")
Back to Journals » International Journal of Women's Health » Volume 14
Exploring Unknown Predictors of Maternal Anemia Among Tribal Lactating Mothers, Andhra Pradesh, India: A Prospective Cohort Study
Authors Gupta A , Kollimarla M, Reddy B V, Noorani Shaik Y, Kakkar R, Aravindakshan R
Received 27 June 2022
Accepted for publication 25 August 2022
Published 3 September 2022 Volume 2022:14 Pages 1219—1236
DOI https://doi.org/10.2147/IJWH.S380159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Arti Gupta,1 Mounika Kollimarla,1 Venkatashiva Reddy B,1 Yusuf Noorani Shaik,2 Rakesh Kakkar,3 Rajeev Aravindakshan1
1Department of Community and Family Medicine, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India; 2ICDS Project, Guntur, Andhra Pradesh, India; 3Department of Community and Family Medicine, All India Institute of Medical Sciences, Bathinda, Punjab, India
Correspondence: Arti Gupta, Department of Community and Family Medicine, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India, Tel +91-9013902976, Email [email protected]
Introduction: Anemia is a serious public health issue in India, especially among women, adolescent girls, and young children. Tribal people reside mostly in remote underserved regions with little or no basic civic amenities which makes them a highly vulnerable group of Indians. The study aimed to identify unknown risk factors for anemia among tribal lactating mothers.
Methodology: It was a mixed method prospective cohort study for 10 months carried out among 340 scheduled tribes (ST) mothers in 10 clusters in Guntur district, Andhra Pradesh, India. Data collection using a questionnaire, 24 hours dietary recall, anthropometric measurement, and hemoglobin estimation was done. Weekly local recipe talk in the mother’s kitchen, informal group discussions, was conducted for 12 weeks after baseline data collection. The audio and video tapes of the weekly local recipe talk in the mothers kitchen were transcribed verbatim and then translated into English. The individual responses were grouped as barriers related to acceptability, availability, accessibility, use and utilization, appropriateness, and nutrition environment.
Results: A total of 340 mothers were enrolled initially of which 315 mothers were studied in an end-line survey with an attrition rate of 7.3%. Over 80% mothers belonged to Yerukula, Yenadis, Lambadi/Sugali tribes, respectively. A total of 345 weekly local mother kitchen recipe talks were conducted in 10 clusters. In the present study, only few mothers mentioned food accessibility and availability issues. Surprisingly, lack of skill to cook the commonly consumed local food item among Indian mothers were recorded. Lack of time for cooking, lack of knowledge of nutritious benefits of food, and use of ready to eat food were other important key findings.
Conclusion: The study documents initiation of transition of the tribal lactating mothers towards urbanization. The lack of knowledge of cooking, coupled with lifestyles of urban areas exposes the early aged, poor, low literate mothers to the trap of anemia.
Keywords: anemia, lactating mothers, dietary, iron, tribes
Introduction
India is home to around 104 million tribal people. They make up 8.6% of the country’s population and are divided into 705 tribes. Tribal people have remained marginalized in terms of geography, socioeconomics, politics, and, as a result, the national mentality. In tribal territories, health and healthcare are still unsolved issues.1 As per Census 2011, 90% of Tribal people reside in rural areas, only 40.6% have good houses; 74.7% use open defecation; 22.6% have toilet facilities within the premises; 54.4% of literacy rate; Drop Out Rates boys is 50.4%; high infant mortality rate 62.1 per 1000 live births; high child mortality rate of 35.8 per 1000 children; only 17.7% Institutional deliveries and high prevalence of any anemia (<12.0 g/dl) in women 68.5%.2 Thus tribal people reside mostly in remote underserved regions with little or no basic civic amenities which makes them a highly vulnerable group of Indians.
Anemia is a serious public health issue in India, especially among women, adolescent girls, and young children. Anemia is linked to delayed mental and psychomotor development as well as an increased chance of maternal death, in addition to increased morbidity and negative effects on physical well-being.3 Malnutrition is the underlying cause of higher IDA prevalence among these vulnerable population groups particularly the diets of preschool-age children are grossly deficit in iron and the pregnant and menstruating women do not meet additional iron requirements in India.4
Reproductive-aged women are considered to be a nutritionally vulnerable segment of the population. Infants face a series of serious nutritional challenges, such as energy-protein malnutrition and micronutrient deficiencies. Due to increasing nutritional demands for rapid growth and inappropriate eating habits, the prevalence of malnutrition is high, which affects their growth and development. While the role of energy and proteins on physical growth is well established, recent studies have stressed the importance of micronutrients in enhancing full growth potential.3
The cutoff value for hemoglobin concentration in the blood to be anemic are the same for a lactating mother and reproductive-age women even though there is increased demand for calorie and nutrients during lactation.4 In addition, the national guidelines state Administer tablets of IFA (60 mg of iron and 0.5 mg of folic acid) daily for at least 100 days, after 1st trimester for prophylaxis against anemia and double the dose in case of anemia is diagnosed. During puerperium women, iron supplementation for 180 days is advised. The 180 days IFA supplementation is not received by many mothers during puerperium.5
Estimates of Anemia Mukt Bharat shows in India in 2021 the prevalence of any anemia, moderate anemia, and severe Anemia is 69%, 66%, and 3.3%, respectively.6 National Family and Health survey 5, 2019–21 data stated in India, 57% of non-pregnant women aged 15–49 years were anemic with hemoglobin <12.0 g/dl.7 Numerous maternal interventions had been researched like women’s empowerment, m-health technologies, conditional cash transfers, water, sanitation and hygiene, and agricultural interventions to address anemia.8 Several other studies had been conducted to increase IFA and fortified food consumption among the reproductive age group of women.9 The significant impact of a school-based nutrition program on increasing mothers’ knowledge, attitude, and practice, as well as their children’s nutritional status, was evaluated in a cluster randomized controlled trial.10 The present study aimed to identify unknown risk factors for anemia among tribal lactating mothers through Weekly local recipe talk in the mother’s kitchen.
Materials and Methods
The mixed method research study was conducted in Guntur district Andhra Pradesh, India. From June 2021 to April 2022, a cohort study was undertaken among lactating mothers of infants in the Guntur region of Andhra Pradesh, India. Mothers in selected households were eligible for participation if they met the criteria for a target group, such as having lived in the study area for at least 6 months, living in a selected household at the time of data collection, belonging to an Andhra Pradesh tribe, and giving their consent to participate. Mothers who had indications of acute infection or who refused to agree were eliminated. The sample size computations were based on estimated incidence assumptions with a 15% precision and a 95% confidence interval (1.96). The number of clusters was ten and the design impact is two. The cohort’s sample size was 340 lactating mothers. The list of scheduled tribe mothers with a child under the age of one year was acquired from 23 Integrated Child Development Services (ICDS) Scheme projects, Guntur, Department of Women and Child Development, Andhra Pradesh. ICDS is one of the health programmes of the Government of India for early childhood care and development. Each project site was separated between urban and rural regions, with number of Anganwadis, ICDS child care centre, facilities catering to both. The project locations with a minimum of 50 eligible mothers in urban or rural settings were listed. From the following list, five clusters were chosen at random in both urban and rural regions. Guntur, Tenali, Mangalagiri, Amruthalur, and Repalle were the urban clusters studied, while Bollapalli, Chilkapuripeta, Amaravati, Prathipadu, and Pedakkani were the rural clusters studied in the Guntur district [Figure 1]. In the specified clusters, a list of eligible mothers was obtained. A total of 34 eligible mothers were studied at random within each cluster.
 |
Figure 1 Map showing the location of the study area. *Red Pointer indicates the studied cluster’s location. |
After ascertaining the eligibility of the participant, detailed information about the study including publication of anonymised responses was given through the Participant Information Sheet and written informed consent was obtained. The study complies with the Declaration of Helsinki. Both these documents were in Telugu and any difficult words were explained by Anganwadi workers. The study has been approved by the All India Institute of Medical Sciences Mangalagiri ethics committee. [AIIMS/MG/IEC/2021-22/105] Baseline data collection about socio-demographic characteristics, 24 hour dietary recall, anthropometric, iron supplemental intake, antenatal history, morbidity-related data, and Hemoglobin estimation in both urban and rural locations. Weight and height were measured as per World Health Organization standard guidelines. Hemoglobin was measured using Hemocue 301 as per standard protocol. A weekly local recipe talk was held in the mother’s kitchen by project staff for 12 weeks. Each session included a subgroup of mothers. Three sessions were held at different sites in a cluster every week to facilitate that each mother had actively engaged at least once a week. One of the research participants, or anganwadis, kitchens were used. Five to ten mothers were engaged in a weekly local recipe talk in the mother’s kitchen. Anganwadi staff and volunteers were also asked to participate in the discussion. Raw materials were handed to mothers and they were taught to prepare during a weekly local recipe discussion in their kitchens. When there was no access to a kitchen, a visual diary was used. Mother’s weight, height, hemoglobin and 24-hour dietary recall was repeated after 12 weeks of follow up.
For Weekly local recipe talk in mothers’ kitchen visual diary was created. It was based on the 24-hour dietary intake of the participants in the baseline survey. We use SECA Culina 852 Diet & Kitchen Scale to weigh the raw food ingredients. National Institute of nutrition guidelines was used to design for Weekly local recipe talk in the mother’s kitchen. A total of 12+1 recipes (12 vegetarians and one nonvegetarian) were designed for each 12-week follow-up. The non-vegetarian recipe was not included individually to maintain exposure of women to weekly mother kitchen recipe talks, as some candidates were vegetarian.
They were green leafy vegetable rice, ragi laddu, pesarattu, drumstick leaves dhal, vegetable idly, sesame laddu, amaranth curry, ragi malt, date poli, black gram laddu, ponnaganni chapathi, coriander, and mint chutney and gogu chicken to cover cereal-based, legume-based, vegetable-based, snack-based, a sweet dish based, nonveg, fruit-based and nuts-based food groups. These contain diet information for various iron-rich food products as well as cooking ways to improve the current inadequate diets with a basic understanding of iron content in cooked meals and consumed portions.
The days were fixed for different sites in a cluster to conduct Weekly local recipe talk in the mothers kitchen. The participants and Anganwadi workers were informed before the day of the visit. Also, a WhatsApp group was formed for each cluster, and time and venues were updated regularly for Weekly local recipe talk in the mothers kitchen.
Weekly local recipe talk in the mothers kitchen was an informal group discussion with mothers. At the start of the Weekly local recipe talk in the mothers kitchen the project staff showed the mothers raw food materials and asked them to identify the same. This was followed by general questions like tell about usual home food preparation behaviour for this food item? How do mothers feel about the nutrition status of this food item cooking? Did mothers cook these food item meals? How do mothers prepare this food item? Where do mothers eat their meals? Why? In the next step, mothers were asked to explain the way of cooking the food recipe? And at the end, the project staff explained and demonstrated the rights and wrongs of cooking the food recipe, and explain the nutritive value of this food item.
All Quantitative data were entered using Microsoft Excel 2010 and analyzed using IBM SPSS Statistics Base v28.0 compatible with Windows. The data was checked for normality. Univariate analysis was done. factors. Step-wise selection was employed to obtain the variables that were significant at the level of P < 0.05 and were entered into the final multivariate logistic regression models. The audio and video tapes of the Weekly local recipe talk in the mothers kitchen were transcribed verbatim and then translated into English. The individual responses were grouped as barriers related to acceptability, availability, accessibility, use and utilization, appropriateness, and nutrition environment that was formed the basis of our thematic results. Qualitative data analysis was done using ATLAS.ti 22 Educational Single User License.
Results
A total of 340 mothers were enrolled initially of which 315 mothers were studied in an end-line survey with an attrition rate of 7.3%. Over 80% mothers belonged to Yerukula, Yenadis, Lambadi/Sugali tribes, respectively. Anemia was found in 63.82% of women with haemoglobin less than 12 gm/dl at baseline (95% CI: 58.5 to 68.7). The baseline prevalence of anemia was more among mothers aged twenty years or more. Nearly one-fifth of mothers (22.4%) were married at an age less than 18 years. Anemia was significantly more among mothers who had menarche at an age less than 13 years (p = 0.03) Rural mothers were more anemic (50.7%) compared to urban (49.3%). Nearly half of the mothers were not literate (46.1%). The prevalence of anemia with the literacy status of mothers was significantly associated (p < 0.03). Over three-fourth anemic mothers were homemakers (84.8%) and belonged to the lower or lower-middle socioeconomic class (82.9%). The prevalence of anemia among mothers was nearly equal to the type of house. Anemia was almost double among mothers with a parity of three or more. [Table 1]
 |
Table 1 Association of Selected Characteristics with Anemia Among Mothers at Baseline (n = 340) |
The unadjusted relative risk for factors associated with the anemia in mothers after three months of follow-up. Anemia was significantly associated with the lower and lower-middle socioeconomic status of the mother with a Relative Risk of 1.35 (1.08 to 1.71) (p < 0.01) in the end-line survey. Multiple logistic regression was used to identify factors associated with anemia among mothers at the end-line survey with entry and removal probability of 0.05 and 0.50 respectively was used. The dependent variable was the age at menarche, residence, occupation, socioeconomic status, overcrowding, female child presence, post-natal visit, post-natal consumption of IFA tablets, and age of the last child in months. Anemia was significantly associated with the socioeconomic status of the mother with a relative risk of 2.33 (1.19 to 4.57) (p = 0.014). Anemia among mothers was significantly associated with the age of the last child with a relative risk of 0.58 (0.34 to 0.98), p = 0.04. [Table 2]
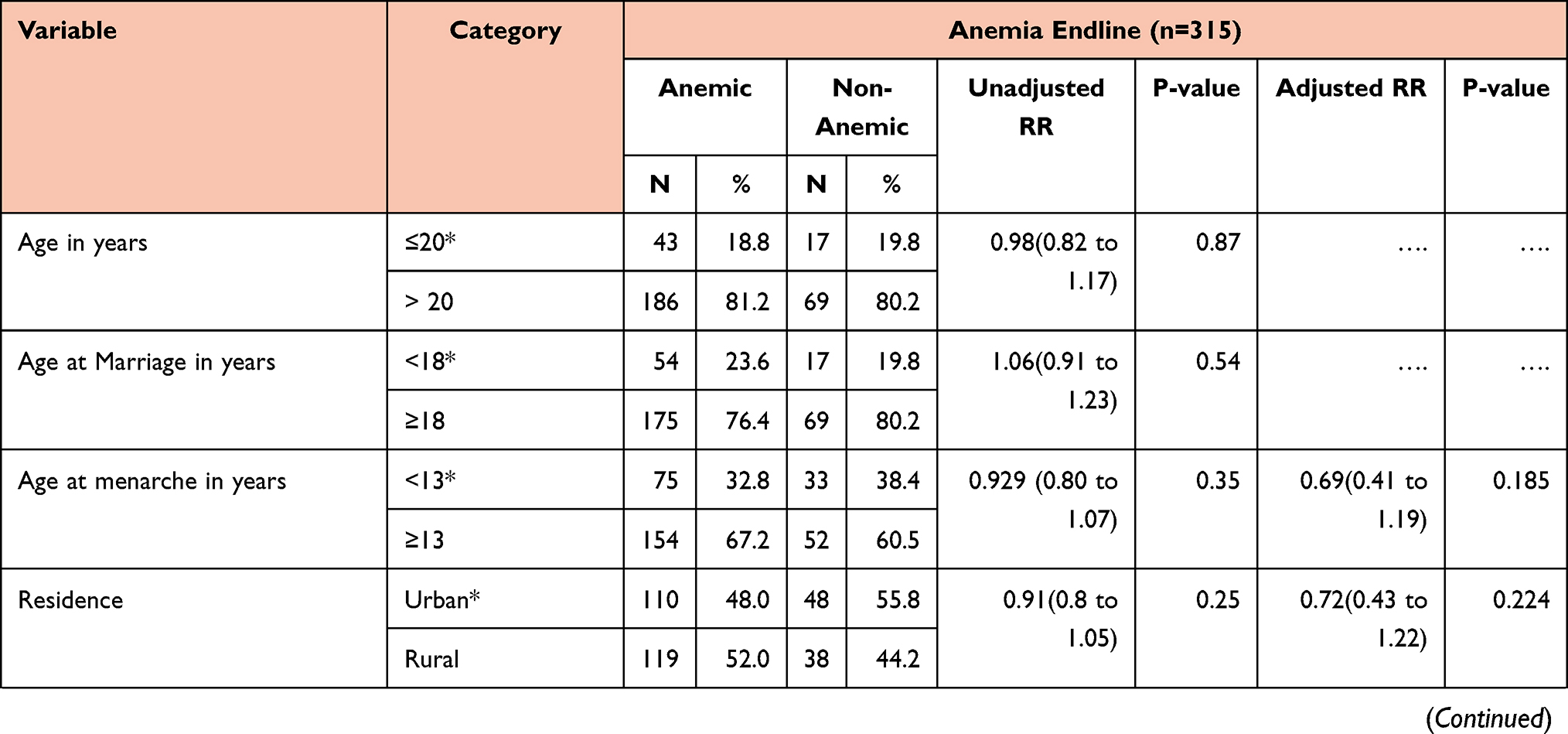 |  |  |
Table 2 Unadjusted and Adjusted Relative Risk for Various Risk Factors for Mothers at End-Line (n = 315) |
A total of 345 Weekly local recipe talks in the mother’s kitchen were conducted over 3 months in 10 clusters. The thematic analysis identified seven overarching themes from 12 weeks, Weekly local recipe talk in mothers kitchen: (I) acceptability, (II) availability, (III) accessibility, (IV) use and utilization (V) appropriateness (VI) nutrition environment and (VII) Affordability as a barrier to consumption of iron-rich diet [Table 3]
 |
Table 3 The Themes and Codes Identified in the Weekly Local Recipe Talk in Mothers Kitchen |
Figure 2 shows the Treemap Beta, to visualize flat and hierarchical coded data of weekly local recipe talk in the mother’s kitchen as rectangles that are sized and colored based on quantitative variables that are a number of barrier quotations to an iron-rich diet. The themes are described below with illustrative quotes.
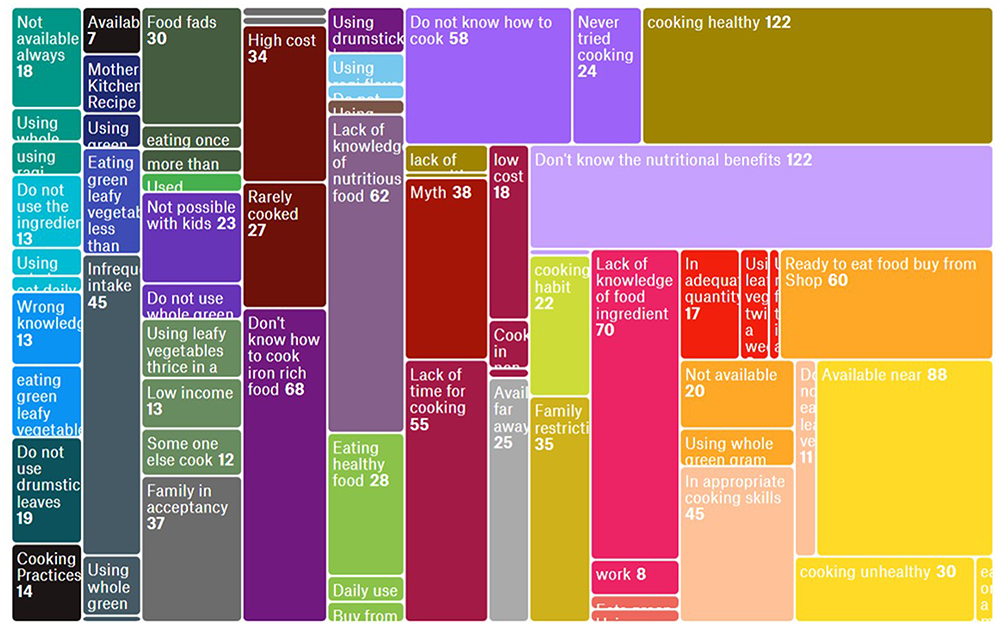 |
Figure 2 The Treemap Beta illustrating quotation count with codes for weekly local recipe talk in mother’s kitchen. |
Theme 1: Acceptability
Overall, all of the food ingredients discussed in the weekly local recipe talk in the mother’s kitchen were acceptable to mothers. Indian kitchens are opportunities for families to prepare and share healthy foods. Children and adults frequently share meals. Family habits established will carry through life. Food acceptance and enjoyment by the family are key for cooking in the kitchen. Food and food habits serve are a basic part of the culture. Nutrition is influenced by multiple social factors. Family food restrictions originate early in life and persist throughout. The present study recorded a few families’ food acceptancy concerns and family restrictions that restrict the intake of iron-rich food of mothers.
Week 1: All Candidates: We know about the nutritive values of green leafy vegetables and we also want to cook but also, we don’t cook regularly because in our family my in-laws and elders whatever they bring we should cook those only. We will not tell anything either its good for health or not because it’s our responsibility whatever they like we will be following those things only madam
Week 2: Candidate 721: At my home my husband and family members they are not having interest to drink ragi malt daily so I too also not having interest to make ragi malt
Week 3: Candidate 606:-I don’t ever try. we are using mostly black gram whole for preparing idli, dosa etc … at my home they will not bring because they will not eat and my husband will not eat madam
Week 6: Semsame laddu “Candidate 112: No madam. We didn’t see but my elders they are telling like that so we are following”, “Candidate 322: my grandmother told so we never eat in pregnancy time”, “Candidate 933: But my elders don’t allow me to eat that … ”
Week 7: Candidate 1029: My elders don’t allow us to eat the leafy vegetables when we are lactating, we only eat the tinda and snake gourd curry.
Week 8: Ragi Malt: Candidate 512:- It causes cold madam. So, my elders shouted at me that’s why I didn’t drink.
Week 11: Ponnaganni Chapathi: “Candidate 313:- before marriage I eat madam after marriage not eat madam”, Candidate 903: In my home we all are a joint family, at least we make 1.5kg of wheat flour. By making that amount of chapati, we don’t have any idea how to make the leafy vegetable chapati. My mother will be tired after doing that much chapatis, so she can’t add the leafy vegetable to it”, “Candidate 1004: After delivery I am at my mother’s house. That time I ate more green leafy vegetables. But after coming to my mother-in-law house we don’t use this regularly.
Week 12: “Candidate 523: My mother in law doesn’t allow us to make that … ”, “Candidate 607: We have to eat what my mother in law cooks, if she cooks then we eat that … ”, “Candidate 807: My husband doesn’t like it more …., “Candidate 934: Nothing, we don’t know all these before. But now my elders don’t allow us to make all these … ”, “Candidate 1004: My mother makes that, but my mother-in-law did not make that. When my mother makes that we eat most likely that.”, etc
Theme 2: Accessibility
Smattering food accessibility constraints were stated by the few mothers. Mothers without access to iron-rich food ingredients further hinder the cooking of iron-rich diet.
Week 3: “Candidate 110: Green gram whole are not available nearby us and for buying green gram we have to go long. So we use to make normal dosa which is preparing with black gram dal”, “Candidate 415: 40min or 1hrs time for the market madam”
Week 4: Candidate 816: In my locality I never see people using drumstick leaves
Week 7: Amaranth leaves: Candidate 205: yes madam, it is available in the market but house to market very long madam
Week 11: Ponnaganti leaves Candidate 816&817: In this locality it is not available. We have to go to the market at the center.
Theme 3: Affordability
In addition, lack of amenities and low income further restricted few mothers to purchase limited and low-cost food ingredients.
“Candidate 206: have a problem madam that much of the cost we didn’t effort.”, “Candidate 209: having work but less salary we get and not balance both homework and outside work.”, “Candidate 528: yes madam, we suffer with money problem madam”, “Candidate 104: I don’t buy but when we went for begging if someone gives we will eat otherwise don’t eat” “Candidate 816: We don’t have gas for cooking. It is not convenient to cook with a wood stove.”, “Candidate 426: no gas madam”, “Candidate 428: no gas madam”
Theme 4: Appropriateness
Lack of nutrition in the diet has been linked to appropriate cooking skills. Daily nutrient intake and the overall nutritional status of mothers are related to cooking practices. An inadequate quantity or dilution or infrequent intake of iron-rich food ingredients in recipes leads to iron deficiency and a negative impact on health.
Week 2: Candidate 720: Why means we don’t like to drink frequently. If we use ragi flour it will give strength to us and At my home ragi flour is there but I don’t have interest to cook frequently
Week 7: Candidate 207: available madam but I never cook. I mostly cook these two only rarely cook Gongura.
Week 8:“Candidate 113:- 2 spoons ragi madam.Interviewer:- You are using 2 spoons for 4 members”, Coriander chutney: “Candidate 133,112:Twice in a week that too very little quantity we are using for curry”, Pesarattu: “Candidate 818: For 250gms of green gram I add 1.5kg of rice … ”
The problem is likely not only lack of time, money, and knowledge about cooking skills and how to prepare iron-rich food; lack of amenities; and access to healthy food ingredients, but a lot of the social myths about cooking and eating behaviours.
Week 1: Candidate 726: Gap means … … my parents told to us if we eat green leaves in maternal period our child will suffer with diarrhea so we stopped to take green leaves in that time and again we started to take after few days
Week 10: Black Gram laddu: “Candidate 625: My elders they are telling if we eat sunnunda cold and cough will occur to us so”, “Candidate 811: We don’t eat it because it is sweet. We fear that we will get cold.”
Week 12: Candidate 607: If we eat leafy vegetables the new born baby did not digest that and their pee also in green color that’s why we don’t eat that …
Week 2: Candidate 113: If we drink ragi malt my children will get cold and cough so i don’t drink too much
Week 6: Sesame ladoo Candidate 204: in pregnancy time pregnancy miss carriage madam
“Candidate 212: no madam, same reason heat and miss carriage”, “Candidate 309:- pregnancy time says don’t eat madam”, “Candidate 405:- I eat in my 3rd month of pregnancy. At that time I didn’t know we don’t eat things so I eat I lost my pregnancy, madam.”, “Candidate 416:- pregnancy miss carriage madam it gives heat to the body”, “Candidate 905: During lactating also we don’t eat this … ”, “Candidate 925: They eat that, but we fear if the baby gets cold that’s why we don’t eat”, “Candidate 933: My elders don’t allow us to eat sweet items because it causes cold … ”, “Candidate 934: If we eat sesame seeds during pregnancy period it will lead to abortion … ”, “Candidates 625&631:-My in laws told if we eat when we are in pregnant it will get abort so we didn’t eat that time”
Theme 5: Availability
Few participants emphasized the nonavailability of the food ingredients sometimes or always. This may imply a particular risk for these candidates to poor nutrition outcomes. They expressed that the nonavailability of food ingredients makes it difficult for them to use. The majority of participants did not claim the availability of the food ingredients as a difficulty to their daily dietary intake.
Week 3: Candidate 110:- Green gram whole are not available nearby us and for buying green gram we have to go long. So we use to make normal dosa which is preparing with black gram dal
Week 4: Candidate 816: In my locality I never see people using drumstick leaves
Week 7: Interviewer: Spinosus amaranth has red colored shoots. Generally, we have higher nutrients in spinosus amaranth than green amaranth leaves. Iron is rich in spinosus amaranth leaves … Is spinosus amaranth leaves available for you?, Candidate 519: It is available very less … Candidate 521&523: It is available in the fields …
Theme 6: Nutrition Environment
The amount of time spent preparing and cooking meals has the potential to affect diet quality and health. Lack of time to cook was commonly reported, especially with the work and kids. Lack of time among mothers for cooking is the critical finding of the present study.
Week 2: “Candidate 818: We don’t have the time with children … early morning all are busy with going to work ….”, “Candidate 816: My children don’t wait until the food is prepared … ”, “Candidate 925: Not like that, we don’t have time to cook that … ”, “Candidate 607: We have kids so we don’t have time to cook also it’s not possible to cook daily”
Week 3: “Candidate 903: Not about cost, but here all are going for work so they don’t have time … ” “Candidate 912: I don’t have time with children … ”, “Candidate 934: It is not possible to cook during work season …, We are going to field work, that’s why we don’t have time … ”
Week 4: CANDIDATE 816: I don’t have time to make that …
Week 5: “Candidate 819: Some people have lactating babies that’s why we are unable to cook all these … ”, “Candidate 913: It is not possible to make breakfast daily in the morning with a kid. That’s why we buy that from the hotel … If I have time I will definitely prepare that … ”
Week 6: “Candidate 323:- yes madam don’t have time to do”, “Candidate 924: Now it is field work season, so everyone is busy with work, so we don’t have time ….”, “Candidate 925: We know the process but we don’t have the time that is the problem … ”, “Candidate 934: Now all are busy with field work. We don’t have time to cook all these, and now we find it difficult to cook rice and curries with work … ”
Week 8: “Candidate 925: We don’t have time to make this, our time will be spent cooking rice and curry … ”, “Candidate 1027: We don’t have time with children … ”, “Candidate 925: I don’t have time. After my daughter comes I will definitely cook that … ”, “Candidate 405:I am working outside and no time, so we can make the ragi malt madam”
Week 9: “Candidate 404:- did madam we did only Sundays madam with kids we don’t have time”, “Candidate 933: We poli very occasionally at home, we don’t have time to cook. All are going to field work so we don’t have time … ”, “Candidates 606: We don’t have time to prepare because of kids”
Week 10: “Candidate 518: We don’t have time. We all go to field work ….”, “Candidate 520: We all are busy with field work. we don’t have time to cook all these …, “Candidate 719: I don’t have time to cook these items and all because of kids”, “Candidate 933: We are busy with field work so we don’t have time to do that ….
Week 11: “Candidate 308:- with kid don’t have time to did madam”, “Candidate 817: No, I don’t have time with kids … ”, “Candidate 817: Yes, it is very tasty. Actually we are about to make nutritional food, but we can’t because we don’t have time with kids and also the ingredients are not available for you …, “Candidate 829: We don’t have time. We went to Guntur for work. That’s why I don’t make that at home ….”, “Candidate 523: We all went to field work. We finish our household chores and cook some food and go to the fields daily … ”, “Candidate 1004: I know that but I don’t have time with kids … ”
Many mothers preferred ready-to-eat food rather than cooking food at home. Mothers do not eat healthily because of the ease of ready-to-eat food from shops, or restaurants, while about the same number stated they just do not have time to cook nutritious meals.
“Candidate 1004: Making chapati at home is very less because it increases body heat. And my mother in law doesn’t cook this because it takes a lot of time. We buy ready-made chapati from the shop. That packet contains 10 chapatis.”, “Candidate 902: Most of the time we buy from the shop. If we give 5 rupees to children they buy this from the shop. We eat this very less but my children eat that more … ”, “Candidate 903: In my area most of the people don’t make breakfast, I don’t go for any work so we make dosa, idly, poori, chapati and paratha … In my area most of them don’t cook, all of us buy from hotels … Because of time most of us buy from hotels other than cooking in home … ”, “Candidate 310: I don’t cook anything. but i am buy form outside tiffin madam”, “Candidate 913: It is not possible to make breakfast daily in the morning with a kid. That’s why we buy that from the hotel … If I have time I will definitely prepare that … ”, “Candidate 902: We can’t do that, but we eat poli from the shop … ”, “Candidate 925: We buy weakly one time from the sweet shop.”, “Candidate 925: We make very rarely, mostly we buy from the shop … ”, “Candidate 925: Tea also we don’t make at home we drink that at hotel … ”, “Candidate 925: We buy sesame seeds laddu from the shop … ”, “Candidate 1027: No, we buy them from the shop … ”, “Candidate 817: We never tried making poli at home. Only we buy from the shop … ”
Theme 7: Use and Utilization
Dietary interventions are frequently part of anemia programs. Particularly iron-rich foods are included in the diet plan for anemia. In the kitchen cooking, healthy food can help to reduce the anemia burden. Challengingly in the present study, many mothers expressed they do not know how to cook for the particular iron-rich ingredient. Few mothers stated they ever tried cooking.
Week 4: Drumstick leaves “CANDIDATE 625:-We heard but we don’t know how to prepare”, “Candidate 712:- I don’t know how to prepare”, “Candidate 819: I don’t know the process … ”, “Candidate 814: We don’t know … ”, “Candidate 607:- We don’t know the cooking process”etc
Week 6: “Candidate 112:-We don’t know how to prepare recipes using sesame seeds”, “Candidate 813&812: We don’t know the process … ” Candidate 912: We don’t know the process …, “Candidate 934: I don’t know … ”, “Candidate 925: I know that … ”, “Candidate 811: I don’t know how to use sesame seeds … ”,etc
Week 7: “Candidate 913: We don’t have elders to cook all these … ”, “Interviewer:- Ok. Don’t ever you cook? Candidate 631:-No madam”, “Candidate 321:- I never cook madam”.etc
Week 8: “Candidate 723: I don’t know my mother she used to prepare ragi malt at my home”, “Candidate 831: We don’t know how to add milk in ragi malt … ”, “Candidate 1007: We don’t know how to add milk in ragi malt … ”etc
Week 9: Interviewer: Do you have any idea of preparing bobbatlu? “Candidate 101,103: No madam.”, “Candidates 508,511,512: No madam”, “Candidate 113: I don’t know”, “Candidates 606,607: No madam”, “Candidate 1027: I tried that but it is not well cooked … ”, “Candidate 909: I don’t know how to make that?”, “Candidate 720: We don’t know how to prepare” etc
Week 10: Black gram laddu: “Candidate 113:-I don’t know how to cook, “Candidate 206:- we don’t know the process”, “Candidate 520: I don’t know about this ….”. “Candidate 527,532,529:- I also don’t know madam”, “Candidate 530:- I don’t do laddu madam”, “Candidate 824: We don’t know how to make this … ”, “Candidate 1004: I don’t know how to make that … ”, “Candidate 1009: I don’t know … ”, “Candidate 1027: We don’t know how it is prepared …, “Candidate 1028: We never asked them and they also didn’t tell us … ”etc
Week 11: Ponnaganni Chapathi: “Candidate 212:- yes madam but we don’t cook ever”, “Candidate 807: I don’t even know how to make it and I can’t make that … ”, “Candidate 807: I don’t know … ” etc
Arduously mothers do not know how to cook iron-rich food in particular. Most mothers do know cooking but how to cook to retain iron content and other nutrients in food was missing. Almost all women practiced washing green leafy vegetables after cutting.
“How did you wash your green leafy vegetables?”, “Candidate 324,318:-clean after cut madam”, “Candidate 404:- wash after cut madam”, “Candidate 423:- clean after cut madam”, “Candidate 313: washing after cutting the green leaves”, “Candidate 905: We wash it after chopping … ” etc
Candidate 607: Long ago my mother in law made chutney with these leaves but I don’t know how she made that …
Pesarattu: Candidate 311: I know this cooking process but I don’t know how it to make
Candidate 913: It’s true. Last time you showed us drumstick leaves dal I cooked that at home and my husband likes that. If you tell me now to make amaranth curry then I cooked that at home. I don’t know how to cook all these ….
The present study also identified a lack of knowledge of iron-rich food ingredients among some mothers. Many mothers do not know of the benefits of good nutrition of many routinely consumed food items in their diet. Knowledge of adding iron-rich foods to the diet to get more iron and help fight iron deficiency anemia was lacking. Many mothers do not know much about iron-rich food ingredients from their parents, grandparents, or in-laws.
Week 2: “Do you know any benefits of ragi laddu, Candidate 321,324: - We don’t know”, “Candidate 113:- No madam”, “Candidate 311,325,327,328:- candidate are saying no madam”. etc.
Week 3: “Did you know the health benefits of green gram?, Candidate 1007: We don’t know the benefits but we eat that … ”, “Candidate 924: We don’t know that”, “Candidate 816: I don’t know …, “Candidate 829: No … ”, “Candidate 1027: We know only eating, we don’t know the benefits … ” etc
Week 4: Do you know about nutritional values of drumstick leaves? Candidate 726:- We know only it is good for our health. Remaining values and all I don’t know madam”. etc.
Week 5: Candidate 812: We only think it is good, we don’t know the benefits … etc.
Week 6: “Interviewer:-Do you know the nutritional values of sesame seeds? Candidates 607&608:-No madam”, “Candidates 625&631:-We don’t know madam” etc.
Week 7:Amaranth Curry: “Interviewer:Do you know the nutritional values of these leaves?, Candidate 112&133:- No madam”, “Candidate 705&722:- No madam” etc.
Week 8: “Candidate 311: - I will drink ragi java but I don’t know benefits of the ragi flour”, “Candidate 730: I don’t have any idea madam”, “Candidate 723: I don’t know madam”, “Candidate 113:- No madam”, “Candidate 508:- No madam” etc.
Week 9: “Interviewer: Do you know the nutritional values of dates?”: “Candidate 101,103:We don’t know”, “Candidate 113: No madam”, “Candidates 606,607: No madam.”, “Candidate 819: We don’t know … ” etc.
Week 12: Coriander Chutney: “Interviewer: Do you know the nutritional values of these?”, “Candidate 512: We don’t know madam it gives good smell and taste to the curry so we are using”etc.
Food fads in diets restricted mothers for food groups or nutrients may result in missing out on the health benefits that an iron rich diet can bring.
Week 4: Candidate 719: “While cooking drumstick leaves smell will come so we are not having interest to cook
Alarming number of mothers mentioned they Do not eat leafy vegetables, Do not use drumstick leaves, Do not use ragi flour, Do not use the iron rich ingredient, Do not use whole green gram etc.
Week 10: Candidate 925: “We don’t make them. When a girl becomes mature we make these laddu to them and also we make these black gram laddu to children who are very weak …
Week 8: Candidate 516: We take more sorghum flour for rotis. We don’t use ragi flour that much. Normally ragi flour is used by pregnant ladies more
Discussion
Weekly local recipe talk in the mother’s kitchen is the first of its kind of health education series to explore unknown risk factors for anemia among tribal lactating mothers. A total of 340 mothers and children were enrolled in the study and with a response rate of 73.6%. After three months of following, 315 were studied in end line with an attrition rate of 7.3%. One-fifth of the mothers were aged less than or equal to 20 years (19.1%). Nearly one-fifth of the mothers were married at age less than 18 years (22.4%). About 41.8% of mothers were not literate or less than primary class. The corresponding figures for fathers were 40% non-literate or less than primary class. Census 2001 reported in Andhra Pradesh, among all STs 48.3% were not literate or below primary.11 Census 2011 reported the ST literacy in Guntur district in Andhra Pradesh to be 46.45%.7 In 2021 the present study reported of the total studied mothers, 84.7% were homemakers and three-fourth (75%) of the husbands were laborers and 6.5% were farmers. As per census 2011, out of total STs workers in Guntur district, Andhra Pradesh, agricultural labourers constituted 71.25% and farmers 6.97% respectively.12
Primary Census Abstract for the total population, scheduled castes, and scheduled tribes, 2011 mentioned Andhra Pradesh had a 5.53% ST population.13 The percentage of ST Total Population to District Total Population in Guntur is 5.06%.12 In the present study, of the total 27%, 24.7%, and 30.9% of mothers belonged to Yerukulas, Yenadis, and Lambadi/Sugali tribes, respectively. Ten percent of women belonged to Chenchu. Primary Census Abstract for the total population, scheduled castes, and scheduled tribes, 2011 also reported Yerukulas, Yenadis, Lambadi/Sugali, and Chenchu tribes to be dominant tribes in Guntur district, Andhra Pradesh.14
Nearly half (47.6%) of study participants lived in Kutcha houses or Semi-pucca houses compared to 41.3% as reported by Census 2011. Of the total 139 (40.9%) had Consanguineous marriages. Nearly three-fourth of the study participants belong to lower (47.4%) or lower-middle (32.9%) socio-economic strata using the modified B.G. Prasad scale for May 2021. A study in 2012 reported that 85.9% population of tribes in Andhra Pradesh were below the poverty line.15
The developing world has the highest frequency of anemia, which has multiple reasons. ST women are more likely to be under nourish as a result of their poor living conditions, eating habits, healthcare system availability, accessibility, and cost, education standard, awareness level, and multiple pregnancies. In the baseline, survey anemia was significantly more among mothers who had menarche at an age less than 13 years, with low literacy status of mothers. Anemia was almost double among mothers with a parity of three or more. After a follow-up of 3 mothers’ anemia was significantly associated with the lower and lower-middle socioeconomic status of a mother. In multivariate analysis, anemia was significantly associated with the socioeconomic status of a mother and the age of the last child. Similarly, anemia was found to be significantly associated with epidemiological factors such as age, respondents’ education, and socioeconomic status in a cross-sectional study conducted in Bhubaneswar, Orissa, involving 240 women of reproductive age.16 A study mentioned underweight among reproductive-age women is influenced by age, socio-economic status, literacy status, area of residence, marital status, etc.17
A national survey of 26 states in India stated women’s education and standard of living have a key role in reducing anemia.18 Anemia was linked to lower household income (p = 0.022) and lower husband education (p = 0.021) in a study.19 The low socioeconomic status of marginalized groups has resulted in widespread anemia and undernutrition, with women suffering the poorest health outcomes. Low socioeconomic status, very low literacy rates, poverty, and more live births may have contributed to the women of the Munda community having lower hemoglobin levels.20
The present study recorded a few families’ food acceptancy concerns and family restrictions that restrict the intake of iron-rich food of mothers. A study stated during the period when reproductive women are in the early years of marriage they are under the supervision of the mother-in-law. Mother-in-law significantly impacts the nutrition status of pregnant women.21 Anemia was related to women who shared decision-making authority with others in the home.19
In the present study, few mothers mentioned some food accessibility issues. Mothers who do not have access to iron-rich dietary items make it much more difficult to prepare an iron-rich diet. In addition, few women were dependent on limited and low-cost ingredients due to a lack of amenities and a poor income. Inappropriate cooking has been related to a lack of nutrients in the diet. Cooking techniques have an impact on moms’ daily food intake and overall nutritional health. Iron insufficiency is caused by insufficient quantities, dilution, or occasional consumption of iron-rich dietary ingredients in recipes, which has a detrimental influence on health. Only a few participants said that the food items were not always or occasionally unavailable. This might indicate a higher likelihood of poor nutrition outcomes for these people. They stated that the lack of food item availability made it tough for them to use.
The amount of time mothers spends preparing and cooking meals can have an impact on the quality of diet and health. There was a lot of talk about not having enough time to cook, among mothers, especially with work and kids. In addition to many own factors, the lack of time among tribal mothers to cook in the present study is one of the most important factors is that mothers do not have enough time to cook. A study was conducted on five focus groups with pregnant individuals (n = 20) in Southeast Michigan in 2019 regarding the mental energy of meal planning, family preferences, and time constraints to healthy home cooking.22
Surprisingly, many mothers in the present study stated that they do not know how to cook at all and how to cook the particular iron-rich item. This is showcased in the large practice of consuming ready-to-use food. Also, a few mothers admitted they never tried cooking. Pulses were consumed less frequently in a survey of Midwestern US University students due to unfamiliarity with them, a lack of awareness of their nutritional advantages, and a general lack of cooking self-efficacy.23
In the present study, lack of nutritive knowledge of mothers of commonly available food items was more worrisome. A study from Australia revealed a significant positive correlation between nutrition knowledge score and iron intake with r = 0.25 (P = 0.01).24 Nutrition knowledge was found to be strongly related to healthy eating in adult research, and the impact remained even after adjusting for demographic characteristics.25
Weekly local mother kitchen recipe talks not only promote optimal nutrition and health in women and children but also address food insecurity in families as a whole. The study provided a platform for mothers to share their experiences and learn about iron-rich diet. Weekly local mother kitchen recipe talks must be ramped up as an addition to supplemental nutrition services provided by ICDS. Weekly local mother kitchen recipe talks are not difficult to sustain. The inclusion of this evidence-based Weekly local mother kitchen recipe intervention in the current ICDS programme will be a blessing for young mothers who are illiterate, inexperienced, and financially disadvantaged. The study had limitation namely weekly local mother kitchen recipe talks were informal group discussion.
Conclusion
The food habits and lifestyle patterns of tribal mothers differ from one another. Food consumption patterns alter with socioeconomic status even within the same tribal group. Anemia is increased by poverty, which is compounded by a lack of awareness and lack of cooking skills. In recent years, the indigenous people have seen a social, economic, and cultural upheaval. To understand inequities in dietary intake, cost-effective, creative, and adaptive interventions like Weekly local mother kitchen recipe talks are urgently needed to design health program.
Acknowledgment
Our sincere gratitude to Prof (Dr.) Mukesh Tripathi sir, Director AIIMS Mangalagiri for guidance and support. We are grateful to Mrs. B Manoranjani, Project Director, ICDS, Guntur, Andhra Pradesh for her immense support. We also thank Child development project officers, Anganwadi workers and Anganwadi helpers, Guntur, Andhra Pradesh for the time and coordination. We thank Mrs. Alluri Vasanthi and Mrs. Veerabathina Kamala, project staff, ICMR Extramural 4621-2020, Department of Community and Family Medicine, AIIMS Mangalagiri for their commendable work. Our Special thanks to Dr. Cyanam Anjali Devi, visiting Professor, Department of Food and Nutrition, Osmania University, Hyderabad, Dr. Rupsa Banerjee, Assistant Professor, International Institute of Health Management Research, New Delhi, Dr. Desham Chelimela, Assistant Professor, Community Medicine, Malla Reddy women's college, Hyderabad, Dr. Navya Krishna Naidu, Tutor, Department of Community and Family Medicine, AIIMS Mangalagiri for training the staff. We also thank Mrs. Archana Gupta, Chartered accountant and Dr P. Siva Santosh Kumar, Senior Resident, Department of Community and Family Medicine, AIIMS Mangalagiri for assisting in data coding and cleaning. We thank all the participant mother's for their active participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Indian Council of Medical Research, Extramural Adhoc Project 4621-2020.
Disclosure
Dr Arti Gupta reports a patent Copyright for Iron rich food recipe from Mothers kitchen book issued to Copyright authority of India. The authors report no other conflicts of interest in this work.
References
1. Report of The Expert Committee On Tribal Health, Tribal Health in India, Bridging the gap and a Roadmap for the Future, Policy Brief, Ministry of Health and Family Welfare, Government of India and Ministry of Tribal Affairs, Government of India. Available from: https://nhm.gov.in/index1.php?lang=1&level=1&sublinkid=1110&lid=630.
2. Ministry of Tribal Affairs: govt of India. Available from: http://tribal.nic.in.
3. Nutrition in India. National Family Health Survey (NFHS-4). Available from: http://www.rchiips.org/nfhs/nutrition_report_for_website_18sep09.pdf.
4. Guidelines for Control of Iron Deficiency Anaemia. Adolescent Division, Ministry of Health and Family Welfare, Government of India; 2013.
5. Bharat AM. Department of Family Welfare, Ministry of Health & Family Welfare, Government of India. Available from: http://vikaspedia.in/health/health-campaigns/anemia-mukt-bharat.
6. Maternal IFA Supplementation Score Card. Anemia Mukt Bharat, Ministry of Health and Family Welfare, Government of India. Available form: https://anemiamuktbharat.info/wp-content/uploads/2021/03/MH-Score-Card-Anemia-up-to-Jan21-01-03-2021.pdf.
7. National Family Health Survey (NFHS - 5), 2019–21, Ministry of Health and Family Welfare, Government of India. Available form: https://dhsprogram.com/pubs/pdf/FR375/FR375.pdf.
8. Salmuth V, Brennan E, Kerac M, McGrath M, Frison S, Lelijveld N. Maternal-focused interventions to improve infant growth and nutritional status in low-middle income countries: a systematic review of reviews. PLoS One. 2021;16(8):e0256188. doi:10.1371/journal.pone.0256188
9. Ahamed F, Yadav K, Kant S, Saxena R, Bairwa M, Pandav CS. Effect of directly observed oral iron supplementation during pregnancy on iron status in a rural population in Haryana: a randomized controlled trial. Indian J Public Health. 2018;62(4):287–293. doi:10.4103/ijph.IJPH_313_17
10. Angeles-Agdeppa I, Monville-Oro E, Gonsalves JF, Capanzana MV. Integrated school based nutrition programme improved the knowledge of mother and schoolchildren. Matern Child Nutr. 2019;15 Suppl 3(Suppl3):e12794. doi:10.1111/mcn.12794
11. Andhra Pradesh, Data highlights: the scheduled tribes Census of India; 2001. Available from: https://censusindia.gov.in/tables_published/scst/dh_st_andhra.pdf.
12. Statistical Abstract, Andhra Pradesh-2017. Available from: https://core.ap.gov.in/cmdashboard/Download/Publications/Excels/Statistical%20abstract%202017.xlsx.
13. Census of India. Tribal Population In India- How Many, Where Etc. Dr. C. Chandramouli, Registrar General & Census Commissioner, India, Ministry Of Home Affairs; 2011. Available from: https://www.nhm.gov.in/images/pdf/Announcement/Dr_Chandramouli.pdf.
14. Tables_ Basic Statistics As Per Census 2011, Andhra Pradesh.xls. Available from: https://aptribes.gov.in/pdfs/table6.pdf.
15. Babu KS. Socio-economic and health conditions of some major tribes in Andhra Pradesh. Social Work Chronicle. 2012;1(2):31–49.
16. Panigrahi A, Sahoo PB. Nutritional anemia and its epidemiological correlates among women of reproductive age in an urban slum of Bhubaneswar, Orissa. Indian J Public Health. 2011;55(4):317–320. doi:10.4103/0019-557X.92415
17. Hashan MR, Rabbi MF, Haider SS, Das Gupta R. Prevalence and associated factors of underweight, overweight and obesity among women of reproductive age group in the Maldives: evidence from a nationally representative study. PLoS One. 2020;15(10):e0241621. doi:10.1371/journal.pone.0241621
18. Bharati P, Som S, Chakrabarty S, Bharati S, Pal M. Prevalence of anemia and its determinants among nonpregnant and pregnant women in India. Asia Pac J Public Health. 2008;20(4):347–359. doi:10.1177/1010539508322762
19. Krupp K, Placek CD, Wilcox M, et al. Financial decision making power is associated with moderate to severe anemia: a prospective cohort study among pregnant women in rural South India. Midwifery. 2018;61:15–21. doi:10.1016/j.midw.2018.02.014
20. Sucharithadevi S, Tejaswini E, Devi S, et al. Nutritional status of rural and tribal pregnant woman of Karimnagar district, Telangana. Pharma Innovation J. 2017;6:479–481.
21. Varghese R, Roy M. Coresidence with mother-in-law and maternal anemia in rural India. Soc Sci Med. 2019;226:37–46. doi:10.1016/j.socscimed.2019.02.027
22. Garcia T, Duncanson K, Shrewsbury VA, Wolfson JA. A qualitative study of motivators, strategies, barriers, and learning needs related to healthy cooking during pregnancy. Nutrients. 2021;13(7):2395. doi:10.3390/nu13072395
23. Winham DM, Davitt ED, Heer MM, Shelley MC. Pulse knowledge, attitudes, practices, and cooking experience of midwestern US university students. Nutrients. 2020;12(11):3499. doi:10.3390/nu12113499
24. Leonard AJ, Chalmers KA, Collins CE, Patterson AJ. The effect of nutrition knowledge and dietary iron intake on iron status in young women. Appetite. 2014;81:225–231. doi:10.1016/j.appet.2014.06.021
25. Swaminathan S, Ghosh S, Varghese JS, Sachdev HS, Kurpad AV, Thomas T. Dietary iron intake and anemia are weakly associated, limiting effective iron fortification strategies in India. J Nutr. 2019;149(5):831–839. doi:10.1093/jn/nxz009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.