Back to Archived Journals » Pathology and Laboratory Medicine International » Volume 16
Expression of Her-2 and Ki-67 in Gastric Cancer Formalin Fixed Paraffin Embedded Tissue Blocks and Their Correlation with Histological Grades at the Uganda Cancer Institute Pathology Laboratory
Authors Wasswa H ![]() , Birungi A, Amadile L
, Birungi A, Amadile L ![]() , Kasadha R
, Kasadha R ![]() , Nabaasa S, Ninsiima JL, Okecha T
, Nabaasa S, Ninsiima JL, Okecha T ![]() , Ssedyabane F
, Ssedyabane F ![]() , Atwine R, Tibenderana L
, Atwine R, Tibenderana L
Received 20 July 2024
Accepted for publication 9 December 2024
Published 16 December 2024 Volume 2024:16 Pages 23—33
DOI https://doi.org/10.2147/PLMI.S468753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Paul Zhang
Hassan Wasswa,1,2 Abraham Birungi,3 Lawrence Amadile,1 Richard Kasadha,1 Saphurah Nabaasa,1 Jolly Lydia Ninsiima,1 Tonny Okecha,2 Frank Ssedyabane,1 Raymond Atwine,3 Lauben Tibenderana1
1Department of Medical Laboratory Sciences, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Pathology and Laboratory Medicine, Uganda Cancer Institute, Kampala, Uganda; 3Department of Pathology, Faculty of Medicine; Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Hassan Wasswa, Department of Medical Laboratory Science; Faculty of Medicine, Mbarara University of Science of Science and Technology, Mbarara, P.O. Box 1410, Uganda, Tel +256-752992310, Email [email protected]
Background: Her-2/neu, the human epidermal growth factor receptor-2, is an oncogene reported to be excessively expressed in gastric cancer. This over-expression is a criteria for treatment with trastuzumab. An antigen linked to nuclear proliferation is Ki-67, and the level of gastric cancer aggression is reflected in its expression.
Objective: To determine the expression of Her-2 and Ki-67 in gastric cancer formalin-fixed paraffin-embedded (FFPE) tissue blocks and their correlation with histological grades at the Uganda Cancer Institute pathology laboratory, with each block representing one gastric cancer case.
Methods: A laboratory cross-sectional study was conducted among 75 endoscopic gastric cancer patient cases. Each case was assessed utilizing immunohistochemistry (IHC) for the expression of Her-2 and Ki-67. Spearman correlation coefficient was used to ascertain the expression and its correlation to histological grades.
Results: The age range of gastric cancer cases was 26 to 80 years, with a mean age of 54. Poorly differentiated histology (43%) was the most profound. Her-2 over-expression was 20%. High Ki-67 expression was 56%, and the low Ki-67 expression was 7%. Her-2 overexpression correlated significantly with moderate differentiation (rs = 0.336, p = 0.003) and poor differentiation (rs = − 0.229, p = 0.048). A significant correlation between moderate differentiation of gastric carcinoma with low intensity of Ki-67 staining was noted (rs = 0.255, p = 0.028).
Conclusion: The aggressiveness of gastric cancer may be indicated by the over-expression of Her-2 and a high Ki-67.
What This Study Adds: This study provides additional information on the relevance of Her-2 and a high Ki-67 over-expression in diagnosis, prognostic monitoring, and management of gastric cancer in Uganda.
Keywords: human epidermal growth factor receptor 2, immunohistochemistry, nuclear proliferation-associated antigen, histology grade
Introduction
Gastric carcinoma stomach cancer, which is also called gastric cancer (GC), is a malignant disease that starts in the stomach.1 In the year 2020, there were one million new cases, and 769,000 fatalities, or one out of every 13 deaths worldwide, stomach cancer continues to be a major cancer, ranking fifth globally in incidence and fourth in death.2
Diagnosis of cancer is by use of a biopsy that is subjected to histology processes that lead to the production of a Hematoxylin and Eosin (H&E) stained section that is ultimately examined microscopically if there are any cancer cells present. The cancer cells can then be graded according to their degree of differentiation. The oncogene human epidermal growth factor receptor 2 (Her-2) has been demonstrated to be overexpressed in gastric cancer.3 According to Wang, Habuchi,4 of individuals with stomach cancer, has an overexpression of Her-2, and its over-expression is a requirement for treatment with trastuzumab.
Her-2 has been discovered to be overexpressed in several neoplasms; the most researched of them is breast cancer, where overexpression was observed in 10–34% of the instances.5 A fully humanized monoclonal antibody called trastuzumab blocks the activation of the Her-2 receptor by specifically targeting its extracellular domain. In order to treat breast cancer that is Her-2-positive, trastuzumab is currently commonly utilized and has been demonstrated to increase patient survival.6 Studies on its anticancer efficacy in patients with gastric adenocarcinomas that are positive for HER2 have been prompted by this.
Lazăr, Tăban,7 showed the nuclear proliferation-associated antigen Ki-67 to be demonstrated throughout the cell cycle’s growth and synthesis phases but not during the resting stage. The percentage of cells in the cell cycle that are active is revealed by this antigen. Oncogene or tumor suppressor gene alterations may have an impact on a patient’s prognosis for gastric cancer. According to several studies showing a link between strong proliferative ability and a dismal prognosis in a range of neoplasias, the expression levels of Ki-67 represent the aggressiveness of tumors and their prognosis.
The current study’s objective was to ascertain the expression of Her-2 and Ki-67 in gastric cancer patients and their correlation with histological grades at the pathology laboratory of Uganda Cancer Institute.
Methodology
Ethical Consideration
Approval to conduct this research was sought from the Department of Medical Laboratory Science, Faculty Research Committee (FREC), Mbarara University of Science and Technology Research Ethical Committee (MUST- 2023-852), and the administration of Uganda Cancer Institute gave the administrative clearance. Study numbers were utilized to ensure the confidentiality of the information collected. To avoid unwanted access, laboratory results were securely stored and shared with only those permitted. Also, we analysed archived samples which had been collected from patients who had given informed consent to have their samples archived and used for research purposes; this was in accordance with the declaration of Helsinki.
Study Design and Site
This was a laboratory-based cross-sectional study, carried out in the pathology laboratory of the Uganda Cancer Institute located in Kawempe South division, Kampala Uganda. As of January 2023, the UCI pathology lab has four pathologists, four technologists, and one cytotechnologist. According to the laboratory records from 2017 to 2022, the laboratory receives an average of 12 gastric cancer cases annually.
Study Population
We used endoscopically obtained Formalin Fixed Paraffin Embedded (FFPE) tissues blocks for gastric cancer, each block representing one gastric cancer case.
Sampling Procedure
Purposive sampling was performed by checking both histology record books and the laboratory information management system (LIMS) for only gastric carcinoma cases.
Selection Criteria
All gastric carcinoma cases archived in the UCI pathology Laboratory from the 1st August 2017 to 31 December 2022 were included in the study. We excluded all gastric carcinoma cases that were poorly processed and non-substantial for IHC analysis.
Sample Size Estimation
The method used to determine the sample size was that of Kish’s Leslie’s formulae8 and found to be 60 endoscopically obtained gastric cancer cases. Much as the calculated sample size was 60 endoscopically obtained gastric cancer cases, we were able to retrieve 75 gastric cancer cases that also passed the inclusion criteria, hence the 75 gastric cancer cases, were used as the sample size.
Chronological Flow of Laboratory Procedures
The laboratory procedures included; retrieving archived gastric cancer histology results along with their corresponding paraffin wax tissue processed blocks, with each block representing one patient, and both were assigned study codes. Then, we did microtomy and floating out, H&E staining, IHC staining, microscopic examination, reporting of study results, and quality control.
H&E Staining
The regressive H&E staining was used, and these sections were examined by a pathologist to confirm the gastric cancer diagnosis and determine the histology grading. Sections were first taken to water, then stained in Harris hematoxylin for 10 minutes, differentiated in 1% acid alcohol, until only the nucleus stained, washed in tap water to stop the differentiating action, blued in running tap water for 5 minutes, stained with Eosin y for 1 minute, rinsed in 95% alcohol to wash of excess eosin, rapidly dehydrated using absolute alcohol in 3 changes, cleared using xylene in two changes, and used D.P.X to mount.
Immunohistochemistry Staining for Expression of Her-2 and Ki-67
Sections of the chosen gastric cancer cases were made at 3–4 µm and floated out with BIO-OPTICA© microscope slides that were positively charged, left to completely air-dry, and then baked for 2 hours at 60°C. Sections were dewaxed using xylene in 3 changes for 2 minutes in each, hydrated through graded alcohols, and then given a two-minute gentle rinse with distilled water.
Epitope recovery was done within a Biocare Medical decloaking chamber by incubating the slides in an HIER Epitope retrieval solution containing 0.01 M sodium citrate buffer at pH 6.0 and temperatures of 95°C for 30 minutes. After cooling, the slides were cleaned in Tris buffer saline (TBS) for a minute. Immunostaining was performed with the aid of the NovolinkTM Polymer Detection System. Endogenous peroxidase was quenched by applying a peroxidase block (3–4% (v/v) hydrogen peroxide) to every slide for 15 minutes.
After that, the slides were cautiously washed for 3 minutes in Tris buffer, one drop of rabbit monoclonal primary antibody PATHWAY anti-Her-2/neu (clone 4B5) [REF number 790–4286] at a pre-diluted concentration of 6ug/mL and one drop of a rabbit monoclonal primary antibody against Ki-67 (CONFIRM, clone 30–9), [REF number 790–4286] at a pre-diluted concentration of 2ug/mL were subsequently applied to the slides, and they were incubated for 30 and 35 minutes respectively, gently washed three times in Tris buffer while at room temperature.
Slides were then incubated with NovolinkTM Post-primary [Rabbit anti-mouse IgG (<10µg/mL)] and then allowed slides to incubate at ambient temperature for half an hour. After that, slides were cautiously washed for 3 minutes in Tris buffer. Novolink Polymer was added to the slides for incubation, [Anti-rabbit poly-HRP-IgG (<25µg/mL)], and then 30 minutes were spent incubating at room temperature. The slides were then given a 3 minute gentle rinse in Tris buffer.
A freshly prepared DAB (diaminobenzidine) working solution was used to develop peroxidase activity by incubating the slides for 7 minutes. DAB working solution was prepared by adding 50 µL of Novolink TM DAD chromogen to 1 mL of Novolink TM DAB substrate. Slides were given a 5-minute distilled water rinse.
With Mayer’s hematoxylin, slides were counter stained for one minute before being washed with water, blued in running tap water for 3 minutes, dehydrated in graded alcohol, cleared in 3 changes of xylene, and then mounting was done using D.P.X.
We used known controls for staining; H&E, (colon tissue). Her-2 (known positive score +3, score 2+, score 1+ score 0), of breast and gastric cancer tissue, and Ki-67 (Known breast cancer tissue with low, moderate, and high Ki-67 score).
Determining Expression Levels of Her-2
A pathologist graded the slides using the Hofmann scoring method9 From this system, staining of 10% of tumor cells is the commonly used cut-off threshold for HER2 membranous positive. When less than 10% of the tumor cells exhibited either membrane staining or reactivity, the score was zero, (Figure 1A) A 1+ score denoted faint membrane staining, (Figure 1B) A 2+ score denoted weak-to-moderate full membrane staining, (Figure 1C) A 3+ score denoted complete membrane staining that was moderate to intense, (Figure 1D). For this study, we did not have any gastric cancer case belonging to score 1+ category, what is presented in Figure 1B is the control slide.
 |
Figure 1 Expression levels of Her-2 in gastric cancer, scale bar 100µm. |
Determining Expression Levels of Ki-67
The Ki-67 expression was rated by a pathologist, counting 1000 cells per slide allowed us to calculate the proportion of cells expressing Ki-67, and this is in accordance with the same Ki-67 scoring system used by Ahmed and Al-Tamimi10 to determine the expression of Ki-67 in gastric adenocarcinoma. Furthermore, in a study done on a similar antigen to Ki-67, proliferating cell nuclear antigen (PCNA), for the evaluation of the prognostic significance of PCNA in laryngeal squamous cell carcinoma,11 very similar cut-off percentages were used as for what we used on Ki-67.
The score for the proportion of positive cells was as follows: 10% or less of the tumor cells had to stain to indicate low proliferative expression (Figure 2A). Moderate proliferative expression was 10% to 40%, the staining of tumor cells (Figure 2B), and high proliferative expression was greater than 40%, of tumor cells staining (Figure 2C).
 |
Figure 2 Expression levels of Ki-67 in gastric cancer, scale bar 100µm. |
Determining Histology Grades in Gastric Cancer
Histology grades were determined by a pathologist using H&E microscopic examination and categorized as well, moderately, and poorly differentiated (see Figure 3A–C respectively).
 |
Figure 3 Well, moderately, and poorly differentiated gastric cancer histology grades, scale bar 100µm. |
Data Analysis Plan
Through the use of the Histology Register and Request Forms, information about every retrieved gastric cancer case was acquired from the UCI Pathology Laboratory; each of these was assigned a study identification number. The information gathered comprised of the patient’s age in years, gender, and histology diagnosis.
Data was collected with a data collection tool. Following the study’s data collection, an Excel spreadsheet was used to analyze the data using STATA version 17. For specific objectives 1 and 2, expression levels of Her-2 and Ki-67 were represented in the form of frequencies and percentages. To achieve specific objectives 3 and 4, expression levels of Her-2 and Ki-67 were correlated with histology grade. A categorical variable, of expression levels of Her-2, Ki-67, and histology grade were correlated, a significance level of <0.05 was chosen, and Spearman correlation test was employed.
Results
Case Characteristics
We considered a total of 75 endoscopically obtained gastric cancer cases in this study of which more than half 44/75 (59%) were males. The study’s average age of the cases was 54 years, having a range of 26 to 80 years. Almost two-thirds 49/75 (65%) were above the age of 50 years. Most of the cases examined were poorly differentiated, 32/75 (43%) %) as displayed in Table 1 below.
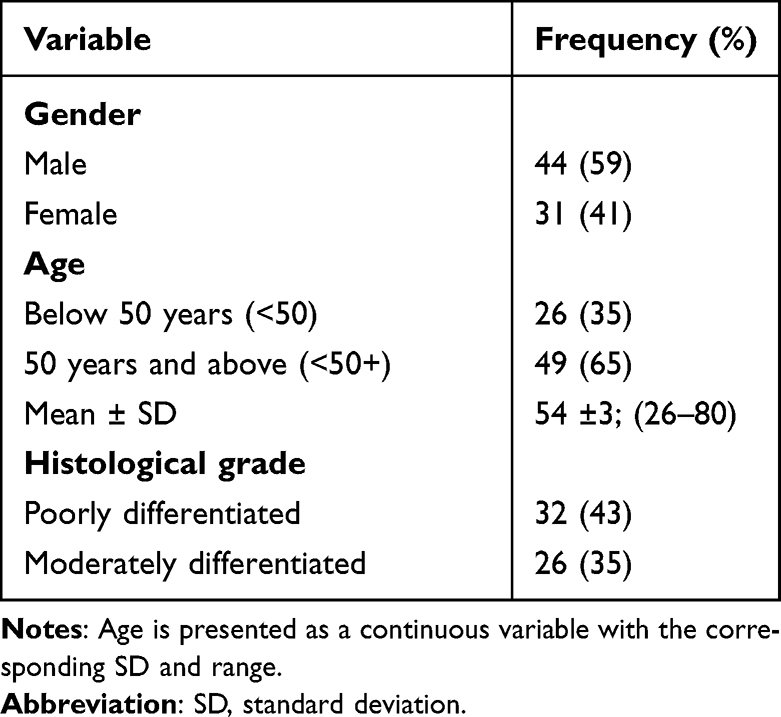 |
Table 1 Case Characteristic at the UCI Pathology Laboratory |
Expression Level of Her-2 in Gastric Cancer Cases at the UCI Pathology Laboratory
The majority of the gastric cancer cases showed a negative Her-2 expression (see Figure 1A) of 57/75 (76%), while only 15/75 (20%) showed a positive expression (see Figure 1D) as displayed in Table 2 below.
 |
Table 2 Her-2 Expression Among Gastric Cancer Cases at the UCI Pathology Lab |
Expression Level of Ki-67 in Gastric Cancer Cases at the UCI Pathology Laboratory
The majority of the gastric cancer cases 42/75 (56%) showed a high Ki-67 expression (see Figure 2C) while only 5/75 (7%) of them showed a low Ki-67 expression (see Figure 2A) as shown in Table 3 below.
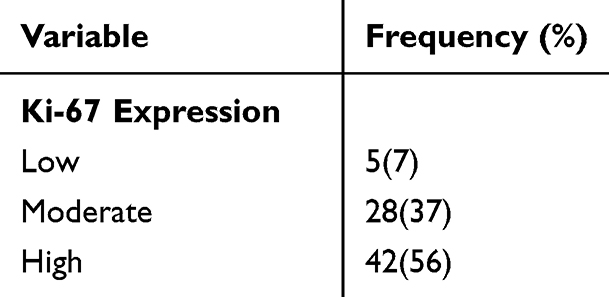 |
Table 3 Expression of Ki-67 Among Gastric Cancer Cases at the UCI Pathology Lab |
Correlation Between Expression of Her-2 and Histology Grades in Gastric Cancer Cases at theUCI Pathology Laboratory
Correlation between expression of Her-2 and histology grades was done using Spearman correlation coefficient. A 95% confidence interval was employed, less than or equal to 0.05 was the threshold for a statistically significant P-value.
Her-2 overexpression showed a correlation with both moderately and poorly differentiated gastric cancer histology grades (see Figure 3B and C respectively) as shown in Table 4 below.
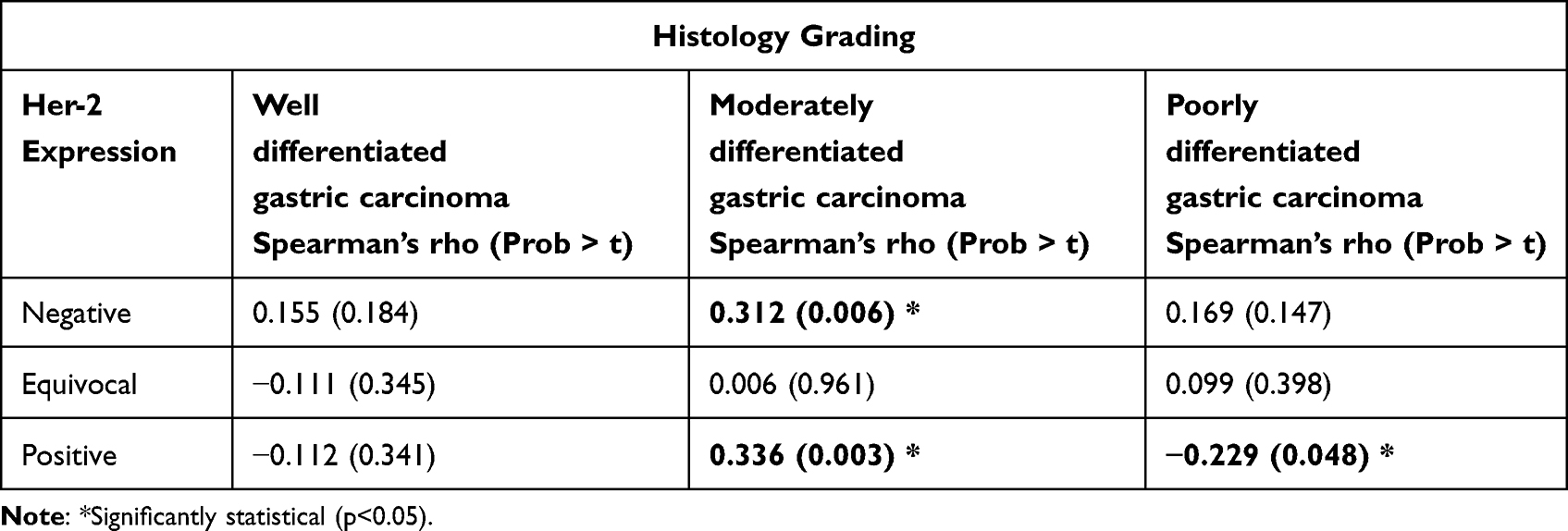 |
Table 4 Correlation Between Expression of Her-2 and Histology Grades in Gastric Cancer Cases at the UCI Pathology Laboratory |
Correlation Between Expression of Ki-67 and Histology Grades in Gastric Cancer Cases at the UCI Pathology Laboratory
Correlation between expression of Ki-67 and histology grades was done using Spearman correlation coefficient. A 95% confidence interval was employed, less than or equal to 0.05 was the threshold for a statistically significant P-value. Ki-67 expression levels that showed a correlation with histology grades were as follows:
Ki-67 low expression showed a weak positive correlation with moderately differentiated gastric carcinoma (see Figure 3B). Ki-67 moderate expression showed a positive and negative correlation with well- and moderately differentiated gastric carcinomas, respectively (see Figure 3A and B respectively), while high Ki-67 expression showed a positive correlation with well-differentiated gastric carcinoma (see Figure 3A), as shown in Table 5 below:
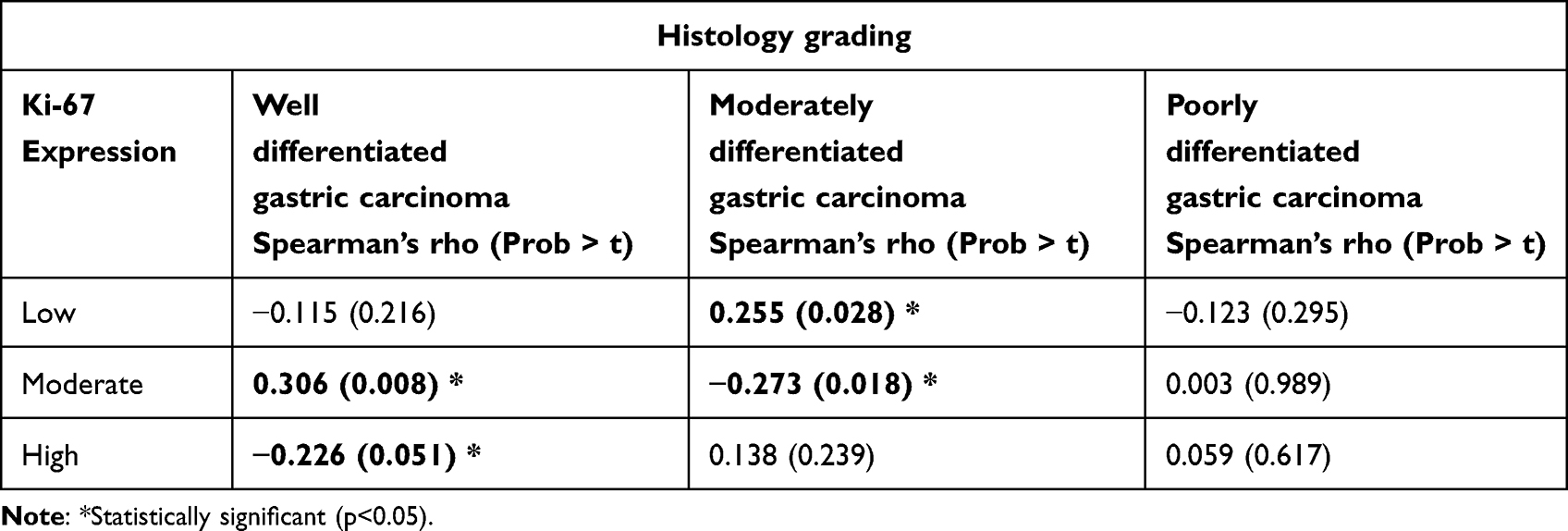 |
Table 5 Correlation Between Expression of Ki-67 and Histology Grades in Gastric Cancer Cases at the UCI Pathology Laboratory |
Discussion
A summary of the current study findings in comparison with finding from other studies are shown in Table 6 below.
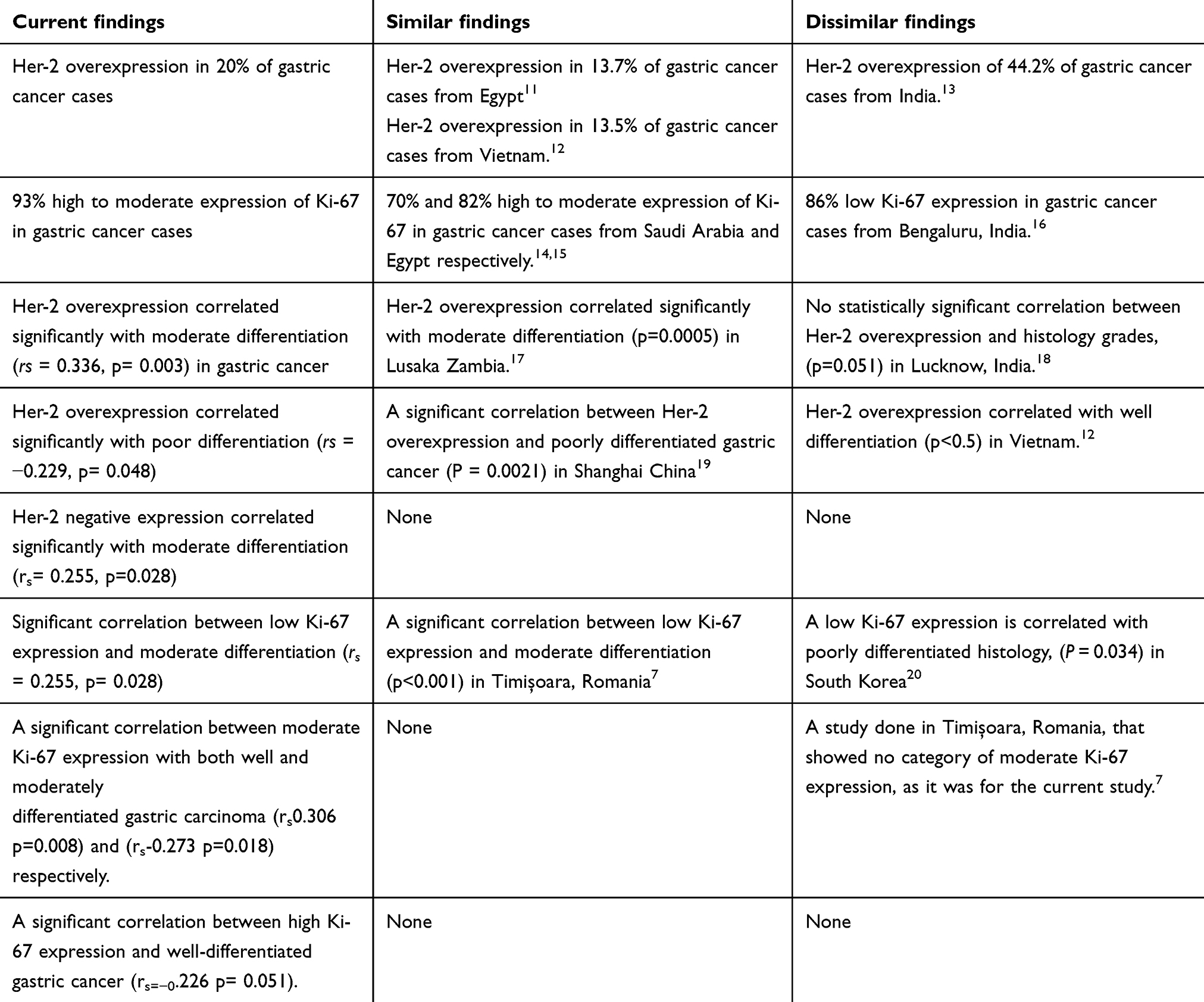 |
Table 6 Summary of Current Study Findings in Comparison with Findings from Other Studies |
Expression of Her-2 in Gastric Cancer Cases at the Uganda Cancer Institute Pathology Laboratory
In gastric cancer, determining the Her2/neu status has become crucial for determining how the patient will respond to anti-molecular treatment (such as Trastuzumab) in addition to traditional therapy (Jeung et al, 2012). In the present study, overexpression of Her-2 (IHC score 3+) was detected in 20% of gastric cancer cases. These results are consistent with research conducted in Egypt and Vietnam of 13.7% and 13.5%, respectively.13,21 The findings from these studies are similar to each other probably due to the use of the same Her-2 scoring system for gastric cancer by Hofmann, Stoss.9
The current study findings, however, are different from those reported in India, involving 52 gastric cancer cases, that demonstrated Her-2 overexpression in 44.2% of the cases.22 The difference in these findings compared to the ones of the current study could be based on the possibility that the study from India included more gastric cancer cases of Lauren’s intestinal sub type, compared to the current study, which did not consider such classification. This possibility is supported by Chu, Li,23 who conducted a study in Zhejiang Province, China, and noted that Her-2 protein overexpression was observed in 23.9% of the cases, in which the Lauren intestinal subtype had a higher likelihood of having overexpressed Her-2 protein (P = 0.001).
A study by Raj, Verma14 in Uttar Pradesh, India, used 65 gastric cancer cases, and it found 41.5% of the cases, scored as IHC 3+ (overexpression). These results differ from those of the current study which showed a Her-2 overexpression of 20%. The cause of the difference could most likely be because the study done by Raj et al included some gastric cancer cases that scored equivocal on IHC (see Figure 1C) and then Her2/neu gene was amplified on them, then scored as Her2/neu (3+) positive (4/18). This could have increased the frequency of the reported Her-2 overexpression, in that study, unlike the present study that did not involve gene amplification for IHC Her-2 equivocal gastric cancer cases. Furthermore, the study done in Uttar Pradesh, India, involved both mucosal and gastrectomy samples.
Expression of Ki-67 in Gastric Cancer Cases at the Uganda Cancer Institute Pathology Laboratory
In the present study, generally, Ki-67 from high to moderate expression was seen in 93% of the gastric cancer cases, these findings are similar to those done from Saudi Arabia and Egypt of 70% and 82%, respectively.10,15 The similar findings among the studies could be attributed to the possibility that these studies included more high-grade gastric cancer cases than the low grade. Ko, Go,24 found that a high Ki-67 expression is associated with high-grade, advanced-stage gastric cancer.
Looking at a study done in Bengaluru, India, by Pranjali and Sulatha16 that included a total of 57 gastric cancer cases, 86% of cases reported low Ki-67 expression index, with only 14% cases showing a high expression, these findings contradict those of the current study that showed 56% cases with a high Ki-67 expression. The contradiction between the two studies could be attributed to the fact that the study done in Bengaluru demonstrated the use of both specimens from gastrectomy and gastric biopsies with gastric cancer, while in the present investigation, only gastric biopsies were used.
Correlation Between Her-2 Expression and Histological Grades of Gastric Cancer Cases at the UCI Pathology Laboratory
In the present investigation, it was revealed that Her-2 overexpression correlated significantly with moderate differentiation (rs = 0.336, p = 0.003) in gastric cancer. This was in keeping with findings documented by Kasochi, Julius,17 who conducted a study from Lusaka Zambia, among 57 gastric cancer cases, and revealed that Her-2 overexpression was correlated with moderately differentiated tumors (p = 0.0005). The similarity in the findings between the two studies may be attributed to the use of similar methods that were both cross-sectional in nature and the use of endoscopically obtained gastric cancer cases.
Furthermore, from a study done by Roy, Nyodu18 in Lucknow, India, that involved 68 gastric cancer cases, the results showed no statistically significant correlation between Her-2 overexpression and histology grades (p = 0.051). Findings from this study contradicted those from the present study most likely because the study from Lucknow, India, considered gastric or gastroesophageal junction cancer cases, while the current study only included gastric cancer cases. This is supported by Van Cutsem, Bang25 who documented that in comparison to GC (21.4%), GEJ adenocarcinomas had a greater proportion of Her-2 positive tumors (32.2%).
In the present study, Her-2 overexpression correlated significantly with poor differentiation (rs = −0.229, p = 0.048). These findings were in agreement with the findings obtained by He, Bian19 in Shanghai, China, where 197 gastric cancer cases were used, and it was found that there was a correlation between Her-2 overexpression and poorly differentiated gastric cancer cases (P = 0.0021). The similarity in the findings of the two studies could be attributed to the fact that both studies could have included more cases of gastric cancer with poor differentiation and no lymph node metastases.19
However, the results from the current study are different from those reported in 2017 from Vietnam where it was noted that Her-2 overexpression correlated with well differentiation (p < 0.5), but not moderate and poor differentiation.12 This could have been because the study done in Vietnam, categorized histology grades into only two groups, namely, well differentiation and undifferentiated, while the current study categorized differentiation into three groups, namely, well, moderate, and poor.
In the present study, Her-2 negative expression correlated significantly with moderate differentiation (rs = 0.255, p = 0.028) however, we were unable to identify any other studies that supported or contradicted our findings.
Correlation Between Ki-67 Expression and Histological Grades in Gastric Cancer Cases at the Uganda Cancer Institute Pathology Laboratory
From the present study, the correlation between low Ki-67 expression (see Figure 2C) and moderate differentiation was significant (rs = 0.255, p = 0.028). These findings are near those obtained by Lazăr, Tăban,7 from a study done in Timişoara, Romania, that involved 61 gastric cancer cases, and it was noted that there was a correlation between low Ki-67 expression and moderate differentiation (p < 0.001). The similarity between the two studies is attributed to the possibility that both studies included largely tumors of moderately differentiated histology having similarly low intensity of Ki-67 staining.
However, the current study findings contradicted those in a study done by Lee, Kim,20 in South Korea, and the findings indicated a low Ki-67 expression being correlated with poorly differentiated histology (P = 0.034). The difference between this study and the findings from the current study could be linked to the difference in the Ki-67 scoring system used, for example, the study in South Korea categorized the Ki-67 expression into four categories, namely, very low (<25%), low (25–30%), moderate (50–75%), high (>75%), unlike the present study, that had only three categories for Ki-67 expression, namely, low (<10%), moderate (10–40%) and high (>40%).
Moderate Ki-67 expression showed a significant correlation with both well and moderately differentiated gastric carcinoma of (rs0.306 p = 0.008) and (rs-0.273 p = 0.018) respectively. These findings are not in keeping with those from a study done in Timişoara, Romania, that showed no category of moderate Ki-67 expression, as it was for the current study.7
High Ki-67 expression showed a significant correlation (rs=−0.226 p = 0.051), with well-differentiated gastric cancer. These findings differ from those obtained from a study done by Lazăr, Tăban7 in Romania, where it was observed that high Ki-67 expression had a proportion of 0% for well-differentiated gastric carcinoma. The discrepancy in findings between these two studies could probably be linked to the fact that (Lazăr, Tăban7) had no cases that showed high Ki-67 expression in well-differentiated gastric carcinoma.
A significant correlation between high Ki-67 expression and well-differentiated gastric cancer (rs=−0.226 p = 0.051) was noticed for the current study, however we were unable to identify any other studies that supported or contradicted our findings.
The study had an adequately calculated the sample size with power. The study followed the standard reporting guidelines for histology and Her-2, Ki-67 IHC staining. Well-optimized H&E and IHC staining protocols were used, and calibrated equipment was used. All research assistants had good experience in the tasks assigned to them.
Limitations of the Study
Cold ischemia and fixation time were not under our control, as samples were already fixed.
Antigens lose their antigenicity or diffuse into the surrounding tissues as a result of poor fixation or delayed fixation, causing failure of antigens to be expressed. Blocks that are not properly fixed do not process well with paraffin and this leads to the production of poor or failed sections, poor staining outcomes, and section washing of the slide during antigen retrieval.
Conclusion
Her-2 overexpression had a prevalence of 20%, and all the cases expressed Ki-67, with high expression dominating. The expression of Her-2 and Ki-67 showed a positive correlation, with histology grades. The aggressiveness of gastric cancer may be indicated by overexpression of Her-2 and a high Ki-67 nuclear proliferation index.
Abbreviations
DAB, 3, 3’- diaminobenzidine tetrahydrochloride; GLOBOCAN, Global Cancer Incidence, Mortality and Prevalence; H&E, Hematoxylin and Eosin; Her-2, Human epidermal growth factor receptor 2; IHC, Immunohistochemistry; Ki-67, Nuclear proliferation-associated antigen; T stage, This describes the size and growth of the primary stomach tumor; ToGA, Trastuzumab for Gastric Cancer; UCI, Uganda Cancer Institute; FFPE, Formalin Fixed Paraffin Embedded.
Data Sharing Statement
Upon reasonable request, the associated author will make all of the data used to compile this article available.
Acknowledgment
We acknowledge the tremendous work done by all the authors and research assistants. Thanks to the administration of UCI for accepting this research to be done in its pathology laboratory.
The authors are solely responsible for the views and opinions in this article.
The abstract of this study was uploaded to the Mbarara University of Science and Technology (MUST) repository on January 24th 2024: https://med.must.ac.ug/mbarara-university-of-science-and-technology-honors-exceptional-masters-dissertation-defenders-in-The-department-of-medical-laboratory-science/.
Funding
Financial support for this project was secured by the corresponding author. Also, the management of the Uganda Cancer Institute provided the antibodies, detection kits, and all histology and IHC staining consumables used in this study.
Disclosure
We hereby declare that we have no conflicting interests.
References
1. Roukos DH, Agnantis NJ, Fatouros M, Kappas AM. Gastric cancer: introduction, pathology, epidemiology. Gastric Breast Cancer. 2002;1(1):1–3.
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Yu D, Hung M-C. Overexpression of ErbB2 in cancer and ErbB2-targeting strategies. Oncogene. 2000;19(53):6115–6121. doi:10.1038/sj.onc.1203972
4. Wang L, Habuchi T, Takahashi T, et al. No association between HER‐2 gene polymorphism at codon 655 and a risk of bladder cancer. Int J Cancer. 2002;97(6):787–790. doi:10.1002/ijc.10129
5. Kaptain S, Tan LK, Chen B. Her-2/neu and breast cancer. Diagn Mol Pathol. 2001;10(3):139–152. doi:10.1097/00019606-200109000-00001
6. Tewari M, Kumar A, Mishra R, Kumar M, Shukla HS. HER2 expression in gastric and gastroesophageal cancer: report from a tertiary care hospital in North India. Indian J Surg. 2015;77(S2):447–451. doi:10.1007/s12262-013-0871-y
7. Lazăr D, Tăban S, Sporea I, et al. Ki-67 expression in gastric cancer. Results from a prospective study with long-term follow-up. Rom J Morphol Embryol. 2010;51(4):655–661.
8. Kish L. Methods for design effects. J off Stat. 1995;11(1):55.
9. Hofmann M, Stoss O, Shi D, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008;52(7):797–805. doi:10.1111/j.1365-2559.2008.03028.x
10. Ahmed A, Al-Tamimi DM. Incorporation of p-53 mutation status and Ki-67 proliferating index in classifying Her2-neu positive gastric adenocarcinoma. Libyan J Med. 2018;13(1):1466573. doi:10.1080/19932820.2018.1466573
11. Bedeer A, El-Rashidy M, Elzayat S, Elsherif H. Evaluation of the prognostic significance of P53 and Proliferating cell nuclear antigen (PCNA) in laryngeal squamous cell carcinoma. Int J Cancer Biomed Res. 2020;4(3):169–176.
12. Phan DAT, Nguyen VT, Hua TNH, Ngo QD, Doan TPT, Thai AT. HER2 status and its heterogeneity in gastric carcinoma of Vietnamese patient. J Pathol Transl Med. 2017;51(4):396–402. doi:10.4132/jptm.2017.04.24
13. Abdel-Aziz A, Ahmed RA, Ibrahiem AT. Expression of pRb, Ki67 and HER 2/neu in gastric carcinomas: relation to different histopathological grades and stages. Ann Diagn Pathol. 2017;30:1–7. doi:10.1016/j.anndiagpath.2017.05.003
14. Raj N, Verma D, Kumar A, Rai P, Rao RN. HER2 oncogene amplification and immunohistochemical profiling in gastric adenocarcinoma. Discoveries. 2018;6(4):e83. doi:10.15190/d.2018.6
15. Almabrouk NM, El-Maraghy MN-E, Badr AME, Meckawy GR, Shakweer MM. Prognostic utility of Ki-67 in gastric carcinoma. Immunopathologia Persa. 2021;8(1):e14–e. doi:10.34172/ipp.2022.14
16. Pranjali C, Sulatha K, Vijaya V M. CDX2 and Ki-67 expression in gastric carcinoma and its association with clinocopathological parameters. Asian Pacific J Cancer Biol. 2022;7(3):255–263. doi:10.31557/apjcb.2022.7.3.255-263
17. Kasochi C, Julius P, Mweemba I, Kayamba V. Human epidermal growth factor receptor 2 overexpression in gastric and gastroesophageal junction adenocarcinoma in patients seen at the university teaching hospital, Lusaka, Zambia. Afr Health Sci. 2020;20(4):1857–1864. doi:10.4314/ahs.v20i4.41
18. Roy PS, Nyodu T, Hazarika M, et al. Prevalence of HER2 expression and its correlation with clinicopathological parameters in gastric or gastroesophageal junction adenocarcinoma in North-East Indian population. Asian Pac J Cancer Prev. 2019;20(4):1139. doi:10.31557/APJCP.2019.20.4.1139
19. He C, Bian X-Y, Ni X-Z, et al. Correlation of human epidermal growth factor receptor 2 expression with clinicopathological characteristics and prognosis in gastric cancer. World J Gastroenterol. 2013;19(14):2171. doi:10.3748/wjg.v19.i14.2171
20. Lee HE, Kim MA, Lee BL, Kim WH. Low Ki‐67 proliferation index is an indicator of poor prognosis in gastric cancer. J Surg Oncol. 2010;102(3):201–206. doi:10.1002/jso.21583
21. El-Gendi S, Talaat I, Abdel-Hadi M. HER-2/Neu status in gastric carcinomas in a series of Egyptian patients and its relation to Ki-67 expression. Open J Pathol. 2015;5(04):101. doi:10.4236/ojpathology.2015.54014
22. Sekaran A, Kandagaddala RS, Darisetty S, et al. HER2 expression in gastric cancer in Indian population—an immunohistochemistry and fluorescence in situ hybridization study. Indian J Gastroenterol. 2012;31(3):106–110. doi:10.1007/s12664-012-0214-0
23. Chu Y, Li H, Wu D, Guo Q. HER2 protein expression correlates with Lauren classification and P53 in gastric cancer patients. Medicine. 2022;101(37):e30647. doi:10.1097/MD.0000000000030647
24. Ko GH, Go S-I, Lee WS, et al. Prognostic impact of Ki-67 in patients with gastric cancer—the importance of depth of invasion and histologic differentiation. Medicine. 2017;96(25):e7181. doi:10.1097/MD.0000000000007181
25. Van Cutsem E, Bang Y-J, Feng-Yi F, et al. HER2 screening data from ToGA: targeting HER2 in gastric and gastroesophageal junction cancer. Gastric Cancer. 2015;18(3):476–484. doi:10.1007/s10120-014-0402-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.