Back to Journals » Patient Preference and Adherence » Volume 16
Factors Affecting the Reception of Self-Management Health Education: A Cross-Sectional Survey Assessing Perspectives of Lower-Income Seniors with Cardiovascular Conditions
Authors Tran SHN ![]() , Weaver RG
, Weaver RG ![]() , Manns BJ, Saunders-Smith T, Campbell T, Ivers N, Hemmelgarn BR, Tonelli M, Pannu R, Campbell DJT
, Manns BJ, Saunders-Smith T, Campbell T, Ivers N, Hemmelgarn BR, Tonelli M, Pannu R, Campbell DJT ![]()
Received 17 December 2021
Accepted for publication 11 March 2022
Published 8 April 2022 Volume 2022:16 Pages 971—981
DOI https://doi.org/10.2147/PPA.S351459
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sophia HN Tran,1,2 Robert G Weaver,2 Braden J Manns,2,3 Terry Saunders-Smith,2 Tavis Campbell,4 Noah Ivers,5,6 Brenda R Hemmelgarn,7 Marcello Tonelli,2,3 Raj Pannu,8 David JT Campbell2,3,9
1Department of Psychology, University of Waterloo, Waterloo, ON, Canada; 2Department of Medicine, University of Calgary, Calgary, AB, Canada; 3Department of Community Health Sciences, University of Calgary, Calgary, AB, Canada; 4Department of Psychology, University of Calgary, Calgary, AB, Canada; 5Department of Family and Community Medicine, University of Toronto, Toronto, ON, Canada; 6Department of Family and Community Medicine, Women’s College Hospital, Toronto, ON, Canada; 7Faculty of Medicine & Dentistry, University of Alberta, Calgary, AB, Canada; 8Emergence Creative, New York, NY, USA; 9Department of Cardiac Sciences, University of Calgary, Calgary, AB, Canada
Correspondence: David JT Campbell, Tel +1 403-210-9511, Email [email protected]
Introduction: Self-management education and support (SMES) programs can prevent adverse chronic disease outcomes, but factors modifying their reception remain relatively unexplored. We examined how perceptions of an SMES program were influenced by the mode of delivery, and co-receipt of a paired financial benefit.
Methods and Patients: Using a cross-sectional survey, we evaluated the perceived helpfulness of a SMES program among 446 low-income seniors at high risk for cardiovascular events in Alberta, Canada. Secondary outcomes included frequency of use, changes in perspectives on health, satisfaction with the program, and comprehensibility of the material. Participants received surveys after engaging with the program for at least 6 months. We used modified Poisson regression to calculate relative risks. Open-ended questions were analyzed inductively.
Results: The majority of participants reported that the SMES program was helpful (> 80%). Those who also received the financial benefit (elimination of medication copayments) were more likely to report that the SMES program was helpful (RR 1.24, 95% CI 1.11– 1.39). Those who received the program electronically were more likely to use the program weekly (RR 1.51, 1.25– 1.84). Both those who received the intervention electronically (RR 1.18, 1.06– 1.33), and those who also received copayment elimination (RR 1.17, 1.05– 1.31) were more likely to state that the program helped change their perspectives on health.
Conclusion: When designing SMES programs, providing the option for electronic delivery appears to promote greater use for seniors. The inclusion of online-delivery and co-receipt of tangible benefits when designing an SMES program for seniors results in favorable reception and could facilitate sustained adherence to health behavior recommendations. Participants also specifically expressed that what they enjoyed most was that the SMES program was informative, helpful, engaging, and supportive.
Keywords: self-management, chronic disease, tailored programs, educational intervention, cardiovascular prevention
Chronic medical conditions are common, with 44% of adults in Canada being diagnosed with one or more chronic conditions.1 Cardiovascular-related chronic conditions, such as diabetes, kidney disease, and heart disease have a substantial impact on survival,2 quality of life,3 and healthcare costs.4 The negative impact Of these conditions can be prevented by health behavior changes which have been shown to prevent complications.5–9 Successfully encouraging patients to undertake these changes is a challenge,10 as only 30–50% of patients adhere to health behavior modification advice provided by a healthcare provider.11 Self-management education and support (SMES) programs can help patients make behavior changes.8,9,12–14 Providing patients with adequate support is fundamental to their success in making and sustaining health behavior modifications.15,16 SMES programs are often recommended17–21 and can be delivered through a variety of methods including in-person,8,9,22,23 over the phone,24 through paper communications,8,9 or via electronic/online-delivery.25 Self-management programs that target specific patient needs are generally preferred12,23,25 and can produce more sustained results in comparison to general health education programming.26 SMES programs can be time- and resource-intensive to develop and deliver,7 and these programs may be unsuccessful if they fail to meet the needs or interests of the target population.27 However, it is unclear what features make SMES programs most effective or appealing,25 and how such programs can be designed to best meet the needs of patients.
In countries like Canada where medication coverage is not fully provided free-of-charge, the financial costs associated with managing chronic conditions are a common barrier to effective self-management.28,29 In particular, when patients’ expenditures on prescription medications exceed 5% of household income, they are more likely to pose a financial barrier.30 Not only can this impact adherence to medications, but it may also impair patients’ ability to engage in proper self-management strategies and health behaviors.31 We therefore postulated that those receiving a co-intervention including elimination of medication copayments (i.e. free medications) would potentially be more amenable to behavior change advice.
If SMES programs are to be used to address the growing burden that chronic conditions place on health care systems, factors that improve patients’ reception of these programs must be examined. In this study, we used data from the Assessing outcomes of enhanced Chronic disease Care through patient Education and a value-baSed formulary Study (ACCESS trial),32 to examine participants’ impressions of a tailored, multi-modal SMES program for cardiovascular prevention targeted at lower-income older adults at high risk of cardiovascular events. While we have previously published a qualitative evaluation of the intervention,33 in the present study, we used a survey to seek feedback from participants more broadly, in order to summarize recipients’ perceptions of the SMES program, and if these were influenced by the mode of delivery (electronic vs paper-based), and/or by co-receipt of a medication copayment elimination intervention.
Methods
ACCESS Trial
The current study was nested within ACCESS (Clinicaltrials.gov #: NCT02579655), a factorial randomized-controlled trial in Alberta, Canada, testing two interventions to improve outcomes in low-income seniors with cardiovascular-related chronic conditions.32 The interventions tested were: a tailored SMES platform; and the elimination of patient-borne copayments for high-value medications used to treat and prevent the progression of cardiovascular conditions. Both interventions were provided for the duration of the study (36 months).
Eligible participants were recruited through long-term care facilities, health care providers, and media advertisements.34 To qualify for the study, participants must have been older adults (≥65 years) with lower income (in Alberta’s lowest income quartile), at high risk of cardiovascular events (based on the presence of chronic health conditions like diabetes and hypertension). The blinded randomized group allocation was in a 1:1:1:1 ratio (self-management education, copayment elimination, both interventions, or usual care/control). Participants were actively recruited from November 2015 to August 2018. Each participant’s intervention commenced immediately after randomization for a span of three years.
The SMES program consisted of weekly mailed postcards (Appendix A), health tools, and access to a website that provided additional resources. These resources were co-developed by a social impact creative design firm. The education and support in the program were delivered through the voice of a fictional peer, named Moxie, with unique branding, to encourage participant engagement.35,36 Self-reported baseline information (including medications, self-reported adherence, chronic conditions, beliefs about the necessity of medication, and concerns about medications37) was used to tailor the messaging participants would receive. Using these variables, participants were assigned to one of 50 pre-specified tracks that determined which precise mailer participants received each week. Mailers were trifold cards with information about health conditions or medications and contained suggestions on chronic disease self-management and preventive care. At pre-specified time points, tangible goods, including a reusable grocery bag (3-months), a health tracker book (6-months), and a pedometer (12-months), were provided to participants to promote healthy behaviors and generate engagement with the SMES program.
Participants who were enrolled in the electronic version were also provided with log-in information to access a secure tailored website,38 built by a health-focused IT consultant (Locus Health, Charlottesville, VA; Appendix B). In addition to their weekly posted paper mailer, these participants received thrice-weekly emails from Moxie with health tips and invitations to check in to their tailored webpage.
Participants randomized to the co-payment elimination groups received full coverage (without copayment) for medications used to treat and prevent the progression of cardiovascular conditions including, but not limited to, antihypertensive, antihyperglycemic, antiplatelet, and cholesterol-lowering medications (Appendix C). This coverage was provided for the duration of their participation in the trial.
Data Collection
The present study is a cross-sectional survey assessment of participants’ perceptions of the Moxie program. The primary outcome was participants’ ratings of helpfulness of the self-management program. Secondary outcomes included the frequency of use, self-reported changes in perspectives on health, satisfaction with the structure of the program, and comprehensibility of the material (Appendix D). Furthermore, an open-text field was provided for survey respondents to describe what they found to be the most helpful aspect of the Moxie program. We chose variables to include as potential confounders that might have independently influenced perceptions of the self-management education program:39–43 age, sex, income, education, ethnicity/race, employment status, country of origin, native language, and health literacy.
Surveys were sent to participants who had recently completed the six-month follow-up assessments for the ACCESS trial (Appendix D). To ensure that participants were at a comparable period in their intervention timeline, participants who had previously completed their six-month follow-up, or who had not yet completed it were not sent this survey. Responses to these surveys were linked to the data collected from participants in their baseline assessments for the ACCESS trial, including sociodemographic characteristics. Approval was granted from the Conjoint Health Research Ethics Board (CHREB) at the University of Calgary (REB#13-1241) and the University of Alberta Health Research Ethics Board (Pro00062473). Written informed consent was received from all participants at the outset of the ACCESS trial. Further, all aspects of this study comply with the Declaration of Helsinki.
Data Analysis
Chi-squared tests were used to examine differences in each outcome by the two exposures (copayment elimination and method of delivery). To calculate relative risk (RR) of the outcomes we used modified Poisson regression,44 adjusting for potential confounding variables.45,46 Pairwise deletion was used to address missing data. Stata version 16 (College Station, Texas) was used for the analysis.
Inductive coding was used to explore open-ended questions assessing which messages and materials of the self-management intervention program participants enjoyed and found most impactful. Participants’ responses to open-ended questions were categorized into categories such as: enjoyment, community/support, reminders, and information.
Results
A total of 1152 surveys were sent out to eligible participants from ACCESS, with 728 participants (63%) responding. Data from those randomized to receive only copayment elimination were excluded from analyses. This left a final sample of 446 respondents who were enrolled in the SMES intervention, 296 (66%) of whom also received the copayment elimination intervention (Figure 1). Most participants (69%, n=306) received only paper delivery, while 31% (n=140) opted to receive the enhanced electronic version of Moxie.
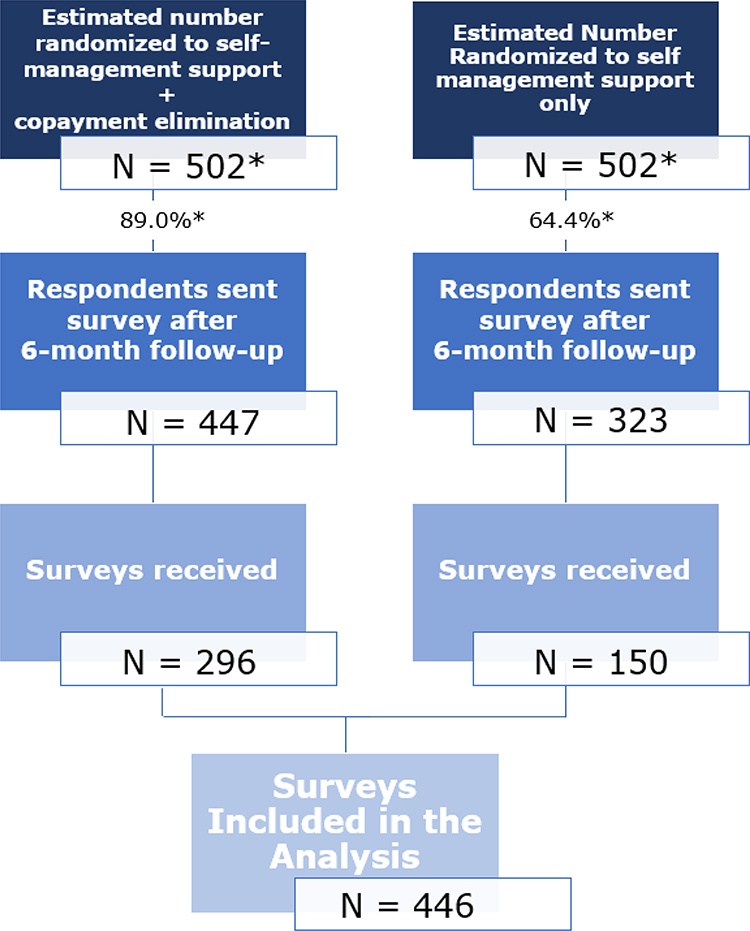 |
Figure 1 Flow chart depicting the source of participants included in the analysis. Note: *Note that estimated number of enrollees randomized based on the response rate to 6-month survey from each respective group. |
The survey respondents included 234 men (52%) and 212 women (48%). Ages ranged from 66–96 years (mean 77.2; SD 5.96). Participants who selected an electronic mode of delivery tended to be younger, more affluent, with more education and greater health literacy (Table 1).
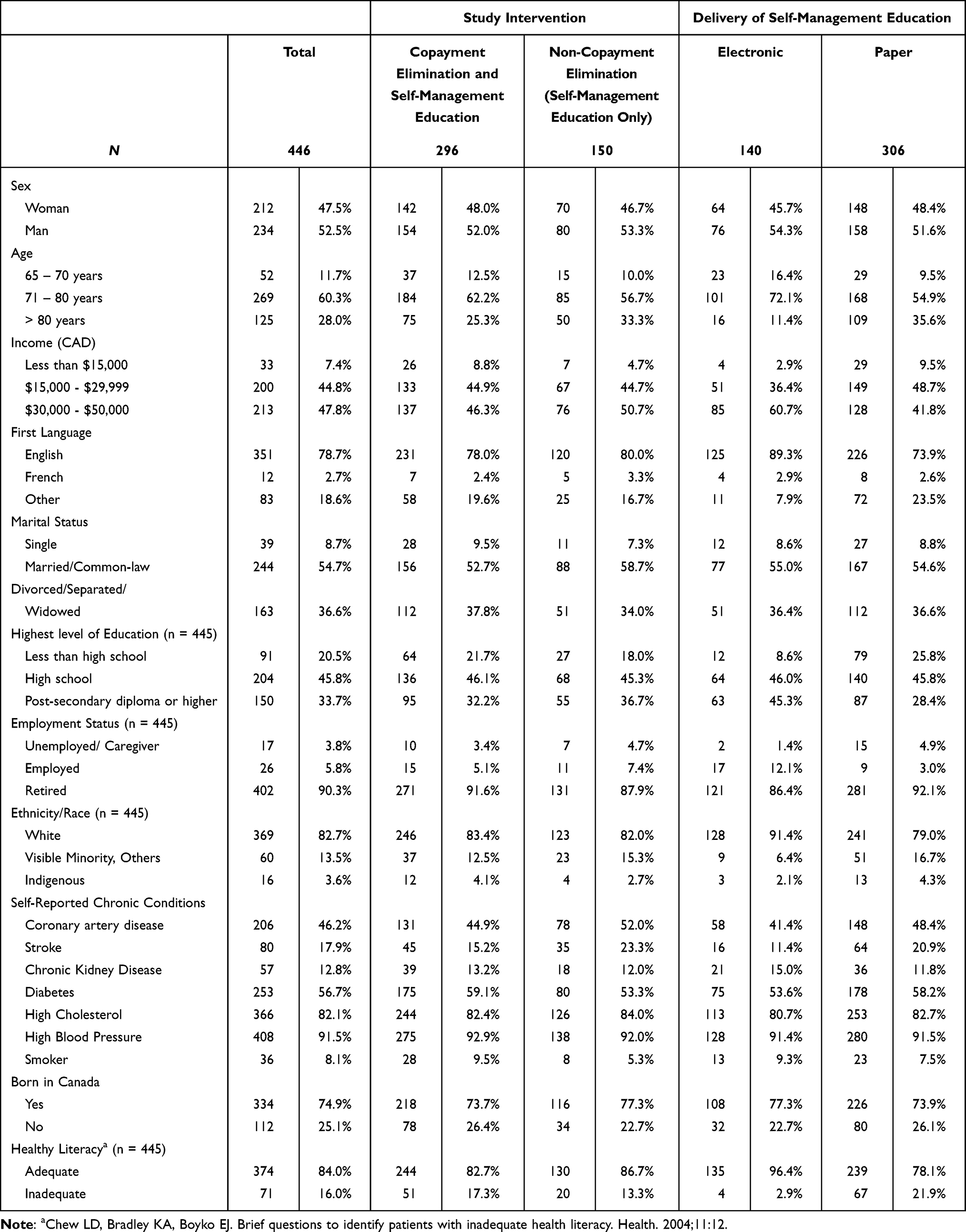 |
Table 1 Participant Characteristics, by Delivery Type and Co-Receipt of Copayment Elimination Intervention |
Helpfulness of Moxie Program & Frequency of Use
Participants were first asked whether they found Moxie (the SMES program) helpful. Most participants rated the SMES program as helpful (83%), regardless of whether the method of delivery was electronic (86%) or paper (81%) (Table 2). A more notable difference was observed between co-payment intervention groups. More participants in the copayment elimination group rated the SMES program as helpful (89%) than those in the non-copayment elimination (71%) group (RR 1.24, 95% CI 1.11–1.39) (Table 2).
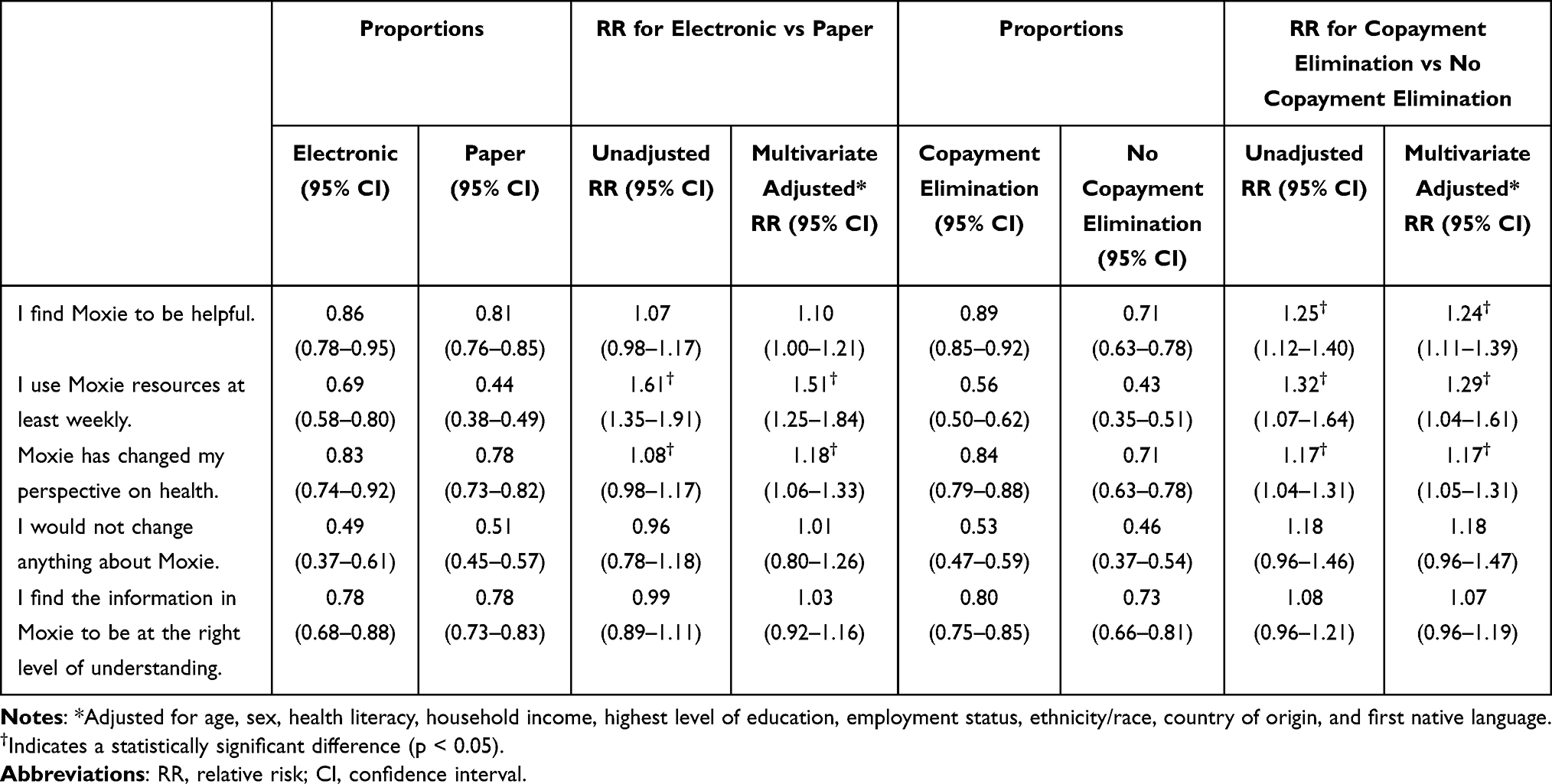 |
Table 2 Association Between Exposure Variables (Method of Delivery and Co-Receipt of Copayment Elimination) and Reception of Self-Management Education Intervention (N = 446) |
To further elaborate on why the SMES program was helpful, participants were asked to identify which specific element of Moxie they found to be most helpful. Recipes (n=254, 57%) and mailers (n=243, 54%) were rated as helpful by more than half of the respondents. In comparison, a smaller number found pedometers (n=148) and other special gifts (n=110) to be helpful. Among electronic participants, roughly half found the emails (n=77) and online articles (n=65) to be helpful.
Participants were also asked in a separate open-text box what they enjoyed most about Moxie. The largest number of participants (n=149) stated that they enjoyed the new information provided by Moxie; one participant stated:
It is informative and gives good points to help you decide what you can do for yourself.
-Woman 1, Age 79
More specifically, participants reported that the new health information provided was informative (66%), kept them up-to-date (4%), and was comprehensive (1%). Others reported that they particularly enjoyed new information about recipes (19%), diet (4%), exercise (3%), and healthy lifestyle recommendations (2%). Finally, participants who enjoyed the new information also reported that it helped them manage their specific conditions (11%).
A smaller number (n=68) stated that they found the reminders to be helpful and the way the materials were provided to be engaging:
I appreciate the humour in the way the information is presented. Receiving the mailers is like receiving a postcard from a friend.
-Woman 2, Age 69
In particular, almost half the participants that reported enjoying the reminders also stated that they helped manage and monitor their health conditions and associated risks. Participants specifically appreciated reminders about their medication (24%), exercise (19%), and diet (12%). Finally, participants also noted that the reminders kept them on track in terms of a healthy lifestyle.
The next most commonly stated helpful feature was that Moxie provided them with a sense of personal support (n=61):
I like the fact that Moxie is in touch with me every week, just like an ‘old friend’.
-Woman 3, Age 81
There were no notable differences in open-ended responses by delivery modality or co-receipt of copayment elimination. Essentially, participants expressed that what they enjoyed most about Moxie was that it was informative, helpful, engaging, and supportive regardless of delivery modality or co-receipt of copayment elimination.
Differences in our modifiable factors were more discernable in terms of frequency of use. A greater proportion of participants who received information electronically reported that they used Moxie at least weekly (69%), compared to those who received the intervention in paper format only (44%) (adjusted RR 1.51, 95% CI 1.25–1.84). A higher proportion of participants who received copayment elimination (56%) used the program at least weekly in comparison to participants who did not receive copayment elimination (42%) (adjusted RR 1.29, 95% CI 1.04–1.61) (Table 2).
Changes in Perspectives on Health
To shed light on whether the SMES program had a substantive impact, we also asked whether Moxie changed participants’ perspectives on their health. The majority of participants reported that the SMES program changed their perspectives on health, which was slightly more commonly reported by those receiving the information electronically (83%) than by those on the paper-based program (78%) (adjusted RR 1.18, 95% CI 1.06–1.33) (Table 2). Those receiving copayment elimination (84%) were also more likely to report a change in perspective than those who did not (71%) (adjusted RR 1.17, 95% CI 1.05–1.31) (Table 2). Of the participants that reported a change in perspective, approximately half reported that they were more informed about dietary modifications and more motivated to get physically active (Table 3). A smaller proportion of participants reported that the program helped provide strategies to manage stress (32%) and medication (38%); and improved relationships (34%) or communication (29%) with their medical team.
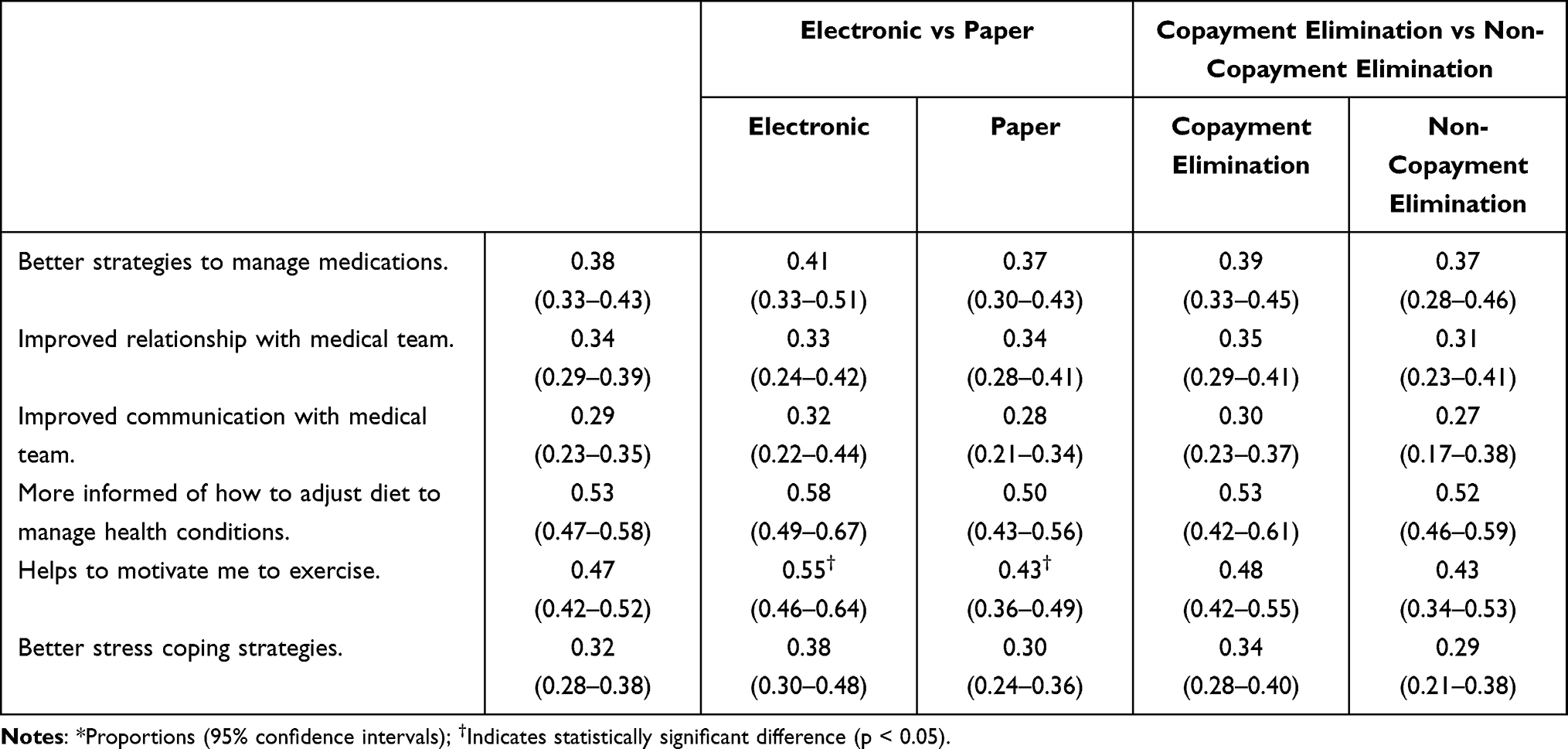 |
Table 3 Participants’ Reported Change in Health Perspectives (N = 446)* |
Satisfaction with Structure & Comprehensibility of the Program
To determine what could be done to improve the SMES program, participants were asked if they would change anything about Moxie. Roughly half the participants responded that they would not change anything about Moxie. This did not vary by mode of delivery or co-receipt of copayment elimination. Of the 144 who wanted to change something about Moxie, the most frequent suggestion was for less frequent contact (n=75); however, another 41 people suggested that they would have preferred more frequent contact from Moxie. The second-highest number (n=58) suggested that Moxie could be improved by providing updated materials and information. A smaller proportion (n=43) suggested a different style of messaging, with most asking that the messaging be more sophisticated, in-depth, or tailored.
Approximately three-quarters of the respondents felt that the comprehensibility of the materials (i.e. whether they found the language and messaging to be at the correct level of understanding) was appropriate. This did not vary by either exposure variable.
Discussion
The majority of participants perceived the tailored SMES program to be helpful. The participants’ positive reception of this tailored SMES program is consistent with previous findings that patients prefer intervention programs that are tailored.9,13,14,24 Regardless of delivery modality or co-receipt of medication copayment elimination, participants reported that the SMES program was informative and engaging. This is particularly important because engaging patients in health behavior change can be challenging.11 As patients were involved in the design, modification, and implementation of this SMES program, this suggests that patient involvement is beneficial when developing health education programs that resonate with the target audience. The lack of difference between the two modes of delivery for seniors is also an important finding, as an online SMES program is likely more sustainable in the long term in comparison to a paper-based version. An online SMES program would easily allow for future extensions, the ability to update information, and to customize user preferences.
Another feature that participants frequently reported enjoying was the sense of support that the program provided. This finding is meaningful as previous studies have found that providing patients with adequate support is fundamental to successfully making and sustaining health behavior modifications.15,16 The findings from this study suggest that personalization and support are crucial components to also consider when designing SMES programs for lower-income seniors. In particular, tailoring an SMES program for a specific population successfully fosters an informative, engaging, and supportive environment, important for facilitating changes to health behavior.
We noted several important differences with regard to perceptions based upon the method of delivery and co-receipt of medication copayment elimination. Although our target population consisted of seniors, those who received the intervention electronically accessed the program more frequently and were more likely to report that it increased their motivation to become more physically active. This finding is novel as there is an absence of studies examining the effectiveness of online SMES programs for older adults.12 As the electronic mode of delivery provided participants with feedback when they answered a daily question, this finding is consistent with the literature demonstrating that timely feedback is important in SMES.25 Finally, coupling the education intervention with copayment elimination increased the likelihood that participants found the intervention to be helpful, used it weekly, and reported that it changed their perspectives on health. A possible explanation for this successful outcome is that when seniors with a potentially limited income do not have to worry about the cost of co-payments, this enables them to focus more wholeheartedly on a self-management education program.
A strength of this study is the use of both qualitative and quantitative data, which allows for both standardized data collection and meaningful insight into patients’ perspectives of the design and implementation of the SMES program. As previously alluded to, the inclusion of older adults (65+) with chronic cardiovascular conditions is also a strength, as this demonstrated the efficacy of electronic delivery of the SMES program. This is a novel finding within a population that is often underrepresented in the research literature.
Limitations
A limitation of this study is that the results can only be generalized to older adults with lower-incomes and cardiovascular-related chronic diseases, although this is a very important population who are at the highest risk of hospitalization. Further research on the acceptability of SMES programs should be conducted in other populations. Additionally, only the method of delivery and co-receipt of copayment elimination were examined as exposure variables within this study, but many other potentially modifiable factors could change the reception of SMES. For example, whether caregiver involvement influences participants’ reception of a self-management program also should be considered in future studies as this is another variable that could impact how accessible SMES programs are. As this was a cross-sectional study (nested within an RCT), a cause-and-effect relationship cannot be assumed, and there may be confounding variables that were not accounted for in our regression analysis; however, we were able to adjust for several important confounders. Finally, it is important to note that the outcome used in this study (subjective acceptability) is an intermediate proxy – a participant’s reported reception of the self-management intervention may have no bearing on their actual health behaviors, or ultimately on their chronic disease-related outcomes. Further, the use of self-report data could be subject to social-desirability effects and is a proxy indicator of actual usage. Additionally, the receipt of copayment elimination could have resulted in reporting biases, as those receiving these benefits might have been incentivized to provide more positive feedback. The final ACCESS results will use objective clinical outcomes that will provide a more robust evaluation of the true efficacy of this intervention. However, this study provides important mechanistic information about the acceptability of such interventions in this population.
Conclusion
Our study findings have practical implications for scaling and implementing tailored SMES programs, which has been identified as a need in the literature.47,48 Specifically, the findings from this study suggest that researchers and health program managers who intend to implement or evaluate SMES programs should consider offering electronic means of receiving the program when the intended population consists of older adults. Furthermore, our findings suggest that pairing SMES with tangible benefits has the potential to enhance uptake and positive reception.
Abbreviations
SMES, Self-Management Education and Support; ACCESS, Assessing outcomes of enhanced Chronic disease Care through patient Education and a value-baSed formulary Study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Public Health Agency of Canada. Prevalence of chronic diseases among Canadian adults. 2019. Available from: https://www.canada.ca/en/public-health/services/chronic-diseases/prevalence-canadian-adults-infographic-2019.html.
2. Preston SH, Choi D, Elo IT, Stokes A. Effect of diabetes on life expectancy in the United States by race and ethnicity. Biodemography Soc Biol. 2018;64(2):139–151. doi:10.1080/19485565.2018.1542291
3. Megari K. Quality of life in chronic disease patients. Health Psychol Res. 2013;1(3):e27. doi:10.4081/hpr.2013.932
4. McBrien KA, Manns BJ, Chui B, et al. Health care costs in people with diabetes and their association with glycemic control and kidney function. Diabetes Care. 2013;36(5):1172–1180. doi:10.2337/dc12-0862
5. Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI. Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PLoS One. 2019;14(8):e0220116. doi:10.1371/journal.pone.0220116
6. Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: a randomized trial. Med Care. 1999;37(1):5–14. doi:10.1097/00005650-199901000-00003
7. Monsivais D, Reynolds A. Developing and evaluating patient education materials. J Contin Educ Nurs. 2003;34(4):172–176. doi:10.3928/0022-0124-20030701-09
8. Rief JJ, Mit GR, Zickmund SL, et al. Promoting patient phronesis: communication patterns in an online lifestyle program coordinated with primary care. Health Educ Behav. 2013;40(3):311–322. doi:10.1177/1090198112452863
9. Seligman H, Wallace A, Dewalt D, et al. Facilitating behavior change with low-literacy patient education materials. Am J Health Behav. 2007;31:S69–S78. doi:10.5993/AJHB.31.s1.9
10. Newsom JT, Huguet N, McCarthy MJ, et al. Health behavior change following chronic illness in middle and later life. J Gerontol B Psychol Sci Soc Sci. 2012;67(3):279–288. doi:10.1093/geronb/gbr103
11. Campbell DJ, Ronksley PE, Manns BJ, et al. The association of income with health behavior change and disease monitoring among patients with chronic disease. PLoS One. 2014;9(4):e94007. doi:10.1371/journal.pone.0094007
12. Bolle S, Van Weert JCM, Daams JG, Loos EF, De Haes HCJM, Smets EMA. Online health information tool effectiveness for older patients: a systematic review of the literature. J Health Commun. 2015;20(9):1067–1083. doi:10.1080/10810730.2015.1018637
13. Glasgow RE, Eakin EG, Toobert DJ. How generalizable are the results of diabetes self-management research? The impact of participation and attrition. Diabetes Educ. 1996;22(6):573–585. doi:10.1177/014572179602200605
14. Sorensen G, Emmons K, Hunt MK, Johnston D. Implications of the results of community intervention trials. Annu Rev Public Health. 1998;19(1):379–416. doi:10.1146/annurev.publhealth.19.1.379
15. Coleman MT, Newton KS. Supporting self-management in patients with chronic illness. Am Fam Physician. 2005;72(8):1503–1510.
16. Dwarswaard J, Bakker EJ, van Staa A, Boeije HR. Self-management support from the perspective of patients with a chronic condition: a thematic synthesis of qualitative studies. Health Expect. 2016;19(2):194–208. doi:10.1111/hex.12346
17. Barnason S, White-Williams C, Rossi Laura P, et al. Evidence for therapeutic patient education interventions to promote cardiovascular patient self-management: a scientific statement for healthcare professionals from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2017;10(6):e000025. doi:10.1161/HCQ.0000000000000025
18. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
19. Nerenberg KA, Zarnke KB, Leung AA, et al. Hypertension Canada 2018ʹs guidelines for diagnosis, risk assessment, prevention, and treatment of hypertension in adults and children. Can J Cardiol. 2018;34(5):506–525. doi:10.1016/j.cjca.2018.02.022
20. Sherifali D, Berard LD, Gucciardi E, Macdonald B, Macneill G. Self-management education and support. Can J Diabetes. 2018;42(sS):S36–S41. doi:10.1016/j.jcjd.2017.10.006
21. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Diabetes Educ. 2017;43(1):40–53. doi:10.1177/0145721716689694
22. Teng H-L, Yen M, Fetzer S, Sung J-M, Hung S-Y. Effects of targeted interventions on lifestyle modifications of chronic kidney disease patients: randomized controlled trial. West J Nurs Res. 2013;35(9):1107–1127. doi:10.1177/0193945913486202
23. Rankin D, Cooke D, Elliott J, Heller S, Lawton J. Supporting self-management after attending a structured education programme: a qualitative longitudinal investigation of type 1 diabetes patients’ experiences and views. BMC Public Health. 2012;12(1):652. doi:10.1186/1471-2458-12-652
24. Weinert C, Cudney S. My health companion[c]: a low-tech personal health record can be an essential tool for maintaining health. Online J Rural Nurs Health Care. 2012;12(1):3. doi:10.14574/ojrnhc.v12i1.36
25. Morton K, Dennison L, May C, et al. Using digital interventions for self-management of chronic physical health conditions: a meta-ethnography review of published studies. Patient Educ Couns. 2017;100(4):616–635. doi:10.1016/j.pec.2016.10.019
26. Marín G, Burhansstipanov L, Connell CM, et al. A research agenda for health education among underserved populations. Health Educ Q. 1995;22(3):346–363. doi:10.1177/109019819402200307
27. Blackberry ID, Furler JS, Best JD, et al. Effectiveness of general practice based, practice nurse led telephone coaching on glycaemic control of type 2 diabetes: the patient engagement and coaching for health (PEACH) pragmatic cluster randomised controlled trial. Br Med J. 2013;347:f5272. doi:10.1136/bmj.f5272
28. Campbell DJ, Manns BJ, Weaver RG, Hemmelgarn BR, King-Shier KM, Sanmartin C. Financial barriers and adverse clinical outcomes among patients with cardiovascular-related chronic diseases: a cohort study. BMC Med. 2017;15(1):33. doi:10.1186/s12916-017-0788-6
29. Campbell DJ, King-Shier K, Hemmelgarn BR, et al. Self-reported financial barriers to care among patients with cardiovascular-related chronic conditions. Health Rep. 2014;25(5):3–12.
30. Hennessy D, Sanmartin C, Ronksley P, et al. Out-of-pocket spending on drugs and pharmaceutical products and cost-related prescription non-adherence among Canadians with chronic disease. Health Rep. 2016;27(6):3–8.
31. Law MR, Cheng L, Kolhatkar A, et al. The consequences of patient charges for prescription drugs in Canada: a cross-sectional survey. CMAJ Open. 2018;6(1):E63–E70. doi:10.9778/cmajo.20180008
32. Campbell DJ, Tonelli M, Hemmelgarn B, et al. Assessing outcomes of enhanced chronic disease care through patient education and a value-based formulary study (ACCESS)-study protocol for a 2x2 factorial randomized trial. Implement Sci. 2016;11(1):131. doi:10.1186/s13012-016-0491-6
33. Fletcher J, Saunders-Smith T, Tsuyuki R, Hemmelgarn B, Tonelli M, Campbell D. Pharmacist and patient perspectives on recruitment strategies for randomized controlled trials: a qualitative analysis. BMC Med Res Methodol. 2020;20. doi:10.1186/s12874-020-01140-6
34. Kakumanu S, Manns BJ, Tran S, et al. Cost-effectiveness and efficacy of recruitment strategies used in a large pragmatic clinical trial targeting low-income seniors: a comparative descriptive analysis. Trials. 2019;20. doi:10.1186/s13063-019-3652-5
35. Emergence. Moxie; 2019. Available from: https://www.emergence-creative.com/moxie.
36. Marketwired. Introducing MOXIE, the first personalized communications platform that will improve your health; 2015.
37. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14(1):1–24. doi:10.1080/08870449908407311
38. Locus Health. Welcome to MOXIE! mymoxie.ca; 2020.
39. Gucciardi E, DeMelo M, Offenheim A, Stewart DE. Factors contributing to attrition behavior in diabetes self-management programs: a mixed method approach. BMC Health Serv Res. 2008;8(1):33. doi:10.1186/1472-6963-8-33
40. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
41. Figaro MK, Elasy T, BeLue R, Speroff T, Dittus R. Exploring socioeconomic variations in diabetes control strategies: impact of outcome expectations. J Natl Med Assoc. 2009;101(1):18–23. doi:10.1016/S0027-9684(15)30806-3
42. Sarkar U, Piette JD, Gonzales R, et al. Preferences for self-management support: findings from a survey of diabetes patients in safety-net health systems. Patient Educ Couns. 2008;70(1):102–110. doi:10.1016/j.pec.2007.09.008
43. Clouston SA, Manganello JA, Richards M. A life course approach to health literacy: the role of gender, educational attainment and lifetime cognitive capability. Age Ageing. 2017;46(3):493–499. doi:10.1093/ageing/afw229
44. Zou G. A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702–706. doi:10.1093/aje/kwh090
45. Persoskie A, Ferrer RA. A most odd ratio: interpreting and describing odds ratios. Am J Prev Med. 2017;52(2):224–228. doi:10.1016/j.amepre.2016.07.030
46. Knol MJ, Le Cessie S, Algra A, Vandenbroucke JP, Groenwold RHH. Overestimation of risk ratios by odds ratios in trials and cohort studies: alternatives to logistic regression. Can Med Assoc J. 2012;184(8):895. doi:10.1503/cmaj.101715
47. Merrill RM, Lindsay CA, Shields EC, Stoddard J. Perspective: have the focus and sophistication of research in health education changed? Health Educ Behav. 2007;34(1):10–25. doi:10.1177/1090198106288564
48. Orlandi MA, Landers C, Weston R, Haley N. Diffusion of health promotion innovations. In: Health Behavior and Health Education: Theory, Research, and Practice. San Francisco, CA, US: Jossey-Bass; 1990:288–313.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.