Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Factors Affecting Infection Control Performance of School Health Nurses During the COVID-19 Pandemic in South Korea
Received 3 January 2022
Accepted for publication 29 March 2022
Published 19 April 2022 Volume 2022:15 Pages 805—814
DOI https://doi.org/10.2147/JMDH.S356939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mi-Ra Yim,1 Boyoung Kim2
1Tongyeong Jungang Middle School, Tongyeong, South Korea; 2College of Nursing, Chonnam National University, Gwangju, South Korea
Correspondence: Boyoung Kim, Tel +82-62-530-4936, Email [email protected]
Purpose: Many patients with coronavirus disease 2019 (COVID-19) are asymptomatic or infected by unclear infection routes. Significant group infections may result from transmission in schools, and thus, it is necessary to improve infection control efficiency in schools by identifying the factors associated with the performance of COVID-19 infection control by school health nurses.
Methods: The participants were 130 school health nurses in Korea. The survey variables included knowledge of COVID-19, infection control attitude, job stress, and school organizational culture.
Results: The results demonstrated that among the variables, infection control attitude, job stress, and the level of infection control in schools perceived by school health nurses were significant. The explanatory power of the model including these variables was 25.8% (F=14.39, p< 0.001, R2=0.255, Adj-R2=0.258).
Conclusion: The results showed that the infection control attitude and job stress of school health nurses had a significant effect on their infection control performance during the COVID-19 pandemic. The results will be used as basic data for developing programs to enhance the competence of school health nurses to manage new infectious diseases.
Keywords: infection, knowledge of COVID-19, job stress, organizational culture, COVID-19, school health nurse
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has changed everyday life, and the school life of children is no exception.1 To ensure safety and learning rights of the students, the Korean Ministry of Education decided to begin the new school year with online classes.2 As of 2021, the Ministry of Education developed plans for flexible management of academic affairs, including elementary school students attending school in turn, and middle and high school students attending school every other week for selected grades.3 Since Korean schools reopened in March 2021 after the COVID-19-related closure, the infection rate has been 3.49 per 100,000 students.4 Despite the initiation of vaccination drives for high school seniors and education workers, the COVID-19 infection rate still corresponds to a national infectious disease crisis level. Therefore, intensive prevention and control measures in schools remain necessary.5
Particularly, owing to the overcrowding in schools, there is a possibility of rapid transmission of infectious diseases, raising concerns about “silent spreader groups”.6,7 School health teachers play a significant role in such circumstances, because they are responsible for infection control. If confirmed cases occur at schools, temporary COVID-19 screening centers are set up, and in-person learning is substituted with online classes. Health teachers’ workload increases considerably because of the need to test and observe the students, teachers, and staff.8 As an infection control tower, health teachers manage confirmed and suspected cases, provide prevention education, and manage quarantine supplies and activities. Relevant knowledge is essential for performing safe and high-quality infection control.9 Inadequate knowledge can directly influence behavior and lead to delayed diagnosis, poor infection control practice, and rapid spread of the disease.10 As systematic infection control training can make a difference in knowledge and performance to prevent infections,11 determining whether health teachers have adequate knowledge is essential for providing systematic training.
Additionally, the outbreak of infectious diseases is related to the attitude toward and performance of infection control. Positive attitudes toward infection control can increase compliance with infection control practices;12 that is, one must have the right knowledge and attitude for the desired behavior to occur.13 Health teachers must have adequate knowledge related to COVID-19 to provide relevant information and education to students, parents, and school staff. Moreover, infection control based on positive attitudes can contribute to preventing and reducing the spread of infectious diseases.14 However, since schools are overcrowded, they mainly rely on mask wearing and body temperature checks amid the imposition of strict social distancing measures. The job pressure of health teachers is increasing, along with their educational, environmental, and administrative workloads.
School organizational culture refers to elements that encompass the basic assumptions, beliefs, values, attitudes, behavioral norms, symbols, and semantics that members naturally share through repeated experiences in the external environment and internal problem-solving processes that affect the lives and behaviors of school members.15 While performing infection control, the work environment of school organizations can directly or indirectly affect the behavior of health nurses, who accept and implement changes.16 Therefore, school organizational culture, comprising components such as cohesion, professional competence, cooperation, expectations for the organization, and decision-making processes of school members, can be a significant predictor of health nurses’ infection control performance. This study investigated the factors associated with health nurses’ infection control performance during the COVID-19 pandemic to provide basic management data.
Method
Design and Participants
This study employed a descriptive correlational design. A convenience sample of health nurses was selected using the following inclusion criteria: 1) working at elementary, middle, and high schools in Korea, 2) experienced in performing infection control activities related to COVID-19 in school environments, and 3) understood the purpose and method of the study and agreed to participate.
Procedures
Data were collected online from February 26 to April 7, 2021, after obtaining approval from Gyeongsang National University’s Institutional Review Board (GIRB-A21-Y-0009). The first and corresponding authors received IRB approval while attending Gyeongsang National University. During this period, the Korean government had imposed strict social distancing measures, based on reports of over 500 new cases every day and growing concerns about a fourth wave. Hence, online surveys were conducted by posting Google forms link on online bulletin boards for health teachers in three provinces nationwide. The survey had a consent form that explained the study’s purpose, necessity, and method, and assured anonymity and confidentiality of the participants. They were informed that they could withdraw at any time. Only those who agreed to participate answered the survey, and received coupons as a token of appreciation.
Measures
General and job-related characteristics were measured using 13 multiple-choice questions: age, final education, teaching experience, nursing (clinical) experience, school location, health class status, experience transferring students/staff to screening centers, experience with confirmed cases, self-diagnosis, thermal imaging camera installation and body temperature measurement, level of infection control perceived by public health teachers, and effective ways to prevent COVID-19.
Knowledge of COVID-19 was measured using an instrument developed by Yoon17 for nurses. It was revised for this study to reflect the 7th edition of the COVID-19 response guidelines by the Korea Disease Control and Prevention Agency.18 The tool comprises 23 questions. Scores ranged from 0 to 23 (incorrect answers 0, correct answers 1); the higher the score, the higher the knowledge level. Kuder-Richardson Formula 20 (KR-20) was 0.71 in this study.
Infection control attitude was measured using a tool developed by Park19 and modified and supplemented by Kim.20 It was further modified for this study according to the situations in schools during COVID-19. It comprised 10 items rated on a five-point Likert scale (1: not at all, 5: very much), and negatively worded items were reverse coded. A high score means that the beliefs or tendencies considered to be important in infection control are high. The Cronbach’s α was 0.66 in the original study and 0.81 in this study.
Job stress was measured using a scale developed by Kim,21 which was adapted to suit the situations in schools during COVID-19. It comprised 15 items rated on a five-point Likert scale (1: not at all, 5: very much). Job stress refers to the degree of burden experienced due to the duties or responsibilities of the worker. The Cronbach’s α was 0.89 in the original study and 0.91 in this study.
School organizational culture was assessed using a tool developed by Moon & Jang,22 which was modified and supplemented to suit the situations in schools during the COVID-19 pandemic. It comprised nine items rated on a five-point Likert scale (1: not at all, 5: very much). School organizational culture refers to the shared values, beliefs, and ideological goals according to the unique characteristics of the school that affect the behavior patterns, norms, and expectations of school members. The Cronbach’s α was 0.84 in the original study and 0.91 in this study.
COVID-19 infection control performance was measured using a tool developed by Yoon18 for nurses. It was modified and supplemented for this study to reflect the 7th edition of the COVID-19 response guidelines.18 The tool used a four-point Likert scale (1: never performed, 4: always performed); infection control performance refers to actions performed to prevent infection and spread in accordance with the COVID-19 prevention and control measures. The Cronbach’s α was 0.93 in the original study and 0.91 in this study.
Sampling
The minimum sample size including 10 predictors was 118 (based on a significance level of 0.05, a medium-sized effect of 0.15, and a power of 0.80 for a two-sided multiple linear regression analysis using G*Power.23 There were questions with clear answers, and those who gave wrong answers were considered unreliable and forced to drop out of the survey. For example, we used questions like “Please check No. 4 regardless of the content of the question.” Participants who did not follow the instructions were excluded. Data from 130 respondents were used for the final analysis, excluding 13 responses with incomplete answers. Compared with previous study,24 this study secured representativeness because the age group and teaching experience of the participants were similar.
Validity and Reliability
Prior to the study, a total of 11 experts (eight school health nurses with more than 10 years of teaching experience and three nursing professors) assessed the content validity of the tools used to measure infection control attitude, job stress, school organizational culture, and COVID-19 infection control performance (Supplemental Table A). A four-point Likert scale (4: very relevant, 1: not relevant) was used to assess the validity of the items. The content validity index (CVI) was calculated to select items with a CVI score of 0.8 or higher. Infection control attitude was modified by adding the term “COVID19,” and the CVI was 0.96. The tool for school organizational culture was configured to suit the situations in schools during the COVID-19 pandemic, and the CVI was 0.96. After deleting five items with overlapping meanings, the CVI of the tool for job stress was 0.89. The final tool for COVID-19 infection control integrated two items with overlapping meanings; one item related to protective equipment (level D) was deleted because it was irrelevant to schools. The CVI was 0.90.
Data Analysis
The collected data were analyzed using the IBM SPSS/WIN 25.0 program. The general characteristics, job-related characteristics, and main variables were analyzed as frequency, percentage, mean, and standard deviation using descriptive statistics. The difference in COVID-19 infection control performance according to general and job-related characteristics was analyzed using an independent t-test and one-way analysis of variance; Scheffe’s test was conducted post-hoc. A stepwise multiple linear regression analysis was performed to confirm the variables’ association with COVID-19 infection control performance. The reliability of the instruments was measured by Cronbach’s α.
Results
Differences in COVID-19 Infection Control Performance According to General and Job-Related Characteristics
Table 1 shows the difference in participants’ COVID-19 infection control performance according to their general and job-related characteristics. Their average age was 45.22±9.64 (26–62) years, and the average teaching experience was 13.09±10.26 (1–39) years. The level of COVID-19 infection control in schools perceived by health teachers was in the order of “above average” (n=67, 74.6%), “average” (n=28, 21.5%), and “below average” (n=5, 3.9%). A multiple response analysis of effective measures to prevent COVID-19 showed that 106 participants (81.5%) mentioned washing facilities and supplies, thorough preventive measures by schools, and individual quarantine, followed by establishing infectious disease countermeasures at metropolitan and provincial offices of education and developing response systems (n=42, 32.3%), student vaccination (n=31, 23.8%), reporting infectious disease outbreaks and epidemic monitoring for patient statistics analysis (n=21, 16.2%), and systematic health classes (n=17, 13.1%). The degree of COVID-19 infection control in schools variable showed a difference in the participants’ COVID-19 infection control performance (F=9.04, p<0.001).
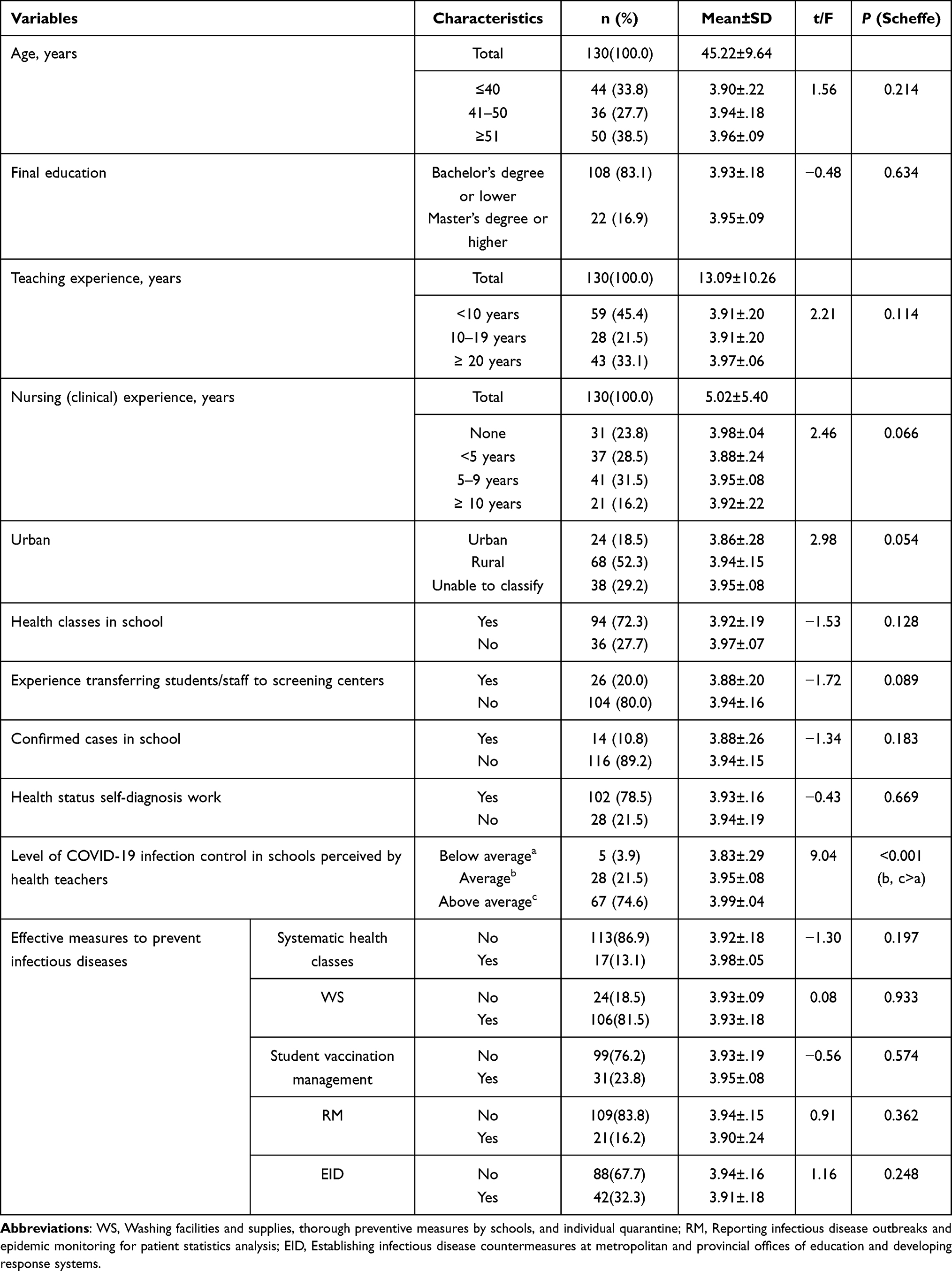 |
Table 1 Differences in Infection Control Performance According to Participants’ General and Job-Related Characteristics |
COVID-19 Knowledge, Infection Control Attitude, Job Stress, School Organizational Culture, and COVID-19 Infection Control Performance
Table 2 provides information on the participants’ COVID-19 knowledge, infection control attitude, job stress, school organizational culture, and COVID-19 infection control performance.
 |
Table 2 COVID-19 Knowledge, Infection Control Attitude, Job Stress, School Organizational Culture, and COVID-19 Infection Control Performance |
The average score for COVID-19 knowledge was 15.57±1.36, and the proportion of correct answers was 68%. The average scores for infection control attitude and job stress were 45.27±4.12 and 45.61±11.46, respectively. The average scores for school organizational culture and infection control performance were 37.42±5.86 and 47.18±2.01, respectively.
Relationships Between COVID-19 Knowledge, Infection Control Attitude, Job Stress, School Organizational Culture, and COVID-19 Infection Control Performance
Table 3 presents the relationships between the participants’ COVID-19 knowledge, infection control attitude, job stress, school organizational culture, and COVID-19 infection control performance. COVID-19 infection control performance was positively correlated with infection control attitude (r=0.38, p<0.001) and school organizational culture (r=0.42, p<0.001), and negatively correlated with job stress (r=−0.34, p<0.001). However, there was no significant correlation with COVID-19 knowledge (r=0.12, p=0.188).
 |
Table 3 Correlations Between Study Variables |
Factors Associated with COVID-19 Infection Control Performance
Table 4 shows the results of a stepwise multiple linear regression analysis to analyze the degree of the variables’ association with participants’ COVID-19 infection control performance. Based on various previous studies,24,25 we selected variables with differences in COVID-19 infection control performance according to general characteristics and job-related characteristics as Step 1 and variables with significance in the remaining correlation coefficients as Step 2 for the analysis. Performing a Multiple linear regression with too many independent variables may lead to overfitting, even if the model is significant.26 Therefore, we performed a distinction between Step 1 and 2 using a stepwise multiple linear regression.
 |
Table 4 Stepwise Multiple Linear Regression Analysis of Variables Associated with COVID-19 Infection Control Performance |
Five general characteristics showing a significant difference in COVID-19 infection control performance, including the degree of infection control in schools perceived by health teachers (below average), COVID-19 knowledge, infection control attitude, job stress, and school organizational culture, were used as independent variables. The value of the Durbin-Watson statistic used to detect the presence of autocorrelation between the error terms was 1.88, which is close to 2.0, indicating that there was no autocorrelation. Standardized residuals were obtained to identify whether the distribution of error terms could be considered normal; three values were smaller than −3; however, as they did not deviate significantly from −3, the distribution of error terms was assumed to be normal. The tolerance limit and variance inflation factor were calculated to determine multicollinearity between the independent variables. The tolerance limit was 0.98–0.99, higher than 0.10, and the variance inflation factor was 1.01–1.02, less than 10; thus, there was no multicollinearity between the independent variables.
According to the analysis, it was found that the variables that have the greatest influence on the performance of COVID-19 infection control are in the order of infection control attitude, job stress, and the degree of school control perceived by school health nurses. In other words, it can be said that the more positive the infection control attitude, the lower the job stress, the higher the management level of the school compared to the lower than the average, the higher the performance of COVID-19 infection control. Among the general characteristics input in Step 1, the variable affecting the infection performance was the degree of school control perceived by school health nurses. Therefore, it can be said that the married compared to the unmarried and in a fine health status compared to the below average, the better the health promotion behavior. The ratio explained by the variables was 11.1%. The main variables that were additionally added in Step 2 influencing the performance of infection were infection control attitude and job stress. Therefore, it can be said that the more positive the attitude toward infection control and the lower the job stress, the higher the performance of COVID-19 infection control. The ratio additionally explained by the variables input in Step 2 was 14.7%, and the total explanation power of Step 2 was 25.8% (F=14.39, p<0.001, R2=0.255, Adj-R2=0.258).
Discussion
The ongoing COVID-19 pandemic has necessitated strict social distancing measures. However, owing to overcrowding, schools rely mainly on wearing masks and checking body temperature, which may not be completely effective in controlling infections, considering the silent spreaders. Therefore, we investigated the factors associated with the COVID-19 infection control performance of health nurses, who manage quarantine activities in schools, to increase the efficiency of health care.
First, the results showed that the more positive the attitude toward infection control, the higher the performance of COVID-19 infection control. This is consistent with two studies on COVID-1927,28 and a study related to Middle East respiratory syndrome (MERS).19 Attitudes or individual positions on specific events or diseases and knowledge about disease affect decisions about physical health and health promotion behaviors.29,30 COVID-19 is characterized by uncertainty and variability. Attitude is significant in accepting variability. The importance of attitude is clear from the mature civic awareness that created the word “K-quarantine” during the pandemic. As the number of deaths and confirmed cases continue to rise, the results of this study reconfirm that the health teachers’ attitude toward infection control is a significant factor in preventing the spread of group infections in schools31 and establishing a safe school environment.
Second, job stress was associated with the performance of COVID-19 infection control. Job stress is a negative factor that reduces job satisfaction, aggravates dissatisfaction, and impedes development, ultimately affecting students.32 Our results are consistent with a study on the negative impact of job stress on job performance among health teachers in secondary schools during the MERS outbreak in Korea.33 As infection control does not produce immediately visible results, it can become a lower priority if there is a heavy health workload, lack of time, or insufficient resources.34 The health workload in schools during the pandemic is excessive for one health teacher to handle, because they are required to manage the entire school and take care of the students in person. Therefore, properly distributing and coordinating the increased workload in schools can help reduce the job stress involved in infection control. Additionally, strategic approaches for cooperation and communication between school members should be considered to reduce the job stress associated with infection control tasks.
Third, the level of infection control in schools perceived by health teachers was associated with their infection control performance, whereas school organizational culture was not significantly associated with it. School organizational culture is an invisible scale, but the level of infection control in schools was considered significant because it is the health teacher’s subjective evaluation of the overall status of COVID-19 infection control in schools, including outbreak monitoring, prevention control, academic management, and administrative support. Health teachers play a significant role in supporting public health by preventing the spread in schools and communities during an epidemic.35 A study on the roles of health teachers during COVID-19 also emphasized their unique position to act as health professionals during the pandemic.36
In the literature on infection control in other countries, health officials were assigned to schools under different circumstances. For example, Germany formulated a COVID-19 mitigation act to allow schools to respond to infectious diseases, emphasize social distancing and sanitation, enable medical institutions to handle health checkups and management, and focus on education to prevention and control infectious diseases.37 The UK developed and distributed COVID-19 test kits for schools, designated teachers from community health centers to be responsible for health and safety, and promoted mandatory health education for all students.38 In schools in Korea, COVID-19 response teams are responsible for managing self-report before school, measuring body temperature when students come to school, managing students and staff with suspected symptoms, and education and promotion on preventing infectious diseases and managing health.39 These examples indicate that schools should be linked with health authorities because their environment is vulnerable to infectious diseases; further, it is important to establish a systematic approach suitable for educational institutions. Institutional frameworks should also be prepared to check and evaluate whether health teachers are familiar with their role in COVID-19 infection control.
Lastly, knowledge related to COVID-19 was not significant in performing infection control. Due to lack of previous studies on health teachers, we have to make comparisons with the general public. A study on the anxiety, knowledge, infection possibility, preventive possibility, and preventive behavior level of COVID-19 in the general public, found the knowledge about COVID-19 was not significance.40 Although knowledge of emerging infectious diseases had a significant influence on infection control performance,41 studies on knowledge of MERS isolation guidelines42 and H1N1 influenza43 reported no significant influence on infection control performance; thus, the relationship between knowledge and performance remains unclear. Some studies, however, found that knowledge boosts attitude and improves performance.14,44 A high level of knowledge is expected to affect infection control behavior. However, as some studies report, knowledge does not directly lead to performance; thus, conducting repeated studies on health teachers in various regions and environments, and comparing the results is necessary.
Although health education and student health care are the main role and responsibilities of Korean school health nurses, they are forced to perform tasks other than those specified by law, such as administrative work. They also experience various conflicts in school because other school members have distorted expectations of their roles. These aspects may harm their infection control performance. In particular, it is necessary to assess the situation of schools and supplement insufficient personnel, facilities, and supplies according to the decision of school nurses, and frequent feedback on the degree of control is a significant factor influencing infection control. To supplement these factors, guidelines need to be prepared to provide practical and specific reports to local education agencies and receive support to facilitate the infection control performance of school health nurses during the COVID-19 pandemic.26 In terms of the degree of school management perceived by health nurses, the scope of performing infectious disease control tasks in schools is extensive and urgent, so it is difficult for school nurses to handle it alone, which can lead to high job stress. Therefore, the increased workload of school nurses needs to be properly distributed and coordinated to reduce their job stress and enable them to perform infectious disease control tasks effectively. Smooth communication and cooperation with other school members are also needed.
This study is significant as it is the first to examine knowledge, infection control attitude, job stress, and school organizational culture in relation to health nurses’ performance in controlling COVID-19 infections. It also measured the objective knowledge of health teachers rather than their level of knowledge related to COVID-19. However, each school may have a different understanding of infection control guidelines for COVID-19, and there are limits to generalizing the results because the survey was only conducted on health nurses in certain regions. Therefore, further research on the infection control performance of health nurses should consider various other factors. As this is a cross-sectional quantitative study, in-depth qualitative studies should be performed by adding new variables among the factors associated with the infection control of new infectious diseases by health nurses. Lastly, as health nurses were exposed to high risks of infection, working closely with suspected cases of COVID-19, studies on factors that affected their mental and physical health should be conducted, post pandemic.
Conclusions
This study aimed to identify factors affecting the infection control performance of school health nurses during the COVID-19 pandemic. Infection control attitude had the most significant influence among the variables that affect the performance of COVID-19 infection control, followed by job stress and the level of infection control in schools perceived by health nurses. The results showed the need to assess the overall situation of schools and supplement insufficient personnel, facilities, and supplies according to the decision of school nurses. Frequent feedback on the degree of control was also a significant factor influencing infection control. Therefore, it is necessary to improve these areas for the level of infection control in schools perceived by health nurses.
Acknowledgments
The authors would like to thank all the anonymous participants in the research.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Martinsson E, Garmy P, Einberg EL. Nurses’ experience of working in school Health Service during the COVID-19 pandemic in Sweden. Int J Environ Res Public Health. 2021;18(13):6713. doi:10.3390/ijerph18136713
2. Ministry of Education. Announcement of teaching plans for elementary school, elementary school, middle school, high school, and special schools report; 2020. Available from: https://www.moe.go.kr/boardCnts/view.do?boardID=294&boardSeq=80510&lev=0&searchType=null&statusYN=W&page=32&s=moe&m=020402&opType=N.
3. Lee YS, Shin BC, Jung YS. A study of the paradoxes in school education caused by Covid 19. Korean J Educ Res. 2021;59(1):131–165.
4. Ministry of Education. Ministry of Education Student legal infectious disease outbreak. 2021.
5. Gyeongsangnam-do Office of Education. 2020 student health promotion master plan: health management; 2020. Available from: http://www.gne.go.kr/board/view.gne?boardId=workroom&startPage=9&dataSid=1161143.
6. Feng N, Luo J, Li H, et al. Behaviours related to infectious disease and family factors in primary and middle school students. J Cent South Univ. 2015;40(6):681–687. doi:10.11817/j.issn.1672-7347.2015.06.018
7. Ministry of Education. Announcement: education basic statistical results. Available from: https://www.moe.go.kr/boardCnts/view.do?boardID=294&lev=0&statusYN=W&s=moe&m=0204&opType=N&boardSeq=81682.
8. Lim K, Kim J. School health teachers’ experience of coping with the COVID-19 Pandemic. J Korean Soc Sch Health. 2021;34(1):76–86. doi:org/10.15434/kssh.2021.34.1.76
9. Sun Y, Wang D, Han Z, Gao J, Zhu S, Zhang H. Disease prevention knowledge, anxiety, and professional identity during COVID-19 pandemic in nursing students in Zhengzhou, China. J Korean Acad Nurs. 2020;50(4):533–540. doi:10.4040/jkan.20125
10. Wahed W, Hefzy E, Ahmed M, Hamed N. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J Commun Health. 2020;45(6):1241–1251. doi:10.1007/s10900-020-00882-0
11. June KJ, Choi E. Infection control of hospital nurses: cases of Middle East respiratory syndrome. Korean J Occup Health Nurs. 2016;25(1):1–8. doi:10.5807/kjohn.2016.25.1.1
12. Kyung DE, Shin YS. Factors associated with nurses’ nursing intention toward COVID-19 patients. Korean J Adult Nurs. 2021;33(4):376–386. doi:10.7475/kjan.2021.33.4.376
13. Coreil J. Health behavior in developing country. In: Gochman DS, editor. Handbook of Health Behavior Research III. New York: Plenum Press; 1997:182–183.
14. Park S, Han J, Kwak K. The influence of nursing students’ knowledge, attitudes and infection prevention behaviors for COVID-19 upon the nursing intention for patients with the emerging infectious diseases. J Korean Acad Nurs. 2021;5(1):13–23. doi:10.34089/jknr.2021.5.1.13
15. Hanson E. Educational Administration and Organizational Behavior.
16. Bae S, Lee H, Kim Y. The structural relationship among learning organization climate of the school, transformational leadership of the principal, and change acceptance attitude of teachers. J Vocat Educ Res. 2014;33(6):97–118.
17. Yoon S. Correlations between Nurses’ Knowledge of COVID-19 and Infection Control Compliance, Resilience, and Psychosocial Well-Being. [Master’s thesis]. Seoul, South Korea: The Graduate School of Chung-Ang University; 2020.
18. Korea Disease Control and Prevention Agency. Guidelines for Response to Viral Infectious COVID19.
19. Park GS. The Study on the Health Center Avian Influenza Worker’s Knowledge, Attitude and Practical Skills about Management of Avian Influenza. [Master’s thesis]. Gimhae, Taiwan: Inje University; 2006.
20. Kim M. The convergence study of nursing students’ knowledge, attitudes and preventive behaviors against MERS in South Korea. J Korea Converg Soc. 2017;8(4):149–157. doi:10.15207/JKCS.2017.8.4.149
21. Kim J. Effects of Job Stress and Teacher Efficiency Focused on School Health Teachers Job Satisfaction. [Master’s thesis]. Gwanjgu: Graduate School of Education Chonnam National University; 2012.
22. Moon J, Jang K. The performance of healthcare-associated infection control guideline among hospital nurses: a structural equation model. Iran J Public Health. 2018;47(5):648–657.
23. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. doi:10.3758/BF03193146
24. Lee H, Shin S. Effects of elementary school health teachers’ COVID-19 knowledge and resilience on their performance at infection control. J Korean Pubilc Health Nurs. 2021;35(2):297–309.
25. Kim S, Ra J. Influencing factors on nursing practices for healthcare-associated infections control in intensive care unit. Korean J Healthc Assoc Infect Control Prev. 2018;23(2):39–52. doi:10.14192/kjhaicp.2018.23.2.39
26. Hair J, Anderson R, Tatham R, Black W. Multivariate Data Analysis. Upper Saddle River, New Jersey: Prentice Hall; 1998.
27. Shubay MA, Mashyakhy M, Agili DEA, Albar N, Quadri MF. Associated with infection-control behavior of Dental Health–care workers during the COVID-19 pandemic: a cross-sectional study applying the theory of planned behavior. J Multidiscip Healthc. 2020;12(13):1527–1535. doi:10.2147/JMDH.S278078
28. Almohammed OA, Aldwihi LA, Alragas AM, Almoteer AI, Gopalakrishnan S, Alqahtani NM. Knowledge, attitude, and practices associated with COVID-19 among healthcare workers in hospitals: a Cross-Sectional Study in Saudi Arabia. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.643053
29. Park S. Knowledge, attitude, and preventive behaviors related to Middle East Respiratory Syndrome (MERS) in adults. J Korean Pubilc Health Nurs. 2019;33(1):33–46.
30. Jeong H, Cho O, Yoo Y. High blood pressure-related knowledge and health behavior among first-year college students. J Korean Pubilc Health Nurs. 2009;23(2):285–295.
31. Krishnaratne S, Pfadenhauer LM, Coenen M. Measures implemented in the school setting to contain the COVID-19 pandemic: a rapid scoping review. Cochrane Database Syst Rev. 2020;12:CD013812. doi:10.1002/14651858.CD013812
32. Lee M. The association between health teachers’ stress, burnout, and self-efficacy: a path analysis approach. J Korea Acad Ind Coop Soc. 2020;21(1):317–325.
33. Kang I, Cho S, Jeong H. Factors affecting job stress of school nurse in secondary school. J Korean Soc Sch Health. 2010;23(2):286–295.
34. Um Y. Grounded Theory Study on the Experiences and Roles of School Health Teachers in Responding to Infectious Diseases. [Doctoral thesis]. Seoul, South Korea: The Graduate School of Chung-Aug University; 2021.
35. Hoke AM, Keller CM, Calo WA, Sekhar DL, Lehman EB, Kraschnewski JL. School nurse perspectives on COVID-19. J Sch Nurs. 2021;37(4):292–297. doi:10.1177/1059840521992054
36. Ministry of Education. May 2020 overseas education information trend data; 2020. Available from: https://moe.go.kr/boardCnts/view.do?boardID=407&boardSeq=81162&lev=0&searchType=null&statusYN=W&page=2&s=moe&m=020204&opType=N.
37. Department for education. 2020 Ministry of Education. Kindergarten, Elementary, Middle and High School, Special Education School COVID-19 Infection Prevention Control Guide (N0.2). Seoul: Ministry of Education; 2020.
38. Ministry of Education. News and promotion; 2021. Available from: https://www.moe.go.kr/main.do?s=moe.
39. McDonald CC. Reopening schools in the time of pandemic: look to the school nurses. J Sch Nurs. 2020;36(4):239–240. doi:10.1177/1059840520937853
40. Jung A, Hong E. A study on anxiety, knowledge, infection possibility, preventive possibility and preventive behavior level of COVID-19 in general public. Int J Adv Comput Technol. 2020;10(8):87–98. doi:10.22156/CS4SMB.2020.10.08.087
41. Nour M, Elamin F. Knowledge, attitude and practices of healthcare providers towards MERS-CoV infection at Makkah hospitals, KSA. Int Res J Med Med Sci. 2015;3(4):103–112.
42. Kim S, Song R. Knowledge and practice of middle east respiratory syndrome isolation precaution among hospital nurses. J Korean Acad Fundam Nurs. 2018;25(1):46–57. doi:10.7739/jkafn.2018.25.1.46
43. Choi J, Yang N. Perceived knowledge, attitude, and compliance with preventive behavior on influenza A (H1N1) by university students. J Korean Acad Adult Nurs. 2010;22(3):250–259.
44. Choi Y, Lee E. A study on knowledge, attitude, infection management intention & educational needs of new respiratory infectious disease among nurses who unexperienced NRID (SARS & MERS). J Korea Acad Industr Coop Soc. 2019;20(2):721–731. doi:10.5762/KAIS.2019.20.2.721
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.