Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Factors Associated with Acute Pulmonary Embolism in Patients with Hypoxia After off-Pump Coronary Artery Bypass Grafting: A Case-Control Study
Authors Yu HY, Bai YP, Song XC, Miao F, Guo XL, Wang X, Su WL
Received 31 October 2023
Accepted for publication 25 January 2024
Published 7 February 2024 Volume 2024:17 Pages 573—583
DOI https://doi.org/10.2147/JMDH.S447534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hai-Yan Yu,1,* Yun-Peng Bai,2,* Xu-Chen Song,1 Fang Miao,1 Xiao-Ling Guo,1 Xing Wang,3 Wen-Ling Su1
1Department of Endocrinology, Tianjin Chest Hospital, Tianjin, 300070, People’s Republic of China; 2Department of Cardiac Surgery, Tianjin Chest Hospital, Tianjin, 300070, People’s Republic of China; 3Department of Imaging, Tianjin Chest Hospital, Tianjin, 300070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen-Ling Su, Department of Endocrinology, Tianjin Chest Hospital, No. 261 of Taierzhuang South Road, Jinnan District, Tianjin, 300070, People’s Republic of China, Tel +86-18702263436, Email [email protected]
Purpose: This study aims to explore the factors linked to the occurrence of acute pulmonary thromboembolism (PE) within a cohort of patients exhibiting hypoxic saturation (oxygen saturation levels falling below 93%), subsequent to undergoing off-pump coronary artery bypass grafting (OPCABG).
Methods: A retrospective case-control study was conducted. A total of 296 patients met the inclusion and exclusion criteria, divided into PE group (100 cases) and non-PE group (196 cases) according to whether they had PE or not. The preoperative and postoperative information of patients were collected and statistically analyzed.
Results: The results from a multivariate logistic regression analysis indicated the following factors were independently linked to PE following OPCABG: history of smoking (OR = 3.019, 95% CI, 1.437– 6.634, P = 0.004), preoperative arterial oxygen partial pressure ≤ 78.9 mmHg (OR = 3.686, 95% CI, 1.708– 8.220, P = 0.001), presence of postoperative lower extremity deep venous thrombosis (OR = 4.125, 95% CI, 1.886– 9.310, P < 0.001), elevated postoperative D-dimer levels > 6.76 mg/l (OR = 8.078, 95% CI, 3.749– 18.217, P< 0.001), postoperative NT-BNP levels (OR = 1.001, 95% CI: 1.000– 1.001, P = 0.011), and elevated postoperative pulmonary arterial pressure > 33.0 mmHg (OR = 10.743, 95% CI: 3.422– 37.203, P < 0.001). The developed nomogram exhibited a high predictive accuracy with an area under the curve of 0.913 (95% CI: 0.878– 0.948).
Conclusion: When patients have a history of preoperative smoking, decreased preoperative arterial oxygen pressure, postoperative lower limb DVT, increased postoperative pulmonary artery pressure, and elevated postoperative D-Dimer and NT pro-BNP levels, it is recommended to take perioperative preventive measures, timely diagnostic evaluation, and if necessary, anticoagulant treatment. In addition, the results of this study may improve the diagnostic sensitivity of medical staff for postoperative PE in OPCABG, thereby increasing the detection rate and potentially reducing the need for excessive medical imaging procedures.
Keywords: case-control study, off-pump coronary artery bypass grafting, prediction model, pulmonary embolism, risk factor
A Letter to the Editor has been published for this article.
Introduction
Coronary artery bypass grafting (CABG) is considered the most effective surgical intervention for myocardial revascularization among individuals afflicted with coronary artery disease (CAD), imparting a substantial enhancement to patients’ quality of life and a prolonged lifespan.1,2 In contrast, the off-pump coronary artery bypass grafting (OPCABG) technique circumvents multiple adverse physiological effects, including water and electrolyte imbalances, disturbances in acid-base equilibrium, erythrocyte and platelet deterioration, stress-related responses, and ischemia-reperfusion injury, consequently amplifying the success rate of the procedure.2 The occurrence of hypoxia following coronary artery bypass surgery is not an infrequent event. Postoperative hypoxia may be presented through manifestations such as pleural effusion, heart failure, and acute pulmonary embolism. Continual monitoring of blood oxygen levels, employing pulse oximetry-derived oxygen saturation (SpO2), serves as a valuable method for the early detection of hypoxemia.3
Pulmonary embolism (PE) constitutes a critical postoperative complication and represents one of the principal etiologies of unforeseen fatalities within hospital settings.4 Owing to the absence of distinct clinical indicators of PE and the prevalence of nonspecific symptoms in patients, such as chest discomfort, dyspnea, tachycardia, and lower extremity edema subsequent to OPCABG,5,6 the condition is prone to oversight by both medical practitioners and patients alike. Furthermore, conventional diagnostic modalities like arterial blood gas analysis, electrocardiography (ECG), and cardiac ultrasound exhibit limited specificity in the identification of acute PE.5,6 The utilization of computed tomography pulmonary angiography (CTPA), although an effective diagnostic tool, is impeded by its relatively elevated cost, as well as potential concerns related to radioactivity and contrast agent administration, rendering it unsuitable for widespread screening. This, in turn, results in a heightened incidence of misdiagnosis and undiagnosed cases of PE following OPCABG.7 Alarmingly, fatal PE accounts for approximately 20% of unexplained deaths subsequent to cardiac surgical procedures, with nearly half of these fatalities going undiagnosed prior to death.8 In the context of cardiac surgery with systemic heparinization and prevalent postoperative administration of antiplatelet and/or anticoagulant therapies, the incidence of PE subsequent to CABG is relatively infrequent, standing at approximately 9%.9 Notably, the occurrence of PE following OPCABG exhibits substantial variability across different research studies, with a range spanning from 0.4% to 9.5% and an average rate of approximately 3.4%.8 Consequently, while PE occurrence subsequent to OPCABG is an uncommon event, its timely diagnosis and treatment are of paramount importance due to the potential for severe threats to patient well-being, prolonged hospitalization, escalated medical expenses, and increased susceptibility to legal disputes.10 On a positive note, the swift and effective diagnosis and management of postoperative PE can significantly curtail mortality rates.10,11
Hence, healthcare practitioners should remain vigilant about the prospect of PE incidence after OPCABG. Nevertheless, the precise factors contributing to the onset of PE following OPCABG are not yet comprehensively elucidated. Therefore, the objective of this study is to discern the underlying factors associated with PE and assess their predictive value in the context of hospitalized patients experiencing hypoxia, defined as an oxygen saturation level below 93%, subsequent to OPCABG.
Materials and Methods
Study Design and Patients
We conducted a retrospective case-control study and analyzed the medical records of patients who experienced hypoxia following OPCABG surgery at our hospital from February 2016 to September 2019. A total of 4445 patients who underwent OPCABG and 296 patients met the inclusion and exclusion criteria. The patients were divided into PE group (100 cases) and non-PE group (196 cases) according to whether they had PE or not (Figure 1).
 |
Figure 1 Flow chart of patient enrollment. |
The inclusion criteria were: 1) patients met the surgical criteria and accepted the OPCABG operation and 2) developed hypoxia (room air oxygen saturation < 93%)11 within one week after being removed from ventilator support post-surgery. The exclusion criteria were: patients with allergies to iodine contrast agents, severe liver or kidney dysfunction.
This study was conducted in accordance with the declaration of Helsinki. The study was approved by the Ethics Committee of Tianjin Chest Hospital (2022LW-015). As this is a retrospective study, the clinical data of the patients involved are all based on the patient’s past medical history and actual diagnosis and treatment data during hospitalisation. This study does not interfere with routine diagnosis and treatment, does not affect patients’ medical rights, and does not increase additional risks to patients. Therefore, after discussion with the Ethics Committee of Tianjin Chest Hospital, it was decided to waive the requirement for informed consent from patients. In addition, patients’ clinical data will be used for scientific research and confidentiality will be ensured. The patient’s consent was informed and obtained during hospitalisation.
Data Collection and Definition
The information pertaining to eligible patients was collected, encompassing various factors such as age, gender, prior medical history (like diabetes, hypertension, and cerebral infarction), individual history (such as smoking), occurrences of preoperative acute myocardial infarction, laboratory tests conducted before and after surgery (including parameters like hematocrit, blood platelet count, levels of NT-proB-type natriuretic peptide (NT-proBNP), and preoperative D-dimer levels), left ventricular ejection fraction (EF) before and after surgery, arterial oxygen partial pressure before surgery, the number of bypassed coronaries, duration of stay in the intensive care unit (ICU), fibrinogen levels, pulmonary arterial pressure after surgery, and extremity venous ultrasound within a week after the surgical procedure. Smoking history was characterized as having smoked a minimum of 30 packs per year or having quit smoking for less than 15 years.12 As part of the standard postoperative protocol, all patients in the study underwent an ultrasound examination of the veins in their lower limbs within one week after the surgery. Lower extremity deep venous thrombosis (DVT) was determined based on specific criteria, including the presence of no/low/medium/high substantive echo in the vein’s lumen, the absence of independent blood flow within the thrombus, lack of compression in the venous vessels, red blood cell aggregation, slow blood flow, and significant widening of the vascular diameter.10 DVT was monitored within one week after the operation. Plasma D-dimer levels were measured using the latex-enhanced immunoturbidimetry method, with the normal range being less than 0.5 mg/L. Following the surgery, a cardiac ultrasound was conducted, and a cardiologist specializing in cardiac ultrasound determined the pulmonary artery systolic pressure. Postoperative patients were treated with low molecular weight heparin anticoagulation (4000–6000 IU every 12 hours), and their coagulation function was evaluated within 24 hours after surgery. If there were no coagulation problems, single or even dual antiplatelet drugs were administered as soon as possible, including aspirin enteric coated tablets and clopidogrel sulfate. The baseline dosage was aspirin enteric coated tablets (0.1 g) and clopidogrel sulfate (75 mg). And adjust the dosage according to the actual situation of the patient. After transitioning from the ICU to the general ward, patients were encouraged to move and leave their beds. Risk assessment for individuals with acute PE was conducted using a simplified version of the sPESI scale.10,11 Within a week after the surgery, PE was monitored and diagnosed via CTPA when a blockage was observed within a pulmonary artery.13
Statistical Analysis
The data analysis involved using SPSS 22.0 (IBM Corporation, Armonk, NY, USA). For continuous data following a normal distribution, the t-test was employed. For continuous data with a skewed distribution, the rank-sum test was utilized. Categorical data were subjected to the chi-squared test. Potential factors associated with PE were incorporated into a binary logistic regression equation for multivariable logistic regression analysis. To create the nomogram, the RMS software package with R language was employed, with variables having P-values < 0.20 included in the multivariable logistic regression. The nomogram was validated using bootstrap. Receiver operating characteristics (ROC) curves were used to assess the predictive value of variables and nomograms. Statistical significance was determined with two-sided P-values < 0.05.
Results
Among the patients included in the study, 100 patients had PE, accounting for 33.8%. The patient characteristics were generally similar between those with PE (PE group) and those without (non-PE group), except for differences in age (P < 0.001), smoking history (P < 0.001), preoperative arterial oxygen partial pressure (P < 0.001), postoperative ICU stay (P < 0.001), postoperative NT-proBNP levels (P < 0.001), postoperative pulmonary arterial pressure (P < 0.001), postoperative D-dimer level (P < 0.001), and a lower incidence of postoperative extremity DVT (P < 0.001) (refer to Table 1). In Figure 2, the postoperative D-dimer levels, with a cut-off value of 6.765 mg/l, had an area under the ROC curve (AUC) of 0.829, while the preoperative arterial oxygen partial pressure, with a cut-off value of 78.9 mmHg, had an AUC of 0.707, and the postoperative pulmonary arterial pressure, with a cut-off value of 33 mmHg, had an AUC of 0.652. The results of the multivariate logistic regression analysis indicated that several factors were independently linked to postoperative PE after OPCABG. These factors include a history of smoking (OR = 3.019, 95% CI 1.437–6.634, P = 0.004), preoperative arterial oxygen partial pressure ≤ 78.9 mmHg (OR = 3.686, 95% CI, 1.708–8.220, P = 0.001), the occurrence of postoperative lower extremity DVT (OR = 4.125, 95% CI 1.886–9.310, P < 0.001), elevated postoperative D-dimer levels surpassing 6.76 mg/l (OR = 8.078, 95% CI 3.749–18.217, P < 0.001), postoperative NT-BNP levels (OR = 1.001, 95% CI 1.000–1.001, P = 0.011), and elevated postoperative pulmonary arterial pressure exceeding 33.0 mmHg (OR = 10.743, 95% CI 3.422–37.203, P < 0.001), as illustrated in Figure 3. Additionally, a nomogram constructed using these variables demonstrated an AUC of 0.913 (95% CI 0.878–0.948) for the prediction of PE after OPCABG. This nomogram incorporated factors such as smoking history, preoperative arterial oxygen partial pressure, postoperative DVT, postoperative D-dimer, postoperative NT-BNP levels, and postoperative pulmonary arterial pressure, as shown in Figure 4. The analysis of potential factors linked to acute PE risk stratification (sPESI) following OPCABG surgery revealed that patients categorized as having moderate and high PE risk were notably more prone to having a history of diabetes (P = 0.040), a prior acute myocardial infarction (P = 0.013), elevated levels of NT-proBNP before and after the surgery (P = 0.001 and P = 0.006, respectively), increased d-Dimer levels (P = 0.027), reduced preoperative and postoperative left ventricular ejection fraction (P = 0.012 and P = 0.001, respectively), and higher postoperative pulmonary artery pressure (P = 0.024) in comparison to patients with a low PE risk (see Table 2).
 |
Table 1 Basic Characteristics |
 |
Table 2 Comparison of Risk Factors in Patients with Acute PE at Different Risk Stratification (sPESI) After OPCAB Surgery |
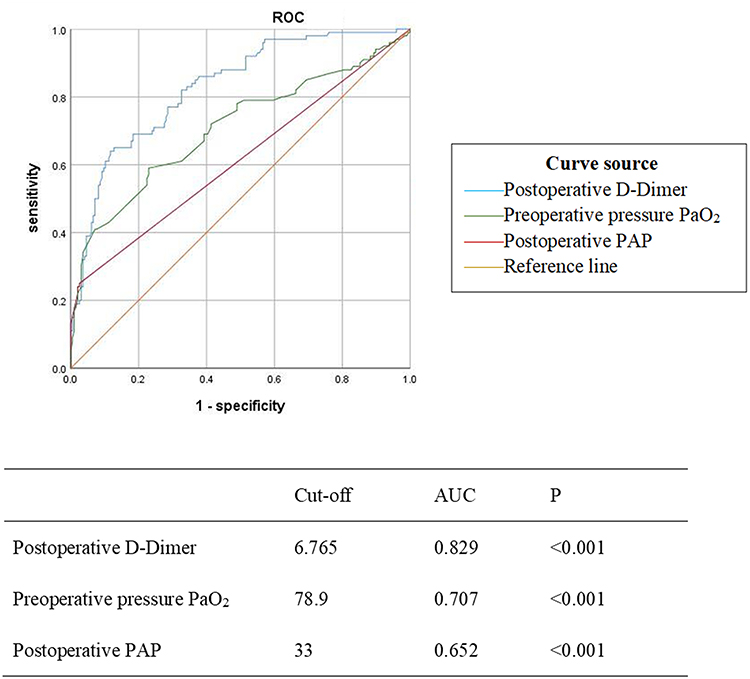 |
Figure 2 Receiver operating characteristics (ROC) analysis for the estimation of optimal variable thresholds. |
 |
Figure 3 Multivariate logistic regression analysis. |
 |
Figure 4 (A) The nomograph for pulmonary embolism. (B) Receiver operating characteristics (ROC) analysis to determine the predictive value of the nomograms. (C) Bootstrap was used to verify the prediction model. |
Discussion
In this retrospective review of 296 individuals who underwent OPCABG and subsequently experienced low oxygen levels, it was found that a prior smoking habit, pre-surgery oxygen deficiency, post-surgery DVT, increased post-surgery D-dimer levels, and heightened post-surgery pulmonary arterial pressure were each linked independently to the diagnosis of PE. The study focused on a specific group of patients: those who had hypoxia (oxygen saturation below 93%) after undergoing OPCABG surgery. This group was deliberately chosen due to their compromised respiratory function, which could explain the relatively high occurrence of PE in the study. Patients recovering from OPCABG may experience symptoms like chest pain, shortness of breath, cough, palpitations, and other non-specific complaints. These symptoms also happen to be indicators of PE, a severe condition with a low occurrence rate and a poor prognosis. This makes the likelihood of misdiagnosis and delayed treatment quite significant. To objectively assess the patients, PaO was used as a measure to provide a clear and easily detectable indication of their oxygenation status, helping to ensure a more targeted approach to patient screening and avoid unnecessary evaluations. Prior research has identified various risk factors for PE following OPCABG, with a primary focus on a patient’s medical history and the circumstances before or during surgery. Zhou et al14 found that factors such as ejection fraction, smoking history, number of grafts, surgery duration, and age were associated with an increased risk of acute PE after OPCABG. Du et al15 reported that a history of bleeding disorders, congestive heart failure in the 30 days leading up to surgery, and surgery lasting over 310 minutes were linked to a higher likelihood of venous thromboembolism after CABG. In contrast, our study places importance on the postoperative clinical signs, laboratory tests, and examinations to enhance the early detection of PE after OPCABG. This approach facilitates the prompt initiation of anticoagulant therapy, thereby enhancing patient safety after a surgical procedure.
Our current study demonstrates that a history of smoking is an independent factor associated with PE after OPCABG. This is due to the prolonged exposure of smokers to CO, which reduces the ability of hemoglobin to carry oxygen, resulting in tissue hypoxia and increased blood and plasma viscosity.16 Various chemicals in tobacco, such as nicotine, can directly harm vascular endothelial cells.17 Smoking also encourages a hypercoagulable state,18 thereby raising the risk of PE.19 As a result, a patient’s smoking history prior to surgery should be closely monitored, and precautions against postoperative PE should be reinforced in clinical practice.
Additionally, preoperative arterial oxygen partial pressure and hypoxia can contribute to the production of oxygen free radicals, vascular endothelial damage, the release of inflammatory factors, an increase in procoagulant factors, and the inhibition of natural anticoagulant mechanisms and fibrinolysis.20 Postoperative hypoxia can have an even more significant impact, particularly in the context of surgical trauma. The incidence of PE in patients with chronic obstructive pulmonary disease is notably high, ranging from 28% to 51%,21 which supports the elevated occurrence of PE observed in our study. Preoperative arterial oxygen partial pressure can offer insight into a patient’s baseline pulmonary function before surgery. The results of our study reveal that low preoperative oxygen partial pressure is a substantial risk factor for PE in patients experiencing hypoxia following OPCABG. If preoperative blood gas analysis indicates low oxygen partial pressure or poor pulmonary function in patients scheduled for OPCABG, healthcare providers can consider enhancing preoperative pulmonary function exercises as a means to reduce the risk of postoperative PE.20 Furthermore, patients with these risk factors should be vigilant about the possibility of PE following surgery. DVT frequently leads to PE22 and is often without noticeable symptoms.21 Lower extremity DVT can be effectively examined using a noninvasive, rapid, and cost-effective ultrasound. Consequently, all postoperative patients in the study underwent ultrasound examination. The results revealed that the occurrence of DVT after OPCABG was notably higher in patients with PE (74%) compared to those without PE (26.5%), consistent with previous research.23 Aside from deep vein catheterization during the perioperative period, prolonged postoperative bed rest can be linked to DVT. The two groups exhibited a significant disparity in their ICU stay. However, multivariable logistic regression indicated that ICU stay was not a major risk factor for postoperative PE. This discrepancy may be attributed to the difference between ICU stay and actual time spent in bed. Therefore, for patients with extended ICU stays, using supportive instruments can enhance blood flow in the lower extremities, and for those who are discharged from the ICU, promoting early mobilization can be advantageous in reducing the risks of postoperative DVT and PE. D-dimer serves as a widely used marker that reflects the state of fibrinolysis in clinical settings, aiding in the early detection of PE.24 Following OPCABG surgery, the stress induced by the procedure can trigger fibrinolysis, leading to elevated D-dimer levels. Consequently, relying solely on D-dimer for excluding PE after OPCABG has its limitations. Nevertheless, there is an observed correlation between D-dimer levels and the occurrence of PE in OPCABG patients in clinical practice. An earlier study23 noted that PE predominantly occurs within two weeks post-OPCABG, with an average onset period of 12.7 days. It is advisable for patients without contraindications to receive a combination of low-molecular-weight heparin anticoagulant and dual antiplatelet medications within one week after OPCABG. Elevated NT-proBNP levels in patients with PE are probably a result of heightened right ventricular stress and impairment.25 Analyzing multiple studies, it becomes evident that increased NT-proBNP levels correlate with the presence of acute PE and a greater likelihood of unfavorable PE-related outcomes.26 Therefore, NT-proBNP levels may serve as a valuable indicator for the post-surgery diagnosis or prediction of PE. However, it is worth noting that in this particular study, the OR value for NT-proBNP in relation to PE is 1.001, a finding that would benefit from further confirmation with a larger sample size.
High pulmonary artery pressure presents a significant challenge during anesthesia and surgery.27 Various surgical procedures, including cardiac, abdominal, and obstetric surgeries, are contraindicated in cases of pulmonary hypertension due to the heightened risk of complications.28 Moreover, increased pulmonary artery pressure can result from the physical blockage of lung blood vessels, causing elevated pulmonary vascular resistance.29 This suggests the potential presence of PE, even in the absence of observable symptoms. Elevated pulmonary artery pressure is also linked to endothelial damage and turbulent blood flow, both of which are risk factors for PE.6 In this study, PE was monitored within a week post-operation, and patients continued to receive low-molecular-weight heparin in conjunction with dual antiplatelet therapy until CTPA scans were performed. Large-area PE cases were rare in this study, with most patients exhibiting lobar or segmental PE. This may explain the relatively low median pulmonary systolic pressure in post-operative patients with PE, and why the difference between the PE and non-PE groups was not statistically significant. Additionally, the study had a relatively small number of participants and significant data dispersion. Individually, each of these factors may have limited predictive capability for identifying PE in patients who have undergone OPCABG and are experiencing hypoxia. However, when combined in a nomogram, they exhibit a strong predictive ability, achieving an AUC of 0.913. PE following surgery is a critical condition, but it occurs relatively infrequently. Nevertheless, the presence of PE significantly impacts patient prognosis, and the rate of both misdiagnosis and missed diagnosis is high, resulting in a heightened risk of medical disputes. The symptoms of PE are non-specific, such as chest pain, shortness of breath, cough, palpitations, and other common signs, which can easily be attributed to the post-OPCABG recovery process. Blood oxygen saturation, as an intuitive indicator of a patient’s oxygen levels, is readily accessible, easy to monitor, and offers a relatively objective measure. Therefore, the nomogram could serve as a valuable tool in identifying PE among these patients. In accordance with the results of the multivariate analysis, an examination predicated on the sPESI stratification of individuals diagnosed with PE revealed a significant correlation between moderate and high-risk PE patients and the presence of diabetes, preoperative acute myocardial infarction, elevated preoperative and postoperative NT-proBNP levels, increased D-dimer concentrations, diminished preoperative and postoperative left ventricular ejection fraction, and heightened postoperative pulmonary artery pressure. Notably, these factors have been established in prior research as contributing factors to the development of PE.5,6 The identification of these factors may prove invaluable for preemptive patient triage, offering an opportunity to assess and stratify patients based on their susceptibility to PE.
Furthermore, it is noteworthy that among the 100 patients who developed postoperative PE in this study, only 1 experienced sudden death, indicating a relatively low mortality rate and favorable prognosis. Nonetheless, a proactive stance towards preoperative preventive measures is strongly advocated for high-risk PE patients. It is recommended that a timely diagnostic evaluation be administered post-surgery, with the application of appropriate therapeutic interventions when warranted. In light of the assessment of factors such as the examination-related risks, financial implications, and adherence to patient welfare within the context of actual clinical practice, it is imperative to acknowledge that the present investigation did not encompass the entirety of patients subjected to OPCABG. Rather, a discerning approach was adopted, wherein individuals exhibiting clinical indicators suggestive of PE, (ie, hypoxia) were selectively included. It is pertinent to acknowledge the potential for the inadvertent omission of the diagnosis of partially asymptomatic PE. However, it is worth noting that previous research has demonstrated that this cohort of patients tends to exhibit a favorable prognosis subsequent to antiplatelet therapy.30 Furthermore, it is paramount to acknowledge that the retrospective nature of the study imposes certain limitations owing to the constraints inherent to the data available in the medical records. To address these limitations, we plan to conduct a prospective study encompassing comprehensive data collection to refine and augment the precision of the outcomes.
Conclusion
To summarize, when patients have a history of preoperative smoking, decreased preoperative arterial oxygen pressure, postoperative lower limb DVT, increased postoperative pulmonary artery pressure, and elevated postoperative D-Dimer and NT proBNP levels, it is recommended to take perioperative preventive measures, timely diagnostic evaluation, and if necessary, anticoagulant treatment. In addition, the results of this study may improve the diagnostic sensitivity of medical staff for postoperative PE in OPCABG, thereby increasing the detection rate and potentially reducing the need for excessive medical imaging procedures.
Data Sharing Statement
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. The study was approved by the Ethics Committee of Tianjin Chest Hospital (2022LW-015).
Consent for Publication
The requirement for informed consent was waived by the committee.
Acknowledgments
The authors acknowledge the help of colleagues in cardiac surgery and radiology.
Funding
This study was funded by Tianjin Key Medical Discipline (Specialty) Construction Project, Tianjin Municipal Health Commission Science and Technology Project (RK20012).
Disclosure
None of the authors have any financial disclosure or conflict of interest to report for this work.
References
1. Murashita T. The Current Perspectives on Coronary Artery Bypass Grafting. London: IntechOpen; 2020.
2. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
3. Jubran A. Pulse oximetry. Crit Care. 2015;19(1):272. doi:10.1186/s13054-015-0984-8
4. Wilsey HA, Pandya K, Beavers C, Xiaoshu L, Ather A. Comparison of Venous Thromboembolism Prophylactic Measures Post Coronary Artery Bypass Graft Surgery. Am J Cardiovasc Drugs. 2019;19(6):589–595. doi:10.1007/s40256-019-00354-4
5. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41(4):543–603. doi:10.1093/eurheartj/ehz405
6. Busse LW, Vourlekis JS. Submassive pulmonary embolism. Crit Care Clin. 2014;30(3):447–473. doi:10.1016/j.ccc.2014.03.006
7. Rahman IA, Hussain A, Davies A, Bryan AJ. NICE thromboprophylaxis guidelines are not associated with increased pericardial effusion after surgery of the proximal thoracic aorta. Ann R Coll Surg Engl. 2013;95(6):433–436. doi:10.1308/003588413X13629960048154
8. Shennib H, Endo M, Benhameid O. A feasibility study of the safety and efficacy of a combined clopidogrel and aspirin regimen following off-pump coronary artery bypass grafting. Heart Surg Forum. 2003;6(5):288–291.
9. Lahtinen J, Ahvenjarvi L, Biancari F, et al. Pulmonary embolism after off-pump coronary artery bypass surgery as detected by computed tomography. Am J Surg. 2006;192(3):396–398. doi:10.1016/j.amjsurg.2005.08.005
10. Panhwar MS, Ginwalla M, Kalra A, et al. Association of Acute Venous Thromboembolism With In-Hospital Outcomes of Coronary Artery Bypass Graft Surgery. J Am Heart Assoc. 2019;8(19):e013246. doi:10.1161/JAHA.119.013246
11. Geerts WH, Bergqvist D, Pineo GF, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S–453S. doi:10.1378/chest.08-0656
12. Toumazis I, Bastani M, Han SS, Plevritis SK. Risk-Based lung cancer screening: a systematic review. Lung Cancer. 2020;147:154–186. doi:10.1016/j.lungcan.2020.07.007
13. Kline JA. Diagnosis and Exclusion of Pulmonary Embolism. Thromb Res. 2018;163:207–220. doi:10.1016/j.thromres.2017.06.002
14. Zhou J, Cao X, Du Y, Shi Y, Pan W, Jia S. Risk factors for acute pulmonary embolism in patients with off-pump coronary artery bypass grafting: implications for nursing. J Int Med Res. 2020;48(11):300060520971445. doi:10.1177/0300060520971445
15. Du W, Zhao X, Nunno A, Li Y, Gu Y. Risk factors for venous thromboembolism in individuals undergoing coronary artery bypass grafting. J Vasc Surg Venous Lymphat Disord. 2020;8(4):551–557. doi:10.1016/j.jvsv.2019.06.022
16. Tapson VF. The role of smoking in coagulation and thromboembolism in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(1):71–77. doi:10.1513/pats.200407-038MS
17. Liu C, Zhou MS, Li Y, et al. Oral nicotine aggravates endothelial dysfunction and vascular inflammation in diet-induced obese rats: role of macrophage TNFalpha. PLoS One. 2017;12(12):e0188439. doi:10.1371/journal.pone.0188439
18. Cheng YJ, Liu ZH, Yao FJ, et al. Current and former smoking and risk for venous thromboembolism: a systematic review and meta-analysis. PLoS Med. 2013;10(9):e1001515. doi:10.1371/journal.pmed.1001515
19. Hannan EL, Racz MJ, Walford G, et al. Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 2003;290(6):773–780. doi:10.1001/jama.290.6.773
20. Aksu K, Donmez A, Keser G. Inflammation-induced thrombosis: mechanisms, disease associations and management. Curr Pharm Des. 2012;18(11):1478–1493. doi:10.2174/138161212799504731
21. Choi KJ, Cha SI, Shin KM, et al. Prevalence and predictors of pulmonary embolism in Korean patients with exacerbation of chronic obstructive pulmonary disease. Respiration. 2013;85(3):203–209. doi:10.1159/000335904
22. Intiso D, Di Rienzo F, Iarossi A, et al. Thrombocytosis after Hip and knee surgery in the rehabilitation setting: is it an occasional phenomenon? Relationship with deep venous thrombosis and functional outcome. BMC Musculoskelet Disord. 2015;16(1):90. doi:10.1186/s12891-015-0550-1
23. Tregouet DA, Delluc A, Roche A, et al. Is there still room for additional common susceptibility alleles for venous thromboembolism? J Thromb Haemost. 2016;14(9):1798–1802. doi:10.1111/jth.13392
24. Keller K, Beule J, Balzer JO, Dippold W. D-Dimer and thrombus burden in acute pulmonary embolism. Am J Emerg Med. 2018;36(9):1613–1618. doi:10.1016/j.ajem.2018.01.048
25. Kruger S, Graf J, Merx MW, et al. Brain natriuretic peptide predicts right heart failure in patients with acute pulmonary embolism. Am Heart J. 2004;147(1):60–65. doi:10.1016/S0002-8703(03)00528-3
26. Lega JC, Lacasse Y, Lakhal L, Provencher S. Natriuretic peptides and troponins in pulmonary embolism: a meta-analysis. Thorax. 2009;64(10):869–875. doi:10.1136/thx.2008.110965
27. Blaise G, Langleben D, Hubert B. Pulmonary arterial hypertension: pathophysiology and anesthetic approach. Anesthesiology. 2003;99(6):1415–1432. doi:10.1097/00000542-200312000-00027
28. Ramakrishna G, Sprung J, Ravi BS, Chandrasekaran K, McGoon MD. Impact of pulmonary hypertension on the outcomes of noncardiac surgery: predictors of perioperative morbidity and mortality. J Am Coll Cardiol. 2005;45(10):1691–1699. doi:10.1016/j.jacc.2005.02.055
29. Hoeper MM, Mayer E, Simonneau G, Rubin LJ. Chronic thromboembolic pulmonary hypertension. Circulation. 2006;113(16):2011–2020. doi:10.1161/CIRCULATIONAHA.105.602565
30. Yun JL, Li XY. Prevalence of pulmonary embolism at autopsy among elderly patients in a Chinese general hospital. J Geriatr Cardiol. 2016;13(11):894–898. doi:10.11909/j.issn.1671-5411.2016.11.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Prediction Nomogram for Severe Obstructive Sleep Apnea in Snoring Patients: A Retrospective Study
Teng G, Zhang R, Zhou J, Wang Y, Zhang N
Nature and Science of Sleep 2023, 15:231-243
Published Date: 17 April 2023
Establishment and Validation of a Nomogram Prediction Model for the Severe Acute Pancreatitis
Li B, Wu W, Liu A, Feng L, Li B, Mei Y, Tan L, Zhang C, Tian Y
Journal of Inflammation Research 2023, 16:2831-2843
Published Date: 8 July 2023
Increased Incidence and Risk Factors of Infections by Extended-Spectrum β-Lactamase-Producing Enterobacterales During the COVID-19 Pandemic: A Retrospective Case-Control Study
Geng Y, Li F, Chen C, Liu Z, Ma X, Su X, Meng H, Lu W, Wang X, Pan D, Liang P
Infection and Drug Resistance 2023, 16:4707-4716
Published Date: 20 July 2023
Risk Factors for Granulomatous Mastitis and Establishment and Validation of a Clinical Prediction Model (Nomogram)
Zeng Y, Zhang D, Fu N, Zhao W, Huang Q, Cui J, Chen Y, Liu Z, Zhang X, Zhang S, Mansoor KM
Risk Management and Healthcare Policy 2023, 16:2209-2222
Published Date: 20 October 2023
Analysis of Risk Factors and Development of a Predictive Model for Delirium in ICU Patients: Construction, Validation, and Clinical Implications
Li X, Zhang W, Wang T, Qiu Z, Sun X, Qu W, Zhang G
International Journal of General Medicine 2025, 18:3727-3737
Published Date: 5 July 2025