Back to Journals » ImmunoTargets and Therapy » Volume 8
Factors Associated With Adherence To Immunosuppressive Therapy And Barriers In Asian Kidney Transplant Recipients
Authors Ganjali R ![]() , Ghorban Sabbagh M, Nazemiyan F, Mamdouhi F, Badiee Aval S, Taherzadeh Z, Heshmati Nabavi F
, Ghorban Sabbagh M, Nazemiyan F, Mamdouhi F, Badiee Aval S, Taherzadeh Z, Heshmati Nabavi F ![]() , Golmakani R, Tohidinezhad F
, Golmakani R, Tohidinezhad F ![]() , Eslami S
, Eslami S ![]()
Received 18 April 2019
Accepted for publication 18 September 2019
Published 7 November 2019 Volume 2019:8 Pages 53—62
DOI https://doi.org/10.2147/ITT.S212760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Shurin
Raheleh Ganjali, 1 Mahin Ghorban Sabbagh, 2, 3 Fatemeh Nazemiyan, 2, 4 Fereshteh Mamdouhi, 2, 3 Shapour Badiee Aval, 5 Zhila Taherzadeh, 6 Fatemeh Heshmati Nabavi, 7 Reza Golmakani, 8 Fariba Tohidinezhad, 1 Saeid Eslami 1, 9, 10
1Department of Medical Informatics, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 2Kidney Transplantation Complications Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 3Department of Nephrology, Montaseriyeh Organ Transplantation Hospital, Mashhad University of Medical Sciences, Mashhad, Iran; 4Department of Nephrology, Ghaem Hospital, Mashhad University of Medical Sciences, Mashhad, Iran; 5Complementary Medicine Research Center, Faculty of Traditional Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 6Neurogenic Inflammation Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 7School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran; 8Department of Emergency Medicine, Doctor Shariati Hospital, Mashhad University of Medical Sciences, Mashhad, Iran; 9Pharmaceutical Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 10Department of Medical Informatics, University of Amsterdam, Amsterdam, The Netherlands
Correspondence: Saeid Eslami
Department of Medical Informatics, Mashhad University of Medical Sciences, Azadi Street, Mashhad, Iran
Tel +98 513 800 2429
Fax +98 513 800 2445
Email [email protected]
Background: Medication non-adherence is the major risk factor for rejection episodes. The aim of this study was to determine the risk factors associated with adherence to immunosuppressive regimen and its barriers among kidney transplant (KT) recipients.
Methods: A cross-sectional study was performed in two outpatient post-transplant clinics in Mashhad, northeast of Iran. All patients who attended the clinics from August to October 2017 were included. Patients’s knowledge, adherence to immunosuppressive regimen, and quality of life were measured using the Kidney Transplant Understanding Tool, Basel Assessment of Adherence to Immunosuppressive Medications Scale (BAASIS), and SF-12V2 questionnaire, respectively. The barriers in adhering immunosuppressive regimen were investigated by Immunosuppressive Therapy Barriers Scale. Logistic regression was used to screen the significant risk factors of medication non-adherence.
Results: In this study, 244 KT recipients were included with a mean age of 39.6± 12.5 years. Based on the BAASIS score, 111 (45.5%) patients were adherent to immunosuppressive regimen. Female patients were more likely to be adherent (OR=0.48, p< 0.01). The patients with higher level of quality of life were more likely to follow immunosuppressive medications (OR=1.078, p< 0.05). The main barriers were as follows: concurrent use of many immunosuppressants, lack of knowledge about the usefulness of immunosuppressive medications, confusion in medication taking, and difficulty in remembering medication taking.
Conclusion: More than half of the KT recipients were non-adherence to immunosuppressive regimen. These findings highlight the need for designing interventions in order to reduce or eliminate these barriers and consequently increase medication adherence among KT recipients.
Keywords: immunosuppressive regimen, medication adherence, quality of life, kidney transplantation
Corrigendum for this paper has been published
Background
Kidney transplantation (KT) is acknowledged as the major advance in renal replacement therapy for patients with irreversible kidney failure. In recent years, patients’ survival rates have improved with the improvements in surgical operation techniques as well as treatment with more effective immunosuppressants. Despite the advances in immunosuppressive therapy, medication-taking behaviors remain as a major challenge in the therapeutic chain. Patient and graft survival rates are greatly affected by the patients’ adherence to medication regimen (esp. immunosuppressants).1 The WHO defines medication adherence as a match between patient’s behavior and the medical team’s recommendations.2 Medication non-adherence is the major risk factor for rejection episodes.3 Non-adherence to immunosuppressive medication multiplies the rejection episodes up to 7 times higher.4 Non-adherence to immunosuppressive medications has been the main focus of transplant communities in recent years. The actual prevalence of non-adherence rate in different communities varies between 0% and 68 %.3,5,6 Irregular intake of immunosuppressants by KT recipients not only results in poor short- and long-term graft outcomes, but also can be considered as a reason for decreased productivity and quality of life as well as increased treatment costs.7–9 Because the risk factors of medication non-adherence differ between societies, health care organizations face challenges to design effective interventions aiming to increase patients’ knowledge about immunosuppressant adherence. Iran is a developing country with different socioeconomic population groups. It is the most active country in the field of KT in the Middle East Society for Organ Transplantation region.10 Over 65% of the KT costs is due to immunosuppressive non-adherence. Rejection is one of the most important post-transplant complications which is severely associated with patients adherence to immunosuppressive regimen. Identifying the related factors and barriers can assist health care providers to remove barriers and increase immunosuppressive adherence, as well as reducing costs associated with graft rejection. This article is part of an information technology-based intervention, aiming to increase adherence to immunosuppressive medications by means of presenting regular structured education material to KT recipients. Therefore, the aims of this study were 1) to estimate the prevalence rate of non-adherence to immunosuppressive regimen among KT recipients and 2) to determine the factors associated with adherence to immunosuppressive medications.
Materials And Methods
Setting And Participants
A cross-sectional study was performed in two outpatient post-transplant clinics from August 2017 to October 2017 in Mashhad, northeast of Iran. One of the outpatient clinics belonged to the Montaserieh Transplant Center. This is the only transplant center in the northeast of Iran. The other clinic belonged to a nephrologist, which provides follow-up services to a large number of KT recipients. The inclusion criteria were as follows: 1) history of deceased or living donor KT, 2) having 18 years of age or more, and 3) having acceptable graft function (did not need any types of dialysis at the time of enrollment). The patients who refused to continue participation in the study were excluded. This study was approved by the Institutional Ethics Committee of the Mashhad University of Medical Sciences (Number: 951645, IR.MUMS.fm.REC.1396.160).
Data Collection
A total of 732 KT recipients lived in Mashhad in July 2017. To estimate the sample size, Morgan table was applied. Before entering the clinic, patient’s information was checked through the electronic scheduling system in order to determine whether the patient meets the inclusion criteria. Eligible volunteers signed the informed consent after receiving verbal and written explanation. The patients were asked to complete the questionnaires. If the patient had low literacy level, a trained research assistant was asked to read the questionnaires’s items and record the patient’s responses. The average response time for the questions was between 20 and 30 mins. Subsequently, a series of demographic and clinical variables were extracted from the medical records. In order to assure participants about the confidentiality of their data, information was recorded without their first and last name.
Instruments
Knowledge
The Kidney Transplant Understanding Tool (K-TUT) was used to evaluate patients’ knowledge about the post-KT therapeutic recommendations.11 The K-TUT is a proper instrument to measure the knowledge of both KT recipients and the patients suffering from a chronic kidney disease and waiting to receive a graft. At first, this questionnaire was translated to the target language (Persian) by two experts (forward translation) and then retranslated to its original language by another expert (backward translation). Content validity of the final questionnaire was calculated by running a Delphi session, in which 4 nephrologists and 4 coordinator nurses took part. Following content, validity indices were computed: content validity index (CVI) and content validity ratio (CVR).

where  is the number of experts who gave a score of 3 or 4 to each item’s relevancy and n is the total number of experts.
is the number of experts who gave a score of 3 or 4 to each item’s relevancy and n is the total number of experts.

where  is the number of experts who stated that the item is “necessary” and n is the total number of experts.
is the number of experts who stated that the item is “necessary” and n is the total number of experts.
If the CVI value of an item was less than 0.78, it was considered as invalid and was removed consequently. The questionnaire’s internal consistency was evaluated using test–retest method. Based on this method, the questionnaire was given to 25 patients two times with 1 week interval. To test the reliability of the internal consistency, Cronbach’s alpha coefficient estimation was used and alpha equal to or greater than 0.7 was considered satisfactory.
Adherence to immunosuppressive medications is evaluated using different self-report instruments. The Basel Assessment of Adherence to Immunosuppressive Medications Scale (BAASIS)12 is a proper self-report instrument consisting of four items which assesses adherence to immunosuppressive medications over a period of 4 weeks. This instrument assesses four dimensions, including missing a dose, continuous missing of several doses, deviation from the exact medication-taking time for more than 2 hrs, and reducing the amount of each dose. This instrument uses 6-point Likert rating scale (0=never, 1=once a month, 2=every 2 weeks, 3=every week, 4=more than once a week, and 5= very day). Patients selecting “never” are considered as adherent patients, and those selecting other choices are considered as non-adherent patients. This instrument was translated into Persian by two experts using the forward–backward translation method. Subsequently, the translated version was compared with the original one by the third expert, and discrepancies between the two experts were removed in order to prepare the final draft approved by all the translators. Cronbach’s alpha was used to determine the internal consistency. The value greater than or equal to 0.78 was interpreted as acceptable.
Quality Of Life
In this study, SF-12V2 questionnaire was used to evaluate patients’ quality of life. The Persian version of this questionnaire was validated by Montazeri et al (2011).13 This questionnaire consists of 12 items which provides a general understanding of patient’s health, physical performance, physical health, emotional problems, physical pain, social function, vitality, vital energy, and mental health which results to a maximum score of 48.
Re-Hospitalization
Previous studies indicated that low adherence to immunosuppressive medications was associated with higher re-hospitalization rate.14 The final diagnosis of the cause of hospital readmissions was determined by the nephrologists and coded into the hospital information system of the Montaserieh Transplant Center. The definitions of these readmission etiologies were determined by consensus of the research team. Readmission defined as times of hospital readmission after kidney transplant causes graft dysfunction or infection. Infection was defined as the body temperature greater than 38°C due to any types of viral, bacterial, or fungal infections when the patient required in-hospital care. Infection was defined as the body temperature greater than 38°C due to any types of viral, bacterial, or fungal infections when the patient required in-hospital care. Moreover, increased creatinine was defined as 30% increase of serum creatinine in compare with the previous level and the urine protein greater than 500 (mg/day) was defined as proteinuria. The frequency of patient’s hospitalization due to infection increased creatinine and proteinuria was fetched from the hospital information system using the International Classification of Diseases and health problem 10th revision (ICD-10).
Barriers Of Adherence To Immunosuppressive
The barriers of adherence to immunosuppressive medications were determined using the Immunosuppressive Therapy Barriers Scale (ITBS).10 This instrument included 13 items, among which the first 8 items were categorized as unintentional, and the next 5 items were categorized as intentional. The responses were anchored on a 6-point Likert scale (1: strongly disagree to 5: strongly agree). The overall score ranges between 13 and 65, with higher scores indicating more barriers for medication adherence. This instrument was also translated using the forward–backward translation method by qualified translators. Cronbach’s alpha was used to determine the internal consistency. The value greater than or equal to 0.85 was interpreted as acceptable.
Statistical Analysis
Descriptive statistics were used to report quantitative variables. Ranking variables were summed up by proportions. Because a large number of variables were measured (increasing the Type 1 error), the first step involves selecting the variables associated with using different tests. The univariate analysis was performed using the independent-samples t-test, Mann–Whitney U-test, and Chi-square or Fisher exact tests.
The multi-variate analysis was performed by entering the variables with p<0.2 into a binary logistic regression model. Data were analyzed using SPSS version 23 (IBM SPSS Inc., Armonk, NY, USA).
Results
Analysis Of Questionnaires
K-TUT: A total of 12 items were removed due to low CVI and CVR values. The final questionnaire consists of 9 true/false and 13 multiple-choice questions (more than one correct answer). One score was given to each correct answer. The maximum knowledge score was 57. Higher knowledge scores indicated more KT knowledge. The Cronbach’s alpha of the test–retest reliability was 0.85 (p<0.05).
BAASIS: Overall internal reliability (Cronbach’s alpha=0.78, p<0.05) was acceptable.
ITBS: Overall internal reliability (Cronbach’s alpha=0.79, p<0.05) was acceptable.
Analysis Of Survey
A total of 244 KT recipients were included in this study with a mean age of 39.6±12.5 years (18–75). Participants’ demographics are described in Table 1. A total of 43% (106) of participants were female and 72% (175) were married. Only 16% (40) had academic education level. About 60% of participants received their graft from deceased donors. The mean time since transplantation was 59.1±54 months. About 90% underwent hemodialysis before transplantation (Table 1). The average number of hospitalizations due to complications (eg, infection, the presence of protein in the urine, and the increased creatinine) was 1.3±2 and the mean duration of post-transplant hospitalizations was 13±24 days. Moreover, the mean of blood serum creatinine of the participants was 1.8±1.1 (mg/dL).
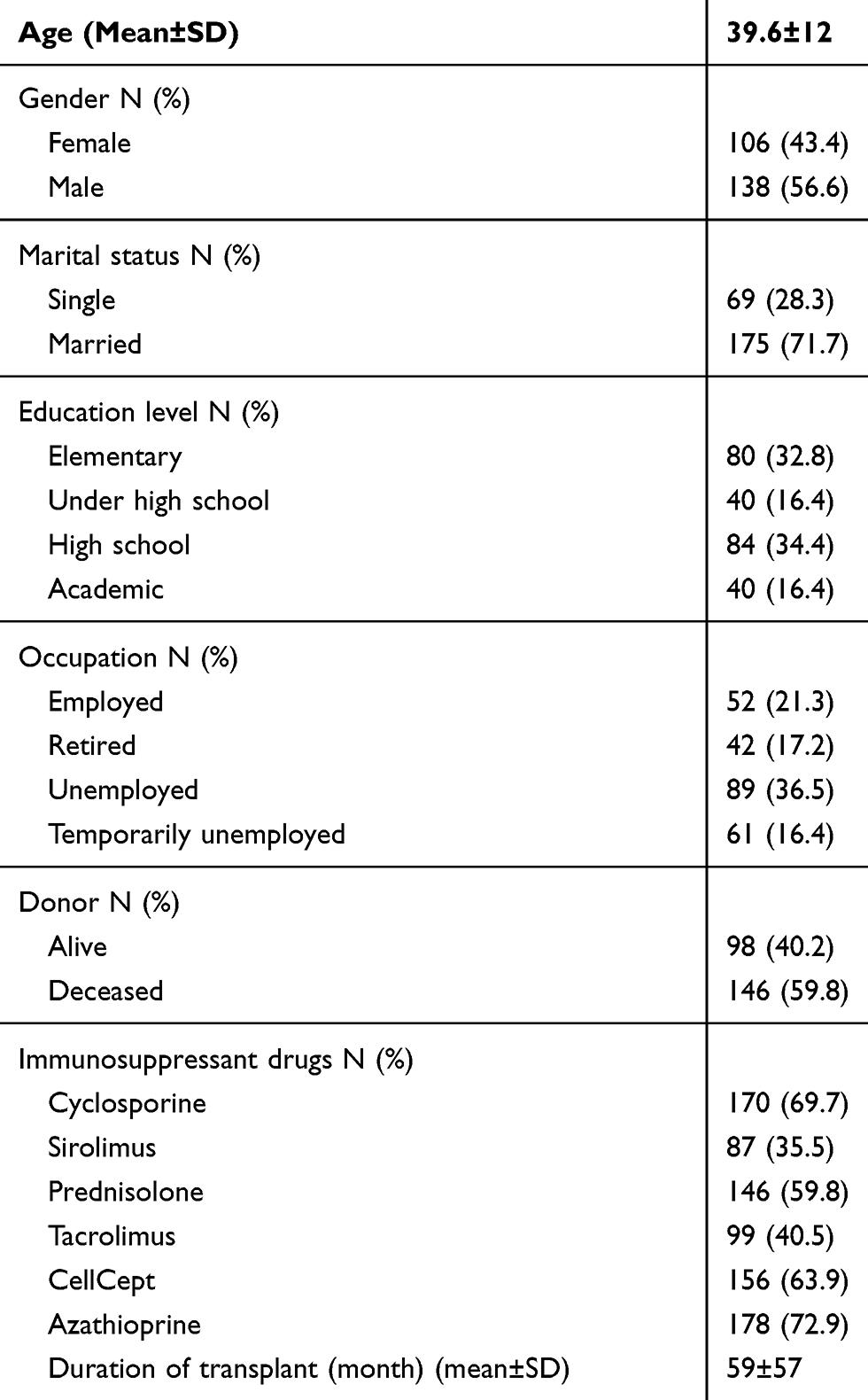 |
Table 1 Demographics Of Participants (n=244) |
About 54.5% (133) of participants were non-adherent to immunosuppressive medications. About 19.5% (26) of the non-adherent participants did not take their prescribed medication at least once during the past 4 weeks. About 10.5% (14) of patients forgot to take several continuous doses of their immunosuppressive medications at least one time during the past 4 weeks. Also, 40% (54) of the non-adherent participants had taken their immunosuppressive medications with a 2-hr delay from the exact consumption time at least one time during the past 4 weeks. Finally, 11% (14) of these patients reduced their immunosuppressive medications at least one time during the previous 4 weeks (Table 2).
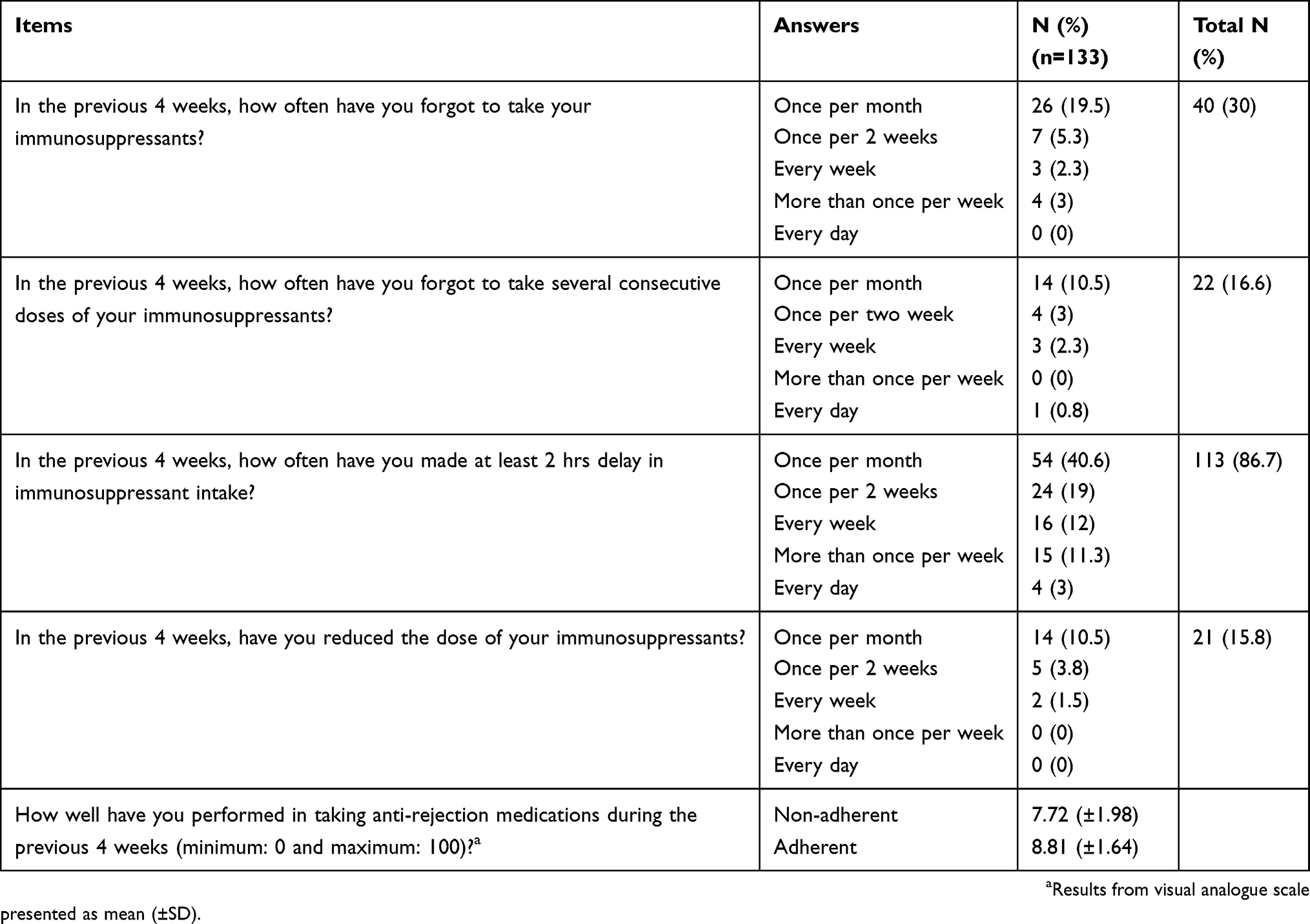 |
Table 2 Non-Adherence Measured Using BAASIS (n=133) |
The mean transplant knowledge score was 41±6.3 (of 57). In this study, 55% (135) of cases had a score of 50% to 75%, and 41% (99) of cases obtained 75% to 99% of the total score. The mean score of quality of life was 31±6. The majority of the participants (N=152, 62%) had a moderate level of quality of life (Level 2), and only 24% (N=58) had a good quality of life (Level 3). Demographic variables such as age and marital status had no significant relationship with medication adherence. Moreover, transplant knowledge, the mean number of hospitalization times, duration of hospitalization due to infection, increased creatinine, and proteinuria were not significantly associated with adherence to immunosuppressive medications. The variables of clinical outcomes such as the type of donor, transplant rejection rate, transplant duration, the dialysis duration, and the level of serum creatinine had no significant relationship with adherence to immunosuppressive medications. Gender, education level, occupation, and quality of life were significantly different between adherent and non-adherent patients (Table 3).
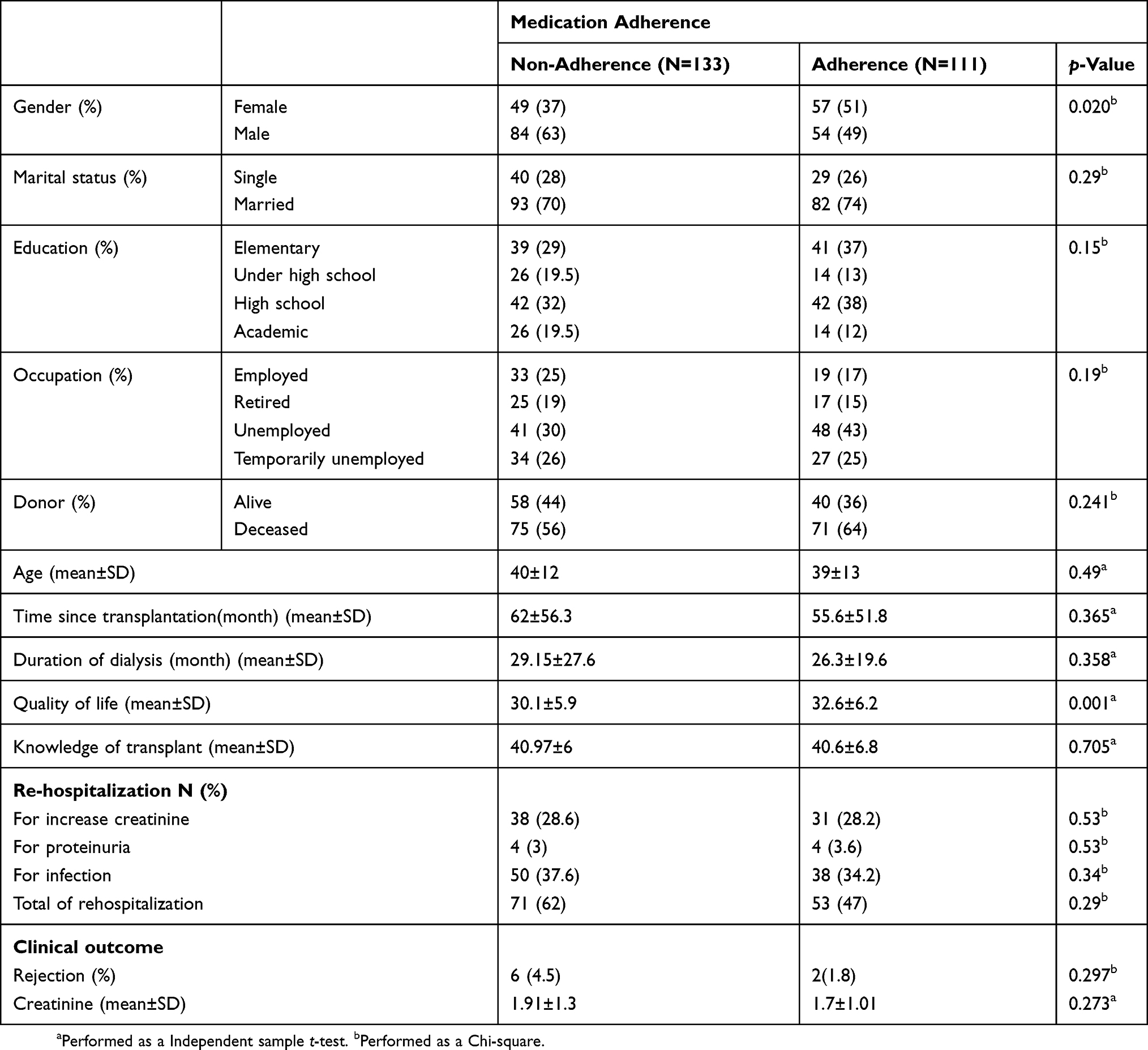 |
Table 3 Comparing Input Variable In Medication Non-Adherent And Adherent Patient Among Kidney Transplant Recipients (n=244) |
Logistic regression analysis was used to describe the relationship of four independent variables, including gender, education level, occupation, and quality of life on adherence to immunosuppressive medications in kidney transplant recipients. Among the aforementioned independent variables, quality of life had a significant relationship with medication adherence (OR=1.078, CI=1.03 to 1.12, p<0.05). Kidney transplant recipients with higher level of quality of life were more likely to follow immunosuppressive medications. As a matter of fact, a one unit increase in quality of life score was associated with an odds ratio of 1.07 (CI=1.03 to 1.12) for medication adherence.
Gender evaluation in kidney transplant patients had a significant relationship with medication adherence. In fact, women were two times more likely to be adherent than the men (OR=0.48, CI=0.28 to 0.83, p<0.01).
Barriers To Immunosuppressant Adherence
The ITBS mean score was 42±4.5. The mean score of unintentional and intentional items were 28.9±4 and 13±2.5, respectively (Figure 1).
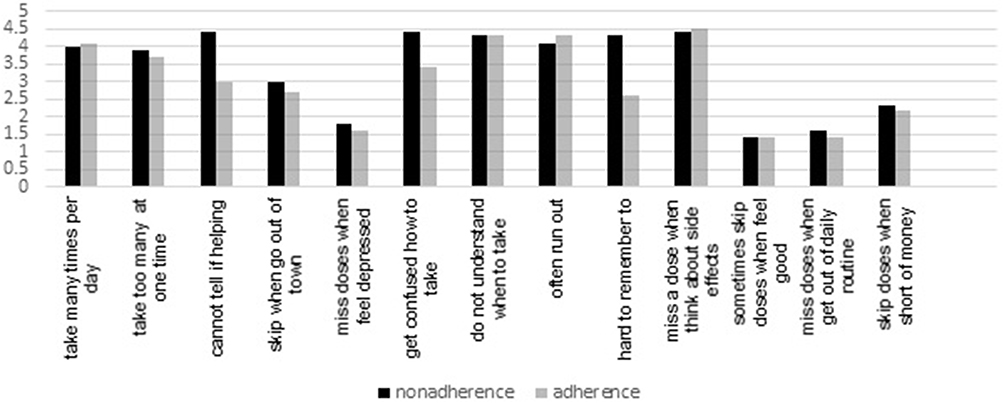 |
Figure 1 Barriers to medication adherence: comparison of ITBS mean scores between adherent and non-adherent patient. |
A total of 4 of 13 individual items in ITBS had a significant relationship with medication adherence based on BAASIS (Table 4). The relevant factors in this study were the concurrent use of many immunosuppressants, lack of knowledge about the usefulness of immunosuppressive medications, confusion about medication taking, and difficulty in remembering the medication taking. The remaining 9 items had no relation with medication adherence. Among four items associated with medication adherence, three were associated with unintentional items, and one was associated with intentional items.
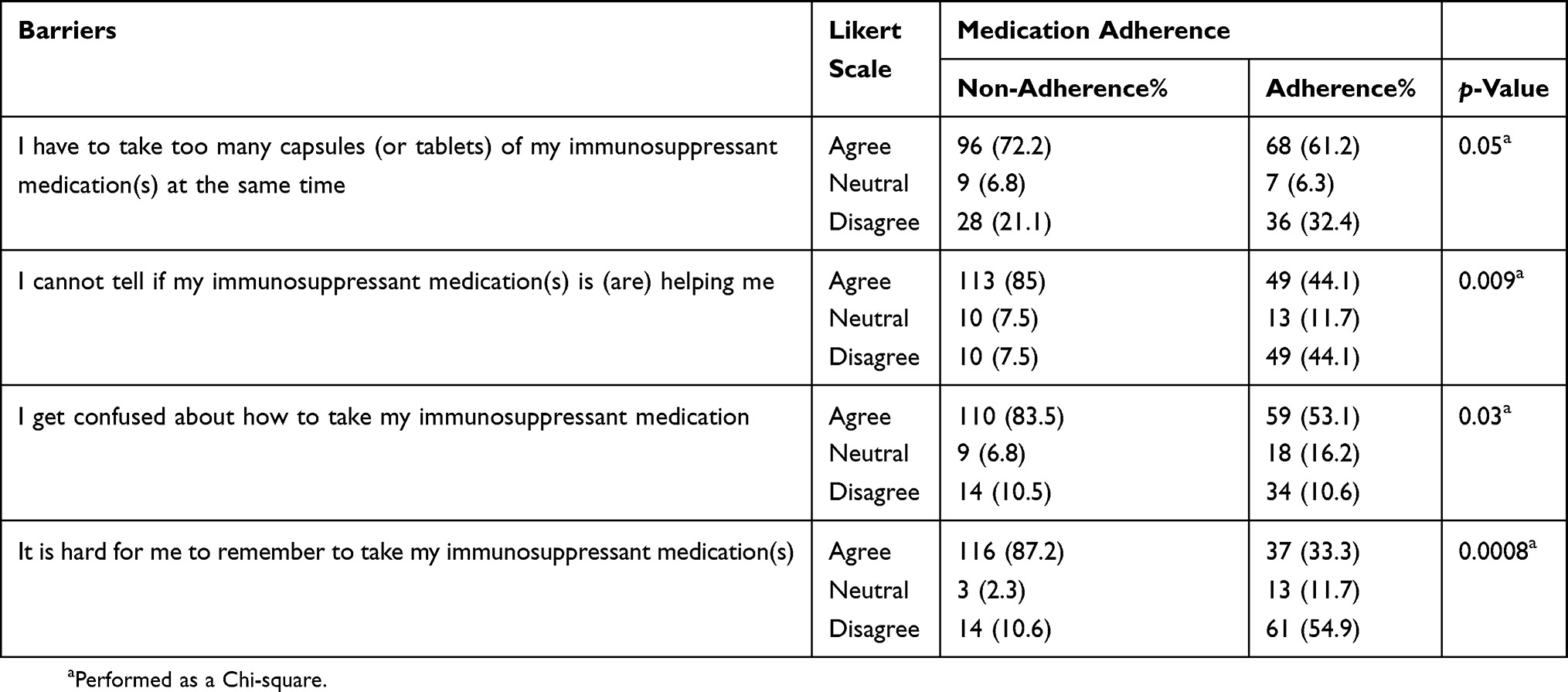 |
Table 4 Significant Barriers To Immunosuppressant Adherence |
Discussion
The aim of the present work was to conduct a cross-sectional study to determine the prevalence rate of non-adherence to immunosuppressive regimen and its barriers among the KT recipients. About 54.5% (113) of the participants were non-adherent to immunosuppressants. Quality of life and gender had significant relationship with medication adherence. Medication adherence rate in this sample was in accordance with what has been reported in the previous studies. Similar studies showed that medication non-adherence rate varied between 0% and 68%.3,5,6 High medication non-adherence rate in the present study may be due to the fact that medication non-adherence is underestimated when using a self-report approach.15 Majority of the patients were non-adherent, and 113 (86.7%) reported delays in taking their immunosuppressants. To reduce graft rejection episodes, it has been proposed that adherence to immunosuppressive medications should be over 97%, and only one dose per month could be missed out.15 Missed doses need more attention than the delayed doses.16 Therefore, designing interventions on missed doses is more likely to improve clinical outcomes. There are many barriers to medication non-adherence.17
In our study, gender was found to have a significant relationship with immunosuppressive medication adherence, and women showed a higher level of adherence than men. However, previous studies showed that medication adherence is not significantly correlated with gender.18–20 In similar studies, the medication adherence was significantly higher in men.21,22 In the current study, women had more tendency than men to maintain health, which can be attributed to the culture, fear of losing their family, and rejection.
Other studies showed that there is a significant inverse relationship between quality of life and medication adherence.23,24 On the other hand, the present study showed that a significant direct relationship existed between quality of life and medication adherence.
Previous studies also showed that there is no clear difference between the intentional and unintentional risk factors of medication adherence.3 According to the results of the present study, the main barriers associated with medication non-adherence were as follows: concurrent use of many immunosuppressants, lack of knowledge about the usefulness of immunosuppressive medications, confusion in medication taking, and difficulty in remembering medication taking. Studies have also shown that medication non-adherence is unintentional when it is uncontrollable, and this is mostly due to incompetency in remembering.25 In a cross-sectional study, about 62% of patients basically accepted forgetfulness as an unintentional reason.18,26,27 In this study, one of the factors associated with non-adherence was forgetfulness. In fact, efforts for reducing non-adherence level must be accompanied by strategies to reduce or eliminate forgetfulness. The use of reminders and interventional technologies to reduce this factor seems to be effective. Other studies concluded that medication non-adherence is closely related to therapeutic factors such as the complexity of the ordered regimen.16,22,26 This study also identified the complexity of prescribed therapeutic doses and the simultaneous use of multiple medications as factors associated with non-adherence. Reducing the number of daily doses effectively reduces the unintentional factors of medication non-adherence.
Adequate knowledge about the benefits of immunosuppressive medications for transplantation may be correlated with medication adherence.28 In this study, the lack of knowledge about the usefulness of immunosuppressive medications was significantly related to the medication non-adherence. The mean patients’ knowledge on therapeutic recommendations was moderate. Thus, there is a need for educational interventions aiming to improve the attitudes and knowledge of individuals. Patient education has the potential to improve outcomes over the long term.29
In our study, it was shown that there was no relationship between medication non-adherence and transplant complications (ie, readmission, and duration of post-transplant hospitalizations). It is necessary to design other studies using other methods for investigating the relationship between non-adherence and rehospitalization rates due to infection complications and acute transplant rejection. Factors related to health system can affect post-transplant medication adherence.16 Non-adherence factors related to health care system were as follows: inadequate health services, non-reimbursement by health insurance organizations, lack of knowledge and training of caregivers, short and limited counseling, and inadequate capacity to instruct and educate the patients.30,31
The most important aspect of this study was sampling from two specialized centers, having the most number of outpatient records of transplant recipients in northeast of Iran. The use of self-report measurements is considered as a strength due to its low cost and ease of use by the patients. Moreover, the large sample size and collection of a large number of variables are the strength of this study.
The first limitation of the present study was the use of a self-report approach in measuring medication adherence. Self-report methods may underestimate the actual rate of medication non-adherence, because the patient intentionally shows himself or herself in the context of medication adherence, and as such may conceal the reality. Second, the design of this study as a cross-sectional study (lack of follow-up) would be an obstacle for analyzing long-term medication non-adherence and outcomes. Third, it is very likely that the patients attending the clinics via an electronic scheduling system have relatively higher medication adherence due to higher socioeconomic level. This bias in sample selection may lead to overestimation of the medication adherence. On the other hand, since Montaserieh Transplant Center is the only state-owned center covering transplant patients, it is more likely that patients with lower socioeconomic levels are admitted to the center. This might adjust the rate of adherence to overestimation.
Based on the findings of the current study, it is suggested that 1) using the identified barriers, interventions can be designed to improve medication adherence among KT recipients (eg, reminders) 2) an effective remote monitoring program can enhance patient medication adherence, improve therapeutic outcomes, and decrease the waste of health care resources, and 3) use of interactive voice response systems and mobile health systems, can potentially improve the medication adherence.
Conclusion
More than half of the kidney transplant recipients were non-adherent to immunosuppressants. Factors influencing adherence to immunosuppressive medications were gender, quality of life, and factors related to medication non-adherence were concurrent use of many immunosuppressants, lack of knowledge about the usefulness of immunosuppressive medications, confusion about medication taking, and difficulty in remembering medication taking. Explored factors and barriers can help health care providers to overcome barriers and reduce health care costs associated with graft rejection.
Abbreviations
IT, information technology; K-TUT, Kidney Transplant Understanding Tool; BAASIS, Basel Assessment of Adherence to Immunosuppressive Medications Scale; ITBS, Immunosuppressive Therapy Barriers Scale; LOS, length of stay.
Ethics Approval And Consent To Participate
This study was approved by the Ethics Committee of Mashhad University of Medical Sciences and Medical School (Grant Number 951645, IR.MUMS.fm.REC.1396.160). The study was carried out in accordance with the principles of the Declaration of Helsinki.
Data Availability
The data used to support the findings of this study are restricted by the Ethics Committee of Mashhad University of Medical Sciences in order to protect patient privacy. Data are available from Saeid Eslami (corresponding author; [email protected]) for researchers who meet the criteria for access to confidential data.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Gorevski E, Succop P, Sachdeva J, et al. Is there an association between immunosuppressant therapy medication adherence and depression, quality of life, and personality traits in the kidney and liver transplant population? Patient Prefer Adherence. 2013;7:301–307. doi:10.2147/PPA.S34945
2. Hedayati P, Shahgholian N, Ghadami A. Nonadherence behaviors and some related factors in kidney transplant recipients. Iran J Nurs Midwifery Res. 2017;22(2):97–101. doi:10.4103/ijnmr.IJNMR_220_15
3. Griva K, Davenport A, Harrison M, Newman SP. Non-adherence to immunosuppressive medications in kidney transplantation: intent vs. forgetfulness and clinical markers of medication intake. Ann Behav Med. 2012;44(1):85–93. doi:10.1007/s12160-012-9359-4
4. Mahdavi-Mazdeh M, Heidary-Rouchi A, Aghighi M, Rajolani H. Organ and tissue transplantation in Iran. Saudi J Kidney Dis Transpl. 2008;19(1):127.
5. Dew MA, DiMartini AF, De Vito Dabbs A, et al. Rates and risk factors for nonadherence to the medical regimen after adult solid organ transplantation. Transplantation. 2007;83(7):858–873. doi:10.1097/01.tp.0000258599.65257.a6
6. Moreso F, Torres IB, Costa-Requena G, Serón D. Nonadherence to immunosuppression: challenges and solutions. Transplant Res Risk Manage. 2015;7:27–34. doi:10.2147/TRRM.S50796
7. Chisholm MA, Lance CE, Williamson GM, Mulloy LL. Development and validation of the immunosuppressant therapy adherence instrument (ITAS). Patient Educ Couns. 2005;59(1):13–20. doi:10.1016/j.pec.2004.09.003
8. Constantiner M, Cukor D. Barriers to immunosuppressive medication adherence in high-risk adult renal transplant recipients. Dial Transplant. 2011;40(2):60–66. doi:10.1002/dat.20536
9. De Bleser L, Matteson M, Dobbels F, Russell C, De Geest S. Interventions to improve medication‐adherence after transplantation: a systematic review. Transplant Int. 2009;22(8):780–797. doi:10.1111/j.1432-2277.2009.00881.x
10. Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar A-R. Design and implementation content validity study: development of an instrument for measuring patient-centered communication. J Caring Sci. 2015;4(2):165. doi:10.15171/jcs.2015.017
11. Rosaasen N, Taylor J, Blackburn D, Mainra R, Shoker A, Mansell H. Development and validation of the kidney transplant understanding tool (K-TUT). Transplant Direct. 2017;3(3):e132. doi:10.1097/TXD.0000000000000647
12. de Oliveira Marsicano E, Da Silva Fernandes N, Colugnati F, et al. Transcultural adaptation and initial validation of Brazilian-Portuguese version of the Basel assessment of adherence to immunosuppressive medications scale (BAASIS) in kidney transplants. BMC Nephrol. 2013;14(1):108. doi:10.1186/1471-2369-14-108
13. Montazeri A, Vahdaninia M, Mousavi SJ, Asadi-Lari M, Omidvari S, Tavousi M. The 12-item medical outcomes study short form health survey version 2.0 (SF-12v2): a population-based validation study from Tehran, Iran. Health Qual Life Outcomes. 2011;9(1):12. doi:10.1186/1477-7525-9-40
14. Lee SY, Chu SH, Oh EG, Huh KH. Low adherence to immunosuppressants is associated with symptom experience among kidney transplant recipients. Transplant Proc. 2015;47(9):2707–2711. doi:10.1016/j.transproceed.2015.09.056
15. Cossart AR, Staatz CE, Campbell SB, Isbel NM, Cottrell WN. Investigating barriers to immunosuppressant medication adherence in renal transplant patients. Nephrology. 2017;24(1):102–110.
16. Greenstein S, Siegal B. Compliance and noncompliance in patients with a functioning renal transplant: a multicenter study. Transplantation. 1998;66(12):1718–1726. doi:10.1097/00007890-199812270-00026
17. Chisholm-Burns MA, Spivey CA, Tolley EA, Kaplan EK. Medication therapy management and adherence among US renal transplant recipients. Patient Prefer Adherence. 2016;10:703–709. doi:10.2147/PPA.S104646
18. Chisholm-Burns M, Pinsky B, Parker G, et al. Factors related to immunosuppressant medication adherence in renal transplant recipients. Clin Transplant. 2012;26(5):706–713. doi:10.1111/j.1399-0012.2011.01589.x
19. Massey EK, Tielen M, Laging M, et al. The role of goal cognitions, illness perceptions and treatment beliefs in self-reported adherence after kidney transplantation: a cohort study. J Psychosom Res. 2013;75(3):229–234. doi:10.1016/j.jpsychores.2013.07.006
20. Russell CL, Ashbaugh C, Peace L, et al. Time‐in‐a‐bottle (TIAB): a longitudinal, correlational study of patterns, potential predictors, and outcomes of immunosuppressive medication adherence in adult kidney transplant recipients. Clin Transplant. 2013;27(5). doi:10.1111/ctr.12122.
21. Chisholm-Burns MA, Spivey CA, Wilks SE. Social support and immunosuppressant therapy adherence among adult renal transplant recipients. Clin Transplant. 2010;24(3):312–320. doi:10.1111/j.1399-0012.2009.01060.x
22. Obi Y, Ichimaru N, Kato T, et al. A single daily dose enhances the adherence to immunosuppressive treatment in kidney transplant recipients: a cross-sectional study. Clin Exp Nephrol. 2013;17(2):310–315. doi:10.1007/s10157-012-0713-4
23. Fredericks EM, Magee JC, Opipari‐Arrigan L, Shieck V, Well A, Lopez MJ. Adherence and health‐related quality of life in adolescent liver transplant recipients. Pediatr Transplant. 2008;12(3):289–299. doi:10.1111/j.1399-3046.2008.00901.x
24. Hamedan MS, Aliha JM. Relationship between immunosuppressive medications adherence and quality of life and some patient factors in renal transplant patients in Iran. Glob J Health Sci. 2014;6(4):205.
25. Schäfer‐Keller P, Steiger J, Bock A, Denhaerynck K, De Geest S. Diagnostic accuracy of measurement methods to assess non‐adherence to immunosuppressive drugs in kidney transplant recipients. Am J Transplant. 2008;8(3):616–626. doi:10.1111/j.1600-6143.2007.02127.x
26. Schmid-Mohler G, Thut MP, Wuthrich RP, Denhaerynck K, De Geest S. Non-adherence to immunosuppressive medication in renal transplant recipients within the scope of the integrative model of behavioral prediction: a cross-sectional study. Clin Transplant. 2010;24(2):213–222. doi:10.1111/j.1399-0012.2009.01056.x
27. Simons LE, McCormick ML, Mee LL, Blount RL. Parent and patient perspectives on barriers to medication adherence in adolescent transplant recipients. Pediatr Transplant. 2009;13(3):338–347. doi:10.1111/j.1399-3046.2008.00940.x
28. Weng FL, Chandwani S, Kurtyka KM, Zacker C, Chisholm-Burns MA, Demissie K. Prevalence and correlates of medication non-adherence among kidney transplant recipients more than 6 months post-transplant: a cross-sectional study. BMC Nephrol. 2013;14(1):261. doi:10.1186/1471-2369-14-261
29. Mathes T, Großpietsch K, Neugebauer EAM, Pieper D. Interventions to increase adherence in patients taking immunosuppressive drugs after kidney transplantation: a systematic review of controlled trials. Syst Rev. 2017;6(1):236. doi:10.1186/s13643-017-0633-1
30. Iurchenko A. Medication non adherence: finding solutions through design thinking approach. arXiv Preprint arXiv:1708.02924. 2017.
31. Nerini E, Bruno F, Citterio F, Schena FP. Nonadherence to immunosuppressive therapy in kidney transplant recipients: can technology help? J Nephrol. 2016;29(5):627–636. doi:10.1007/s40620-016-0273-x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.