Back to Journals » Infection and Drug Resistance » Volume 16
Extracorporeal Membrane Oxygenation in Severe Acute Respiratory Distress Syndrome Caused by Chlamydia abortus: A Case Report
Authors Huang J, Liu C, Zhou Z, Xia H, Zhu Z, Lu J, Lin J, Chen Z, Ye Q, Zuo L
Received 6 March 2023
Accepted for publication 16 May 2023
Published 19 June 2023 Volume 2023:16 Pages 3893—3901
DOI https://doi.org/10.2147/IDR.S411331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jiequn Huang,1 Changzhi Liu,1 Zhujiang Zhou,1 Han Xia,2 Zhensheng Zhu,2 Jianhai Lu,1 Jingcheng Lin,1 Zhen Chen,1 Qimei Ye,1 Liuer Zuo1
1Department of Intensive Care Unit, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde Foshan), Foshan, Guangdong, People’s Republic of China; 2Department of Scientific Affairs, Hugobiotech Co, Ltd, Beijing, People’s Republic of China
Correspondence: Liuer Zuo, Department of Intensive Care Unit, Shunde Hospital, Southern Medical University (The First People’s Hospital of Shunde, Foshan), Foshan, Guangdong, People’s Republic of China, Email [email protected]
Background: Pneumonia infected by Chlamydia abortus (C. abortus) is rare, especially complicated with severe acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS).
Case Presentation: We presented the clinical details of a 44-year-old male who was diagnosed with C. abortus pneumonia, which rapidly progressed and ultimately led to ARDS, sepsis and MODS. Although he was initially diagnosed with pneumonia upon admission, no pathogenic bacteria were detected in sputum by conventional tests. Empirical intravenous infusion of meropenem and moxifloxacin was administered, but unfortunately, his condition deteriorated rapidly, especially respiratory status. On Day 2 after extracorporeal membrane oxygenation (ECMO) initiation, metagenomic next-generation sequencing (mNGS) was performed on the patient’s bronchoalveolar lavage fluid, which indicated an infection with C. abortus. The patient’s antimicrobial therapy was adjusted to oral doxycycline (0.1g every 12h), intravenous azithromycin (0.5g every day), and imipenem and cilastatin sodium (1g every 6h). The patient’s condition improved clinically and biologically. However, the patient was discharged due to financial reasons and unfortunately passed away eight hours later.
Conclusion: Infections with C. abortus can result in severe ARDS and serious visceral complications which necessitate prompt diagnosis and active intervention by clinicians. The case highlights the significance of mNGS as an essential diagnostic tool for uncommon pathogens. Tetracyclines, macrolides or their combinations are effective choices for treatment of C. abortus pneumonia. Further study is needed to explore the transmission routes of C. abortus pneumonia and establish precise guidelines for antibiotic treatment.
Keywords: Chlamydia abortus, ECMO, pneumonia, acute respiratory distress syndrome, metagenomic next-generation sequencing
Introduction
Chlamydia abortus is a non-motile, obligate intracellular Gram-negative bacteria that belongs to the Chlamydiales family. It primarily colonizes the placenta of ruminants such as sheep, goats, cattle, pigs, horses, among others, and can cause abortion.1 Human infections with C. abortus are infrequent, but they can result in severe symptoms, especially in pregnant women and immunocompromised individuals, such as abortion, stillbirth, and gestational sepsis.2 Studies reported that the primary mode of transmission is through direct contact with infected animals or secondary contaminated environments and the oronasal mucosa, and there is little risk of contracting the infection through indirect contact from visiting or living near a farm affected by C. abortus.3,4 Until now, the exact route of infection and the infectious dose for humans remain unclear.
As far as we know, pneumonia is rarely caused by C. abortus and there are only five cases have been reported worldwide.5–9 However, it should be noted that none of these patients received venovenous extracorporeal membrane oxygenation (VV-ECMO), a life-saving rescue therapy for acute respiratory distress syndrome (ARDS) patients when conventional ventilator strategies have proven to be ineffective. Here, we described the first case of severe pneumonia caused by C. abortus, who developed refractory ARDS and was treated with ECMO. The patient received a combination of medical therapy with doxycycline and azithromycin, along with imipenem and cilastatin sodium in China.
Case Presentation
A 44-year-old male, who was a chronic hepatitis B virus carrier with normal liver function, was admitted to the local hospital with a seven-day history of dry cough, shortness of breath and hypodynamia. Three days prior to admission, he experienced frequent coughing with yellow-white sputum and high fever (38.9°C). The patient had a 20-year history of smoking approximately twenty cigarettes daily. Upon querying the patient’s wife, we learned that he worked as a handyman but denied recent exposure to sick animals or visiting to farms.
On admission, physical examination showed a temperature of 38.7°C, heart rate of 134/min, respiratory rate of 24/min, blood pressure of 124/70 mmHg, and fine crackles in the left lung. A chest computed tomography (CT) scan demonstrated patchy high-density shadows with blurred margins present in both the posterior segment of the left upper lung and the dorsal segment of the lower lung, which is indicative of pan-lobar pneumonia (Figure 1). Laboratory tests showed slightly elevated leucocyte count (10.77 × 109/L), D-dimer and glucose levels (31.21 mg/L and 9.93 mmol/L, respectively), while other indicators such as blood urea nitrogen (27.57 mmol/L), creatinine (576 umol/L), C reactive protein (>200 mg/L), procalcitonin (PCT) (36.33 ug/L), alanine aminotransferase (107 IU/L), aspartate aminotransferase (401 IU/L), lactic dehydrogenase (2119 IU/L), creatine kinase (4620 IU/L), and serum total bilirubin (67.1 umol/L) were significantly elevated. In contrast, the serum albumin and serum sodium levels were found to be predominantly decreased to 25.8 g/L (normal: 40–55 g/L) and 128 mmol/L (normal: 137–147 mmol/L), respectively. Arterial blood gas analysis (nasal cannula at 3 L/minute inhalation) showed normal pH (7.45), PaO2 (71.3mmHg) and blood lactate (1.5mmol/L), decreased PaCO2 (25.5mmHg) and PO2/FiO2 (216.1mmHg). Samples of sputum, urine and blood were collected for culture, while no pathogenic bacteria, fungi of viruses were found. Acid-fast staining of sputum was negative on three separate occasions. Considering the clinical assessment and the possibility of infection from rare pathogens, the patient was diagnosed with pneumonia, and empiric treatment was initiated with intravenous infusion of meropenem (1g every 8h) and moxifloxacin (0.4 g every day). The clinical course of the patient is depicted in Figure 2.
 |
Figure 1 Chest computed tomography scans on the 0th day of hospitalization in the local hospital (A and B). CT scans showed patchy high-density shadows with blurred margins in both the posterior segment of the left upper lung and the dorsal segment of the lower lung. |
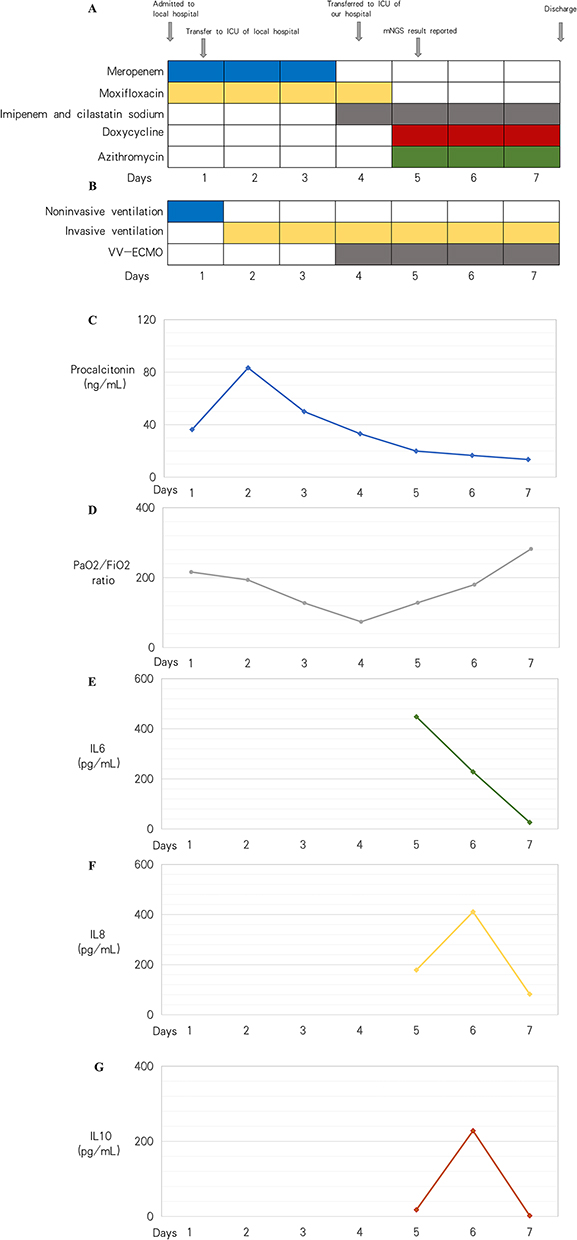 |
Figure 2 The clinical course of the patient with Chlamydia abortus infection. (A) Antibiotic application during hospitalization. (B) The types of ventilation in the clinical course. (C–G) The changes of procalcitonin, PO2/FiO2, IL-6, IL-8 and IL-10 on each day. |
After 6 hours of hospitalization, the patient’s respiratory status deteriorated and delirium was observed. As a result, the patient required intubation and ventilator (A/C, FiO2 80%, f 15 breaths/min, Vt 480 mL, PEEP 3.0 cmH2O). He was then immediately transferred to the intensive care unit (ICU) of local hospital. Repeated blood-gas analysis showed that the pH level was at 7.23, PaCO2 at 34mmHg, PaO2 at 193.5mmHg, PO2/FiO2 at 193.5mmHg, and blood lactate at 1.3mmol/L. After the family requested to transfer him to our hospital for further treatment, the patient was taken to the ambulance. However, during transportation, he experienced episodes of significant hypoxemia with oxygen saturation (SpO2) ranging from 60% to 70%. Additionally, a large amount of hemorrhagic fluid gushed out from the tracheal tube, and wet and dry rales could be heard clearly in both lungs. Arterial blood-gas analysis showed that the pH level was at 7.29, PaCO2 at 30.4mmHg, PaO2 at 73.7mmHg, PO2/FiO2 at 73.7mmHg, and blood lactate at 2.3mmol/L. Obviously, the patient developed ARDS and due to this, the transfer was terminated. To treat this condition, lung-protective ventilation, deep sedation, analgesia, paralysis using neuromuscular blocker and continuous renal replacement therapy were administered. Additionally, prone-position ventilation was given to ameliorate hypoxia.
On the second day after intubation, the patient’s condition worsened with an increase in bilateral pulmonary infiltrates, leucocyte count and PCT levels (19.54 × 109/L and 83.26 ug/L, respectively). The ventilatory parameters were also high (A/C, FiO2 100%, f 15 breaths/min, Vt 450mL, PEEP 18 cmH2O). A decision was made to establish VV-ECMO with the initial settings: flow 4.5L/min, 3475 RPM and sweep gas flow 4 L/min. The patient underwent cannulation using a left femoral–right internal jugular vein approach. To maintain a plateau pressure <25 cmH2O, ventilatory parameters were set to a tidal volume of 6 mL/kg, PEEP 10 cmH2O, and a respiratory rate of 15 bpm. Subsequently, the patient was transferred to the ICU of our hospital for further care, which is the nearest tertiary care facility. The patient’s Acute Physiology and Chronic Health Evaluation II score upon admission was 17. To get more information on pathogen, bronchoalveolar lavage fluid (BALF) sample was obtained to perform metagenomic next-generation sequencing (mNGS) detection (Hugobiotech Co., Ltd., Beijing, China). Follow-up laboratory testing results showed IL-6 level was at 447.9 pg/mL (normal range < 7.0 pg/mL), IL-8 at 178.6 pg/mL (normal range < 62.0 pg/mL), and IL-10 at 17.8 pg/mL (normal range < 9.1 pg/mL). Given the increased pulmonary infiltrates and the progressively elevated levels of inflammatory markers, intravenous antibiotic therapy was continued with moxifloxacin (0.4 g every day), but meropenem (1g every 8h) was switched to imipenem and cilastatin sodium (1g every 6h). On Day 2 of ICU hospitalization, C. abortus was detected with 2246 specific reads by mNGS tests of BALF (Figure 3A). Because human infection with C. abortus is rare, it was double-checked by PCR assay with a 178bp validation sequence (Figure 3B). Delightedly, the PCR products were confirmed as C. abortus by sanger sequencing (Figure 3C), which eventually confirmed the diagnosis of C. abortus pneumonia. Based on the results of mNGS and PCR, oral doxycycline (0.1g every 12h) in combination with intravenous azithromycin (0.5g every day) was administered. As chlamydia infection is typically a mixed infection, intravenous administration of imipenem and cilastatin sodium (1g every 6h) was continued. Over the next few days, there was a significant improvement in the patient’s symptoms and inflammation indicators (PCT [13.55 ug/L], IL-6 [26.3 pg/mL], IL-8 [82.2 pg/mL], and IL-10 [2.1 pg/mL]). The neuromuscular blocker was discontinued, and the dosage of norepinephrine was gradually down-regulated. There was also a significant improvement in pulmonary infiltrates as observed through chest X-ray (Figure 4), as well as a significant improvement in lung compliance. However, the patient’s liver function continued to deteriorate despite treatment, with serum total bilirubin of 506.36 μmol/L. On Day 4 of ICU hospitalization, the patient’s relatives made the difficult decision to forgo further treatment due to financial reasons. On December 15, 2021, the patient was weaned off ECMO and discharged with the result of arterial blood gases as follows: pH 7.44, PO2 112.8 mmHg, PCO2 34 mmHg, PO2/FiO2 282 mmHg, blood lactate 2.1 mmol/L. Unfortunately, just eight hours after being discharged, the patient passed away.
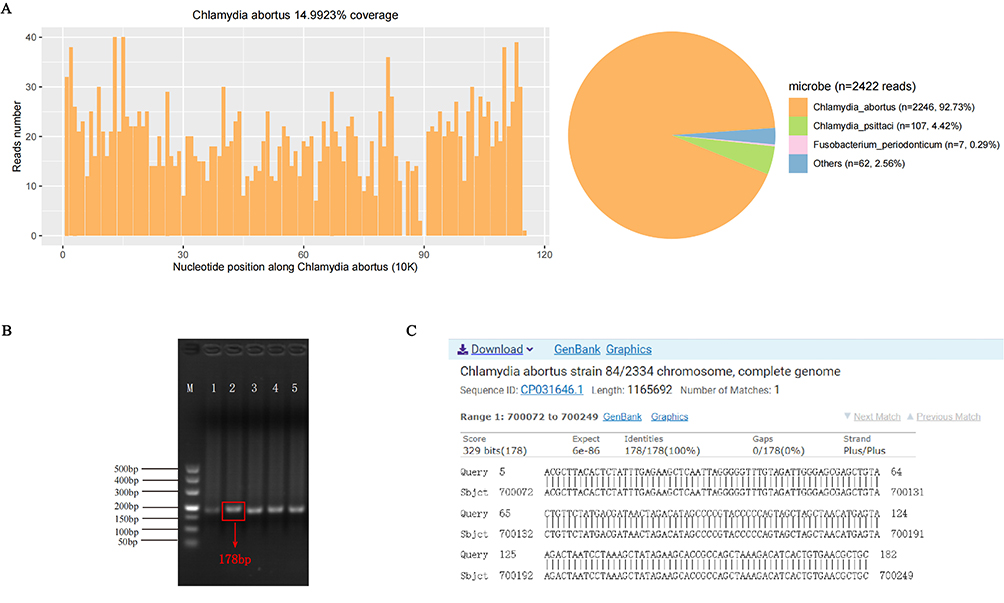 |
Figure 3 Diagnosis of Chlamydia abortus infection using mNGS test and following verification using PCR and sanger sequencing. (A) The unique mapping reads of C. abortus was 2246 with 14.99% genome coverage. (B) PCR detected 178 base-pair products in BALF sample with specific primers (for example, Primer 2, forward primer: ACGCTTACACTCTATTTGAGAAGCT, reverse primer: GCAGCGTTCACAGTGATGTCTT). (C) NCBI sequence alignment result. The “Query” lines indicate the sanger sequencing result of the PCR product, and the “Sbjct” lines show the reference sequence from NCBI database. The identity between the sequence obtained from Sanger sequencing and a reference C. abortus sequence (GenBank accession no. CP031646.1) was 100%. |
 |
Figure 4 Chest X-ray scans on the abnormality in lungs during the VV-ECMO support hospitalization. (A) Chest X-ray on the first day of VV-ECMO showed exudation, consolidation, and bilateral pleural effusion in both lungs, especially in the left lung. (B) Chest X-ray on the third day of VV-ECMO showed the exudation, consolidation, and bilateral pleural effusion were relieving than before. |
Discussion
To the best of our knowledge, this is the first reported case of a patient receiving ECMO treatment for C. abortus pneumonia. While C. abortus is a well-documented zoonotic pathogen that has been primarily associated with manifestation of abortion, stillbirth, or gestational septicaemia in pregnant women,10–13 it was no previously known to infect the human respiratory tract until Ortega et al5 reported the first atypical pneumonia related to C. abortus in Spain in 2016. Subsequent studies by Pichon et al6 in France in 2020, and more recently by Liu et al,9 Zhu et al,7 and Imkamp et al8 in China and Switzerland in 2022 revealed four additional cases of atypical pneumonia caused by C. abortus (Table 1). Fortunately, these cases were not life-threatening and patients finally recovered well because of timely diagnosis and correct antibiotic treatment, whereas our patient’s case of C. abortus infection was particularly severe resulting in rapid progression to severe ARDS and serious visceral complications. The timely administration of VV-ECMO treatment allowed for temporary rest of the patient’s lungs, which in turn provided the necessary time to clarify the diagnosis and ensure the effectiveness of antibiotic treatment. As a result, there was a significant improvement in the patient’s clinical symptoms and inflammation indicators. Our case demonstrates that C. abortus infection can be life-threatening, and ECMO plays an important role in the management of severe ARDS caused by rare pathogens. Until now, the source of human infection with C. abortus is unclear. According to studies of previously reported cases,3,5–8,14 it appears that most patients with C. abortus infection had a history of direct or indirect exposure to infected animals. Direct contact (infected animals or their products, contaminated aerosols or dust) and indirect contact (visiting or living on or near farms affected by endemic abortion) can all be the risk factors for infection.3 In the present case, the patient’s wife reported no typical direct exposure to infected animals or their products. Therefore, we suspect that the patient may have contracted the infection through an indirect mode of transmission.
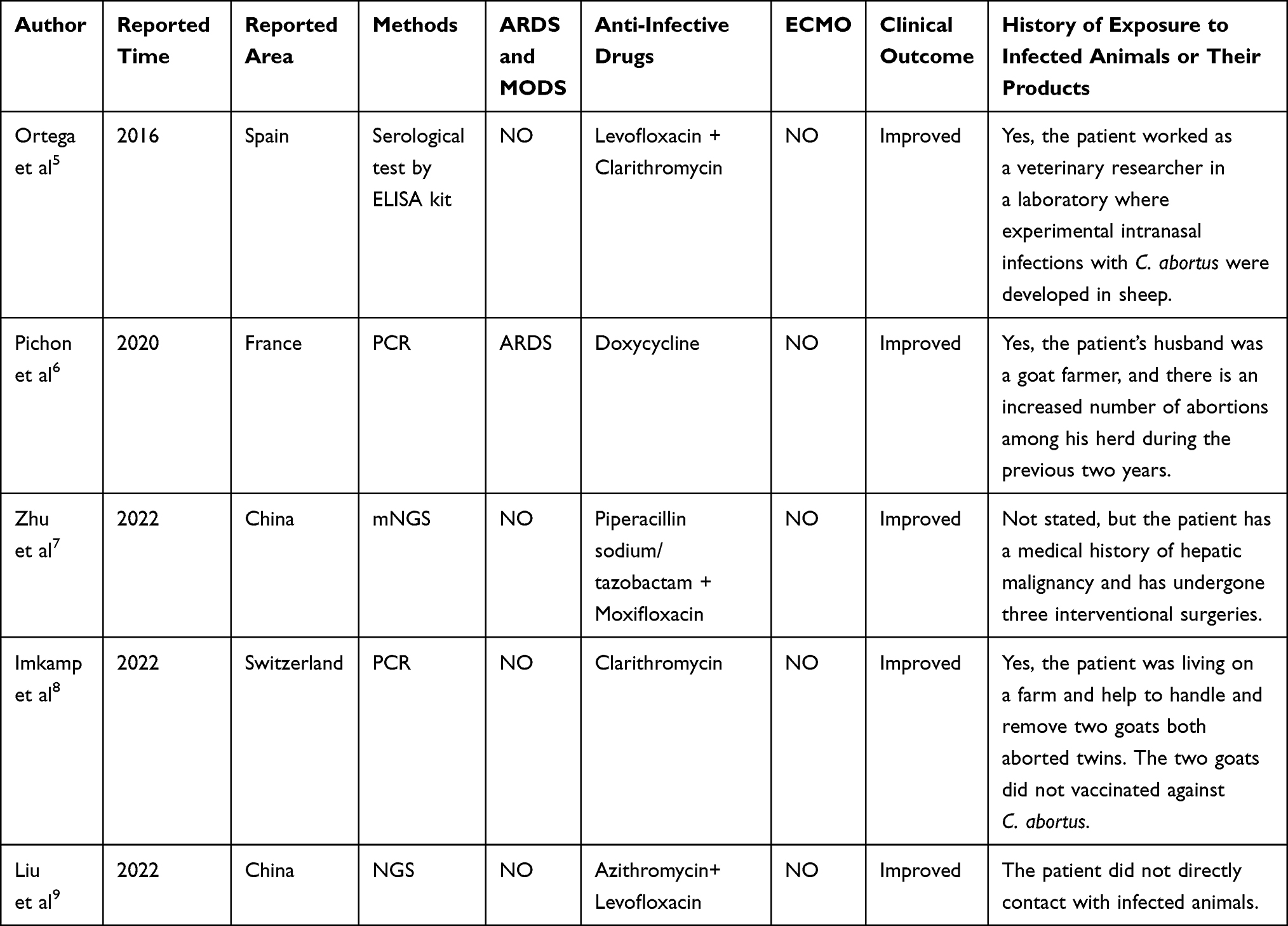 |
Table 1 Summary of Case Reports on Chlamydia abortus Pneumonia |
At present, there are no serological tests approved for the specific diagnosis of C. abortus infection in humans. Hence, PCR remains the primary method for diagnosing C. abortus infection.1 However, the molecular technique is a highly targeted test and requires several a priori assumptions. It is typically performed only in cases where clinicians suspect C. abortus infection.15 No pathogenic bacteria were found in sputum by traditional methods in our article, which made precision diagnosis and treatment challenging. mNGS is an unbiased method that can theoretically detect all pathogens of clinical samples and is especially suitable for novel, rare and atypical etiologies of complicated infectious diseases.16 Additionally, it is characterized by fast detection speed and its results are less affected by prior antibiotic exposure.17 Therefore, we performed mNGS and finally clarified that the pathogen was C. abortus in our patient. PCR was used to further verify the result. Interestingly, the first case of C. abortus pneumonia reported in China was also diagnosed via mNGS technology at an earlier time.7 Comparing with traditional methods, mNGS could be the most promising comprehensive diagnostic tool that is broadly applicable to rarely infectious disease diagnostics.
C. abortus infection can be a rare but severe and life-threatening disease as seen in our patient who developed MODS and deteriorated quickly. Therefore, correct and timely treatment is essential. Chlamydiae are generally susceptible to antibiotics that inhibit DNA and protein synthesis, including tetracyclines, macrolides and quinolones.18 There are no established treatment guidelines for C. abortus infections in humans so far. Since C. abortus was previously classified as a subspecies of C. psittaci, current treatment recommendations for C. psittaci have been used as a guide for treating C. abortus infections. Tetracycline antibiotics are the drug of perfect choice for C. psittaci infection in humans, with the oral dosage form for mild cases and intravenous injection recommended for severe cases.19 Among them, doxycycline is often considered the most effective treatment for various tropical diseases, zoonotic infections, and empiric treatment of undifferentiated febrile illnesses.14 Recent in vitro test suggested a possible therapeutic advantages of doxycycline on clearing C. abortus infection in epithelial cells.20 In addition, macrolide antibiotics are considered the best alternative agents in patients for whom tetracyclines are contraindicated. Macrolide drugs such as azithromycin have also been confirmed to be effective against C. psittaci in vitro.19,21 According to a report by Fang et al, omadacycline, a novel tetracycline, will be a new option for the treatment of severe C. psittaci infection due to its good safety profile and no requirement for dose adjustment in special populations.22 In some cases, quinolones are effective but are less effective compared to tetracyclines and macrolides.23 The patient presented in this study had initially been treated with meropenem and moxifloxacin, but his pulmonary function continued to deteriorate, indicating poor efficacy or insufficient treatment. Given the therapeutic options described in the literature, patient’s condition, and to prevent the possibility of mixed infection caused by chlamydia, we opted for a combination therapy of doxycycline and azithromycin along with imipenem and cilastatin sodium. Although this patient’s condition improved clinically and biologically, it was unfortunate that he had to be discharged for financial reasons and eventually passed away.
It is worth noting that this case has its limitations. Our review of a case series involving patients with C. abortus revealed that exposure to infected animals had played a significant role in the transmission of the disease. However, given the severity of our patient’s illness, we were unable to gather trustworthy epidemiological information through personal interaction. This raised the concern that his exposure history could have been overlooked. Furthermore, timely and accurate diagnosis, coupled with prompt treatment, resulted in a noticeable improvement in the patient’s clinical and biological condition. If his relatives decided to continue with the suggested treatment plan, there was a good chance he would be discharged from the hospital with a favorable prognosis.
Conclusion
Infections with C. abortus can result in severe ARDS and serious visceral complications which necessitate prompt diagnosis and active intervention by clinicians. The case highlights the significance of mNGS as an essential diagnostic tool for uncommon pathogens. Tetracyclines, macrolides or their combinations are effective choices for treatment of C. abortus pneumonia. Further study is needed to explore the transmission routes of C. abortus pneumonia and establish precise guidelines for antibiotic treatment.
Abbreviations
C. abortus, Chlamydia abortus; VV-ECMO, Venovenous extracorporeal membrane oxygenation; ARDS, Acute respiratory distress syndrome; CT, Computed tomography; PCT, Procalcitonin; BALF, Bronchoalveolar lavage fluid; mNGS, Metagenomic next-generation sequencing; PCR, Polymerase chain reaction; MODS, Multiple organ dysfunction syndrome; DNA, Deoxyribonucleic acid.
Data Sharing Statement
The dataset supporting the conclusions of this article is included in the article. Specific laboratory or imaging data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This case had obtained the consent of the Ethics Committee of Shunde Hospital, Southern Medical University (The First People's Hospital of Shunde Foshan) (Approval Number: KYLS20220606). Written informed consent was obtained from the patient’s relatives for publication of this case report.
Consent for Publication
Written informed consent for publication of case-related details and clinical images was obtained from the patient’s relatives.
Funding
This study was funded by the Scientific Research Start Plan of Shunde Hospital, Southern Medical University (The First People's Hospital of Shunde Foshan) (CRSP2022006).
Disclosure
The authors declare that they have no competing interests.
References
1. Turin L, Surini S, Wheelhouse N, Rocchi MS. Recent advances and public health implications for environmental exposure to Chlamydia abortus: from enzootic to zoonotic disease. Vet Res. 2022;53(1):37. doi:10.1186/s13567-022-01052-x
2. Pospischil A, Thoma R, Hilbe M, Grest P, Zimmermann D, Gebbers JO. Abort beim Menschen durch Chlamydophila abortus (Chlamydia psittaci serovar1) [Abortion in humans by Chlamydophila abortus (Chlamydia psittaci serovar 1)]. Schweiz Arch Tierheilkd. 2002;144(9):463–466. German.
3. Meijer A, Brandenburg A, de Vries J, Beentjes J, Roholl P, Dercksen D. Chlamydophila abortus infection in a pregnant woman associated with indirect contact with infected goats. Eur J Clin Microbiol Infect Dis. 2004;23(6):487–490.
4. Cheong HC, Lee CYQ, Cheok YY, Tan GMY, Looi CY, Wong WF. Chlamydiaceae: diseases in primary hosts and zoonosis. Microorganisms. 2019;7(5):64.
5. Ortega N, Caro MR, Gallego MC, et al. Isolation of Chlamydia abortus from a laboratory worker diagnosed with atypical pneumonia. Ir Vet J. 2015;69:8.
6. Pichon N, Guindre L, Laroucau K, Cantaloube M, Nallatamby A, Parreau S. Chlamydia abortus in Pregnant Woman with Acute Respiratory Distress Syndrome. Emerg Infect Dis. 2020;26(3):628–629.
7. Zhu C, Lv M, Huang J, et al. Bloodstream infection and pneumonia caused by Chlamydia abortus infection in China: a case report. BMC Infect Dis. 2022;22(1):181.
8. Imkamp F, Albini S, Karbach M, et al. Zoonotic Chlamydiae as rare causes of severe pneumonia. Swiss Med Wkly. 2022;152:w30102.
9. Liu M, Wen Y, Ding H, Zeng H. Septic shock with Chlamydia abortus infection. Lancet Infect Dis. 2022;22(6):912.
10. Walder G, Hotzel H, Brezinka C, et al. An unusual cause of sepsis during pregnancy: recognizing infection with chlamydophila abortus. Obstet Gynecol. 2005;106(5):1215–1217. doi:10.1097/01.AOG.0000161060.69470.9c
11. Pospischil A, Thoma R, Hilbe M, Grest P, Gebbers JO. Abortion in woman caused by caprine Chlamydophila abortus (Chlamydia psittaci serovar 1). Swiss Med Wkly. 2002;132(5–6):64–66.
12. Roberts W, Grist NR, Giroud P. Human abortion associated with infection by ovine abortion agent. Br Med J. 1967;4(5570):37.
13. Essig A, Longbottom D. Chlamydia abortus: new aspects of infectious abortion in sheep and potential risk for pregnant women. Curr Clin Microbiol Rep. 2015;2(1):22–34.
14. Burgener AV, Seth-Smith HMB, Kern-Baumann S, et al. A case study of zoonotic chlamydia abortus infection: diagnostic challenges from clinical and microbiological perspectives. Open Forum Infect Dis. 2022;9(10):ofac524.
15. Li N, Li S, Tan W, Wang H, Xu H, Wang D. Metagenomic next-generation sequencing in the family outbreak of psittacosis: the first reported family outbreak of psittacosis in China under COVID-19. Em microbes infect. 2021;10(1):1418–1428.
16. Goldberg B, Sichtig H, Geyer C, Ledeboer N, Weinstock GM. Making the leap from research laboratory to clinic: challenges and opportunities for next-generation sequencing in infectious disease diagnostics. mBio. 2015;6(6):e01888–15.
17. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240.
18. Kohlhoff SA, Hammerschlag MR. Treatment of Chlamydial infections: 2014 update. Expert Opin Pharmacother. 2015;16(2):205–212.
19. Balsamo G, Maxted AM, Midla JW, et al. Compendium of Measures to Control Chlamydia psittaci Infection Among Humans (Psittacosis) and Pet Birds (Avian Chlamydiosis), 2017. J Avian Med Surg. 2017;31(3):262–282.
20. Diensthuber D, Simnacher U, Peters S, Walther P, Essig A, Hagemann JB. Clearing Chlamydia abortus infection in epithelial cells and primary human macrophages by use of antibiotics and the MDM2-p53-inhibitor nutlin-3. Diagn Microbiol Infect Dis. 2022;103(3):115715.
21. Teng XQ, Gong WC, Qi TT, et al. Clinical analysis of metagenomic next-generation sequencing confirmed chlamydia psittaci pneumonia: a case series and literature review. Infect Drug Resist. 2021;14:1481–1492.
22. Fang C, Xu L, Tan J, Tan H, Lin J, Zhao Z. Omadacycline for the Treatment of Severe Chlamydia psittaci Pneumonia Complicated with Multiple Organ Failure: a Case Report. Infect Drug Resist. 2022;15:5831–5838.
23. Wang L, Shi Z, Chen W, Du X, Zhan L. Extracorporeal Membrane Oxygenation in Severe Acute Respiratory Distress Syndrome Caused by Chlamydia psittaci: a Case Report and Review of the Literature. Front Med. 2021;8:731047.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Metagenomic Next-Generation Sequencing Contributes to the Diagnosis of Pneumonia Caused by Chlamydia abortus in a Male Patient: Case Report and Literature Review
Gong F, Chen Z, Chang J, Liu J, Wang X, Mo W, Tan M, Jiang T
Infection and Drug Resistance 2023, 16:3463-3468
Published Date: 2 June 2023
Chlamydia Abortus-Induced Pneumonia with Psychiatric Symptoms and Pneumomediastinum: A Case Report
Ding B, Xu Z, Li Y, Ma Z
Infection and Drug Resistance 2025, 18:6999-7006
Published Date: 30 December 2025