")
Back to Journals » International Journal of General Medicine » Volume 16
Factors Affecting the Delay of intravenous Thrombolysis in Hyperacute Ischemic Stroke Patients: A Single Centre Study
Authors Amalia L
Received 21 March 2023
Accepted for publication 24 May 2023
Published 31 May 2023 Volume 2023:16 Pages 2157—2163
DOI https://doi.org/10.2147/IJGM.S412262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lisda Amalia
Department of Neurology, Faculty of Medicine, Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Lisda Amalia, Department of Neurology, Faculty of Medicine, Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital, Jl. Pasteur 38, Bandung, 40161, Indonesia, Email [email protected]
Introduction: Intravenous thrombolysis with r-tPA is the gold standard procedure in managing acute ischemic stroke recommended by the World Stroke Association, which is performed by injecting the drug r-tPA (Alteplase) intravenously. Generally, the preparation time to achieve thrombolysis is divided into pre-hospital and in-hospital. If this time can be shortened, the efficacy of thrombolysis can be increased. This study aims to determine the factors that can affect the delay in thrombolysis.
Methods: This is an analytic observational study with a retrospective cohort design in ischemic stroke confirmed by a neurologist at the neurology emergency unit of Hasan Sadikin Hospital (RSHS) from January 2021 to December 2021 and divided into two groups, delay and non-delay thrombolysis. A logistic regression test was performed to determine the independent predictor of delayed thrombolysis.
Results: There were 141 patients with an ischemic stroke diagnosis confirmed by a neurologist at the neurological emergency unit at Hasan Sadikin Hospital (RSHS) from January 2021 to December 2021. A total of 118 (83.69%) patients were included in the “delay” category, while 23 (16.31%) patients were included in the “non-delay” category. Patients included in the “delay” category had an average age of 58.29+11.19 years with a male-to-female sex ratio of 57%, while patients included in the “non-delay” category had an average age of 55.57+15.55 years with a male-to-female sex ratio of 66%. The NIHSS admission score was a significant risk factor for delayed thrombolysis. Through multiple logistic regression, it was found that age, onset, female gender, NIHSS admission score, and NIHSS discharge score were independent predictors of delayed thrombolysis. However, all of them were not statistically significant.
Conclusion: Gender, risk factors for dyslipidemia, and arrival onset are independent predictors of delayed thrombolysis. Prehospital factors contribute relatively more to the delay in thrombolytic action.
Keywords: factor, hyperacute, ischemic, stroke, thrombolysis
Introduction
According to the World Health Organization (WHO), stroke is a clinical sign that develops rapidly from focal or global cerebral dysfunction, lasts more than 24 hours or causes death, and occurs without any apparent cause other than vascular causes. A stroke occurs when blood flow to the brain is lost due to blockage or rupture of blood vessels, resulting in a lack of oxygen and sudden death of some brain cells. Stroke is a neurological emergency that is the 3rd cause of death and disability in the world. Stroke is generally divided into ischemic stroke (80%) and hemorrhagic (20%).1,2
Ischemic stroke is a disease that begins with a series of changes in the brain which, if not treated immediately, can cause the death of the affected part of the brain. Ischemic stroke is caused by obstruction or cessation of blood supply to the brain. Failure to supply blood will cause impaired function of the brain or in which nerve cell death (necrosis) has occurred.3,4 In the early minutes to several hours after the onset of neurological dysfunction in stroke patients is the only time of opportunity to prevent death or permanent disability so that it becomes a target for prompt and appropriate treatment for stroke patients in that period so that acute stroke management becomes optimal. Most of the causes of stroke is a blood clot that clogs the arteries that supply the brain, so the administration of clot-busting agents (thrombolytics) is considered an effort that can reduce the damage from ischemia by returning blood flow to normal. A high rate of clinical improvement is achieved when blood flow is restored soon after the blockage occurs. The most widely used agent, approved for use, is a thrombolytic agent with recombinant tissue plasminogen activator (r-tPA).5,6
Intravenous thrombolysis with r-tPA is the gold standard procedure in managing acute ischemic stroke recommended by the World Stroke Association, which is performed by injecting the drug r-tPA (Alteplase) intravenously. Patients who are candidates for r-tPA recipients are screened according to inclusion and exclusion criteria based on standard operating procedures and existing guidelines. In general, the preparation time to achieve thrombolysis is divided into two, namely the time from onset to hospital admission (onset-to-door-time [ODT]) or pre-hospital and from the time the patient enters the emergency room until the thrombolysis drug is administered (door-to-needle time [DNT]) or in-hospital. If this time can be shortened, the efficacy of thrombolysis can increase.6,7 However, in a study conducted in Wuhan, only 9.81% of patients in 2020 and 8.12% of patients in 2019 met the criteria for thrombolysis.3
From the onset to hospital admission (onset-to-door-time [ODT]) or pre-hospital, awareness and knowledge of patients and families are needed to recognize the symptoms of a stroke. Awareness of symptoms and their severity, willingness to take them to the hospital immediately without waiting for symptoms to improve, distance from home, availability of an ambulance or vehicle, and referral system can affect during this time. Some patients and their families may not recognize a stroke’s early signs and symptoms. In contrast, others may recognize the symptoms and signs of a stroke and realize the importance of first treatment at the hospital to immediately take the patient to the hospital. The behavior of patients or other families towards stroke with mild symptoms tends to wait for symptom improvement rather than directly taking the patient to the hospital. Long distances and limited transportation modalities can also extend the time to arrive at the hospital. A good referral system between hospitals can speed up preparation time for thrombolysis.8–13
The time from the emergency room door until the thrombolysis drug is given (door-to-needle time [DNT]) or in-hospital is also influenced by several internal factors in the hospital, namely triage efficiency, efficiency of multidisciplinary acute stroke services, and informed consent to patients or families regarding thrombolysis. Triage requires varying times in carrying out emergency treatment screening so that appropriate screening for recognizing stroke and acute stroke codes can be carried out immediately.11–17 If this time can be shortened, then the efficacy of thrombolysis can be increased. This study aims to determine the factors that can affect the delay in thrombolysis.
Methods
This is an analytic observational study with a retrospective cohort design in 141 patients with a diagnosis of ischemic stroke enforced by a neurologist at the emergency department on admission of neurology at Hasan Sadikin Hospital (RSHS), during the period from January 2021 to December 2021. Patients were categorized into two categories; namely, patients with the “delay” category were defined as patients who experienced delayed thrombolysis (thrombolysis time > 60 minutes). In contrast, patients with the “non-delay” category were defined as patients who do not experience delayed thrombolysis (thrombolysis time < 60 minutes).
Retrieval of medical record data will be carried out following the ethical provisions of Hasan Sadikin Hospital by maintaining the confidentiality of the patient. Demographic data, clinical characteristics, rt-PA screening, and ischemic stroke outcomes will be recorded and further analyzed to determine the factors that affect thrombolysis delay. Risk factors such as lipid profile and uric acid level were performed for study subjects. Factors that can be intervened will be improved so that hyperacute ischemic stroke services can run optimally. Statistical analysis used univariate analysis and a logistic regression test by estimating the Odds Ratio (OR) parameter.
The study was conducted after obtaining ethical approval from the research ethics committee of RSUP Dr. Hasan Sadikin Bandung (LB.02.01/X.6.5/403/2022). This study complied with all relevant ethical regulations (including The Declaration of Helsinki). All patients had obtained written informed consent.
Results
There were 141 patients diagnosed with ischemic stroke enforced by a neurologist at the neurology emergency unit of Hasan Sadikin Hospital (RSHS) from January 2021 to December 2021. 118 (83.69%) patients were included in the “delay” category. In comparison, 23 (16.31%) patients were included in the ‘non-delay’ patients category. Patients included in the “delay” category had an average age of 58.29 + 11.19 years with a male to a female sex ratio of 57%, while patients included in the “non-delay” category had an average age of 55.57+15.55 years with a male to a female sex ratio of 66% (Table 1). In patients with the “delay” category, hypertension was the most common risk factor, experienced by 80 (67.8%) patients, followed by dyslipidemia in 51 (43.2%) patients. Whereas, in patients in the “non-delay” category, hypertension was also the most common risk factor, experienced in 13 (56.5%) patients, followed by smoking in 6 (26.1%) patients. Patient demographic characteristics are shown in Table 1 as follows. There was a significant effect on gender and risk factors for dyslipidemia and hyperuricemia on delayed thrombolysis (p<0.05). Both age and risk factors such as hypertension, hypercoagulation, diabetes mellitus, smoking, rheumatic heart disease, previous stroke episodes, atrial fibrillation, chronic kidney disease, and coronary heart disease did not have a statistically significant effect on thrombolysis delay. The average time from onset to hospital admission in the “delay” category of patients was 39.97+64.30 hours, while in patients with the “non-delay” category, it was 3.11+0.94 hours. In both “delay” and “non-delay” patients, weak limbs were found to be the most common clinical manifestation in 113 (95.76%) patients and 22 (95.65%) patients, respectively. The mean score of the National Institutes of Health Stroke Scale (NIHSS) for admission in patients with the “delay” category was 10.65 + 5.08, while in patients with the “non-delay” category, it was 11.96 + 5.00 hours. The mean score of the National Institutes of Health Stroke Scale (NIHSS) for discharge in patients in the “delay” category was 4.82 + 4.55, while in patients in the “non-delay” category, it was 4.7 + 4.96 hours. Obtaining the onset of arrival is a significant factor for the delay in diagnosis (p <0.05). Both clinical manifestations, admission NIHSS score, and discharge NIHSS score had no statistically significant effect on thrombolysis delay. The clinical characteristics of the patients are shown in Table 2.
 |
Table 1 Demographic Characteristics of Ischemic Stroke Patients |
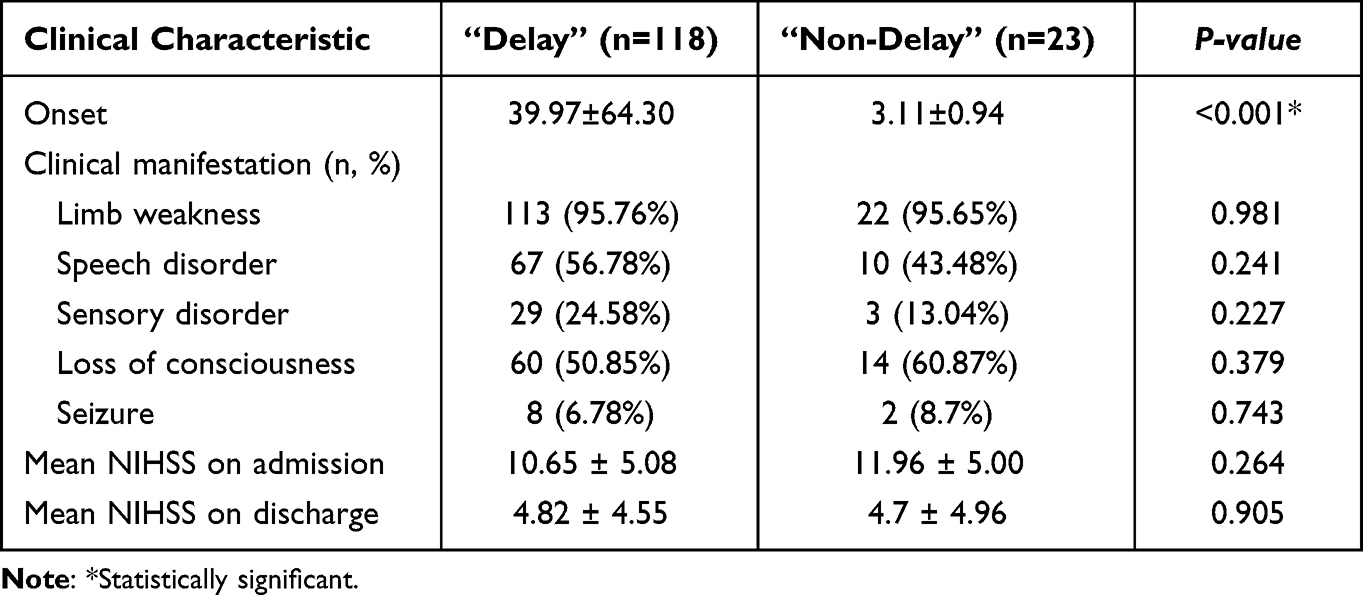 |
Table 2 Clinical Characteristics of Intravenous Thrombolysis Patients |
For factors that have a p-value <0.05, multiple logistic regression tests were performed to determine the independent predictor factors for delayed thrombolysis. It was found that male gender, risk factors for dyslipidemia, and arrival onset were independent predictors of delayed thrombolysis (Table 3).
 |
Table 3 Regression Logistics of Delayed Intravenous Thrombolysis Patients |
Discussion
In this study, it was found that the onset of the arrival of patients was significantly related to delayed thrombolysis (p <0.001), where the rapid onset of arrival tended not to delay thrombolysis. In contrast, the long onset of arrival managed to delay thrombolysis. This is different from the research conducted by Erqing Chai et al. Thrombolysis time or onset-to-door is an independent risk factor associated with delayed thrombolysis in patients undergoing rt-PA at the Department of Cerebrovascular Disease Center of Gansu Provincial Hospital, in addition to NIHSS score and decision time. The study states that there is an inverse relationship between the onset of arrival and thrombolysis time, known as the “3-hour effect”. The door-to-needle time between patients in the hospital with a beginning of arrival at the start of the window period was longer than that of patients with a beginning of the arrival of almost 3 hours. In that study, the ‘3-hour effect’ could significantly impair thrombolysis time, a decision related to the degree of emergency perceived by physicians. Physicians pay more attention to critically ill patients with an onset close to the window period.14,18
In this study, there was no significant relationship between clinical manifestations and thrombolysis time, but clinical manifestations tended to have a higher rate in patients with delayed thrombolysis. This is the same as a study by Chai et al which stated that patients with a shorter symptom progression time had a longer thrombolysis time and were treated with less urgency. It is known that the effect of intravenous thrombolysis decreases significantly with increasing time from onset to the needle. However, these results can be a wrong assumption because there were significant population differences between delayed and non-delay patients in this study.14
The NIHSS score is also an independent risk factor associated with delayed thrombolysis.14 The NIHSS score is a relatively universal and concise stroke rating scale worldwide, especially for evaluating neurological deficits in treating acute ischemic stroke.19 The NIHSS score level can more accurately reflect the patient’s clinical situation intuitively.20,21 In our study, patients with higher admission NIHSS scores had a lower risk of hospital delay although not statistically significantly related, which could be explained by the fact that clinical manifestations of severe signs and symptoms can easily it is easy to convince family members and those closest to them to immediately take acute ischemic stroke patients to the hospital to get further emergency treatment from a doctor. Patients with a higher NIHSS score undergo an examination as soon as the patient arrives at the hospital, thereby reducing the risk of delayed thrombolysis.14
In this study, hypertension was a risk factor experienced by most patients undergoing rt-PA. Patients who experience delayed thrombolysis have a higher proportion of hypertension than those who do not share delayed thrombolysis. This is the same as the study by Mowla et al, which stated that severe hypertension significantly contributes to slowing thrombolysis. Blood pressure above 185/110 mm Hg on arrival is a contraindication to thrombolysis. In that study, investigators did not actively reduce hypertension >185/110 mmHg at triage when acute ischemic stroke was suspected. Lowering blood pressure could significantly decrease brain tissue perfusion, leading to further ischemic compromise. Instead, the investigators monitored blood pressure closely until the thrombolysis. If there was no spontaneous fall below 185/110 mm Hg, the first dose of antihypertensives was administered in the ED before thrombolysis. This causes hypertensive patients to experience delayed thrombolysis potentially.22,23
Based on the results of multiple logistic regression tests, it was found that gender and dyslipidemia were independent predictors of delayed thrombolysis with statistically significant effects. In contrast, the onset of arrival and hyperuricemia were independent predictors of delayed thrombolysis, with results that were not statistically significant. The potential causes of delayed thrombolytic therapy are numerous and can be divided into two categories, namely pre-hospital and in-hospital factors, from symptom onset to treatment administration. Prehospital factors contribute relatively more to the delay. Many delays are multifactorial, ranging from factors related to the patient, transportation, and referral systems to delays in and out of the hospital. For example, delayed symptom recognition is more likely with increasing distance from the care center and at lower priority triage which is more likely if the symptoms observed in the patient are atypical.24
Delay in contacting emergency medical services has been found to contribute to more than half of cases of prehospital delay,25 which may result from the patient’s or family’s perception that the symptoms are not severe enough to warrant a visit to the health care facility and medical treatment26,27 or that the symptoms28,29 More severe stroke symptoms were correlated with an earlier presentation to the emergency department than those that resolved rapidly, or mild, symptoms were associated with a delay in patient presentation to the emergency department (ED).25
Female gender is thought to be associated with the late presentation of patients to the ED, which is inversely proportional to the results of this study. However, relevant studies do not control for the age factor, namely female patients who visit the emergency department due to acute ischemic stroke are older than male patients.30,31 Living alone is also an independent predictor factor associated with delay in patient presentation to the emergency room 30 which shows results relatively similar to an older age.32,33 Older people more often live alone and have strokes without realizing it. Living alone makes seeking care difficult and also delays the process of referral and diagnosis.30
In-hospital factors can be divided into delays in assessment, uncertainties associated with imaging, and delays related to decision-making and administration of thrombolysis.24 In this study, it was found that relatively younger patients presenting to the ED with acute stroke were more likely to receive thrombolytic therapy compared to older patients. However, younger patients are more likely to experience a delay in diagnosis because stroke presentation is less common in a relatively younger age range, and the presence of atypical presentations is more likely to occur in a relatively younger age group,34 so treatment with thrombolysis may be delayed for done.35
Several studies evaluate the usefulness of coordinated stroke warning systems and their effect on thrombolysis time. A Swedish national survey of 49,907 patients admitted with acute stroke over two years found a decrease in delayed thrombolysis time and an increase in the thrombolysis rate in cases of stroke alert when compared with cases in which stroke alerts or stroke alerts were not activated.36
One solution to improve the emergency room administration system to shorten Door-to-Needle (DNT) at RSHS is to have a running “Code Stroke”. Code Stroke is a rapid response system to treat acute ischemic stroke patients by getting immediate therapy so that the outcomes obtained are effective and maximum. Code Stroke aims to prioritize and expedite services to diagnose and provide management of hyperacute stroke cases, specifically hyperacute ischemic stroke cases, which are candidates for intravenous thrombolysis and is expected to shorten administration time in the emergency room.
Conclusion
Male gender, risk factors for dyslipidemia, and arrival onset are independent predictors of delayed thrombolysis. Prehospital factors contribute relatively more to the delay in thrombolytic action. Further research needs to be done on what factors influence the delay in intravenous thrombolysis, whether awareness about stroke or access to hyper acute stroke services.
Data Sharing Statement
No additional data is available.
Funding
No funding research.
Disclosure
There is no competing interest.
References
1. Thrift AG, Cadilhac DA, Thayabaranathan T, et al. Global stroke statistics. Int J Stroke. 2014;9(1):6–18. doi:10.1111/ijs.12245
2. Feigin VL, Stark BA, Johnson CO, et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):1–26. doi:10.1016/S1474-4422(21)00252-0
3. Ross I. Caplan’s stroke: a clinical approach. JAMA. 2011;305:99. doi:10.1001/jama.2010.1941
4. Kuriakose D, Xiao Z. IMP para qué es el ictus, tipos y causas. También para datos epidemiológicos y tratamientos. Int J Mol Sci. 2020;21(20):1–24.
5. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:344–418. doi:10.1161/STROKEAHA.118.022606
6. Herpich F, Rincon F. Management of acute ischemic stroke. Crit Care Med. 2020;48(11):1654–1663. doi:10.1097/CCM.0000000000004597
7. Permenkes 2019 RI No. 43. Pedoman nasional pelayanan kesehatan [National Guideline Health Services]; 2019 :1–13. Indonesian.
8. Haki C, Cetiner M, Kaya H. Factors affecting the arrival time to hospital of patients with acute ischemic stroke. Sanamed. 2020;15(2):145–151. doi:10.24125/sanamed.v15i2.419
9. Al Khathaami AM, Mohammad YO, Alibrahim FS, Jradi HA. Factors associated with late arrival of acute stroke patients to emergency department in Saudi Arabia. SAGE Open Med. 2018;6:205031211877671. doi:10.1177/2050312118776719
10. Kim YS, Park SS, Bae HJ, et al. Stroke awareness decreases prehospital delay after acute ischemic stroke in Korea. BMC Neurol. 2011;11:11. doi:10.1186/1471-2377-11-11
11. Mahmoud Hewedi K, El Din Tharwat Mohamed M, Awad Yousef Abo Sleem M. Pre hospital and in hospital delays after the onset of acute ischemic stroke in a sample of Egyptian patients. Al-Azhar Med J. 2019;48(4):311–322. doi:10.21608/amj.2019.64940
12. Abraham S, Krishnan S, Thaha F, et al. Factors delaying management of acute stroke: an Indian scenario. Int J Crit Illn Inj Sci. 2017;7(4):224–230. doi:10.4103/IJCIIS.IJCIIS_20_17
13. Eissa A, Krass I, Bajorek BV. Barriers to the utilization of thrombolysis for acute ischaemic stroke. J Clin Pharm Ther. 2012;37(4):399–409. doi:10.1111/j.1365-2710.2011.01329.x
14. Chai E, Li C, Jiang L. Factors affecting in-hospital delay of intravenous thrombolysis for acute ischemic stroke A retrospective cohort study. Medicine. 2019;98(19):1–4. doi:10.1097/MD.0000000000015422
15. Huang Q, Ma QF, Feng J, et al. Factors associated with in-hospital delay in intravenous thrombolysis for acute ischemic stroke: lessons from China. PLoS One. 2015;10(11):1–9. doi:10.1371/journal.pone.0143145
16. Lachkhem Y, Rican S, Minvielle É. Understanding delays in acute stroke care: a systematic review of reviews. Eur J Public Health. 2018;28(3):426–433. doi:10.1093/eurpub/cky066
17. Mikulík R, Kadlecová P, Czlonkowska A, et al. Factors influencing in-hospital delay in treatment with intravenous thrombolysis. Stroke. 2012;43(6):1578–1583. doi:10.1161/STROKEAHA.111.644120
18. Thrombolysis I, Nedeltchev K, Arnold M, et al. Pre- and in-hospital delays from stroke onset to intra-arterial thrombolysis. Stroke. 2003;34:1230–1234. doi:10.1161/01.STR.0000069164.91268.99
19. Wang R, Zeng J, Chen X, et al. Risk factors of hemorrhagic transformation after intravenous thrombolysis with rt-PA in acute cerebral infarction. QJM. 2018;112:323–326.
20. Garcia Pastor A, Diaz Otero F, Gil Navarro S, et al. Vascular imaging before intravenous thrombolysis: consequences of in-hospital delay in applying two diagnostic procedures. J Neuroimaging. 2015;25:397–402. doi:10.1111/jon.12148
21. Huang Q, Ma QF, Jia JP, et al. Referral leads to prehospital delay of intravenous thrombolysis for acute ischemic stroke in Beijing. Int J Stroke. 2015;10:E80–E81. doi:10.1111/ijs.12568
22. McKay C, Hall AB, Cortes J. Time to blood pressure control before thrombolytic therapy in patients with acute ischemic stroke: comparison of labetalol, nicardipine, and hydralazine. J Neurosci Nurs. 2015;47:327–332. doi:10.1097/JNN.0000000000000170
23. Mowla A, Doyle J, Lail NS, et al. Delays in door-to-needle time for acute ischemic stroke in the emergency department: a comprehensive stroke center experience. J Neurol Sci. 2017;376:102–105. PMID: 28431590. doi:10.1016/j.jns.2017.03.003
24. Sharobeam A, Jones B, Walton-Sonda D, et al. Factors delaying intravenous thrombolytic therapy in acute ischaemic stroke: a systematic review of the literature. J Neurol. 2021;268(8):2723–2734. doi:10.1007/s00415-020-09803-6
25. Faiz KW, Sundseth A, Thommessen B, et al. Factors related to decision delay in acute stroke. J Stroke Cerebrovasc Dis. 2014;23(3):534–539. doi:10.1016/j.jstrokecerebrovasdis.2013.05.007
26. Gu HQ, Rao ZZ, Yang X, et al. Use of emergency medical services and timely treatment among ischemic stroke. Stroke. 2019;50(4):1013–1016. doi:10.1161/STROKEAHA.118.024232
27. De Silva DA, Yassin N, Toh AJ, et al. Timing of arrival to a tertiary hospital after acute ischaemic stroke—a follow-up survey 5 years later. Ann Acad Med Singap. 2010;39(7):513–515. doi:10.47102/annals-acadmedsg.V39N7p513
28. Vidale S, Beghi E, Gerardi F, et al. Time to hospital admission and start of treatment in patients with ischemic stroke in northern Italy and predictors of delay. Eur Neurol. 2013;70(5–6):349–355. doi:10.1159/000353300
29. Faiz KW, Sundseth A, Thommessen B, et al. Reasons for low thrombolysis rate in a Norwegian ischemic stroke population. Neurol Sci. 2014;35(12):1977–1982. doi:10.1007/s10072-014-1876-4
30. de Ridder I, Dirks M, Niessen L, et al. Unequal access to treatment with intravenous alteplase for women with acute ischemic stroke. Stroke. 2013;44(9):2610–2612. doi:10.1161/STROKEAHA.113.002263
31. Madsen TE, Sucharew H, Katz B, et al. Gender and time to arrival among ischemic stroke patients in the Greater Cincinnati/Northern Kentucky Stroke Study. J Stroke Cerebrovasc Dis. 2016;25(3):504–510. doi:10.1016/j.jstrokecerebrovasdis.2015.10.026
32. Yanagida TFS, Inoue T, Suzuki S. Causes of prehospital delay in stroke patients in an urban ageing society. J Clin Gerontol Geriatr. 2014;5(3):77–81. doi:10.1016/j.jcgg.2014.02.001
33. Birnbaum LA, Rodriguez JS, Topel CH, et al. Older stroke patients with high stroke scores have delayed door-to-needle times. J Stroke Cerebrovasc Dis. 2016;25(11):2668–2672. doi:10.1016/j.jstrokecerebrovasdis.2016.07.013
34. Singhal AB, Biller J, Elkind MS, et al. Recognition and management of stroke in young adults and adolescents. Neurology. 2013;81(12):1089–1097. doi:10.1212/WNL.0b013e3182a4a451
35. Dodds JA, Xian Y, Sheng S, et al. Thrombolysis in young adults with stroke: findings from get with the guidelines-stroke. Neurology. 2019;92(24):e2784–e2792. doi:10.1212/WNL.0000000000007653
36. Eriksson M, Glader EL, Norrving B, Stegmayr B, Asplund K. Acute stroke alert activation, emergency service use, and reperfusion therapy in Sweden. Brain Behav. 2017;7(4):e00654. doi:10.1002/brb3.654
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.