")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Factors Associated with an Inadequate Volume of Expressed Milk Among Mothers of Preterm and Low Birth Weight Neonates Admitted to Neonatal Intensive Care Units of Government Hospitals in Addis Ababa, Ethiopia
Authors Kedida MH, Asfaw HM , Abebe F
Received 1 July 2022
Accepted for publication 22 December 2022
Published 5 January 2023 Volume 2023:14 Pages 1—10
DOI https://doi.org/10.2147/PHMT.S380807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Misgana Hirpha Kedida, Hussen Mekonnen Asfaw, Fikirtemariam Abebe
School of Nursing and Midwifery, College Health Science, Addis Ababa University (AAU), Addis Ababa, Ethiopia
Correspondence: Hussen Mekonnen Asfaw, Email [email protected]
Background: Around 15 million live newborns are born prematurely each year around the world before 37 weeks. One cause of inadequate nursing is prematurity. The goal of this study was to find parameters linked to an insufficient volume of expressed milk among mothers of preterm and low birth weight neonates at government hospitals in Addis Ababa, Ethiopia.
Methods: An nstitution-based cross-sectional study was conducted on a total of 124 mothers who were available in neonatal intensive care units during the study period in government hospitals that provided such units.
Results: One-third of the responders (33.9%) were unable to express the necessary amount of milk. An inadequate volume of expressed breast milk was significantly associated with a baby’s stable health status (AOR=0.24; CI=0.07– 0.86), the fair (subcritical) health status of the baby (AOR=0.178; CI=0.04– 0.76), worry about the volume of milk (AOR=7.50; CI=3.32– 16.95), and worry about the baby’s health status (AOR=4.63; CI=2.21– 9.70).
Conclusion: According to our findings, 33.9% of mothers were unable to express sufficient amounts of milk. To produce an adequate volume of expressed breast milk, health care workers must address mothers’ psychological issues in the neonatal intensive care units and give all necessary care to prevent neonatal deterioration.
Keywords: inadequate volume, breast milk expression, preterm, low birth weight, neonatal intensive care unit
Background
Globally, among live births annually about 15 million are born prematurely before 37 completed weeks. A direct complication of preterm birth accounts for one million deaths each year, and the preterm is a risk factor for neonatal death.1 Born preterm is one factor for suboptimal breastfeeding. Suboptimal breastfeeding is responsible for 11.6% of under-five deaths globally per year.1
As preterm neonates have poor coordination of sucking and swallowing because of neuronal immaturity and have decreased oromotor tone, generating lower intraoral pressures during sucking they are not able to suck breast.2 This has an impact on early breastfeeding initiation which has a negative impact on increasing milk supply. In such circumstances, early initiation of breast milk expression has a similar role in increasing milk supply.3 When mothers of preterm neonates face inadequate milk supply they start to feed formula milk and for this reason the neonates miss the benefits of breast milk.4
The method of milk expression affects breast milk expression practice. As a study conducted in the UK showed, using double pumping significantly increases milk production when compared to a single pump. Using a double pump was the most significant predictor for milk volume among mothers of preterm infants.5 The use of a double pump has a positive effect on the volume of expressed breast milk for preterm infants in NICU. Low social support is also associated with low breast milk expression during hospitalization.6
Mothers whose infants are admitted to the NICU face more challenges than other mothers in expressing the required milk volume. This is because physical separation from infant can hinder milk supply.7 Proximity to the baby during milk expression is associated with a higher volume of expressed milk.8 Mothers of infants admitted to the neonatal intensive care unit should be sensitively supported to enable them to have skin-to-skin contact with their infants, recognize their infants’ behavior cues, and effectively express breast milk soon after birth.
Expressing the required milk volume is also associated with the physical environment of the NICU and the health status of the neonate. The physical environment of the NICU may not be conducive for pumping, and the infant’s illness may preclude oral feeding for some time. These challenges are most prominent for mothers of preterm infants; as such infants will not be able to breastfeed for up to several weeks until they transition from tube feedings to oral feedings.9
According to a study done in Portugal, mothers who delivered extremely low birth infants are more likely to worry about inadequate milk supply. Worries related to inadequate milk supply hinder milk supply in NICU among mothers’ preterm neonates. Difficulties with breast milk expression and physical separation from infants are factors that hinder milk supply in NICU.7
Initiation of milk expression within one hour following delivery increases milk volume and decreases time to lactogenesis stage II in mothers of VLBW infants. A study done in Florida showed mothers who start milk expression within one hour following delivery expressed more milk than those who start milk expression after one hour following delivery.10 Whereas a study in Finland showed early initiation of breast expression within six hours following delivery increased amount of milk when compared to those who start breast expression after six hours. In another way, more frequent expression per day (more than six times per day) increased the amount of expressed milk.4,11
In Ethiopia, there are limited data on the expressed milk volume required among mothers of preterm and low birth weight neonates admitted to the neonatal intensive care unit. Mothers of these groups face challenges in fulfilling the required volume of expressed breast milk because of different reasons. Thus, this study aimed to assess the parameters linked to an insufficient volume of expressed milk among mothers of preterm and low birth weight neonates at government hospitals in Addis Ababa, Ethiopia.
Methods and Materials
Study Area
The study was conducted in Addis Ababa, the capital city of Ethiopia, and the seat of the charter of the African Union. There are 11 sub-cities in the metropolis, with a population prediction of 3.6 million by 2020 according to the central statistics office.12 There are 13 government hospitals in Addis Ababa, with five under the federal government, six under the Addis Ababa city health bureau, one controlled by the police force, and one owned by the defense army. Ten hospitals in the city currently offer NICU services.
Study Design and Sampling Procedures
An institution-based cross-sectional study was conducted in government hospitals from April 5 to May 15, 2020.
The study included mothers of preterm and LBW infants who were available in the NICU during the study period. The sample size was determined by using single proportion formula ( ) with assumptions of breast milk expression practice being 50%, with a 5% level of significance and margin of error of 5%. Since the total population size was less than 10,000, an adjustment formula (
) with assumptions of breast milk expression practice being 50%, with a 5% level of significance and margin of error of 5%. Since the total population size was less than 10,000, an adjustment formula ( ) and an addition of 10% non-response rate was included. With this assumption, the minimum required sample size was 130. From 11 government hospitals that provide NICU care, four institutions were chosen by lottery. The population proportion sampling approach was used to assign the number of participants to each hospital based on their admission load.
) and an addition of 10% non-response rate was included. With this assumption, the minimum required sample size was 130. From 11 government hospitals that provide NICU care, four institutions were chosen by lottery. The population proportion sampling approach was used to assign the number of participants to each hospital based on their admission load.
Respondents were selected from neonatal intensive care units in hospitals. Each public hospital was first assigned an identification number. A total of four public hospitals were chosen using lottery methods, and sample size allocations were made based on the patient load at each public hospital. Systematic random sampling was employed to choose research participants from several intensive care units. Following that, sample size allocations were calculated based on the patient load at each public hospital. Systematic random sampling was used to choose research participants from selected intensive care units.
All mothers of preterm (<34 weeks) and low birth weight infants admitted to a neonatal intensive care unit during the study period who had difficulty breast feeding were included, whereas mothers of preterm infants who were ≥34 weeks of gestational age, mothers whose infants medically kept nothing by mouth, and mothers whose only option was to feed formula milk were excluded.
Operational Definition
Inadequate Volume of Expressed Milk
If the mother could not express the required amount of milk (the calculated volume of milk-based daily energy requirement using the weight of the baby) during one or more session.
Adequate Required Milk Volume
If the mother is able to express the required amount of milk (the calculated volume of milk-based daily energy requirement using the weight of the baby) during each session.
Data Collection
The data was collected using a standardized questionnaire administered by interviewers. The data-gathering tool was adapted from previous similar studies4,7,10,13,14 and adapted to the local situation. To ensure consistency and accuracy, the data collection instrument was written in English and then translated into the local language (Amharic) by a language expert and then back into English by another individual. Data collectors were chosen based on their past data-gathering experience, qualification relevance, further training in infant care, and ability to communicate in the local language.
Three days of training were provided to familiarize data collectors and supervisors with the instrument and interview methodology. Ethical considerations, participant and interviewer well-being, preventing under-reporting, and maintaining confidentiality were all emphasized. The data-collection procedures were pretested in a neonatal critical care unit outside of the study site with 10% of the sample population. The pretest was used to improve the questionnaire and familiarize data collectors with the technology.
Measurements
Required milk volume was the amount of milk required for the baby over 24 hours calculated based on daily energy requirement, which was calculated using the weight of the baby in calories and ordered on patient chart after convertion to milliliters. It was assessed by asking the mother to fulfill the requirement during each session of breast expression and cross-checked with the record on the baby’s chart. The volume of the milk was measured by syringe leveled in milliliters and this was done by NICU nurses assigned in the unit.
The independent variables such as age, family support, education, care provider support, knowledge, method of pumping, relaxation, lack of privacy, health status of the neonate, stress, worry of the neonatal condition and complications of pregnancy were independent variables of this study.
Care provider support: this was measured by asking the mother whether she has got support on the techniques of breast milk expression during the start of breast milk expression. The response option was “yes” or “no”. She was also asked whether she knows the benefits of colostrum or not. The response options was “yes” or “no”.
Family support: This was assessed by asking the mother if she recives any assistance while excepressing milk, in addition to daily living assistance from her family, from the time she gave birth to the time she was interviweed.
Data Analysis
In EPI Info version 4.6.0.2 program, the pre-coded responses were double entered to verify their consistency and then exported to SPSS for window version 26 for statistical analysis used for percentage, frequency, bivariate and multivariate logistic regression analysis. Variables found to be significant at bivariate level (p <0.05) were selected and included in multiple logistic regression models. Then, logistic regression analysis models were used to measure the odds ratio to estimate association and to control the potential confounding variables with a 95% confidence interval. Using odds ratios compared to the comparison group and 95% confidence levels, the strength and direction of the relationship is presented.
Ethical Considerations
The Institutional Review Board (IRB) of Addis Ababa University’s School of Nursing and Midwifery, College of Health Sciences, approved the study for scientific and ethical integrity, including the verbal informed consent process. The verbal consent was accepted by the IRB of the college. The Addis Ababa Health Bureau’s Public Health Research and Emergency Response Directorate provided ethical approval. The health bureau of the Addis Ababa city government gave its written clearance. Medical directors and relevant unit heads were asked for permission at each health facility. Specific customers who participated in the study provided verbal consent prior to data collection. Each participant received enough information to make an informed decision. Confidentiality was tightly preserved for each piece of information, and the interview was conducted in a secure place. At the completion of the interview, those in need received general information, referrals, and follow-up connections. The researchers would like to confirm that this study followed the Declaration of Helsinki.
Results
Socio-Cultural Characteristics of Study Participants
The response rate in this study was 124 (95.4%). Most of the respondents (76, 60.3%) were in the age group of 18–30 years and the mean age was 29.3 years. For 40% of the respondents, the current pregnancy was their first pregnancy. The educational level of near to half of the respondents was grades 9–12, while about 14% of them had no formal education. Most (96, 77%) of the respondents had ANC follow up during current pregnancy; among these, more than half (54, 56.3%) of them had got advice on BF while only 16 (16.7%) of them had got advice on BME. Almost all (121, 97.6%) of the respondents knew that human breast milk is more important than other milk (formula milk, cow milk) for baby and about two-thirds of the respondents knew the benefits of colostrum (Table 1).
 |
Table 1 Socio-Cultural Characteristics Among Mothers of Preterm and LBW Neonates Admitted to the NICU of Government Hospitals in Addis Ababa, Ethiopia, 2020 (n=12) |
Hand-expression method was used among three-fourths of respondents whereas hands-on pump was the least used method to express milk. About 39 (32%) respondents had got instruction/support on the method of their choice; of these, half of them had got instruction on method of their choice from health care workers whereas only 5 (12.8%) had got instruction from their family. About 27 (22%) respondents expressed for 30 minutes once they started expressing the breast while about two-thirds expressed for less than 30 minutes (Table 1).
Maternal Comfort Data
Most of the respondents expressed milk for their baby in NICU and most (98, 79%) were not comfortable when expressing milk. Among those who were not comfortable when expressing milk, about 31 (32%) said that it was due to the physical environment of the NICU. Near to 85 (70%) respondents were not giving KMC to their baby (Table 2).
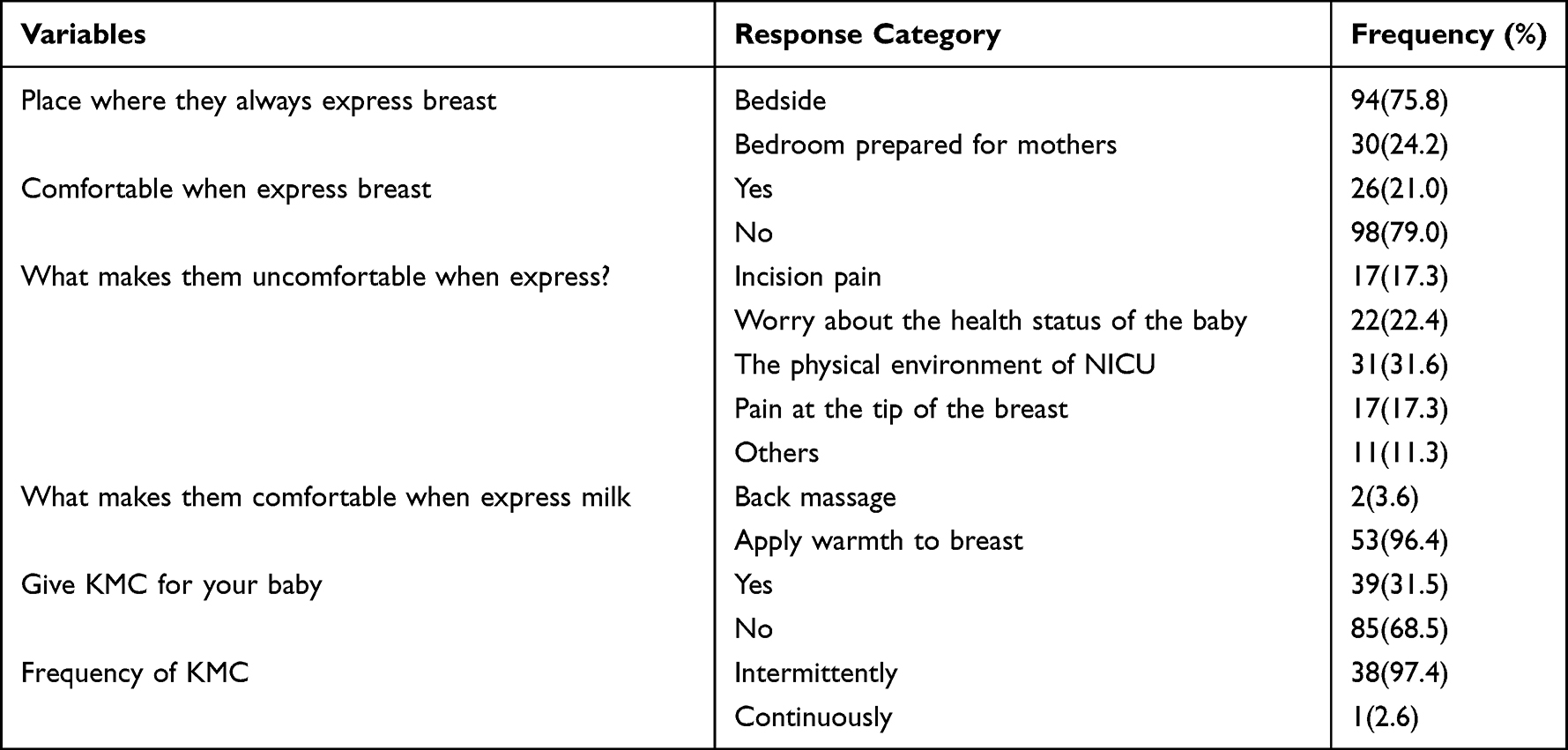 |
Table 2 Maternal Comfort Data Among Mothers of Preterm and LBW Neonates Admitted to NICU of Government Hospitals in Addis Ababa, Ethiopia, 2020 |
Neonatal Factors
The frequency of neonates grouped as very low birth weight and low birth weight based on their birth weight was the same (61, 49.2%), with a mean of 1455.75 grams. The minimum and maximum birth weights were 800 grams and 2250 grams, respectively. Two-thirds of the respondents gave birth to SVD and about 86 (70%) of their neonates were in the late neonatal period. More than half (67, 54.0%) of neonates were in a stable condition whereas 19 (15.3%) were in critical condition. Also, more than half (68, 54.6%) of neonates were able to suck at their mother’s breast (Table 3).
 |
Table 3 Neonatal Characteristics of Preterm and LBW Neonates Admitted to the NICU of Government Hospitals in Addis Ababa, Ethiopia, 2020 (n=124) |
Psychological Factors
More than half (68, 54.8%) of respondents were worried about the amount of milk they express whereas about 68 (55%) respondents were not worried about the health status of their baby. Nearly 60% of respondents were not worried about the prognosis of their baby while about 48 (39%) were (Figure 1).
 |
Figure 1 Psychological data among mothers of preterm and low birth weight neonates admitted to the neonatal intensive care unit of government hospitals in Addis Ababa, Ethiopia, 2020 (n=124). |
Pregnancy-Related Factors
Almost all the mothers gave birth at a gestational age of 28–34 weeks, which can be classified as less or equal to 32 weeks and 32+1 to 34 weeks. About 43 (35%) respondents encountered pregnancy-related complications, the most commonly encountered being pregnancy-induced hypertension (PIH) (Figure 2).
 |
Figure 2 Pregnancy-related data among mothers of preterm and low birth weight neonates admitted to the neonatal intensive care unit of government hospitals in Addis Ababa, Ethiopia, 2020 (n=124). |
All of the respondents were late (6 hours after birth) to initiate breast milk expression and, of these, more than half (71, 57.3%) started milk expression after a period of days. The maximum time to start breast milk expression was 10 days. About 42 (34%) respondents were not able to express the amount of milk requested by the physician. Forty percent of respondents expressed less than eight times per 24 hours (Figure 3).
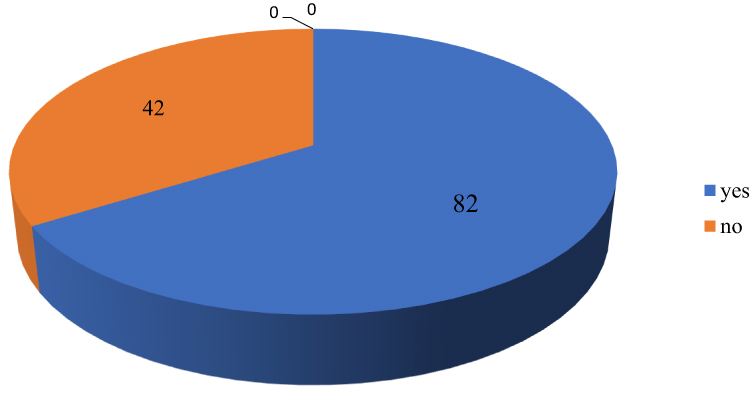 |
Figure 3 Breast milk expression practice among mothers of preterm and low birth weight neonates admitted to the neonatal intensive care unit of government hospitals in Addis Ababa, Ethiopia, 2020 (n=124). |
Factors Associated with Volume of Expressed Breast Milk
Stable health status of the baby (AOR=0.24; CI=0.07 to 0.86), the fair (subcritical) health status of the baby (AOR=0.178; CI=0.04–0.76), worry about volume of milk (AOR=3.51; CI=1.40–8.80) and worry about the health status of the baby (AOR=3.88; CI=1.61–9.35) were significantly associated with an inadequate volume of expressed breast milk. Those mothers whose babies were in a stable condition were less likely to express an inadequate volume of milk than those whose babies were in a critical condition and mothers whose babies were in a subcritical condition were less likely to express an inadequate volume of milk when compared to those mothers whose babies were critical. Mothers who worry about the volume of milk were 7.50 times more likely to express an inadequate volume of milk when compared to those who do not worry about the volume of the breast milk. Mothers who worry about the health status of their baby were 4.63 times more likely to express an inadequate volume of milk than those who do not worry. Frequency of milk expression less than eight times (AOR=5.98; CI=2.60–13.73) was significantly associated with an inadequate volume of expressed milk. Mothers who express milk less than 8 times per 24 hours were 5.98 times more likely to face an inadequate volume of milk when compared to those who express 8–12 times per 24 hours (Table 4).
 |
Table 4 Multivariate Results of Factors Associated with the Volume of Expressed Milk Among Mothers of Preterm and LBW Admitted to the NICU of Government Hospitals in Addis Ababa, Ethiopia, 2020 (n=124) |
Discussion
One-third (33.9%) of the respondents were not able to express the amount of milk required by their baby. Stable health status of baby, subcritical (fair) health status of baby, worry about milk volume, worry about the health status of baby, and frequency of milk expression (less than 8 times per 24 hours) were factors significantly associated with the volume of expressed milk.
The stable health status of the baby and subcritical (fair) health status of the baby were factors identified as helping mothers to express an adequate amount of milk. About 85% percent of mothers whose babies were in stable and subcritical conditions expressed an adequate volume of milk. This is similar to a study conducted in Portugal investigating whether infant wellbeing was a facilitator of adequate milk volume.7 Previous studies revealed that early initiation of breast milk expression, use of a double pump, and proximity to the baby were facilitators of adequate milk volume.5,8,15
Previous studies showed that worries related to inadequate milk supply, difficulty with expressing from the breast, physical separation, cesarean section delivery, and pregnancy-induced hypertension were associated with low volume of expressed breast milk.7,16 In the present study worrying about the amount of milk expressed was 7.5 times more likely to affect milk volume than not worrying. This is similar to a study done in Portugal.7 In addition, the present study showed that worry about the health status of the baby was significantly affected by milk volume. Mothers who worry about the health status of their baby are 4.63 times more likely to express an inadequate amount of milk as per requirement by the physician. Those mothers who expressed milk less than 8 times per 24 hours were 5.98 times more likely to express an inadequate amount of milk as per requirement. This is comparable with the finding of a study done in Finland, which indicated that mothers who expressed more frequently were able to express a greater amount of milk than those who express less frequently,11 even though the cutoff point for frequency is different.
Limitations
The limitations of this study were the cross-sectional nature of the study whereby it is difficult to establish a causal relationship. Also, milk volume was assessed based on the amount of milk required by a baby that was ordered by the physician based on the daily energy/fluid requirement of the baby. The daily requirement of milk is calculated by considering the health status of the baby and only trophic feeding is ordered until full feeding is started. So the present study cannot assess the exact volume of milk the mother can express per day. Further study should be conducted to determine the volume of milk the mothers can express per day.
Conclusion and Recommendation
The present study revealed that only 66.1% of mothers were able to express the required amount of milk for the baby. Worry about the amount of milk, worry about the health status of the baby and inadequate frequency (<8 times per 24 hours) were factors significantly associated with the volume of expressed milk. Stable health status and subcritical (fair) health status of the baby were factors that facilitate an adequate amount of expressed milk. So to promote an adequate amount of expressed breast milk, health care providers have to alleviate the psychological problems of mothers in the NICU and provide all possible care to prevent deterioration of neonates. Further study should be carried out to explore the detailed practice of breast expression by observing during expression and measuring the exact volume.
Acknowledgment
We are very grateful to Addis Ababa University for sponsoring this research. We would like to express our most heartfelt thanks to the women who participated in this study and for sharing such useful information. We would like to thank mothers who participated in this study by sharing important information with us. Lastly, we extend our deepest thanks to data collectors. This is an extract from the thesis entitled “Breast Milk Expression Practice and Factors Affecting It Among Mothers of Preterm and Low Birth Weight Neonates Admitted to Neonatal Intensive Care Unit of Government Hospitals in Addis Ababa, Ethiopia, 2020”, available in Addis Ababa University archive but not published. It is the common work of the three authors of this manuscript; see URI: http://etd.aau.edu.et/handle/ 123456789/24204).17
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or all of these areas; participated in the drafting, revising, or critical review of the article; gave final approval of the version to be published; and agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no financial or non-financial competing interests in this work.
References
1. Blencowe HCS, Chou D, Oestergaard M, et al. Born Too Soon: the global epidemiology of 15 million preterm births. Reprod Health. 2013;10(S2). doi:10.1186/1742-4755-10-S1-S2
2. Lehtonen L. Assessment and optimization of neurobehavioral development in preterm infants.pdf. In: Fanaroff & Martin’s Neonatal-Perinatal Medicine [Internet]. Philadelphia: Elsevier; 2015.
3. Brown CRL DL, Legge A, Bryanton J, Semenic S, Semenic S. Factors influencing the reasons why mothers stop breastfeeding. Can J Public Health. 2014;105(3):e179–e85. doi:10.17269/cjph.105.4244
4. Daljeet KAK, Geetanjli K, Praveen K. Current practices related to feeding Preterm neonates with expressed breast milk: a pilot project. COJ Nurse Health Care. 2018;3:3.
5. Fewtrell MSKK, Ahluwalia JS, Nicholl R, Lucas A, Burton P. Predictors of expressed breast milk volume in mothers expressing milk for their preterm infant. Arch Dis Child Fetal Neonatal Ed. 2016;2016:F502–F506.
6. Fabiyi CRK, Norr K, Yoder JC, Vasa R, White-Traut R, White-Traut R. The association of low social support with breast milk expression in low-income mother–preterm infant dyads. J Hum Lact. 2015;31(3):490–497. doi:10.1177/0890334415586199
7. Elisabete ARM, Mariana A, Conceição N, Susana S, Silva S. Factors influencing parent reports of facilitators and barriers to human milk supply in neonatal intensive care units. J Hum Lact. 2016;32(4):695–703. doi:10.1177/0890334416664071
8. Acuña-M JU, de la Noelia CB, Javier BL, et al. Volume of milk obtained in relation to location and circumstances of expression in mothers of very low birth weight infants. J Hum Lact. 2014;30(1):5.
9. World Health Organization. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services. Geneva: World Health Organization; 2017.
10. Parker LASS, Kelechi T, Kelechi T, Mueller M, Mueller M. Effect of early breast milk expression on milk volume and timing of lactogenesis stage II among mothers of very low birth weight infants: a pilot study. J Perinatol. 2012;32:4. doi:10.1038/jp.2011.78
11. Ikonen R, Paavilainen E, Helminen M, Kaunonen M. Preterm infants’ mothers’ initiation and frequency of breast milk expression and exclusive use of mother’s breast milk in neonatal intensive care units. J Clin Nurs. 2018;27(3–4):e551–e8. doi:10.1111/jocn.14093
12. Centeral Statistical Agency E. Population Projections for Ethiopia 2007–2037. Addis Ababa: Centeral Statistical Agency E; 2013.
13. Paula SSQ, Nikki P, Jenna T, Tucker J. Breast milk expression and maintenance in mothers of very low birth weight infants: supports and barriers. J Hum Lact. 2010;26(4):368–375. doi:10.1177/0890334410371211
14. Becker GESH, Cooney F, Cooney F. Methods of milk expression for lactating women. Cochrane Database Syst Rev. 2016;2016(9). doi:10.1002/14651858.CD006170.pub5
15. Parker LASS, Krueger C. Association of timing of initiation of breast milk expression on milk volume and timing of lactogenesis stage ii among mothers of very low-birth-weight infants. Breast Feed Med. 2015;10(2):84–91.
16. Murase MLN, Morrow AL, Hatsuno M, et al. predictors of low milk volume among mothers who delivered preterm. J Hum Lact. 2014;30(4):10. doi:10.1177/0890334414543951
17. Misgana Hirpha kedida HMA, Fikirte Abebe Fanta. Breast milk expression practice and factors affecting it among mothers of preterm and low birth weight neonates admitted to neonatal intensive care unit of government hospitals in Addis Ababa, Ethiopia; 2020. Available from: http://etd.aau.edu.et/handle/123456789/24204.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.