Back to Journals » Patient Preference and Adherence » Volume 20
Facilitating and Hindering Factors in Discharge Preparation During the Hospital-to-Home Transition Period for Newly Diagnosed Tuberculosis Patients: A Qualitative Study
Authors Yu Q, Hu Y, Yao R, Zhang T, Huang L, Li Y, Wan B, Xie F ![]() , Shao X, Yang X
, Shao X, Yang X
Received 11 February 2026
Accepted for publication 19 June 2026
Published 24 June 2026 Volume 2026:20 602859
DOI https://doi.org/10.2147/PPA.S602859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Qiaolin Yu,1,* Yinping Hu,1,* Rong Yao,1 Ting Zhang,1 Leilei Huang,1 Yuanyuan Li,1 Bin Wan,2 Fanghui Xie,1 Xiaoli Shao,1 Xiaoyi Yang1
1The Department of Tuberculosis, Public Health Clinical Center of ChengDu, Chengdu, Sichuan, People’s Republic of China; 2The Department of Nursing, Public Health Clinical Center of ChengDu, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyi Yang, The Department of Tuberculosis, Public Health Clinical Center of ChengDu, Chengdu, Sichuan, People’s Republic of China, Tel +86 18200426273, Email [email protected] Xiaoli Shao, The Department of Tuberculosis, Public Health Clinical Center of ChengDu, Chengdu, Sichuan, People’s Republic of China, Tel +86 13684032494, Email [email protected]
Objective: The aim of this study is to identify the barriers and facilitating factors affecting discharge preparation during the hospital-to-home transition period for treatment-naïve tuberculosis patients, thereby providing a basis for the development of personalised interventions.
Methods: This study employed a qualitative descriptive research design. Using purposive and maximum diversity sampling strategies, 15 treatment-naïve tuberculosis patients were selected from an infectious diseases hospital in western China to participate in semi-structured in-depth interviews. The interview data was then organised, analysed and distilled using the Colaizzi 7-step analysis method.
Results: The discharge experience during the hospital-to-home transition period for newly diagnosed TB patients comprised two themes and seven subthemes. These included facilitating factors for discharge preparedness diverse home-based treatment supervision methods, plentiful digital healthcare resources, strong desire to return to work, and robust social support and impeding factors for discharge preparednessLack of disease knowledge, Unmet needs regarding patient self-management and a heavy psychological burden.
Conclusion: This study demonstrates that the discharge preparedness of newly diagnosed TB patients during the hospital-to-home transition is influenced by multiple factors. Healthcare professionals should conduct precise assessments of patients’ discharge preparedness challenges, utilizing these factors to deliver targeted discharge preparation training.
Keywords: initial treatment, tuberculosis, discharge preparation, qualitative research
Introduction
TB is a significant infectious disease posing a grave threat to human health and life. Newly diagnosed TB refers to pulmonary TB that is identified for the first time, has not previously undergone anti-tuberculosis treatment, or has received irregular or inappropriate anti-tuberculosis treatment for no more than one month following diagnosis.1 According to WHO statistics, in 2025 there were approximately 10.7 million new cases of tuberculosis worldwide (compared to 10.8 million in 2023), with approximately 1.23 million deaths attributed to the disease, representing a case-fatality rate of 11.5%.2
The treatment period for newly diagnosed TB patients is typically no less than six to eight months.3 Even after discharge from hospital, prolonged home-based anti-tuberculosis medication is required.4 Following discharge, patients may still encounter a range of challenges concerning treatment and prevention, such as insufficient knowledge about TB, poor self-management and coping abilities, misconceptions about their health status, medication side effects, lack of family support, and low self-efficacy. These factors may lead to patients discontinuing treatment prematurely, thereby increasing the risk of disease recurrence and drug resistance, which in turn contributes to higher rates of unplanned readmission.5,6 A systematic review incorporating 145 studies reported a combined recurrence rate of 2.26 per 100 person-years (95% CI, 1.87–2.73).7 With the ongoing advancement of TB control strategies and the deepening of patient-centred care principles, hospital-to-home transition management has become a critical component in enhancing treatment outcomes for newly diagnosed TB cases. Readiness for discharge, as the core concept of this transitional phase, directly determines whether patients can achieve a smooth transition from hospital to home and influences the continuity and success rate of subsequent treatment.8 Research indicates that thorough discharge preparation is not only crucial for enhancing patients’ quality of life following hospital discharge, but also exerts a positive influence on accelerating the recovery process and reducing readmission rates.9,10
However, Current research on the discharge preparedness of newly diagnosed tuberculosis patients has primarily focused on surveys of the current situation and the exploration of influencing factors (such as disease awareness, family support and models of medical guidance);11,12 qualitative studies that explore patients’ experiences of preparedness in depth are relatively limited. Consequently, this study employs semi-structured in-depth interviews to analyse patients’ personal experiences during the discharge preparation process and comprehensively examine the facilitating and hindering factors. The aim is to gain an in-depth understanding of their unmet needs and to provide a reference for the development of targeted, individualised support strategies for discharge preparation.
Methods
Study Design
Descriptive qualitative research is grounded in naturalistic inquiry, emphasizing the diversity of participants lived experiences and its inherent interconnectedness. By collecting participants’ direct descriptions and interpretations of events, this methodology presents phenomena themselves in a coherent, structured manner, thereby intuitively revealing their essential characteristics. It is particularly suited to studies examining people’s perceptions, feelings, and influencing factors regarding specific experiences, behaviours, or situations.13
This study employed a descriptive qualitative research methodology (as shown in Supporting information 1) to explore the lived experiences of newly diagnosed TB patients during the transition phase from hospital to home. Its aim is to provide the most direct description and presentation of these patients’ experiences during this transitional period, while directly summarising the factors influencing their hospital-to-home transition journey, thereby enabling low-inference interpretation. It does not seek to develop theories regarding discharge preparation for this transition phase nor to conduct deep interpretations of the underlying meanings of patients’ discharge experiences. Consequently, this research methodology is considered appropriate.
Participants
Participants were selected through purposive sampling based on the principle of maximum variation, considering factors such as patients’ sex, age, educational level, marriage, Housing situation, Employment status, Monthly income, medical expense, primary carer, and hospital stay(d). The study subjects comprised newly diagnosed TB patients admitted to a designated infectious diseases hospital in Chengdu, China, between July and November 2025. Interviews were conducted as patients prepared for discharge.
Inclusion criteria: (1) Newly diagnosed TB patients according to WHO guidelines.14 (2) Age ≥ 18 years; (3) Receiving first-line anti-tuberculosis drugs (isoniazid, rifampicin, pyrazinamide, ethambutol); (4) Patients with a doctor’s order for discharge; (5) Normal cognitive and communication abilities, capable of completing the interview independently; (6) Informed consent and voluntary participation (as shown in Supporting information 2).
Exclusion criteria: (1) Severe dysfunction of vital organs such as the heart or lungs, and serious mental illness; (2) Recent occurrence of major events significantly impacting sleep or psychological well-being, such as severe trauma or the death of a close relative.
The sample size was determined on the basis of data saturation and the absence of new themes.15 In this study, the first signs of saturation were observed following the 13th interview; after completing the 14th and 15th interviews, it was confirmed that no new themes had emerged, and data collection was therefore terminated. Ultimately, 15 patients were interviewed.
Research Tools
Researcher
In this study, the researcher served as the primary research instrument. The principal investigator was a clinical nurse with over five years’ nursing experience, possessing profound insight into operational procedures and occupational characteristics. Throughout the research implementation, the investigator conducted scientific design and execution under the continuous supervision of two postgraduate nursing students and one psychological counsellor. To mitigate potential observer bias arising from the researcher’s professional identity, an additional interviewer role was fulfilled by the psychological counsellor. This interviewer served as the Head Nurse of the TB Department at a Grade A tertiary infectious diseases hospital. Possessing extensive counselling and management experience, she established strong rapport with the target population, meeting the competency requirements for interviewers in qualitative research.
Prior to commencing the research, investigators underwent systematic training to familiarise themselves with the characteristics and analytical procedures of Colaizzi’s seven-step analysis method for describing qualitative research, followed by assessment. Concurrently, they gained insight into the latest research landscape and developments within the study’s subject domain, thereby ensuring thorough preparation for the subsequent research endeavour.
General Demographic Survey Form
A self-administered demographic questionnaire, including patients’ sex, age, educational level, marriage, Housing situation, Employment status, Monthly income, medical expense, primary carer, and hospital stay(d) (see Table 1).
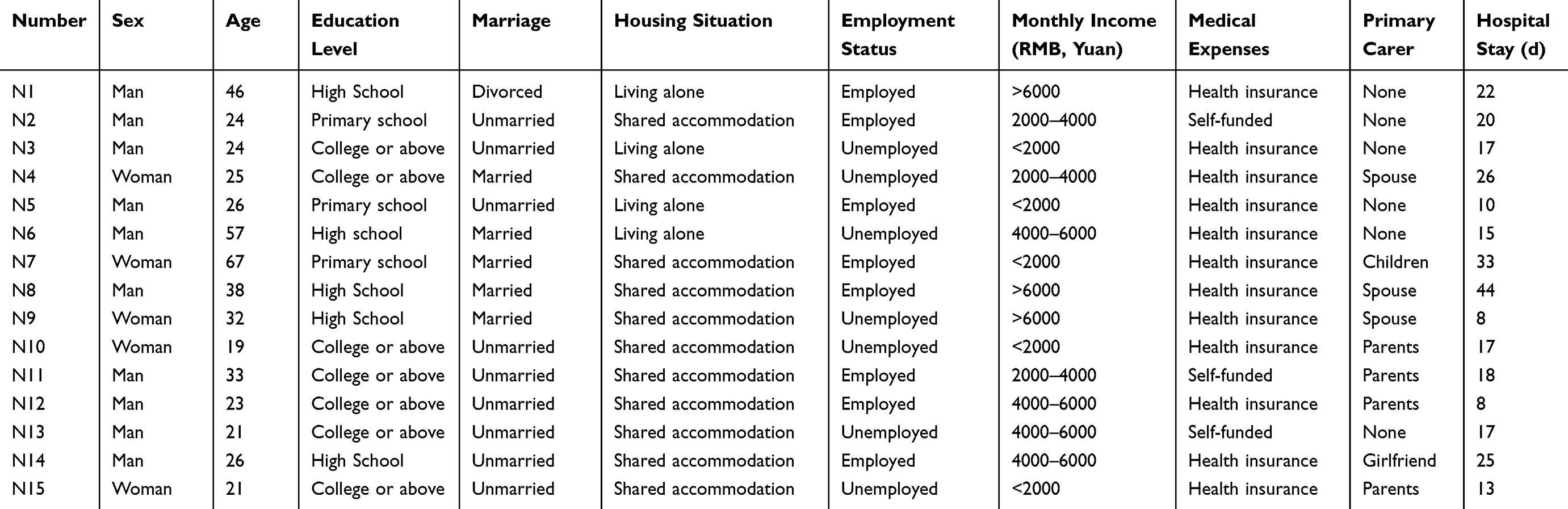 |
Table 1 General Information of Patients (n=15) |
Interview Outline
Based on the research objectives, the investigator, under the guidance of postgraduate students, drafted preliminary interview outlines through reviewing relevant literature.16–18 Following discussions within the research team (comprising two postgraduate students, one psychological counsellor, two senior nurses, and one nursing manager), the interview content was finalised to produce a first draft.
Prior to the formal interviews, the researcher obtained informed consent from three newly diagnosed TB patients undergoing hospital-to-home transition. A preliminary interview guide was used for pre-interviews, the results of which were excluded from the formal data analysis. During the interview process, the sequence and content of the guide were adjusted based on feedback, ultimately establishing the formal interview guide (see Figure 1).
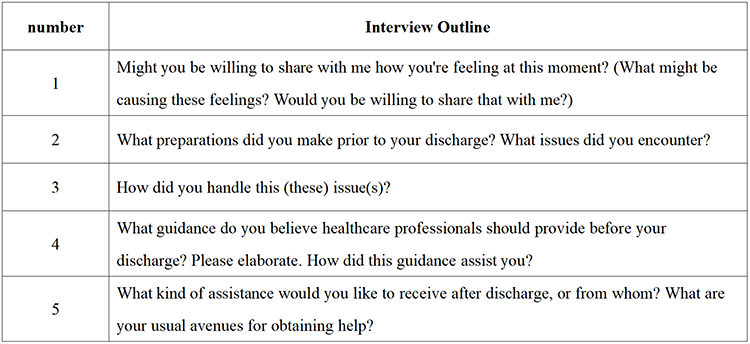 |
Figure 1 Interview Guide for Discharge Experiences During the Hospital-to-Home Transition Period for Newly Diagnosed TB Patients. |
Data Collection
This study employed face-to-face semi-structured interviews. The specific procedure comprised: sample recruitment, scheduling interview times, determining interview locations, and the actual implementation of the interview process.
Recruitment of Participants
Researchers first obtained consent from the Head of Nursing and departmental supervisors before requesting them to post recruitment notices in relevant departmental WeChat groups. Upon contacting newly diagnosed TB patients meeting eligibility criteria, researchers inquired whether they consented to participate in the study. Should consent be declined, the process concluded immediately; if consent was granted, interview times and locations were arranged.
Interview Process
- The day before the interview, the researcher reminded the participant of the time and location (a quiet, undisturbed office) and briefly informed them of the expected duration of the interview (30–60 minutes).
- The interview consists of two parts: in the first part, patients complete a questionnaire on general demographic information. Secondly, prior to the commencement of the study, the researchers explained the purpose, significance and confidentiality principles of the study to the patients in detail. Only after obtaining the patients’ informed consent did the researchers begin recording the interviews. All interviews were conducted by personnel with experience in qualitative research. Interviewers ensured the depth of the interviews by flexibly adjusting the sequence of questions, following the interviewee’s train of thought and probing further where appropriate; observing non-verbal cues such as facial expressions and body language; and employing interview techniques including verbal clarification, confirmation, response, repetition, probing and summarisation.
Data Analysis Methods
Interview Transcript and Compilation
Within one hour of the interview concluding, researchers supplemented and refined the interview notes based on on-site records and recollection. They annotated details of non-verbal cues and special circumstances arising during the interview (such as key concerns raised spontaneously by the interviewee or points of emotional fluctuation), ensuring the comprehensiveness, accuracy, and timeliness of the material. Within 24 hours of the interview, two researchers repeatedly listened to and cross-checked the recordings. These were transcribed using the Quark app, then collated with handwritten notes to produce a Chinese verbatim transcript. This transcript was subsequently returned to the interviewee for verification.
Data Induction and Analysis
Upon completion of the text organisation, two researchers first standardised and optimised the transcribed texts, subsequently employing Colaizzi’s seven-step analysis method to examine the data:19
(1) Carefully review the transcribed text; (2) Extract meaningful patient statements relevant to the designed research questions; (3) Code the extracted content; (4) Interpret coded perspectives to identify common concepts forming themes and name these themes; (5) Elaborate themes pertinent to the research phenomenon; (6) Select representative responses to articulate the fundamental structure constituting the research phenomenon; (7) Return analytical findings to each participant for content validation. Once everything had been verified, the analysis and extraction process began. The analysis and coding were carried out using Nvivo 11.0 software. Within 24 hours of the interviews being completed, two researchers conducted independent, blind coding; they transcribed and cross-checked the audio recordings and field notes, and identified themes. Data collection and analysis were conducted simultaneously, with data collection continuing until saturation was reached. In this study, the first signs of saturation were observed following the 13th interview. After completing the 14th and 15th interviews, it was confirmed that no new themes had emerged, and data collection was therefore terminated. Ultimately, this study included a total of 15 interviewees. Any discrepancies arising during the coding process were resolved through collective discussion within the research team.
Quality Control
This study establishes a quality control system based on four dimensions—transparency, credibility, reliability and generalisability—to ensure the rigour of the research. With regard to research transparency, the study strictly adheres to the COREQ (Consolidated Criteria for Reporting Qualitative Research) guidelines20 and A worked example of qualitative descriptive design: A step-by-step guide for novice and early career researchers,16 providing a clear account of the entire process—including research design, data collection, analytical procedures and the presentation of results—to ensure the traceability of the research process. To maintain a complete audit trail, this study retained interview recordings, verbatim transcripts and records of non-verbal behaviour; preserved multiple versions of coding manuals, analytical memos and records of discussions between the two coders; and compiled a diary of reflections on the interviews. These records ensure that every step, from the raw data to the research conclusions, can be independently reviewed and traced.
Research credibility refers to the extent to which research findings accurately reflect the participants’ experiences. In this study, the interviewer engaged in thorough communication with the interviewee prior to the formal interview to establish a solid foundation for interaction; during the interview, the interviewer confirmed mutual understanding in real time through methods such as paraphrasing, probing questions and summarising; Following the interviews, preliminary analysis results were shared with the participants to solicit their feedback and suggestions, and contact details were retained for subsequent verification; in addition to verbatim transcription of the interview content, detailed records were kept of the interview setting, as well as non-verbal behaviours such as facial expressions and body language, and these were combined with interview reflection diaries to enhance the authenticity of the data and the researcher’s sensitivity in interpretation.
Research reliability refers to the stability, documentability and reproducibility of the research process. This study employed a process of independent coding by two researchers followed by cross-validation; the two researchers carried out the coding independently and reached consensus on any discrepancies through discussion, thereby ensuring the stability and reproducibility of the data analysis.
Research generalisability refers to the extent to which research findings can be applied to other contexts. This study not only provides a detailed description of the respondents’ characteristics, the research context and the data collection process to enhance the generalisability of the results to similar scenarios, but also includes first-line tuberculosis patients from diverse backgrounds to enrich the data dimensions, thereby further improving the comparability of the research conclusions.
Reflectiveness was taken into account throughout the research process. The researchers have a clinical background in tuberculosis care, and their professional experience may have influenced the interpretation of the data, particularly with regard to assumptions concerning patients’ readiness for discharge. Consequently, prior to the commencement of the study, the researchers underwent systematic training in qualitative research and were assessed; the research team held regular discussions to discuss interpretations, with team members possessing varying levels of clinical and research experience. To assist readers in assessing the relevance of the study findings, a detailed description of the participants’ characteristics and the recruitment process is provided.
Ethical Issues
This study obtained written informed consent from patients prior to interviews and was reviewed by the Ethics Committee of Chengdu Public Health Clinical Medical Centre (YJ-K2025-36-01). The research adheres to the principles of voluntariness, informed consent, confidentiality, and non-maleficence. Participants voluntarily engage in the study and retain the right to withdraw at any stage without incurring any disadvantage.
Result
General Information on Respondents
The study involved interviews with 15 patients, comprising 10 males and 5 females, aged between 19 and 67 years (mean age: 32.13 ± 14.20 years). Demographic details are presented in Table 1. To protect participants’ privacy, they are designated by codes N1 to N15. The study identified three main themes and 12 corresponding sub-themes, as outlined in Table 2.
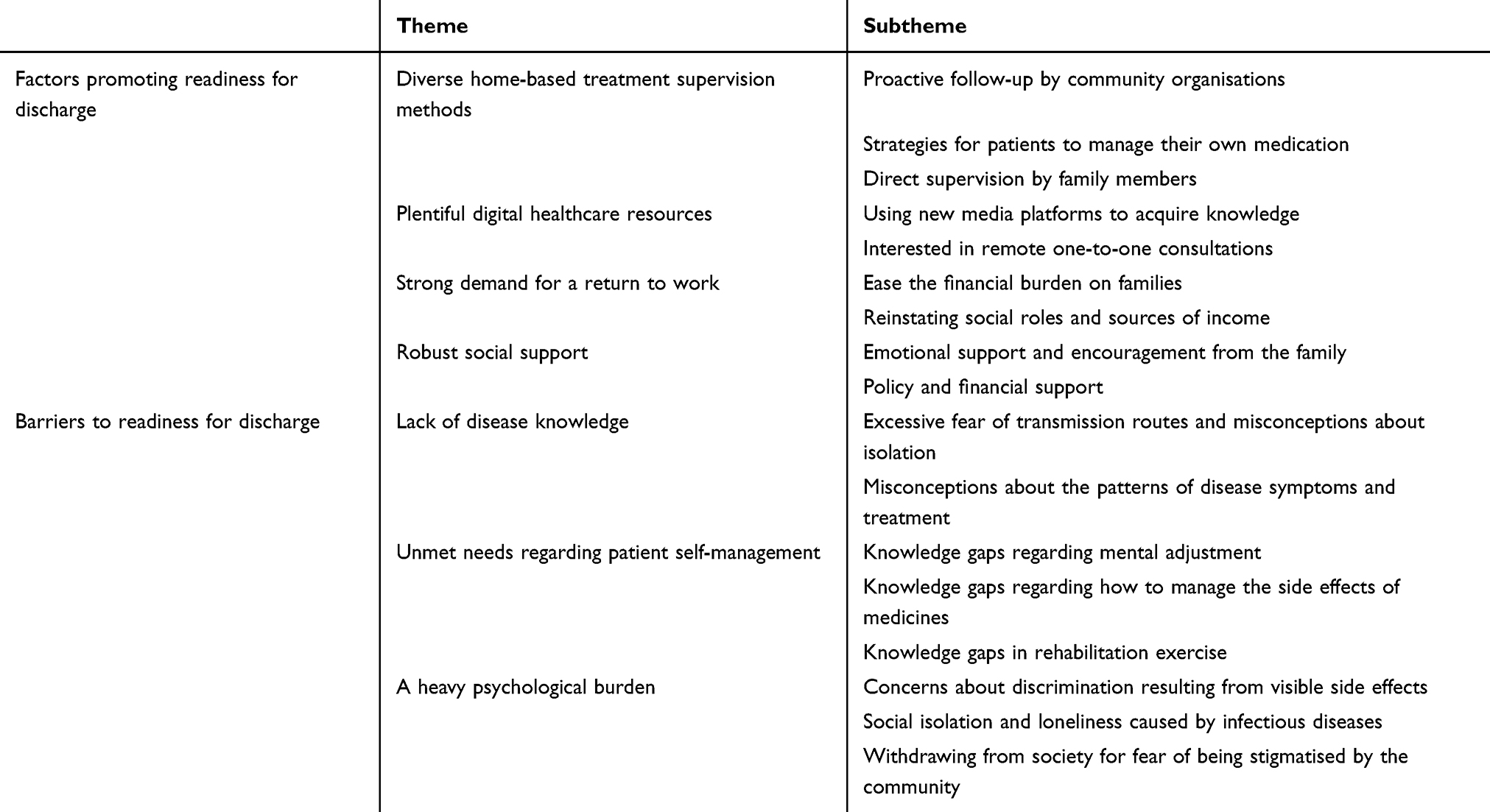 |
Table 2 Themes and Subthemes |
Interview Results
Factors Promoting Readiness for Discharge Among Patients with Newly Diagnosed TB
Home Treatment Supervision and Management Methods are Diverse
Diverse approaches to the supervision and management of home-based treatment can effectively improve the readiness of newly diagnosed tuberculosis patients for discharge.
Most patients are able to take proactive steps to help them remember to take their medication, such as using reminders, setting alarms, and pre-dosing their medication and placing it in a prominent location.
N15:I have already noted the follow-up appointment and medication times in my diary, and set the alarm clock.
Family members are explicitly assigned a supervisory role, ensuring process control through daily reminders and checks for missed doses.
N14:My sister says she will definitely supervise me taking my medication and attending follow-up appointments once we get home.
N11:My parents monitor me daily to ensure I take my medication without omission.
Community healthcare facilities have established a systematic, outreach-based management approach through proactive telephone follow-ups, medication adherence checks and reminders for follow-up appointments, whilst also encouraging patients to register with their local community health centre upon discharge.
N4:In our neighbourhood, they’d be ringing up any time to check if I’d taken my meds on time, or when I was due for my next check-up.
Plentiful Digital Healthcare Resources
Digital technology, as a tool to support the post-discharge management of patients with primary tuberculosis, plays a significant role in improving their readiness for discharge. Some patients are able to access information on tuberculosis through WeChat official accounts, hospital newsletters, and Douyin.
These new media platforms, with their low barriers to access, bite-sized content and the ability to be consulted repeatedly, meet patients’ basic needs for disease-related information following discharge.
N3:I like to look up tuberculosis-related content on official accounts and WeChat channels.
N9:I follow some hospital official accounts, which push tuberculosis-related knowledge. Additionally, there are resources on Douyin and science popularisation platforms.
Compared with generic new media content updates, some patients prefer to have the opportunity to communicate directly with healthcare professionals, such as asking for the telephone number of the doctor’s office or the attending physician’s WeChat ID or telephone number. This indicates that patients seek medical information through multiple channels.
N13:I would like the telephone number for the doctor’s surgery so that I can call them after I’m discharged to ask for advice about tuberculosis.
N14:There is an online consultation service via WeChat, but I’d still prefer to have my GP’s phone number or WeChat contact details… it’s just a bit more convenient.
Strong Demand for a Return to Work
Patients newly diagnosed with tuberculosis face dual pressures from both their families and their illness, and bear a heavy financial burden. They need to return to work to alleviate this financial strain; this need to return to work is one of the key drivers motivating them to actively cooperate with their treatment. This study found that patients face dual financial pressures stemming from their illness and their dependence on their families, which leads them to view “returning to work as soon as possible” as the key to resolving their predicament. Patients hope that by returning to work, they can alleviate the financial burden on their families and rebuild their social identity; returning to work is seen as a means of ceasing to draw on family resources and instead contributing to the household income. At the same time, returning to work is also an important way for patients to rebuild their social identity and restore their sense of self-worth.
N4:I am currently unemployed… I hope to get better as soon as possible so I can go back to work; I don’t want to be a burden on my family (laughs).
N9:I am all set to be discharged from hospital, and I am planning to look for a new job soon… so I can ease the burden of future medical bills a little.
N3:I’d like to be discharged as soon as possible and get back to work. As my hospital stay has been quite long and I have lost a fair bit of time, I’d really like to get back into the swing of things at work as quickly as possible.
Robust Social Support
This study found that strong social support is a key factor in promoting readiness for discharge among patients with newly diagnosed tuberculosis. Its role is manifested in helping patients overcome both psychological and material barriers: emotional support helps overcome the psychological barrier of whether patients are willing to face their illness, whilst policy and financial support address the material constraints regarding whether patients can continue treatment. Encouraging words and supportive actions from family members essentially convey unconditional acceptance to the patient. This support alleviates the patient’s fears of being “rejected” or “a burden”, enabling them to approach their preparations for discharge with a greater sense of calm.
N8:My family have all advised me not to bear too heavy a burden over my illness. We are always here for you, and we will help you through it.
Government support schemes and health insurance reimbursement free patients from the dilemma of being unable to afford treatment by directly reducing out-of-pocket costs, allowing them to focus on post-discharge care management.
N7:Having learnt a bit about how medical insurance works, I have realised that medical tests, medication and hospital stays are very expensive. What would originally have cost ten or twenty thousand yuan now only costs a few thousand after the insurance claim has been processed.
Barriers to Discharge Readiness Among Newly Diagnosed TB Patients
Lack of Disease Knowledge
The lack of knowledge about tuberculosis among patients receiving initial treatment manifests, during the discharge preparation phase, as excessive fear of transmission routes, misconceptions regarding isolation, and misunderstandings about the symptoms and treatment patterns of the disease; all of which may pose a risk to effective post-discharge treatment and disease prevention and control.
The interviews revealed that some patients have an inaccurate understanding of how tuberculosis is transmitted and have adopted isolation measures that go beyond what is necessary, such as asking family members to move elsewhere or insisting on eating alone. Although such behaviour stems from a well-intentioned desire to prevent transmission, it essentially reflects an overreaction to the routes of transmission and a misjudgement of the risks associated with everyday contact.
N15:After being discharged and returning home, I asked my parents to go live in the pastoral area while I stayed alone at home to prevent them from getting infected.
N7:Upon returning home, during mealtimes, one must dine alone (at a table by oneself).
Some patients, due to a lack of basic understanding of the symptoms of the disease and the treatment regimen, tend to neglect the treatment schedule, request extra medication, and underestimate the necessity of treatment during asymptomatic phases; they also believe that, as they are not experiencing any symptoms, there is no need to make preparations for discharge.
N2:If I am discharged home, I’d prefer to take a larger supply of medication so I can wait longer before needing a new prescription.
N6:From the start until now, I have never had a cough, nor any other symptoms. What preparations are needed? None at all.
Unmet Needs Regarding Patient Self-Management
This study found that the health education needs of treatment-naïve tuberculosis patients extend beyond basic knowledge of the disease, and that their self-management needs remain unmet, particularly in terms of psychological adjustment, physical tolerance and functional recovery following discharge. Patients not only require knowledge of disease management, but also wish to learn methods for relieving stress and regulating their emotions, reflecting a concern for their psychological adjustment following discharge.
N3:I am fairly familiar with the dietary advice, protective measures, and follow-up appointments. What I am hoping for is some psychological support – any good methods for managing stress after discharge?
There is a clear need for information on adverse drug reactions and strategies for managing them;
N5:I’d like to know, above all, about the side effects of taking tuberculosis medication.
A desire to learn about rehabilitation exercises and ways to alleviate post-medication discomfort, as well as a proactive approach to restoring function and improving quality of life.
N13:I’d like to understand more about rehabilitation-related matters, such as therapeutic exercises. Also, after taking antiviral medication, I experience some physical discomfort – are there any ways to alleviate this.
A Heavy Psychological Burden
Patients newly diagnosed with tuberculosis bear a heavy psychological burden; this burden stems from the accumulation of multiple pressures and has a direct impact on their readiness for discharge.
Some patients have reported that the physical changes caused by the side effects of their medication mean they must constantly be on guard against the stares of others.
N4:After taking the TB medication, I have had side effects like extremely dry skin and flaking… I am afraid others will look at me strangely, and I do not know what to do.
Most patients feel that the infectious nature of the disease makes it a “taboo subject”, leaving them unable to confide in friends or even family members, and forcing them to cope with the psychological strain on their own; fearing gossip from neighbours, they choose to stay indoors, shut themselves away in their rooms and withdraw from society.
N14:I must have been under immense psychological pressure to contract this illness, given its infectious nature. It’s difficult to discuss with friends, and telling family is heartbreaking (sighs). What preparations can one make alone.
N15:I am terribly afraid of the neighbours and their gossip if I go home after being discharged… I will just stay indoors in my own room, no need to make any preparations.
Discussion
This study examines the facilitating and hindering factors affecting discharge preparation among treatment-naïve tuberculosis patients. The study identified seven themes: the facilitating factors included diverse methods of supervising home-based treatment, abundant digital healthcare resources, a strong desire to return to work, and good social support; the hindering factors included a lack of knowledge about the disease, unmet patient self-management needs, and a heavy psychological burden. To ensure the interpretative validity of the research findings, this study adhered to the COREQ guidelines for quality control to ensure research transparency; enhanced credibility through real-time verification during interviews, post-interview feedback, and the recording of non-verbal behaviour; ensured reliability through independent coding by two researchers and consensus discussions; and improved generalisability through detailed descriptions of participants’ backgrounds and the inclusion of a diverse sample. These quality assurance measures have endowed the seven themes identified in this study with strong internal validity and external generalisability.
Accurately Assess Patients’ Discharge Readiness Challenges and Utilise Digital Resources to Deliver Targeted Discharge Preparation Training
The findings of the interviews indicate that a lack of knowledge about the disease among treatment-naïve tuberculosis patients reduces their readiness for discharge. Respondents still lack a clear understanding of the modes of transmission and the importance of regular treatment for tuberculosis. This is consistent with the findings of Wang et al,21 suggesting that a lack of disease-related knowledge is not an isolated phenomenon, but a widespread issue among treatment-naïve patients From the perspective of health literacy theory, this deficiency is not merely a matter of “not knowing”, but rather a combined lack across three dimensions: functional health literacy (eg understanding disease transmission), interactive health literacy (eg actively seeking information on disease prevention and control), and critical health literacy (eg assessing the reliability of information) Consequently, traditional “one-size-fits-all” health education is unlikely to be effective. Previous systematic reviews,22 have indicated that the systematic application of digital resources in tuberculosis prevention and control not only broadens the channels for health education but also enables real-time monitoring and interactive services, thereby providing patients with more efficient care. The findings from the interviews conducted in this study also support this view; the majority of patients stated that digital channels such as new media platforms, remote consultations, WeChat official accounts, telephone and Douyin enable them to satisfy their basic need for disease-related knowledge and to access the health information they require in a timely manner. The findings of interviews conducted by Li et al23 with 15 elderly patients with hip fractures also indicate a desire for diverse digital health education methods. In summary, we believe that in preparing first-line tuberculosis patients for discharge, full use should be made of digital resources to establish a support system characterised by “personalised educational content, intelligent educational methods and diverse educational formats”. Specifically, tools such as knowledge graphs, animated educational videos and intelligent Q&A bots can be utilised to deliver precise health guidance; in terms of format, group education and individual education should be conducted in a complementary manner; and in terms of role expansion, nurses should proactively assume the roles of digital education organisers and content providers, establishing online learning platforms and regularly addressing carers’ practical concerns online, thereby effectively facilitating the transition from “hospital treatment” to “home care”.
Prioritising the Mental Health of People with Tuberculosis and Improving Their Experience of Discharge Preparation
Tuberculosis is characterised by chronic infectiousness, recurrent episodes and the need for long-term treatment.24,25 Once diagnosed, patients not only have to cope with the physical burden of the disease itself, but also commonly experience anxiety about their prognosis and feelings of guilt about being a “burden on their family”, resulting in a heavy psychological burden.26–28 The findings of this study further corroborate this point; for example, N15 has confined themselves to their home for a long time, refusing to go out for fear of being discriminated against by others. Previous studies have shown29–31 that the prevalence of psychological problems such as anxiety and depression among tuberculosis patients ranges from 7% to 56%. Therefore, paying attention to the mental health of patients with newly diagnosed tuberculosis is not only a matter of humanistic care, but also a crucial step in improving their experience of discharge preparation, as well as enhancing their adherence to treatment and quality of life following discharge. It is worth noting that this study found that strong social support can effectively alleviate patients’ psychological burden. Respondents clearly stated that the ongoing support and encouragement from family members, as well as the government’s policy on reimbursing the costs of tuberculosis treatment, had significantly reduced their psychological stress and boosted their confidence in treatment. This finding is highly consistent with social support theory. This theory posits that social support, by providing emotional support, financial assistance and information, can mitigate the negative psychological impact of stressful events on individuals For patients receiving initial treatment for tuberculosis, the process of returning home from hospital is in itself a stressful transition; at this stage, the strength of the social support system is directly linked to the patient’s psychological coping ability and their experience of discharge preparation. Consequently, healthcare professionals should fully identify and mobilise patients’ existing social support resources, whilst helping to address any gaps in their support systems. They should establish patient-centred, discharge-preparedness-oriented home rehabilitation plans, incorporate family members into the health education system, and guide them in mastering basic psychological support skills. At the same time, they should proactively explain institutional support measures-such as medical insurance reimbursement policies and community follow-up managemen-to patients, thereby reducing the sense of helplessness arising from information asymmetry.
To Establish a Service System for Home-Based Treatment Management and Improve the Readiness of Tuberculosis Patients for Discharge
The treatment of tuberculosis is a long and challenging process that requires patients to engage in ongoing self-management, including adhering to medication regimens, maintaining a balanced diet, engaging in moderate exercise, and keeping a positive mental outlook. In this study, respondents indicated that they wished to know what rehabilitation exercises they could perform at home and what methods were available to help them self-regulate and cope with the stress of the illness. This suggests that, whilst patients recognise the need for self-management, they face significant difficulties in putting this into practice. From the perspective of “self-efficacy” within self-management theory, patients’ repeated questions about “exactly what to do” reflect precisely their lack of confidence in translating cognition into action. It is therefore particularly crucial to help them bridge the gap between cognition and behaviour and to cultivate practical self-management skills.
This study found that the involvement of family members and management support from the community provide a viable pathway for enhancing patients’ self-management capabilities. Feedback from respondents indicated that, following discharge, family members and the community participated in the patients’ disease management through personalised approaches such as text message follow-ups, smart reminders and electronic pill boxes. Consequently, healthcare professionals should establish a home-based care service system built upon the family-community foundation, guiding family members to master core skills such as medication supervision, symptom recognition and emotional support, thereby enabling them to serve as the direct pillar of the patient’s daily care. Relying on primary healthcare institutions, digital management tools (such as text message reminders, smart pillboxes and remote follow-ups) should be integrated to provide patients with continuous medication reminders and health monitoring. By combining the functions of close-proximity care within the home with remote support from the community, patients are encouraged to gradually consolidate their disease knowledge into stable self-management behaviours within real-life contexts, ultimately achieving a transition from “treatment adherence” to “health autonomy”.
We Provide Personalised Support Services to Help Patients Return to Work
This study found that, due to high treatment costs and significant financial pressure on their families, some respondents regarded “returning to work as soon as possible” as one of the key motivations for their treatment. According to reports,32–34 over 50% of tuberculosis patients face financial difficulties due to the costs of treatment, transport and accommodation. When these expenses become a significant burden, patient’s motivation to undergo treatment shifts. They will actively cooperate with their treatment, not only to cure the disease itself, but also to fundamentally improve their family’s financial situation by recovering as soon as possible and returning to work. The results of a South African study involving interviews with tuberculosis patients who had completed their treatment35 revealed that patients were eager to return to work. Returning to work not only helps improve patients’ financial circumstances but also holds significant psychosocial importance. Being able to resume normal work is the most direct way for patients to demonstrate to society that they have recovered and no longer pose a risk of transmission. Furthermore, the social interaction and sense of support from colleagues provided by the workplace play a positive role in the patients’ psychological recovery. It is therefore recommended that healthcare professionals proactively offer personalised support services for returning to work in their clinical practice. By taking into account the patient’s family financial situation and the physical demands of the job, they should draw up individualised return-to-work schedules to help patients alleviate financial pressure through an early return to work; assist patients in communicating with their employers, providing necessary medical certificates to minimise employment discrimination resulting from their illness; offer psychological adjustment guidance to help patients cope with any stigma or avoidance by colleagues that may arise upon returning to work; and boost their confidence in recovery and returning to work by encouraging them to actively cooperate with treatment.
It should be noted, however, that the patients in this study were all from a single hospital in western China; the need for support in returning to work may be influenced by regional economic conditions, employment protection policies and the extent of disease stigma. When applying the findings to different contexts, local circumstances should be taken into account.
Strengths and Limitations
This study employed semi-structured interviews to precisely capture the subjective experiences and underlying needs of newly diagnosed TB patients during their family transition period in hospital. It identified factors facilitating and hindering - home transition period, uncovering factors that facilitate and impede discharge readiness. This provides empirical evidence for establishing an assessment system for discharge readiness among newly diagnosed TB patients and formulating tiered, targeted discharge intervention strategies. It also lays a theoretical foundation for optimising TB continuity of care service models, enhancing patients’ home self-management capabilities, and improving long-term recovery outcomes.
The study has several limitations. Firstly, this research constitutes a single-centre investigation conducted at one hospital in southwestern China, resulting in a relatively limited sample size. This introduces geographical constraints in sample selection, thereby limiting the generalisability and applicability of the findings. Secondly, the research was conducted solely from the patient’s perspective; subsequent studies may explore this topic from multiple levels and dimensions, including the perspective of carers. Thirdly, future research should increase the sample size and ensure a balanced gender ratio in order to obtain a more representative sample; it could also include additional analyses of how participants’ characteristics influence the factors facilitating and hindering discharge preparation.
Conclusions
This study adopts a qualitative approach to examine discharge preparedness among first-line tuberculosis patients during the hospital-to-home transition period. The findings reveal that patients’ discharge preparedness is influenced by multiple factors, including the mode of home treatment supervision, levels of social support, the need to return to work, access to digital healthcare resources, a lack of disease knowledge, unmet self-management needs, and psychological burdens. Discharge preparation occurs against a backdrop where clinical recovery, home care and social support are intertwined; there is a dynamic interplay between various practical challenges and patients’ expectations of recovery, sense of personal responsibility and external support. Although digital healthcare has expanded access to health services, it remains difficult to effectively address individualised needs such as knowledge gaps and psychological anxiety. Future clinical interventions should focus on precise discharge assessments, personalised health education and integrated home monitoring, thereby addressing gaps in health literacy, alleviating psychological stress and optimising care during the transition period.
Overall, this study contributes to a deeper understanding of the real-life challenges patients face in preparing for discharge during the transition period. It provides a basis for clinical nursing practice, thereby improving patients’ experience of discharge preparation, reducing the risk of readmission, and supporting patients’ smooth reintegration into society.
Abbreviation
TB, tuberculosis.
Data Sharing Statement
The data and materials that support the findings of this study are available from Miss Xiaoyi Yang upon reasonable request.
Ethical Approval Statement
This study was approved by the Medical Ethics Committee of Public Health Clinical Centre of Chengdu (NO YJ-K2025-36-01). This study was conducted in accordance with the Declarationof Helsinki. Written informed consent was obtained from all participants, including for the publication of anonymizedresponses and direct quotes.
Acknowledgments
The authors thank all who participated in this study and provided valuable input.
Funding
This research was funded by the Health Commission of Sichuan Province Medical Science and Technology Program (24QNMP049) and the Chengdu Municipal Health Commission Subjects (2025631and 2025296).
Disclosure
The authors affirm that no conflicts of interest exist regarding this research.
References
1. Furin J, Cox H, Pai M. Tuberculosis. Lancet Lond Engl. 2019;393:1642–14. doi:10.1016/S0140-6736(19)30308-3
2. World Health Organization. Global tuberculosis report 2025. Geneva, Switzerland: World Health Organization; 2025.
3. Fekadu G, Chow DY-W, You JHS. The pharmacotherapeutic management of pulmonary tuberculosis: an update of the state-of-the-art. Expert Opin Pharmacother. 2022;23:139–148. doi:10.1080/14656566.2021.1967930
4. Ruan Q-L, Yang Q-L, Sun F, et al. Recurrent pulmonary tuberculosis after treatment success: a population-based retrospective study in China. Clin Microbiol Infect. 2022;28:684–689. doi:10.1016/j.cmi.2021.09.022
5. Weiangkham D, Umnuaypornlert A, Saokaew S, et al. Effect of alcohol consumption on relapse outcomes among tuberculosis patients: a systematic review and meta-analysis. Front Public Health. 2022;10:962809. doi:10.3389/fpubh.2022.962809
6. Jhaveri TA, Jhaveri D, Galivanche A, et al. Barriers to engagement in the care cascade for tuberculosis disease in India: a systematic review of quantitative studies. PLoS Med. 2024;21:e1004409. doi:10.1371/journal.pmed.1004409
7. Vega V, Rodríguez S, Van der Stuyft P, et al. Recurrent tuberculosis: a systematic review and meta-analysis of the incidence rates and the proportions of relapse and reinfection. Thorax. 2021;76:494–502. doi:10.1136/thoraxjnl-2020-215449
8. Rochefort CM, Rathwell BA, Clarke SP. Rationing of nursing care interventions and its association with nurse-reported outcomes in the neonatal intensive care unit: a cross-sectional survey. BMC Nurs. 2016;15:46. doi:10.1186/s12912-016-0169-z
9. Tong H-J, Qiu F, Fan L. Effect of hospital discharge plan for children with type 1 diabetes on discharge readiness, discharge education quality, and blood glucose control. World J Clin Cases. 2021;9:774–783. doi:10.12998/wjcc.v9.i4.774
10. Weiss ME, Yakusheva O, Bobay KL, et al. Effect of implementing discharge readiness assessment in adult medical-surgical units on 30-day return to hospital: the READI randomized clinical trial. JAMA Network Open. 2019;2:e187387. doi:10.1001/jamanetworkopen.2018.7387
11. Yang H. Current Status and Influencing Factors of Discharge Readiness in Pulmonary Tuberculosis Patients. Jishou University; 2024. doi:10.27750/d.cnki.gjsdx.2024.000307
12. Wang J, Rao Q, Zhou L, et al. The correlation between the need for continuing care services, influencing factors, and social support and discharge readiness among discharged patients with pulmonary tuberculosis in China: a cross-sectional study. Appl Nurs Res. 2024;77:151789. doi:10.1016/j.apnr.2024.151789
13. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33:77–84. doi:10.1002/nur.20362
14. World Health Organization. WHO Consolidated Guidelines on Tibercuosis: Modue 4: Treatment - Drug-Resistant Tubercuosis Treatment, 2022 Update. Geneva: World Health Organization; 2022.
15. Kerr C, Nixon A, Wild D. Assessing and demonstrating data saturation in qualitative inquiry supporting patient-reported outcomes research. Expert Rev Pharmacoecon Outcomes Res. 2010;10:269–281. doi:10.1586/erp.10.30
16. Villamin P, Lopez V, Thapa DK, et al. A worked example of qualitative descriptive design: a step-by-step guide for novice and early career researchers. J Adv Nurs. 2025;81:5181–5195. doi:10.1111/jan.16481
17. Shringarpure K, Gurumurthy M, Sagili KD, et al. Patient adherence to tuberculosis treatment in the indian subcontinent: systematic review and meta-synthesis of qualitative research. BMJ Open. 2023;13:e063926. doi:10.1136/bmjopen-2022-063926
18. Fenta MD, Ogundijo OA, Warsame AAA, et al. Facilitators and barriers to tuberculosis active case findings in low- and middle-income countries: a systematic review of qualitative research. BMC Infect Dis. 2023;23:515. doi:10.1186/s12879-023-08502-7
19. Park K-O, Park S-H, Yu M. Physicians’ experience of communication with nurses related to patient safety: a phenomenological study using the colaizzi method. Asian Nurs Res. 2018;12:166–174. doi:10.1016/j.anr.2018.06.002
20. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
21. Wang J, Zhang Y, Rao Q, et al. Factors affecting the readiness for hospital discharge of initially treated pulmonary tuberculosis patients in China: a phenomenological study. BMC Public Health. 2024;24:2312. doi:10.1186/s12889-024-19793-z
22. Lee Y, Raviglione MC, Flahault A. Use of digital technology to enhance tuberculosis control: scoping review. J Med Internet Res. 2020;22:e15727. doi:10.2196/15727
23. Li S, Song M, Zhang WL, et al. Discharge preparation service needs of elderly patients with Hip fracture: a qualitative study. Mil Nurs. 2025;42:48–51. doi:10.3969/j.issn.2097-1826.2025.11.012
24. Martinez L, Shen Y, Mupere E, et al. Transmission of mycobacterium tuberculosis in households and the community: a systematic review and meta-analysis. Am J Epidemiol. 2017;185:1327–1339. doi:10.1093/aje/kwx025
25. World Health Organization. Global Tuberculosis Report 2024. Geneva: World Health Organization; 2024.
26. Paulo BX, Peixoto B. Emotional distress patients with several types of tuberculosis. A pilot study with patients from the sanatorium hospital of huambo. Int J Mycobacteriol. 2016;5 Suppl 1:S58. doi:10.1016/j.ijmyco.2016.11.002
27. Patel N, Patel H, Varu J, et al. The invisible toll: unveiling the prevalence and predictors of depression and anxiety among pulmonary tuberculosis (TB) patients and their households in Gujarat, India. Cureus. 2024;16:e65015. doi:10.7759/cureus.65015
28. Dixit K, Rai B, Aryal TP, et al. Stigma, depression, and quality of life among people with pulmonary tuberculosis diagnosed through active and passive case finding in Nepal: a prospective cohort study. BMC Glob Public Health. 2024;2:20. doi:10.1186/s44263-024-00049-2
29. Kumpuangdee S, Roomruangwong C, Sophonphan J, et al. Prevalence of depression and anxiety in pulmonary tuberculosis patients and its association with unsuccessful treatment outcome: a prospective cohort study. Indian J Tuberc. 2023;70:297–302. doi:10.1016/j.ijtb.2022.05.007
30. Mohammedhussein M, Alenko A, Tessema W, et al. Prevalence and associated factors of depression and anxiety among patients with pulmonary tuberculosis attending treatment at public health facilities in Southwest Ethiopia. Neuropsychiatr Dis Treat. 2020;16:1095–1104. doi:10.2147/NDT.S249431
31. Koyanagi A, Vancampfort D, Carvalho AF, et al. Depression comorbid with tuberculosis and its impact on health status: cross-sectional analysis of community-based data from 48 low- and middle-income countries. BMC Med. 2017;15:209. doi:10.1186/s12916-017-0975-5
32. Akalu TY, Clements ACA, Wolde HF, et al. Economic burden of multidrug-resistant tuberculosis on patients and households: a global systematic review and meta-analysis. Sci Rep. 2023;13:22361. doi:10.1038/s41598-023-47094-9
33. Kuye J, Sindani IS, Shube MA, et al. Households of tuberculosis (TB) patients face high TB-related costs in Somalia. BMC Glob Public Health. 2025;3:53. doi:10.1186/s44263-025-00175-5
34. Assebe LF, Negussie EK, Jbaily A, et al. Financial burden of HIV and TB among patients in Ethiopia: a cross-sectional survey. BMJ Open. 2020;10:e036892. doi:10.1136/bmjopen-2020-036892
35. Soeker MS, Jainodien A, Smith M. The challenges that individuals with MDRTB and TB experience when returning to work after completing TB treatment in the western cape, South Africa. Work Read Mass. 2025;81:3247–3257. doi:10.1177/10519815251330123
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Illness Experience and Unmet Needs of Pulmonary Tuberculosis Patients: A Meta-Synthesis Guided by the Symptom Experience Model
Yang Y, Yu Q, Zhao X, Yao R, Shen J, Jiang S, Yang X, Wan B
Patient Preference and Adherence 2026, 20:565692
Published Date: 12 February 2026