Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Factors Affecting the Qualification Rate of Hand Disinfection Among Physicians: A Cross-Sectional Survey
Authors Liu Y, Yuan S, Wang LY, Chen S, Li Y, Ma W
Received 8 August 2023
Accepted for publication 1 December 2023
Published 14 December 2023 Volume 2023:16 Pages 4091—4097
DOI https://doi.org/10.2147/JMDH.S430604
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yan Liu, Song Yuan, Li-Yi Wang, Si Chen, Yang Li, Wei Ma
Department of Infection Control, The Second Hospital of Hebei Medical University, Shijiazhuang, People’s Republic of China
Correspondence: Wei Ma, Department of Infection Control, The Second Hospital of Hebei Medical University, No. 215 of Heping West Road, Shijiazhuang, 050000, People’s Republic of China, Tel +86-18603297270, Fax +86 (311) 66007439, Email [email protected]
Objective: The objective of this study is to examine the qualification rate of hand disinfection in the surgical department wards and analyze the influencing factors.
Methods: A surprise assessment was carried out to evaluate the daily adherence to hand hygiene protocols in the surgical department wards. We aimed to investigate the factors that impact the qualification rate of hand disinfection.
Results: In this study, the qualification rate of hand disinfection was determined to be 64.38%. Notably, this rate exhibited significant variations based on gender, age, surgical site, and department category. Specifically, the qualification rate of hand disinfection among female participants stood at 82.35%, surpassing the qualification rate observed among male counterparts of 52.83%. Furthermore, doctors in the age group of 41– 50 years demonstrated the highest qualification rate, and the abdominal surgical site exhibited the most noteworthy qualification rate, reaching 79.49%. The outcomes of the multiple logistic regression analysis highlighted the significance of age and gender as influential factors impacting the qualification rate. Specifically, doctors aged 51 years or older exhibited the lowest hand hygiene compliance, whereas female doctors demonstrated a notably higher qualification rate compared to their male counterparts.
Conclusion: The disheartening qualification rate of hand disinfection highlights a concerning lack of awareness regarding hand hygiene among surgeons in their professional duties. Consequently, targeted interventions are imperative, focusing on intensified training, educational initiatives, enhanced supervision, and internal performance evaluations for key groups. The findings not only serve as a valuable database but also offer a viable roadmap for similar hospitals to reinforce the management of nosocomial infections.
Keywords: hand hygiene, hand disinfection, influencing factors, qualification rate, surgeons
Introduction
Nosocomial infections, often referred to as hospital-acquired infections, encompass infectious events that transpire during a patient’s stay in a healthcare facility. These infections originate from pathogens within the hospital environment, even though the actual onset of the infection may manifest after the patient’s discharge from the hospital. This definition excludes infectious events that have already occurred or are in a latent, pre-existing state before the patient’s admission to the hospital.1 Multiple clinical epidemiological studies have highlighted that the transmission of pathogenic bacteria through hand contact constitutes a significant factor contributing to the occurrence of nosocomial infections.1–4 Furthermore, it has been substantiated that the prevalence of nosocomial infections is intricately linked to the hand hygiene practices of healthcare professionals.5 Hand hygiene operations, encompassing both handwashing and hygienic hand disinfection, serve the purpose of mitigating the risk associated with the transmission of pathogenic bacteria by medical personnel during various procedures.6 Findings from related studies have consistently underscored that hand hygiene practices represent the most cost-effective, convenient, and efficacious measure for controlling nosocomial infections. It has been shown that stringent adherence to proper hand hygiene protocols can substantially reduce the incidence of nosocomial infections by nearly 30%.6–8 The Chinese health administrative authorities established management norms and fundamental guidelines for hand hygiene among medical workers in 2009, subsequently updated in the 2019 edition. Despite these efforts, the overall compliance rate for hand hygiene among medical workers in China remains relatively low. In this study, a field sampling survey was conducted in April 2020 to assess the daily implementation of hand hygiene in the wards of surgical departments. The survey was conducted without prior notification, with the objective of determining the qualification rate of hand disinfection among workers in surgical departments and providing recommendations to enhance hand hygiene compliance in the hospital.
Methods
Participants
In April 2020, clinical surgeons from various departments, including vascular surgery, glandular surgery, general surgery, gynecology, neurosurgery, and obstetrics, were chosen as participants for the study.
The inclusion criteria were as follows: (1) All participants were registered hospital staff members; (2) All participants held the position of attending doctors or higher; (3) All participants had the ability to provide medical services to patients independently; (4) At the time of sampling for this study, none of the participants had been in direct contact with patients or their clothing.
Exclusion criteria for the study were as follows: (1) Participants who were on leave or undergoing training outside the hospital; (2) Participants who were in internship, apprenticeship, or the standardized training period; (3) Participants who were engaged in relevant medical operations during the unannounced inspection on hand hygiene implementation.
Sampling methods
Hand skin samples from the medical staff were collected in the wards of each surgical department during patient examinations following a precise seven-step hand washing procedure. Specifically, the participants’ fingers were closed together, and cotton swabs moistened with sterile eluent (0.9% NaCl solution) containing a suitable neutralizing agent were used. The infection control department scraped the skin twice, moving from the heel to the end of the facies volaris of both hands. The swabs were then placed in test tubes after cutting off the operating end and promptly sent for testing.
Evaluation Indicator
The collected samples underwent a 48-hour incubation period on a nutrient agar plate at 37 °C. After incubation, the plates were examined, and colony counts were meticulously recorded. Hand disinfection was deemed qualified if the colony counts were less than or equal to 10/cm2. In contrast, counts exceeding 10/cm2 indicated unqualified hand disinfection. The qualification rate of hand disinfection was subsequently calculated based on these criteria.
Statistical Analysis
The survey data were meticulously organized and classified using Excel software, while the statistical analysis was conducted utilizing SPSS 19.0 software data package. The count data were represented as percentages (%), and differences among various data sets were assessed through one-way analysis employing the chi-square test. Items showing significant differences in the one-way analysis were further categorized and subjected to multiple logistic regression analysis to identify the influencing factors impacting hand hygiene compliance. The significance level for the tests was set at α = 0.05, and differences were deemed statistically significant when P < 0.05.
Results
General Information and the Distribution
This study encompassed a cohort of 87 doctors, comprising 53 males and 34 females. Within the cohort, there were 68 attending doctors and 19 associate chief doctors and above. Participants had varying years of professional experience: 33 had less than 5 years of experience, 28 had 5–10 years of experience, and 26 had ≥ 11 years of experience. There are 39 doctors who performed abdominal surgeries, 31 who performed head and spine surgeries, and 17 who performed vessel and thyroid gland surgeries. In terms of departmental classification, 32 doctors were from the department of obstetrics and gynecology, 31 doctors were from the department of neurosurgery, and 24 from other surgical departments (Table 1).
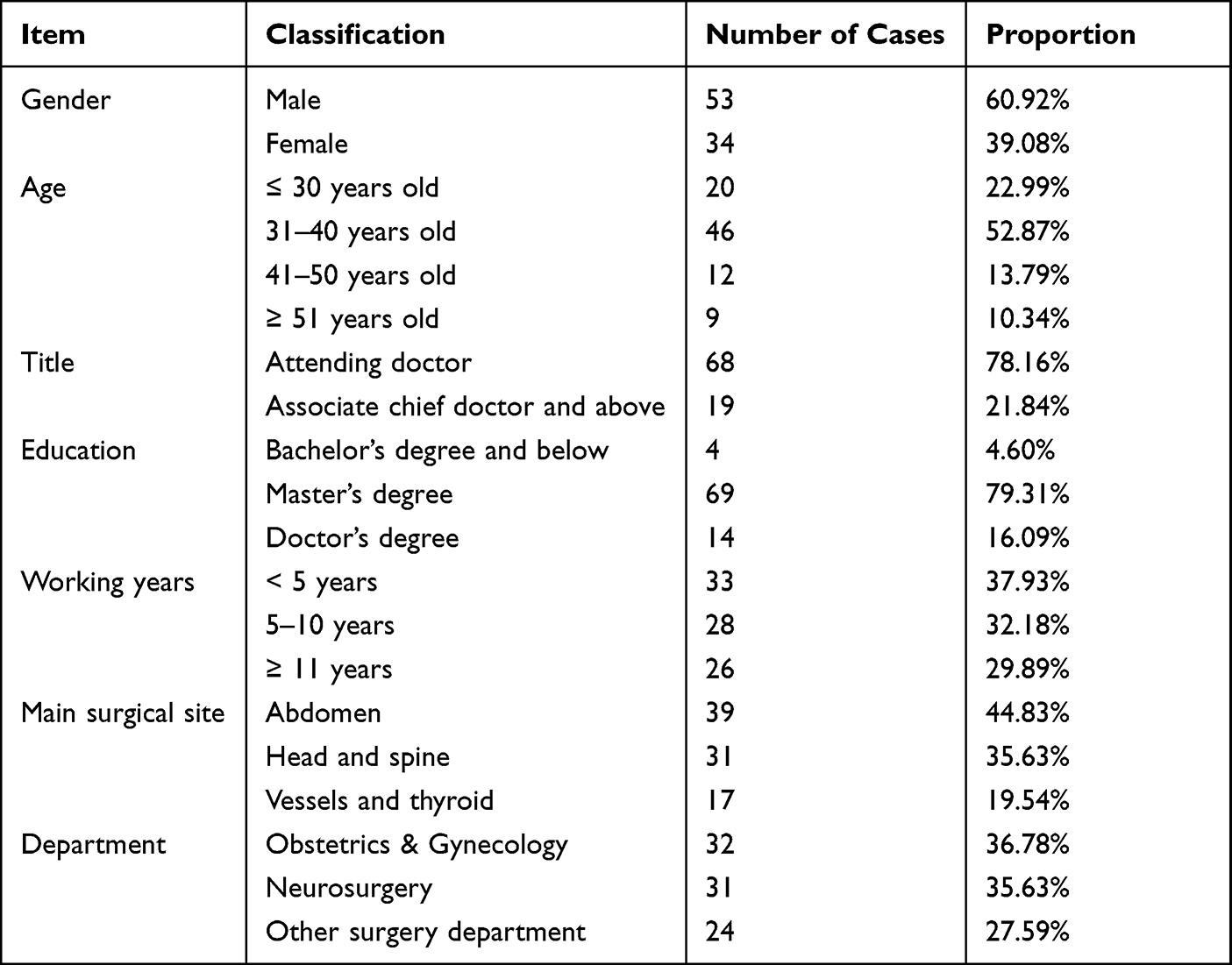 |
Table 1 General Data and the Composition Ratio of Doctors |
Comparative Analysis of the Qualification Rate of Hand Disinfection Among the Study Participants
In this cohort, the qualification rate of hand disinfection stood at 64.38% (56 out of 87 participants), displaying significant variations based on gender, age, surgical site, and department category. Female participants exhibited a higher qualification rate at 82.35% compared to their male counterparts at 52.83%. Notably, doctors aged between 41 and 50 years old achieved the highest qualification rate at 91.67%, while those aged 51 years and above had the lowest rate at 22.22%. The highest qualification rate was 79.49% for doctors whose primary operation site was the abdomen, while the lowest rate was only 35.29% for doctors whose primary operating site was vessels and thyroid. Table 2 displays the detailed comparison analysis of the qualification rate of hand disinfection.
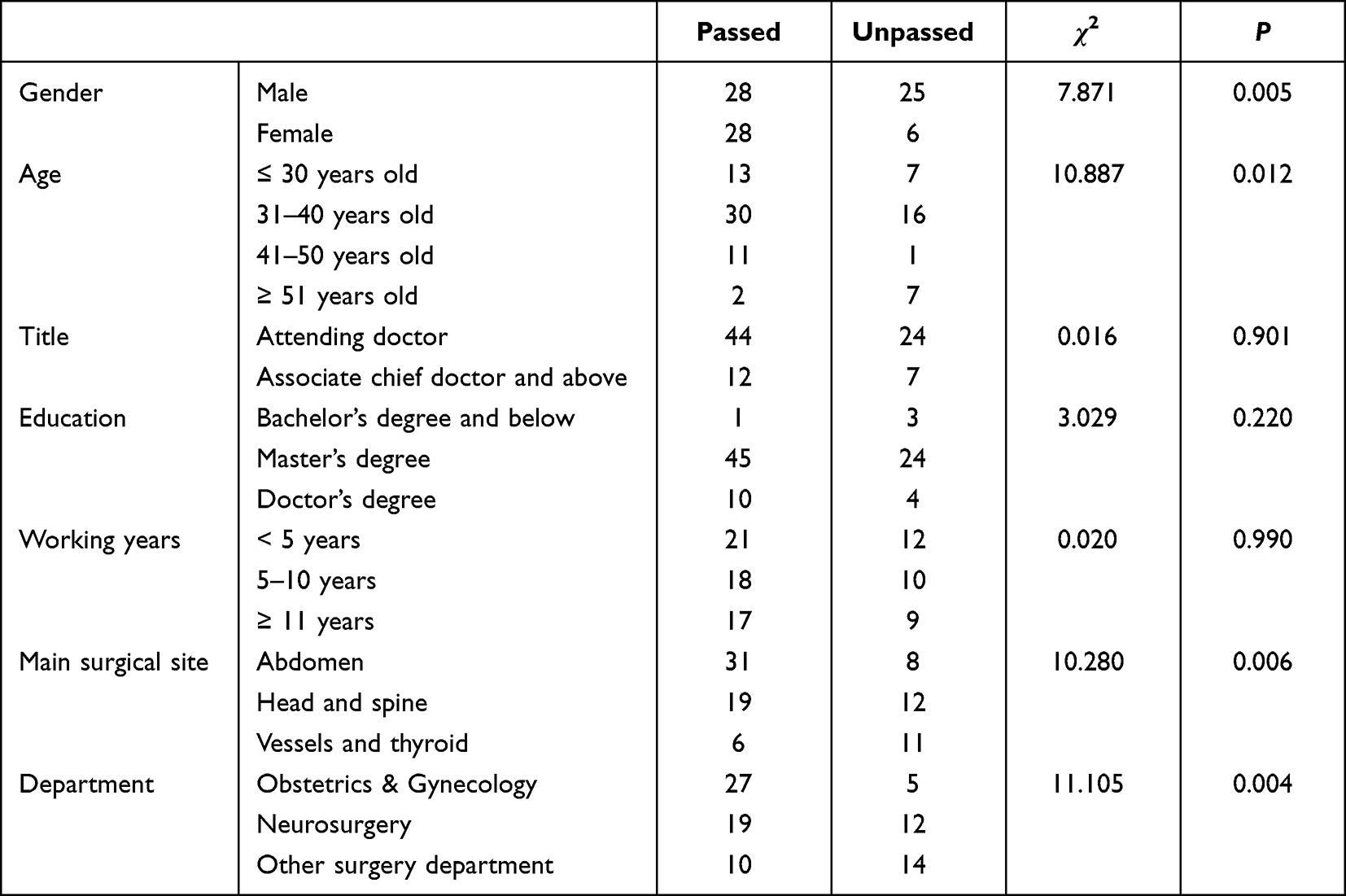 |
Table 2 The Comparative Analysis of Qualification Rate of Hand Disinfection |
Analysis of Factors Influencing the Qualification Rate of Hand Disinfection Among Surgeons
In the multiple logistic regression analysis, the variables showing differences in the univariate analysis were considered as independent variables, while the qualification status of hand disinfection served as the dependent variable. The results of the regression analysis indicated that age and gender significantly influenced hand hygiene compliance. Doctors aged 51 years and older exhibited the lowest hand hygiene compliance, with doctors aged 31–40 and 41–50 having 0.108 and 0.018 times higher rates of unqualified disinfection, respectively than those aged 51 and older. Female doctors also had 0.135 times more unqualified disinfections than their male counterparts. These findings emphasize the need for special attention and measures by the infection control department. The detailed results of the logistic regression analysis is presented in Table 3.
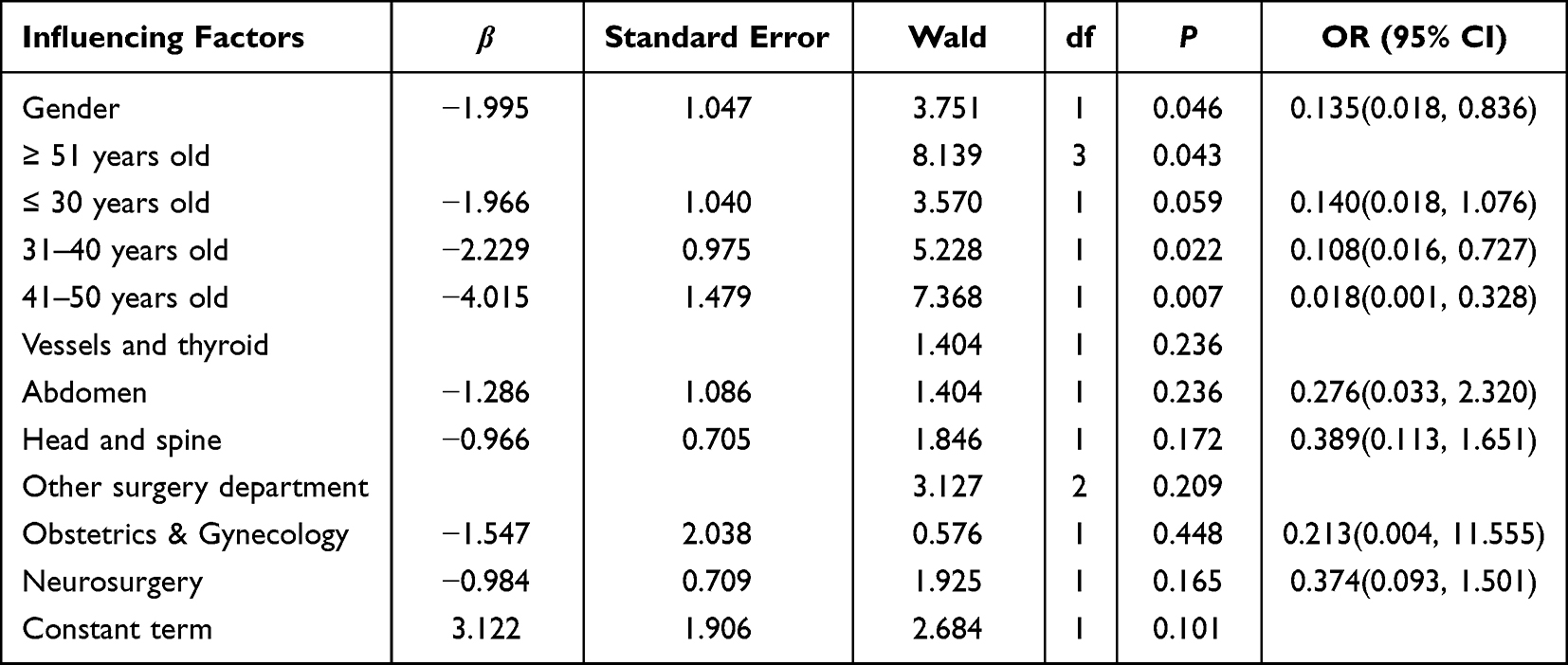 |
Table 3 The Results of Logistic Regression Analysis |
Discussion
Nosocomial infections pose a significant challenge to healthcare institutions in terms of public health.2,9 The findings of this study revealed a hand disinfection qualification rate of 64.38% among doctors, showing significant variations based on gender, age, surgical site, and department category Age and gender have proven to be significant factors affecting the qualification rate. Doctors aged 51 years or older exhibited the lowest compliance with hand hygiene, while female doctors demonstrated a significantly higher qualification rate compared to their male counterparts.
The hospital’s infection control department conducted an unannounced field sampling survey, ensuring unbiased results by avoiding any conscious increase in the number and quality of hand hygiene operations that might have occurred with prior notification. The compliance rate of hand hygiene before direct contact with patients was 100% based on bacterial culture results. However, the overall performance compliance rate was 64.38%, indicating suboptimal hand hygiene practices among surgeons in the hospital. This highlights the need for improvement in their standardized operations. Upon specific analysis, significant differences in hand hygiene compliance rates were observed across various demographic factors, including gender, age, surgical site, and department type. The qualification rate of hand disinfection among females was notably higher at 82.35%, in contrast to the 52.83% rate observed among males. This gender disparity aligns with previous research conducted by Chinese scholars in the same domain.10,11 In terms of age groups, doctors aged 41–50 years exhibited the highest qualification rate for hand disinfection at 91.67%. Following closely were doctors aged 31–40 years, with a rate of 65.22%, and doctors aged ≤ 30 years, with a rate of 65.00%. In stark contrast, doctors aged ≥ 51 years displayed the lowest qualification rate for hand disinfection, standing at a mere 22.22%. The findings of this study indicated that doctors at both ends of the age spectrum in our hospital exhibited the lowest compliance with hand hygiene, highlighting the occurrence of the phenomenon colloquially referred to as “poor head and tail”. Some potential reasons have been proposed:11,12 (1) Experienced surgeons often prioritize surgical technique as the primary factor contributing to successful surgery, leading them to overlook the significance of hand hygiene; (2) The doctors’ hands were utilized for bacterial count measurements during sample collection, potentially leading them to underestimate the importance of hand hygiene as they are already required to wear gloves before surgery to maintain aseptic conditions; (3) Junior doctors might not prioritize hand hygiene compliance due to limited exposure to relevant training and medical safety incidents, resulting in suboptimal hand hygiene practices. The highest qualification rate was 79.49% for doctors operating primarily in the abdomen, followed by the cranium and spine (61.29%) and vessels and thyroid (35.29%). The relatively high qualification rate of hand disinfection in abdominal surgeries could be attributed to the predominantly female composition of gynecology and obstetrics doctors, who tend to pay greater attention to hand hygiene due to their gender advantage. Additionally, neurosurgeons operating on cranial and spine sites may have a heightened awareness of hand hygiene and a higher qualification rate due to the elevated risk associated with their surgical procedures.
In addition, we conducted a multivariate regression analysis of the factors that could influence hand hygiene performance. The results of the multiple logistic regression analysis revealed that age and gender significantly influenced hand hygiene compliance. Doctors aged 51 years or older demonstrated the poorest hand hygiene performance, with those aged 31 to 40 and 41 to 50 exhibiting 0.108 and 0.018 times higher rates of passing hand hygiene compliance, respectively, compared to their older counterparts. Female doctors had a 0.135 times higher rate of passing hand hygiene performance than male doctors. Interestingly, the infection control department and internal quality control teams exhibited the highest hand hygiene compliance rates. To address the identified issues, the following preventive and control measures are recommended: (1) Enhance hand hygiene training for new and junior doctors. Mandatory courses on hand hygiene and nosocomial infection prevention should be implemented for these doctors. Increase the frequency and intensity of training and education, coupled with rigorous inspections, to establish a culture of meticulous hand hygiene founded on both awareness and practice. (2) In future sample surveys assessing the qualification rate of hand disinfection, it is advisable to increase the representation of male and senior doctors. As this demographic group has been identified to have the lowest hand disinfection qualification rate, their increased participation will heighten their awareness. Implementation of internal management measures, such as “reward and punishment”, alongside increased participation of male and senior doctors, will likely contribute to an overall improvement in the hand disinfection qualification rate. (3) Display hand hygiene posters prominently and ensure the availability of hand hygiene supplies. Research has shown that increasing psychological cues and simplifying operational methods can enhance medical workers’ compliance with hand hygiene protocols.13–17 In line with these findings, it is suggested that hospitals place hand hygiene posters in prominent locations and provide ample, user-friendly hand hygiene facilities for medical personnel. (4) Regular and unannounced hand hygiene inspections are essential to ensure compliance. The study results underline a concerning lack of hand hygiene awareness among doctors. Implementing internal notifications or management measures, such as withholding bonuses, may be necessary to enforce adherence to hand hygiene protocols, particularly for doctors who repeatedly fail to comply.
A limitation of this study is its relatively small sample size. To gain a more comprehensive understanding of the factors influencing hand hygiene implementation, it is crucial to expand the study’s sample size in future research. Additionally, the absence of data on the hand size of medical personnel could introduce potential bias to the results and should be considered in future studies to ensure accuracy and reliability.
Conclusions
In this study, an unannounced inspection was carried out to assess the qualification rate of hand disinfection among surgeons, and to analyze the influencing factors. The results revealed significant variations in the qualification rate based on gender, age, surgical site, and department category. Moreover, age and gender were identified as significant factors impacting the qualification rate, in this study. These insights are valuable for hospitals, enabling them to conduct focused hand hygiene inspections and implement corrective measures. The findings also offer valuable recommendations for enhancing hand hygiene management, especially in comparable hospital environments.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of the Second Hospital of Hebei Medical University. A written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from Hebei Medical Science Research Project Plan Project, Research on the Application of Logical Decision Algorithms for Polymorphic System Data Analysis in Hospital Infection Response Strategies and Quality Control (No.20210460).
Disclosure
None of the authors have any financial disclosure or conflicts of interest.
References
1. Pires D, Gayet-Ageron A, Guitart C, et al. Effect of wearing a novel electronic wearable device on hand hygiene compliance among health care workers: a stepped-wedge cluster randomized clinical trial. JAMA Netw Open. 2021;4(2):e2035331. doi:10.1001/jamanetworkopen.2020.35331
2. Bonine CJ. Strategies for promoting hand hygiene compliance on inpatient psychiatric units. J Psychosoc Nurs Ment Health Serv. 2021;59(5):21–24. doi:10.3928/02793695-20201013-09
3. Sadeghi-Moghaddam P, Arjmandnia M, Shokrollahi M, et al. Does training improve compliance with hand hygiene and decrease infections in the neonatal intensive care unit? A prospective study. J Neonatal Perinatal Med. 2015;8(3):221–225. doi:10.3233/NPM-15915001
4. Hong TS, Bush EC, Hauenstein MF, et al. A hand hygiene compliance check system: brief communication on a system to improve hand hygiene compliance in hospitals and reduce infection. J Med Syst. 2015;39(6):69. doi:10.1007/s10916-015-0253-z
5. Gedamu H, W/Giorgis T, Tesfa G, et al. Hand washing practice among health care workers in Ethiopia: systemic review and meta-analysis 2020. Heliyon. 2021;7(5):e06972. doi:10.1016/j.heliyon.2021.e06972
6. National Health Commission of the People’s Republic of China. Specification of Hand hygiene for healthcare workers, WST313-2019. Available from: http://www.nhc.gov.cn/fzs/s7852d/201912/70857a48398847258ed474ccd563caec/files/2cbd30e67c52445098c8db23eed0af0b.pdf
7. El Marjiya Villarreal S, Khan S, Oduwole M, et al. Can educational speech intervention improve visitors’ hand hygiene compliance? J Hosp Infect. 2020;104(4):414–418. doi:10.1016/j.jhin.2019.12.002
8. Demirel A. Improvement of hand hygiene compliance in a private hospital using the Plan-Do-Check-Act (PDCA) method. Pak J Med Sci. 2019;35(3):721–725. doi:10.12669/pjms.35.3.6
9. Wang T, Ju ZY, Liu AX. Analysis of influencing factors and intervention strategies for hand hygiene among medical personnel. Chin J Disinfect Sci. 2019;36(12):928–930+933.
10. Zheng S, Yang Q, Wang X, et al. Capability, opportunity, motivation, and hand hygiene behavior in healthcare workers: a structural equation modeling. Psychol Res Behav Manag. 2022;15:2219–2228. doi:10.2147/PRBM.S373287
11. Liang J, Wang Q, Wang J. Evaluation of the influence of ”Internet +” hand hygiene management model on medical staff’s hand hygiene compliance. Minerva Surg. 2023;78(2):214–216. doi:10.23736/S2724-5691.21.09097-3
12. Gould DJ, Creedon S, Jeanes A, et al. Impact of observing hand hygiene in practice and research: a methodological reconsideration. J Hosp Infect. 2017;95(2):169–174. doi:10.1016/j.jhin.2016.08.008
13. An B, Yang SJ. The evaluation of a multimodal hand hygiene improvement strategy in Cambodian hospitals. J Infect Dev Ctries. 2020;14(9):1047–1053. doi:10.3855/jidc.13090
14. Poulose V, Punithavathi A, Ali M, et al. Improving hand hygiene in a medical ward: a multifaceted approach. BMJ Open Qual. 2022;11(2):e001659. doi:10.1136/bmjoq-2021-001659
15. Adama BI. The impact of multimodal strategy intervention program on hand hygiene compliance at a University Teaching Hospital in Sierra Leone (Ola During Children’s Hospital). Infect Control Hosp Epidemiol. 2020;41(S1):S498–S499.
16. Tang K, Berthé F, Nackers F, et al. Hand hygiene compliance and environmental contamination with gram-negative bacilli in a rural hospital in Madarounfa, Niger. Trans R Soc Trop Med Hyg. 2019;113(12):749–756. doi:10.1093/trstmh/trz070
17. Daba C, Atamo A, Debela SA, et al. Observational assessment of hand hygiene compliance among healthcare workers in public hospitals of Northeastern Ethiopia. Int J Environ Health Res. 2023;23:1–11. doi:10.1080/09603123.2023.2168629
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.