Back to Journals » Patient Preference and Adherence » Volume 20
Illness Experience and Unmet Needs of Pulmonary Tuberculosis Patients: A Meta-Synthesis Guided by the Symptom Experience Model
Authors Yang Y, Yu Q, Zhao X, Yao R, Shen J, Jiang S, Yang X, Wan B
Received 6 September 2025
Accepted for publication 28 January 2026
Published 12 February 2026 Volume 2026:20 565692
DOI https://doi.org/10.2147/PPA.S565692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yulan Yang,1,2,* Qiaolin Yu,3,* Xia Zhao,1 Rong Yao,3 Jing Shen,2 Shasha Jiang,2 Xiaoyi Yang,3 Bin Wan1
1The Department of Nursing, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, People’s Republic of China; 2College of Nursing, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3The Department of Tuberculosis, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Wan, The Department of Nursing, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, People’s Republic of China, Tel +86 13881956592, Email [email protected]
Purpose: Patients’ illness experiences and needs are central to pulmonary tuberculosis management and have important implications for treatment engagement and health outcomes. This study addresses this gap by systematically synthesizing qualitative evidence to provide a comprehensive understanding of pulmonary tuberculosis patients’ illness experiences and unmet needs, guided by the Symptom Experience Model.
Methods: PubMed, Web of Science, Embase, PsycINFO, CINAHL, ProQuest, the Cochrane Library, CNKI, VIP, Wanfang, and SinoMed were searched from inception to December 2024 for qualitative or mixed-methods studies on the illness experience of pulmonary tuberculosis patients. Studies were screened and appraised using the Joanna Briggs Institute Critical Appraisal Checklist for Qualitative Research. Meta-integration techniques were used for synthesis. The Symptom Experience Model provided the interpretive framework for analysis. This review followed PRISMA 2020 guidelines for reporting systematic reviews. The PROSPERO registration was dated July 24, 2024 (Registration Number: CRD42024572729).
Results: Twenty-one studies were included, comprising a total of 469 participants. A total of 36 themes were identified, grouped into nine descriptive categories and synthesized into two overarching findings. First, patients experience complex illness-related challenges, including physical symptoms, psychological distress, disrupted social roles, uncertainty about the future, and, in some cases, post-traumatic growth. Second, multiple unmet needs were identified, including inadequate health education, insufficient emotional support, stigma, barriers to healthcare access, and lack of socioeconomic support. While the Symptom Experience Model helped explain symptom perception and coping behaviors, it was less effective in addressing structural determinants such as poverty and systemic stigma.
Conclusion: Pulmonary tuberculosis causes profound suffering shaped by both individual responses and wider social contexts. Interventions should address emotional and cognitive processes, strengthen social support, and consider patients’ lived realities. The Symptom Experience Model could be expanded to better reflect socioecological influences.
Keywords: tuberculosis, narrative medicine, health services needs and demand, qualitative research
Introduction
Pulmonary tuberculosis (TB) remains one of the leading infectious diseases globally and continues to pose a significant public health challenge, particularly in high-burden countries such as China. In 2023, an estimated 748,000 new TB cases were reported in China, with an incidence rate of 52 per 100,000 population, ranking third globally.1 While advancements in diagnostics and chemotherapy have improved clinical outcomes, TB’s prolonged treatment (≥6 months) imposes a multidimensional burden: patients endure fluctuating physical symptoms (eg, fatigue, hemoptysis), severe drug side effects (eg, hepatotoxicity), and psychosocial distress (eg, stigma, isolation).2,3 These challenges are compounded by socioeconomic disparities, particularly in rural and low-income populations where treatment adherence often falters.4
Existing research predominantly prioritizes biomedical outcomes—drug resistance, sputum conversion rates, mortality5,6—while neglecting the subjective illness experience. Although qualitative studies have explored fragmented aspects (eg, stigma perception,7 financial stress),8 a theory-driven synthesis of how patients dynamically perceive, appraise, and adapt to symptoms remains absent. This gap hinders interventions that address not isolated symptoms, but the feedback loops between physiological distress, cognitive appraisals (eg, “Is my cough contagious?”), and socially constrained behaviors (eg, treatment abandonment).
The Symptom Experience Model (SEM), originally developed in oncology, provides a useful framework for understanding how individuals perceive, interpret, and respond to symptoms.9,10 The model conceptualizes symptom experience as a dynamic process encompassing physiological perception, cognitive appraisal, emotional response, and behavioral coping. Unlike models that focus primarily on illness representations, SEM emphasizes the interrelationships between symptom appraisal and coping behaviors, making it particularly relevant for conditions requiring long-term treatment and sustained self-management, such as pulmonary tuberculosis.11 Although SEM has been applied to various chronic conditions (eg, symptom appraisal shaping adherence in HIV;12 fatigue management in diabetes),13 its application to infectious diseases such as TB remains strikingly limited. In particular, how patients with pulmonary tuberculosis experience and interpret symptoms, respond emotionally, and articulate related care needs has not been comprehensively synthesized.
Therefore, this review aimed to systematically synthesize qualitative evidence to address the following research questions: (1) How do patients with pulmonary tuberculosis experience and interpret their illness? (2) What unmet needs do they report during the course of diagnosis and treatment? These experiences and needs were interpreted through the lens of the Symptom Experience Model to enhance understanding of patient-centered tuberculosis care.
Methods
This study adopts a qualitative evidence synthesis approach using meta-integration, guided by the SEM. The SEM serves as a conceptual framework to inform the research questions, data extraction, and thematic synthesis. This model emphasizes the multidimensional nature of symptom experience, including perception, evaluation, emotional response, and coping strategies. Reporting adhered to the PRISMA 2020 checklist14 (Supplementary File 1). This study protocol has been registered in PROSPERO (registration number: CRD42024572729).
Search Methods
Comprehensive computer search was conducted for studies on the illness experience of pulmonary tuberculosis patients in databases such as CINAHL, Embase, PubMed, ProQuest, The Cochrane Library, psyINFO, Web of Science, Wanfang Database, China National Knowledge Infrastructure, VIP, and China Biomedical Literature Service System from the establishment of the database to December 2024. The subject terms were then combined with free words to obtain relevant literature, and finally the literature was systematically searched. The English search terms included “tuberculosis/tuberculoses/pulmonary/pulmonary tuberculosis”, “emotions/experience/experience of illness/feeling/need/require/opinions/”, “qualitative study/phenomenology/grounded theory/descri*/action research/focus groups/interview”; the Chinese search terms included “pulmonary tuberculosis/pulmonary tuberculosis/tuberculosis”, “attitude/viewpoint/feeling/illness experience/experience”, “qualitative/qualitative research/phenomenology/grounded theory/narrative research/ethnography/action research”, etc. The detailed search strategies for each database, along with the number of records retrieved at each stage, are presented in Supplementary File 2.
Inclusion and Exclusion Criteria
The inclusion criteria will include the following: Participants: Patients diagnosed with pulmonary tuberculosis; (2) Phenomena of interest: Patients’ illness experiences, including their perceptions, feelings, and expectations regarding the disease (no restriction on the duration since diagnosis); (3) Context: Experiences across the full course of diagnosis, treatment, and daily life with pulmonary tuberculosis; (4) Study type: Original qualitative studies.
The exclusion criteria will include the following: (1) Duplicate publications or studies lacking extractable qualitative data; (2) Reviews, conference proceedings, or commentaries; (3) Studies published in languages other than Chinese or English; (4) Abstract-only articles without full-text access; (5) Studies rated as Grade C in methodological quality appraisal.
Search Outcome
A total of 5479 articles were retrieved. After removing duplicates, 3967 records remained. Title and abstract screening resulted in 59 studies, of which 21 met the inclusion criteria after full-text review. Two researchers (the first and second authors), both trained in evidence-based methods, independently screened the studies. Disagreements were resolved through discussion with a third researcher (the third author) to ensure accuracy and reliability. The complete search process and study selection are illustrated in Figure 1.
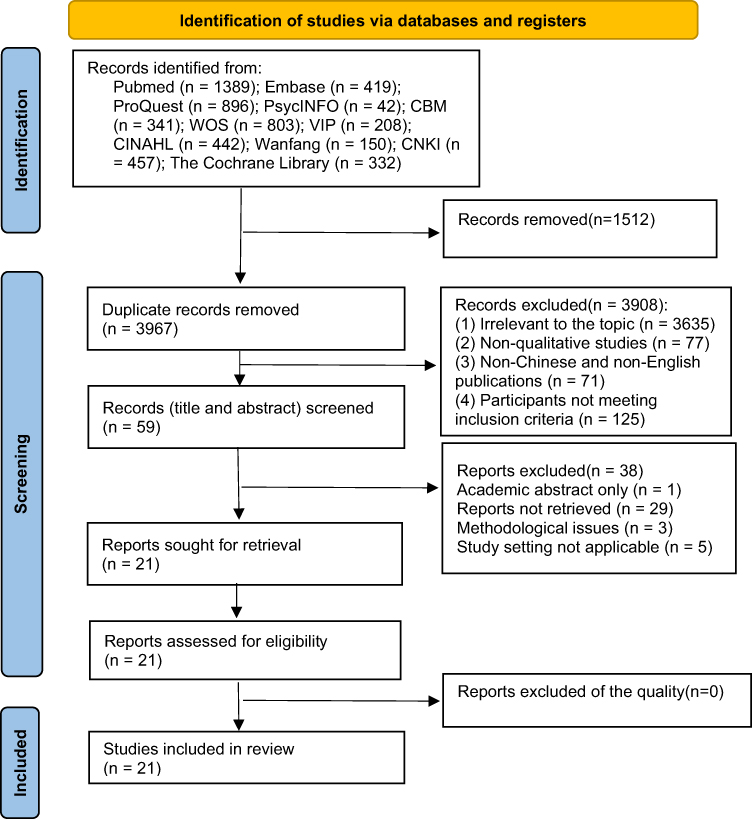 |
Figure 1 Search process and study selection of research article. |
Quality Appraisal
Two researchers independently assessed study quality using the JBI Critical Appraisal Checklist for Qualitative Research, which consists of 10 items rated as “Yes,” “No,” “Unclear,” or “Not applicable.” Studies were graded as A (high quality), B (moderate quality), or C (low quality).15 Only studies rated A or B were included. Any disagreements were resolved through discussion with a third researcher to ensure methodological consistency.
All 21 included articles were rated as Grade B, suggesting a potential risk of bias. Although all studies reported approval by an ethics review committee, none explicitly discussed the influence of researchers on the study or the reciprocal impact of the study on the researchers—criteria important for reflexivity in qualitative research.
Data Abstraction
Data extraction included: first author, publication year, country, interview setting, data collection method, phenomenon of interest, participant characteristics, methodological quality rating, and key findings. All included studies were imported into NVivo 12 for coding and management. Discrepancies in data abstraction were discussed with a third researcher until consensus was reached.
Synthesis
Thematic synthesis followed the three-step approach proposed by Thomas and Harden: (1) line-by-line coding of study findings; (2) organization of codes into descriptive themes; and (3) generation of analytical themes.
To enhance theoretical depth, the SEM was used as a guiding framework. A deductive-inductive approach was adopted to map patient narratives into four SEM domains:
Symptom perception – recognition and reporting of symptoms;
Cognitive appraisal – personal interpretations and beliefs about symptoms;
Emotional response – reactions such as fear, stigma, and distress;
Behavioral coping – symptom management strategies, including treatment adherence and social withdrawal.
A coding matrix was developed to align themes with SEM components. Themes that did not fully align with SEM were further analyzed with attention to broader social and structural influences, such as poverty, stigma, and healthcare access. This dual-layered synthesis approach enabled both theoretical integration and contextual sensitivity.
Results
Study Characteristics
The basic characteristics of the included studies are presented in Table 1. Across the 21 studies, a total of 469 participants were included.
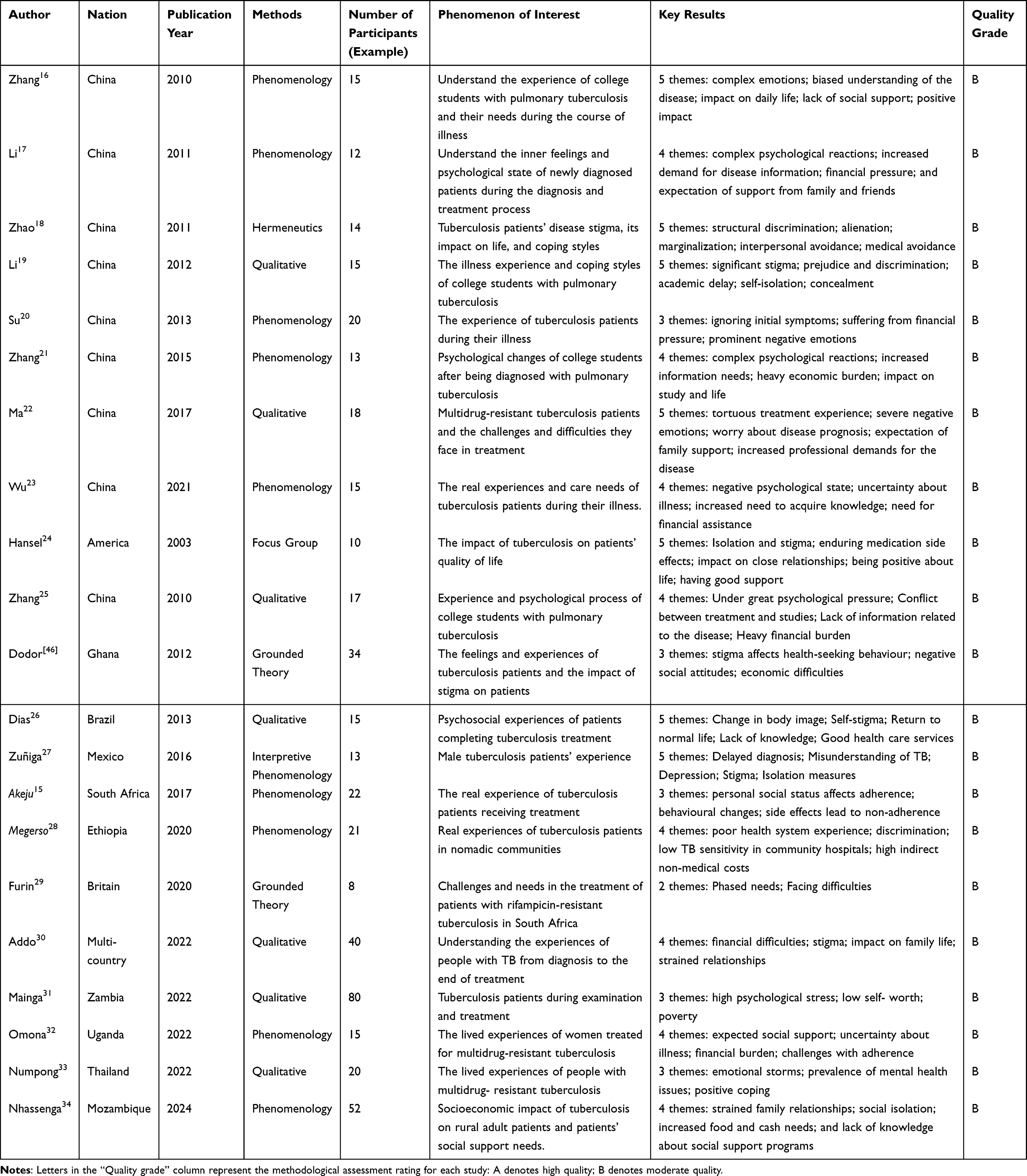 |
Table 1 Basic Characteristics of the Included Studies |
Meta-Integration Results
Based on 21 qualitative studies, this meta-integration extracted 36 credible findings, which were organised into nine descriptive categories and further synthesised into two integrated results: diverse and underrepresented disease experiences and multiple unmet needs among patients with pulmonary tuberculosis.
The first integrated result captures patients’ complex illness experiences, encompassing negative and positive psychological responses, adverse physiological experiences, stigma and discrimination, treatment-related difficulties, concerns about future life and prognosis, and post-traumatic growth. The second integrated result reflects patients’ unmet needs, including demands for disease-related knowledge, financial assistance, social support, and combined physiological and psychological care. Together, these findings delineate the multifaceted nature of pulmonary tuberculosis from the patient perspective (Figure 2).
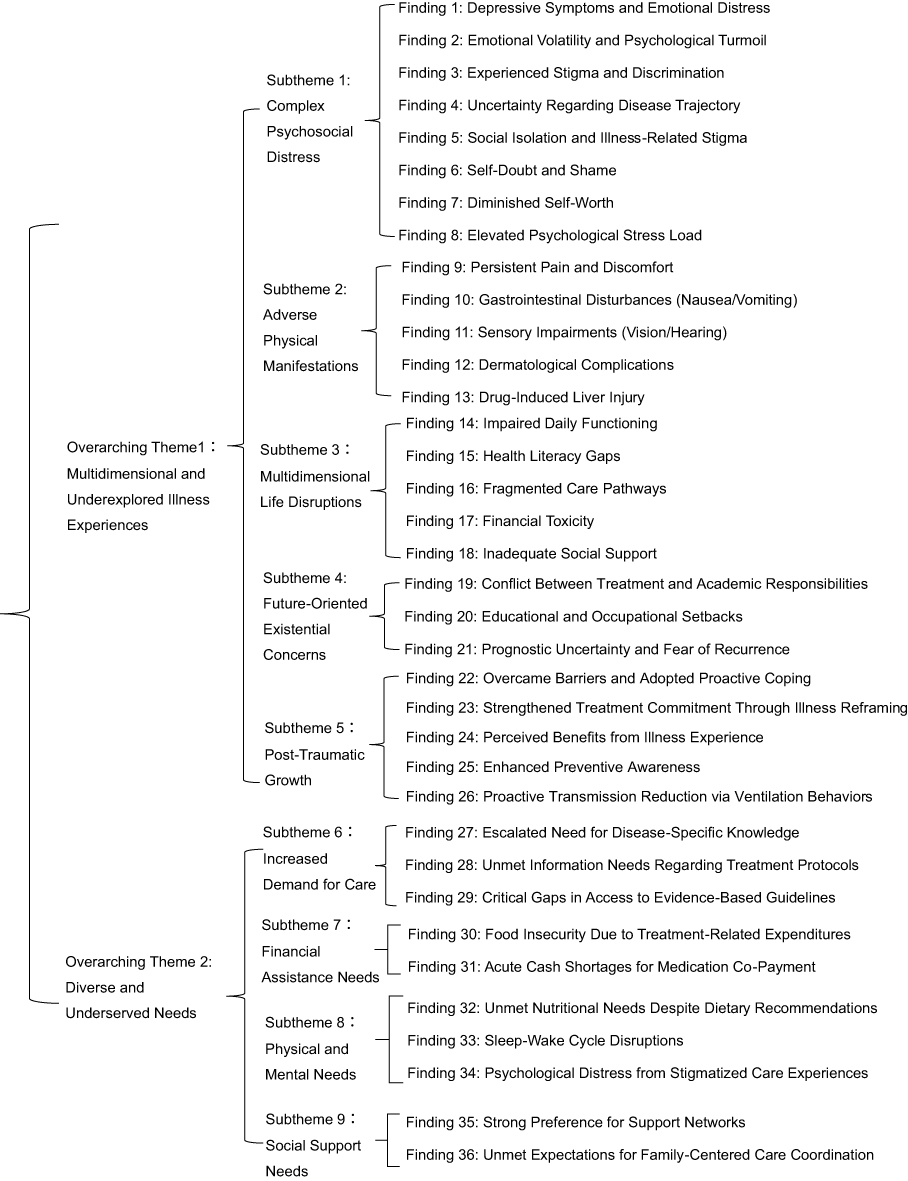 |
Figure 2 Meta-Synthesis Findings. |
Integration Result 1: Diverse and Underrepresented Disease Experiences
Category 1: Complex Negative Psychological Experiences
The disease experience of tuberculosis patients changes continuously as the disease progresses. When the disease is diagnosed, patients are shocked (“After the test, I was diagnosed with tuberculosis. I was surprised”17) and have doubts (“I have had repeated headaches, low fever, and coughs”22). When they learn that they have been infected by people around them, they feel angry (“My cousin has tuberculosis, but she didn’t tell me. As a result, she infected me. I was so angry”16). Most patients feel depressed and fearful (“When I first heard that I had tuberculosis, I felt like the sky was falling. I was very scared”19); at the same time, they are afraid of infecting others and feel very guilty (“At that time, my whole class went for a check-up. If someone was infected, I would feel guilty and even have a sense of guilt”27) and despair (“I was very desperate and even thought about committing suicide because of this disease”20). Some patients feel relieved when they are diagnosed (“When I started coughing up blood, my first reaction was cancer. Then I went for a check-up and they said I had a little tuberculosis. Hey, that’s fine now”29). During treatment, due to the infectiousness of tuberculosis, stigma was activated (“For me, this is a shame”32). Patients encountered discrimination due to tuberculosis infection (“Since I was found taking tuberculosis drugs, the people I used to live with are no longer willing to live in the same area or room with me. I can only live alone”17), and patients’ self-esteem was reduced (“For me, this disease is disgusting and I hate myself”26).
Category 2: Adverse Physiological Experience
The disease has a significant impact on the patient’s physiological condition. Patients often feel tired and weak (“After the treatment, I feel more tired and still feel weak. I don’t have as much energy as before”25); severe pain (“The joint pain is unbearable”17); some patients experience sleep disorders (“I go to bed early, but I can’t fall asleep and I am easily woken up”19), suffer from the disease (“I began to feel like I was being eaten, my voice was weak, my strength decreased, and my heart seemed to have no room to rest”18), and changes in body image (“I used to have light skin, but my skin became very dark”34). Patients discontinued treatment due to intolerable side effects (“The joint pain was unbearable, so I stopped treatment”17), leading to challenges with adherence.
Category 3: Facing Multiple Difficulties
Suffering from pulmonary tuberculosis causes patients to face multiple difficulties, including insufficient social support, a tortuous treatment experience, a heavy economic burden, and a lack of knowledge about the disease. At the same time, their daily lives and families are also greatly affected. These difficulties seriously affect the quality of life and treatment compliance of patients. When patients return to work and life, they lack social support, suffer discrimination and unfair treatment (“When I went to work, I found that my colleagues were wearing masks, and tears came out all of a sudden”18), and feel alienated (“When I first returned to work, people looked at me and took a step back”25). Many patients’ daily lives are greatly affected. They avoid social interactions and cut off contact with the outside world (“I feel bad when I go home for treatment. I don’t want to go out and see people. After dinner, I sit in the yard for a while and then go to sleep”;27 and avoid the fact of illness (“I try not to touch this topic and don’t think about the disease often. I try to live a disease-free life as usual”25). Some patients avoid medical treatment (“I don’t go to the hospital if I can, especially the infectious disease hospital”34) to avoid being discriminated against by others. During long-term home treatment, the patients’ families are also affected by the disease and family relationships become tense (“My family members don’t allow me to get close to them. People say I will die within a week”26). Many patients have difficulties with information about tuberculosis (“People say the disease is caused by smoking and drinking; I stopped these things a long time ago. I don’t eat on the street, so I don’t know how I got the disease”34), and are unaware of symptoms (“When I started to have signs of tuberculosis, I didn’t know what it was”18). They may even mistake the early symptoms of tuberculosis for malaria (“I started to feel feverish and thought it was malaria, so I bought medicine from the pharmacy”30). A small number of patients do not understand the changes in the course of tuberculosis (“I have been taking medicine as prescribed by the doctor for a long time, but the sputum smear result has not turned positive. It is impossible to cure it completely”23). A small number of patients experience a tortuous treatment process (“I went to a private clinic to seek treatment for loss of appetite, weight loss and abnormal night sweats. They said it was a ‘cold’ and sent me home with a dozen oral medications to be taken within a few weeks. I took the medicine as they recommended, but my health did not improve after taking it. I went to the clinic to explain the situation to them. This time, the diagnosis was ‘typhoid fever’ and I was given a different type of oral medication. A week later, I realized that my health was deteriorating, so I went to a nearby hospital”28). In addition, when describing their medical experiences, patients with drug-resistant TB repeatedly emphasized that treatment was delayed, mainly due to delayed drug resistance testing (“I had TB before and was treated at home on and off for more than a year, but no drug sensitivity test was done”16). Financial burden is also a major problem faced by patients. The high cost of anti-tuberculosis drugs, frequent examinations, and transportation costs are all huge financial pressures, especially for patients in rural areas (“My family is from the countryside, and my parents grow crops and sell food to support my schooling. How can they afford medical treatment?”26); indirect costs of treatment, such as transportation costs, also increase the financial burden on patients (“Sometimes we don’t have transportation costs”31).
Category 4: Worry About the Future
Tuberculosis patients interrupt their studies and work due to the disease and worry about the future, mainly focusing on academic and career prospects, disease recurrence, and uncertainty about prognosis. They face a conflict between treatment and study (“I don’t want to go home. How can I study while receiving treatment at home?”27). Young and middle-aged people are forced to interrupt their studies and work, and are more worried about whether they can smoothly return to their studies or work after recovering from the disease (“I was diagnosed with drug-resistant tuberculosis”,16 “I just changed jobs to a new company. If my boss knew that I had tuberculosis, he would definitely find all kinds of reasons to fire me”23). They worry about disease recurrence (“I am afraid that if I have too much pressure in study or work in the future, tuberculosis will recur”19) and prognosis (“I think the cure rate is only 50% or even lower. The medical staff told me that I need at least 6 months of treatment, but I still haven’t recovered after two years. This makes me worry that I will die soon”23).
Category 5: Post-Traumatic Growth
Patients face tuberculosis head-on, overcome obstacles in the treatment process, have confidence in recovery (“I believe I can survive the disease”21), strengthen their beliefs (“It is difficult, but you have to cheer up and keep moving forward. Don’t give up”25), and become more positive (“There are many things I didn’t do before I got the disease, but now I do them. I am more positive about it”24); they can even think from other people’s perspectives and understand other people’s prejudices (“Sometimes if you put yourself in other people’s shoes, you can understand. If someone else were sick now, I would definitely have some taboos”,27 then have grown from the disease (“I feel that I have grown a lot. Maybe when I encounter difficulties in the future, I may be able to get through it because of my previous experience”19). Patients witnessed other patients die in the hospital (“Many people died in front of me because they didn’t take their medicine”,32 and this experience motivated them to adhere to treatment (“I have to do my best not to skip treatment days”25), and cope with side effects (“I want to vomit, and the nurse told me it will happen and it will pass”17). TB patients actively followed the doctor’s instructions for treatment (“I plan to complete my treatment, even if it means moving to another city, I will ask to be transferred to another clinic”17), became aware of their own bad habits, and gradually developed adjustment plans to cope with the disease, such as balanced diet and exercise (“I exercise more now, walk more, and am more active than before”17); they also took active ventilation measures to reduce the risk of transmission in the home (“I opened the windows to let in fresh air”17). They also practice a range of isolation measures (“When I was diagnosed with TB, my relatives took me to the hospital to take medication, and I kept my distance from them to avoid contaminating them”31), and patients are able to actively manage their own medication (“Take 25 large pills a day”24).
Integration Result 2: Multiple Unmet Needs
Category 6: Demand for Disease Expertise
Faced with the particularity of tuberculosis, patients are eager to learn about disease transmission (“I went home a few days ago and asked my family members whether they needed to take X-rays or collect sputum for examination”33). When faced with complex treatment plans, patients are eager to obtain disease knowledge through multiple channels (“In addition to asking doctors and nurses for information, I also asked friends and searched the Internet for information about tuberculosis”22). They are even eager to get professional help during follow-up visits after discharge (“I really hope that doctors and nurses will personally explain the knowledge and precautions of the full course of chemotherapy for tuberculosis. How can I prevent my family from being infected at home?”22). For adolescent patients, they are eager to obtain health education knowledge about infectious diseases (“Frequent and vigorous publicity on infectious diseases makes people aware of it”19).
Category 7: Need for Financial Assistance
After being diagnosed with pulmonary tuberculosis, patients lose their jobs (“I was fired by the company and have been out of work for eight months”18,24). Treatment costs are expensive (“X-rays are free, but every visit to the doctor still costs a lot of money. Liver protection and tuberculosis pills are expensive”29); indirect costs of treatment, such as transportation costs, will also increase the financial burden on patients (“Some days we don’t have transportation costs, and I have to walk from there (home) to here (medical facility)”34). The financial burden largely hinders patients from seeking further medical treatment.
Category 8: Social Support Needs
The social support needs of TB patients cover emotional, material, medical, legal and social care. Patients experience structural discrimination and expect to receive more support in terms of job protection and legal rights (“I went to work after testing negative, but my boss heard that I was still taking medicine and told me to stay home! I have to take medicine for a year. It seems that the labor law cannot protect us sick employees for such a long time. I was fired after only six months of sick leave!”18). Patients also yearn for material help (“I saw those people infected with HIV a few days ago. They were given food, peanuts, like peanut butter, but not me…”33). The high cost of auxiliary drugs and the fact that they are not covered by discounts (“It’s all self-paid, and a day in hospital costs more than 1,000 yuan. It’s unbearable”29) have led patients to hope for support from medical policies. Patients who experience vulnerability and pain often suffer from severe psychological stress, have a significantly increased degree of dependence on others (“I want my family to come and be with me”16), urgently need help from their family due to the impact of the disease (“My physical condition has deteriorated so much that I can’t stand or walk”26), and crave support to gain the motivation to persist in treatment.
Category 9: Physiological and Psychological Needs
The physiological needs of pulmonary tuberculosis patients mainly include: nutritional support, improved sleep, and restoration of limb function; psychological needs are to cope with social discrimination and obtain psychological comfort. Pulmonary tuberculosis patients usually need adequate nutrition to support the body’s immune function and recovery process. Sometimes they cannot get enough nutrition (“Sometimes my family will go on a hunger strike and I have nothing to eat”34). Due to the side effects of drugs, patients often have sleep disorders, which further affects recovery (“I used to sleep on my side, but now I can’t sleep without taking painkillers…”24). Due to the severity of the disease, some patients’ limb functions are seriously affected (“My physical condition has deteriorated so badly that I can’t stand or walk”26). In addition, patients face discrimination (“They isolated me like the plague”24), are under psychological pressure, and are in urgent need of psychological comfort (“I feel like I have been wronged and need comfort…”19).
Discussion
Strengthening Symptom Management and Multilevel Support Based on the SEM
This study confirms that TB patients’ illness experience is complex and multidimensional, encompassing physical discomfort, cognitive interpretation, emotional responses, and behavioral coping. SEM offers a comprehensive framework to understand these processes and guide targeted interventions.
From the perspective of symptom perception, patients frequently experience severe side effects—such as hepatotoxicity, visual disturbances, and gastrointestinal discomfort—which may be misinterpreted, leading to fear, anxiety, and poor treatment adherence.29,33 To address this, clinicians should implement proactive symptom monitoring and provide educational materials to help patients accurately understand bodily sensations, enhancing their confidence in managing treatment.
Cognitive appraisals of illness also significantly impact treatment engagement. Many patients viewed TB as a stigmatized condition, leading to shame, self-blame, and psychological withdrawal.33 Interventions such as cognitive restructuring, narrative reframing, and family-involved psychoeducation may help patients reconstruct a more positive understanding of their illness.35 Meanwhile, long treatment durations and social isolation frequently induce emotional distress, especially depression and anxiety. Emotional support strategies—like peer sharing, narrative writing, and guided counseling—can be integrated into care pathways to improve emotional resilience.36,37 Notably, patients who successfully reframed their experience often demonstrated stronger treatment adherence and psychological adjustment, indicating the importance of fostering post-traumatic growth and strengthening coping capacity.38 Clinicians should proactively cultivate patients’ adaptive behaviors through continuous encouragement, psychosocial education, and value-guided interventions.
Behaviorally, adaptive coping strategies—such as information-seeking, emotional expression, and social problem-solving—are positively associated with treatment persistence. Clinicians can nurture such behaviors by providing consistent encouragement, structured psychoeducation, and meaning-centered therapeutic engagement.
To enhance conceptual clarity, Table 2 presents a visual mapping between the key dimensions of the SEM and the thematic findings synthesized from the included studies.
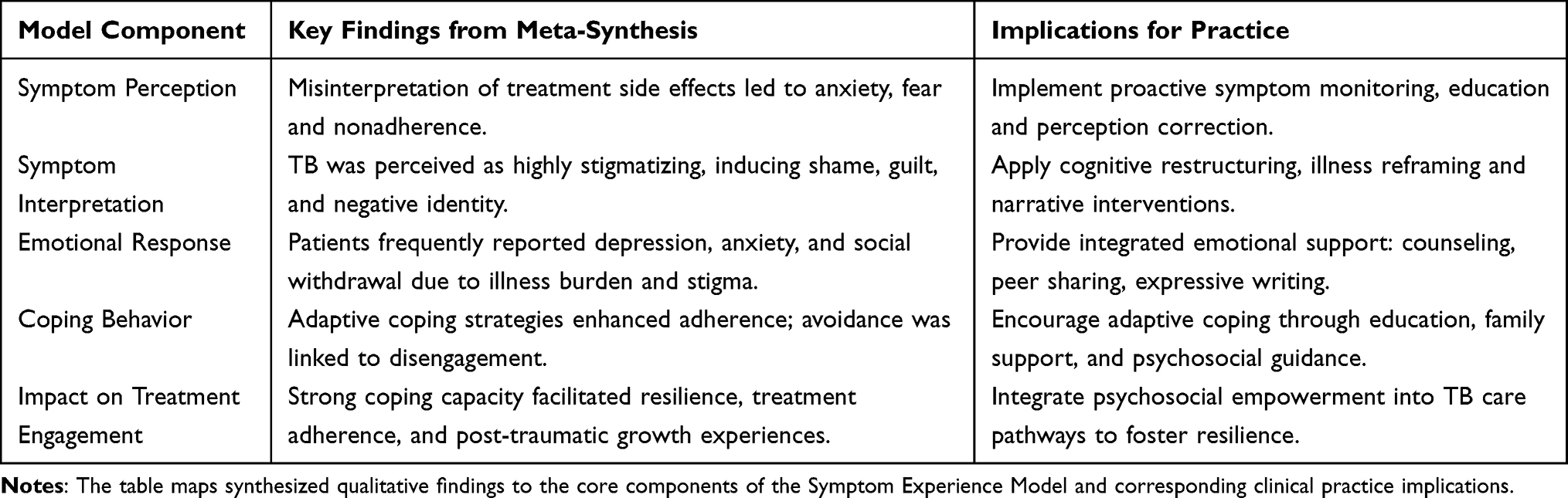 |
Table 2 Mapping Synthesized Findings to the Symptom Experience Model |
Responding to Unmet Needs Across Multiple Levels Within the SEM Framework
Beyond symptom experience, patients in this study expressed numerous unmet needs, including emotional reassurance, continuity of care, financial assistance, and social reintegration. Although these needs vary in scope, they can be addressed within the SEM framework by tailoring interventions across different care levels, which is consistent with findings from previous studies highlighting similar unmet needs among tuberculosis patients.39
At the individual level, establishing trust-based therapeutic relationships and providing empathic communication are crucial to improving patient outcomes.40 Many patients, particularly those dealing with drug-resistant forms of TB or experiencing prolonged hospitalization, often report feelings of isolation and hopelessness. In such cases, consistent emotional support from healthcare professionals can play a vital role in reducing psychological distress. In addition, family support significantly reinforces treatment adherence and alleviates emotional distress, particularly for elderly or socially isolated patients.41 Healthcare teams should incorporate family education, psychological counseling, and social support tools to enhance the patient’s immediate care environment. Encouraging family participation not only fosters a more supportive home environment but also helps ensure continuity of care after discharge.
At the clinical level, current practices often emphasize biomedical indicators while neglecting patients’ subjective symptom experiences.42 This biomedical focus can lead to under-recognition of psychological suffering, fatigue, or social discomfort, which may influence adherence and overall quality of life. To address this gap, healthcare providers should implement real-time symptom tracking systems, incorporate routine psychological assessments, and deliver personalized symptom education.43 Furthermore, involving nurses and allied health professionals in continuous symptom monitoring can improve care continuity and ensure timely emotional support.
At the healthcare system level, persistent challenges such as stigma, inadequate insurance coverage, and insufficient long-term support services remain significant barriers.7,44 These systemic gaps can exacerbate health inequalities, particularly among marginalized populations. Although systemic reforms are beyond this study’s direct scope, our findings underscore the need for policy advocacy and public education initiatives to reduce stigma and facilitate social reintegration. Clinicians should also proactively connect patients with community and government resources to alleviate psychosocial and economic burdens. Collaborative partnerships between public health institutions, community organizations, and healthcare systems may help expand access to essential services and support networks for patients throughout the treatment continuum.
In summary, even without incorporating broader socio-ecological theories, the SEM offers a robust theoretical foundation to guide multilevel interventions. By aligning care strategies with patients’ real-world symptom experiences and their associated needs, healthcare teams can provide more integrated, compassionate, and effective tuberculosis care.
Study Limitations
Despite the strengths of this meta-synthesis, several limitations must be acknowledged. First, the included studies were primarily conducted in low- and middle-income countries and published in English or Chinese, which may limit the cultural and linguistic diversity of perspectives and reduce the generalizability of the findings. Second, there was notable heterogeneity across studies in terms of participant characteristics, TB types (eg, drug-sensitive vs drug-resistant), and treatment phases, which may have influenced the consistency of identified themes. Third, inconsistencies in the definition and conceptualization of “symptom experience” across studies posed challenges for thematic synthesis and may have influenced the comparability and interpretation of findings. Moreover, despite efforts to ensure rigor through quality appraisal and independent coding, the interpretive nature of meta-synthesis carries an inherent risk of researcher bias. Lastly, the exclusion of gray literature and unpublished studies may have introduced publication bias and omitted relevant perspectives.
Conclusion
This qualitative meta-synthesis highlights the complex symptom experiences and unmet needs of TB patients, characterized by the interplay of physical discomfort, emotional distress, and social disruption. While no theoretical framework was applied during data extraction, the findings align closely with SEM, demonstrating how symptom perception, emotional appraisal, and coping behaviors shape the illness experience. However, structural factors—such as poverty, stigma, and healthcare barriers—emerged as critical influences beyond the explanatory scope of the SEM.
Clinicians should not only assess symptom severity but also consider patients’ cognitive and emotional interpretations. Interventions incorporating psychological support, stigma reduction, and personalized health education may strengthen treatment adherence. Addressing structural barriers remains essential to improving equity and patient outcomes.
This review underscores the need for integrated, patient-centered care approaches that go beyond symptom management to include patients’ emotional, cognitive, and social needs. Nurses and clinicians should be trained to recognize the psychological and social dimensions of TB symptoms, particularly those linked to stigma and emotional burden. Health policies should prioritize access to psychological support, health education, and community-based interventions that reduce structural barriers and promote treatment adherence. For researchers, future work should focus on validating and adapting the SEM for TB populations by incorporating socioecological variables. Mixed-methods and longitudinal designs will be essential to explore how symptom experiences evolve over time and how interventions can be tailored to diverse patient contexts.
Clinical Trial Registration
As it was based entirely on previously published studies, this study protocol had registered on the PROSPERO website (CRD42024572729).
Data Sharing Statement
The data and materials that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval Statement
This study involves a qualitative meta-synthesis of published literature and did not require approval from an institutional review board, as no primary data were collected.
Patient Consent Statement
There was no direct contribution from patients to this study because the data were sourced solely from previously published articles.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Project of Sichuan Medical Association (No. S2024036). This research was funded by Science and Technology Project of Sichuan Provincial Health Commission (No. 24QNMP049).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2024. Geneva: World Health Organization; 2024.
2. Méda ZC, Somé T, Sombié I, et al. Patients infected by tuberculosis and human immunodeficiency virus facing their disease, their reactions to disease diagnosis and its implication about their families and communities, in Burkina Faso: a mixed focus group and cross sectional study. BMC Res Notes. 2016;9:373. doi:10.1186/s13104-016-2183-3
3. Sahasrabudhe T, Nilgiri KM. Quantitative study of physical, social, psychological, and environmental challenges faced by patients with drug-resistant tuberculosis. Cureus. 2024;16(9):e69694. doi:10.7759/cureus.69694
4. Lönnroth K, Jaramillo E, Williams BG, et al. Drivers of tuberculosis epidemics: the role of risk factors and social determinants. Soc Sci Med. 2009;68(12):2240–15. doi:10.1016/j.socscimed.2009.03.041
5. Rukasha I, Kaapu KG, Fortune SM, et al. Treatment outcomes for drug-resistant tuberculosis patients on Bedaquiline-based regimens in a mostly rural South Africa. Infect Drug Resist. 2025;18:1819–1829. doi:10.2147/idr.S502302
6. Ieque AL, Palomo CT, Castro Moreira D, et al. Systematic review of tuberculous meningitis in high-risk populations: mortality and diagnostic disparities. Future Microbiol. 2024:1–13. doi:10.1080/17460913.2024.2366604
7. Courtwright A, Turner AN. Tuberculosis and stigmatization: pathways and interventions. Public Health Rep. 2010;125(Suppl 4):34–42. doi:10.1177/00333549101250s407
8. Tanimura T, Jaramillo E, Weil D, et al. Financial burden for tuberculosis patients in low- and middle-income countries: a systematic review. Eur Respir J. 2014;43(6):1763–1775. doi:10.1183/09031936.00193413
9. Dodd M, Janson S, Facione N, et al. Advancing the science of symptom management. J Adv Nurs. 2001;33(5):668–676. doi:10.1046/j.1365-2648.2001.01697.x
10. Armstrong TS. Symptoms experience: a concept analysis. Oncol Nurs Forum. 2003;30(4):601–606. doi:10.1188/03.Onf.601-606
11. Leventhal H, Phillips LA, Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. 2016;39(6):935–946. doi:10.1007/s10865-016-9782-2
12. Xie M, Wang A, Zhang Z, et al. A path analysis on quality of life of people with HIV: validation and refinement of the self-regulatory HIV/AIDS symptom management model. J Assoc Nurs AIDS Care. 2024;35:495–506. doi:10.1097/JNC.0000000000000493
13. Lenore H, Heather L, Janine C, et al. Symptom experience of older adults with type 2 diabetes and diabetes-related distress. J Nursing Res. 2019;68(5):374–382. doi:10.1097/NNR.0000000000000370
14. Page MJ, Mckenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
15. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. 2015;13(3):179–187. doi:10.1097/xeb.0000000000000062
16. Ma XX, Zhang SR, Zhang TH, et al. A qualitative study on illness experience of patients with multidrug-resistant tuberculosis. Chin J Antituberculosis. 2017;39(5):529–532.
17. Akeju OO, Wright SCD, Maja TM. Lived experience of patients on tuberculosis treatment in Tshwane, Gauteng province. Health SA. 2017;22(1):259–267. doi:10.1016/j.hsag.2017.03.001
18. Zhao AQ, Wu PX, Huang HX. Qualitative study of stigma experienced by patients with pulmonary tuberculosis. J Nurs. 2011;18(15):75–78. doi:10.16460/j.issn1008-9969.2011.15.025
19. Zhang SR, Yan H, Zhang JJ, et al. The experience of college students with pulmonary tuberculosis in Shaanxi, China: a qualitative study. BMC Infect Dis. 2010;10:174. doi:10.1186/1471-2334-10-174
20. Zuñiga JA, Muñoz S, Johnson MZ, et al. Mexican American Men’s experience of living with tuberculosis on the U.S.-Mexico Border. Am J Mens Health. 2016;10(1):32–38. doi:10.1177/1557988314555359
21. Zhang AH. Psychological experience of newly diagnosed college students with pulmonary tuberculosis. Yiyao Qianyan. 2015;7:389–390. doi:10.3969/j.issn.2095-1752.2015.07.346
22. Li JD, Chen GF, Yuan YL. Qualitative research of mental experience in first diagnosed young tuberculosis patients. Chin J Modern Nurs. 2011;17(5).
23. Wu WJ, Ying XY, Lou QE. A qualitative study on the illness experience and care needs of patients with pulmonary tuberculosis. Modern Pract Med. 2021;33(5):651–652.
24. Hansel NN, Wu AW, Chang B, et al. Quality of life in tuberculosis: patient and provider perspectives. Qual Life Res. 2004;13(3):639–652. doi:10.1023/B:QURE.0000021317.12945.f0
25. Dias AA, De Oliveira DM, Turato ER, et al. Life experiences of patients who have completed tuberculosis treatment: a qualitative investigation in southeast Brazil. BMC Public Health. 2013;13:595. doi:10.1186/1471-2458-13-595
26. Omona K, Ogwang C. Lived experiences of female patients aged 15-49 years undergoing treatment for multi-drug resistant tuberculosis (MDR-TB) in Lira Regional Referral Hospital, Uganda. Cogent Public Health. 2024;11(1). doi:10.1080/27707571.2023.2292892
27. Li XH, Lu DD, Zhang SR, et al. Experience and coping styles of pulmonary tuberculosis college students. Chin J Modern Nurs. 2012;18(27):3256–3258. doi:10.3760/cma.j.issn.1674-2907.2012.27.011
28. Megerso A, Deyessa N, Jarso G, et al. Lived experiences of tuberculosis patients and their implications for early tuberculosis case identification and management in pastoralist community setting: a qualitative study in Borena zone, Oromia region of Ethiopia. BMC Health Serv Res. 2020;20(1):933. doi:10.1186/s12913-020-05787-1
29. Su L, Sun YM, Lin KK, et al. Qualitative study on the illness experience of pulmonary tuberculosis patients. Mod Preventive Med. 2013;40(1):102–105.
30. Addo J, Pearce D, Metcalf M, et al. Living with tuberculosis: a qualitative study of patients’ experiences with disease and treatment. BMC Public Health. 2022;22(1):1717. doi:10.1186/s12889-022-14115-7
31. Mainga T, Gondwe M, Mactaggart I, et al. Qualitative study of patient experiences of mental distress during TB investigation and treatment in Zambia. BMC Psychol. 2022;10(1):179. doi:10.1186/s40359-022-00881-x
32. Furin J, Loveday M, Hlangu S, et al. “A very humiliating illness”: a qualitative study of patient-centered Care for Rifampicin-Resistant Tuberculosis in South Africa. BMC Public Health. 2020;20(1):76. doi:10.1186/s12889-019-8035-z
33. Numpong S, Kengganpanich M, Kaewkungwal J, et al. Confronting and coping with multidrug-resistant tuberculosis: life experiences in Thailand. Qual Health Res. 2022;32(1):159–167. doi:10.1177/10497323211049777
34. Nhassengo P, Yoshino C, Zandamela A, et al. ‘They didn’t look at me with good eyes’ - experiences of the socioeconomic impact of tuberculosis and support needs among adults in a semi-rural area in Mozambique: a Qualitative Study. Glob Public Health. 2024;19(1):2311682. doi:10.1080/17441692.2024.2311682
35. Liu XF, Ma GX, Gan J, et al. Application status and suggestion of quality of life scale for pulmonary tuberculosis patients. Chin J Antituberculosis. 2020;42(03):200–203.
36. Desanto D, Velen K, Lessells R, et al. A qualitative exploration into the presence of TB stigmatization across three districts in South Africa. BMC Public Health. 2023;23(1):504. doi:10.1186/s12889-023-15407-2
37. Coventry PA, Meader N, Melton H, et al. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: systematic review and component network meta-analysis. PLoS Med. 2020;17(8):e1003262. doi:10.1371/journal.pmed.1003262
38. Storm M, Fortuna KL, Brooks JM, et al. Peer support in coordination of physical health and mental health services for people with lived experience of a serious mental illness. Front Psychiatry. 2020;11:365. doi:10.3389/fpsyt.2020.00365
39. Li PZ, Guo HG. Effects of narrative nursing on psychological status and quality of life in patients with pulmonary tuberculosis. J Clin Nurs Pract. 2021;7(4):124–126.
40. Shiratani KN. Psychological changes and associated factors among patients with tuberculosis who received directly observed treatment short-course in metropolitan areas of Japan: quantitative and qualitative perspectives. BMC Public Health. 2019;19(1):1642. doi:10.1186/s12889-019-8001-9
41. Munro SA, Lewin SA, Smith HJ, et al. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007;4(7):e238. doi:10.1371/journal.pmed.0040238
42. Wang XB, Li XL, Zhang Q, et al. A survey of anxiety and depressive symptoms in pulmonary tuberculosis patients with and without tracheobronchial tuberculosis. Front Psychiatry. 2018;9:308. doi:10.3389/fpsyt.2018.00308
43. Bukenya D, Mayanja BN, Nakamanya S, et al. What causes non-adherence among some individuals on long term antiretroviral therapy? Experiences of individuals with poor viral suppression in Uganda. AIDS Res Ther. 2019;16(1):2. doi:10.1186/s12981-018-0214-y
44. Li Y, Ehiri J, Tang S, et al. Factors associated with patient, and diagnostic delays in Chinese TB patients: a systematic review and meta-analysis. BMC Med. 2013;11:156. doi:10.1186/1741-7015-11-156
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Facilitating and Hindering Factors in Discharge Preparation During the Hospital-to-Home Transition Period for Newly Diagnosed Tuberculosis Patients: A Qualitative Study
Yu Q, Hu Y, Yao R, Zhang T, Huang L, Li Y, Wan B, Xie F, Shao X, Yang X
Patient Preference and Adherence 2026, 20:602859
Published Date: 24 June 2026