Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Factors Associated to Community Practices Toward the COVID-19 Pandemic: A Cross-Sectional Study in Indonesia
Authors Trisyani Y ![]() , Emaliyawati E
, Emaliyawati E ![]() , Nuraeni A
, Nuraeni A ![]() , Mirwanti R
, Mirwanti R ![]() , Ibrahim K
, Ibrahim K ![]() , Pramukti I
, Pramukti I ![]() , Sutini T
, Sutini T ![]() , Nurhamsyah D
, Nurhamsyah D ![]()
Received 24 January 2024
Accepted for publication 17 April 2024
Published 29 April 2024 Volume 2024:17 Pages 1901—1912
DOI https://doi.org/10.2147/JMDH.S455396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yanny Trisyani,1 Etika Emaliyawati,1 Aan Nuraeni,1 Ristina Mirwanti,1 Kusman Ibrahim,2 Iqbal Pramukti,3 Titin Sutini,4 Donny Nurhamsyah1
1Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Medical Surgical Nursing, University of Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Community Nursing, Padjadjaran University, Sumedang, West Java, Indonesia; 4Department of Mental Health Nursing, Padjadjaran University, Sumedang, West Java, Indonesia
Correspondence: Yanny Trisyani, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Ir. Soekarno KM. 21, Hegarmanah, Jatinangor, Sumedang, West Java, 45363, Indonesia, Tel +6281222073465, Fax +622287793411, Email [email protected]
Background: COVID-19 still continue to spread and affects most nations globally to date. In this context, community knowledge, attitudes, and practices (KAP) toward COVID-19 are the most important for controlling and preventing the infectious pandemic disease.
Objective: This study aimed to investigate the factors associated with community practices related to COVID-19.
Methods: Cross-sectional study was conducted on 330 residents of Sumedang District, Indonesia. Selection of the sample using stratified random sampling. KAP toward COVID-19 was measured using the WHO questionnaire which is valid and reliable. The data were analyzed using the Rasch model, Pearson correlation, and linear regression.
Results: This study revealed that most respondents tend to answer correctly on the sociality and disease transmission knowledge (+2.08 logit; SE 1.63), incorrectly in conceptual knowledge (logit measure − 2.05; SE 0.45), tended to have a positive attitude (+1.6 logit; 0.54) and practice (+1.63 logit; SE 0.61). Based on the results of the Wright map, the most challenging statement for respondents was to use masks. Knowledge and attitude were significantly associated with the practice of COVID-19 prevention (p< 0.001). Attitude is the dominant factor influencing society practice towards COVID-19 (Stand. Estimate= 0.2737; 95% CI=0.1608– 0.378; p< 0.001) and knowledge play an important role in improving COVID-19 prevention behaviour.
Conclusion: New insight from this research shows that even attitude is the most dominant factor, yet this study also indicated that knowledge is critical for positive attitudes of society to support COVID-19 prevention practices. Since, knowledge is the basis for positive attitudes in preventing the transmission of Covid 19. Therefore, health education that explicates concepts, sociality and disease transmission is important to boost attitudes of the society in the practice of Covid 19 prevention.
Keywords: attitude, COVID-19, Indonesia, knowledge, practice
Introduction
Coronavirus disease (COVID-19) is still spreading throughout the world to date and has affected 200 countries.1 It was declared as a pandemic by the World Health Organization (WHO) on March 11 2020. Globally, as of July 5 2023, around 767.726.861 cases of COVID-19 were confirmed, and as many as 6.948.764 people died from this virus.2 Southeast Asia ranks in the top 5 of the highest cases of COVID-19 in the world, including Indonesia. As of June 2023, there were 6.812.127 confirmed cases of COVID-19 in Indonesia and 161,879 deaths related to the disease.3 This prevalence rate will continue to increase, and there is a chance for new variants of COVID-19 to emerge that may be dangerous, so control of this disease must be carried out.4 Currently in Indonesia, there was an increase in positive Covid 19 cases in December 2023, which was dominated by the Omicron XBB 1.5 subvariant.5
The high prevalence rate due to COVID-19 is in line with the transmission route of this virus.6 The main transmission route of this virus is via droplets, so the process of spreading the virus is straightforward and fast.7 In addition, the clinical manifestations of COVID-19 are similar to those of pneumonia, namely fever, cough, dyspnea, hypoxemia, and bilateral infiltrates on chest radiography, and until now, the effective treatment specifically for COVID-19 patients is still unclear.8 In addition, the large number of asymptomatic cases of people who can transmit the disease can also contribute to increased cases and death rates.9 Therefore, prevention of disease transmission is a critical way to control the COVID-19 pandemic.
The control of COVID-19 has been carried out by many governments in various countries worldwide, including Indonesia.2 The recommendation from the Indonesian government to implement health protocols such as wearing masks, washing hands, and not gathering in large numbers was very effective in controlling this virus.10 In addition, previous studies have reported that vaccination is also quite effective in reducing the spread of COVID-19.11 However, the emergence of new symptoms caused by other COVID-19 variants indicates that high vaccination coverage does not always ensure effective control of COVID-19.12,13 Therefore, one of the main actions in this situation is protective and healthy practice by all members of society. People need to be aware of preventive behaviour to achieve optimal outbreak control.7
Health practice plays an essential role in limiting the spread of disease in society.14 Despite the unprecedented national action in fighting the outbreak, the success or failure of these efforts hinges on the people’s15 behaviour. Several factors, such as knowledge and attitudes,16 influence13 Community practices.14 Previous studies reported that unmarried marital status, educational status, inability to read and write, living in a rural area, and poor knowledge and attitudes were also factors associated with poor community practices related to COVID-19 prevention.17
Several studies related to knowledge, attitude, and practice (KAP) have been conducted both in Indonesia and outside Indonesia.18–23 However, methodologically, no research has analyzed KAP related to COVID-19 using the Rasch model approach. This model has advantages over group-centred statistics, particularly in measuring attitudes, perceptions, behaviour, etc.24–26 The advantages of this model include being able to provide liner scales with the same intervals, able to predict missing data, provide more precise estimations, able to detect model inaccuracies, and able to meet valid data measurement requirements.27
The COVID-19 pandemic is under control in Indonesia, as evidenced by the reduced number of positive cases and the high number of vaccinations in the community.28 The high vaccination rate shows that most people have received the COVID-19 vaccine. Vaccination is one of the most effective strategies for controlling a pandemic by establishing community or herd immunity.6 As significant numbers of the population are vaccinated, the risk of transmission and disease severity can be significantly reduced, even if the virus is still circulating.29
However, COVID-19 is a virus that has the ability to mutate very quickly, and the mutated characteristics of the virus greatly influence the process of spreading or transmission.30 Previous study concluded that the virus that causes COVID-19 has the most mutations in the targets of various nucleocapsid gene primers and probes.31 These changes can affect the properties of the virus. This new variant may have the ability to spread rapidly and cause disease severity. Additionally, new variants might alter the performance of vaccines, diagnostic tools, therapeutic drugs, and other preventative measures.32 Moreover, the current vaccination program may not necessarily able to protect someone from future mutations of the COVID-19 virus, and other ways that are also important to control it is through increasing KAP.12,13
For this reason, an assessment of community knowledge, attitudes and practices can help provide better public awareness and insight to identify gaps and strengthen community prevention efforts related to COVID-19.33 Evidence shows that community knowledge, attitudes and practices regarding disease control prevention are very effective in tackling a pandemic diseases.9,34–36 Therefore, this study aims to identify community knowledge, attitudes, and practices during the COVID-19 outbreak using the Rasch model. Using the Rasch model has many advantages. Sumitomo (2014) states that analysis using the Rasch model can provide a linear scale with the same intervals, provide more precise estimates, detect model inaccuracies, predict missing data, and fulfil valid data measurement requirements.37 Moreover, the Wright map can be analyzed using the Rasch model, which can describe the variables more comprehensively.38,39 Therefore, the research results will have better validity.
Materials and Methods
Study Design
This study was a cross-sectional study. A cross-sectional design was used to conduct a population-based survey.40 In addition, this study used the Rasch model to transform data by considering the advantages possessed by this model, such as being able to provide a liner scale with the same intervals; can predict missing data; can provide a more precise estimate; able to detect inaccuracy model; and finally able to produce replicable measurements.37
Study Participants and Data Collection
The research was conducted in Sumedang District, West Java, Indonesia. The participants of this study were recruited from 36 primary health center and quota sampling was utilised with several inclusion criteria such as: (1) respondents aged at least 18 years, (2) able to write and read, (3) stable condition at the time of data collection, and (4) willing to become research respondents. Meanwhile, the exclusion criteria were (1) the inability to speak Indonesian and (2) the respondent’s unstable condition during data collection. Respondents were recruited from 36 primary health center (PHC) in Sumedang District, West Java, Indonesia. Quota sampling according to the number of respondents for each PHC was different, so the participant selection process was adjusted to the total number health center visitors at each PHC.
The data collection was conducted from may to July 2021 by filling out the questionnaire directly from the researcher. Before filling out the questionnaire, the researcher explained the aims and benefits of the study and asked their willingness to participate. Informed consent, in accordance with the Declaration of Helsinki was provided to all respondents.41 Then, respondents who are willing to participate signed proof of consent (written consent) to become respondents. A total of 330 people participated in this study and filled out questionnaires. All respondents returned the questionnaire without exception.
Research Instruments
The demographic questionnaire includes gender, age group (year), occupation (health-related), marital status, number of households, level of education, living place, and sources of information. In addition, to identify the KAP community using a questionnaire that has been developed in the research by Erfani et al (2020).42 The KAP questionnaire consists of Conceptual knowledge (18 items) and sociality and disease transmission knowledge (8 items), attitude (15 items), and practice (12 items).42 This study classified the knowledge questionnaire into two categories (conceptual knowledge and sociality and disease transmission knowledge). Conceptual knowledge identified disease characteristics, disease symptoms, and disease prevention and control, while sociality and disease transmission knowledge identified the route of disease transmission and high-risk groups.42 In addition, to assess the general community attitude towards this disease, 15 questions were asked where the answering and scoring systems were true=3, false = 1, and no opinion =2. Then, regarding the general public’s practice and approach questionnaire towards this disease, 12 questions were asked, with the same scoring system as before (true = 3, false = 1, no opinion = 2).42 All instruments used were tested for validity and reliability with good results.
Reliability and Validity of Instruments
Based on Rasch approach analysis, all instruments (knowledge, attitude, and practice) used in this study have an excellent reliability value with a reliability value of 0.98–0.99 (Table 1). Meanwhile, person reliability tends to be weak, with a value <0.67 (Table 1). It shows that the consistency of the respondents’ answers tends to be weak; this result can also be predicted that the answer was homogenous. However, the quality of the items on the instrument is excellent. Based on Cronbach’s Alpha value, the interaction between a person (respondent answers) and items (instruments) shows quite well on attitude and practice variables, respectively (0.68 and 0.67), very good on knowledge sociality and disease transmission knowledge (0.82), and not good on conceptual knowledge (0.58) (Table 1).
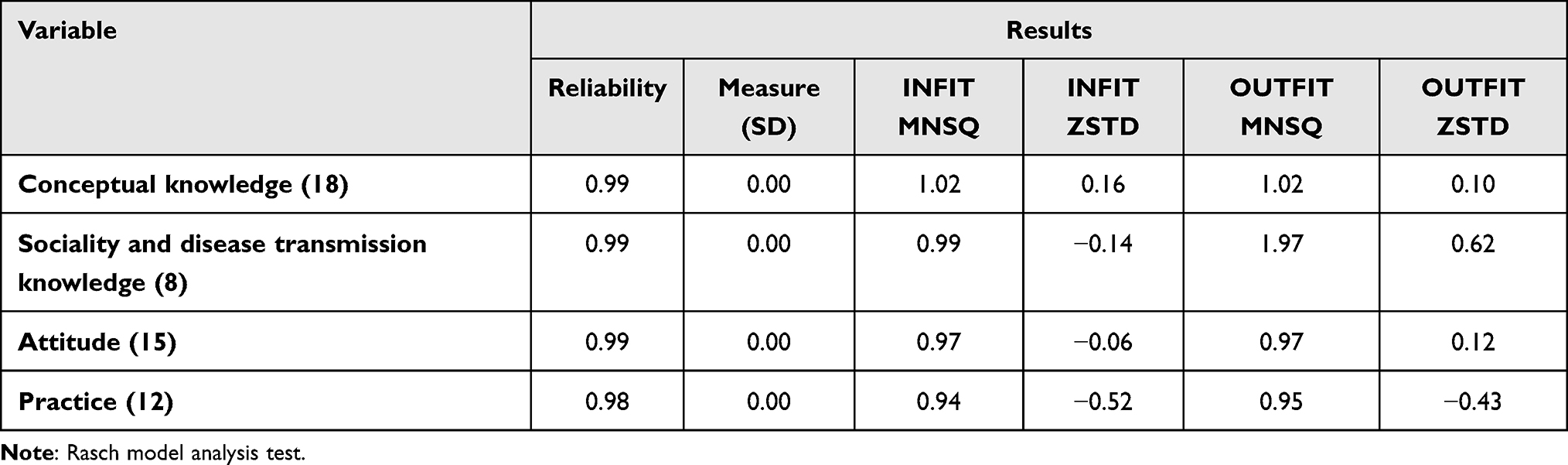 |
Table 1 Reliability of Person and Item of Instruments |
The instrument’s validity in the Rasch model is determined by the MNSQ Infit-Outfit value, which ideally should be close to 1 in the 0.5–1.50 range. Besides, it is also determined by the value of Infit-outfit ZSTD, ideally close to 0.0 in the range −2.0–2.0. The whole instruments meet this rule (Table 1), so it can be concluded that the data items in this study fit the Rasch model. Another identification for the validity test is to use the uni-dimensionality test. This test evaluates whether the instrument can measure what it should.37 The uni-dimensionality measurement requirements are met if the raw variance data is ≥ 20%. The measurement of raw variance data on knowledge Conceptual knowledge is 50.3%; this means that the instrument can measure variables well. Regarding sociality and disease transmission knowledge, the raw variance data value is 59.9%, close to 60%, which means this instrument can measure variables very well. Likewise, the respective raw variance data values for the attitude and behavior instruments were 40.9% and 39.1%, which means the tool could measure these variables correctly.
Ethical Consideration
Ethical principles such as autonomy, beneficence, nonmaleficence and justice are applied to all respondents. Moreover, this study received ethical clearance from the Padjadjaran University research ethics committee with letter number 035/UN6/KEP/EC/2021 and follows the Declaration of Helsinki. Respondents in this study were previously given information about the aims and benefits of the research both orally and in writing. Then, respondents who are willing to participate sign proof of consent to become respondents. This study is voluntary, and respondents can refuse or leave the process without any consequences. Data obtained from respondents is analyzed in groups and only used for academic purposes so that researchers keep all information obtained confidential.
Statistical Analyses
The statistical analysis used is descriptive, bivariate, and multivariate analysis. All demographic data and variables were tested for distribution normality using a Kolmogorov–Smirnov test. Numerical data were presented as mean ± SD, while categorical data were presented as frequency and percentage proportions as appropriate. The variables of KAP were transformed using the Rasch model approach.37 Univariate analysis of these three variables was based on the logit measure (SE). In the Rasch model, the results/scores of each variable have been transformed into a logit which shows that a value below logit 0.0 (item logit) indicates a more accessible aspect and above that value indicates a more challenging part.37 In this study, negative values indicate poor knowledge, attitudes and practices, while positive values indicate better results.
The author used the Pearson correlation test to determine the relationship between knowledge and attitudes towards practices related to COVID-19.43 In addition, the Spearman rank test was to find out the relationship between demographic characteristics towards practices related to COVID-19 and linear regression to see the dominant factor of practices using the Jamovi software version 2.3.21.43 The test using linear regression has gone through an assumption test where the heteroscedasticity value using Breusch-Pagan (p=0.067), Goldfeld-Quandt (p=0.322), and Harrison-McCabe (p=0.315) shows p>0.05.43
Results
Demographic Characteristics of Respondents
A total of 330 participants completed the questionnaire. The demographic characteristics are presented in Table 2. Most respondents are female (70.6%), with the age category of 21–30 years (28.2) dominating. Almost all respondents (90.6%) have non-health-related jobs. More than two-thirds of respondents were married (79.4%), with the number of households ≤ 4 (75.5%). In addition, most respondents have junior secondary school (30%) and live in their own homes (94.8%).
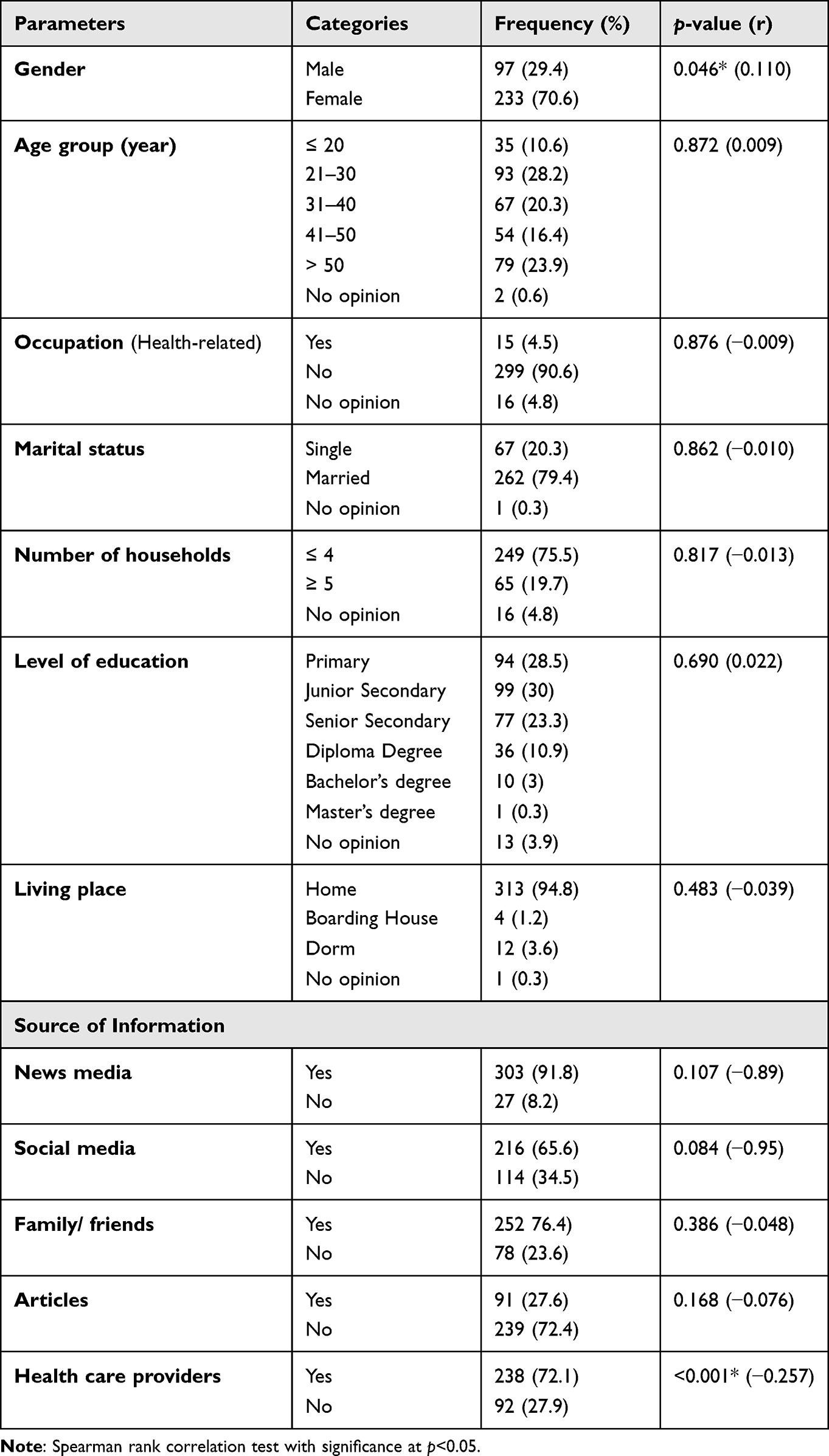 |
Table 2 Correlation Between Demographic Characteristics and Practice Toward COVID-19 (n=330) |
Respondents were asked where they obtained information related to COVID-19. Table 2 shows the distribution of sources of information regarding COVID-19. 91.8% of respondents received information through news media, 65.6% through social media, 76.4% through family or friends, only 27.6% through articles, and 72.1% through healthcare providers.
Knowledge, Attitude, and Practice Toward COVID-19
Data on knowledge, attitude, and behaviour variables in this study were analyzed using the Rasch model approach. Table 3 shows the number of respondents that differ in each variable. It happens because the Rasch model allows researchers can take out extreme values data that can affect the quality of group data. Therefore, extreme values, data outliers from each variable, are excluded from getting quality results.
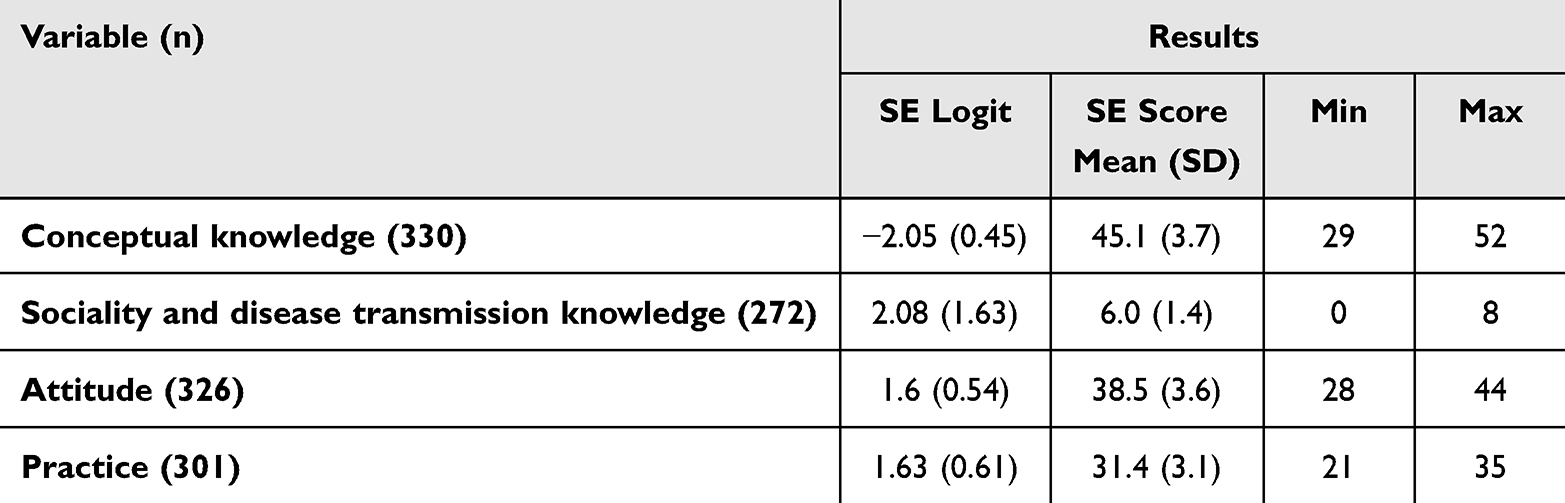 |
Table 3 The Summary of Community Knowledge, Attitudes, and Practice Regarding COVID-19 Using the Rasch Model Approach |
Concerning the logit values obtained, Table 3 shows that most respondents answered correctly on the sociality and disease transmission knowledge variable (measure +2.08 logit; SE 1.63) and tend to have positive attitudes (measure +1.6 logit; 0.54) and practice (measure +1.63) logit; SE 0.61). Meanwhile, in conceptual knowledge, respondents tend to answer questions incorrectly (logit measure −2.05; SE 0.45).
Based on the results of the Wright map distribution (see Figure 1), it can be seen that the statement that was the most challenging question for respondents to do was item number 12 (use of masks), followed by statement 6 (avoiding going to work). While the statement that, according to them, the most capable of doing is item no 7 (washing hands frequently).
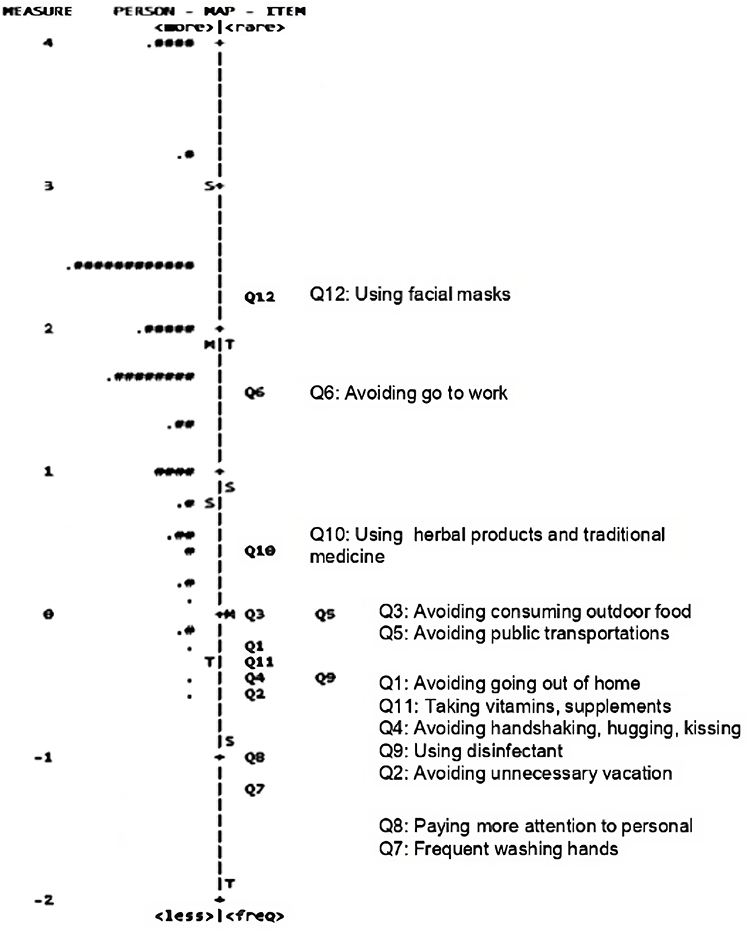 |
Figure 1 Wright Map of Practice. Notes: The persons are on the left side of the line, and items are located on the right of the line. More able (easier to practice) persons are located at the bottom of the map. More difficult (more difficult to be practiced) items are located at the top of the map. Each “#” represents 3 persons. Each represents 1–2 persons (M = mean; S=1 standard deviation from the mean; T = 2 standard deviations from the mean). |
Correlation Between Knowledge, Attitude, and Practice Toward COVID-19
Table 4 shows the correlation between knowledge, attitude, and practice toward COVID-19. Conceptual knowledge (p<0.001; r=0.261), sociality and disease transmission knowledge (p<0.001; r=0.481), and attitude (p<0.001; r=0.506) were significantly associated with the practice regarding COVID-19. In addition, Table 2 shows that gender (p=0.046; r=0.110) and resources from healthcare providers (p=<0.001; r=−0.257) were significantly associated with the practice towards COVID-19.
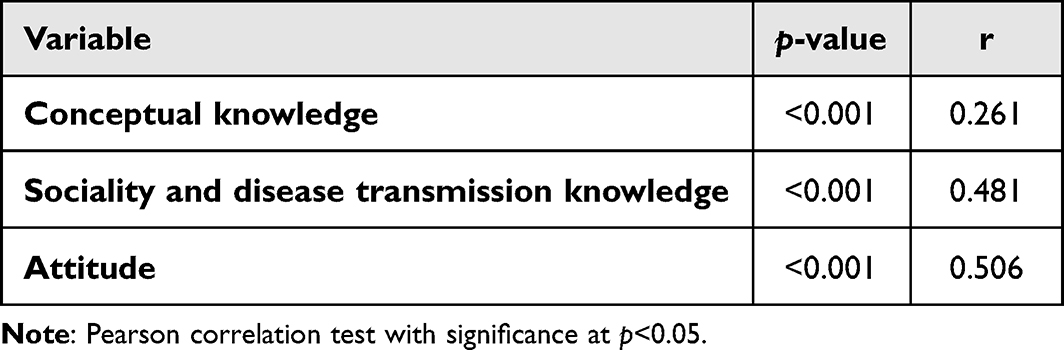 |
Table 4 Correlation Between Knowledge, Attitudes Towards COVID-19 Practices (n=330) |
Table 5 presents the correlation between conceptual knowledge, sociality and disease transmission knowledge, and attitude with practice through a linear regression test. Sociality and disease transmission knowledge (Stand. Estimate= 0.2107; 95% CI=0.0941–0.327; p<0.001) and attitude (Stand. Estimate= 0.2737; 95% CI=0.1608–0.378; p<0.001) significantly affect practice. Among these variables, attitude has the most significant influence on practice, equal to 27.4%. In addition, sociality and disease transmission knowledge was estimated to contribute 21.1% to practice, while conceptual knowledge only contributed 4.9%. However, the other 46.6% of factors that influence practice did not identify in this study.
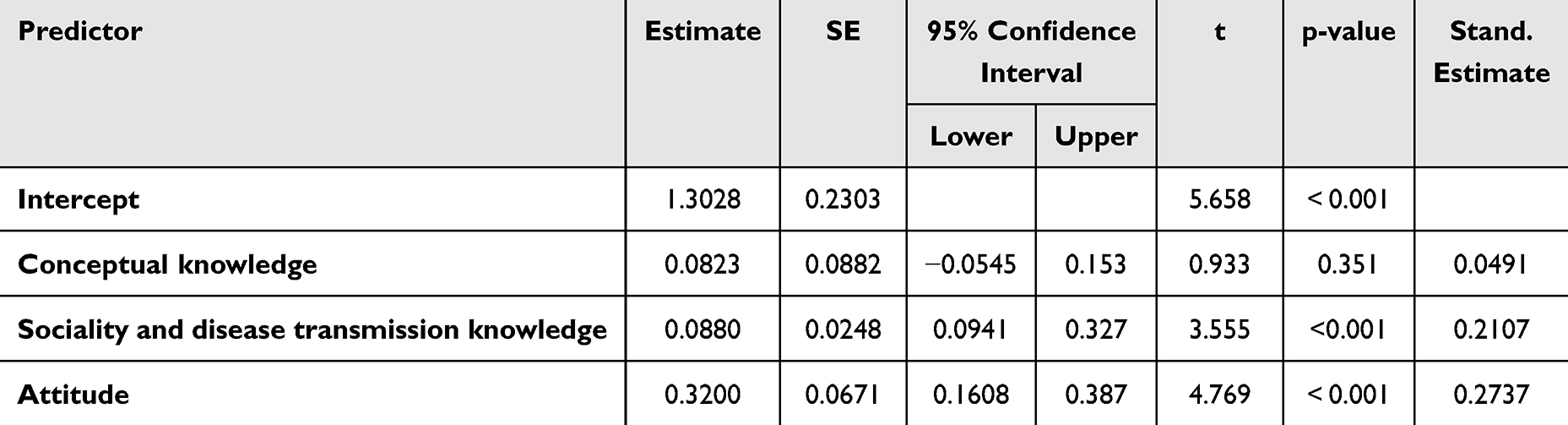 |
Table 5 Effect of Knowledge, Attitude Toward Practice Regarding COVID-19 |
The plot diagram in Figure 2 shows how conceptual knowledge, sociality and disease transmission knowledge, and attitudes affect practice. All variables show a unidirectional effect on practice improvement. However, of these three variables, attitude is the variable that has the most significant influence on practice regarding COVID-19 (Figure 2c). This aligns with the correlation test in Table 5, which shows that attitude determines the most significant contribution (27.4%). In addition, Figures 2a and b show that sociality and disease transmission knowledge more significantly influence community practice than conceptual knowledge.
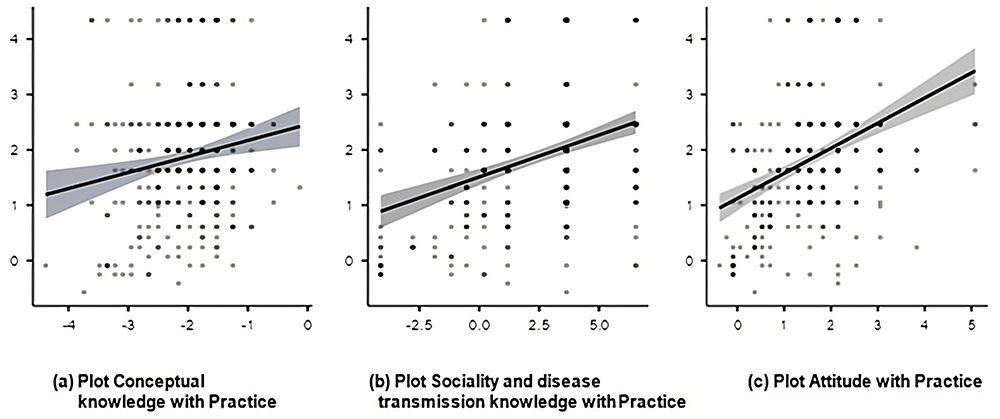 |
Figure 2 Plot of the relationship between knowledge and attitudes towards practice in preventing COVID-19. Noted: (a) Plot Conceptual knowledge with practice; (b) Plot Sociality and disease transmission knowledge with practice; (c) Plot Attitude with Practice. |
Discussion
This study identifies factors related to COVID-19 prevention practices in Indonesia using the Rasch model approach. Knowledge, attitudes and practices are important factors in controlling the transmission of infectious diseases such as COVID-19, so it is essential to identify it continuously.21 In this study, the categorization of community practices related to COVID-19 used a Log Odds Unit (logit) score so that the results of the analysis of practice will be more accurate and validated appropriately compared to several previous studies, which only used an average score or by dividing it into good behaviour or bad.18–23
The results showed that most of respondents answered correctly on the sociality and disease transmission knowledge variable. However, respondents tended to answer incorrectly on the conceptual knowledge aspect. In addition, the respondents had attitudes and practices that tended to be positive (see Table 3). This shows that community knowledge about disease transmission routes and high-risk groups is sufficient to make people have positive attitudes and practices even though they do not know the concept of the disease.
In this study, respondents’ practice towards COVID-19 tended to be positive (logit +1.63 measure; SE 0.61) (see Table 3). Figure 2 shows the results of the Wright map analysis; the most challenging thing for respondents to do was item number 12 (use of masks), followed by statement 6 (avoiding work). Meanwhile, according to them, the statement that was the most capable was point no 7 (washing hands frequently). Previous studies showed the same results, which said that, in general, research respondents had practices against positive COVID-19.15,44–46 In addition, a study conducted in Indonesia also said that most of the respondents had a positive attitude toward COVID-19 prevention.18–20 Positive practice can undoubtedly reduce the rate of transmission due to COVID-19.34 Health practice is based on three factors, namely knowledge, attitude, and practice.16 These three factors are interrelated but do not always affect each other. The research conducted by Salman et al (2020) indicated that preventive measures against COVID-19 have not been conducted satisfactorily even though the participants have good attitudes and knowledge.46
In this study, attitude (Stand. Estimate= 0.2737; 95% CI=0.1608–0.378; p<0.001) is the most dominant factor influencing community practice towards COVID-19 prevention. These results show that people with a positive attitude are 27.4 times more likely to show positive practices related to preventing the transmission of COVID-19. This is confirmed by the results of the correlation analysis using plot diagrams (see Figure 2c), where attitudes have the most significant gradient in determining practice. In addition, a previous literature review reported that KAP against COVID-19 in various countries in the world also said that attitude is the main factor in the formation of positive practice among people towards preventing COVID-19 transmission.37.
Attitudes are beliefs about certain objects or ideas, either pleasant or unpleasant, that produce behavioural tendencies.47 A pleasant attitude occurs when individuals have a positive and supportive perception of preventing COVID-19 such as using masks, maintaining distance, washing hands, etc.42 Individuals with a positive attitude will be more consistent in implementing preventive measures in daily life.42 Meanwhile, individuals with an unpleasant attitude (negative perception) may refuse or feel uncomfortable with preventive measures. So this can increase the risk of spreading the virus in the community.48 Therefore, attitudes are needed to encourage preventive practices against COVID-19.48 Community attitudes can also mediate between knowledge and practice, so they have a significant role in changing one’s practice.19,22,34
Another factor that influences community practice towards COVID-19 is disease transmission knowledge (the route of disease transmission and high-risk groups) (Stand. Estimate= 0.2107; 95% CI=0.0941–0.327; p<0.001). Knowledge related to disease transmission is one of the important factors to note in the context of COVID-19 prevention, especially in Indonesia.18–20 A high knowledge score will be needed for better preventive measures.34 In addition, community knowledge, especially in preventing the spread of the SARS-CoV-2 virus, is very useful in suppressing the transmission of the virus.9 Our findings show that the high number of correct answers in this aspect is strongly influenced by various sources of information obtained by respondents regarding the prevention of transmission of COVID-19 (see Table 2). Therefore, knowledge play an important role in improving COVID-19 prevention behaviour.48
Among all demographic characteristics, gender (p=0.046; r=0.110) and sources of information from healthcare providers (p<0.001; r=−0.257) were significantly correlated with practice in preventing the transmission of COVID-19. This aligns with previous studies in Indonesia,49 Malaysia,50 Iran,51 and Saudi Arabia.52 Studies conducted in Bangladesh reported that the female gender, older age, and higher education had positive attitudes and practices towards COVID-19.53 Previous studies reported that male respondents had more negative attitudes and practices towards preventing COVID-19.53 In addition, respondents thought that the most accurate source of information regarding COVID-19 came from health workers (57.7%).54 This study concluded that female respondents who received information from health service providers tended to show positive attitudes and practices toward the prevention of COVID-19. Likewise, information from healthcare providers will increase respondents’ knowledge so that prevention awareness will increase.54
Apart from this research variable, several other factors can contribute to community practice towards preventing COVID-19. Studies in Indonesia indicated that a government policy requiring people to comply with health protocols can increase awareness of better preventive practices.44 In addition, a study in Malaysia also reported the same thing, which said that the Malaysian government’s ability to overcome disease and deal with crises due to COVID-19 was excellent so that this could reduce the prevalence rate of transmission from COVID-19.50 Then, a study was conducted among 404 chronic disease patients in Ethiopia showing that unmarried marital status, educational status, unable to read and write, living in a rural area, less than average monthly income, and poor knowledge were significant factors related to the poor practice of COVID-19 transmission.17
Information about COVID-19, the symptoms that appear for sufferers and prevention efforts that can be undertaken must be communicated through health promotion activities, community service, and other activities.17 Providing leaflets door to door to the public (traders, pedicab drivers, online motorcycle taxi drivers, public transportation drivers followed by placing media in public areas is an effort that can be done. Thus, it is hoped that all levels of community, especially those with low access to information, can read and understand about COVID-19.
Strengths and Limitations
In this study, only two factors were analyzed that related to community practice in preventing the transmission of COVID-19, namely knowledge and attitudes. Based on the study’s results, it was shown that as many as 46.6% of other factors needed to be identified to determine factors that could potentially influence people’s behaviour in preventing the transmission of COVID-19, such as family income, ability to read and write, and others.
Conclusions
Respondents in this study demonstrated good knowledge, positive attitudes, and practices that support COVID-19 prevention. There is a significant correlation between knowledge, attitudes, and practice in preventing the transmission of COVID-19. Attitude is the most dominant factor that affects public practices regarding COVID-19 prevention followed by knowledge about sociality and disease transmission.
New insights from this research shows that knowledge also has an important role in improving COVID-19 prevention practices of the society. Since, knowledge is the basis for positive attitudes in preventing the transmission of Covid 19. Therefore, health education that explicates concepts, sociality and disease transmission knowledge is critical to build positive attitudes of the community to improve the practice of Covid 19 prevention.
Acknowledgments
All authors would like to thank Padjadjaran University, Bandung, West Java, Indonesia, for facilitating funding for the publication of this research. The author also thanks the Sumedang Regional Government for funding this research process.
Disclosure
The authors report no conflicts of interest in this research.
References
1. Setiati S, Azwar MK. COVID-19 and Indonesia. Acta Med Indones. 2020;52(1):84–89.
2. World Health Organization. WHO Coronavirus (COVID-19) Dashboard; 2023. Available from: https://covid19.who.int/.
3. Ministry of Health of the Republic of Indonesia. Circular Number 1 of 2023 Task Force for COVID-19 Handling; 2023. Available from: https://covid19.go.id/id/artikel/2023/06/16/circular-number-1-2023-task-force-covid-19-handling.
4. Fontanet A, Autran B, Lina B, Kieny MP, Karim SSA, Sridhar D. SARS-CoV-2 variants and ending the COVID-19 pandemic. Lancet. 2021;397(10278):952–954. doi:10.1016/S0140-6736(21)00370-6
5. Ministry of Health of the Republic of Indonesia. COVID-19 Cases Rise Again, Community Asked to Remain Disciplined in Prokes. Redaksi Sehat Negeriku; 2023. Available from: https://sehatnegeriku.kemkes.go.id/baca/umum/20231206/5244404/kasus-covid-19-naik-lagi-masyarakat-diminta-tetap-disiplin-prokes/.
6. World Health Organization. Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations; 2020. Available from: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations.
7. NeJhaddadgar N, Pirani N, Heydarian N, et al. Knowledge, attitude, and practice toward the COVID-19 infection among adults Iran: a cross-sectional study. J Public Health Res. 2022;11(4). doi:10.1177/22799036221129370
8. Yesudhas D, Srivastava A, Gromiha MM. COVID-19 outbreak: history, mechanism, transmission, structural studies and therapeutics. Infection. 2021;49(2):199–213. doi:10.1007/s15010-020-01516-2
9. Puspitasari IM, Yusuf L, Sinuraya RK, Abdulah R, Koyama H. Knowledge, attitude, and practice during the COVID-19 pandemic: a review. J Multidiscip Healthc. 2020;13:727–733. doi:10.2147/JMDH.S265527
10. Ministry of Health of the Republic of Indonesia. Health Protocols for Communities in Public Places and Facilities in the Context of Prevention of COVID-19. Emerging Infections; 2023. Available from: https://covid19.kemkes.go.id/protokol-covid-19/protokol-kesehatan-bagi-masyarakat-di-tempat-dan-fasilitas-umum-dalam-rangka-pencegahan-covid-19.
11. Zheng C, Shao W, Chen X, Zhang B, Wang G, Zhang W. Real-world effectiveness of COVID-19 vaccines: a literature review and meta-analysis. Int J Infect Dis. 2022;114:252–260. doi:10.1016/j.ijid.2021.11.009
12. Zhang M, Liang Y, Yu D, et al. A systematic review of Vaccine Breakthrough Infections by SARS-CoV-2 DeltaVariant. Int J Biol Sci. 2022;18(2):889–900. doi:10.7150/ijbs.68973
13. Bergwerk M, Gonen T, Lustig Y, et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N Engl J Med. 2021;385(16):1474–1484. doi:10.1056/NEJMoa2109072
14. Elayeh E, Aleidi SM, Ya’acoub R, Haddadin RN. Before and after case reporting: a comparison of the knowledge, attitude and practices of the Jordanian population towards COVID-19. PLoS One. 2020;15(10):1–17. doi:10.1371/journal.pone.0240780
15. Kundu S, Al Banna MH, Sayeed A, et al. Knowledge, attitudes, and preventive practices toward the COVID-19 pandemic: an online survey among Bangladeshi residents. J Public Heal. 2021.
16. Notoatmojo. Promosi Kesehatan, Teori Dan Aplikasinya. Jakarta: Rineka Cipta; 2012.
17. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards covid-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949–1960. doi:10.2147/IDR.S258736
18. Mujiburrahman Riyadi ME, Ningsih MU. Knowledge Related to Increasing COVID-19 Prevention Behavior in the Community. J Keperawatan Terpadu. 2021;2(2):130–140.
19. Sutiningsih D. The relationship between the level of knowledge and attitudes with the practice of preventing COVID-19 among internet users in the city of Semarang. J Epidemiol Kesehat Komunitas. 2021;6(2):300–306. doi:10.14710/jekk.v6i2.11886
20. Kurniawan D. The Relationship of Knowledge Level with Behavior Prevention Covid-19 in the Work Area of the Jekan Raya Puskesmas in 2022. J Surya Med. 2022;9(1):67.
21. Iradukunda PG, Pierre G, Muhozi V, Denhere K, Dzinamarira T. Knowledge, Attitude, and Practice Towards COVID-19 Among People Living with HIV/AIDS in Kigali, Rwanda. J Community Health. 2021;46(2):245–250. doi:10.1007/s10900-020-00938-1
22. Zhong BL, Luo W, Li HM, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
23. Pantow RJ, Rumayar AA, Tucunan AAT, et al. Gambaran Perilaku Masyarakat Terhadap Pencegahan Corona Virus Disease 19 (Covid-19) Di Desa Malat Utara Kecamatan Gemeh Kabupaten Kepulauan Talaud. Kesmas. 2021;10(3):9–18.
24. Ardiyanti D. Application of the Rasch Model on the Development of the Self-Efficacy Scale in Student Career Decision Making. J Psikol. 2017;43(3):248.
25. Melianasari D. Rasch Stacking Analysis: career Decision Making Self-Efficacy (CDMSE) of Students Based on Gender. Psychocentrum Rev. 2022;4(2):210–217. doi:10.26539/pcr.42996
26. Boone W, Staver J, Yale M. Rasch Analysis in the Human Sciences. Dordrech: Springer; 2014.
27. Sumintono B, Widhiarso W. Application of the Rasch Model to Research in the Social Sciences. Trim B, editor. Cimahi: Trim Komunikata Publishing House; 2014. Available from https://www.researchgate.net/publication/268688933_Aplikasi_Model_Rasch_untuk_Penelitian_Ilmu-Ilmu_Sosial_edisi_revisi.
28. World Health Organization. COVID-19 Vaccination Post Introduction Evaluation (Cpie) in Indonesia; 2023.
29. She J, Hou D, Chen C, Bi J, Song Y. Challenges of vaccination and herd immunity in COVID-19 and management strategies. Clin Respir J. 2022;16(11):708–716. doi:10.1111/crj.13543
30. Hebbani AV, Pulakuntla S, Pannuru P, Aramgam S, Badri KR, Reddy VD. COVID-19: comprehensive review on mutations and current vaccines. Arch Microbiol. 2021;204(1):8. doi:10.1007/s00203-021-02606-x
31. Wang R, Hozumi Y, Yin C, Wei G-W. Mutations on COVID-19 diagnostic targets. Genomics. 2020;112(6):5204–5213. doi:10.1016/j.ygeno.2020.09.028
32. Islam S, Islam T, Islam MR. New Coronavirus Variants are Creating More Challenges to Global Healthcare System: a Brief Report on the Current Knowledge. Clin Pathol. 2022;15.
33. Tomar BS, Singh P, Nathiya D, et al. Indian Community’s Knowledge, Attitude, and Practice toward COVID‑19. Indian J Soc Psychiatry. 2021;37:48–56. doi:10.4103/ijsp.ijsp_133_20
34. Wake AD. Knowledge, Attitude, Practice, and Associated Factors Regarding the Novel Coronavirus Disease 2019 (COVID-19) Pandemic. Infect Drug Resist. 2020;13:3817–3832. doi:10.2147/IDR.S275689
35. Maheshwari S, Gupta PK, Sinha R, Rawat P. Knowledge, attitude, and practice towards coronavirus disease 2019 (COVID-19) among medical students: a cross-sectional study. J Acute Dis. 2020;9(April):100–104. doi:10.4103/2221-6189.283886
36. Alnasser AHA, Al-tawfiq JA, Al-kalif MSH, et al. Public Knowledge, Attitudes, and Practice towards COVID-19 Pandemic in Saudi Arabia: a Web-Based Cross-Sectional Survey. Med Sci. 2021;9(11):1–12.
37. Sumintono B, Widhiarso W. Aplikasi Model Rasch Untuk Penelitian Ilmu-Ilmu Sosial (Edisi Revisi). Trim Komunikata Publishing House; 2014.
38. Jimam NS, Ismail NE, Dangiwa DA, et al. Use of Rasch Wright map to understand the quality of Healthcare Workers’ Knowledge, Attitudes, and Practices for Uncomplicated Malaria (HKAPIUM). J Pharm Bioresour. 2021;18(3):237–244. doi:10.4314/jpb.v18i3.8
39. Sumintono B. Rasch Model Measurements as Tools in Assessment for Learning. Int J Med. 2018;173(2017):38–42.
40. Setia MS. Methodology Series Module 3: cross-sectional Studies. Indian J Dermatol. 2016;61(13):261–264. doi:10.4103/0019-5154.182410
41. Salako SE. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
42. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak- A population-based survey in Iran. Bull World Health Organ. 2020;13(3):2–17.
43. Polit & Beck. Nursing Research: Principle and Methods.
44. Simanjorang C, Tooy GC, Wuaten G, Pangandaheng N. Knowledge, Attitudes, and Practices Towards COVID-19 among North Sulawesi Indonesia Residents. J Heal Educ. 2021;6(2):57–64. doi:10.15294/jhe.v6i2.42869
45. Srichan P, Apidechkul T, Tamornpark R, et al. Knowledge, attitudes and preparedness to respond to COVID-19 among the border population of northern Thailand in the early period of the pandemic: a cross-sectional study. WHO South-East Asia J Public Heal. 2020;9(2):118–125. doi:10.4103/2224-3151.294305
46. Salman M, Mustafa ZU, Asif N, et al. Knowledge, attitude and preventive practices related to COVID-19: a cross-sectional study in two Pakistani university populations. Drugs Ther Perspect. 2020;36(7):319–325. doi:10.1007/s40267-020-00737-7
47. Notoadmojo. Daftar Isi: Promosi Kesehatan Dan Perilaku Kesehatan; 2012.
48. Lee M, Kang B, You M. Knowledge, attitudes, and practices (KAP) toward COVID-19: a cross-sectional study in South Korea. BMC Public Health. 2021;21(295):1–10. doi:10.1186/s12889-021-10285-y
49. Muslih M, Susanti HD, Rias YA, Chung MH. Knowledge, Attitude, and Practice of Indonesian Residents toward COVID-19: a Cross-Sectional Survey. Int J Environmental Res Public Heal. 2021;18:4473.
50. Azlan AA, Hamzah MR, Sern TJ, Ayub HS, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):1–15. doi:10.1371/journal.pone.0233668
51. Honarvar B, Lankarani KB, Kharmandar A, et al. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health. 2020;65(6):731–739. doi:10.1007/s00038-020-01406-2
52. Al-hanawi MK, Angawi K, Alshareef N, et al. Knowledge, Attitude, and Practice Toward COVID-19 Among the Public in the Kingdom of Saudi Arabia: a Cross-Sectional Study. Front Public Health. 2020;8(May):1–10.
53. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an onlinebased cross-sectional study. PLoS One. 2020;15:1–17. doi:10.1371/journal.pone.0239254
54. Umeta B, Mulugeta T, Mamo G, et al. An analysis of COVID-19 information sources. J Pharm Policy Pract. 2022;15(1):49. doi:10.1186/s40545-022-00446-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Knowledge, Attitudes, and Perceptions of Tuberculosis in Indonesia: A Multi-Center Cross-Sectional Study

Kaaffah S, Kusuma IY, Renaldi FS, Lestari YE, Pratiwi ADE, Bahar MA
Infection and Drug Resistance 2023, 16:1787-1800
Published Date: 28 March 2023
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024