")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Factor structure of the Persian version of general, social, and negative self-consciousness of appearance domains of Derriford Appearance Scale 59: an application in the field of burn injuries
Authors Sadeghi-Bazargani H, Zare Z, Ranjbar F
Received 2 September 2016
Accepted for publication 3 November 2016
Published 16 January 2017 Volume 2017:13 Pages 147—154
DOI https://doi.org/10.2147/NDT.S121250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Homayoun Sadeghi-Bazargani,1 Zahra Zare,2 Fatemeh Ranjbar3
1Road Traffic Injury Research Center, Department of Statistics and Epidemiology, Faculty of Health, Tabriz University of Medical Sciences, Tabriz, Iran; 2Department of Statistics and Epidemiology, Faculty of Health, Tabriz University of Medical Science, Tabriz, Iran; 3Research Center of Psychiatry and Behavioral Sciences, Tabriz University of Medical Sciences, Tabriz, Iran
Background: The Derriford Appearance Scale 59 (DAS59) is a widely used measure of the spectrum of psychological distress and dysfunction that is characteristic of disfigurement. Also, disfigurement due to burn injury leads to feeling guilty or less socially competent, avoiding social situations, suicide, poor self-esteem, sexual difficulties, and depression. Therefore, the purpose of this study was to translate and culturally adapt three subscales of DAS59 into Persian language and to investigate its factor structure for Iranian burned patients.
Method: Translation–back translation of the scale into Persian was done. The internal consistency of the translated scale was evaluated by Cronbach’s alpha. Next, construct validity of the translated instrument was assessed by exploratory factor analysis using principal components and rotation of varimax methods. This research involved a convenience sample of 189 adult burned patients with disfigurement in their face, head, ears, neck, hands, and legs.
Result: The Cronbach’s alpha for overall scale, subscales 1, 2, and 3 were 0.93, 0.93, 0.89, and 0.80, respectively. The best solution from the principal components analysis of the 40 items of the DAS59 revealed three factors corresponding to the three subscales with 20 items: factor 1 (general self-consciousness of appearance) consisted of 9 statements accounting for 33.23% of the variance (eigenvalue =9.23); factor 2 (social self-consciousness of appearance) consisted of 7 statements accounting for 22.91% of the variance (eigenvalue =1.53); and factor 3 (negative self-concept) consisted of 4 statements accounting for 14.98% of the variance (eigenvalue =1.13).
Conclusion: The factor structure of the three subscales of DAS59 provides a widely acceptable, psychometrically robust, factorial self-report scale to assess distress and dysfunction in problems of appearance among Iranian burned patients, and facilitates further research into the efficacy of treatment approaches for problems of appearance and early investigation of therapeutic outcome.
Keywords: burns, disfigurement, validity, psychological scale, appearance, Derriford (DAS59)
Introduction
Disfigured individuals, either facially or physically, face with problems in their daily life compared to attractive people or those without disfiguration, which is assessed based on two overlapping perspectives. The first perspective is “view from the outside” such as impacts of appearance from social perceptions and interactions. Meanwhile, studies have shown that disfigured individuals feel guilty or less socially competent and receive less attention from others. The second perspective is “view from the inside” such as impacts of appearance from individual perceptions of self-concept, emotional well-being, and quality of life, which lead to a level of anxiety, avoidance from social situation, suicide, poor self-esteem, sexual difficulties, and depression.1–3
Here, the concept of the term “disfigurement” refers to “visible difference” or “unusual appearance” due to a mark, rash, scar, or graft on a person’s skin or an asymmetry or paralysis to a person’s face or body.4
Body image is a multidimensional concept that is affected by disfigurement or changing appearance.5
Sarah Grogan defines body image as “a person’s perceptions, thoughts, and feelings about his or her body.” In addition, she defines the construct of body image disturbance relatively simply as “a person’s negative thoughts and feelings about his or her body.”6
On the other hand, researchers have identified four components of attitudinal body image: 1) overall satisfaction–dissatisfaction with one’s appearance; 2) emotions about one’s appearance, including anxiety and discomfort; 3) investment in one’s appearance, erroneous thoughts or beliefs about one’s body, and body image schemas; and 4) avoidance of situations or objects because of their elicitation of body image concerns.7
Congenital defects, traumatic events, and disease processes are the three common causes of disfigurement.3
Burn injuries are among the most devastating of all injuries and a major global public health problem. Approximately 90% of burn injuries occur in low- to middle-income countries.8 Specifically, burn injury has been considered a major health problem in Iran.9
Major burns, defined by the American Burn Association, in terms of percentage of total body surface area (TBSA) burned, location, or secondary complications,10 may result in pain, shock, sepsis, etc.11
Burn injury is often a devastating event with long-term physical, psychological, social, and economic impacts of burn injuries as well as burn-related disabilities and disfigurements. Therefore, long-term significant psychological distress was diagnosed among approximately one-third of burned patients.12–15
Burned patients experience issues with social interaction and social life as well as psychological problems due to scarring and changed appearance. These complications may be related to demographic and individual variables (eg, age, sex, socioeconomic status), burn site, skin color, time to heal, and burn severity.16
Moreover, decreased quality of life and delayed reintegration into society resulting from post-burn scar are the greatest unmet challenges in burn rehabilitation.17
One of the greatest barriers to function and the most visible stigma of injury is the development of scarring after burn injury due to advances in critical care and surgical management over the past several decades.
A great concern for patients and a challenging problem for clinicians is the hypertrophic scarring after surgical procedures and trauma, especially, burns, which was defined by Peacock as scars raised above the skin level but within the confines of the original lesion.18 It leads to esthetical defects, dissatisfaction with appearance, and functional disability, which in turn lead to decreased quality of life, decreased ability to live independently, and delayed reintegration into society.17
Hypertrophic scar is the most common cicatrix formed after a burn, the prevalence of which is reportedly as high as 70%.19
According to a systematic review study, the prevalence of hypertrophic scarring in the studies ranged from 32% to 72%.16
According to another study, the prevalence of at least mild to moderate symptoms of depression was 46%. There was a significant correlation between depressive symptoms and body image dissatisfaction in burn reconstruction patients. Compared with other traumatic injury group, rate of clinically significant symptoms of depression in the burn reconstruction sample is high.
Considerable amount of recent empirical documentation have demonstrated the role of body image in the short-term and long-term adjustment in adult as well as in child survivors. The single most important predictor of long-term psychosocial functioning is body image.20
Many variables influence an individual’s adaptation to disfigurement after burn injury. For instance, burn survivors with residual scarring or disfigurement have negative adjustment if appearance was important for them even before burning.20
Body image dissatisfaction was affected by female gender, placing a great importance on physical appearance, the presence of facial burns, and the percentage of TBSA burned directly.20,21
Findings from a study demonstrated that body image with physical appearance plays a central role in social interactions and selection of partners. Judgements based on appearance affected social interaction and selection of partner.22
In a study that investigated romantic experiences of adolescents with a visible difference, those participants that were concerned with their appearance reported fear of negative evaluation.23
The fear was based on their own perceptions rather than the reality of their appearance.
It has been confirmed that concerns about appearance are common in the general population.24 Also, a clear association has been found between body sites and mean scores of participants reporting concern with features at those body sites.25
Consequently, it is necessary to consider the psychological aftermaths of burn scars along with the medical issues.
Thus far, several psychometric scales have been developed in order to measure the effects of disfigurement or body image dissatisfaction caused by diseases or trauma, but only four patient-reported outcome measurements have been developed specifically for burned patients: Burn Specific Health Scale, Satisfaction with Appearance, Social Comfort Questionnaire, and Perceived Stigmatization Questionnaire.16
Burn Specific Health Scale-Brief version was validated for Iranian burn survival. This questionnaire was designed to assess the level of functioning and health-related quality of life in adult burn survivors, but it has only 3 items about body image.26
On the other hand, more focused and appropriate measures of the effects of living an aesthetic problem of appearance, such as the Appearance Schemas Inventory,27 the Body Image Avoidance Questionnaire,28 and the Body Dysmorphic Disorder Examination,29 suffer from low content validity, restricted range of applicability, impracticability, or limited psychometric development.24,30
None of these measures were designed specifically to assess the spectrum of symptomatology that is relevant to the wide range of difficulties experienced by patients living with appearance issues.24
These findings highlighted the need to develop or validate relevant psychological scales and instruments that would measure the specific emotional and behavioral problems of disfigurement in native-speaking people with burn injury, especially in low- to middle-income countries including Iran where psychological care is not adequately and systematically provided for traumatized patients.
The Derriford Appearance Scale (DAS59) is a 59-item factorial scale measuring appearance-related distress, social anxiety, and avoidance, standardized on both general and hospital populations whose lives are dominated by their body-image disturbance and self-consciousness of appearance and those for whom appearance is of no concern. On the other hand, DAS59 is applicable to people concerned about their appearance and to those who are not, or people with visible difference to others and those whose difference is only apparent to themselves.
The factors are shown to be clinically meaningful and identified as General Self-Consciousness of Appearance, Social Self-Consciousness of Appearance, Sexual and Bodily Self-Consciousness of Appearance, Negative Self-Concept, and Facial Self-Consciousness of Appearance.24,30
To determine a valid scale, the authors selected three domains of scale, the General Self-Consciousness of Appearance, Social Self-Consciousness of Appearance, and Negative Self-Concept, which include 40 items.
The purpose of this study was to translate and culturally adapt the three subscales of DAS59 into Persian language and to investigate their factor structure for Iranian burned patients.
Methods
Participants, setting, and sampling
This research involved a convenience sample of 189 burned adult patients (≥16 years of age) with disfigurement in the face, head, ears, neck, hands, and legs. The research was performed over 12 months in three hospitals in Tehran, Tabriz, and Kermanshah provinces of Iran. The sample comprised either former burned patients who were referred to hospitals for cosmetic surgeries or individuals burned recently who were receiving ongoing care from hospitals.
Selection of Derriford Appearance Scale 59
The 59-item Derriford Appearance Scale (DAS59) was developed by Tony Carr et al. The scale was initially developed from a cross-sectional design using clinical and nonclinical populations with problems of appearance and a pre–post intervention design using plastic surgery patients.
The DAS59 was developed to measure the spectrum of characteristic of disfigurement, deformities, and aesthetic problems of appearance, such as psychological distress and dysfunction.30
The scale development process: translation and back-translation
The translation process was performed according to the translation and cultural adaptation group.31 The original English version was translated (forward translation) into Persian separately by three self-governing official translators. Then, one researcher who mastered both languages reviewed the translations in terms of their inconsistencies with the original version. Minor revisions were suggested in some areas and, finally, one Persian version of the scale was created. Subsequently, it was translated back from Persian to English by another official translator. The back-translated version and the original version were compared in order to be similar in structure and meaning. The authors compared the original version with the back-translated version (harmonization). An expert panel consisting of epidemiologists and a psychologist was asked with the questionnaire’s conceptual equivalence. Finally, according to their recommendations, minor changes were made and pilot testing was performed.
The authors translated this scale to elementary reading level in order to be applicable and understandable for patients of different education levels.
A trained interviewer read out the questions to illiterate patients, exactly like the translated scale without any interpretation to prevent from influencing the patients’ answers. Stages of translation process are shown in Figure 1.
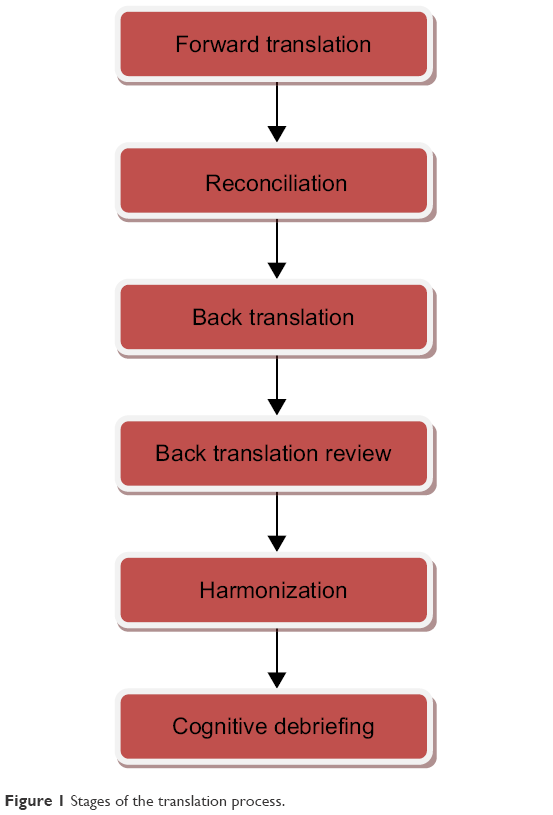 | Figure 1 Stages of the translation process. |
Ethical considerations
Approval for the study was obtained from the ethics committee of Tabriz University of Medical Science. Verbal informed consent was obtained from all of the participants. The ethics committee did not require that written informed consent be obtained because this was a questionnaire based study and some patients were illiterate.
Data analysis
Stata (version 13) was used in the analysis of factor structure of DAS59. Statistical methods were used according to the objective as follows.
Assessment of internal consistency
To determine the instrument’s internal consistency, Cronbach’s alpha was determined.
Assessment of construct validity
To determine the construct validity of DAS59, exploratory factor analysis using principal components and the rotation of varimax methods was conducted. The questionnaire was distributed among 189 burned victims in Tabriz, Tehran, and Kermanshah. Selection of the number of factors to be rotated was based on conjunctive criteria requiring the eigenvalue of the factor to be greater than 1 and the use of the scree test. A uniqueness score below 0.7 was considered as the criterion for selecting items having adequate communality.
Results
Socio-demographic characteristics
In this study, 189 burned patients (105 men, 55.56%) with an average age of 32 (SD =9.37) ranging from 16 to 60 years were recruited. Most participants were educated at the high school level (from 7 to 12 years of education), while 10 (5.32%) participants were illiterate, and 39 (20.74%) had received college education. Majority of patients (77.78%) lived in urban areas. Of all participants, 121 (64.02%) were married. The median TBSA of burning was 20%, with a range of 10%–37%.
Internal consistency
The Cronbach’s alpha for overall scale, subscales 1, 2, and 3 were 0.93, 0.93, 0.89, and 0.80, respectively.
Factor structure
Exploratory factor analysis was used according to different factors frequently. Ultimately, the 3-factor model was the best result of a simple pattern of loadings based on eigenvalues >1, as well as a total of 71% of variance was explained by the 3-factors model. The Kaiser–Meyer–Olkin index was 0.88.
The best solution from the principal components analysis of the 40 items of the DAS59 revealed three factors corresponding to the three subscales with 20 items remaining.
Factor 1 (General Self-Consciousness of Appearance) consisted of 9 statements accounting for 33.23% of the variance (eigenvalue =9.23). Factor 2 (Social Self-Consciousness of Appearance) consisted of 7 statements accounting for 22.91% of the variance (eigenvalue =1.53). Factor 3 (Negative Self Concept) consisted of 4 statements accounting for 14.98% of the variance (eigenvalue =1.13).
The structure of extracted factors from correlation between the factor loadings and questions using the principal components method and varimax rotation is shown in Table 1.
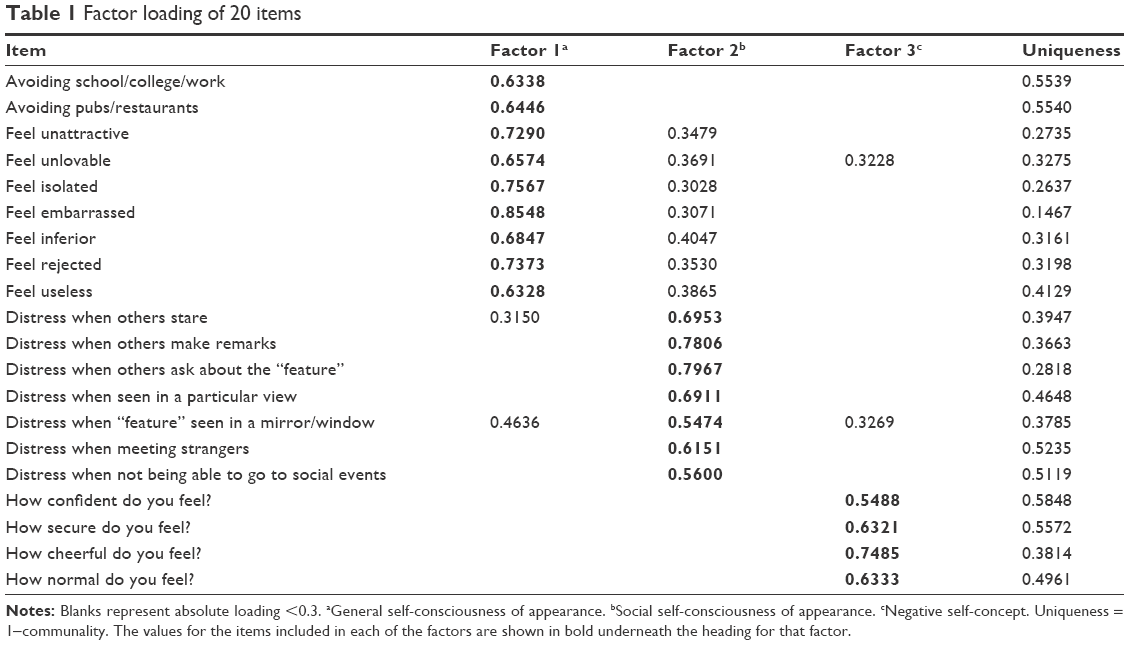 | Table 1 Factor loading of 20 items |
Discussion
This study describes the factor structure of DAS59 to assess the difficulties experienced by the Iranian burned patients through living with a problem in appearance. The high level of internal consistency (Cronbach α=0.93) suggests that the item sampling from the original scale effectively represented the item set and those 20 items that remained after the principal components analysis reflect the main factor of self-consciousness of appearance underlying the original scale.
The factor structure had acceptable eigenvalues (9.23–1.13), and also the scale and subscales showed good homogeneity (Cronbach alphas 0.93–0.80). The exploratory factor analysis recognized three subscales that can be used to differentiate between various manifestations of disfigurement due to burn injury. These findings reinforce the work of Tony Carr et al who viewed complications caused by disfigurement as multidimensional. Although DAS59 had been developed to measure psychological distress and dysfunction due to disfigurement, deformities, and aesthetic problems of appearance, the subscale development undertaken suggests that the concept of the feeling of having disfigured appearance can, in fact, be expanded to include feelings of depression and anxiety.30
This phenomenon was observed in this study, and we validated the factor structure of Persian version of three subscales of this scale just for burned victims with disfigurement. In exploratory factor analysis, this study’s subscales were similar from the original instrument.
The findings of this study suggest that the DAS59 may be a valuable instrument for research on social-behavioral burn.
These results from a sample of burned patients from various regions of Iran provisionally confirm the selection of 20 items and indicate a meaningful factorial structure.
According to the studies, dysfunction and distress arising from a problem of appearance is independent from the degree of visible disagreement, therefore, the sample of this study consisted of patients with burn scars in face, head, neck, ears, hands, and legs.
According to the statements of psychologists and sociologists, appearance nowadays is not only a biologic phenomenon but also a social phenomenon. In addition, evaluation of an individual’s appearance is affected by the cultural norms which are present in the society.
Appearance is central to social experience and social interaction for Iranian people, who are renowned for placing a high value on appearance, and individuals are judged based on their appearance.
Consequently, a person with disfigurement may face with problems such as failure to return to work, receiving less respect from others, or not being able to get appropriate job. Nevertheless, they may encounter problems to communicate with their friends, partner, and family. These conditions result in psychological complications for the burned patients.
In Iran, a majority of the studies have been conducted to find out psychological distress and dysfunction among burned patients, but we did not find any studies that had localized a questionnaire in conjunction with Iran’s cultural adaptation specifically to disfigured burned patients. Meanwhile, another scale that is under publishing is being developed by our research team for assessing irrational cognitions among burned patients.
Although there are scales that measure psychological problems related to aesthetic problems or body image dissatisfaction, they did not have overall consideration on problems related to appearance.
Table 2 illustrated various scales developed for assessing appearance in general and related scales for burns.
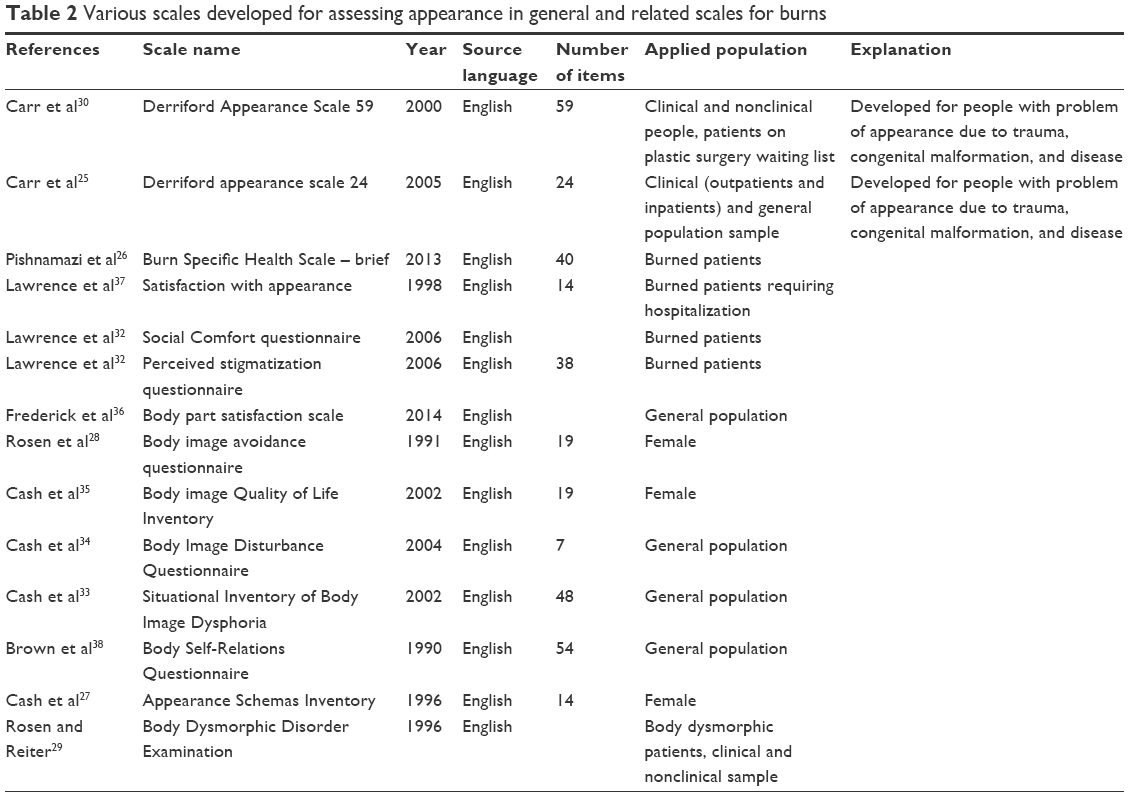 | Table 2 Various scales developed for assessing appearance in general and related scales for burns |
The Derriford Appearance Scale provided an effective measure and description of the difficulties associated with living with a problem of appearance. The scale is highly homogenous and measures an underlying construct that is called “self-consciousness of appearance”.30 It may help to answer questions of theoretical interest in the psychological aspect of problems related to appearance to investigate psychological interventions such as cognitive behavioral therapies.24
Conclusion
The factor structure of the three subscales of DAS59 provides a widely acceptable, psychometrically robust, factorial self-report scale to assess distress and dysfunction in problems of appearance among Iranian burned patients and facilitates further research into the efficacy of treatment approaches for problems of appearance and early investigation of therapeutic outcome. Although a psychometric scale cannot substitute for a comprehensive clinical assessment, it is to be hoped that routine clinical assessments may also be improved by the inclusion of an effective, psychometric scale such as the DAS59 which its factor structure has been validated for Iranian burned victims.
Acknowledgments
This study was supported financially by the Tabriz University of Medical Sciences.
The authors would like to thank Tabriz and Kermanshah University of Medical Sciences and Burn Research Center at Iran University of Medical Sciences. The authors appreciate the patients who participated in this research project. The authors also thank all the staff in the Sina, Shahid Motahhary, and Emam Khomeini university hospitals at Tabriz, Tehran, and Kermanshah provinces of Iran for their efforts in the project.
Disclosure
The authors report no conflicts of interest in this work.
References
Soni CV, Barker JH, Pushpakumar SB, et al. Psychosocial considerations in facial transplantation. Burns. 2010;36(7):959–964. | ||
Moss TP. The relationships between objective and subjective ratings of disfigurement severity, and psychological adjustment. Body Image. 2005;2(2):151–159. | ||
Thompson A, Kent G. Adjusting to disfigurement: processes involved in dealing with being visibly different. Clin Psychol Rev. 2001;21(5):663–682. | ||
Partridge J. Psycho-social reflections on craniofacial morphogenesis. Semin Cell Dev Biol. 2010;21(3):333–338. | ||
Cash TF, Santos MT, Williams EF. Coping with body-image threats and challenges: validation of the body image coping strategies inventory. J Psychosom Res. 2005;58(2):190–199. | ||
Bergstrom RL, Neighbors C. Body image disturbance and the social norms approach: an integrative review of the literature. J Soc Clin Psychol. 2006;25(9):975. | ||
Grabe S, Hyde JS. Ethnicity and body dissatisfaction among women in the United States: a meta-analysis. Psychol Bull. 2006;132(4):622–640. | ||
Williams JA, Yankina A, Choe YS, Dokukina L, Brazol M. Effects of nutritional supplementation on prealbumin concentrations in pediatric burn patients: a randomized, controlled trial. Open Nutr J. 2013;7(1):20–25. | ||
Sadeghi-Bazargani H, Mohammadi R. Epidemiology of burns in Iran during the last decade (2000–2010): review of literature and methodological considerations. Burns. 2012;38(3):319–329. | ||
Association AB. Guidelines for service standards and severity classifications in the treatment of burn injury. Bull Am Coll Surg. 1984;69(10):24–30. | ||
Patterson DR, Everett JJ, Bombardier CH, Questad KA, Lee VK, Marvin JA. Psychological effects of severe burn injuries. Psychol Bull. 1993;113(2):362–378. | ||
Reeve J, James F, McNeill R, Brown P, Cameron L, Mills S. Functional and psychological outcomes following burn injury: reduced income and hidden emotions are predictors of greater distress. J Burn Care Res. 2011;32(4):468–474. | ||
World Health Organization. A WHO Plan for Burn Prevention and Care. 2008. Available from: http://apps.who.int/iris/bitstream/10665/97852/1/9789241596299_eng.pdf. Accessed September 16, 2009. | ||
Van Loey NE, Van Son MJ. Psychopathology and psychological problems in patients with burn scars. Am J Clin Dermatol. 2003;4(4):245–272. | ||
Fauerbach JA, McKibben J, Bienvenu OJ, et al. Psychological distress after major burn injury. Psychosom Med. 2007;69(5):473–482. | ||
Lawrence JW, Mason ST, Schomer K, Klein MB. Epidemiology and impact of scarring after burn injury: a systematic review of the literature. J Burn Care Res. 2012;33(1):136–146. | ||
Finnerty CC, Jeschke MG, Branski LK, Barret JP, Dziewulski P, Herndon DN. Hypertrophic scarring: the greatest unmet challenge after burn injury. Lancet. 2016;388(10052):1427–1436. | ||
Peacock Jr EE, Madden JW, Trier W. Biologic basis for the treatment of keloids and hypertrophic scars. South Med J. 1970;63(7):755–760. | ||
Bombaro KM, Engrav LH, Carrougher GJ, et al. What is the prevalence of hypertrophic scarring following burns? Burns. 2003;29(4):299–302. | ||
Corry N, Pruzinsky T, Rumsey N. Quality of life and psychosocial adjustment to burn injury: social functioning, body image, and health policy perspectives. Int Rev Psychiatry. 2009;21(6):539–548. | ||
Thombs BD, Haines JM, Bresnick MG, Magyar-Russell G, Fauerbach JA, Spence RJ. Depression in burn reconstruction patients: symptom prevalence and association with body image dissatisfaction and physical function. Gen Hos Psychiatry. 2007;29(1):14–20. | ||
Levine MP, Smolak L. Body image development in adolescence. Body Image: A Handbook of Theory, Research, and Clinical Practice. 2002:74–82. | ||
Hoogewerf CJ, van Baar ME, Middelkoop E, van Loey NE. Impact of facial burns: relationship between depressive symptoms, self-esteem and scar severity. Gen Hosp Psychiatry. 2014;36(3):271–276. | ||
Harris DL, Carr AT. The Derriford Appearance Scale (DAS59): a new psychometric scale for the evaluation of patients with disfigurements and aesthetic problems of appearance. Br J Plast Surg. 2001;54(3):216–222. | ||
Carr T, Moss T, Harris D. The DAS24: a short form of the Derriford Appearance Scale DAS59 to measure individual responses to living with problems of appearance. Br J Health Psychol. 2005;10(2):285–298. | ||
Pishnamazi Z, Rejeh N, Heravi-Karimooi M, Vaismoradi M. Validation of the Persian version of the Burn Specific Health Scale – brief. Burns. 2013;39(1):162–167. | ||
Cash TF, Labarge AS. Development of the Appearance Schemas Inventory: a new cognitive body-image assessment. Cognit Ther Res. 1996;20(1):37–50. | ||
Rosen JC, Srebnik D, Saltzberg E, Wendt S. Development of a body image avoidance questionnaire. J Consult Clin Psychol. 1991;3(1):32. | ||
Rosen JC, Reiter J. Development of the body dysmorphic disorder examination. Behav Res Ther. 1996;34(9):755–766. | ||
Carr T, Harris D, James C. The Derriford Appearance Scale (DAS-59): a new scale to measure individual responses to living with problems of appearance. Br J Health Psychol. 2000;5(2):201–215. | ||
Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. | ||
Lawrence JW, Fauerbach JA, Heinberg LJ, Doctor M, Thombs BD. The reliability and validity of the Perceived Stigmatization Questionnaire (PSQ) and the Social Comfort Questionnaire (SCQ) among an adult burn survivor sample. Psychol Assess. 2006;18(1):106–111. | ||
Cash TF. The situational inventory of body-image dysphoria: psychometric evidence and development of a short form. Int J Eat Disord. 2002;32(3):362–366. | ||
Cash TF, Phillips KA, Santos MT, Hrabosky JI. Measuring “negative body image”: validation of the Body Image Disturbance Questionnaire in a nonclinical population. Body Image. 2004;1(4):363–372. | ||
Cash TF, Fleming EC. The impact of body image experiences: development of the body image quality of life inventory. Int J Eat Disord. 2002;31(4):455–460. | ||
Frederick D, Bohrnstedt GW, Hatfield E, Berscheid E. Factor structure and validity of the Body Parts Satisfaction Scale: results from the 1972 Psychology Today survey. Psihologijske Teme. 2014;23(2):223–242. | ||
Lawrence JW, Heinberg LJ, Roca R, Munster A, Spence R, Fauerbach JA. Development and validation of the satisfaction with appearance scale: assessing body image among burn-injured patients. Psychol Assess. 1998;10(1):64. | ||
Brown TA, Cash TF, Mikulka PJ. Attitudinal body-image assessment: factor analysis of the Body-Self Relations Questionnaire. J Pers Assess. 1990;55(1–2):135–144. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.