")
Back to Journals » International Journal of General Medicine » Volume 16
Expression of YT Domain Family Protein in Oral Squamous Cell Carcinoma and Its Correlation with the Prognosis
Authors Shi R, Li SM, Gao L, Zhi KQ, Ren WH
Received 2 February 2023
Accepted for publication 25 May 2023
Published 5 June 2023 Volume 2023:16 Pages 2263—2270
DOI https://doi.org/10.2147/IJGM.S407030
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rui Shi,1,2,* Shao-Ming Li,1,3,* Ling Gao,1,3,* Ke-Qian Zhi,1,3 Wen-Hao Ren1,3
1Department of Oral and Maxillofacial Surgery, The Affiliated Hospital of Qingdao University, Qingdao, 266003, People’s Republic of China; 2School of Stomatology of Qingdao University, Qingdao, People’s Republic of China; 3Key Laboratory of Oral Clinical Medicine, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke-Qian Zhi; Wen-Hao Ren, Department of Oral and Maxillofacial Surgery, the Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China, Email [email protected]; [email protected]
Background: Proteins contained in the conserved YTH521-b homologous (YTH) domain, have m6A-dependent RNA binding activity. As an important part of YTH domain family proteins, YTHDF1 and YTHDF3 were shown to be associated with many cancers. This paper aimed to reveal the relationship between the expression of these two proteins and the clinical prognosis of OSCC, providing certain guidance for clinical treatment of OSCC.
Methods: We detected the expression of YTHDF1 and YTHDF3 in 120 OSCC patients by immunohistochemical analysis. Statistical analysis was used to determine whether the high or low expression of these two genes was significantly associated with age, gender, histological type, clinical stage, or lymph node metastasis. The correlation curve and survival curve of the two genes were produced to evaluate the potential clinical significance.
Results: We find the expression of YTHDF1 and YTHDF3 was increased in OSCC tissues compared to adjacent normal tissues. The statistical analysis showed that the expression of YTHDF1 and YTHDF3 was significantly associated with the clinical stage and histological type in OSCC patients. There was also a significant correlation between the expression of YTHDF1 and YTHDF3. A high expression of YTHDF1 and YTHDF3 was related to poor patient prognosis.
Conclusion: Our findings suggest that a high expression of YTHDF1 and YTHDF3 may be related to poor patient prognosis.
Keywords: YTHDF1, YTHDF3, PROGNOSIS, oral squamous cell carcinoma
Introduction
OSCC is the most common head and neck malignancy.1,2 Although it has a relatively standard treatment protocol, including surgery, radiotherapy, and chemotherapy, the prognosis of OSCC patients is still poor.3 The 5-year survival rate has not improved significantly. Therefore, it is particularly important to clarify the molecular mechanism behind OSCC and deliver precisely targeted therapy.
M6A is the most abundant internal modification in mammalian mRNAs.4,5 M6A is dynamically and reversibly regulated by methyl-transferases, which act as writers, binding proteins, which act as readers, and demethylases, which act as erasers. Despite its functional importance in various physiological events, the role of m6A in chemical carcinogenesis remains largely unknown. M6A is known to regulate gene expression through m6A readers, which is a group of proteins that can recognize the modification in m6A.6 YTHDF1 and YTHDF3 are the important compose of “readers”.YTHDF1, YTHDF2, and YTHDF3 are found in the cytoplasm of homologous YT domain family proteins.7 YTHDF1 promotes the translation of m6A-methylated mRNA, and the translation of YTHDF2 accelerates the decay of m6A-methylated mRNA. YTHDF3, YTHDF2, and YTHDF1 were shown to significantly promote the metabolism of m6A-methylated mRNA.8–10 The dynamic interplay between m6A pathway components cooperatively regulates the fine-tuning of mRNA metabolism and translation.11 YTHDF1 and YTHDF3 are closely related to the prognosis of many cancers. Besides, YTHDF1 and YTHDF3 has been identified as a novel prognostic biomarker in a variety of cancers, including lung cancer, hepatocellular carcinoma, and acute myeloid leukemia.10 However, the mechanism of YTHDF1 and YTHDF3 in OSCC has not been established.
In our current study, we investigated that over-expression of YTHDF1 and YTHDF3 was correlated with clinical progression and poor prognosis in patients of OSCC.All the results laid the foundation for the biological mechanisms of OSCC.
Materials and Methods
Patients
One hundred and twenty cases of OSCC were retrieved from the Department of Oral and Maxillofacial Surgery between 2015 and 2020 by searching the electronic Hospital Information System Clinical and confirming that follow-up data were available for all the study patients. All 120 patients studied were clinically and histologically proven to have primary OSCC.The patients with an average age of 53 years. The results from all 120 cases recommended that none of patients underwent chemotherapy and suffered from additional recurrences. The project was approved by the local ethics committees, and informed consent was obtained from the study patients.
Tissue Specimens
Immunohistochemical analysis was performed on the formalin-fixed paraffin-embedded specimens of the clinically and histologically proven OSCC cases and the corresponding adjacent non-tumoral tissues, including 18 stage-I patients, 51 stage-II patients, 23 stage-III patients, and 28 stage-IV patients. TNM staging was performed according to the American Joint Committee on Cancer (AJCC).Among the selected cases, 83 patients were lymph node-negative, and 37 were lymph node-positive, indicating metastasis. With regard to the histological degree of differentiation, 71 cases were well-differentiated, 29 were moderately differentiated, and 20 were poorly differentiated.
Immunohistochemical Staining
The resected OSCC specimens and their corresponding normal tissues were immediately immersed in 4% neutral-buffered formalin, fixed overnight, and embedded in paraffin according to standard procedures. Serial sections (4-mm) cut from representative formalin-fixed, paraffin-embedded cancer tissue onto glass slides were used for immunohistochemical staining. Endogenous peroxidase activity was blocked using 0.3% hydrogen peroxide. After incubation with normal goat serum (ZSGB-BIO), the sections were incubated with anti-YTHDF1 polyclonal antibody and anti-YTHDF-3 antibody (diluted 1:200) overnight at 4•C. The sections were then incubated with biotinylated goat anti-rabbit IgG (ZSGB-BIO) at room temperature for 30 min. Between each step, the sections were washed with three changes of phosphate-buffered saline (PBS) for 3 min. The reaction product was visualized with DAB stain for 2 min. The tissue sections were then dehydrated with ethanol and xylene, mounted, and cover-slipped.
The expression of YTHDF1 and YTHDF3 was examined in five different fields at 20× magnification using a microscope equipped to study the expression. Distinctly positive cells demonstrated a diffuse brown signal in the cytoplasm, independent of intensity. To eliminate inter-observer bias, the expression of YTHDF1 and YTHDF3 was analyzed independently by two pathologists unaware of the patients’ clinical information. Based on the immunostaining scores, the specimens were divided into two groups to determine expression range through image j software.Those with more than 45% immunopositive cells, which were considered positive for protein overexpression, and those with immunostaining scores of 45% or less, which were considered negative for protein over-expression.
Statistical Analysis
Statistical analysis was carried out using SPSS26 software. The chi-squared test was used to examine possible associations between the pathology, immunohistochemical, and clinical results. The Kaplan-Meier method was used to calculate the postoperative survival rate from diagnosis to the occurrence of disease-related death, and to test the difference between the curves. The Log rank test was used to determine statistical significance. Spearman’s bivariate correlation was used to analyze the expression of YTHDF1 and YTHDF3 in OSCC tissues. A Cox proportional hazards model was used to identify factors with an independent influence on survival; hazard ratios (HR) and 95% confidence intervals (CI) were calculated. In the final multivariate Cox regression model, only those variables that were significant in the univariate analysis were included. P < 0.05 was considered statistically significant.
Results
High Expression of YTHDF1 and YTHDF3 is Correlated with Malignant Clinicopathological Features in OSCC Patients
In a series of OSCC cases with a high expression of YTHDF1 and YTHDF3, we tested the association between YTHDF1 and YTHDF3 levels and clinicopathological stages in the progression of OSCC. To further define the clinical significance of protein expression levels in the progression of OSCC, we used statistical analysis techniques to examine the correlation between YTHDF1 and YTHDF3 levels and disease stages. Our results showed that the expression of YTHDF1 was significantly correlated with the clinical stage (P = 0.028) and histological classification (P = 0.001). There was no significant association with age (P = 0.183), lymph node metastasis (P = 0.155) and gender (P = 0.870). High YTHDF3 expression was related with clinical stage (P = 0.005) and histological classification (P = 0.013).There was no significant association between age (P = 0.721), lymph node metastasis (P = 0.20) and gender (P = 0.631) (Table 1).
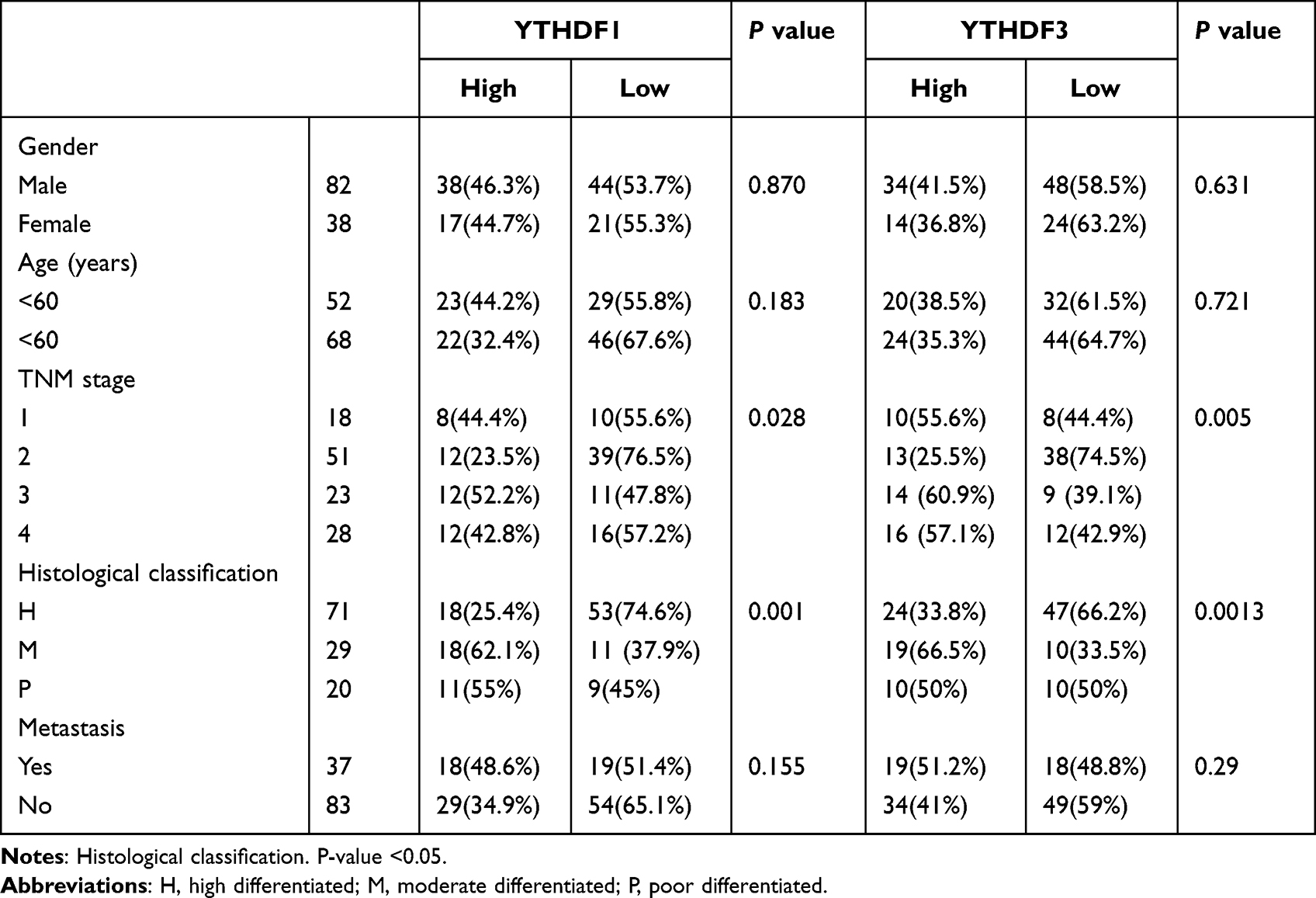 |
Table 1 Relations Between YTHDF1 or YTHDF3 Expression and Clinicopathological Parameters |
Immunohistochemical Findings
The results of the expression of YTHDF1and YTHDF3 were as follows. The expression of YTHDF1 (Figure 1A) and YTHDF2 (Figure 1B) in normal tissues was rarely observed. YTHDF1 was mainly located in the cytoplasm (Figure 2), whereas YTHDF3 was expressed in both the cytoplasm and nucleus (Figure 3). A comparison of the frequency of expression of each histological grade of OSCC showed that the worse the degree of differentiation, the higher the level of expression of both proteins. These results indicated that the overexpression of YTHDF1 and YTHDF3 may cause them to act as oncogenes, involved in the occurrence and development of OSCC.
 |
Figure 1 Negative expressions of YTHDF1 (A) and YTHDF3 (B) observed in the basal cells, epithelial cells and lamina propria. |
 |
Figure 2 YTHDF1 immunostaining showing expression in cytoplasm of OSCC (A) Well differentiated, (B) moderately differentiated, (C) poorly differentiated). |
 |
Figure 3 YTHDF3 immunostaining showing expression in cytoplasm of OSCC (A) Well differentiated, (B) moderately differentiated, (C) poorly differentiated). |
Up-Expression of YTHDF1 and YTHDF3 Predicts Poor Prognosis of OSCC
Clinicopathological analysis verified our hypothesis that the expression of both proteins in cancer tissues would increase. We calculated the postoperative survival curves of patients with high and low YTHDF1 and YTHDF3 expression. All 120 follow-up patients had a follow-up period of 100 months. The survival rate showed that YTHDF1 and YTHDF3 overexpression was associated with shorter survival and poorer prognosis (Figure 4). As shown in Table 2, the univariate analysis of Cox regression suggested that YTHDF1 expression (P=0.00053), TNM-stage (P=0.00064) were significant prognostic factors in OSCC. Furthermore, the multivariate analysis of Cox regression suggested that YTHDF1 expression (P=0.045) and TNM-stage (P=0.038) were determined as an independent prognostic factor for patients with OSCC. Meanwhile, as shown in Table 3, the univariate analysis of Cox regression suggested that YTHDF3 expression (P=0.0041), TNM-stage (P=0.021) were also significant prognostic factors in OSCC. Furthermore, the multivariate analysis of Cox regression suggested that YTHDF3 expression (P=0.039) and TNM-stage (P=0.045) were determined as significant risk factors with OSCC. (Table 2 and Table 3).
 |
Table 2 Univariate and Multivariate Analysis of Clinicopathological Features in Patients with OSCC and YTHDF1 |
 |
Table 3 Univariate and Multivariate Analysis of Clinicopathological Features in Patients with OSCC and YTHDF3 |
 |
Figure 4 (A) Survival rates demonstrated that patients with YTHDF1 amplification had a trend towards shorter poor prognosis, (B) Survival rates demonstrated that patients with YTHDF3 amplification had a trend towards shorter poor prognosis. |
Association of YTHDF1 and YTHDF3 in OSCC Tissues
We examined the correlation between YTHDF1 and YTHDF3 by Spearman correlation.The results indicated that similar profiles of YTHDF1 and YTHDF3 were found in primary cancer tissues from most patients (P<0.05). Therefore, the level of YTHDF1 might reflect the expression level YTHDF3 to a certain extent.
Discussion
Many studies have focused on the potential link between m6A and cancer.5 The role of m6A modifications may be different in different tumors. Changes in m6A also affect cancer progression, including proliferation, growth, invasion, and metastasis.12 Proteins contained in the conserved YTH521-b homologous (YTH) domain, including YTHDF1-3 and YTHDC1-2, have m6A-dependent RNA binding activity.7 Proteins containing the YTH domain are involved in many RNA processes, such as mRNA splicing, nuclear export, translation, and post-transcriptional regulation.12,13 In recent years, studies have found that the protein containing the YTH domain plays an important role in the process of post-transcriptional modification, regulating the expression of genes related to cancer and other processes.14 However, the relationship between YTHDF1, YTHDF3, and OSCC needs to be studied further.
Here, our research is the first study, to our knowledge, to assess the association between YTHDF1, YTHDF3 expression and clinicopathological features in OSCC. We found that the high expression of YTHDF1, YTHDF3 was not statistically related to age (P=0.183, P=0.732), gender (P=0.870, P=0.631), or lymph node metastasis (P=0.115, P=0.29). However, it was closely related to the histological type (P=0.001, P=0.0013) and TNM stage (P=0.028, P=0.005). We also evaluated the effect of YTHDF1 and YTHDF3 on the survival of patients with OSCC (Figure 4). We found that patients with a high expression of YTHDF1 and YTHDF3 had poor survival outcomes (P<0.05). In addition, the results of the univariate analysis showed that YTHDF1 and YTHDF3 were independent risk factors for OSCC (Table 2 and Table 3). Meanwhile, the high expression of YTHDF1 and YTHDF3 was also closely related to the poor prognosis of HCC and BRC patients.15,16 The expression pattern of YTHDF1 and YTHDF3 related regulatory factors may be considered as prognostic biomarkers.
To further investigate the mechanism of the carcinogenesis process, immunohistochemical method was used to detect the expression of YTHDF1 and YTHDF3 in OSCC tissues. The study showed that there were considerable differences between OSCC tissues and the corresponding adjacent non-tumor tissues and that the expression of YTHDF1 and YTHDF3 was increased significantly in cancer tissues. YTHDF1 was mainly expressed in the cytoplasm (Figure 2). YTHDF3 was expressed in the cytoplasm and also in the nucleus (Figure 3). This was similar to the expression of YTHDF1 and YTHDF3 in breast cancer and OSCC,15 indicating that YTHDF1 and YTHDF3 may be contributing factors to the expression of cancer.
According to previous studies, YTHDF1 could promote the translation of m6A-modified mRNA in the cytoplasm, and the over-expression of YTHDF1 could enhance the expression of c-Myc protein, indicating that YTHDF1 expression promoted c-Myc expression. At the same time, YTHDF1 can directly interact with c-Myc mRNA, which indicates that YTHDF1 regulates the expression of c-Myc mRNA in a certain way.17 YTHDF3 plays a leading role in accelerating the decay of mRNA and can regulate the RNA accessibility of YTHDF1-2. YTHDF3 affects the translation and decay of methylated mRNAs through synergy with YTHDF1 and YTHDF2. YTHDF3 can affect the functions of YTHDF1 and YTHDF2,10,18 suggesting that YTHDF1 and YTHDF3 may be involved in the activation of some signal pathways in OSCC, and then activate tumor expression. In the course of our research, we were surprised to find that the expressions of YTHDF1 and YTHDF3 were very similar according to Spearman correlation. All tumour sections studied showed a positive correlation of YTHDF1 and YTHDF3 (Figure 5, P<0.05). This association is statistically significant, it is worth pondering whether the direct regulation of YTHDF1 and YTHDF3, activates the tumour via a variety of signaling pathways of cancer, and further promotes the progression of the tumour.
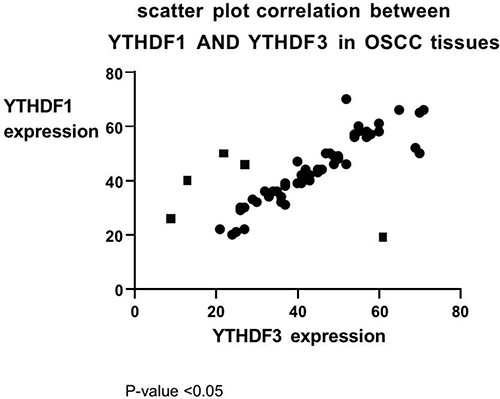 |
Figure 5 Scatter plot showing there is a correlation between YTHDF1 and YTHDF3 in the OSCC observed. |
Therefore, a comprehensive understanding of the molecular and biological characteristics of YTHDF1 and YTHDF3 will expand our understanding of the role of m6A modifications in tumors, provide potential markers and prognostic evaluation for OSCC, and propose new therapeutic targets.
Conclusion
Our study revealed differences in the expression of YTHDF1 and YTHDF3 in OSCC and analyzed the relationship between gene expression and clinicopathology and patient prognosis. We found that the expression of YTHDF1 and YTHDF3 was increased in OSCC and played an important role in long-term patient prognosis. The in-depth study of these two genes may be helpful for a better understanding of OSCC. This study has laid the foundation for further study of the biological mechanisms of OSCC.
Data Sharing Statement
The datasets used or analysed during the current study available from the corresponding author on reasonable request.
Ethics Statement and Consent to Participant
The project was approved by the Qingdao University affiliated hospital (QYFYMZJJ26812). All methods were performed in accordance with the relevant guidelines and regulations.The ethics committee of the institute agree informed consent because the data that were collected were secondary data. The investigation conforms to the principles outlined in the declaration of Helsinki.
Funding
This work was supported by no funding.
Disclosure
Rui Shi, Shao-ming Li, Ling Gao have contributed equally to this work, to be the co-first authors. The authors declare no conflict of interest.
References
1. Sasahira T, Kirita T. Hallmarks of cancer-related newly prognostic factors of oral squamous cell carcinoma. Int J Mol Sci. 2018;19(8):2413. doi:10.3390/ijms19082413
2. Zanoni DK, Montero PH, Migliacci JC, et al. Survival outcomes after treatment of cancer of the oral cavity (1985–2015). Oral Oncol. 2019;90:115–121. doi:10.1016/j.oraloncology.2019.02.001
3. Ma S, Chen C, Ji X, et al. The interplay between m6A RNA methylation and noncoding RNA in cancer. J Hematol Oncol. 2019;12(1):121. doi:10.1186/s13045-019-0805-7
4. Sun T, Wu R, Ming L. The role of m6A RNA methylation in cancer. Biomed Pharmacother. 2019;112:108613. doi:10.1016/j.biopha.2019.108613
5. Roignant J-Y, Soller M. m6A in mRNA: an ancient mechanism for fine-tuning gene expression. Trends Genet. 2017;33(6):380–390. doi:10.1016/j.tig.2017.04.003
6. Zhou B, Liu C, Xu L, et al. N6 -methyladenosine reader protein YT521-B homology domain-containing 2 suppresses liver steatosis by regulation of mRNA stability of lipogenic genes. Hepatology. 2021;73(1):91–103. doi:10.1002/hep.31220
7. Zhao W, Qi X, Liu L, Ma S, Liu J, Wu J. Epigenetic regulation of m6A modifications in human cancer. Mol Ther Nucleic Acids. 2020;19:405–412. doi:10.1016/j.omtn.2019.11.022
8. Worpenberg L, Paolantoni C, Longhi S, et al. Ythdf is a N6-methyladenosine reader that modulates Fmr1 target mRNA selection and restricts axonal growth in Drosophila. EMBO J. 2021;40(4):e104975. doi:10.15252/embj.2020104975
9. Shi H, Wang X, Lu Z, et al. YTHDF3 facilitates translation and decay of N6-methyladenosine-modified RNA. Cell Res. 2017;27(3):315–328. doi:10.1038/cr.2017.15
10. Niu Y, Zhao X, Wu Y-S, Li -M-M, Wang X-J, Yang Y-G. N6-methyl-adenosine (m6A) in RNA: an old modification with a novel epigenetic function. Genomics Proteomics Bioinformatics. 2013;11(1):8–17. doi:10.1016/j.gpb.2012.12.002
11. Wang X, Zhao BS, Roundtree IA, et al. N(6)-methyladenosine modulates messenger RNA translation efficiency. Cell. 2015;161(6):1388–1399. doi:10.1016/j.cell.2015.05.014
12. Kasowitz SD, Ma J, Anderson SJ, et al. Nuclear m6A reader YTHDC1 regulates alternative polyadenylation and splicing during mouse oocyte development. PLoS Genet. 2018;14(5):e1007412. doi:10.1371/journal.pgen.1007412
13. Liu S, Li G, Li Q, et al. The roles and mechanisms of YTH domain-containing proteins in cancer development and progression. Am J Cancer Res. 2020;10(4):1068–1084.
14. Liu L, Liu X, Dong Z, et al. N6-methyladenosine-related genomic targets are altered in breast cancer tissue and associated with poor survival. J Cancer. 2019;10(22):5447–5459. doi:10.7150/jca.35053
15. Zhao W, Cui Y, Liu L, et al. METTL3 facilitates oral squamous cell carcinoma tumorigenesis by enhancing c-myc stability via YTHDF1-mediated m6A modification. Mol Ther Nucleic Acids. 2020;20:1–2.
16. Zhao X, Chen Y, Mao Q, et al. Overexpression of YTHDF1 is associated with poor prognosis in patients with hepatocellular carcinoma. Cancer Biomark. 2018;21(4):859–868. doi:10.3233/CBM-170791
17. Jin D, Guo J, Wu Y, et al. m6A mRNA methylation initiated by METTL3 directly promotes YAP translation and increases YAP activity by regulating the MALAT1-miR-1914-3p-YAP axis to induce NSCLC drug resistance and metastasis. J Hematol Oncol. 2019;12(1):135. doi:10.1186/s13045-019-0830-6
18. Wang P, Wang X, Zheng L, Zhuang C. Gene signatures and prognostic values of m6A regulators in hepatocellular carcinoma. Front Genet. 2020;11:540186. doi:10.3389/fgene.2020.540186
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.