior education on HF. The discriminant power of each test item was analyzed using the Corrected Item-Total Correlation Coefficient. The research team decided to use self-created HF knowledge questionnaire based on the 2016 ESC-HF guidelines2 because in Poland there are no validated tools for the HF knowledge assessment.
Self-care behaviors were measured using the European Heart Failure Self-care Behaviour Scale questionnaire (9-EHFScBS), which contains nine statements, and has been adapted for the Polish population.27,28 Five of these statements are related to aspects of self-care, including body mass control, limitation of fluid intake, use of low-salt diet, use of medications as prescribed, and physical activity. The remaining four statements assess the level of symptom reporting (shortness of breath, excessive fatigue, lower extremity swelling, and body mass increase in one week), which are indicative of disease progression. The questionnaire also enables the assessment of the level of self-care in terms of the individual statements. The scores varied from 9 to 45, with a lower score corresponding to better self-care.27,29,30
Ethics Approval and Funding
The study was performed in line with the ethical principles for clinical research based on the Declaration of Helsinki. The Bioethics committee at the Medical University of Warsaw approved the project (approval number: KB/3/A/2019). The study was funded by Novartis Pharma Poland.
Statistical Analysis
All continuous variables were presented as the mean values and standard deviations (SD). For categorical variables, absolute and relative frequencies were presented. The predictive value of the analyzed variables on HF knowledge status and self-care behaviors were calculated using multivariable linear regression analysis. To analyze differences between groups for the dependent variables (ie, results in the knowledge and self-care tests), a mixed analysis of variance (ANOVA) was performed in the 3x2x2x2 plan, including an intra-group factor of time measurement (ie, before the start of the educational program vs immediately after the educational program vs three months after the program) and three inter-group factors: number of hospitalizations (one vs more than one), duration of the disease (<1 year vs >1 year), and prior education (attendance vs no education). A value of P < 0.05 was considered significant for all tests. All statistical analyses were performed using the SAS® software, version 9.4.
A sample size of 199 patients is required to achieve a statistical significance of P < 0.05. This was calculated on the assumption that a patient has a baseline score of 10 points, and their knowledge improves by 10% (1 point) after 3 months, with a standard deviation of 5 points and a statistical power of 80%. Due to the innovative nature of this study, and a lack of prior published results, this sample size calculation assumes a large diversity of results among the patients. Moreover, the loss of contact with some patients over the 3-month follow-up should be accounted for. If the loss to follow-up is estimated at 20%, the number of patients enrolled in the study should be 250.26
Results
Patient Characteristics
In total, 259 patients with ADHF were included in the program. In terms of their sociodemographic characteristics, 75% (193/259) were younger than 70 years old, and 76% (198/259) of participants were male. Overall, 10% (27/259) had undergone higher education, 67% (173/259) lived in cities, 23% (60/259) were professionally active, and 83% (216/259) lived with a family.
All participants had an ejection fraction below 40%. A total of 68% of patients were diagnosed with HF more than one year prior, while 14% (36/259) were first diagnosed with HF during the current hospitalization (de novo). Regarding the history of previous HF decompensations, 74% (193/259) of patients had been hospitalized at least once in the last year, and 76% had at least one comorbidity (ie, chronic obstructive pulmonary disease, diabetes, atrial fibrillation or stroke). All participants were asked about prior disease education delivered by a healthcare professional (HCP). Only 25% (65/259) had been previously educated: 20% by a cardiologist, 3% by a nurse, and 3% by a primary care physician. The characteristics of the studied sample are presented in Table 1.
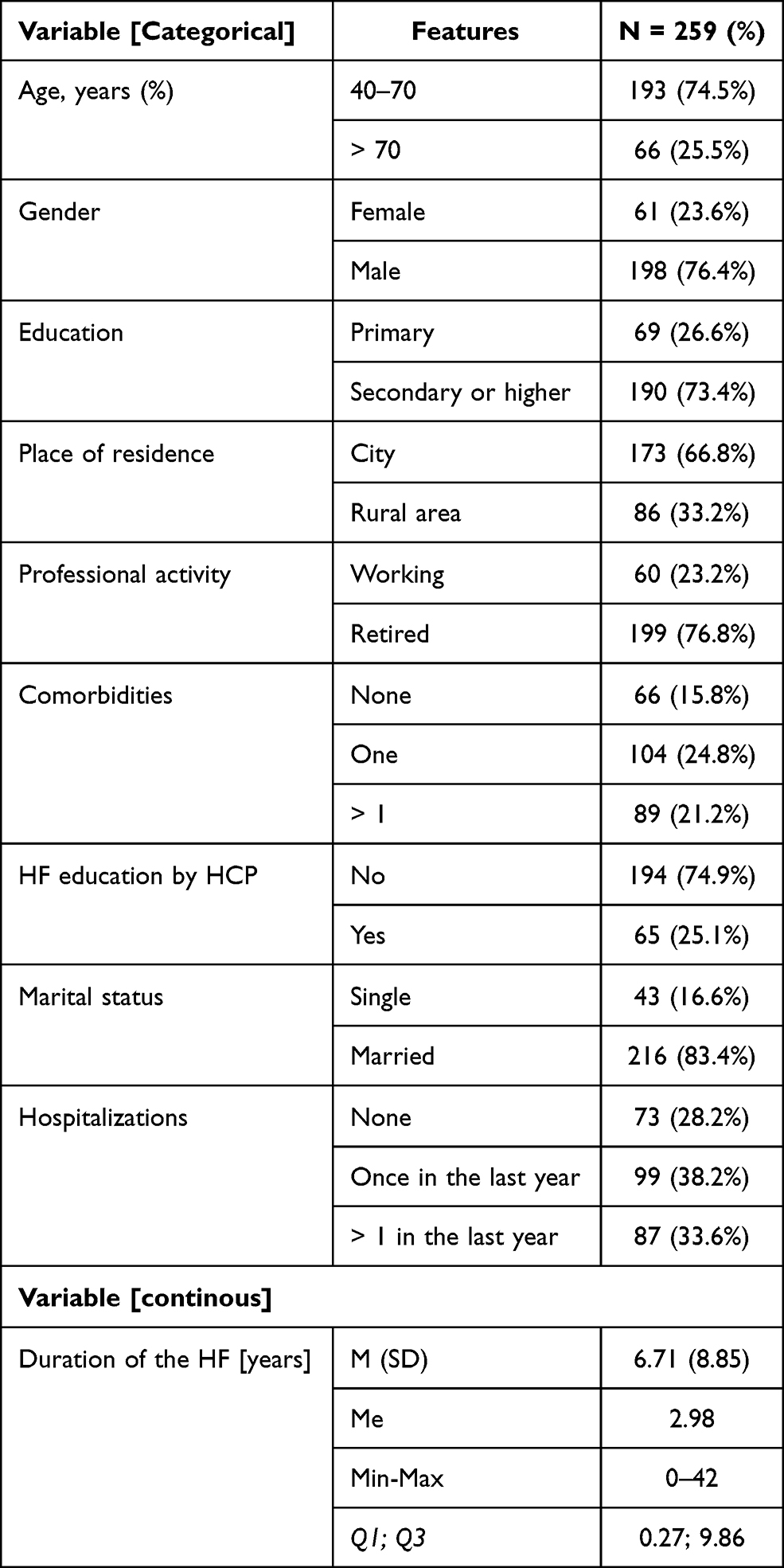 |
Table 1 Sociodemographic Characteristic of the Study Group |
HF Knowledge and Self-Care Behavior Outcomes
The alpha Cronbach for the HF knowledge test was 0.859. Satisfactory reliability of the HF knowledge test was also found for all three measurements, both independently and when patients were divided into groups, in terms of (1) disease duration, (2) number of hospitalizations, and (3) prior education of patients (Table 2). The discriminant power of individual test items, as estimated by Corrected Item-Total Correlation, is in the range of 0.33–0.66 in each of the three measurements. The value of the correlation coefficient of individual test items was not less than the minimum acceptable value 0.20. The alpha Cronbach for the 9-EHFScBS questionnaire was 0.888.
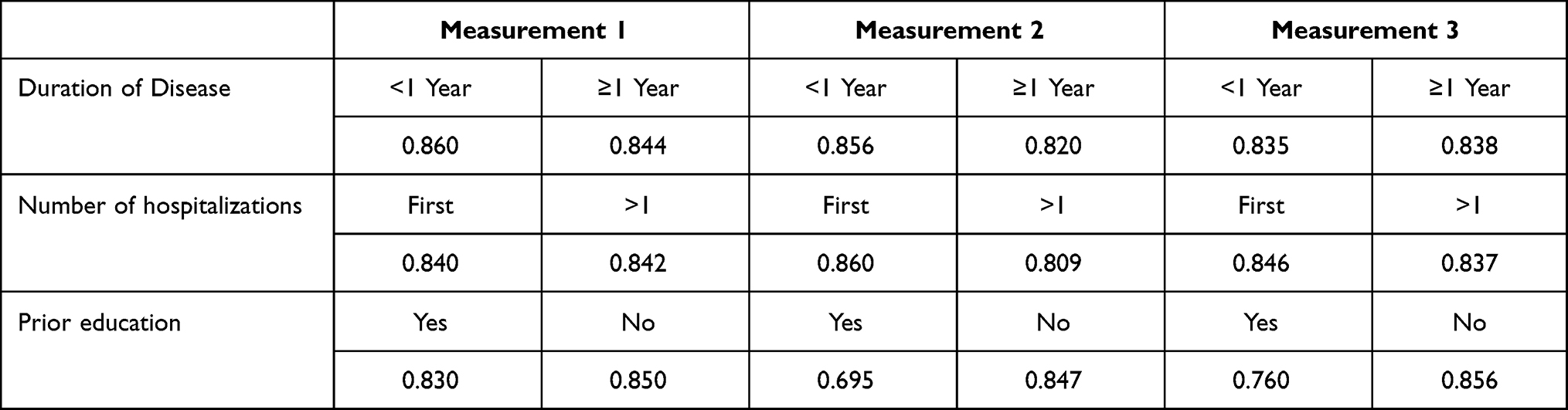 |
Table 2 Cronbach’s Alpha Reliability Coefficients for the Knowledge Test in Each of the Three Measurements, Stratified According to Disease Duration, Number of Hospitalizations, and Prior Education on HF |
The mean (SD) score obtained from the HF knowledge questionnaire was 8.25±4.34 out of a possible 20 points (the higher the score, the better). Regarding self-care behaviors, the mean (SD) score of the 9-EHFScBS questionnaire was 25.2±9.5 out of a possible 45 points (the lower the score, the better). The baseline level of HF knowledge (assessed by the HF knowledge questionnaire) and self-care (assessed by the 9-EHFScBS questionnaire) with respect to the various factors such as age, gender, education, place of residence, professional activity, marital status, comorbidities, prior HF hospitalizations, time to HF diagnosis, and prior disease education is presented in Table 3.
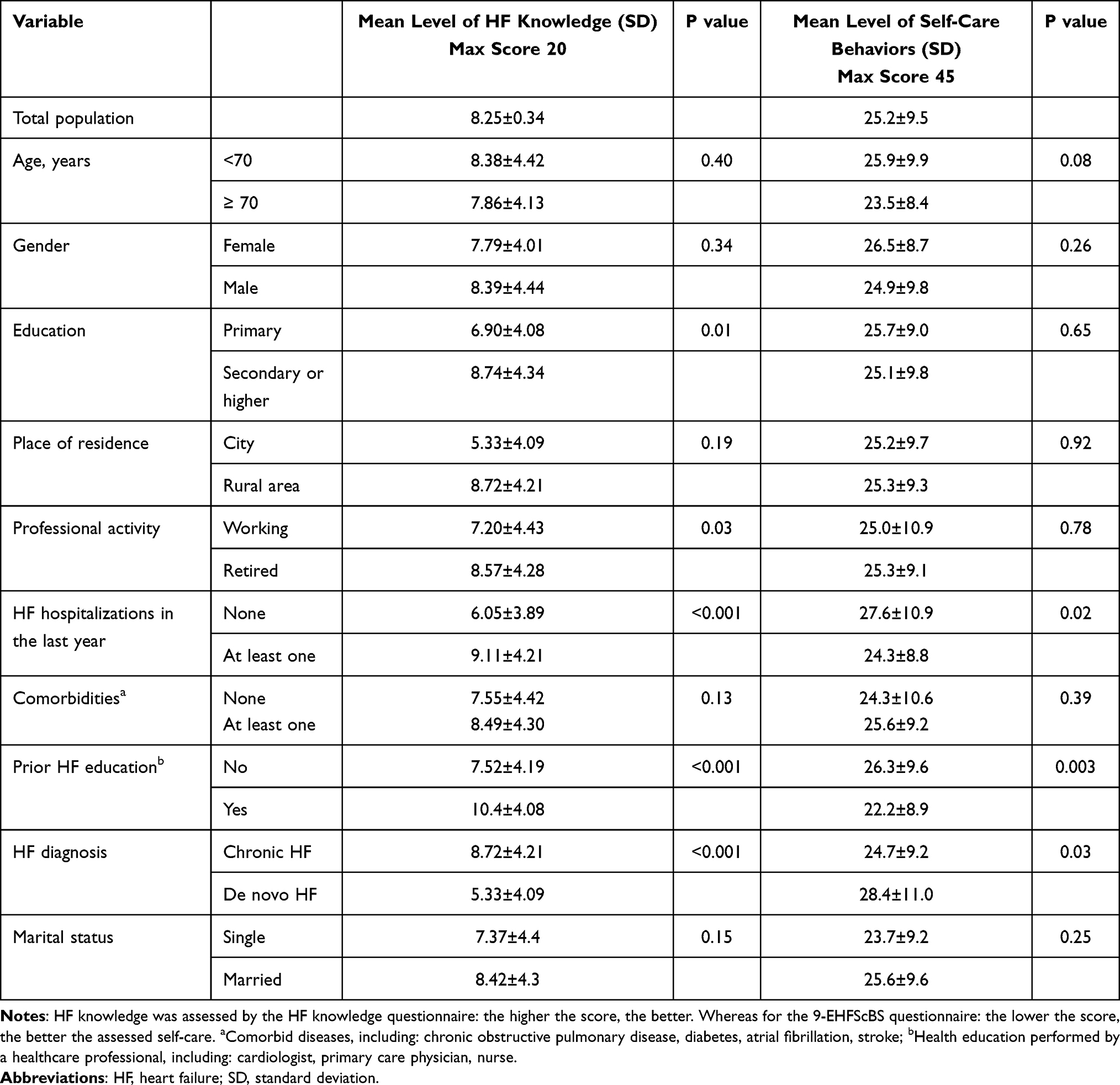 |
Table 3 Relationships Between Sociodemographic and Clinical Parameters and the Level of Heart Failure Knowledge and Self-Care Among Patients with Acute Decomposed Heart Failure at Baseline (Ie, Before Any Educational Activities Were Performed) |
The multivariable regression analysis showed that the independent factors associated with a higher level of HF knowledge were education, prior HF hospitalizations, and previous disease education.
The independent factors associated with improved self-care behaviors were age and prior disease education (Table 4).
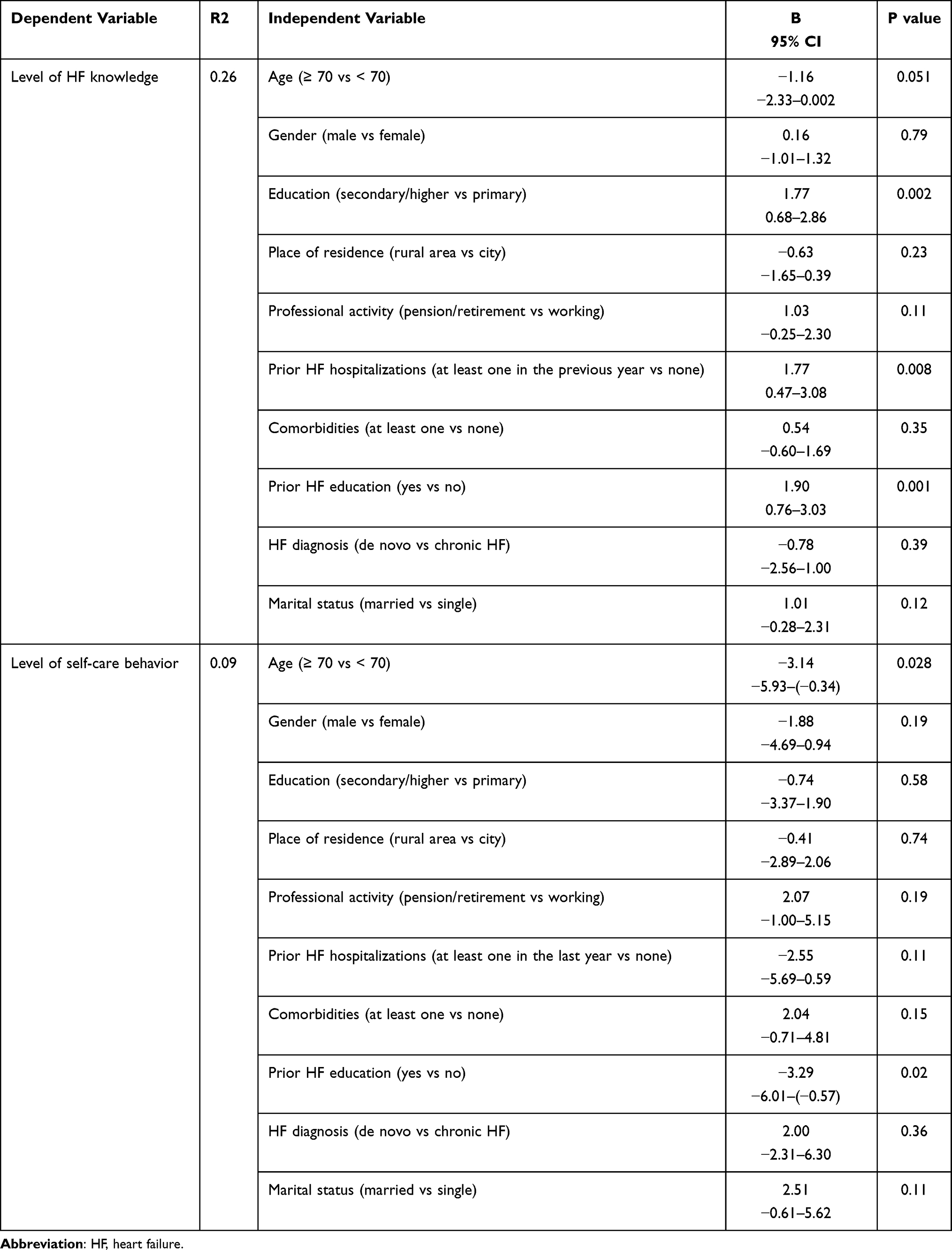 |
Table 4 Multivariable Regression Analysis of the Influence of Various Independent Factors on the Level of Heart Failure Knowledge and the Level of Self-Care Behavior (The Baseline Scores Were Used) |
Level of Knowledge About HF and Self-Care Behavior in Patients Before Participating in the Program and After Completing the Program
The four-factor mixed ANOVA showed a significant main effect of the measurement time on the level of knowledge about HF (F [2, 450] = 195.101; P < 0.001, ηp2 = 4.64). The highest level of HF knowledge was obtained by respondents three months after the end of the educational program (visit 5; M = 17.63, SD = 0.36). This result was significantly higher than those obtained before the start of the program (visit 1; M = 8.05, SD = 0.492) and after finishing in-hospital education (visit 2; M = 15.79, SD = 0.366). Additionally, the number of previous hospitalizations had a significant effect on the level of knowledge about HF (F [1, 225] = 4.88; P = 0.028, ηp2 = 0.021). People who were hospitalized for the first time obtained lower results in the knowledge tests (M = 13.09, SD = 0.37) than those who were hospitalized previously (M = 14.57, SD = 0.52; P = 0.022).
Measurement time also had a significant effect on the knowledge of self-care behavior (F [1, 226] = 12.66; P < 0.001, ηp2 = 0.053). More self-care behaviors were displayed by the respondents after the end of the educational program (visit 5; M = 36.20, SD = 1.27) than before the start of the program (visit 1; M = 29.42, SD = 1.14). The level of education on HF prior to participation in the program also had a significant effect on self-care behaviors (F [1, 226] = 8.04; P = 0.005, ηp2 = 0.034). People who took part in educational activities before participating in the program showed more self-care behaviors (M = 35.86, SD = 1.35) than those who had not previously participated in any training (M = 31.28, SD = 1.19; P = 0.012). The duration of HF and the number of hospitalizations had no significant effect on self-care behavior (Table 5). In patients who had not been previously hospitalized, those who did not undergo education on HF before the program showed less self-care behaviors (M = 25.38, SD = 1.23) than those who were previously educated (M = 36.67, SD = 3.10; P < 0.001). Meanwhile, in patients who were re-hospitalized, those who were educated before participating in the program did not differ in terms of self-care behavior (M = 31.14, SD = 1.33) from those who had not previously had any educational activities on HF (M = 28.96, SD = 2.72; Figure 1).
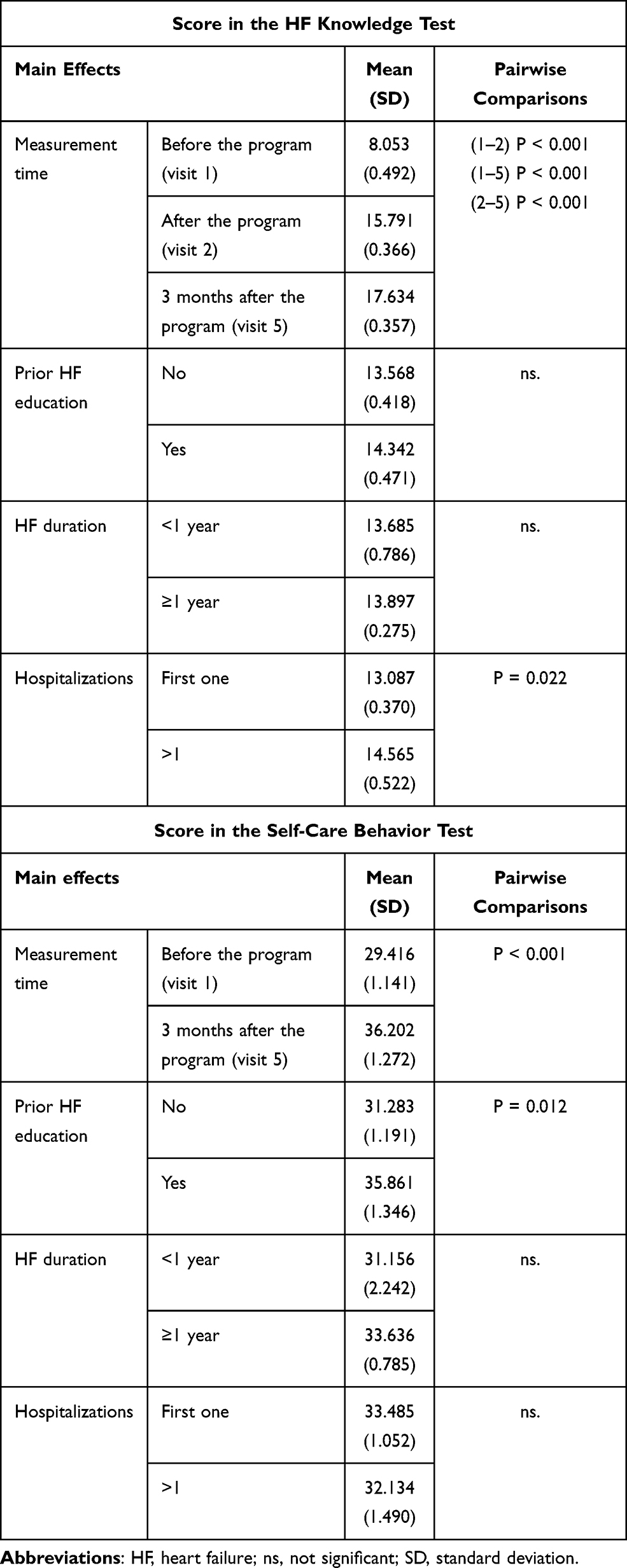 |
Table 5 Summary of Scores on the Heart Failure (HF) Knowledge and Self-Care Tests |
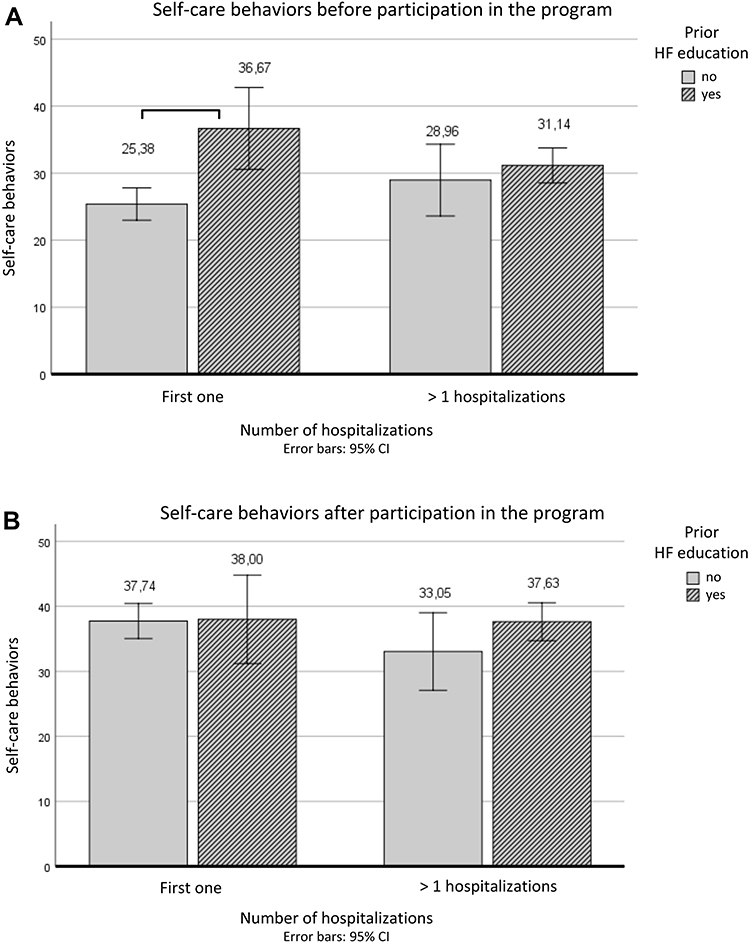 |
Figure 1 Self-care behaviors (A) before participation and (B) after participation in the program in patients stratified according to the number of hospitalizations and participation in any educational activities on heart failure (HF). |
All data are available upon request.
Discussion
“The Weak Heart” program revealed an insufficient level of disease knowledge among program participants. Similarly, the single-center survey-based registry performed by Plotka and colleagues showed that 61% of patients perceive HF as a curable disease, and although patients generally know the most alarming symptoms, most do not attribute them to HF.31 Self-care in HF is fundamental but remains a challenge for multidisciplinary teams.25 In our research, self-care abilities assessed by the 9-EHFScBS questionnaire were also insufficient. Likewise, the mean score on the 9-EHFScBS scale reported by Uchmanowicz et al was 27.65±7.13,28 which is in line with other studies.29,32–37 Moreover, Ni et al found that the HF knowledge and self-care behaviors was also low in their survey of 113 patients visiting the HF clinic: the mean score on the HF knowledge questionnaire was 11.6±2.4 (with a maximum score of 17) and the mean score on the self-care scale was 16.6±3.2 (with a maximum score of 30).38
Although some socio-demographic and clinical characteristics have previously been described in the literature to influence the level of self-care in HF patients, the data are inconclusive.39 In particular, the experience, motivation, habits, cultural beliefs and values, functional and cognitive abilities, confidence, support, and access to care among HF patients are potential barriers encountered in daily clinical practice.30 Riegel et al identified seven main reasons why self-care remains a challenge.40 The authors pointed out two categories: (a) behavior change factors, which address habits, lack of motivation, decision making, and the challenges of persistence; and (b) illness-related factors, such as multi-morbidity, symptoms, and stress.40 The implementation of specific educational solutions can be an effective action in overcoming the above-mentioned challenges for self-care.40 Multivariable regression analysis in our study showed that factors such as the level of education, previous HF hospitalizations, and disease education influence the level of disease knowledge, while age and disease education influenced compliance with self-care behaviors. These findings reflect those of Ni et al, although they found that in addition to previous HF hospitalizations and disease education, female sex had an impact on HF knowledge, and marital status (but not age) influenced self-care behaviors.38 Meanwhile, others have shown that older age is associated with a lower level of disease knowledge.41 Indeed, older patients may face difficulties acquiring new skills connected to self-care due to declining cognitive abilities, which leads to worse HF prognosis and increased comorbidities.42 However, its impact on disease education is not clear. In the present study, age was independently associated with self-care behaviors (P = 0.03) but not with HF knowledge (P = 0.051). Uchmanowicz et al revealed that patients with HF might have worse self-care because of their cognitive deficits. Age was the strongest predictor of worse MMSE scores.43 Lainsack et al also stressed that adequate self-care behavior related to HF reflects the actions that a patient undertakes to maintain health and well-being.13 Elderly patients are often less actively involved in their own care and treatment which may cause inadequate implementation of self-care behaviors in the period after discharge from the hospital, especially if they live alone. Therefore, education of self-care strategies involving behaviors such as taking medication, monitoring symptoms, and recognizing exacerbation of symptoms should be individualized and adjusted to the capabilities of elderly HF patients much more than simple education which only aims to enhance HF knowledge.
Previous studies have also shown that patients with a higher education learn more and better engage in self-care.44,45 Although our data confirmed that secondary or higher education had a positive influence on the level of HF knowledge, it had no impact on self-care behavior. These differences can be partially explained by the fact that only 25% of the patients who participated in our program had undergone prior education by HCPs. Indeed, these patients who were previously educated had the highest scores in both the HF knowledge and 9-EHFScBS questionnaires. Riegel et al reported that previous hospitalizations and some experience with the disease resulted in better self-care among HF patients.36 These results suggest that patients learn not only through interventional activities, but also through their own experience. It should be emphasized that most patients in the three-month follow-up obtained significantly better results in the knowledge test than at the beginning of the program.36 One of the factors that contributed to the improvement in knowledge about HF was the number of previous hospitalizations.36 Correspondingly, we found patients with chronic HF who were diagnosed for at least one year, and those with frequent hospitalizations had higher HF knowledge than those diagnosed de novo without previous hospitalizations. However, these factors did not affect the level of self-care behaviors.
We found that previous HF education by HCPs was the only factor that positively affected both the level of HF knowledge and self-care behaviors, and the same conclusions were derived in the Ni study.38 Similarly, González et al proved that the application of the one-year nursing intervention among HF patients had a positive impact on self-care behavior, irrespective of the educational level.46 Chen et al also emphasizes the importance of predischarge educational interventions, as HF patients who received a profiled educational program showed better self-care behaviors and fewer re-hospitalizations during the year.20 Furthermore, our finding that health education is important for shaping behavior is aligned with other studies.47,48 Therefore, patient-centered education is important for improving compliance with self-care recommendations and HF prognosis.49
Meanwhile, Agvall et al found individuals who participated in educational HF management programs in Sweden showed improvements in self-care behaviors.44 Similarly, in a randomized controlled trial by Koelling et al, discharge education was found to improve HF knowledge and self-care behaviors, and have a positive impact on clinical outcomes.10 Moreover, targeted multimedia educational intervention may prove to be an effective factor in reducing unplanned readmission in people with HF.50 Indeed, active education that includes self-care behavior practice is necessary to change patients’ self-care abilities effectively.15,51 Correspondingly, we found active disease education and close contact with a devoted HF team were important for enhancing self-care behaviors among patients with ADHF.
Therefore, although disease education alone can influence self-care behaviors, other factors should be considered when planning interventions for developing self-care abilities in patients with HF.39 The present study provided insight into the importance of education of HF patients, taking into account clinical outcomes and benefits.
Multidisciplinary team-based interventions significantly improve HF knowledge and self-care as found in a recent systematic review of randomized controlled trails RCTs. The findings of this study indicated that pharmacist-involved multidisciplinary HF management resulted in a significant improvement in HF knowledge, but not in self-care.52 “The Weak Heart” program included only nurse-led educational interventions, because multidisciplinary care for patients with HF is currently not a standard approach in Poland. Currently, qualified nurses are frequently responsible for educational activities, but other multidisciplinary team members could also be involved after obtaining adequate training.
Limitations
Some important limitations of the analysis must be acknowledged. “The Weak Heart” was a quasi-experimental educational program. We only enrolled patients hospitalized due to ADHF who may have a higher level of HF knowledge and motivation to improve self-care behavior. Moreover, we have decided to include only patients with reduced ejection fraction to get a more uniform population, meaning the results cannot be generalized to the whole HF population. We also used an unstandardized HF knowledge questionnaire to assess patients’ knowledge, which makes it difficult to compare the results to those presented in other studies. Additionally, our study lacked a control group. On the other hand, the lack of a multidisciplinary intervention in the “The Weak Heart” program can also be considered a limitation, but this was omitted due to practical reasons since multidisciplinary care for patients with HF is not standard in Poland. Finally, we utilized inclusion criteria that eliminated patients with cognitive impairments and non-compliant behaviors.
Conclusion
Our research revealed that the level of both disease knowledge and self-care abilities among patients with ADHF in Poland is currently insufficient. The multivariable regression analysis showed that secondary and higher education as well as the number of prior HF hospitalizations served as independent factors associated with a higher level of HF knowledge but not with self-care behaviors, while patients’ age below 70 was associated with improved self-care behaviors but not with HF knowledge. Disease education was the only independent factor that positively influenced both HF knowledge and self-care behaviors. Factors such as gender, place of residence, professional activity, marital status, comorbidities and the time to HF diagnosis showed no significant correlation either with the level of HF knowledge or self-care behaviors. Therefore, to improve patients’ adherence to HF recommendations, standardized models of education based on HF management guidelines should be implemented.
Acknowledgments
The study was supported by Novartis Pharma Poland. The preparation for the submission of this paper was provided by Proper Medical Writing Sp. z o.o. and funded by Novartis.
Disclosure
JK: employee of Novartis; ML, MG, ML, JN, AP, and IU: honoraria and consulting fees from Novartis; ML, AP, and JN: involved in clinical trials sponsored by Novartis. EAJ: honoraria and consulting fees from Novartis and Vifor Pharma. The authors report no other conflicts of interest in this work.
References
1. Van Riet EES, Hoes AW, Wagenaar KP, et al. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur J Heart Fail. 2016;18(3):242–252. doi:10.1002/ejhf.483
2. Ponikowski P, Voors A, Anker S, et al. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
3. OECD. Health at a Glance 2015. OECD Indicators; 2015.
4. Gierczynski J, Gryglewicz J, Karczewicz E, Zalewska H Niewydolność serca – analiza kosztów ekonomicznych i społecznych [Heart failure – analysis of economic and social costs]. Uczelnia Łazarskiego, Warszawa 2013. Available from: http://www.niewydolnosc-serca.pl/ns_raport2013.pdf.
5. Greene SJ, Fonarow GC, Vaduganathan M, et al. The vulnerable phase after hospitalization for heart failure. Nat Rev Cardiol. 2015;12(4):220–229. doi:10.1038/nrcardio.2015.14
6. Sosnowska-Pasiarska B, Bartkowiak R, Wozakowska-Kaplon B, et al. Population of Polish patients participating in the Heart Failure Pilot Survey (ESC-HF Pilot). Kardiol Pol. 2013;71(3):234–240. doi:10.5603/KP.2013.0034
7. Balsam P, Tymińska B, Opolski G, et al. Predictors of one-year outcome in patients hospitalised for heart failure: results from the polish part of the heart failure pilot survey of the European Society of Cardiology. Kardiol Pol. 2016;74(1):9–17. doi:10.5603/KP.a2015.0112
8. Krumholz HM, Amatruda J, Smith GL, et al. Randomized trial of an education and support intervention to prevent readmission of patients withheart failure. J Am Coll Cardiol. 2002;39(1):83–89. doi:10.1016/S0735-1097(01)01699-0
9. Rich MW, Beckham V, Wittenberg C, et al. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N Engl J Med. 1995;333:1190–1195.
10. Koelling TM, Johnson ML, Cody RJ, Aronson KD. Discharge education improves clinical outcomes in patients with chronic heart failure. Circulation. 2005;111(2):179–185. doi:10.1161/01.CIR.0000151811.53450.B8
11. Lilijeroos M, Kato NP, van der Wal MH, et al. Trajectory of self-care behaviour in patients with heart failure: the impact on clinical outcomes and influencing factors. Eur J Cardiovasc Nurs. 2020;19(5):421–432. doi:10.1177/1474515120902317
12. Riegel B, Moser DK, Anker SD, et al. State of the science: promoting self-care in persons with heart failure: a scientific statement from the American Heart Association. Circulation. 2009;120(12):1141–1163. doi:10.1161/CIRCULATIONAHA.109.192628
13. Lainscak M, Blue L, Clark AL, et al. Self-care management of heart failure: practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2011;13(2):115–126. doi:10.1093/eurjhf/hfq219
14. Vidan MT, Martin Sanchez FJ, Sanchez E, et al. Most elderly patients hospitalized for heart failure lack the abilities needed to perform the tasks required for self-care: impact on outcomes. Eur J Heart Fail. 2019;21(11):1434–1442. doi:10.1002/ejhf.1559
15. Hwang B, Pelter MM, Moser DK, Dracup K. Effects of an educational intervention on heart failure knowledge, self-care behaviors, and health-related quality of life of patients with heart failure: exploring the role of depression. Patient Educ Couns. 2020;103(6):1201–1208. doi:10.1016/j.pec.2020.01.007
16. Reid KRY, Reid K, Esquivel JH, et al. Using video education to improve outcomes in heart failure. Heart Lung. 2019;48(5):386–394. doi:10.1016/j.hrtlng.2019.05.004
17. Zeng W, Chia SY, Chan YH, et al. Factors impacting heart failure patients’ knowledge of heart disease and self-care management. Proc Singapore Healthc. 2017;26(1):26–34. doi:10.1177/2010105816664537
18. Sahebi A, Mohammad-Aliha J, Ansari-Ramandi M, Naderi N. Investigation the relationship between self-care and readmission in patients with chronic heart failure. Res Cardiovasc Med. 2015;4(1):e25472. doi:10.5812/cardiovascmed.25472
19. Seraji M, Rakhshani M. The effect of education on performance and awareness rate of hospitalized heart failure patients regarding their self-care behaviors and methods. J Res Health. 2018;8(1):61–67. doi:10.29252/acadpub.jrh.8.1.61
20. Chen HM, Wang ST, Wu SJ, et al. Effects of predischarge patient education combined with postdischarge follow-ups on self-care, readmission, sleep, and depression in patients with heart failure. J Nurs Res. 2020;28(5):e112. doi:10.1097/JNR.0000000000000395
21. van der Wal MHL, van Veldhuisen DJ, Veeger NJ, et al. Compliance with non-pharmacological recommendations and outcome in heart failure patients. Eur Heart J. 2010;31(12):1486–1493. doi:10.1093/eurheartj/ehq091
22. Carlson B, Hoyt H, Gillespie K, et al. Predictors of heart failure readmission in a high-risk primarily hispanic population in a rural setting. J Cardiovasc Nurs. 2019;34(3):267–274. doi:10.1097/JCN.0000000000000567
23. Askren-Gonzalez A, Frater J. Case management programs for hospital readmission prevention. Prof Case Manag. 2012;17(5):219–226. doi:10.1097/NCM.0b013e318257347d
24. Albert NM. Fluid management strategies in heart failure. Crit Care Nurse. 2012;32(2):20–32. doi:10.4037/ccn2012877
25. Lee CS, Bidwell JT, Paturzo M, et al. Patterns of self-care and clinical events in a cohort of adults with heart failure: 1 year follow-up. Heart Lung. 2018;47(1):40–46. doi:10.1016/j.hrtlng.2017.09.004
26. Kolasa J, Uchmanowicz I, Wleklik M, et al. “The Weak Heart” as an educational model for patients hospitalised due to decompensation of heart failure with reduced ejection fraction. Folia Cardiol. 2020. Mar 28 [Epub ahead of print].
27. Jaarsma T, Arestedt KF, Martensson J, et al. The European heart failure self-care behaviour scale revised into a nine-item scale (EHFScB-9): a reliable and valid international instrument. Eur J Heart Fail. 2009;11(1):99–105. doi:10.1093/eurjhf/hfn007
28. Uchmanowicz I, Wleklik M. Polish adaptation and reliability testing of the nine-item European Heart Failure Self-care Behaviour Scale (9-EHFScBS). Kardiol Pol. 2016;74(7):691–696. doi:10.5603/KP.a2015.0239
29. Dickson VV, Melkus GD, Katz S, et al. Building skill in heart failure self-care among community dwelling older adults: results of a pilot study. Patient Educ Couns. 2014;96(2):188–196. doi:10.1016/j.pec.2014.04.018
30. Jaarsma T, Cameron J, Riegel B, Stromberg A. Factors related to self-care in heart failure patients according to the middle-range theory of self-care of chronic illness: a literature update. Curr Heart Fail Rep. 2017;14(2):71–77. doi:10.1007/s11897-017-0324-1
31. Plotka A, Prokop E, Migaj J, et al. Patients’ knowledge of heart failure and their perception of the disease. Patient Prefer Adherence. 2017;11:1459–1467. doi:10.2147/PPA.S126133
32. Cocchieri A, Riegel B, D’Agostino F, et al. Describing self-care in Italian adults with heart failure and identifying determinants of poor selfcare. Eur J Cardiovasc Nurs. 2015;14(2):126–136. doi:10.1177/1474515113518443
33. Dickson VV, Deatrick JA, Riegel B. A typology of heart failure self-care management in nonelders. Eur J Cardiovasc Nurs. 2008;7(3):171–181. doi:10.1016/j.ejcnurse.2007.11.005
34. Riegel B, Carlson B. Is individual peer support a promising intervention for persons with heart failure? J Cardiovasc Nurs. 2004;19(3):174–183. doi:10.1097/00005082-200405000-00006
35. Riegel B, Vaughan DV, Goldberg LR, Deatrick JA. Factors associated with the development of expertise in heart failure self-care. Nurs Res. 2007;56(4):235–243. doi:10.1097/01.NNR.0000280615.75447.f7
36. Riegel B, Driscoll A, Suwanno J, et al. Heart failure self-care in developed and developing countries. J Card Fail. 2009;15(6):508–516. doi:10.1016/j.cardfail.2009.01.009
37. Yehle KS, Sands LP, Rhynders PA, Newton GD. The effect of shared medical visits on knowledge and self-care in patients with heart failure: a pilot study. Heart Lung. 2009;38(1):25–33. doi:10.1016/j.hrtlng.2008.04.004
38. Ni H, Nauman D, Burgess D, et al. Factors influencing knowledge of and adherence to self-care among patients with heart failure. Arch Intern Med. 1999;159(14):1613–1619. doi:10.1001/archinte.159.14.1613
39. Sedlar N, Lainscak M, Martensson J, et al. Factors related to self-care behaviours in heart failure: a systematic review of European heart failure self-care behaviour scale studies. Eur J Cardiovasc Nurs. 2017;16(4):272–282. doi:10.1177/1474515117691644
40. Riegel B, Dunbar SB, Fitzsimons D, et al. Self-care research: where are we now? Where are we going? Int J Nurs Stud. 2019;23:103402. doi:10.1016/j.ijnurstu.2019.103402
41. Lee CS, Vellone E, Lyons KS, et al. Patterns and predictors of patient and caregiver engagement in heart failure care: a multi-level dyadic study. Int J Nurs Stud. 2015;52(2):588–597. doi:10.1016/j.ijnurstu.2014.11.005
42. Cichocka-Radwan A, Lelonek M. Annual prognostic factors in chronic heart failure in patients over 80 years old. Kardiol Pol. 2017;75(2):164–173. doi:10.5603/KP.a2016.0132
43. Uchmanowicz I, Jankowska-Polańska B. Cognitive deficits and self-care behaviors in elderly adults with heart failure. Clin Interv Aging. 2017;12:1565–1572. doi:10.2147/CIA.S140309
44. Agvall B, Alehagen U, Dahlström U. The benefits of using a heart failure management programme in Swedish primary healthcare. Eur J Heart Fail. 2013;15(2):228–236. doi:10.1093/eurjhf/hfs159
45. Rockwell JM, Riegel B. Predictors of self-care in persons with heart failure. Heart Lung. 2001;30(1):18–25. doi:10.1067/mhl.2001.112503
46. González B, Lupón J, Domingo M, et al. Educational level and self-care behaviour in patients with heart failure before and after nurse educational intervention. Eur J Cardiovasc Nurs. 2014;13(5):459–465. doi:10.1177/1474515113510810
47. Redman BK. Accountability for patient self-management of chronic conditions; ethical analysis and a proposal. Chronic Illn. 2007;3(1):88–95. doi:10.1177/1742395307079196
48. Smith B, Forkner E, Krasuski RA, et al. Educational attainment has a limited impact on disease management outcomes in heart failure. Dis Manag. 2006;9(3):157–166. doi:10.1089/dis.2006.9.157
49. Kolasa J, Maciejewski C, Zych A, et al. The role of health education in heart failure patients. Folia Cardiol. 2019;14(3):252–257. doi:10.5603/FC.2019.0058
50. Boyde M, Peters R, New N, et al. Self-care educational intervention to reduce hospitalisations in heart failure: a randomised controlled trial. Eur J Cardiovasc Nurs. 2018;17(2):178–185. doi:10.1177/1474515117727740
51. van der Wal MHL, Jaarsma T, Moser DK, et al. Compliance in heart failure patients: the importance of knowledge and beliefs. Eur Heart J. 2006;27(4):434–440. doi:10.1093/eurheartj/ehi603
52. Parajuli DR, Kourbelis C, Franzon J, et al. Effectiveness of the pharmacist-involved multidisciplinary management of heart failure to improve hospitalizations and mortality rates in 4630 patients: a systematic Review and Meta-Analysis of Randomized Controlled Trials. J Card Fail. 2019;25(9):744–756. doi:10.1016/j.cardfail.2019.07.455
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.