Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Extracellular(Serum) Levels of Matrix Metalloproteinases in Pediatric Type 1 Diabetes Mellitus and Association with Diabetic Ketoacidosis and Cerebral Edema
Authors Xu Q, Yang Y, Huang Q, Xie L, Feng Y ![]() , Yang L
, Yang L ![]()
Received 6 December 2024
Accepted for publication 12 March 2025
Published 20 March 2025 Volume 2025:18 Pages 819—830
DOI https://doi.org/10.2147/DMSO.S507337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mark D. DeBoer
Qingbo Xu,1,2 Yu Yang,1,2 Qiang Huang,1– 3 Liling Xie,1,2 Yaqin Feng,1,2 Li Yang1,2
1Department of Endocrinology, Jiangxi Provincial Children’s Hospital, Nanchang, Jiangxi, 330038, People’s Republic of China; 2The Affiliated Children’s Hospital of Nanchang Medical College, Nanchang, Jiangxi, 330038, People’s Republic of China; 3Jiangxi Medical College, Nanchang University, Nanchang, 330006, People’s Republic of China
Correspondence: Li Yang, Email [email protected]
Background: Type 1 diabetes mellitus (T1DM) in children is associated with acute complications such as diabetic ketoacidosis (DKA) and the severe risk of diabetic ketoacidosis-related cerebral edema (DKACE). Matrix metalloproteinases (MMPs) are implicated in inflammation and tissue remodeling, potentially contributing to these complications. This study explores the role of MMPs as biomarkers in pediatric T1DM patients with DKA and DKACE.
Methods: We conducted a systematic cross-sectional study at Jiangxi Children’s Hospital, enrolling 56 pediatric patients with T1DM, categorized into three groups: T1DM without complications, DKA, and DKACE. Serum levels of MMP-2, MMP-3, and MMP-9 were measured through ELISA. Statistical analyses assessed correlations between MMPs, glucose metabolism, and inflammatory markers, evaluating potential biomarker utility in disease characterization.
Results: MMP-3 and MMP-9 levels were significantly elevated in the DKACE group compared to the T1DM and DKA groups, exhibiting strong correlations with decreased pH and bicarbonate levels (both p < 0.001). MMP-2 levels were reduced in DKACE, correlating positively with pH and bicarbonate levels. Post-clinical improvement analyses demonstrated no significant differences in MMP levels between DKA and DKACE groups, suggesting stabilization post-treatment regardless of initial acidosis severity.
Conclusion: The distinct patterns of MMP-3 and MMP-9 elevations in DKACE highlight their potential as biomarkers for identifying and monitoring severe DKA complications. The findings suggest these enzymes play a significant role in cerebral edema pathophysiology, making them viable targets for future therapeutic interventions.
Keywords: pediatric diabetic ketoacidosis, cerebral edema, matrix metalloproteinases, type 1 diabetes mellitus
Graphical Abstract:
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune disease that destroys insulin-producing beta cells, causing poor glucose control and risking complications like diabetic ketoacidosis (DKA) and diabetic ketoacidosis-related cerebral edema (DKACE). As an acute complication marked by insulin deficiency, DKA presents both immediate and long-term health risks. Cerebral edema (CE) is a formidable complication that may affect 0.5–1% of pediatric patients suffering from DKA. This complication carries a grave prognosis, with mortality rates reaching as high as 50–60%. Beyond mortality, the potential for significant damage to the central nervous system in survivors poses a substantial clinical challenge.1 These acute complications pose significant clinical challenges and contribute to increased morbidity and potential mortality in the pediatric population. Understanding the pathophysiological mechanisms underlying these complications is essential for improving patient outcomes and developing targeted therapeutic strategies.
Matrix metalloproteinases (MMPs), a family of zinc-dependent endopeptidases, are recognized for their role in the degradation of extracellular matrix components. Recent studies have implicated MMPs in various pathological processes, including inflammation, tissue remodeling, and vascular permeability, suggesting their potential involvement in the exacerbation of T1DM complications.2,3 The role of MMPs in such pathophysiological states is increasingly recognized for their ability to disrupt the function of cerebral vascular endothelial barriers and degrade extracellular matrix components. Inflammatory and oxidative stress responses are exacerbated by MMP activity, which can further propagate brain injury and complicate the clinical picture of DKA.4 Research has underscored alterations in the balance between MMPs and their endogenous inhibitors, tissue inhibitors of metalloproteinases (TIMPs), in various inflammation-related diseases, including sepsis.5,6 MMPs have the potential to impair the function of the cerebral vascular endothelial barrier and degrade extracellular matrix components. Their overexpression and dysregulation are closely associated with DKA.7 Notably, MMP-2, MMP-3, and MMP-9 have been highlighted in the context of neuroinflammation and blood-brain barrier disruption, both of which are critical factors in the development of cerebral edema. As proteolytic enzymes, MMPs are released predominantly by leukocytes during inflammatory states and are key mediators in the subsequent inflammatory and oxidative processes that can lead to cerebral injury.8 However, the correlation between MMPs and DKACE remains unclear.
This study was designed to explore the correlation between MMP levels and the clinical spectrum of T1DM complications in children. Through a comprehensive biochemical analysis, we aimed to elucidate the correlations between MMP levels, glucose metabolism, and inflammatory markers, providing insights into the pathophysiology of T1DM complications. Furthermore, we assessed the dynamics of MMP expression post-clinical intervention, contributing to the understanding of their role in disease stabilization and recovery in affected children. The findings from this study underscore the clinical relevance of MMPs in pediatric diabetes management and offer a foundation for future research into therapeutic interventions targeting these proteolytic enzymes.
Materials and Methods
Participants
The selection criteria adhered strictly to the 2020 Expert Consensus Guidelines on Type 1 Diabetes in Chinese Children. These guidelines provide comprehensive criteria ensuring uniformity and precision in the diagnosis and classification of T1DM and its related complications, facilitating robust and reliable data collection for this study.9 The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Jiangxi Children’s Hospital Ethics Committee (Ethics Approval No: JXSETYY-YXKY-20240117). Prior to the commencement of the study, written informed consent was obtained from the parents or legal guardians of all participating subjects, ensuring their comprehensive understanding of the study’s purpose, procedures, potential risks, and benefits.
Study Design
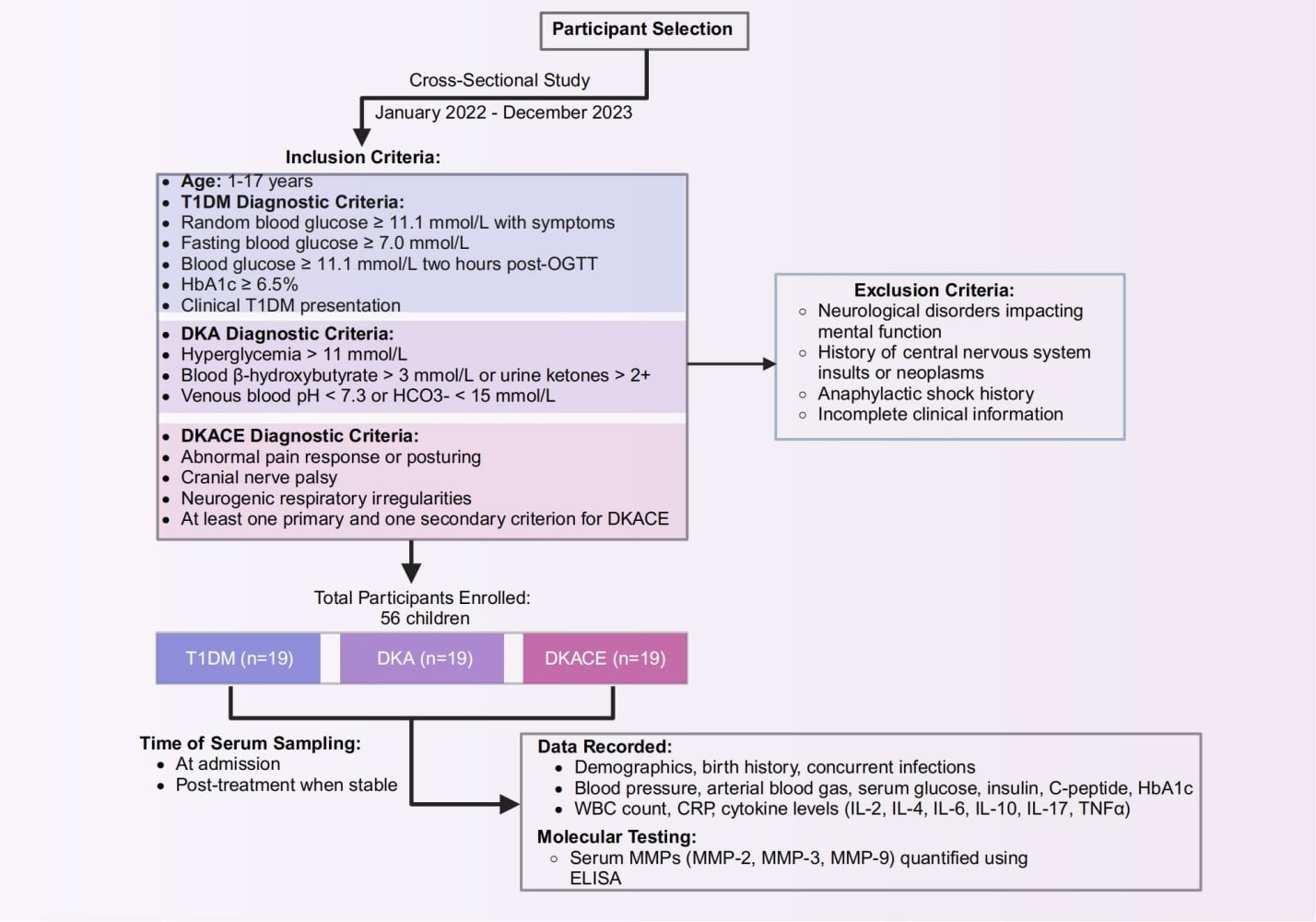
This study was systematically designed to investigate the biochemical and clinical parameters in pediatric patients with T1DM and associated complications, with a particular focus on the role of matrix metalloproteinases. Conducted as a cross-sectional study, it took place at Jiangxi Children’s Hospital over a span extending from January 2022 to December 2023. Based on an estimated effect size from previous studies examining the role of matrix metalloproteinases in diabetic complications and cerebral edema, and using a power of 80% and a significance level of 0.05, the minimum sample size was calculated to be 45 participants. A total of 56 children were enrolled, classified into three distinct groups based on their clinical conditions: those diagnosed with T1DM (n = 19), children experiencing Diabetic Ketoacidosis (DKA, n = 17), and those suffering from Diabetic Ketoacidosis-Related Cerebral Edema (DKACE, n = 20). Participants were recruited from various hospital departments, including the Departments of Endocrinology, Genetics, and Metabolism, as well as the Pediatric Intensive Care Unit (PICU).
Inclusion and Exclusion Criteria
Participants were deemed eligible for inclusion in this study based on established diagnostic criteria for T1DM, DKA, and DKACE. The recruitment process adhered to the following inclusion guidelines:
T1DM Diagnostic Criteria9 (Participants were included if they satisfied at least one of the following criteria): 1. A random blood glucose level ≥11.1 mmol/L, in conjunction with typical diabetes-related symptoms and signs. 2. A fasting blood glucose level ≥7.0 mmol/L. 3. A blood glucose level of ≥11.1 mmol/L two hours post-administration of an oral glucose tolerance test (1.75 g/kg body weight of glucose, up to a maximum of 75 g). 4. A Hemoglobin A1c (HbA1c) level ≥6.5%, determined using a method standardized by the National Glycohemoglobin Standardization Program. 5. Clinical presentation consistent with T1DM subtype characteristics, including rapid onset, potential ketoacidosis; initial C-peptide levels below the normal range or detection limit; and positive serology for at least one of the following autoantibodies: glutamic acid decarboxylase (GAD65), insulinoma-associated antigen-2 (IA-2), ZnT8 transporter, or insulin antibodies. 6. Age at enrollment between 1 to 17 years, accompanied by comprehensive clinical data availability.
DKA Diagnostic Criteria:10 1. Hyperglycemia, characterized by a blood glucose level >11 mmol/L. 2. Presence of ketone bodies, indicated by blood β-hydroxybutyrate >3 mmol/L or urine ketones >2+. 3. Acidosis, defined by a venous blood pH <7.3 or serum bicarbonate (HCO3-) level <15 mmol/L.
DKACE Diagnostic Criteria:9 1. Abnormal motor or verbal responses elicited by pain. 2. Presence of decorticate or decerebrate posturing. 3. Cranial nerve palsy, notably involving cranial nerves III, V, or VI. 4. Neurogenic respiratory irregularities, including snoring, tachypnea, Cheyne–Stokes respiration, or apnea. Primary Criteria: 1. Incontinence of urine or feces that is not age-appropriate. 2. Altered level of consciousness. 3. Sustained reduction in heart rate by more than 20 beats per minute, not associated with sleep or resuscitation activities. Secondary Criteria: 1. Episodes of vomiting. 2. Headaches. 3. Drowsiness increasing difficulty in arousal. 4. Age less than 5 years. 5. Diastolic blood pressure exceeding 90 mmHg. For a diagnosis of DKACE, participants were required to meet at least one diagnostic criterion and one primary criterion or one primary criterion and two secondary criteria.
Participants were excluded if they had: 1. Neurological disorders impacting mental function. 2. A history of central nervous system insults or neoplasms. 3. Anaphylactic shock history. 4. Incomplete clinical information.
Data Collection and Clinical Assessment
Comprehensive demographic and clinical data were collected upon admission, including gender, age, birth history (full-term or preterm), presence of concurrent infections, and duration of illness. Vital statistics such as systolic and diastolic blood pressure were recorded. Laboratory analyses included arterial blood gas values, serum glucose, insulin, C-peptide levels, HbA1c, white blood cells count, C-reactive protein (CRP), and cytokines including interleukins IL-2, IL-4, IL-6, IL-10, IL-17, and tumor necrosis factor-alpha (TNFα).
Quantification of Matrix Metalloproteinases
Serum levels of matrix metalloproteinases (MMP-2, MMP-3, and MMP-9) were quantified using enzyme-linked immunosorbent assay (ELISA) kits procured from Wuhan Boster Biological Engineering Co., Ltd. Blood samples, each with a volume of 4 mL, were collected from the patients’ veins at the time of admission and following the completion of treatment, once the patient’s condition was deemed stable MMP-9 was chosen for analysis due to its critical involvement in the degradation of the extracellular matrix and its known association with blood-brain barrier disruption. The collected blood samples were centrifuged to separate the serum, which was then used for subsequent analysis.
Statistical Analysis
Data analysis was conducted using SPSS version 27.0. For continuous variables that followed a normal distribution, the means and standard deviations were calculated. Independent samples t-tests were used to compare two groups, while one-way ANOVA was applied for comparisons among three or more groups. For variables not following a normal distribution, data were expressed as medians and interquartile ranges. The Mann–Whitney U-test was utilized for comparing two groups, and the Kruskal–Wallis Rank Sum Test was employed for three or more groups. Categorical data were presented as percentages. Correlations between laboratory and clinical markers were explored using either Spearman correlation test or Pearson’s correlation test, to ensure a comprehensive analysis of significant variables. A P-value of less than 0.05 was considered indicative of statistically significant differences or associations across all tests.
Results
Baseline Characteristics of Study Subjects
The study included a total of 56 pediatric patients, categorized into three groups: T1DM without acute complications (n = 19), DKA without cerebral edema (n = 17), and DKACE (n = 20). The baseline characteristics of the participants are detailed in Table 1. The median age of the entire cohort was 9.61 years, with no significant difference observed among the T1DM, DKA, and DKACE groups (p = 0.54). The gender distribution was fairly balanced across all groups, with females representing 57.14% of the total population. The distribution of females in each group was as follows: T1DM (52.63%), DKA (64.71%), and DKACE (55.00%). This variation did not reach statistical significance (p = 0.74). Birth history analysis revealed that the majority of participants, 85.71%, were born full-term, while a small percentage were born prematurely (8.93%) or overdue (5.36%). The proportions were similar across the study groups, with no significant differences detected (p = 0.67). The duration of illness prior to study entry displayed considerable variation, with a median of 18 days [IQR: 7.00, 129.50] for the full cohort. Individual group medians were 31 days for T1DM, 30 days for DKA, and 14 days for DKACE, yet these differences did not achieve statistical significance (p = 0.39). Infection status at admission was present in 55.36% of patients overall, with greater incidence observed in the DKACE group (70.00%), compared to T1DM (42.11%) and DKA (52.94%). However, this difference was not statistically significant (p = 0.21). Mean systolic blood pressure was recorded at 110.00 mmHg [IQR: 99.75, 124.25] across all participants. The systolic blood pressures were 106.00 mmHg, 116.00 mmHg, and 105.00 mmHg for the T1DM, DKA, and DKACE groups, respectively (p = 0.23). Diastolic blood pressure averaged 70.38 mmHg (SD = 11.81) for the complete cohort; while the readings were slightly higher in the DKA group, these differences were not statistically significant (p = 0.28). Overall, the baseline characteristics among the three groups were largely comparable, with no statistically significant differences noted in terms of age, gender, birth history, duration of illness, infection status on admission, or blood pressure measurements.
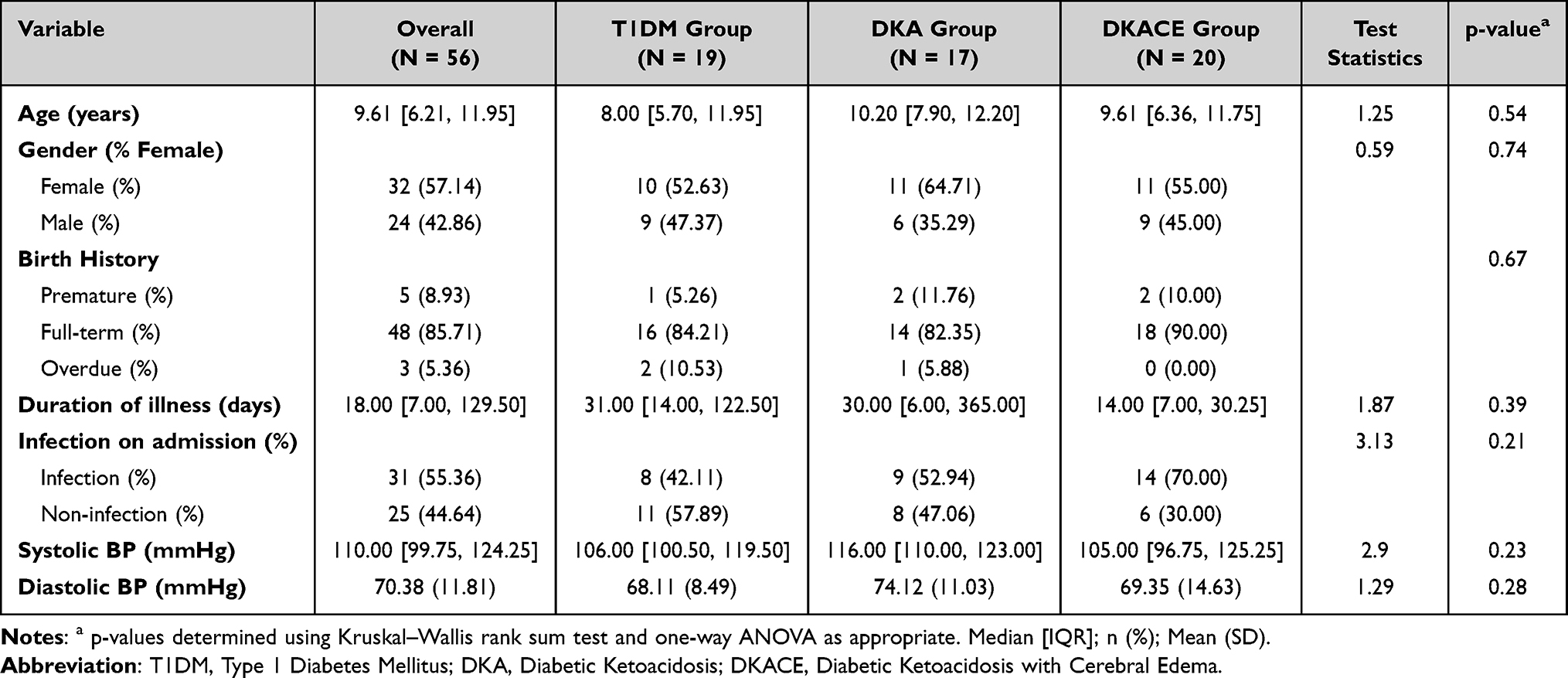 |
Table 1 Baseline Characteristics of Study Participants |
Biochemical Indicator Comparisons
The detailed comparison of laboratory indicators across the three patient groups is presented in Table 2. The analysis reveals significant differences in several biochemical markers, notably related to glucose metabolism and inflammatory responses. Blood glucose levels were significantly elevated in the DKA Group and DKACE Group compared to the T1DM Group, with medians of 23.90 mmol/L [20.56, 29.00] and 28.50 mmol/L [26.63, 34.17], respectively, versus 5.03 mmol/L [4.73, 5.74] in the T1DM group (p < 0.001). Similarly, glycated hemoglobin (HbA1c) percentages were markedly higher in the DKA and DKACE groups (12.40% [11.70, 13.90] and 13.90% [12.10, 14.70], respectively) compared to the T1DM group (5.74% [4.98, 6.26]) with a highly significant p-value of <0.001. The inflammatory markers exhibited distinct patterns across the groups. WBC counts, IL-2, IL-6, and TNF-α levels were significantly elevated in the DKACE Group compared to other groups, indicating a heightened inflammatory response associated with cerebral edema during DKA. The WBC count reached 21.04 × 10^9/L [9.63, 25.19] in the DKACE group (p < 0.001), underscoring the inflammatory nature of this condition. MMPs displayed distinct trends between groups, emphasizing their potential link with cerebral edema. MMP-2 levels were markedly lower in the DKACE Group at 0.83 ng/mL [0.42, 2.68] compared to the T1DM and DKA groups (p < 0.001) (Table 2 and Figure 1A). Conversely, MMP-3 and MMP-9 levels were highest in the DKACE Group, recording values of 29.28 ng/mL [26.04, 33.64] and 23.55 ng/mL (3.38), respectively, indicating a potential correlation between elevated MMP levels and the presence of cerebral edema (p < 0.001 for both) (Table 2, Figure 1B and C). The analysis points towards significant variations in glucose metabolism, inflammatory profiles, and MMP levels among the groups, with high MMP-3 and MMP-9 levels correlating with DKA-related cerebral edema.
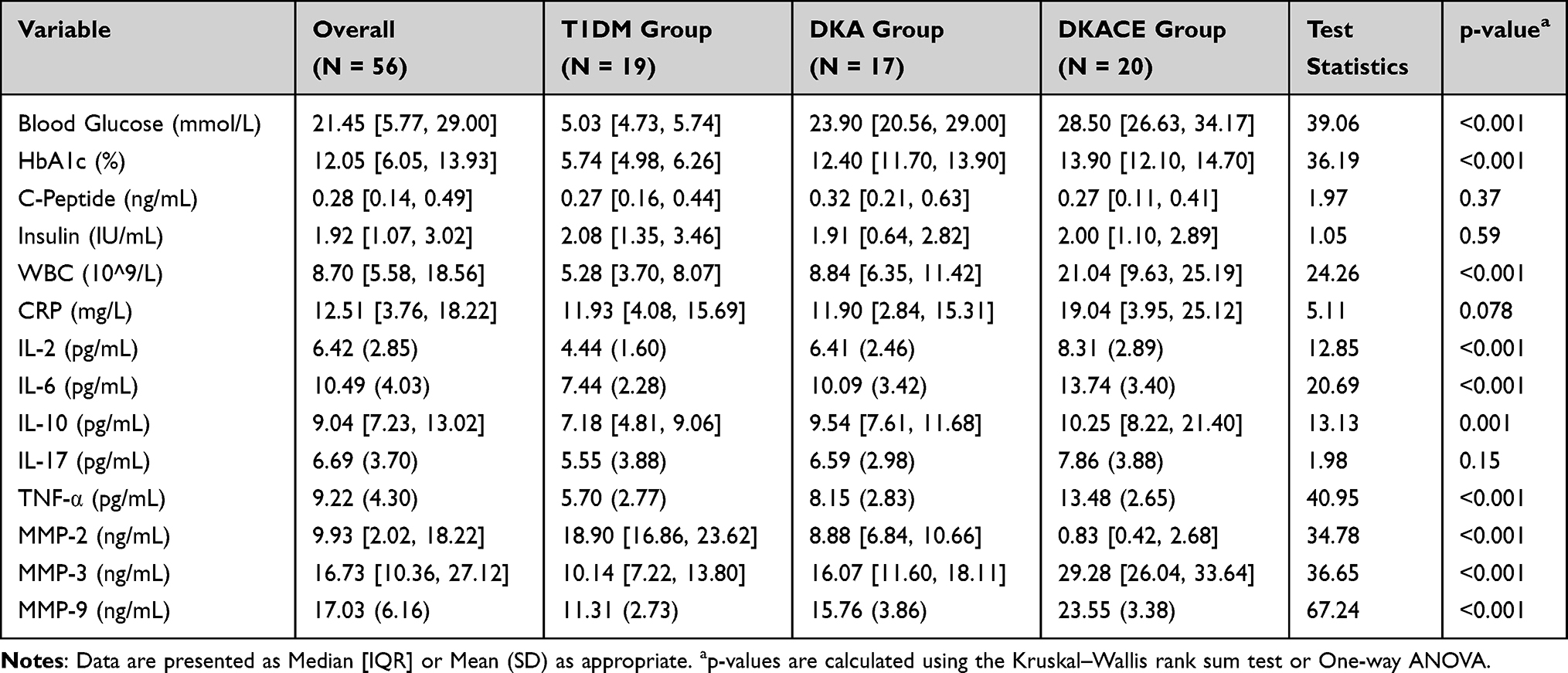 |
Table 2 Laboratory Indicator Comparison Across Three Patient Groups |
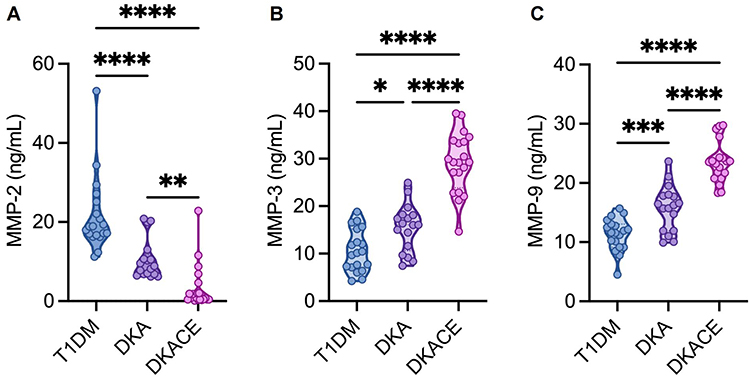 |
Figure 1 Expression Levels of MMPs in Serum of Children with T1DM, DKA, and DKACE. (A) MMP-2 expression levels in serum of children with T1DM, DKA, and DKACE. (B) MMP-3 expression levels in serum of children with T1DM, DKA, and DKACE. (C) MMP-9 expression levels in serum of children with T1DM, DKA, and DKACE. Statistical analysis was performed using one-way ANOVA. * denotes P<0.05; **denotes P<0.01; ***denotes P<0.001; ****denotes P<0.0001. |
Correlation of MMP Levels with Blood Parameters and Inter-MMPs
Figure 2A presents a heatmap showcasing the expression levels of MMP-2, MMP-3, MMP-9, pH, and bicarbonate (HCO3-) across different patient groups. T1DM patients prominently exhibit higher MMP-2 levels. Conversely, DKACE patients show elevated levels of MMP-3 and MMP-9 compared to DKA and T1DM groups. Interestingly, DKACE patients have decreased levels of HCO3- and pH. As shown in Figure 2B, a Spearman correlation heatmap indicates the correlations among MMPs and blood chemistry parameters (Supplementary Tables 1–2). MMP-3 and MMP-9 exhibit a strong positive correlation (r = 0.986, p < 0.0001), and both inversely correlate significantly with pH (MMP-3: r = −0.941, MMP-9: r = −0.959, both p < 0.0001) and HCO3- (MMP-3: r = −0.763, MMP-9: r = −0.784, both p < 0.0001). In contrast, MMP-2 correlates positively with pH (r = 0.608, p < 0.0001) and HCO3- (r = 0.444, p = 0.0006), highlighting differential interaction dynamics with MMP-3 and MMP-9. Figure 2C illustrates the correlation between MMP-2 and MMP-3 levels within patient groups. While no significant correlation is found in T1DM patients, a strong positive linear correlation is evident in DKA (r = 0.8649, p < 0.0001) and DKACE (r = 0.6252, p = 0.0032) patients, especially pronounced in DKA patients. In Figure 2D, consistent with previous observations, T1DM patients exhibit no significant correlation between MMP-2 and MMP-9 levels, whereas DKA (r = 0.8793, p < 0.0001) and DKACE (r = 0.7053, p = 0.0005) patients show strong positive correlations, most notably in DKA patients. Figure 2E further demonstrates the robust positive correlations between MMP-3 and MMP-9 across all patient groups, with significant linear correlations in T1DM (r = 0.9379, p < 0.0001), DKA (r = 0.9937, p < 0.0001), and DKACE (r = 0.9435, p < 0.0001) patients. In summary, Figure 2 suggests differential MMP expression profiles and correlations with blood pH and HCO3- levels in pediatric diabetes patients. The findings indicate that MMP-3 and MMP-9 play a more intertwined role in DKA and DKACE, particularly linked to lower pH and bicarbonate levels, which may be critical in understanding DKA-related cerebral edema pathophysiology.
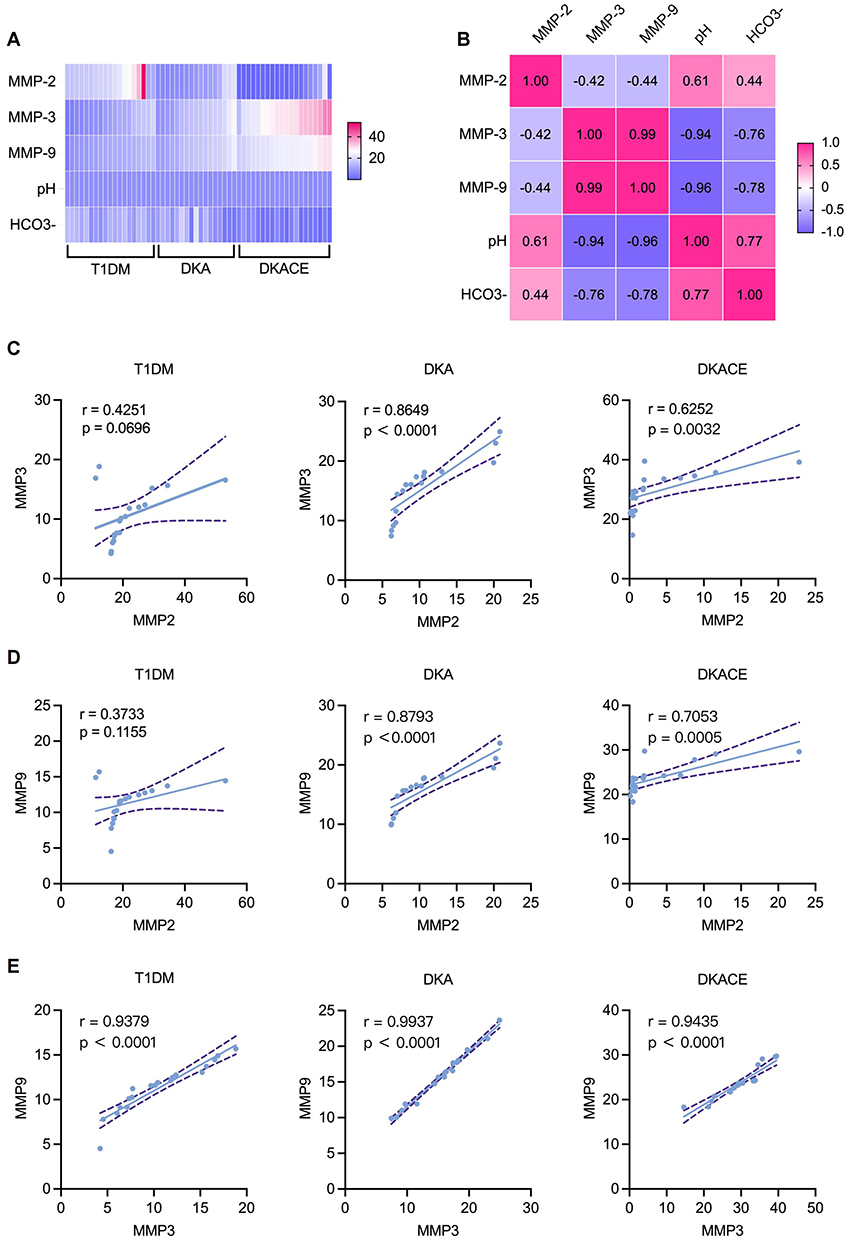 |
Figure 2 Correlation of MMP Levels with Blood Parameters. (A) Heatmap illustrating the expression levels of MMP-2, MMP-3, MMP-9, pH, and bicarbonate (HCO3-) across different patient groups. MMP levels are depicted by color gradients: red indicates levels above 40 ng/mL, white represents levels between 20–40 ng/mL, and blue denotes levels below 20 ng/mL. (B) Spearman correlation heatmap showing correlations among MMPs and blood chemistry parameters in all patients. (C) Correlation between MMP-2 and MMP-3 levels within T1DM, DKA, and DKACE patient groups. (D) Correlation between MMP-2 and MMP-9 levels. (E) Correlation between MMP-3 and MMP-9 levels. |
Comparison of MMP-2, MMP-3, and MMP-9 Levels Post-Clinical Improvement
In this section, we analyzed the post-clinical improvement levels of MMPs - specifically MMP-2, MMP-3, and MMP-9 - in pediatric patients with DKA and those with DKACE. These analyses aimed to investigate potential differences in MMP levels that could underpin cerebral edema development. The results are summarized in Table 3. The median post-improvement level of MMP-2 in the DKACE group (1.65 ng/mL, IQR: 1.28, 4.84) was higher than that in the DKA group (1.38 ng/mL, IQR: 1.04, 2.65). However, this difference did not reach statistical significance (P = 0.563), indicating that MMP-2 levels did not significantly differ between the groups after clinical improvement. Similarly, MMP-3 levels were slightly elevated in the DKACE group (median 3.36 ng/mL, IQR: 1.61, 6.16) compared to the DKA group (median 2.93 ng/mL, IQR: 1.54, 3.98), yet this difference was not statistically significant (P = 0.52). With respect to MMP-9, the median level was similar between the DKACE group (5.42 ng/mL, IQR: 3.72, 6.39) and the DKA group (5.34 ng/mL, IQR: 2.79, 5.97). The P-value for this comparison was 0.739, suggesting no significant disparity in MMP-9 levels post-clinical improvement. Overall, the comparative analysis of MMP levels in DKA and DKACE pediatric patients after clinical recovery did not reveal significant differences in the concentrations of MMP-2, MMP-3, and MMP-9. These observations suggest a universal stabilization of MMP levels post-intervention, irrespective of the initial severity of acidosis. This detailed exploration of MMP behavior post-stabilization underpins their utility as clinical biomarkers, potentially offering valuable insights into the severity and progression of diabetic conditions during and post clinical interventions.
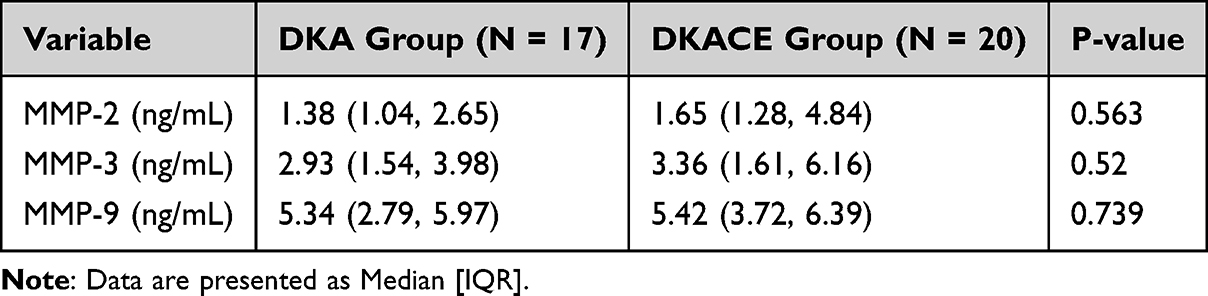 |
Table 3 Comparison of MMP-2, MMP-3, and MMP-9 Levels Post-Clinical Improvement |
Discussion
In this cross-sectional study, we investigated the involvement of MMPs in pediatric patients with T1DM and its acute complications, notably DKA and DKACE. Our findings reveal significant differences in serum MMP-2, MMP-3, and MMP-9 levels among T1DM, DKA, and DKACE groups. Notably, MMP-3 and MMP-9 were elevated in DKACE patients, suggesting a potential role in cerebral edema pathophysiology. The post-treatment analysis indicated normalization of MMP levels, supporting their potential as acute-Phase Inflammatory markers.
Our study aligns with reports indicating that approximately 30% of children with T1DM may experience DKA,11 and 1% of these cases could further develop cerebral edema if untreated.12 Previous studies support the increased incidence of infections in DKA and DKACE cases, echoing our findings where infection rates were higher at the time of admission in these groups.13 Additionally, current literature underscores the neuroinflammatory processes associated with DKACE, which our study corroborated by highlighting the involvement of various inflammatory markers and cytokines in these patients.14,15
From a pathophysiological standpoint, DKA is characterized by inflammatory responses and chemokine secretion, facilitating leukocyte adhesion to cerebral vessels, potentially leading to endothelial dysfunction and instability.16 Previous research has emphasized the pivotal role of MMPs and inflammatory cytokines in exacerbating these conditions.17,18 Our study identified elevated white blood cell counts and increased levels of pro-inflammatory cytokines such as IL-2, IL-6, and TNF-α in the DKACE group, aligning with existing literature that denotes an activated inflammatory response in these patients,19,20 suggesting the activation of inflammation-related factors in diabetic patients.21,22 Additionally, IL-17 enhances the production of pro-inflammatory cytokines (TNF-α, IL-1β, and IL-6), potentially increasing free radicals and inducing β-cell destruction.23 Arif et al24 found a significant increase in IL-17 expression in the pancreas of newly diagnosed T1DM patients. Moreover, treatment with IL-17 neutralizers can prevent T1DM development in NOD mice and inhibit the formation of anti-GAD65 autoantibodies.25 In this study, the elevated IL-17 levels in DKACE patients, while not statistically significant, further hint at the inflammatory milieu present in severe DKA cases.23
In comparing our results to current literature, we noted similar patterns regarding the involvement of MMP-3 and MMP-9 in neuroinflammatory and cerebrovascular permeability alterations.3,4 Our results show that levels of MMP-3, and MMP-9 are higher in patients of the DKACE group compared to T1DM and DKA groups, and these levels are negatively correlated with pH and HCO3- values. Research suggests that MMPs may exacerbate inflammatory responses, with acidic pH directly stimulating the induction and release of cellular MMPs.26,27 Abdul Y et al28 found that serum MMP-3 could serve as a biomarker for cerebral microvascular changes in diabetic patients, with high expression induced in endothelial cells and astrocytes during hyperglycemia. Further studies29 highlights the role of MMP-3 in neural cell death under hypoxic conditions. Additionally, a prior study reported that tissues with abundant leukocytes exhibit more pronounced MMP-3 activity, posing as a main factor in brain tissue damage.30 Glaser N et al31 observed that serum and brain tissue MMP-9 concentrations significantly increase during acute DKA in juvenile rats and decrease 24 hours post-DKA, aligning with our study outcomes. Acute hyperglycemia has also been associated with increased serum MMP-9 levels.32 However, our study diverges from some reports by showing a decrease in MMP-2 levels in DKACE patients, contrary to findings positing its upregulation in inflammatory scenarios.33 Garro A34 reported lower circulating MMP-2 levels in early DKA children compared to diabetic controls. Our post-treatment analyses, conducted once clinical stability was achieved, revealed attenuated MMP levels, reinforcing the notion of MMP upregulation during acute phases, with subsequent normalization upon inflammation resolution, as seen in other studies.5,6 These observations reinforce the hypothesis of transient MMP upregulation during acute phases, followed by normalization upon inflammation resolution.
This study boasts several strengths, including a robust design with clearly defined patient groups and stringent inclusion criteria based on expert consensus guidelines. Our inclusion of various biochemical markers allowed for a comprehensive assessment of inflammatory responses and metabolic derangements across T1DM, DKA, and DKACE. However, limitations include the relatively small sample size, potentially limiting generalizability, and the single-center study setting, which may introduce regional biases. Additionally, the cross-sectional design precludes causal inferences regarding MMP involvement in T1DM complications. The current study sheds light on the serum levels of MMPs and their association with diabetic complications such as DKA and DKACE. While MMPs have been implicated in the pathophysiology of BBB disruption, this study did not include specific BBB permeability markers such as monomeric transthyretin, albumin, plasminogen, and fibrinogen. These markers could potentially offer deeper insights into the mechanisms of BBB dysfunction and its relationship with MMPs. Therefore, we suggest that future studies could benefit from integrating these markers to provide a more comprehensive understanding of BBB integrity in pediatric T1DM and its associated complications.
Limitations of the Study and Future Scope
While serum markers such as MMPs provide valuable insights into the biochemical status of patients, it is important to acknowledge that cerebrospinal fluid (CSF) analysis could potentially offer a deeper understanding of the role of these enzymes in central nervous system complications. CSF samples would allow for a direct assessment of the local inflammatory processes, which might not be fully reflected in serum levels. However, due to ethical constraints and the invasive nature of lumbar puncture, CSF analysis was not feasible within the scope of this study. Thus, the findings presented here are based on serum markers, which, while informative, may not entirely capture the complex interplay of systemic and central nervous system inflammation in pediatric T1DM patients with complications like DKA and DKACE. Moreover, tissue inhibitor of metalloproteinases 1 (TIMP-1), a key regulator of MMP activity, was not included in the current study due to resource limitations and sample size constraints. It is planned to be analyzed in future studies to better understand the MMP/TIMP balance in DKA and cerebral edema pathology. Future studies will incorporate additional markers such as monomeric transthyretin, albumin, plasminogen, and fibrinogen to evaluate their role in BBB permeability. Furthermore, we propose to explore more specific BBB integrity assessments to enhance the accuracy of diagnosing and predicting complications like DKACE. We also acknowledge the limitations of this study, particularly the small sample size for PCT detection. These markers will be explored in future research to establish their potential as biomarkers for BBB integrity and cerebral edema in pediatric T1DM patients. Finally, research into the underlying molecular mechanisms linking MMP dysregulation to endothelial dysfunction and blood-brain barrier disruption in diabetic complications would significantly advance our understanding of these pathological processes.
Conclusion
In conclusion, our study highlights significant shifts in MMP levels among pediatric T1DM patients with acute complications, particularly emphasizing the role of MMP-3 and MMP-9 in DKACE. These findings underscore their potential as biomarkers and therapeutic targets in managing DKA-related cerebral edema, aiming to improve clinical outcomes in pediatric diabetes care. The absence of significant post-stabilization differences in MMP levels suggests an eventual convergence towards homeostasis, marking their potential utility in assessing treatment efficacy. However, further extensive research is crucial to unravel the intricate interactions between MMPs and clinical outcomes in DKA, guiding future therapeutic interventions and optimizing management of pediatric diabetic complications.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Jiangxi Children’s Hospital Ethics Committee (Ethics Approval No: JXSETYY-YXKY-20240117). Prior to the commencement of the study, written informed consent was obtained from the parents or legal guardians of all participating subjects, ensuring their comprehensive understanding of the study’s purpose, procedures, potential risks, and benefits.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jiangxi Provincial Health Commission Science and Technology Plan (No. SKJP220212334).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Tzimenatos L, Nigrovic LE. managing diabetic ketoacidosis in children. Ann Emerg Med. 2021;78(3):340–345. doi:10.1016/j.annemergmed.2021.02.028
2. Sato M, Hwang DM, Guan Z, et al. Regression of allograft airway fibrosis: the role of MMP-dependent tissue remodeling in obliterative bronchiolitis after lung transplantation. The American Journal of Pathology. 2011;179(3):1287. doi:10.1016/j.ajpath.2011.05.032
3. Schmidt A, Liebelt G, Nießner F, von Woedtke T, Bekeschus S. Gas plasma-spurred wound healing is accompanied by regulation of focal adhesion, matrix remodeling, and tissue oxygenation. Redox Biology. 2020;38:101809. doi:10.1016/j.redox.2020.101809
4. de Almeida LGN, Thode H, Eslambolchi Y, et al. matrix metalloproteinases: from molecular mechanisms to physiology. Pathophysiology, and Pharmacology. Pharmacol Rev. 2022;74(3):712–768. doi:10.1124/pharmrev.121.000349
5. Cui N, Hu M, Khalil RA. Biochemical and biological attributes of matrix metalloproteinases. Prog mol Biol Transl Sci. 2017;147:1–73. doi:10.1016/bs.pmbts.2017.02.005
6. Fingleton B. Matrix metalloproteinases as regulators of inflammatory processes. Biochim Biophys Acta mol Cell Res. 2017;1864(11 Pt A):2036–2042. doi:10.1016/j.bbamcr.2017.05.010
7. Hawkins BT, Lundeen TF, Norwood KM, Brooks HL, Egleton RD. Increased blood-brain barrier permeability and altered tight junctions in experimental diabetes in the rat: contribution of hyperglycaemia and matrix metalloproteinases. Diabetologia. 2007;50(1):202–211. doi:10.1007/s00125-006-0485-z
8. Lino Rodrigues K, Vieira Dias Da Silva V, Nunes Goulart da Silva Pereira E, et al. Aerobic exercise training improves microvascular function and oxidative stress parameters in diet-induced type 2 diabetic mice. Diabetes Metab Syndr Obes. 2022;15:2991–3005. doi:10.2147/dmso.S365496
9. Subspecialty Group of Endocrinologic, Hereditary and Metabolic Diseases, the Society of Pediatrics, Chinese Medical Association. [Expert consensus on the standardized diagnosis and management of type 1 diabetes mellitus in Chinese children (2020)]. Zhonghua Er Ke Za Zhi. 2020;58(6):447–454. doi:10.3760/cma.j.cn112140-20200221-00124
10. Subspecialty Group of Endocrinologic, Hereditary and Metabolic Diseases, The Society of Pediatrics, Chinese Medical Association. [Guidelines for the diagnosis and management of diabetic ketoacidosis in children and adolescents (2009)]. Zhonghua Er Ke Za Zhi. 2009;47(6):421–425. Xhosa
11. Lawrence JM, Divers J, Isom S, et al. Trends in prevalence of type 1 and type 2 diabetes in children and adolescents in the US, 2001-2017. JAMA. 2021;326(8):717–727. doi:10.1001/jama.2021.11165
12. Glaser N, Fritsch M, Priyambada L, et al. ISPAD clinical practice consensus guidelines 2022: diabetic ketoacidosis and hyperglycemic hyperosmolar state. Pediatr Diabetes. 2022;23(7):835–856. doi:10.1111/pedi.13406
13. Segerer H, Wurm M, Grimsmann JM, et al. Diabetic ketoacidosis at manifestation of type 1 diabetes in childhood and adolescence—incidence and risk factors. Dtsch Arztebl Int. 2021;118(22):367–372. doi:10.3238/arztebl.m2021.0133
14. Laor L, Sendi P, Martinez P, Totapally BR. Epidemiology and outcomes of cerebral edema in hospitalized children. Pediatr Neurol. 2023;147:148–153. doi:10.1016/j.pediatrneurol.2023.07.020
15. Glaser N, Little C, Lo W, et al. Treatment with the KCa3.1 inhibitor TRAM-34 during diabetic ketoacidosis reduces inflammatory changes in the brain. Pediatr Diabetes. 2017;18(5):356–366. doi:10.1111/pedi.12396
16. Omatsu T, Cepinskas G, Clarson C, et al. CXCL1/CXCL8 (GROα/IL-8) in human diabetic ketoacidosis plasma facilitates leukocyte recruitment to cerebrovascular endothelium in vitro. Am J Physiol Endocrinol Metab. 2014;306(9):E1077–84. doi:10.1152/ajpendo.00659.2013
17. Russo S, Kwiatkowski M, Govorukhina N, Bischoff R, Melgert BN. Meta-inflammation and metabolic reprogramming of macrophages in diabetes and obesity: the importance of metabolites. Front Immunol. 2021;12:746151. doi:10.3389/fimmu.2021.746151
18. Nichols BE, Hook JS, Weng K, Ahn C, Moreland JG. Novel neutrophil phenotypic signature in pediatric patients with type 1 diabetes and diabetic ketoacidosis. J Leukoc Biol. 2022;111(4):849–856. doi:10.1002/jlb.3a1220-826r
19. Stentz FB, Umpierrez GE, Cuervo R, Kitabchi AE. Proinflammatory cytokines, markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with hyperglycemic crises. Diabetes. 2004;53(8):2079–2086. doi:10.2337/diabetes.53.8.2079
20. Rosenzwajg M, Salet R, Lorenzon R, et al. Low-dose IL-2 in children with recently diagnosed type 1 diabetes: a Phase I/II randomised, double-blind, placebo-controlled, dose-finding study. Diabetologia. 2020;63(9):1808–1821. doi:10.1007/s00125-020-05200-w
21. Kountouri A, Korakas E, Ikonomidis I, et al. Type 1 diabetes mellitus in the SARS-CoV-2 pandemic: oxidative stress as a major pathophysiological mechanism linked to adverse clinical outcomes. Antioxidants (Basel). 2021;10(5). doi:10.3390/antiox10050752
22. Ozer G, Teker Z, Cetiner S, et al. Serum IL-1, IL-2, TNFalpha and INFgamma levels of patients with type 1 diabetes mellitus and their siblings. J Pediatr Endocrinol Metab. 2003;16(2):203–210. doi:10.1515/jpem.2003.16.2.203
23. Abdel-Moneim A, Bakery HH, Allam G. The potential pathogenic role of IL-17/Th17 cells in both type 1 and type 2 diabetes mellitus. Biomed Pharmacother. 2018;101:287–292. doi:10.1016/j.biopha.2018.02.103
24. Arif S, Moore F, Marks K, et al. Peripheral and islet interleukin-17 pathway activation characterizes human autoimmune diabetes and promotes cytokine-mediated β-cell death. Diabetes. 2011;60(8):2112–2119. doi:10.2337/db10-1643
25. Emamaullee JA, Davis J, Merani S, et al. Inhibition of Th17 cells regulates autoimmune diabetes in NOD mice. Diabetes. 2009;58(6):1302–1311. doi:10.2337/db08-1113
26. Bassiouni W, Ali MAM, Schulz R. Multifunctional intracellular matrix metalloproteinases: implications in disease. Febs j. 2021;288(24):7162–7182. doi:10.1111/febs.15701
27. Marini S, Fasciglione GF, de Sanctis G, D’Alessio S, Politi V, Coletta M. Cleavage of bovine collagen I by neutrophil collagenase MMP-8. Effect of pH on the catalytic properties as compared to synthetic substrates. J Biol Chem. 2000;275(25):18657–18663. doi:10.1074/jbc.M000283200
28. Abdul Y, Jamil S, Li W, Ergul A. Cerebral microvascular matrix metalloproteinase-3 (MMP3) contributes to vascular injury after stroke in female diabetic rats. Neurochem Int. 2023;162:105462. doi:10.1016/j.neuint.2022.105462
29. Walker EJ, Rosenberg GA. TIMP-3 and MMP-3 contribute to delayed inflammation and hippocampal neuronal death following global ischemia. Exp Neurol. 2009;216(1):122–131. doi:10.1016/j.expneurol.2008.11.022
30. Yang Y, Rosenberg GA. Matrix metalloproteinases as therapeutic targets for stroke. Brain Res. 2015;1623:30–38. doi:10.1016/j.brainres.2015.04.024
31. Glaser N, Chu S, Hung B, et al. Acute and chronic neuroinflammation is triggered by diabetic ketoacidosis in a rat model. BMJ Open Diabetes Res Care. 2020;8(2):e001793. doi:10.1136/bmjdrc-2020-001793
32. Ismael S, Nasoohi S, Yoo A, Mirzahosseini G, Ahmed HA, Ishrat T. Verapamil as an adjunct therapy to reduce tPA toxicity in hyperglycemic stroke: implication of TXNIP/NLRP3 Inflammasome. mol Neurobiol. 2021;58(8):3792–3804. doi:10.1007/s12035-021-02384-z
33. Derosa G, Avanzini MA, Geroldi D, et al. Matrix metalloproteinase 2 may be a marker of microangiopathy in children and adolescents with type 1 diabetes mellitus. Diabetes Res Clin Pract. 2005;70(2):119–125. doi:10.1016/j.diabres.2005.03.020
34. Garro A, Chodobski A, Szmydynger-Chodobska J, et al. Circulating matrix metalloproteinases in children with diabetic ketoacidosis. Pediatr Diabetes. 2017;18(2):95–102. doi:10.1111/pedi.12359
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.