")
Back to Journals » Clinical Interventions in Aging » Volume 18
Facilitators and Barriers of Integrated Care for Older Adults with Multimorbidity: A Descriptive Qualitative Study
Authors Wu J, Xue E, Huang S, Fu Y , Chen D, Shao J, Zhang H, Tang L , Ye Z
Received 11 September 2023
Accepted for publication 5 November 2023
Published 29 November 2023 Volume 2023:18 Pages 1973—1983
DOI https://doi.org/10.2147/CIA.S436294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Jingjie Wu,1 Erxu Xue,1 Siyuan Huang,2 Yujia Fu,3 Dandan Chen,1 Jing Shao,3 Hui Zhang,4 Leiwen Tang,1 Zhihong Ye1
1Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Nursing Department, the First Affiliated Hospital of Ningbo University, Ningbo, Zhejiang, People’s Republic of China; 3School of Nursing, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 4Nursing Department, Guizhou Provincial People’s Hospital, Guiyang, Guizhou, People’s Republic of China
Correspondence: Zhihong Ye, Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, 3rd of East Qingchun Road, Hangzhou, Zhejiang Province, People’s Republic of China, Tel +8613606612119, Email [email protected]
Purpose: A lack of coordinated care leads to multiple adverse effects for older adults with multimorbidity, including high treatment burdens, adverse health outcomes, reduplicated healthcare service utilization, and catastrophic healthcare expenditure. To foster healthy aging, person-centered integrated care that is responsive to older adults has been proposed by the World Health Organization. The objective of this study was to identify factors that impact the successful implementation of integrated care for older adults with multimorbidity in China.
Patients and Methods: From July 2022 to May 2023, 33 healthcare providers and managers involved in the delivery and management of healthcare services for older adults with multimorbidity were recruited from Zhejiang Province, China using purposeful and maximum variation sampling methods. Semi-structured, face-to-face in-depth interviews were conducted by the same interviewer in the participants’ native Chinese language until data saturation was reached. Inductive thematic analysis was used to analyze the data, and then, themes were mapped onto six dimensions using the Rainbow Model of Integrated Care to allow for a comprehensive view of the study’s findings.
Results: Eleven themes were generated as facilitators and barriers to integrated care for older adults with multimorbidity in China. These themes include (1) clinical integration: patient-centered care, (2) professional integration: interdisciplinary teams and training, (3) organizational integration: resources and accessibility, (4) system integration: community and funds, incentives, and health insurance, (5) functional integration: electronic health record systems, workforce, and guidelines, and (6) normative integration: shared mission.
Conclusion: Guided by the Rainbow Model of Integrated Care, various factors at both micro, meso, and macro levels that impact the implementation of integrated care for older adults with multimorbidity in the Chinese context have been identified in this study. The strategies for future interventions and policies should focus on promoting facilitators and addressing barriers.
Keywords: delivery of health care, integrated, aged, older adult, multiple chronic conditions, facilitator, barrier
Introduction
Multimorbidity, referring to the co-existence of two or more long-term conditions in one individual,1 has become an expanding health challenge globally alongside rapid population aging and increasing prevalence of chronic conditions.2,3 Despite an increasing focus on older adults with multimorbidity, this vulnerable population still experiences a lack of coordinated care, which further leads to high treatment burdens,4 myriad adverse health outcomes,5–7 reduplicated healthcare service utilization,8 and catastrophic healthcare expenditure.9,10
To foster healthy ageing, the World Health Organization (WHO) has proposed four action areas, one of which is the delivery of person-centered integrated care and primary healthcare services responsive to older people.11 Integrated care is defined as healthcare that is managed and delivered so that people receive a continuum of health promotion, disease prevention, diagnosis, treatment, management, rehabilitation, and palliative care and is characterized by a high degree of coordination and continuity among healthcare providers working across organizations and levels of healthcare.12,13 Previous studies have demonstrated that integrated care is an effective means of improving symptoms, signs, and health-related quality of life,14,15 as well as reducing hospitalization rates, healthcare expenditure, and all-cause mortality.16,17
Although principles, frameworks, and projects of the healthcare for older adults with multimorbidity have appeared in literature for many years, such as the Guiding Principles of the Care for Older Adults with Multimorbidity published by the American Geriatrics Society18 and the Integrated Care for Older People project proposed by the WHO,11 a majority of studies focus on clinical practice rather than organization management and policy making. However, optimizing healthcare services is not only determined by clinical practice but also characteristics of healthcare system and social context. Therefore, factors that impact the successful implementation of integrated care from both a top-down (policy-driven) and bottom-up (practice-driven) perspectives, which is more consistent with the complex mechanism of integrated care,19 should be highlighted.
Considering the available evidence and the lack of comprehensive research on integrated care in China, the purpose of this study was to identify factors that impact the successful implementation of integrated care for older adults with multimorbidity from the perspective of Chinese healthcare providers and managers. The questions that guided this study were as follows: “What factors contribute to the provision of integrated care for older adults with multimorbidity in the Chinese context?” and, “What factors impede the provision of integrated care for older adults with multimorbidity in the Chinese context?”
Materials and Methods
Theoretical Framework
The Rainbow Model of Integrated Care (RMIC) served as the theoretical framework for this study. This framework combines primary healthcare functions (first contact, continuous, comprehensive, and coordinated care) with integrated care dimensions, including clinical, professional, organizational, system, functional, and normative integration (Figure 1 and Table 1).20 The fundamental principle of primary healthcare is to incorporate the physical, mental, and societal aspects of health and wellness, expressed in RMIC as person-focused and population-based care.20 The person-focused and population-based care perspectives provide a foundation upon which the entire conceptual framework rests, indicating that primary healthcare is the starting point from where to integrate care.20
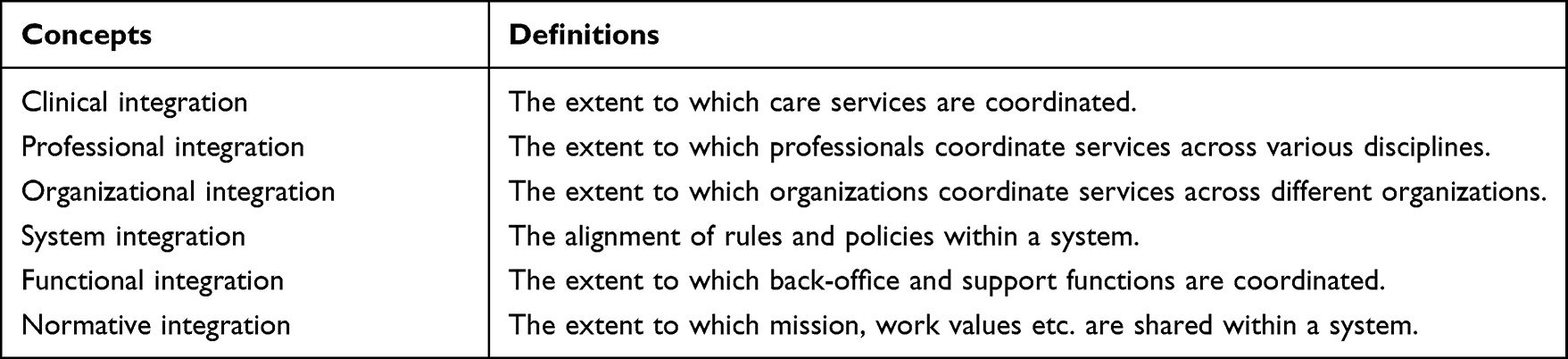 |
Table 1 Key Concepts and Definitions of the Rainbow Model of Integrated Care |
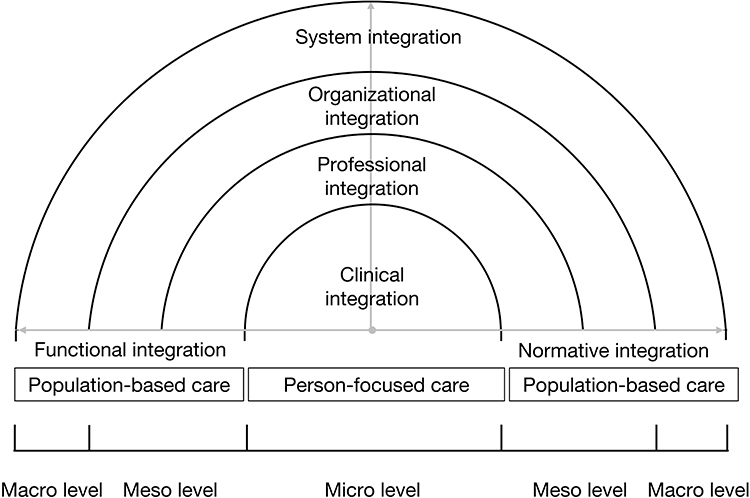 |
Figure 1 The Rainbow Model of Integrated Care. |
Study Design
A descriptive qualitative study design was used in this study to gain rich insights into the perspectives of healthcare providers and managers involved in healthcare service delivery for older adults with multimorbidity.21 The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used to report the study’s findings.22
Study Setting
This study was conducted in urban and rural areas of Zhejiang Province, one of the national pilot provinces of the integrated care system in China. The healthcare system in Zhejiang is a typical three-tiered system, consisting of primary healthcare settings and secondary and tertiary hospitals. Primary healthcare settings include township health stations and village clinics in rural areas and community health centers in urban areas; secondary hospitals include district and county hospitals; and tertiary hospitals include city and provincial hospitals. It is notable that since the 1980s, characterized by excessive marketization, the general population in China does not need to be referred by primary healthcare providers and can directly choose any level of healthcare for their first contact or other services.23
Sampling Strategy and Recruitment
Since various healthcare providers and managers are involved in the delivery and management of integrated care for older adults with multimorbidity, purposeful and maximum variation sampling methods were applied to recruit a diversity of healthcare providers and managers from different disciplines, organizations, and levels of healthcare.24,25 Regional economic development was also considered in this study since it may impact the provision of healthcare services. Thus, healthcare providers and managers working across disciplines were recruited from 11 healthcare organizations of different levels (primary healthcare settings, secondary hospitals, and tertiary hospitals) in Ningbo (highly developed city), Jinghua (moderately developed city), Huzhou (moderately developed city), and Zhoushan (underdeveloped city), Zhejiang Province. Furthermore, to ensure the richness and trustworthiness of data, healthcare providers and managers were limited to those who have participated in healthcare services delivery and management for older adults with multimorbidity for at least two years.
Potential participants were recruited by contacting the heads of the nursing departments in these organizations. The investigator then contacted them by phone and asked if they were willing to participate in the study.
Data Collection
This study employed the method of semi-structured, face-to-face in depth interviews because it is appropriate for exploring various respondents’ perceptions and opinions regarding complex and sometimes sensitive issues.26 To enhance the objectivity, trustworthiness, and richness of the data that were collected from semi-structured interviews, we followed a five-phase method to develop the interview guide (Box 1), including (i) identifying the prerequisites for using semi-structured interviews; (ii) retrieving and using previous knowledge; (iii) formulating the preliminary interview guide; (iv) pilot testing the interview guide; and (v) presenting the complete interview guide.27
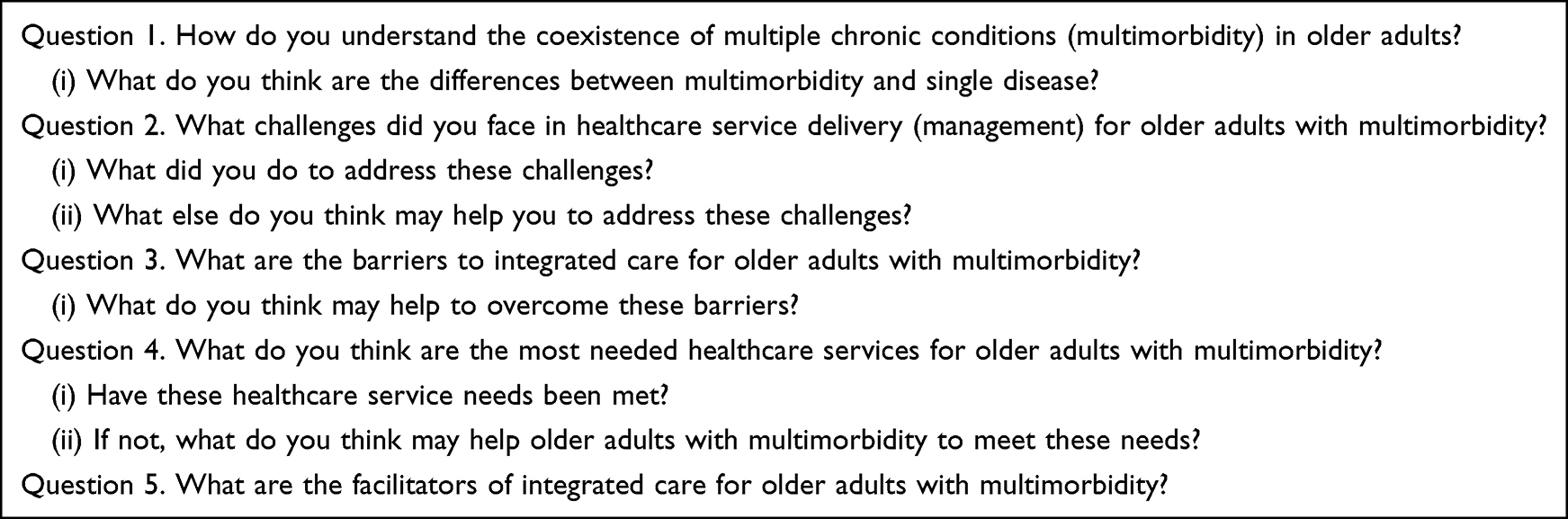 |
Box 1 The Semi-Structured Interview Guide |
Each interview was performed by the same investigator to ensure consistency. The investigator is a Ph.D. candidate who has received professional training in qualitative research and semi-structured interviews. The investigator and interviewees were mutually unknown to each other before the interviews. All interviews were conducted in a quiet area of interviewees’ offices and audio-recorded. To facilitate consistent interpretation, commonly used definitions of key concepts, including “multimorbidity” and “integrated care” were provided before the interviews.1,12,13 Field notes were made during the interviews to document needed contextual information.28
The investigator used professional software (iFLYTEK) to convert the audio recordings into interview transcripts within 24 hours after each interview. The interview transcripts were then analyzed. The assessment of data saturation depended on the analysis conducted for each interview transcript. When the interviewee no longer presented significant additional views, the investigator continued the interviews with two more interviewees. If no additional information emerged, we considered that data saturation had been achieved and concluded the process of data collection.24,25 The data was collected from July 2022 to May 2023.
Data Analysis
Inductive thematic analysis was used for data analysis by two coders.29 They are both Ph.D. candidates with a rich theoretical foundation in qualitative research, thematic analysis, and integrated care. After transcribing and familiarizing with the dataset, initial codes were generated by coders using an iterative approach. Conflicting codes were further discussed between two coders and, if necessary, in consultation with the senior researcher (corresponding author), until a consensus was reached. Similar codes were synthesized into potential themes, and then all codes and themes were checked by two coders through face-to-face discussions to ensure that all themes reflected the codes and the entire dataset. Until a consensus regarding themes and codes was reached within the research group, themes were mapped onto six dimensions of care integration proposed by the RMIC using a previous approach.20,30 The RMIC provided possible connections and facilitated the establishment of themes, subsequently allowing for a comprehensive view of the study’s findings.30 QSR NVivo software (version 12) was used to manage the data.
Rigor
The trustworthiness and rigor of this qualitative study were achieved by ensuring the dependability, confirmability, credibility, and transferability of data.31 The audit trails and field notes of all the transcripts used in data collection and analysis were used to ensure dependability. To enhance confirmability, coding was performed by two independent and well-trained coders and reviewed by all researchers. To ensure credibility, the investigator was trained to conduct semi-structured interviews using an interview guide that was developed through a standardized five-phase method and pilot-tested. The use of data saturation during the collection process ensured the transferability of the findings.
Ethical Consideration
Ethics approval was obtained from the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine (ID: 2022-477-01). Our research protocol is in compliance with the Helsinki Declaration. We have obtained informed consent from all participants and ensured their privacy throughout the study. The participants informed consent included the publication of anonymized responses.
Results
Participant Characteristics
Thirty-three healthcare providers and managers were interviewed from primary healthcare settings (n=7), secondary hospitals (n=22), and tertiary hospitals (n=4). They were from family medicine/public health (n=7), general practice (n=6), geriatrics (n=4), specialties (n=5), rehabilitation (n=1), administration (n=9), and other department (n=1). The detailed information of the interviewees can be found in Supplementary Material Table 1.
Themes
Eleven themes were generated regarding the facilitators and barriers to integrated care for older adults with multimorbidity. These themes were further mapped onto the integrated care dimensions proposed by the RMIC, as shown in Figure 2.
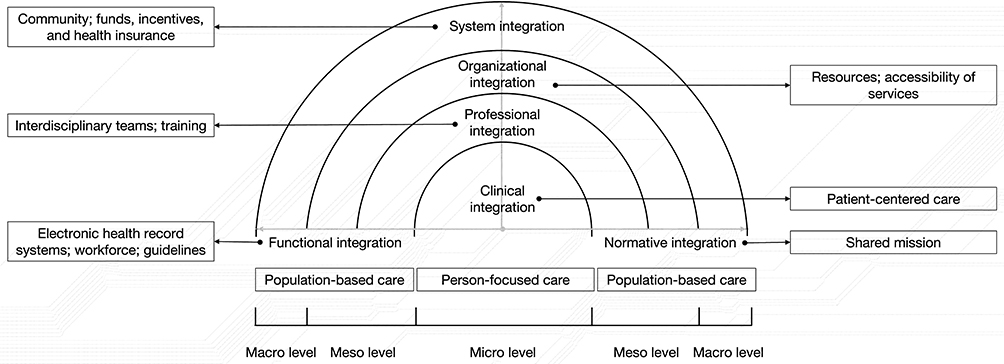 |
Figure 2 Results of the thematic analysis based on the Rainbow Model of Integrated Care. |
Dimension 1: Clinical Integration
Patient-Centered Care
A focus on the patient’s evolving health problems, needs, priorities, and goals through the use of an individual care plan that is dynamically revised was noted by some interviewees as a key facilitator in providing integrated care for older adults with multimorbidity.
The health conditions of older adults with multimorbidity are much more complex than those with only one type of chronic condition. The patient [older adults with multimorbidity] may need hospitalization because their blood pressure has not been well controlled at this time. However, they may not always have only one health problem; they are likely to experience new problems in the future. [.] The purpose of regular provider-patient communication is not only to inquire about patients’ recent conditions but also to provide information for revising patients’ treatment plans dynamically. (#31, Director of Geriatrics)
Moreover, targeting vulnerable populations (eg, older adults living in rural areas, those with physical disabilities, and those lacking social support) who may face unusually great barriers regarding the accessibility of healthcare services was also identified by interviewees as crucial. Some of them believed that home care, which provides multiple healthcare services by family physicians, community nurses, pharmacists, and other professionals at the patient’s homes, might be a facilitator to enhance care accessibility and ensure care equity.
Some old adults live in the mountains. Their children work outside and are often not at home. It is inconvenient and time-consuming for them to go to the township health station and hospital to get medications. (#1, General Practitioner)
More healthcare resources should be brought to patients’ homes to complete the last mile of healthcare. (#6, Director of Family Medicine)
Dimension 2: Professional Integration
Interdisciplinary Teams
Some interviewees pointed out that interdisciplinary teams, consisting of healthcare providers from various disciplines was an advantage that integrated care had over isolated healthcare providers. They mentioned that when multiple healthcare providers served patients separately, the patients might receive different or even conflicting information, which posed a barrier to care coordination and could lead to adverse effects on patient health. Moreover, they expressed that accessing, navigating, and coping with different healthcare services delivered by multiple healthcare providers further increased patients’ and their families’ healthcare costs and treatment burdens.
There was a diabetes patient who used insulin. We advised him to inject insulin at a distance greater than one fist away from the navel, as injecting too close to the navel may damage vessels or nerves. However, he explained that his family physician had instructed him to inject insulin within a 5 cm radius around the navel. (#30, Clinical Nurse of Geriatrics)
Appointing a primary decision-maker in each interdisciplinary team was identified as an additional facilitator to enhance the coordination of healthcare. Well-defined responsibilities, accountabilities, and workflows enable this role to function effectively.
In clinical practice, there is a need for a role to coordinate the opinions of different specialists. (#32, Director of Geriatrics)
Several interviewees highlighted that larger interdisciplinary teams, which included patients and their informal caregivers (mainly family members), also had advantages in promoting shared decision-making and patient-centered care. However, they also stated that it was difficult to transform patients from passive recipients to active participants.
Medicine is not mandatory. As a physician, I cannot force patients to change their lifestyle if they are unwilling to do so. (#8, Director of Neurology)
Vulnerable populations (eg, older adults living in rural areas, those with physical disabilities, and those lacking health and digital literacy) may face catastrophic barriers in care accessibility and self-management tasks. Therefore, it was noted as particularly important to actively involve informal caregivers in the healthcare process. Moreover, interviewees acknowledged that when patients’ informal caregivers were also old adults, especially those with individual or multiple chronic conditions, there might be risks instead of benefits since providing informal care could have adverse effects on the physical and mental health of informal caregivers.
If there is an active engagement of informal caregivers, especially young and middle-aged adults, the quality of life for older adults with multimorbidity can be substantially improved. (#33, Nurse Manager of Nephrology)
Training
Two main challenges regarding professional training were mentioned by interviewees. First, ill-prepared healthcare providers lacked the knowledge, skills, confidence, and motivation to deal with the complexity and heterogeneity of multimorbidity. Additionally, traditional training approaches trained providers from different disciplines in isolation rather than collaboratively. These challenges could further threaten the quality of healthcare and patient safety in an aging society.
Many healthcare providers do not know how to collaborate within a team because previous medical education was isolated, with physicians attending only medical lectures, nurses attending only nursing lectures, and pharmacists attending only pharmacy lectures. (#8, Director of Neurology)
Training all healthcare providers with a basic level of generalist knowledge and skills, such as comprehensive geriatric assessment, the identification of geriatric syndromes and frailty, blood pressure and blood glucose management, and competitions between commonly-used medications were proposed by interviewees to help prepare providers.
Dimension 3: Organizational Integration
Resources
Imbalanced resource distribution with much more resources concentrated at tertiary hospitals was noted by interviewees, particularly those working in primary healthcare settings, as inefficient, costly, and can not meet the healthcare needs of patients with chronic conditions. It was expected by interviewees that policymakers would allocate more high-quality resources to the primary healthcare system.
Whether at an individual or social level, the healthcare expenses for disease treatment are always much higher than those for disease prevention. Healthcare expenses for treating disease complications are also much higher than those for long-term management of diseases. (#8, Director of Neurology)
Accessibility of Services
A good relationship between healthcare providers from different organizations and levels of healthcare was noted as a facilitator for improving care accessibility through expert consultation and referrals. In addition, the long distance between healthcare organizations and limited access to public transportation were identified as barriers regarding physical accessibility of care.
Some medications are unavailable here [a community health center]. Thus, we have to refer patients to a county hospital for the prescription. However, the hospital is distant from our location. (#7, Director of Family Medicine)
Dimension 4: System Integration
Community
A minority of interviews mentioned the important role of the community (eg, well-trained social workers) in facilitating the continuity of care from healthcare organizations to patients’ homes.
These older adults [with multimorbidity] not only have healthcare needs but also need assistance in their daily lives. The latter can be provided by well-trained social workers. However, the operational mechanism of social workers is not yet very mature in China. (#31, Director of Geriatrics)
Funds, Incentives, and Health Insurance
Lots of interviewees reported that inadequate funding from the government, a lack of incentive mechanisms, and insufficient health insurance reimbursement were significant obstacles to integrated care.
Inadequate government funds have made healthcare organizations self-sufficient in finance, which has not only established a linkage between the income of medical staff and the healthcare costs of patients but also impeded the capacity-building of healthcare organizations, especially in primary healthcare settings.
It is important that government funds and health insurance do not create conflicts between patients and healthcare providers. (#8, Director of Neurology)
In addition, the lack of incentive mechanisms may not be sufficient to motivate healthcare providers to provide patient-centered care and work within interdisciplinary teams.
If we prescribe medication excessively to patients, we will be punished. However, if we do not prescribe enough medication to patients, we are not following patient-centered care. Some patients live far away. It is inconvenient for them to make multiple trips to hospitals for prescription. (#10, Director of General Practice)
Furthermore, insufficient reimbursement of health insurance has restricted patients’ access to various healthcare services. For example, economically disadvantaged patients would choose not to use home-based healthcare services because most of these services could not be reimbursed by health insurance.
Dimension 5: Functional Integration
Electronic Health Record Systems
An inadequately integrated electronic health record system that failed to share information among healthcare providers from different organizations and levels of healthcare was identified as an important barrier. Interviewees mentioned that since the electronic health record system was not integrated, much information was self-reported by patients and their informal caregivers, which could lead to recall bias and was considered time-consuming.
The regular follow-up for chronic conditions is carried out by primary healthcare providers. Due to the non-integrated electronic health record system, it is impossible for us [healthcare providers in hospitals] to obtain patients’ updated information from primary healthcare settings, such as the accurate values of blood pressure and blood glucose. (#31, Director of Geriatrics)
Another barrier perceived by interviewees was the lack of patient portals, which would allow patients and informal caregivers to obtain detailed care plans and update their evolving health problems, needs, priorities, and goals on the electronic health record system. However, interviewees also expressed concerns that for older adults with poor digital literacy and who do not have informal caregivers to provide support, the use of patient portals may further exacerbate healthcare inequality.
Workforce
A diminished workforce across all levels of healthcare, especially family physicians, general practitioners, and geriatricians was reported by interviewees that could result in a fast pace and inadequate time for care episodes as well as excessive workloads for healthcare providers. They proposed a better balance between generalists who follow the physio-psycho-social care model and can manage multimorbidity and polypharmacy, and specialists, instead of continuing a growing trend towards specialization.
To address the short supply of generalists in the primary healthcare system, one solution recommended by interviewees was to address the problem of medical staff and the general population’s attitudes towards primary healthcare providers, including any lack of trust or confidence regarding their professionalism.
It is a vicious circle. The more discrimination is experienced in the primary healthcare system, the less highly educated professionals are to work in the primary healthcare system. (#6, Director of Family Medicine)
Guidelines
The complex and heterogeneous nature of older adults with multimorbidity rendered traditional single-disease-focused guidelines often inadequate, complicated clinical decision-making, and posed a substantial challenge to the competence of healthcare providers. Several interviewees hold the view that an integrated approach to multimorbidity should be considered in future guidelines to facilitate evidence-based practice and integrated care. Such guidelines could address clusters of chronic conditions with high prevalence and disease burden, as well as comprehensive management for older adults with multimorbidity.
There are many single-disease-focused guidelines nowadays. As geriatricians, it is challenging for us to be proficient in all prevalent disease guidelines, and make individualized decisions based on patients’ conditions. (#21, Director of Geriatrics)
Dimension 6: Normative Integration
Shared Mission
A focus on holistic healthcare was identified as an essential facilitator of integrated care, and was recommended by some interviewees to be a mission that should be shared by all staff within the healthcare system.
Humans are complex beings with physiological, psychological, and social attributes, and are not simply an accumulation of multiple organs. Physicians treat not just one or several diseases, but a whole person. (#31, Director of Geriatrics)
Discussion
This descriptive qualitative study identified facilitators and barriers to integrated care for older adults with multimorbidity from the perspective of Chinese healthcare providers and managers. Then, these factors were mapped onto clinical, professional, organizational, system, functional, and normative dimensions based on the Rainbow Model of Integrated Care (RMIC) to ensure a comprehensive view of the study’s findings. Although previous studies have explored the management of older adults with multimorbidity from the perspective of healthcare providers and synthesized six themes,23 including the incorporation of shared decision-making and patient preferences, evidence base, patient prognosis, optimizing therapies and health management plans, and care coordination; this study, employing the RMIC as a theoretical framework, identified factors that impact the implementation of integrated care not only at the level of clinical practice but also at the levels of organization management and policy making.
The World Health Organization (WHO) proposes person-centered integrated care and primary healthcare services as a response to population aging, with the goal of promoting healthy aging.11 RMIC also takes both person-focused and population-based care perspectives into consideration and integrates the entire conceptual framework with the functions of primary healthcare.20 The above evidence confirms the importance of primary healthcare in providing integrated care. In this study, we found that many facilitators and barriers to integrated care proposed by Chinese healthcare providers and managers are related to the primary healthcare system. Firstly, as one of the facilitators, it was considered that primary healthcare should undertake the responsibility for home-based healthcare in order to enhance accessibility and reflect patient-centered care. Secondly, the unequal distribution of high-quality healthcare resources between primary care settings and hospitals hindered the development of primary healthcare and was also not conducive to providing efficient and affordable healthcare services, which is congruent with previous studies.32 Therefore, interviewees highlighted that measures should be taken in the future to balance the allocation of resources between healthcare organizations, eliminate the stigmatization of primary healthcare providers, and promote the capacity of the primary healthcare system.
This study also found that coordination and cooperation within the healthcare system are crucial for the implementation of integrated care in China. This is reflected in two aspects: first, the formation of interdisciplinary teams by healthcare providers in the same organization; second, cooperation between providers from different healthcare organizations or levels. Innovative training approaches that emphasize teamwork and integrated electronic health record systems that highlight information sharing were two facilitators for the coordination and cooperation of healthcare providers working across disciplines, organizations, and levels. In previous research, it was found that these research findings are also applicable to the healthcare system in the United Kingdom.33 Active engagement of patients and their informal caregivers was also considered as broad interdisciplinary teamwork, which is consistent with the manifesto proposed by Kunneman and colleagues.34 The shared mission that emphasizes holistic healthcare within the healthcare system was regarded as another facilitator for coordinating healthcare service delivery.
Coordination and cooperation between the healthcare system and other sectors were also believed by interviewees to have the potential to impact the implementation of integrated care. For example, government financial investment in the healthcare system and healthcare insurance, as well as the role of age-friendly communities in increasing the continuity and coordination of care between hospitals and families.35,36
Another contribution of this study is that we found it necessary to provide care and support to healthcare providers while implementing integrated care for patients. This viewpoint has also been proposed by Bodenheimer and Sinsky, who stated that “the care of the patient requires the care of the provider” and included “the work-life balance for healthcare providers” as one of the four main aims of healthcare.37 Several factors mentioned by interviewees, such as the workforce, incentive mechanisms, and guidelines, may contribute to attenuating or eliminating burnout among healthcare providers.
Strengthens and Limitations
One strength of this study is the wide range of participants from different disciplines, organizations, and levels of healthcare. In addition, semi-structured, face-to-face in-depth interviews enable open-ended probing and deeper exploration of participants’ genuine thoughts.38 These two approaches allow for a broad understanding of factors that impact integrated care for older adults with multimorbidity.
This study also has several limitations. Given the wide variation in healthcare systems and integrated care models across the globe, the findings of this study possess significant cultural specificity. This means that they cannot simply be generalized to other cultures or contexts. Furthermore, based on the qualitative methodology, the sampling strategy was aimed to achieve maximum variation among participants and data saturation rather than being numerically representative. Moreover, healthcare providers who do not directly provide services to older adults with multimorbidity in China (eg, clinical pharmacists) were not recruited in this study. Lastly, the participants involved in this study were healthcare providers and managers, while the voice of patients and informal caregivers is not well represented. Patients and informal caregivers should be recruited in the future to express their points of view regarding facilitators and barriers to integrated care.
Conclusion
In this study, various factors that impact the implementation of integrated care for older adults with multimorbidity were identified. The proposal for future interventions and policies should focus on promoting facilitators and addressing barriers.
Acknowledgments
The authors would like to express gratitude to all the participants who voluntarily participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Institute for Health and Care Excellence (NICE). Multimorbidity: clinical assessment and management; 2016. Available from: https://www.nice.org.uk/guidance/ng56.
2. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
3. Yao SS, Cao GY, Han L, et al. Prevalence and Patterns of Multimorbidity in a Nationally Representative Sample of Older Chinese: results From the China Health and Retirement Longitudinal Study. J Gerontol a Biol Sci Med Sci. 2020;75(10):1974–1980. doi:10.1093/gerona/glz185
4. Morris JE, Roderick PJ, Harris S, et al. Treatment burden for patients with multimorbidity: cross-sectional study with exploration of a single-item measure. Br J Gen Pract. 2021;71(706):e381–e390. doi:10.3399/BJGP.2020.0883
5. Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health. 2018;3(7):e323–e332. doi:10.1016/S2468-2667(18)30091-4
6. Marengoni A, Akugizibwe R, Vetrano DL, et al. Patterns of multimorbidity and risk of disability in community-dwelling older persons. Aging Clin Exp Res. 2021;33(2):457–462. doi:10.1007/s40520-020-01773-z
7. Li HW, Lee WJ, Lin MH, et al. Quality of Life among Community-Dwelling Middle-Aged and Older Adults: function Matters More than Multimorbidity. Arch Gerontol Geriatr. 2021;95:104423. doi:10.1016/j.archger.2021.104423
8. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev. 2011;68(4):387–420. doi:10.1177/1077558711399580
9. Zhao Y, Atun R, Oldenburg B, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Glob Health. 2020;8(6):e840–e849. doi:10.1016/S2214-109X(20)30127-3
10. La DTV, Zhao Y, Arokiasamy P, et al. Multimorbidity and out-of-pocket expenditure for medicines in China and India. BMJ Glob Health. 2022;7(11):e007724. doi:10.1136/bmjgh-2021-007724
11. The World Health Organization (WHO). Integrated care for older people: guidelines on community-level interventions to manage declines in intrinsic capacity. Geneva; 2017. Available from: https://www.who.int/publications/i/item/9789241550109.
12. The American Psychological Association (APA). Integrated Health Care; 2013. Available from: https://www.apa.org/health/integrated-health-care.
13. The World Health Organization (WHO). Sixty-Ninth World Health Assembly, A69/39: framework on integrated, people-centred health services. Geneva; 2016. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA69/A69_39-en.pdf?ua=1&ua=1.
14. Chen S, Conwell Y, Xue J, et al. Effectiveness of integrated care for older adults with depression and hypertension in rural China: a cluster randomized controlled trial. PLoS Med. 2022;19(10):e1004019. doi:10.1371/journal.pmed.1004019
15. Rajan R, Brennan L, Bloem BR, et al. Integrated Care in Parkinson’s Disease: a Systematic Review and Meta-Analysis. Mov Disord. 2020;35(9):1509–1531. doi:10.1002/mds.28097
16. Gallagher C, Elliott AD, Wong CX, et al. Integrated care in atrial fibrillation: a systematic review and meta-analysis. Heart. 2017;103(24):1947–1953. doi:10.1136/heartjnl-2016-310952
17. Cronin J, Murphy A, Savage E. Can chronic disease be managed through integrated care cost-effectively? Evidence from a systematic review. Ir J Med Sci. 2017;186(4):827–834. doi:10.1007/s11845-017-1600-5
18. American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. Patient-centered care for older adults with multiple chronic conditions: a stepwise approach from the American Geriatrics Society: American Geriatrics Society Expert Panel on the Care of Older Adults with Multimorbidity. J Am Geriatr Soc. 2012;60(10):1957–1968. doi:10.1111/j.1532-5415.2012.04187.x
19. Kodner DL, Spreeuwenberg C. Integrated care: meaning, logic, applications, and implications--a discussion paper. Int J Integr Care. 2002;2:e12. doi:10.5334/ijic.67
20. Valentijn PP, Schepman SM, Opheij W, Bruijnzeels MA. Understanding integrated care: a comprehensive conceptual framework based on the integrative functions of primary care. Int J Integr Care. 2013;13:e010. doi:10.5334/ijic.886
21. Bradshaw C, Atkinson S, Doody O. Employing a Qualitative Description Approach in Health Care Research. Glob Qual Nurs Res. 2017;4:2333393617742282. doi:10.1177/2333393617742282
22. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
23. Hu H, Liang H, Wang H. Longitudinal study of the earliest pilot of tiered healthcare system reforms in China: will the new type of chronic disease management be effective? Soc Sci Med. 2021;285:114284. doi:10.1016/j.socscimed.2021.114284
24. Mc Namara KP, Breken BD, Alzubaidi HT, et al. Health professional perspectives on the management of multimorbidity and polypharmacy for older patients in Australia. Age Ageing. 2017;46(2):291–299. doi:10.1093/ageing/afw200
25. Moser A, Korstjens I. Series: practical guidance to qualitative research. Part 3: sampling, data collection and analysis. Eur J Gen Pract. 2018;24(1):9–18. doi:10.1080/13814788.2017.1375091
26. Barriball KL, While A. Collecting data using a semi-structured interview: a discussion paper. J Adv Nurs. 1994;19(2):328–335. doi:10.1111/j.1365-2648.1994.tb01088.x
27. Kallio H, Pietilä AM, Johnson M, Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72(12):2954–2965. doi:10.1111/jan.13031
28. Phillippi J, Lauderdale J. A Guide to Field Notes for Qualitative Research: context and Conversation. Qual Health Res. 2018;28(3):381–388. doi:10.1177/1049732317697102
29. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
30. Green J, Willis K, Hughes E, et al. Generating best evidence from qualitative research: the role of data analysis. Aust N Z J Public Health. 2007;31(6):545–550. doi:10.1111/j.1753-6405.2007.00141.x
31. Lincoln Y, Guba E. Naturalistic Inquiry. Beverly Hills, CA: SAGE; 1985.
32. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
33. Anderson M, O’Neill C, Macleod Clark J, et al. Securing a sustainable and fit-for-purpose UK health and care workforce. Lancet. 2021;397(10288):1992–2011. doi:10.1016/S0140-6736(21)00231-2
34. Kunneman M, Griffioen IPM, Labrie NHM, et al. Making care fit manifesto. BMJ Evid Based Med. 2023;28(1):5–6. doi:10.1136/bmjebm-2021-111871
35. Jeste DV, Blazer DG 2nd, Buckwalter KC, et al. Age-Friendly Communities Initiative: public Health Approach to Promoting Successful Aging. Am J Geriatr Psychiatry. 2016;24(12):1158–1170. doi:10.1016/j.jagp.2016.07.021
36. Dambha-Miller H, Simpson G, Hobson L, et al. Integrating primary care and social services for older adults with multimorbidity: a qualitative study. Br J Gen Pract. 2021;71(711):e753–e761. doi:10.3399/BJGP.2020.1100
37. Bodenheimer T, Sinsky C. From triple to quadruple AIM: care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573–576. doi:10.1370/afm.1713
38. Sullivan-Bolyai S, Bova C, Harper D. Developing and refining interventions in persons with health disparities: the use of qualitative description. Nurs Outlook. 2005;53(3):127–133. doi:10.1016/j.outlook.2005.03.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.