Back to Journals » International Journal of General Medicine » Volume 16
Factors Associated with COVID-19 Severity Among Kidney Transplant and Non-Kidney Transplant Patients at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Authors Kidane K, Alemu ZA, Biratu TD, Juhar LH
Received 20 July 2023
Accepted for publication 30 October 2023
Published 6 November 2023 Volume 2023:16 Pages 5097—5108
DOI https://doi.org/10.2147/IJGM.S423805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kal Kidane,1 Zewdie Aderaw Alemu,2 Tolesa Diriba Biratu,2 Leja Hamza Juhar3
1Kidney Transplantation Center, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2School of Public Health, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Department of Internal Medicine, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Tolesa Diriba Biratu, Tel +251923717514, Email [email protected]
Background: The COVID-19 epidemic is a rapidly shifting situation that has resulted in significant regulatory reforms and widespread initiatives to deal with the initial crisis and its effects. The COVID-19 pandemic has had a significant impact on transplantation activities. The COVID-19 pandemic has caused various important challenges in the kidney transplant industry.
Objective: To identify the factors influencing COVID-19 severity in kidney transplant and non-kidney transplant patients at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Methods: A comparative cross-sectional study was conducted. This study included 364 patients (182 kidney transplants and 182 non-kidney transplants). A systematic random sampling was used to select the respondents. Professional nurses collected data for this study using a data extraction tools. Data were analyzed by using SPSS version 25 software. A multivariable logistic regression analysis was performed to identify the association between independent variables and COVID-19 severity with adjusted odds ratio (AOR), and 95% CI for AOR and P-value for testing significance.
Results: This study included 364 patients. Off the total, 34.1% developed severe COVID-19. In Multivariable logistic regression analysis, patients with 60 years and above age groups (AOR = 4.73; 95% CI: 1.86, 12.02), aged 40– 59 years (AOR = 2.70; 95% CI: 1.17, 6.22), chest congestion (AOR = 4.49; 95% CI: 2.37, 8.50), history of muscle or body aches (AOR = 0.47; 95% CI: 0.22, 0.99) shortness of breath (AOR = 3.03; 95% CI: 1.36, 6.74), changed or lost sense of taste or smell (AOR = 2.77; 95% CI: 1.34, 5.71), and muscle pain (AOR = 3.05; 95% CI: 1.40, 6.65) were significant variables associated with COVID-19 severity after adjusting for other variables.
Conclusion: The study revealed that 34.1% of patients had severe COVID-19. The majority of these patients underwent non-kidney transplants. Age groups and symptoms, such as chest congestion, shortness of breath, changed or lost sense of taste or smell, and muscle pain, were significant predictors of COVID-19 disease severity.
Keywords: COVID-19, severe, multivariable, regression, St. Paul‘s, Addis Ababa, Ethiopia
Introduction
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus that can spread from an infected person’s mouth or nose in small liquid particles when coughing, sneezing, speaking, sing, or breathing.1 COVID-19 is a global pandemic that has infected over 82 million people and killed more than 1.8 million worldwide as of December 31, 2020.2 The Covid-19 pandemic is a rapidly changing situation, with dramatic policy changes and universal efforts to deal with the initial crisis and minimize its consequences that have led to the collapse of healthcare systems, negatively affecting transplant programs.3
The COVID-19 pandemic has had a profound effect on transplantation activity.4 The kidney transplant sector is facing significant challenges related to the COVID-19 pandemic.5 There has been tremendous pressure on public-sector facilities to assist with KRT.6 There was a sharp decline in the number of kidney transplants, which resulted in excessive COVID-19-related deaths in KRT patients. COVID-19 has caused high mortality in kidney transplant recipients, especially in the elderly.3 Patients on the waiting list for kidney transplantation and those already transplanted are at serious risk of contracting COVID-19 infection due to immunosuppressants developed during long-lasting chronic kidney disease, which are enhanced in kidney transplant recipients from immunosuppressive treatment to prevent rejection.5
Mortality due to COVID-19 was highest among kidney transplant recipients (KTRs), followed by patients on hemodialysis, and lowest in the general population.7 KTRs are at an increased risk of severe infection, and their outcomes appear to be worse than those of the general population.8 Ethiopia is a sub-Saharan African country that hosted this pandemic and registered a total of 136,365 positive cases and 2087 deaths by late January 2021, the greatest number of cases and deaths in the East African area and the fifth-highest on the continent.9 To our knowledge, no study has been conducted to assess the factors influencing COVID-19 severity in kidney transplant patients and non-kidney transplant patients in this country. Therefore, this study aimed to identify the factors associated with COVID-19 severity among Kidney Transplant and Non-Kidney Transplant Patients at St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia.
Methods and Materials
Study Area and Period
This study was conducted at the St. Paul’s Hospital Millennium Medical College. The first living-related kidney transplant program was established in September 2015, in collaboration with the University of Michigan. Coordinated by the Ethiopian Federal Ministry of Health, the project was geared toward establishing local competency. In 2010, the Ethiopian government identified St. Paul’s Hospital Millennium Medical College (SPHMMC) in the Capital City, Addis Ababa, as the future home for the transplant program. An International Society of Nephrology fellow was recruited in 2012 who established a nephrology unit at SPHMMC with acute inpatient hemodialysis services that were later expanded to provide outpatient hemodialysis as a bridge to kidney transplantation.10
Study Design
A retrospective comparative cross-sectional study was conducted at the St. Paul’s Hospital Millennium Medical College.
Source Population
- The source population for the non-transplant group included all individuals (regardless of age and sex) admitted and followed up for CKD in SPHMMC.
- The transplant group included all individuals (regardless of age or sex) who underwent kidney transplantation at SPHMMC or elsewhere.
Study Population
All selected transplant and non-transplant patients infected by COVID 19 were admitted and followed up at St. Paul’s Hospital Millennium Medical College from March 2020 to January 2023 and fulfilled the inclusion criteria.
Sample Size Determination
The sample size for this study was determined using a double population sample size formula, which assumes that the number of kidney transplants and non-kidney transplants (CKD) was equal, power (1-β), significance level (α), proportion of exposed in the non-transplant group and ratio (non-transplants: kidney transplants).

where n = sample size in cases
r = ratio of unexposed to exposed
Zβ = desired power (typically 80%) =0.84
 = variability (standard deviation)
= variability (standard deviation)
(p1-p2) = Effect size (difference in proportions)
α = desired level of significance (typically 0.05)
A study conducted in Spain indicated that 58.7% of kidney transplant recipients and 42.8% of non-transplant recipients had COVID-19.11 Based on this information and the assumptions mentioned above, the sample size for this study was estimated using Epi Info version 7.1, and 364 samples were obtained (182 transplants = 182 and number of non-transplanted).
Sampling Technique and Procedure
For this study, we included two groups (kidney transplant and non-transplant groups). For these two groups, a systematic sampling method was used to select individuals from the population. A patient record file was used for data extraction based on this list. The interval of the patients’ record files for the transplant group was determined by dividing the total number of kidney transplant patients in the Kidney Transplantation Center by the total number of kidney transplant patients. Similarly, the interval between the patients’ record files for the non-transplant group was determined by dividing the total number of non-kidney transplants by the number of non-transplants.
Inclusion and Exclusion Criteria
Inclusion Criteria
- All patients underwent kidney transplantation (regardless of age and sex) at the St. Paul’s Hospital Millennium Medical College and elsewhere.
- All patients with CKD were admitted and followed up (regardless of age and sex) at St. Paul’s Hospital Millennium Medical College.
Exclusion Criteria
- All AKI patients
- Patients whose charts were not available or incomplete
Study Variable
- Dependent variable was COVID 19 infection (severe or non-severe)
- Independent variables:
Sex, age, educational level, residence, vital signs and symptoms at covid-19 admission, coexisting conditions, and behavioral variables.
Operational Definitions
- Severe COVID-19 was defined as any of the following: oxygen saturation <90% on room air; severe pneumonia; signs of severe respiratory distress (in adults, accessory muscle use, inability to complete full sentences, respiratory rate >30 breaths per minute; and, in children, very severe chest wall in-drawing, grunting, central cyanosis, or presence of any other general danger signs, including inability to breastfeed or drink, lethargy, convulsions, or reduced level of consciousness).
- Non-severe COVID-19 was defined as the absence of the criteria for severe or critical COVID-19.
- Severe COVID-19 was defined as admission (or transfer) to an intensive care unit, need for mechanical ventilation, or death.12
- Mild: no findings of pneumonia on HRCT and presence of mild clinical symptoms.
- Moderate disease: HRCT manifestations compatible with viral pneumonia and presence of respiratory symptoms and fever.
- Critical: having any of the following evidence: occurrence of respiratory failure requiring Mechanical Ventilation, shock, or other organ failure requiring ICU admission and monitoring.13
Data Collection Procedures and Quality Assurance
Data Collection Procedure
The English version of the data abstraction tool was adopted from patient charts and extracted from the related literature review. The tool includes sociodemographic factors, behavioral factors, kidney transplantation, and clinical-related characteristics. Data were collected by nursing professionals working at the Kidney Transplantation Center.
Data Quality Management
Before collecting the actual data from the patients’ records, training was provided to the data collectors, including the pretest. The investigator supervised the data collection, and the data were checked for completeness and accuracy before leaving the actual data collection site. After collection, double entry was performed to minimize entry errors and to increase data quality.
Data Analysis
After the data were obtained, SPSS version 25 software was used to organize and analyze the data. To present the study participants’ characteristics, descriptive statistics such as frequencies and proportions were calculated for categorical variables. The mean and standard deviation were calculated for continuous variables with normal distribution; otherwise, the median and interquartile range were calculated. The results of this study are presented in tables and graphs. Binary logistic regression was used to identify the association between the factors and severity of COVID-19 among the study participants. Variables with a p-value less than 0.20 were selected for multivariable logistic regression. Logistic regression was checked using the Hosmer and Lemeshow goodness-of-fit test (chi-square=12.58, df = 8, P-value = 0.127). The strength of association will be measured using the adjusted odds ratio, and the statistical significance of the variables will be identified with a cutoff point of p-value less than 0.05.
Ethical Consideration
The ethical clearance and approval were obtained from the Institutional Review Board of St. Paul’s Hospital Millennium Medical College prior to starting the study (Reference Number: pm 23/239; dated on 14-October-2022). The supporting letter was obtained from the director of the Kidney Transplantation Centre. Informed verbal consent was obtained from survivors’ study participants, study participants who were not adult from their legal guardians and deceased patient’s next of kin via phone call. This verbal informed consent is approved by the Institutional Review Board of St. Paul’s Hospital Millennium Medical College.
In addition, data were gathered using medical registration numbers; no personal information identifier was gathered or used in the research report. Only the primary investigator and the data collectors had access to the data, and confidentiality was upheld during the whole study. All kidneys were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul. All procedures were carried out in accordance with the Declaration of Helsinki and the pertinent rules and regulations.
Results
Socio-Demographic Characteristics of Study Participants
A total of three hundred sixty-four study subjects (182 transplanted and 182 non-transplanted) were included, with a response rate of 100%. More than two-thirds of the study subjects 252(69.2%) were male. More than one-third of them were 130(35.7%). Among the transplants, less than half of 86(47.3%) were less than 40 years old. The majority of participants were 249(69.2%). Of the total number of non-transplant patients, 134(73.6%) were married. Approximately one in every four was 144(39.6%) with a secondary school education. Almost half of the study participants were 185(50.8%) affiliated with Orthodox religion. More than half of the study participants were unemployed 198(54.4%). The majority of study participants were 258(71.1%) urban residents (Table 1).
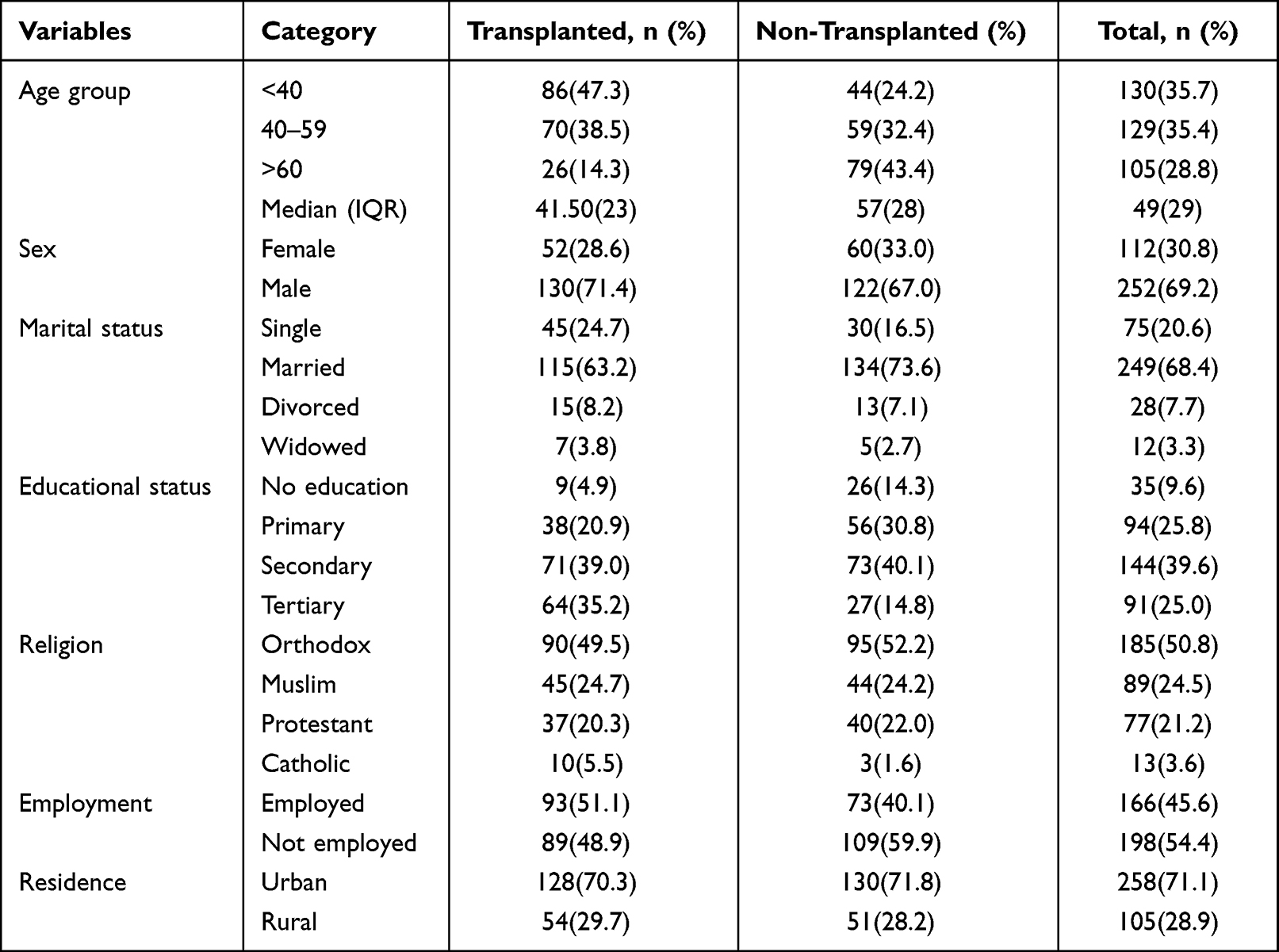 |
Table 1 Socio-Demographic Characteristics of Kidney Transplanted and Non-Transplanted COVID-19 Patients in SPHMMC, 2022 (n = 364) |
Preexisting Comorbidity
The findings of this study indicated that 319 patients (87.6%) had a history of comorbidity. Among the reported comorbidity, more than half (53.0%) of the participants had hypertension. Of these, 98(53.8%) were in the transplantation group. Almost one in four patients (27.2%) had diabetes, of which 49(26.9%) were transplanted and 50(27.5%) were non-transplanted. More than one-third, 131(36.0%) underwent dialysis, of which the majority (53.3%) were non-transplant patients (Table 2).
 |
Table 2 Comorbid Illness Characteristics of Covid-19 Patients Among Kidney Transplanted and Non-Transplanted Patients in SPHMMC, 2022 (n = 364) |
Baseline Vital Sign Characteristics Among Transplanted and Non-Transplanted Patients
As shown in Table 3, vital signs including respiratory rate, body temperature, and oxygen saturation were assessed. The majority of the study participants, 319(87.6%) had respiratory rate levels of less than 29 beats per minute. Among these patients, 169(92.9%) were transplant recipients, and 150(82.4) were non-transplant recipients. More than half, 216(59.3%) of patients had less than or equal to 37.4°C body temperature. Similarly, approximately two-thirds of the 237 patients (65.1%) had normal Oxygen Saturation. Of these, 131(72.0%) were kidney transplant recipients.
 |
Table 3 Baseline Vital Sign Characteristics Among Kidney Transplanted and Non-Transplanted Patients in SPHMMC, 2022 (n = 364) |
Symptomatic Characteristics of COVID-19 Among Study Participants
As illustrated in Table 4, the symptomatic characteristics of COVID-19 in kidney transplant and non-transplant patients were assessed. Half, 182(50.0%), of study participants had fever. Of this patient, more than half, 105(57.7%), of them from transplant. Almost one in four (43.4%) of the study participants had chills. Among the study participants, 91(50.0%) were transplant recipients, and 67(36.8%) were non-transplant recipients.
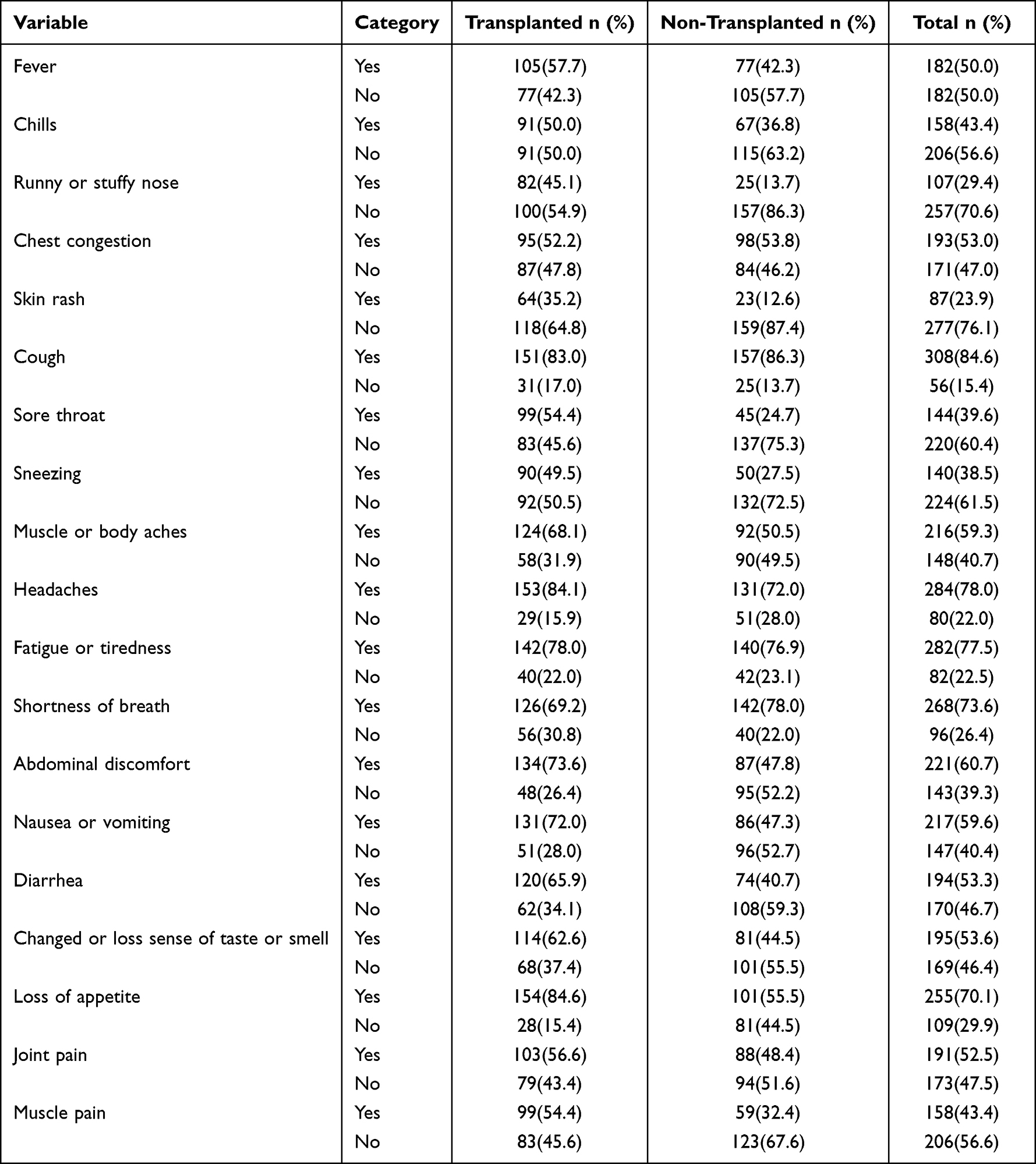 |
Table 4 Symptomatic Characteristics of COVID-19 Among Kidney Transplanted and Non-Transplanted Patients in SPHMMC, 2022 (n = 364) |
Similarly, among patients who had symptomatic, 107(29.4) had runny or stuffy nose, 193(53.0%) chest congestion, cough 308(84.6%), sore throat 144(39.6%), muscle or body aches 216(59.3%), headaches 284(78.0%), shortness of breath 268(73.6%) and loss of appetite 109(29.9%).
Behavioral Characteristic of Study Participants
As shown in Table 5, there were a small number of study participants, 40(11.0%) smoked cigarettes. Among these participants, 22(12.1%), were non-transplant recipients. Less than a quarter, 79(21.7%), of study participants consumed alcohol. Of these patients, 56(30.8) were non-transplant recipients.
 |
Table 5 Behavioral Characteristic of COVID-19 Patients Among Kidney Transplanted and Non-Transplanted Patients in SPHMMC, 2022 (n = 364) |
Severity and Outcome of COVID-19 Patients Among Kidney Transplant and Non-Transplant
As shown in Table 6, more than one-third, 124(34.1%) had severe COVID-19. Among these patients, close to one in every four (41.2%) was from non-kidney transplants. Of these patients, 22(6.0%) were asymptomatic, 110(30.2%) were mild, 108(29.7%) were moderate, 65(17.9%) were severe, and 59(16.2%) were critical. More than half of the 217(59.6%) patients showed an improvement in discharge outcome. The majority (69.8%) were kidney transplant COVID-19 patients. Seventy-six patients (20.9%) died.
 |
Table 6 Severity and Outcome of COVID-19 Patients Among Kidney Transplanted and Non-Transplanted Patients in SPHMMC, 2022 (n = 364) |
Factors Associated with COVID-19 Severity
In the binary logistic regression analysis, age, marital status, employment, residence, presence of comorbidity, signs and symptoms (fever, chills, chest congestion, cough, muscle or body aches, fatigue or tiredness, shortness of breath, abdominal discomfort, diarrhea, changed or loss of sense of taste or smell, loss of appetite, joint pain, muscle pain), body temperature, cigarette smoking, and consumption of alcohol were significantly associated with COVID-19 severity (p = 0.20).
Predictors with a P value less than 0.20 in the binary logistic regression analysis were included in the multivariable logistic regression analysis to control for the effect of confounding variables. Multivariable logistic regression analysis identified age group, chest congestion, muscle or body aches, shortness of breath, change or loss of sense of taste or smell, and muscle pain as being significantly associated with COVID-19 severity at a 5% level of significance.
This study revealed that patients with 60 years were approximately 4.73 times more likely to develop severe COVID-19 (AOR = 4.73; 95% CI: 1.86, 12.02) as compared to patients aged less than 40 years. Similarly, patients those in the 40–59 years’ age groups were 2.70 times more likely to develop severe disease (AOR = 2.70; 95% CI: 1.17, 6.22) compared with patients aged less than 40 years.
Patients who had symptoms of chest congestion were 4.49 times more likely to develop severe COVID-19 (AOR = 4.49; 95% CI: 2.37, 8.50) than those without symptoms. Patients with a history of muscle or body aches were 53% less likely to develop severe disease (AOR = 0.47; 95% CI: 0.22, 0.99) compared to those without a history. Similarly, among patients with symptoms, the odds of developing severe COVID-19 disease with shortness of breath were 3.03 times higher (AOR = 3.03;95% CI: 1.36, 6.74) than those who did not have such symptoms; patients with a changed or lost sense of taste or smell were 2.77 times more likely to develop severe (AOR = 2.77; 95% CI: 1.34, 5.71) compared to patients who did not have such symptoms, and the odds of developing severe COVID-19 among patients with symptoms of muscle pain were 3.05 times higher (AOR = 3.05; 95% CI: 1.40, 6.65) than in patients without symptoms (Table 7).
 |
Table 7 Multivariable Analysis of Factors Associated with COVID-19 Severity Among Kidney Transplanted and Non-Transplanted in SPHMMC, 2022 |
Discussion
COVID-19 causes a variety of symptoms ranging from asymptomatic or mild self-limited infections to severe and critical ventilator-dependent sickness and COVID-19 remains a significant cause of hospitalization and death among chronic kidney diseases. This study aimed to identify the factors associated with COVID19 severity among kidney transplant and non-kidney transplant patients at St. Paul’s Hospital, Millennium Medical College. In the multivariate logistic regression analysis, six variables were identified as significant independent variables that were significantly associated with COVID-19 severity.
This study revealed that 34.1% of the patients had severe COVID-19, and kidney transplantation (26.9%) was not associated with a higher rate of severe disease than non-kidney transplant patients (41.2%). In line with this study, a retrospective cohort study in Saudi Arabia found that 17% of patients with CKD were admitted to the intensive care unit and required mechanical ventilation.14 In contrast to this study, evidence from a systematic review showed that COVID–19 severity had moderate certainty among non–kidney transplant patients.15 A retrospective study from India indicated that 47.5 severity of COVID-19 in the non–kidney transplant patient group (47.5%) had severe COVID-19.16 These differences could be due to sample size, study area, and study design.
This study revealed that COVID-19 severity was higher among patients aged 40–59 years and those aged 60 years or older than in the other age categories. The findings of this study are supported by evidence from a systematic review17 of a study conducted in Turkey,18 Brazil,19 China,20 Qatar21 and Ghana22 which demonstrated that age is significantly associated with COVID-19 severity. A study conducted in our country also supported the finding that age is significantly associated with COVID-19 severity.23
Our findings indicate that the clinical symptoms and severity of COVID-19 are significantly associated with the disease. Patients with symptoms of chest congestion, shortness of breath, a changed or lost sense of taste or smell, and muscle pain were more likely to develop severe COVID-19 than those without. In line with this study, evidence from the COVID-19 Treatment Guidelines indicates that muscle weakness, chest pain, and shortness of breath are associated with severe COVID-19.24
In general, the conclusions of this study have significant implications for the management of COVID-19 severity. Program implementers would benefit from understanding the probable risk factors for COVID-19 severity, so they may prioritize actions to stop complications caused by the severity of the condition.
Strength and Limitation of the Study
To our knowledge, this study is the first to examine kidney transplant and non-kidney transplant covid-19 positive patients. The originality of this study makes it a strength. However, this study has several limitations. The study was conducted in a single-center, hospital-based setting, and the findings may not be generalizable.
Conclusions and Recommendation
This study revealed that 34.1% of patients had severe COVID-19. The majority of these patients underwent non-kidney transplants. From the study findings, we also concluded that age groups between 40 and 59 years, age 60 years or older, and symptoms, such as chest congestion, shortness of breath, changed or lost sense of taste or smell, and muscle pain, were significant predictors of COVID-19 disease severity. Therefore, efficient treatment should be provided to young adults and older patients by focusing on respiratory difficulties and underlying preexisting medical conditions at St. Paul’s Hospital Millennium Medical College. Additionally, chest congestion, shortness of breath, change or loss of taste or smell, and muscle pain can be used as a pre-indication of disease severity, which is necessary for follow-up and care.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; CKD, Chronic Kidney Disease; COVID-19, Corona Virus Disease-19; HRCT, High-Resolution Computed Tomography; ICU, Intensive Care Unit; KTR, Kidney transplant recipients; SPSS, Statistical Packages for Social Sciences.
Acknowledgment
We would like to thank St. Paul’s Hospital Millennium Medical College, GAMBY Medical College, Kidney Transplantation Center Director and Office of the Research Coordination for giving the opportunity to conduct this study.
Author Contributions
All authors contributed significantly to the work that has been reported, whether it be in ideation, study design, execution, acquisition of the data, analysis, and interpretation, or in all of these areas; all participated in writing, revising, or seriously reviewing the paper; given final approval for the version that will be published; chosen the journal to which the article has been submitted; and agreed to be held accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest with regard to this work.
References
1. World Health Organization. Coronavirus Disease; 2022:1–6. Available from: https://www.who.int/health-topics/coronavirus#tab=tab_1.
2. World Health Organization. The impact of COVID-19 on global health goals; 2021:1–12. Available from: https://www.who.int/news-room/spotlight/the-impact-of-covid-19-on-global-health-goals.
3. Villanego F, Mazuecos A, Pérez‐Flores IM, et al. Predictors of Severe COVID-19 in Kidney Transplant Recipients in the Different Epidemic Waves: Analysis of the Spanish Registry. Am J Transplant. 2021;21:2573–2582.
4. Mohan S, King KL, Husain SA, Schold JD. COVID-19–associated mortality among kidney transplant recipients and candidates in the United States. Clin J Am Soc Nephrol. 2021;16(11):1695–1703.
5. Sagnelli C, Sica A, Gallo M, et al. Renal involvement in COVID-19: focus on kidney transplant sector. Infection. 2021:0123456789. doi:10.1007/s15010-021-01706-6
6. Chothia MY, Barday Z, Nel J, Davids MR. Impact of COVID-19 on access to chronic kidney replacement therapy in the public sector of Western Cape Province, South Africa. South African Med J. 2021;111(11):1030. doi:10.7196/SAMJ.2021.v111i11.16113
7. Kumar N, Rana R, Rana DS, Gupta A, Sachdeva MP. SARS-CoV-2 in Kidney Transplant Recipients: a Systematic Review. Transplantology. 2022;3(1):33–48. doi:10.3390/transplantology3010004
8. Tatapudi RR, Kopparti VR, Poosapati A, Metta S, Gongada AR, Vedulla B. SARS-CoV-2 infection in kidney transplant recipients: a single-centre study of 20 cases from India. Int J Nephrol. 2021;2021:1.
9. Amahazion F. Ethiopia’s Battle against COVID-19; 2021:1–7. Available from: https://diplomatist.com/2021/02/12/ethiopias-battle-against-covid-19/.
10. Ahmed MM, Tedla FM, Leichtman AB, Punch JD. Organ Transplantation in Ethiopia. Transplantation. 2019;103(3):449–451. doi:10.1097/TP.0000000000002551
11. Toapanta N, Torres IB, Sellarés J, Chamoun B, Serón D, Moreso F. Kidney transplantation and COVID-19 renal and patient prognosis. Clin Kidney J. 2021;14(Supplement_1):i21–9. doi:10.1093/ckj/sfab030
12. Caillard S, Chavarot N, Francois H, et al. Is COVID-19 infection more severe in kidney transplant recipients? Am J Transplant. 2021;21(3):1295–1303. doi:10.1111/ajt.16424
13. Monfared A, Akhondzadeh L, Mousazadeh M, et al. COVID-19 in renal transplant recipients and general population: a comparative study of clinical, laboratory, and radiological features, severity, and outcome. Virol J. 2021;18(1):1–14. doi:10.1186/s12985-021-01713-x
14. Hakami A, Badedi M, Elsiddig M, et al. Clinical characteristics and early outcomes of hospitalized COVID-19 patients with end-stage kidney disease in Saudi Arabia. Int J Gen Med. 2021;14:4837–4845. doi:10.2147/IJGM.S327186
15. Jdiaa SS, Mansour R, El Alayli A, Gautam A, Thomas P, Mustafa RA. COVID–19 and chronic kidney disease: an updated overview of reviews. J Nephrol. 2022;35(1):69–85. doi:10.1007/s40620-021-01206-8
16. Ramamurthy P, Kulkarni A, Prabhu D, et al. Study of disease severity and outcomes in covid-19 patients with chronic kidney disease at a tertiary care hospital in South India. Cureus. 2022;14(1):1–7.
17. Gao Y D, Ding M DX, Zhang JJ, et al. Risk factors for severe and critically ill COVID-19 patients: a review. Allergy Eur J Allergy Clin Immunol. 2021;76(2):428–455. doi:10.1111/all.14657
18. Oto OA, Ozturk S, Turgutalp K, et al. Predicting the outcome of COVID-19 infection in kidney transplant recipients. BMC Nephrol. 2021;22(1):1–16. doi:10.1186/s12882-021-02299-w
19. De Sandes-freitas V, Viana A, Cristelli MP, et al. High mortality among kidney transplant recipients diagnosed with coronavirus disease 2019: results from the Brazilian multicenter cohort study. PLoS One. 2021;2021:1–20.
20. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
21. Alkadi MM, Al-Malki HA, Asim M, et al. Kidney transplant recipients infected with coronavirus disease 2019: retrospective Qatar experience. Transplant Proc. 2021;53(8):2438–2446. doi:10.1016/j.transproceed.2021.06.001
22. Tannor EK. Challenges in kidney care in a lower middle income country during the COVID-19 pandemic — the Ghanaian perspective. Kidney Int Reports. 2021;6(8):2014–2016. doi:10.1016/j.ekir.2021.06.019
23. Huluka DK, Etissa EK, Ahmed S, et al. Clinical characteristics and treatment outcomes of COVID-19 Patients at Eka Kotebe General Hospital, Addis Ababa, Ethiopia. Am J Trop Med Hyg. 2022;107(2):252–259. doi:10.4269/ajtmh.21-1270
24. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; 2019.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Willingness to receive the COVID-19 vaccine and associated factors among residents of Southwestern Ethiopia: A cross-sectional study
Jabessa D, Bekele F
Patient Preference and Adherence 2022, 16:1177-1185
Published Date: 3 May 2022
Association of Pre-Existing Comorbidities with Disease Severity Among COVID-19 Patients in Eastern Ethiopia
Merga BT, Ayana GM, Raru TB, Alemu A, Negash B, Bekana M, Birhanu A, Dessie Y
Infection and Drug Resistance 2022, 15:2825-2834
Published Date: 1 June 2022
Baseline Thrombocytopenia and Disease Severity Among COVID-19 Patients, Tibebe Ghion Specialized Hospital COVID-19 Treatment Center, Northwest Ethiopia
Asrie F, Tekle E, Gelaw Y, Dagnew M, Gelaw A, Negash M, Kassa E, Bizuneh S, Wudineh D
Journal of Blood Medicine 2022, 13:315-325
Published Date: 10 June 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Incidence, Bacterial Profile and Predictors of Surgical Site Infection After Cesarean Section in Ethiopia, A Prospective Cohort Study
Mezemir R, Olayemi O, Dessie Y
International Journal of Women's Health 2023, 15:1547-1560
Published Date: 13 October 2023