Back to Journals » Clinical Interventions in Aging » Volume 20
Factors Associated with Frailty Transitions Using the Kihon Checklist: A 6-Year Longitudinal Study Among Japanese Residents
Authors Imai N ![]() , Homma D, Horigome Y, Yoda T, Murakami R, Fujii T, Ohashi M, Kawashima H
, Homma D, Horigome Y, Yoda T, Murakami R, Fujii T, Ohashi M, Kawashima H
Received 4 June 2025
Accepted for publication 27 October 2025
Published 30 October 2025 Volume 2025:20 Pages 1821—1834
DOI https://doi.org/10.2147/CIA.S544734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Norio Imai,1 Daisuke Homma,2,3 Yoji Horigome,1 Takuya Yoda,1 Reiko Murakami,1 Toshihide Fujii,4 Masayuki Ohashi,2 Hiroyuki Kawashima2
1Division of Comprehensive Musculoskeletal Medicine, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 2Division of Orthopedic Surgery, Department of Regenerative and Transplant Medicine, Niigata University Graduate School of Medical and Dental Sciences, Niigata, Japan; 3Department of Rehabilitation, Niigata Bandai Hospital, Niigata, Japan; 4Department of Orthopedic Surgery, Agano City Hospital, Agano, Japan
Correspondence: Norio Imai, Division of Comprehensive Musculoskeletal Medicine, Niigata University Graduate School of Medical and Dental Sciences, 1-757 Asahimachi Dori, Chuo-ku, Niigata, 951-8510, Japan, Tel +81252272272, Fax +81252270782, Email [email protected]
Background: The Kihon Checklist (KCL) is widely used in Japan to assess robustness, pre-frailty, and frailty. However, the specific KCL items that predict the maintenance of robustness or transitions between frailty states remain unclear. Identifying these predictors could guide preventive strategies in older adults. This study examined item-level predictors of frailty transitions in a community-dwelling population over 6 years.
Methods: This longitudinal non-interventional study followed residents aged 70 years in 2016 and 76 years in 2022 in Agano City, Japan. Health status was evaluated using the 25-item KCL, and frailty states (robust, pre-frail, frail) were classified by total scores. Changes in responses to each item (yes-to-yes, yes-to-no, no-to-yes, no-to-no) were analyzed. Multivariate logistic regression identified independent predictors of maintaining robustness, transitioning to pre-frailty or frailty, and improving from frailty.
Results: Among the 358 participants that completed both surveys, robustness decreased from 60.9% to 48.6%. Maintaining robustness was independently associated with visiting friends and absence of fear of falling. Transition to pre-frailty was linked with loss of stair-climbing ability, difficulty eating tough foods, and impaired date orientation. Transition to frailty was associated with persistently low body mass index, reduced outings, memory loss recognized by others, and difficulty performing routine tasks. Improvement from frailty was predicted by initiating weekly outings.
Conclusion: Key protective factors included social engagement, absence of fear of falling, oral function, cognitive health, and maintaining body weight. Regular outings prevented frailty and facilitated recovery, highlighting practical community-level intervention targets. Future research should test whether programs targeting these predictors reduce frailty incidence and improve recovery.
Keywords: frailty, Kihon checklist, longitudinal study, important factors
Background
The number of elderly people in Japan is increasing, and estimates show that people aged ≥65 years will account for 30% of the population by 2025 and approximately 38% by 2050,1 whereas the total population of Japan is projected to decrease from 123.8 million in 20242 to approximately 104.7 million in 2050.3 Since an increase in elderly populations will lead to higher medical costs,4 the government is taking measures to extend healthy life expectancy, that is, to maintain a healthy state and prevent a surge in elderly people who need nursing care and support or are bedridden.5
Frailty is a common geriatric syndrome and is more likely to occur in old age, increasing the risk of needing care and support from disability to death.6 Frailty includes physical aspects as well as psychological and social factors.6 Frailty is commonly defined as a biological syndrome of decreased reserve and resistance to stressors, resulting from cumulative declines across multiple physiological systems, and is operationalized by the presence of at least three of the following five components: unintentional weight loss, self-reported exhaustion, weakness (grip strength), slow walking speed, and low physical activity.7 The diagnostic criteria for frailty reported by Fried et al,7 using data from the Cardiovascular Health Study (CHS), include unintentional weight loss (4.54 kg/10 pounds in the past year), self-reported fatigue, weakness (such as grip power), decreased walking speed, and decreased physical activity, some of the most widely used diagnostic criteria for frailty today. The Japanese version of the CHS (J-CHS), a modification of the criteria of Fried et al,7 is widely used in Japan.8
The Kihon Checklist (KCL) is also widely used in Japan as a self-assessment tool to estimate the risk of needing care and support in elderly people living in communities (Figure 1).9,10 Unlike the J-CHS, the KCL includes psychosocial aspects11 and does not include a physical examination, such as walking speed, but rather only a questionnaire. Therefore, the KCL can be applied to a large number of residents (for example, by mail) and in a multidimensional manner12 and is considered a simple survey tool for elderly people living in the community.13 Although the J-CHS criteria are considered an appropriate standard for the diagnosis and research of physical frailty,12 the diagnosis of frailty using the KCL was established based on the J-CHS criteria, and its validity has been ensured even in surveys on community-dwelling populations.12,14 In a systematic review, Sampaio et al13 described the reliability of the KCL in terms of its diagnostic aspect and its effectiveness for intervention in frail persons.
 |
Figure 1 KCL questionnaire items. The KCL consists of 25 items to be answered with a “yes” or “no” response. The 25 items are divided into seven subgroups, including activities of daily life, physical activity, nutritional status, oral function, confinement, cognitive status, and depressive mood. |
The KCL has been reported as a useful and simple tool for predicting long-term care risk,15,16 healthy life expectancy,17 and cognitive function.18 In countries with aging populations, such as Japan, the KCL survey is a valuable tool for assessing and understanding health or frailty status, because it can be administered to a large number of residents at a low cost simultaneously, such as by mail or other self-report methods. Moreover, understanding the process of frailty and predicting its deterioration in the elderly is essential for devising suitable interventions to prevent or delay its progression.
When the KCL is used to assess robustness, pre-frailty, and frailty, it is classified into those three categories based on its score. In other words, although each item of the KCL is divided into domains, such as physical function, nutritional status, oral function, and cognitive function, they are all treated uniformly when assigning scores.15,17 However, few reports describe which items are involved in maintaining robustness or in the transition from robustness to frailty.13,16,19 In a five-year longitudinal survey, Ohashi et al19 reported higher body mass index (BMI) and lower physical activity scores on the KCL as risk factors for the transition from robustness or pre-frailty to frailty.
A number of studies have examined frailty transitions in older populations, particularly focusing on total frailty scores or specific domains, such as mobility and physical function.20,21 We considered that the transition to frailty in a large population may be more efficiently prevented by identifying the characteristics of those most likely to become frail and targeting interventions to those individuals. However, research addressing this perspective remains limited. Therefore, in a previous 6-year longitudinal study,22 we investigated the factors involved in the subsequent maintenance of robustness or the transition from robustness to frailty. Among the 25 KCL items, we reported that regular 15-minute continuous walking, a BMI of at least 18.5 kg/m2, no falls in the past year, going out at least once a week, contact with family and friends, and not feeling helpless were critical factors for maintaining a healthy state or improving from a state of frailty at the initial survey over 6 years.22 However, that study did not find any significant differences between the two groups upon initial survey. Furthermore, that study estimated the 6-year status based on the initial survey results and did not consider changes in responses to each item between the initial and 6-year follow-up surveys.
Therefore, this study aimed to determine the changes in responses to the 25 items of the KCL that contribute to the maintenance of robustness or prevention of frailty. We hypothesized that several predictive factors could be identified for the maintenance of robustness and the prevention of frailty. Moreover, our study period included the coronavirus disease 2019 (COVID-19) pandemic, during which people in Japan were restricted from going out or socializing with others. Therefore, a deterioration of items related to going out and socializing with others was expected.
Methods
Study Design, Setting, and Population
This longitudinal cohort study was designed according to the STROBE checklist for cohort studies, and the completed checklist is provided in Supplementary Table 1. The survey was conducted in Agano City, which has a population of approximately 40,000 (51.5% female), with an aging rate of 34.4%, higher than the average for Niigata Prefecture.23 The Agano City Health Promotion Division previously conducted a municipal project to extend healthy life expectancy and prevent bedriddenness by periodically sending KCLs by mail to elderly persons aged ≥70 years to investigate the prevalence of frailty and explore treatment measures. This study targeted 70-year-old residents. The “elderly” were defined as individuals aged ≥65 years and “late elderly” as those >75 years; and those aged 70 years were categorized as “between elderly and late elderly”. Participants included those who took part in the baseline survey at age 70 in 2016 and completed the follow-up survey at age 76 in 2022. We did not exclude the participants based on the presence or absence of trauma or serious health events. This current study was conducted according to the STROBE reporting guidelines for cohort studies, described along with the corresponding checklist in Supplementary Table 1.
KCL
The KCL is a self-report questionnaire consisting of 25 items to be answered with a “yes” or “no” response. The 25 items are divided into seven subgroups: five items on activities of daily life, five physical activity items, two nutritional status items, three oral function items, three confinement items, three cognitive status items, and five depressive mood items (Figure 1).9 Each question is scored as 0 or 1, indicating positive and negative answers, respectively. The minimum and maximum scores are 0 and 25, respectively. Scores 0–3 are defined as robustness, 4–7 as pre-frailty, and ≥8 as frailty;15 in general, a higher KCL score indicates higher risk of needing assistance or care.15
Statistical Analysis
Results are expressed as medians and interquartile ranges. We further divided the changes in response to each of the 25 KCL items from 2016 to 2022 into four categories: yes-to-yes, yes-to-no, no-to-yes, no-to-no. From 2016 to 2022, we analyzed: 1) changes in the percentages of robustness, pre-frailty, and frailty and 2) how robustness, pre-frailty, and frailty changed.
We used stepwise logistic regression to calculate independently associated factors for participants who were 1) evaluated as robust, whose KCL scores were 1–3 in 2016, and were still evaluated as robust in 2022; 2) evaluated as robust in 2016, transitioned to pre-frailty, and achieved KCL scores of 4–7 in 2022; 3) evaluated as robust in 2016 and transitioned to frailty, with KLC scores ≥ 8 in 2022; and 4) evaluated as frail in 2016, but improved to pre-frailty or robustness in 2022.
We conducted univariate analyses of the 25 KCL items to examine their associations with transitions such as robust-to-robust, robust-to-pre-frail, robust-to-frail, pre-frail-to-frail, and frail-to-robust or pre-frail. Items with p < 0.20 were then included as independent variables in multivariable logistic regression analyses, with each transition pattern treated as a dependent variable. Participants who were pre-frail in 2016 were not excluded from the regression analyses. As a sensitivity analysis, multivariate logistic regression analysis with stepwise method was also conducted for factors not meeting the threshold of p < 0.20 in the univariate analysis. Statistical significance was indicated by p < 0.05. In the residual analysis, if the absolute value of the adjusted residuals was >1.96, it was considered significantly different from the expected frequency at p < 0.05.
DH, PhD, who was not involved in conceptualizing the study, performed the statistical analysis. SPSS software (version 28; IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Ethics Statement
This study was approved by the Niigata University Institutional Review Board (2022-0256, February 2, 2023). All methods in this study were performed in accordance with the relevant guidelines and regulations. The requirement for informed consent was waived, because this was a non-interventional, retrospective study. This study was conducted in accordance with the Declaration of Helsinki. The participants were informed that the survey conducted by Agano City may be used by Niigata University for research purposes.
Results
Participant Selection
In 2016, the population of 70-year-olds in Agano City was 591 (302 females and 289 males), 476 of whom returned survey forms. After excluding those who did not complete the form, 444 survey responses were obtained. In 2022, the KCL was sent again to these 444 individuals, 372 of whom returned the survey forms. After omissions were excluded, 358 [185 females (51.7%) and 173 males] completed the survey in 2016 and 2022, with a follow-up rate of 80.6% (Figure 2). The median KCL significantly increased from 2 (interquartile range, 1–3) in 2016 to 3 (interquartile range, 1–6) in 2022 (p < 0.001). From 2016 to 2022, the chi-square test indicated a significant overall difference among the groups (p = 0.002), the pre-frailty and frailty rates increased from 12.3% to 19.8% (p = 0.406) and 26.8% to 31.6% (p = 0.075), but robustness decreased from 60.9% to 48.6% (p = 0.042) by standardized residuals (Figure 3). Of the participants who were robust at baseline (60.9% of the total), 67.0% (40.8% of the total) remained robust for 6 years (Table 1). In contrast, of those who were robust in 2016, 33.0% did not remain healthy, 23.8% (14.5% of the total) were pre-frail, and 9.2% (5.6% of the total) transitioned to frail (Table 1). Of the 26.8% of participants rated as pre-frail at baseline, 22.9% (6.1% of the total) improved to robust after 6 years, while 26.0% (7.0% of the total) transitioned to frail (Table 1). In addition, 27.3% of those assessed as frail at baseline improved to pre-frailty (3.4% of the total) and 13.6% to robustness (1.7% of the total). The number of participants that provided yes-to-yes, yes-to-no, no-to-yes, no-to-no responses to each question in 2016 and 2022 is described in Table 2.
 |
Table 1 Transitions in Frailty Status Among Community-Dwelling Older Adults Aged 70 Years in 2016 and Followed Up at Age 76 Years in 2022, Agano City, Niigata Prefecture, Japan |
 |
Table 2 Number of Participants That Provided Yes-to-Yes, Yes-to-No, No-to-Yes, and No-to-No Responses to Each Question in 2016 and 2022 for All Participants |
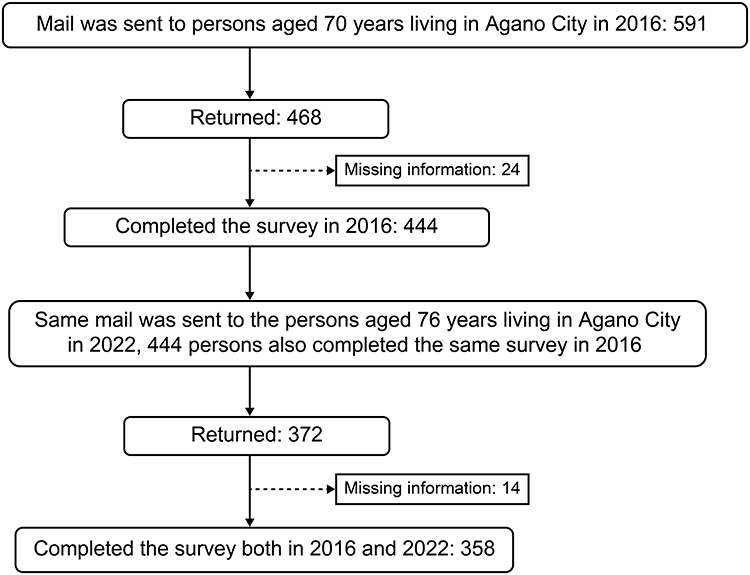 |
Figure 2 Study flow of community-dwelling older adults in Agano City, Niigata Prefecture, Japan, followed from 2016 (age 70 years) to 2022 (age 76 years). Participants were identified from the municipal survey database using the KCL. Exclusion criteria and final analytic sample are shown. This flow diagram demonstrates that 358 participants completed both baseline and follow-up surveys. Abbreviation: KCL, Kihon Checklist. |
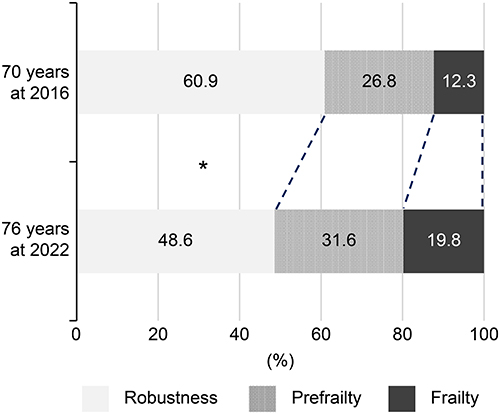 |
Figure 3 Independent predictors of frailty transitions identified via multivariable logistic regression analysis. Forest plots present ORs and 95% CIs for baseline KCL items associated with maintenance of robustness and deterioration to pre-frailty or frailty over six years. Key findings include that visiting friends and participating in community activities were protective, while poor nutritional status increased risk. *p < 0.05 compared with baseline. Abbreviations: OR, odds ratio; CI, confidence interval; KCL, Kihon Checklist. |
In the multivariable logistic regression analyses, the independent variables for each model were selected according to the dependent variable. Specifically, the independent variables used when the dependent variable was robust-to-robust, robust-to-pre-frail, robust-to-frail, and pre-frail-to-frail, as well as those used when the dependent variable was frail-to-robust or pre-frail, are presented in Table 3. Stepwise logistic regression analysis showed that the questions that were independent factors for maintaining robustness were “Q4: Visited friends in 2016 and 2022 [odds ratio (OR), 3.346]” and “Q10: Does not fear falling in 2016 and 2022 (OR, 4.693)” (Table 4). The questions associated with a transition from robustness to pre-frailty were “Q6: Could climb stairs without holding handrails/walls in 2016 but not in 2022”, “Q13: Did not have difficulty chewing tough foods in 2016 but does in 2022”, and “Q20: Knew the current date in 2016 but does not in 2022”. The ORs were 3.484, 2.532, and 3.559, respectively (Table 4).
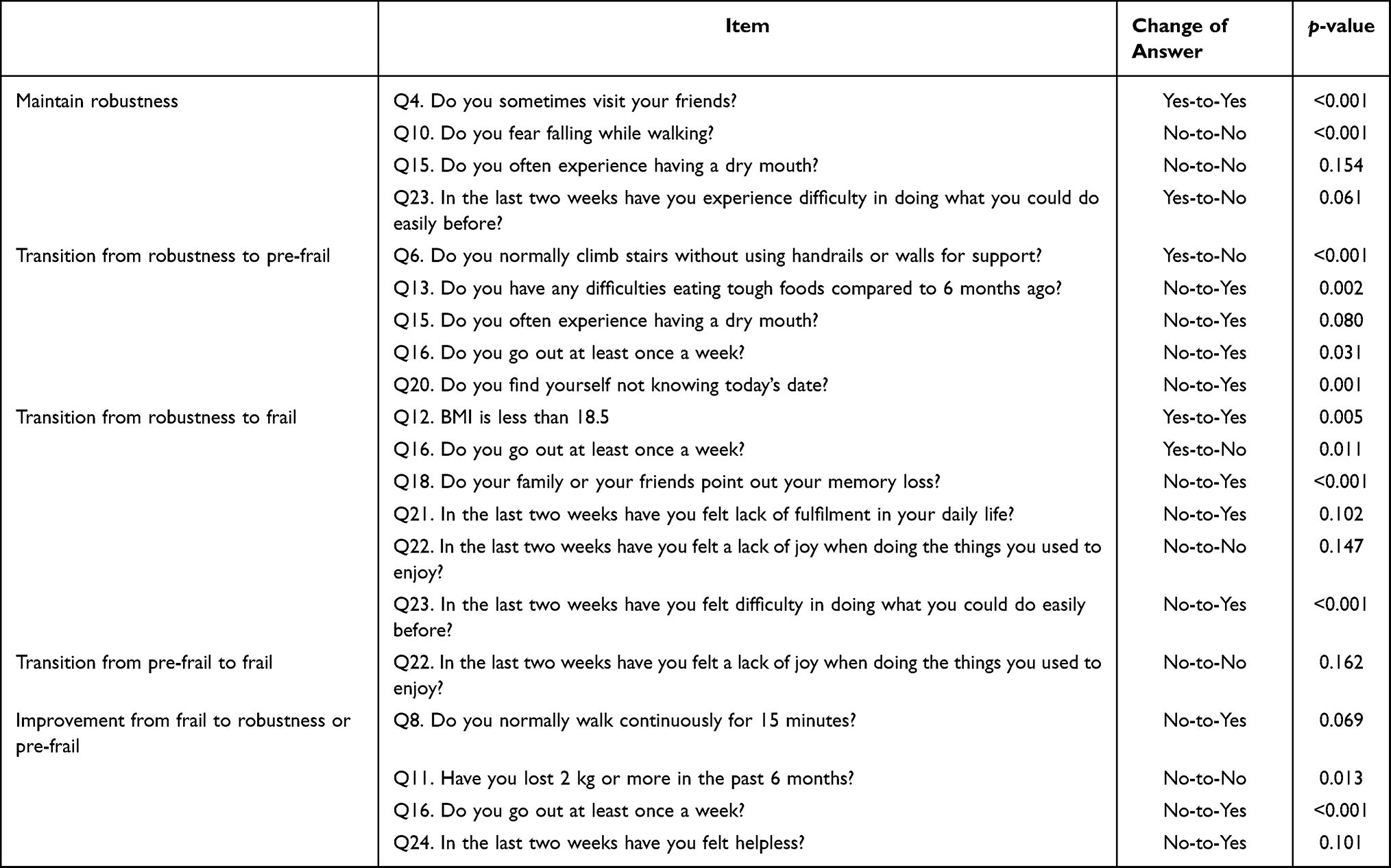 |
Table 3 Item-Level Predictors of Frailty Transitions in Univariate Methods Identified Using the Kihon Checklist (KCL) in Community-Dwelling Older Adults Aged 70 Years in 2016 and Re-Evaluated at Age 76 Years in 2022, Agano City, Niigata Prefecture, Japan |
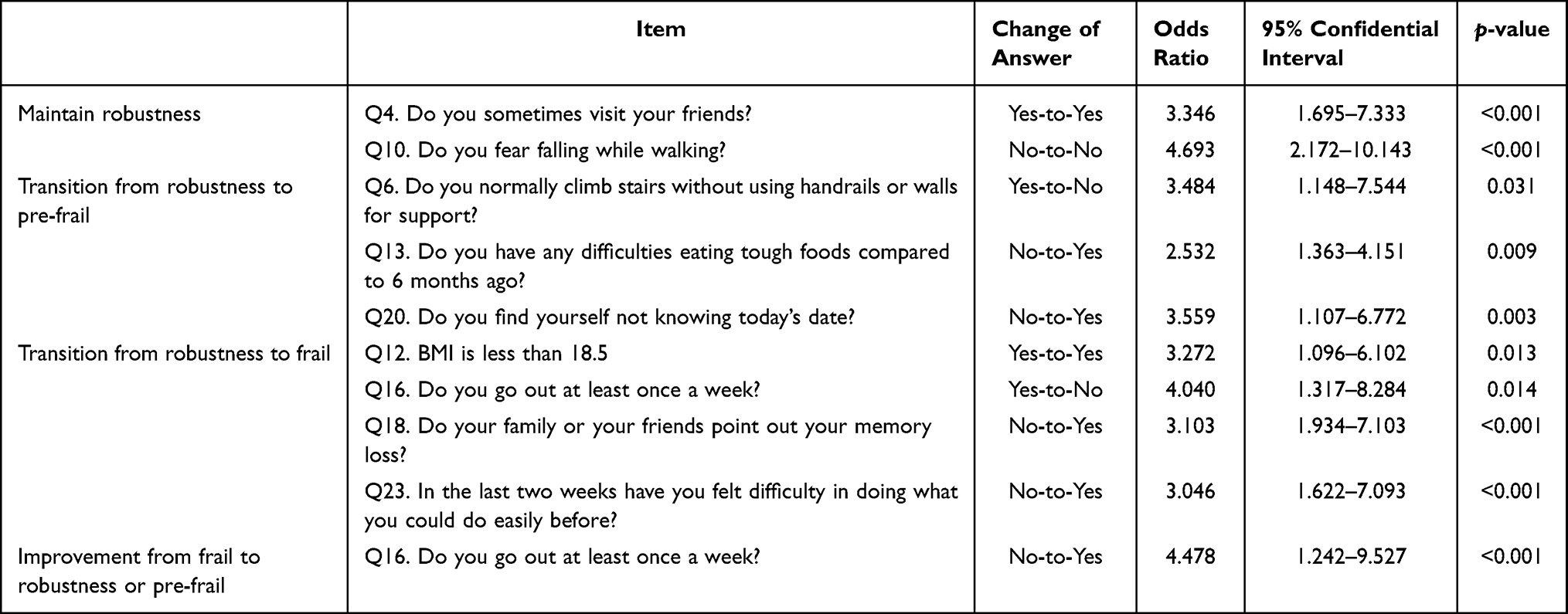 |
Table 4 Item-Level Predictors of Frailty Transitions in Multivariate Logistic Regression Stepwise Method Identified Using the Kihon Checklist (KCL) in Community-Dwelling Older Adults Aged 70 Years in 2016 and Re-Evaluated at Age 76 Years in 2022, Agano City, Niigata Prefecture, Japan |
The questions associated with a transition from robustness to frailty were “Q12: BMI < 18.5 in 2016 and 2022”, “Q16: Went out once weekly in 2016 but not in 2022”, “Q 18: Family/friends did not notice forgetfulness in 2016 but noticed in 2022”, and “Q23: Did not find any difficulty performing any tasks in 2016 but finds difficulty performing such tasks in 2022”. The ORs were 3.272, 4.040, 3.103, and 3.046, respectively (Table 4). The question independently associated with an improvement from frailty to robustness or pre-frailty was “Q16: Did not go out once weekly in 2016 but went out once weekly in 2022, (OR 4.478)” (Table 4). However, no significant factors were independently associated with a deterioration from pre-frailty to frailty. Similar results were obtained in the sensitivity analysis.
Discussion
In the current study, factors found to maintain robustness were visiting friends and not fearing falling while walking. First, visiting friends involves going out, which is important for preventing frailty.22,24,25 Furthermore, engaging in social connections is important for maintaining relationships with others, such as family, relatives, friends, and neighbors. Being connected with others establishes social capital, which comprises trust, relationships, and social networks, and is physically important and prevents social frailty.26,27 Second, fear of falling is considered a risk factor for frailty, similar to the findings of Hirose et al16 in their 1-year longitudinal study. We speculated that this would lead to a reduction in the range of activities and opportunities to go out,28 because falls in older persons are likely to lead to fractures in the vertebrae or hip joints, deterioration of activity status, and even death.29 These two factors may contribute to the prevention of social frailty and poor physical status. Notably, fear of falling did not necessarily translate into activity restriction among participants who remained robust. This may be explained by the adoption of preventive strategies, such as safer route selection, use of supportive devices, or engagement in balance and strength training, as well as by the maintenance of social interactions, which provide psychological support and motivation to remain active. These factors may have mitigated the potentially negative effects of fear of falling on activity levels.
The following factors were identified as contributing to the transition from robustness to pre-frailty: inability to climb stairs without using handrails or walls for support; having difficulties eating tough foods compared to 6 months ago; and not knowing today’s date. First, the ability to climb stairs without using a handrail or wall is a reported factor in maintaining robustness, and the inability to do so is likely to transition to frailty.12,16 These findings are similar to those of the present study. Climbing stairs requires more muscle strength and balance ability than walking on flat ground,30,31 and previous studies have reported that people who can walk continuously for ≥15 min are more likely to remain robust 6 years later.22 Climbing stairs without assistance may be more likely to affect the relatively early stages of physical decline in the KCL, which is more likely to affect the transition to pre-frailty than other physical function-related items.
Second, oral-frailty items, such as difficulty in eating tough foods, also influenced the transition to pre-frailty. Difficulty eating tough foods is likely to occur relatively early in oral frailty,32 and it is presumed that oral intake declines, subsequently leading to weight loss, muscle weakness, and cognitive function decline.28,33 In a survey of residents, Kera et al25 identified the factors that significantly increase each subdomain score of the KCL as “experience of falling”, “oral frailty”, and “housebound”. Furthermore, Hirose et al16 found that not experiencing a dry mouth was a factor in improving from frailty to robustness. Similar to previous reports, our study also showed that “falling”, “oral frailty”, and “housebound” were important factors.
Third, loss of date awareness is affected by a decline in cognitive function. A decline in cognitive function may lead to decreased motivation to become active, making it impossible to maintain robustness.34,35 Thus, physical and oral functions, as well as the maintenance of cognitive function are important for maintaining a robust state of health. In addition, a higher proportion of participants in this group were unable to walk continuously for 15 min, suggesting that reduced walking endurance may represent an early stage of functional decline leading to pre-frailty. Oral frailty also appeared to coexist with lower BMI, supporting the close interrelationship between oral function and nutritional status. Furthermore, decline in cognitive function, as reflected by disorientation in date, may accelerate disengagement from physical and social activities. These findings indicate that deterioration in physical endurance, oral and nutritional status, and cognitive capacity jointly contribute to the transition from robustness to pre-frailty. Kamasaki et al24 found that elderly people with pre-frailty showed distinctive characteristics, including poor physical function, poor nutritional status, and depressive mood, similar to our findings. They stated that elderly persons with pre-frailty should undergo physical and psychological interventions to improve robustness.
The following factors were identified as contributing to the transition from robustness to frailty: BMI <18.5 kg/m2 and difficulty in doing things that could easily be done before. With regard to BMI <18.5 kg/m2, individuals who are underweight at middle age (50–69 years of age) have a higher risk of transitioning to frailty 6–8 years later.19,36 This may be due to muscle weakness and decreased oral intake.37 However, several studies have reported that obesity and high waist circumference adversely affect frailty.37,38 Therefore, below-normal weight and obesity should be avoided; consequently, optimal weight may maintain robustness in older individuals. Previous surveys have concluded that difficulty in doing things that could easily be done before is an important factor in maintaining robustness and preventing the transition to frailty,12,16 similar to our findings. Moreover, increasing difficulty in performing tasks previously done with ease may reflect physical impairment as well as subtle cognitive decline, particularly in executive and attentional functions. This interpretation is supported by the independent association of memory loss recognized by family or friends (Q18) with frailty transition. Taken together, persistently low BMI, reduced outings, memory loss, and task difficulty highlight the interplay of nutritional, social, cognitive, and functional factors in accelerating the direct transition from robustness to frailty.
Several participants improved from frailty to pre-frailty or robustness during the 6-year follow-up. The factor most strongly associated with this improvement was a change in response to “going out at least once per week”, shifting from negative to positive between baseline and follow-up. This suggests that the adoption of regular outings can serve as a catalyst for recovery even among individuals already classified as frail. Going out once per week may represent physical activity and an opportunity for cognitive stimulation and social engagement, which are known to mitigate depressive mood and social isolation. These multidimensional benefits may have contributed to reversing frailty status. Importantly, this finding supports the concept of frailty as a reversible condition and emphasizes the potential of relatively simple lifestyle modifications, such as encouraging routine outings, to facilitate recovery trajectories in older adults.
Frailty is considered reversible; notably, a frail status can return to robustness with appropriate interventions.7 In fact, 40.9% of the frail individuals in this study improved to pre-frailty or robustness after 6 years. Appropriate intervention for frailty is important; however, to the best of our knowledge, key aspects and intervention timing following status changes remain unclear. Although some studies have evaluated all aspects of physical condition, house restraint, and depressive mood as risk factors for frailty,29,39–42 few studies have defined risk factors considering the KCL items.19,43 Ishikawa et al43 conducted a 4-year longitudinal study on community-dwelling older adults in Japan and categorized item responses as “bad”, “worse”, “improved”, or “good” using definitions comparable to those in the present study. They reported that deterioration in the cognitive function domain and worsening of item Q18 were significant risk factors for long-term care certification in the younger subgroup. Although their outcome was long-term care certification, rather than frailty progression or recovery, the findings are conceptually consistent with the present results, considering the close relationship between frailty and the need for long-term care. Similarly, a multivariate analysis by Ohashi et al19 demonstrated that lower baseline scores in the physical activity domain predicted transition to frailty over five years, which also aligns with our findings. To the best of our knowledge, however, no previous studies have investigated the association between changes in responses at baseline and follow-up with the maintenance of robustness or the transition to frailty, underscoring the novelty of the present study.
Through multiple logistic regression analysis, we identified the change in answering Q16: “Do you go out at least once per week?” from no in 2016 to yes in 2022 as an independent factor for improvement from frailty to robustness or pre-frailty. As noted above, our findings suggest that local residents were more likely to transition to frailty when they stopped going out and were more likely to improve from frailty when they started going out. Going out once a week or more is not simply a component of exercise, it is also associated with cognitive function44 and social frailty, such as being house-bound and/or having a depressed mood.45,46 These two aspects highlight the importance of developing the habit of going out and having connections with others.
In this study, 60.9%, 26.8%, and 12.3% of the elderly residents aged 70 years in 2016 were robust, pre-frail, and frail, respectively, as assessed via the KCL (Table 1). The prevalence of frailty in elderly Japanese individuals has been reported to range from 4–17.2% among adults aged ≥65 years.39,47–49 Since the reported prevalence of frailty in our study is comparable to those reported in other studies, our results are considered a valid reflection of the general population living in the area. Furthermore, the prevalence of frailty in our study is similar to those of previous studies during the COVID-19 pandemic in Japan. Several recent studies have examined the effects of the COVID-19 pandemic on frailty in Japan. Hirose et al50 demonstrated that frailty prevalence increased progressively from the pre-pandemic period through the first and second waves, largely due to declines in visiting friends and going out, and proposed the notion of “pandemic-associated frailty”. In a subsequent study, they also reported that robustness declined, and pre-frailty increased between 2020 and 2022, with sustained engagement in hobbies and community activities serving as protective factors.51 Shinohara et al52 further showed in cross-sectional surveys from 2020 to 2023 that reduced food intake and social interactions contributed to worsening frailty, while Yokoro et al53 highlighted that low dietary variety during 2020–2021 was significantly associated with incident frailty. Our study extends these findings by providing long-term, item-level evidence across 6 years, spanning both pre- and post-pandemic phases. In line with pandemic-focused research, we found that social engagement, such as visiting friends and participating in community activities or hobbies, protected against deterioration, whereas lack of participation was a risk factor. We also confirmed the importance of nutritional aspects, including weight loss, consistent with prior reports on dietary variety. Unlike previous studies that primarily addressed short-term pandemic effects, our longitudinal analysis demonstrates that psychosocial and lifestyle-related factors exert sustained influence on frailty transitions in community-dwelling older adults. Consequently, the decrease in visiting friends and going out may be ascribed to several restrictive measures during the COVID-19 pandemic, such as lockdowns and social distancing. Therefore, the frailty observed in our study may be partly described as pandemic-induced frailty.
This study had some limitations. First, the age of the participants was limited to 70 and 76 years for the first and second surveys, respectively, because they were conducted through a municipal project. Reduced age heterogeneity is one of the main limitations in examining frailty trends. Second, we did not assess the frailty status through history-taking or physical examination. Nevertheless, the robustness, pre-frailty, and frailty rates at baseline were comparable to previous reports,39,48–50 and the present findings were considered compatible with those of a natural history study in a community-dwelling population. However, few reports have identified the factors involved in the maintenance of health status, pre-frailty, and transition to frailty using responses at two time points, which is one of the strengths of this study. Third, we did not exclude participants based on the presence or absence of trauma or serious health events, which potentially biased our results. Nevertheless, the reported rate of fragility fractures among the general population aged 70–79 years was 1.3 fractures per 1000 persons per year,54 implying that fractures may have had only a minimal, non-significant impact on the results. Fourth, participant characteristics may have influenced the results. The study included only residents of Agano City who were exactly 70 years old at baseline and agreed to complete both surveys. Such participants might have been relatively health-conscious and socially engaged, compared with those who did not respond, potentially leading to underestimation of frailty prevalence and overestimation of robustness maintenance. Furthermore, as the study population was restricted to a single municipality in Niigata Prefecture, regional lifestyle and healthcare access could have affected the observed frailty transitions. These factors should be considered when interpreting the generalizability of our findings. Finally, we could not compare the numbers and characteristics of participants that completed both surveys in 2016 and 2022 to those that completed only one survey in 2016 to illustrate how the final population represents the target population from our data. In addition, medical illnesses are considered risk factors for frailty,55–57 but their impact on the present study results are unclear, which is another limitation of this study. Despite these drawbacks, our sensitivity analysis served to indicate the validity of the logistic regression results and was regarded as an integral component of the study, and its results were similar to the main results, confirming the credibility of the study findings.
Conclusions
This study demonstrated that changes in specific KCL items were significantly associated with the maintenance of robustness, transition to pre-frailty or frailty, and recovery from frailty among community-dwelling older adults over a 6-year period. Social engagement, absence of fear of falling, oral function, cognitive health, and adequate body weight emerged as protective factors, whereas low BMI, reduced outings, memory decline, and increasing difficulty with daily tasks predicted deterioration. Notably, a proportion of participants improved from frailty to pre-frailty or robustness when they initiated regular weekly outings, underscoring both the reversibility of frailty and the importance of simple lifestyle modifications. These findings align with prior reports on the role of physical activity, nutrition, and psychosocial health in frailty transitions while extending existing evidence by focusing on item-level changes across two time points.
Several points support the credibility of our findings. First, the prevalence of frailty observed in this cohort (12.3% at baseline) was comparable to previously reported prevalence rates in Japan, including those documented during the COVID-19 pandemic by Hirose et al,50 which reinforces the external validity of our results. Second, our methodological procedures enhanced credibility: we validated predictors consistent with previous studies, employed a multicentric study design, and analyzed a sufficiently large sample that met pretested eligibility criteria with a high follow-up rate. These features strengthen both the reliability and generalizability of the study.
Some limitations should be acknowledged. First, several variables were based on single questionnaire items, which may have led to over- or underestimation of associations due to reporting bias. To mitigate this, our sensitivity analysis results were consistent with the main findings, thereby supporting robustness. Second, the study was conducted in a single municipality, potentially limiting generalizability to other populations. Regional lifestyle and healthcare resources may have influenced frailty transitions as well. Future multicenter studies with larger, more diverse populations and objective measures (eg, physical performance tests, medical records) will be needed to validate and extend our findings.
For routine practice, our results emphasize the need to monitor changes in specific KCL items to identify individuals at risk of frailty progression, rather than relying solely on total scores. For future research, multicentric longitudinal studies incorporating objective physical and cognitive assessments are warranted. At the policy level, municipal health initiatives could integrate routine KCL screening with community-based programs promoting social engagement, oral health, balanced nutrition, and regular outings to prevent frailty and support recovery in older adults.
Abbreviations
BMI, body mass index; CHS, Cardiovascular Health Study; COVID-19, coronavirus disease 2019; J-CHS, Japanese version of the Cardiovascular Health Study; KCL, Kihon Checklist; OR, odds ratio.
Data Sharing Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Institutional Review Board of Niigata University reviewed and approved this study (2019-0221, February 2, 2023). We conducted this study according to the relevant guidelines and regulations. The need for informed consent was waived by the Institutional Review Board of Niigata University due to the retrospective nature of the study.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing and publication support. We would also like to thank Ms. Takai for her assistance in data collection in this study.
Author Contributions
NI, MO, TY, YH, TF, RM, and HK conceived and designed the study. NI collected the data. DH analyzed the data. NI wrote the manuscript. DH, MO, TY, YH, TF, RM, and HK critically revised the manuscript for important intellectual content. All the authors have read and approved the final version of the manuscript, and made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
This paper has been uploaded to ResearchSquar as a preprint: https://www.researchsquare.com/article/rs-5046469/v1.
References
1. Cabinet Office. Annual report on the aging society. 2021. Available from: https://www8.cao.go.jp/kourei/english/annualreport/2021/pdf/2021.pdf.
2. Statistics Bureau of Japan. Population estimates (as of October 1, 2024). Tokyo: Statistics Bureau of Japan; 2024. Available from: https://www.stat.go.jp/data/jinsui/2024np/index.html.
3. National Institute of Population and Social Security Research. Population projections for Japan (2023 revision; Population Research Series No. 347). Tokyo: National Institute of Population and Social Security Research; 2023. Available from: https://www.ipss.go.jp/pp-zenkoku/j/zenkoku2023/pp_zenkoku2023.asp?utm_source=chatgpt.com.
4. Arai H, Ouchi Y, Toba K, et al. Japan as the front-runner of super-aged societies: perspectives from medicine and medical care in Japan. Geriatr Gerontol Int. 2015;15(6):673–687. doi:10.1111/ggi.12450
5. Muramatsu N, Akiyama H. Japan: super-aging society preparing for the future. Gerontologist. 2011;51(4):425–432. doi:10.1093/geront/gnr067
6. Walston J, Buta B, Xue QL. Frailty screening and interventions: considerations for clinical practice. Clin Geriatr Med. 2018;34(1):25–38. doi:10.1016/j.cger.2017.09.004
7. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.m146
8. Makizako H, Shimada H, Doi T, Tsutsumimoto K, Suzuki T. Impact of physical frailty on disability in community-dwelling older adults: a prospective cohort study. BMJ Open. 2015;5(9):e008462. doi:10.1136/bmjopen-2015-008462
9. Arai H, Satake S. English translation of the Kihon Checklist. Geriatr Gerontol Int. 2015;15(4):518–519. doi:10.1111/ggi.12397
10. Tomata Y, Hozawa A, Ohmori-Matsuda K, et al. Validation of the Kihon Checklist for predicting the risk of 1-year incident long-term care insurance certification: the Ohsaki Cohort 2006 Study. Nihon Koshu Eisei Zasshi. 2011;58(1):3–13.
11. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. Sci World J. 2001;1:323–336. doi:10.1100/tsw.2001.58
12. Watanabe D, Yoshida T, Watanabe Y, Yamada Y, Miyachi M, Kimura M. Validation of the Kihon Checklist and the frailty screening index for frailty defined by the phenotype model in older Japanese adults. BMC Geriatr. 2022;22(1):478. doi:10.1186/s12877-022-03177-2
13. Sewo Sampaio PY, Sampaio RA, Yamada M, Arai H. Systematic review of the Kihon Checklist: is it a reliable assessment of frailty? Geriatr Gerontol Int. 2016;16(8):893–902. doi:10.1111/ggi.12833
14. Ito K, Kawai H, Tsuruta H, Obuchi S. Predicting incidence of long-term care insurance certification in Japan with the Kihon Checklist for frailty screening tool: analysis of local government survey data. BMC Geriatr. 2021;21(1):22. doi:10.1186/s12877-020-01968-z
15. Satake S, Senda K, Hong YJ, et al. Validity of the Kihon Checklist for assessing frailty status. Geriatr Gerontol Int. 2016;16(6):709–715. doi:10.1111/ggi.12543
16. Hirose T, Sawaya Y, Ishizaka M, Hashimoto N, Kubo A, Urano T. Kihon Checklist items associated with the development of frailty and recovery to robust status during the COVID-19 pandemic. Geriatr Gerontol Int. 2022;22(9):745–752. doi:10.1111/ggi.14447
17. Yamada M, Arai H. Predictive value of frailty scores for healthy life expectancy in community-dwelling older Japanese adults. J Am Med Dir Assoc. 2015;16(11):
18. Tomata Y, Sugiyama K, Kaiho Y, Sugawara Y, Hozawa A, Tsuji I. Predictive ability of a simple subjective memory complaints scale for incident dementia: evaluation of Japan’s national checklist, the “Kihon Checklist”. Geriatr Gerontol Int. 2017;17(9):1300–1305. doi:10.1111/ggi.12864
19. Ohashi M, Yoda T, Imai N, et al. Five-year longitudinal study of frailty prevalence and course assessed using the Kihon Checklist among community-dwelling older adults in Japan. Sci Rep. 2021;11(1):12399. doi:10.1038/s41598-021-91979-6
20. Fallah N, Mitnitski A, Searle SD, Gahbauer EA, Gill TM, Rockwood K. Transitions in frailty status in older adults in relation to mobility: a multistate modeling approach employing a deficit count. J Am Geriatr Soc. 2011;59(3):524–529. doi:10.1111/j.1532-5415.2011.03300.x
21. Hoogendijk EO, Dent E. Trajectories, transitions, and trends in frailty among older adults: a review. Ann Geriatr Med Res. 2022;26(4):289–295. doi:10.4235/agmr.22.0148
22. Imai N, Yoda T, Horigome Y, et al. Determining factors that maintain physical function or increase frailty using the Kihon checklist among community-dwelling older adults: a six-year longitudinal study in Agano, Japan. BMC Geriatr. 2023;23(1):336. doi:10.1186/s12877-023-04055-1
23. Agano City Home Page. Agano city data collection. 2022. Available from: https://www.city.agano.niigata.jp/material/files/group/3/data2022.pdf.
24. Kamasaki T, Otao H, Hachiya M, et al. Domains of the Kihon checklist associated with prefrailty among community-dwelling older adults. Ann Geriatr Med Res. 2023;27(2):106–115. doi:10.4235/agmr.23.0019
25. Kera T, Kawai H, Yoshida H, et al. Classification of frailty using the Kihon checklist: a cluster analysis of older adults in urban areas. Geriatr Gerontol Int. 2017;17(1):69–77. doi:10.1111/ggi.12676
26. Hu S, Jin C, Li S. Association between social capital and frailty and the mediating effect of health-promoting lifestyles in Chinese older adults: a cross-sectional study. BMC Geriatr. 2022;22(1):175. doi:10.1186/s12877-022-02815-z
27. Zhao J, Ma Y, Tanimoto T, et al. Effects of physical activity and stress on the relationship between social capital and quality of life among breast cancer survivors. Sci Rep. 2020;10(1):17746. doi:10.1038/s41598-020-74706-5
28. Tani A, Mizutani S, Oku S, et al. Association between oral function and physical pre-frailty in community-dwelling older people: a cross-sectional study. BMC Geriatr. 2022;22(1):726. doi:10.1186/s12877-022-03409-5
29. Fang X, Shi J, Song X, et al. Frailty in relation to the risk of falls, fractures, and mortality in older Chinese adults: results from the Beijing Longitudinal Study of Aging. J Nutr Health Aging. 2012;16(10):903–907. doi:10.1007/s12603-012-0368-6
30. Cudejko T, Button K, Al-Amri M. Validity and reliability of accelerations and orientations measured using wearable sensors during functional activities. Sci Rep. 2022;12(1):14619. doi:10.1038/s41598-022-18845-x
31. Kontto J, Paalanen L, Sund R, et al. Using multiple imputation and intervention-based scenarios to project the mobility of older adults. BMC Geriatr. 2022;22(1):311. doi:10.1186/s12877-022-03008-4
32. Kim H, Lee E, Lee SW. Association between oral health and frailty: results from the Korea National Health and Nutrition Examination Survey. BMC Geriatr. 2022;22(1):369. doi:10.1186/s12877-022-02968-x
33. Jiang Z, Liu X, Lü Y. Unhealthy oral status contributes to the older patients with cognitive frailty: an analysis based on a 5-year database. BMC Geriatr. 2022;22(1):980. doi:10.1186/s12877-022-03673-5
34. Nari F, Jang BN, Youn HM, Jeong W, Jang SI, Park EC. Frailty transitions and cognitive function among South Korean older adults. Sci Rep. 2021;11(1):10658. doi:10.1038/s41598-021-90125-6
35. Yuan Y, Peng C, Burr JA, Lapane KL. Frailty, cognitive impairment, and depressive symptoms in Chinese older adults: an eight-year multi-trajectory analysis. BMC Geriatr. 2023;23(1):843. doi:10.1186/s12877-023-04554-1
36. Ho HE, Yeh CJ, Chu WM, Lee MC. Midlife body mass index trajectory and risk of frailty 8 years later in Taiwan. J Nutr Health Aging. 2019;23(9):849–855. doi:10.1007/s12603-019-1226-6
37. Reinders I, Visser M, Schaap L. Body weight and body composition in old age and their relationship with frailty. Curr Opin Clin Nutr Metab Care. 2017;20(1):11–15. doi:10.1097/MCO.0000000000000332
38. Suthutvoravut U, Tanaka T, Takahashi K, Akishita M, Iijima K. Living with family yet eating alone is associated with frailty in community-dwelling older adults: the Kashiwa study. J Frailty Aging. 2019;8(4):198–204. doi:10.14283/jfa.2019.22
39. Jung H, Yamasaki M. Association of lower extremity range of motion and muscle strength with physical performance of community-dwelling older women. J Physiol Anthropol. 2016;35(1):30. doi:10.1186/s40101-016-0120-8
40. Katsura T, Abe N, Komata M, et al. The relationship between the houseboundedness and frailty of community-dwelling elderly persons. J Rural Med. 2018;13(2):141–150. doi:10.2185/jrm.2972
41. Marconcin P, Barak S, Ferrari G, et al. Prevalence of frailty and its association with depressive symptoms among European older adults from 17 countries: a 5-year longitudinal study. Int J Environ Res Public Health. 2022;19(21):14055. doi:10.3390/ijerph192114055
42. Schwenk M, Mohler J, Wendel C, et al. Wearable sensor-based in-home assessment of gait, balance, and physical activity for discrimination of frailty status: baseline results of the Arizona frailty cohort study. Gerontology. 2015;61(3):258–267. doi:10.1159/000369095
43. Ishikawa N, Katsura T, Hara M. Changes in Kihon Checklist items and new Certification of long-term care needs among Japanese community-dwelling elders. J Rural Med. 2021;16(4):270–279. doi:10.2185/jrm.2021-032
44. Minaki K, Amano H, Masumoto T, Otani S, Urakami K, Kurozawa Y. Association between frequency of going out and mild cognitive impairment in community-dwelling older adults: a pilot study in frailty prevention groups. Psychogeriatrics. 2022;22(6):833–842. doi:10.1111/psyg.12890
45. Doi T, Tsutsumimoto K, Nakakubo S, Kurita S, Ishii H, Shimada H. Associations between active mobility index and disability. J Am Med Dir Assoc. 2022;23(8):1335–1341. doi:10.1016/j.jamda.2021.08.036
46. Makizako H, Shimada H, Tsutsumimoto K, et al. Social frailty in community-dwelling older adults as a risk factor for disability. J Am Med Dir Assoc. 2015;16(11):
47. Arakawa Martins B, Visvanathan R, Barrie H, et al. Frailty prevalence using Frailty Index, associated factors and level of agreement among frailty tools in a cohort of Japanese older adults. Arch Gerontol Geriatr. 2019;84:103908. doi:10.1016/j.archger.2019.103908
48. Satake S, Shimokata H, Senda K, Kondo I, Toba K. Validity of total Kihon Checklist score for predicting the incidence of 3-year dependency and mortality in a community-dwelling older population. J Am Med Dir Assoc. 2017;18(6):
49. Zhao W, Ukawa S, Sasaki S, et al. Association between moderate physical activity level and subsequent frailty incidence among community-dwelling older adults: a population-based cohort study. J Aging Phys Act. 2023;31(5):815–822. doi:10.1123/japa.2022-0052
50. Hirose T, Sawaya Y, Ishizaka M, Hashimoto N, Kubo A, Urano T. Frailty under COVID-19 pandemic in Japan: changes in prevalence of frailty from 2017 to 2021. J Am Geriatr Soc. 2023;71(5):1603–1609. doi:10.1111/jgs.18237
51. Hirose T, Sawaya Y, Ishizaka M, Hashimoto N, Kubo A, Urano T. Prevalence and factors associated with changes in frailty among community-dwelling older adults in Japan during the COVID-19 pandemic: a prospective cohort study from 2020 to 2022. Geriatr Gerontol Int. 2024;24(1):40–47. doi:10.1111/ggi.14748
52. Shinohara T, Saida K, Tanaka S, Murayama A, Higuchi D. Changes in frailty and lifestyle among community-dwelling older adults: a two-point cross-sectional study during and after the COVID-19 pandemic in Japan. Geriatr Nurs. 2024;58:208–214. doi:10.1016/j.gerinurse.2024.05.014
53. Yokoro M, Otaki N, Yano M, Imamura T, Tanino N, Fukuo K. Low dietary variety is associated with incident frailty in older adults during the coronavirus disease 2019 pandemic: a prospective cohort study in Japan. Nutrients. 2023;15(5):1145. doi:10.3390/nu15051145
54. Imai N, Nozaki A, Shobugawa Y, et al. Incidence of four major osteoporotic fragility fractures among older individuals in Sado, Japan, in 2020. J Bone Miner Metab. 2024;42(6):647–652. doi:10.1007/s00774-024-01529-z
55. García-Esquinas E, Graciani A, Guallar-Castillón P, López-García E, Rodríguez-Mañas L, Rodríguez-Artalejo F. Diabetes and risk of frailty and its potential mechanisms: a prospective cohort study of older adults. J Am Med Dir Assoc. 2015;16(9):748–754. doi:10.1016/j.jamda.2015.04.008
56. Walker SR, Gill K, Macdonald K, et al. Association of frailty and physical function in patients with non-dialysis CKD: a systematic review. BMC Nephrol. 2013;14:228. doi:10.1186/1471-2369-14-228
57. Afilalo J, Karunananthan S, Eisenberg MJ, Alexander KP, Bergman H. Role of frailty in patients with cardiovascular disease. Am J Cardiol. 2009;103(11):1616–1621. doi:10.1016/j.amjcard.2009.01.375
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Geriatric Assessment in the Emergency Department: A Prospective Cohort Study of Process, Clinical, and Patient-Reported Outcomes
O'Shaughnessy Í, Robinson K, Whiston A, Barry L, Corey G, Devlin C, Hartigan D, Synnott A, McCarthy A, Moriarty E, Jones B, Carroll I, Shchetkovsky D, O'Connor M, Steed F, Carey L, Conneely M, Leahy A, Quinn C, Shanahan E, Ryan D, Galvin R
Clinical Interventions in Aging 2024, 19:189-201
Published Date: 7 February 2024
Associations Between Longitudinal Changes in Frailty and Incident Arthritis: A Multi-Cohort Study
Han Z, Qu H, Wang X, Ma H, Song S
Risk Management and Healthcare Policy 2026, 19:591789
Published Date: 17 March 2026