Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Exploring the Support and Involvement of Family Caregivers for Reablement Programs: A Qualitative Study
Authors Mouchaers I ![]() , Metzelthin S, van Haastregt J, Vlaeyen E, Goderis G, Verbeek H
, Metzelthin S, van Haastregt J, Vlaeyen E, Goderis G, Verbeek H
Received 2 June 2023
Accepted for publication 15 September 2023
Published 11 October 2023 Volume 2023:16 Pages 2993—3005
DOI https://doi.org/10.2147/JMDH.S424147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ines Mouchaers,1– 3 Silke Metzelthin,1,2 Jolanda van Haastregt,1,2 Ellen Vlaeyen,4,5 Geert Goderis,3 Hilde Verbeek1,2
1Department of Health Services Research, Faculty of Health Medicine and Life Sciences, CAPHRI Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; 2Living Lab in Ageing and Long Term Care, Maastricht, the Netherlands; 3Department of Public Health and Primary Care, Academic Centre for General Practice, KU Leuven, Leuven, Belgium; 4Department of Public Health and Primary Care, Academic Centre for Nursing and Midwifery, KU Leuven, Leuven, Belgium; 5Faculty of Medicine and Life Sciences, Hasselt University, Hasselt, Belgium
Correspondence: Ines Mouchaers, Department of Health Services Research, P.O. Box 616, Maastricht, 6200 MD, the Netherlands, Tel +31-43 388 28 15, Email [email protected]
Background: Reablement is a person-centered, holistic approach promoting older adults’ participation through social, leisure, and physical activities. Family caregivers are seldom involved in reablement services despite their wish to be an active member of the care team and expressing a need for more support and recognition. The voice of family caregivers is often forgotten when evaluating services such as reablement. Little is known how family caregivers can be involved and supported more effectively in reablement services, therefore the aim of our research is to investigate the perceived support and involvement of family caregivers.
Methods: As part of the TRANS-SENIOR project, we studied perceived support and involvement of family caregivers during and after geriatric rehabilitation, a setting in which principles of reablement, like goal setting and training of daily activities, are applied. In total, fourteen semi-structured interviews were conducted with family caregivers of people admitted to a geriatric rehabilitation facility. Thematic analysis was used.
Results: Results reflected four themes: (1) support for family caregivers, (2) involvement in care, (3) trusting care professionals, and (4) asking for and accepting support. Family caregivers’ experiences with support from care professionals were mainly ambivalent. While caregivers expressing a lack of support and information whilst also indicating that they do not expect to be supported by care professionals. Regarding involvement, caregivers wanted to be involved; ie express their opinion and be involved in decision-making. However, more involvement could also lead to a higher burden.
Conclusion: There is a discrepancy between the perceived support and involvement of family caregivers, their expressed needs, and their expectations of care professionals. A personalized approach is needed to create room for the family caregiver to be an active participant in the care process while also providing the right amount of support, when preferred by the caregiver.
Keywords: informal care, geriatric rehabilitation, primary care, home care
Introduction
The majority of older adults prefer to remain living at home for as long as possible and as independently as possible, even those with frail health and challenging social situations.1,2 An approach to promote independent living among older people is reablement. Reablement is a person-centered, holistic approach that promotes older adults’ active participation in daily activities through social, leisure, and physical activities chosen by the older person in line with their preferences, either at home or in the community.3 Within reablement, care professionals identify the older person’s capabilities and opportunities to maximize their independence by supporting them in achieving their goals, through participation in daily activities, home modifications and assistive devices, and involvement of their social network.3–6 Although the evidence on the effectiveness of reablement remains mixed.7–9 The approach has shown promising results related to activities of daily living (ADL) functioning, quality of life (QoL), and well-being of older adults.9–12
According to the internationally accepted definition of reablement,3 making use of clients’ social network is a strategy to reach their goals. However, previous studies have shown that family caregivers are seldom involved in reablement or are insufficiently supported throughout the process, often resulting in a higher experienced burden.13–16 When involved, they often lack the right information and advice while providing care for their relative.13,14 Moreover, family caregivers expressed a wish for more support and recognition of their needs (eg a break from providing care).13,14 They also indicated that they wanted to be involved and participate in the decision-making regarding care and to be a contributor to the care process of their relative.13,17,18 Insufficient preparation, lack of information and education, poor communication and collaboration with care professionals, and lack of involvement of the family caregivers.19–21 often results in increased anxiety and stress, social isolation, decreased quality of life, financial difficulties, and worse perceived health of the caregiver.21–25
Reablement is not common practice yet in the Netherlands, however, principles of reablement, such as the goal setting aspect, being delivered by an interdisciplinary team of care professionals, and the shared goal of enabling older adults to return or remain at home after regaining their independence, are integrated in geriatric rehabilitation.3,26 Moreover, introducing reablement after geriatric rehabilitation could contribute to maintaining the progress made by the older adult; it could bridge the gap between the regulated rehabilitation environment and clients’ own home environment by focusing on relearning daily skills in that unregulated home environment. Compared to reablement, support for family caregivers seems more developed in geriatric rehabilitation; for example, some geriatric rehabilitation facilities in the Netherlands took on board a consultant on informal care to provide the right support to the caregiver.27 Since little is known about how family caregivers can be involved and supported more effectively during reablement services, we aimed to understand the lived experiences regarding support throughout and involvement in care of family caregivers who care for someone who has been admitted to a geriatric rehabilitation facility. This setting was chosen because of its similarities with reablement and since reablement is not common practice yet in the Netherlands. Getting insight into their experiences is valuable to improve reablement services and to understand how adequate support for family caregivers should be integrated. The aim of this study is to gain insight into the perceived support and involvement of family caregivers during the care process in geriatric rehabilitation and to explore how this support and involvement can be optimized in their opinion.
Materials and Methods
Design
The current study has a qualitative exploratory research design and is based on a phenomenological approach from Heideggerian’s hermeneutic perspective. This approach allows researchers to understand a phenomenon (ie support throughout and involvement in care) as experienced by family caregivers through their stories.28,29 The COREQ guideline was used for the reporting of this study.30
Setting
The study was conducted at the geriatric rehabilitation facility of two large healthcare providers that offer long-term care services in the south of the Netherlands. Geriatric rehabilitation is defined as
A multidimensional approach of diagnostic and therapeutic interventions, the purpose of which is to optimize functional capacity, promote activity and preserve functional reserve and social participation in older people with disabling impairments.26
The goal of geriatric rehabilitation is to enable older adults to return home after successfully completing their rehabilitation trajectory.26 In the Netherlands, a care physician, who is specialized in the care of older persons, leads a multidisciplinary team which supports the older adult to work on their rehabilitation goals and regain independence.31 The average length of stay is about 39 days, after which the majority of patients return home.32 The geriatric rehabilitation facilities in this study pay specific attention to involving and supporting family caregivers throughout the rehabilitation process and the care transition afterwards (eg organized information sessions or employing a consultant on informal care, who offers guidance and support for family caregivers and helps arrange specific types of support, such as respite care).27 These facilities also have the ambition to optimize the support and involvement of family caregivers at their facility.
Participants and Recruitment
A convenience sample of family caregivers was recruited between May 2022 and December 2022.33 Family caregivers closest to the patient, who were providing care and support throughout the institutionalization, were invited to participate while their relative was admitted to the geriatric rehabilitation facility. Additionally, participants needed to be able to participate in the interviews (ie understand and speak the Dutch language). We aimed to include different family caregiver profiles based on, for example, relation type (eg spouse, child, neighbor, etc.), living situation (living with the patient in the same house or not), or working status (eg working, unemployed, retired, etc.). Eligible family caregivers were asked by staff of the healthcare organization whether they were interested in participating in the research and if they could share their contact information with the research team. When interested, researcher IM contacted the participants by telephone to provide additional information about the aim and purpose of the research. Afterwards the interview was planned. Before the start of the interview, the researcher conducting the interview introduced herself as well as her role in the research project. Subsequently, participants received information about the study on paper and orally and were asked to provide written informed consent. Participants were included until data saturation was reached. There was no relationship established between the participants and the researcher conducting the interviews prior to the start of the study.
Data Collection
Background information was collected through a questionnaire, including date of birth, gender, marital status, number of children, educational level, work status, relationship to the patient, reason for the patient’s admission, if and how long they provided care to their relative before admission, hours (per week) of informal care before admission, and if there were other caregivers involved. Semi-structured interviews were conducted between May 2022 and December 2022 in a serial manner either in the rehabilitations facility or at their home. Preferably, participants were the only person present at the interview, however, it was not prohibited that their partner was present in the room. Interviews were conducted by first author IM (MSc, female). At the time of the interviews IM was employed as a PhD candidate with basic experience and training in qualitative research methods. We aimed to interview family caregivers twice at different time points of the care process with a minimum of 4 weeks between both interviews, preferably one interview during inpatient geriatric rehabilitation of their relative and one after discharge, to get a comprehensive view of their experience. A semi-structured interview guide was used, focusing on two overarching topics: (1) their perceived support and involvement during the care process in geriatric rehabilitation and (2) their needs and wishes regarding support and involvement and how support and involvement can be optimized. No field notes were made during or after the interview. Table 1 provides an overview of example questions per overarching topic. All interviews were audio recorded. In order to increase the credibility and confirmability of the data, a member check was conducted after each interview by summarizing the findings and asking if the participant agreed or wanted something to be added. Interviews were planned for approximately one hour each.
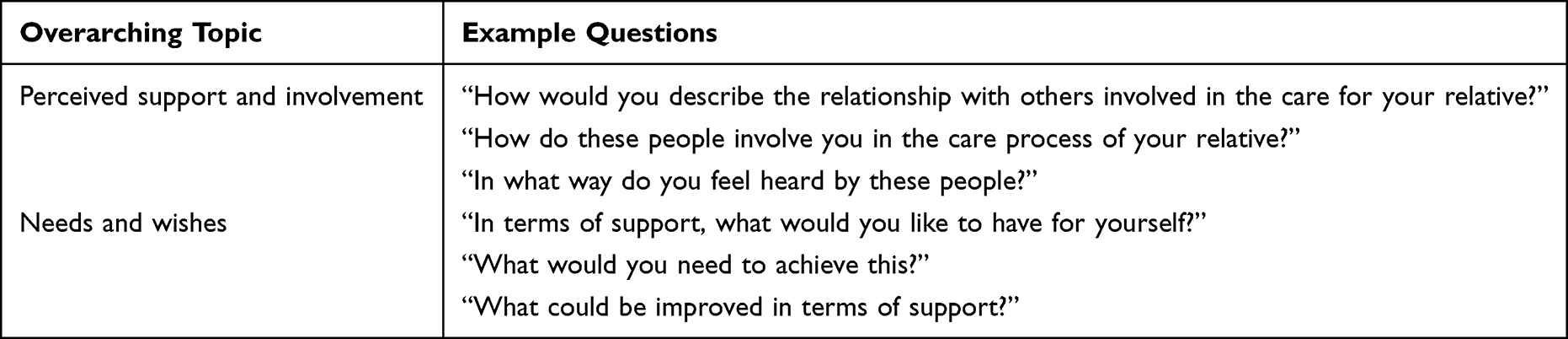 |
Table 1 Overarching Topics and Example Questions for the Semi-Structured Interviews |
Data Analysis
Data were anonymized, transcribed verbatim, and analyzed with support from qualitative data analysis software ATLAS.ti Windows (Version 22.2.5.0). A thematic analysis approach was used, following the steps identified by Braun, Clarke.34,35 A combination of open and axial coding was used. First, the researcher (IM) read the transcripts several times and made notes to familiarize herself with the data. Subsequently, open coding was used to analyze the data. Relationships between codes were identified by means of axial coding. Keeping the research questions in mind, axial coding led to the final themes. The analysis was an iterative process during which initial codes were recoded and relationships and themes were revised. The interviews were coded by the first author and summarized, and subsequently discussed with the second and last author throughout the analysis process. Disagreements were discussed within the research team.
Ethics
Ethical approval for this study was obtained from the FHML Research Ethics Committee (FHML-REC/2022/041). Informal caregivers voluntarily signed informed consent after they were fully informed about the purpose and procedures of the study and had the opportunity to ask additional questions or raise any concerns. The informed consent stated that participation in this study is completely voluntary and withdrawal from the study is possible at any moment, with or without providing a reason, by contacting one of the researchers. Additionally, the informed consent included publication of anonymized responses.
Results
Nine informal caregivers agreed to be interviewed. A more detailed description of the background information is presented in Table 2. Reasons for not participating in more than one interview were unavailability during admission of relative (n = 1) or not being willing to further participate after the first interview (n = 3). The interviews lasted 52 minutes and 50 seconds on average.
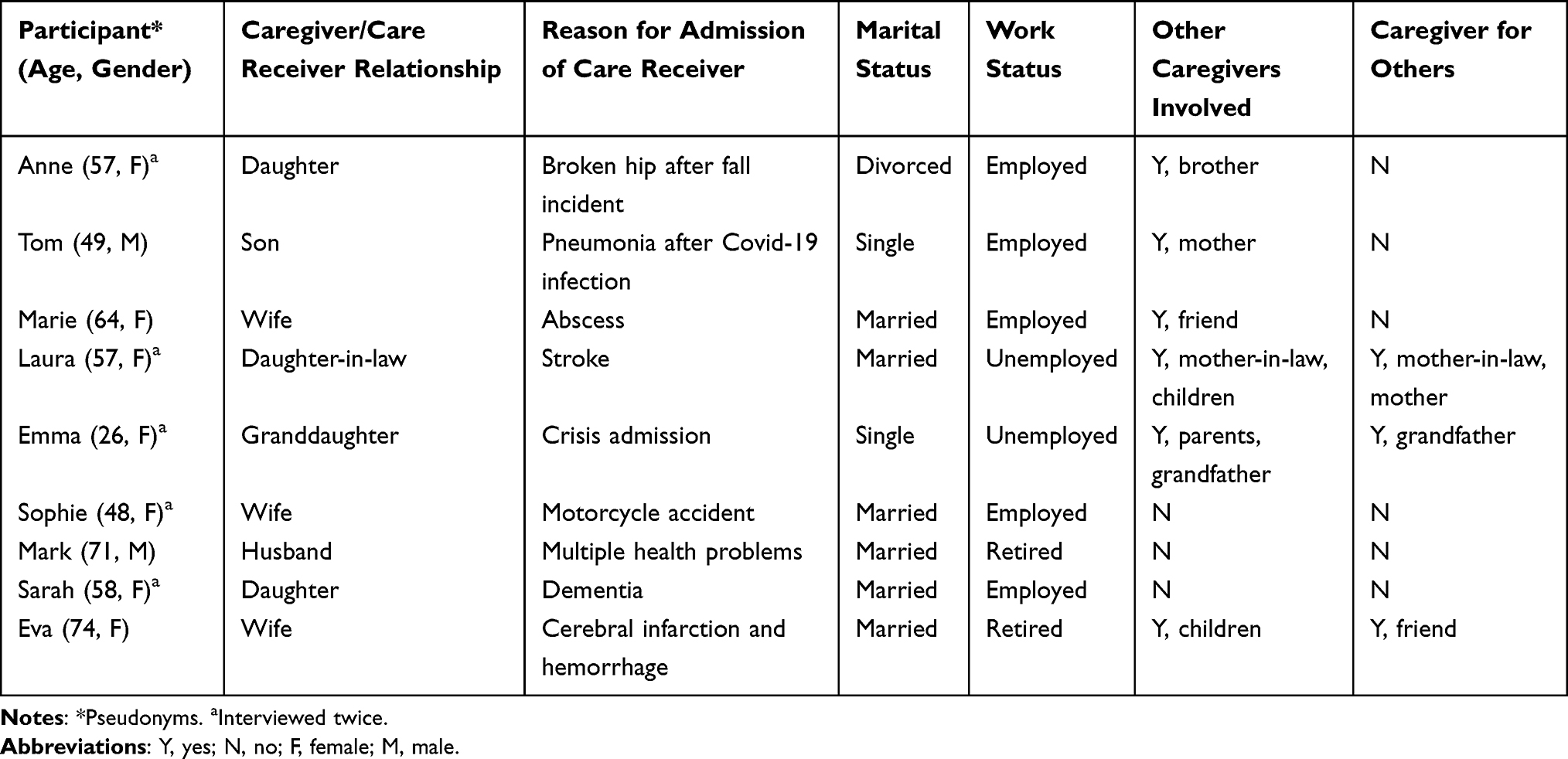 |
Table 2 Participants’ Profiles of Family Caregivers (n = 9) |
The results reflect four overall themes highlighting the family caregivers’ experiences: (1) support for family caregivers, (2) involvement in care, (3) trusting care professionals, and (4) asking for and accepting support (see Table 3). Themes and experiences were relatively similar for the first and the second interviews. Even when their relative lived at home, the family still reflected a lot on the time involved in geriatric rehabilitation.
 |
Table 3 Themes, Sub-Themes, and Description |
Support for Family Caregivers
Participants mentioned three different parties as important sources of support, namely care professionals involved in the care process of their relative, their social network, and their working environment.
Support from Care Professionals
The experiences with support from care professionals were mixed. Some family caregivers stated that they were very well supported by care professionals, whilst most others indicated that they did not receive a lot of support from the care professionals involved their relative’s care. For example, multiple caregivers pointed out that they experienced a lack of guidance during the admission or discharge of their relative and concerning how they could handle their new role as caregiver. Additionally, some participants indicated that they were never or seldom asked how they were doing and pointed out that the contact with care professionals was mostly about their relative:
My mother got discharged from the hospital and transferred to the rehabilitation facility, I knew that […] They brought her up to the second floor, but I didn’t know anything. So I’m at the facility, there was no one at the reception, and I thought ‘where is my mother?’ […] I do think it’s a shame […] I missed that bit of support here. (Anne)
Also, we were not asked, ‘how are you guys doing?’ or anything like that […] we’re not even asked, ‘are you all right?’ […] So yeah, in terms of informal care, there’s not really… (Emma)
No that [contact with doctor] is all about my mother. So I – I don’t think about that at all, now for once I want someone who – who listens to me. (Sarah)
Despite expressing experiencing a lack of support, caregivers also indicated that they did not expect care professionals to support them because that is not their job; their job is to look after their relative. Moreover, they could not see how care staff would be able to support them:
I don’t know if they can contribute to that [getting more time for himself]. I assume they are here to take care of my father, and not me. (Tom)
I think that as a partner – I don’t know if you can get a lot of support in that either – because every situation is different, of course. (Sophie)
However, when looking into the expressed needs of family caregivers, they were ambivalent with respect to their previous expectations regarding not receiving any support from care professionals. When asked about their needs and wishes, participants often indicated that informal care is a challenge and obligation. They wish to hand over most care tasks and just be a relative, which would indicate the need for more support from care professionals to take over basic care needs:
I just want to be able to live my own life again and not actually be at the service of my grandparents, as much as I love doing it for them. […] Yeah, I just want to have that peace of mind that she’s really in the right place [regarding received care] and that we’re not her caregivers anymore but can just go and visit grandma again. Just the way it used to be. (Emma)
Moreover, as mentioned before, family caregivers indicated that they experienced a lack of guidance during specific stages of the care process and more guidance is therefore desirable so that they do not have to figure everything out themselves:
When your relative is admitted then you [as care professionals] can’t say, ‘oh yeah, figure it out for yourself. That’s something for the informal caregiver and the family.’ I think that task is also yours [as care professionals], a bit of guidance. Not just for me, but that it’s also clear to the rest of the people [who care for someone who is admitted] […] There is still a lot to gain there. (Laura)
There is also a need to share their experiences with either professionals or peers. Participants mentioned that having a care professional who opened the door for them to ask questions or share concerns was highly appreciated. Especially the consultant on informal care was praised by family caregivers; they mentioned the consultant was “a relief” (Laura), “an open door” (Anne), “an eye opener” (Sarah):
There are, of course, several sons and daughters who are caregivers for their father and mother, and they are in the same situation as me or that you have, what do you call it, a peer group. […] Then those informal caregivers can sit together, and you get tips and ideas. […] That would provide recognition and acknowledgement. (Sarah)
I really liked the fact that she [the consultant on informal care] called me herself. I also really liked the fact that she says, ‘do you have an hour so we can really talk in person?’ I really like that you can tell her anything you like to say. (Sarah)
Support from Social Network
The perceived support from their social network (ie family members, friends, or neighbors) varied. When participants had a strong social network from which they got a lot of support, they experienced this as very helpful, and they were generally grateful for all the support provided. It also offered a form of relief. When participants mentioned being supported by their social network, it mostly related to offering emotional support, for example, by showing interest and compassion. However, in a few cases, the social network of the caregiver also offered more structural support, for example, by sharing responsibilities or taking over care tasks:
The love I get from the people around me. There’s a bunch of friends who say very often, sometimes twice a week: don’t you feel like coming over, having a coffee, or a glass of wine or something. And those are nice and such important things. (Eva)
Yes my parents do try to be careful not to overburden me. […] They really look after me. […] I just really didn’t have any more energy to go through that discussion [about the right type of care for grandmother] again. So then my mother was like ‘I’ll go and I’ll arrange what I can and we’ll see how it goes from there. (Emma)
However, not being supported by their network led to frustration because family caregivers were unable to share their story or experiences, or they felt alone in carrying out all tasks related to informal care:
That’s frustrating, frustrating that you hope your husband supports you in that or goes with you [to the rehabilitation facility] or says, ‘What can I do for you Sarah?’ […] That bit [of support], I missed that too. […] That also makes it exhausting that I do everything on my own again. (Sarah)
Although participants highly appreciated the support offered by their social network, it was often pointed out that this could also be overwhelming (eg too many texts or phone calls, which only cost time and energy); therefore, some people indicated that they did not look for this support:
However well intentioned, but when people are constantly texting and calling, ‘How is your mother? And how are you?’ That takes up way too much of my time; those are way too many stimuli. (Sarah)
Support from Working Environment
Participants who were still employed expressed that support from the employer and colleagues was much needed and appreciated, for example, being given time off to visit their relative and arrange things. Additionally, being able to vent to colleagues relieved stress, and it was comforting when colleagues showed interest and compassion. However, when the employer was not supportive, it only added to the burden and stress of family caregivers:
I have a good employer. They said, ‘Take your time, and then after that, if you can, come back to work.’ So I was lucky with that. […] They have been very accommodating. They also took those two weeks [during intensive care] very – I hardly had to take any leave. (Sophie)
If he [partner] comes home, then I just need that care leave. They were very difficult about that at work, which I found very unpleasant. […] Because I thought if it goes on like this, I’ll just drop out. I can’t handle all that, it’s just not possible. (Marie)
Involvement in Care
Involving family caregivers in care was discussed in three ways: by informing family caregivers, by consulting family caregivers, or by the participation of family caregivers. Most participants indicated that the involvement was mainly related to informing family caregivers, and included being able to consult care reports, meetings with family and care professionals, information evenings for relatives, or the possibility of attending therapy sessions.
With regard to informing, the experiences varied strongly among family caregivers; it was remarkable that it was often either a very negative or a very positive experience. Family caregivers mentioned that being updated about the status of their relative, receiving a call when something happened, or getting advice contributed to a positive experience. They expressed that they appreciated the amount of information they received, and they indicated that good communication also created a good relationship between them and care professionals. It was noticeable that these people were often the family caregivers who also felt well supported either by care professionals or their social network, who were satisfied with the care delivered, and who generally experienced a lower burden:
That information was incredibly good, and on the ward everything went perfectly. Yes, and in the rehabilitation institution likewise. We were always updated on what was going to happen and how the wound looked […]. Yes, that was really nice. You were very much involved. (Marie)
Contrary to the aforementioned positive experiences, most family caregivers indicated that they were insufficiently and/or incorrectly informed. This often led to frustration, could possibly affect their experienced burden, and had an influence on their relationship with care professionals. Being insufficiently or incorrectly informed was reflected in, for example, not being contacted when something happened to their relative (eg a fall incident) or expecting activities and certain services for their relative based on information folders, which in the end were not provided. Ultimately, these family caregivers expressed a high need for more (accurate) information and better communication with care professionals. Again, we see a possible relationship between the perceived support of family caregivers and their experienced burden; often the people who expressed a high burden and did not feel supported were also the people who felt they were insufficiently informed:
You just don’t know […] how things work there, you never get to speak to anyone, or you have to call, but. It’s not like you can just, when you’re there, just ask, ‘How do you guys think it’s going?’ It’s just. Yeah, you just have to hear it from her [grandmother], while that’s what she’s there [the rehabilitation facility] for, that we can’t believe what she says [because of her condition]. (Emma)
Family caregivers reported rarely being consulted when it came to the care process of their relative and the choices that needed to be made, although this was a strong desire across most of them. It was often mentioned that they wished they were asked more about their opinion because they felt that they knew their relative best and could be of added value when certain decisions had to be made by the care team:
That they listen actually. Listen better to you after all. […] Yes, you know him very well too. That they do listen, like, ‘Okay, it’s. It’s maybe not such a good idea what we’re doing now after all.’ Yes. I know they are the doctors of course, that first of all. But do listen to what – whatever the family thinks. I would have preferred that to be different. (Marie)
Being heard was an important aspect for family caregivers, and the majority of participants felt heard by the care professionals, for example, when they were given the opportunity to express their opinion, ask questions, or express their concerns. This was experienced as pleasant and was also appreciated by most family caregivers:
Knowing that time is taken for you and that even yesterday they said, ‘Do you have any questions?’ That I think, ‘Yes, indeed I have all kinds of questions written down.’ Just the fact that you know there will be a conversation. (Sarah)
Only one family caregiver mentioned something about being an active participant in their relative’s care process, rather than merely being informed or consulted like most other participants. She, for example, wanted to be involved in the decisions that were being made and have a say in this as an equal partner in the care process:
That’s just irritating, and I just want to be able to spar with someone: ‘What do you think?’ That I can help think about the care process. I would just really like that. Because I’ve obviously cared for her at home for so many months […] then if they [care professionals] don’t believe you […] Yeah, that’s just irritating. (Emma)
When asked if family caregivers wanted to be more involved in their relative’s care, many stated that, apart from more adequate information, they did not wish to be more involved because this could add to their perceived burden:
No, I’m fine like this and I think that’s also a bit because I – my head is so full. (Eva)
Trusting Care Professionals
Trust was pointed out as an important determinant of how family caregivers experienced the care process and their role as informal caregiver. Whether or not they trusted the care professionals involved in their relative’s care, contributed to their perceived burden and stress. Both a trusting and non-trusting relationship with the care providers was mentioned by participants. Having trust in the care professionals often seemed related to the satisfaction of family caregivers with the care provided and vice versa. For example, one caregiver mentioned that when they noticed that their relative was not washed in the morning, they had the feeling that they constantly had to oversee the care professionals and what they were doing. When they knew their relative was taken care of well, they could let go of their concerns more easily, indicating a trusting relationship with the care professionals:
Because it just kept going wrong in the rehabilitation facility and so much has gone wrong during the whole process, you have to keep trying to trust that things will go right there [nursing home]. But yes, it’s a bit of a balance between ‘Is it going well and can we trust them? (Emma)
Trusting care professionals was not only related to the care provided. It also became apparent that family caregivers who expressed that they trusted the care professionals involved in the care for their relative were the ones who overall had a positive experience with being supported by those care professionals.
Asking for and Accepting Support
It was noticeable that asking for help is not easy for family caregivers. This might be related to the fact that family caregivers do not feel that they should be supported because it is about their relative, as mentioned before. Additionally, when offered help from their social network, they often did not accept this. There are two apparent reasons for not asking and accepting support. On the one hand, participants did not want to burden others, such as family members or even care professionals.
You have to go and ask if you want something. It’s as simple as that. And that’s not such a strong point of mine. No, that’s me – that’s not me. Rather, I’m someone who does it myself. (Tom)
On the other hand, participants indicated that they do not want to hand over their responsibilities to others, mostly because they were used to doing everything on their own but also because they were afraid of other people’s opinions, which might possibly conflict with their own or the wishes of their relative:
I do it for my mother, and I am happy to do it, and maybe I don’t want to hand it over to anyone else either. […] My mother used to be there for me, and now we are going to turn the tables, and now I am there for her. (Anne)
Discussion
The aim of this study was to gain insight into the perceived support and involvement of family caregivers during the care process in geriatric rehabilitation and to explore how this support and involvement can be optimized in their opinion. The results of this study can be used to improve reablement services and provide insight into how to integrate adequate support for family caregivers. The results of this study reflected four main themes: (1) support for family caregivers, (2) involvement in care, (3) trusting care professionals, and (4) asking for and accepting support. Our findings highlight the variation in family caregivers’ perceived support and involvement.
Family caregivers’ experiences with support from care professionals were often ambivalent, expressing a lack of support and information whilst also indicating that they do not expect to be supported by care professionals. This is supported by Weisser et al,36 who also found that family caregivers experience ambivalent feelings between proactively seeking help and feeling disturbed by increasing numbers of meetings. Additionally, how family caregivers experienced the support they received and how they were involved often related to their perceived burden. This was also found by Boots et al,37 who discovered that family caregivers have a hard time identifying and expressing their needs, which is due to their high subjective burden experienced. When focusing on the needs that caregivers did express, we noticed a need for more guidance and better communication and information. Previous research also concluded that there is a need for more inclusion in the care process (eg being aware of the decisions made or being involved in the discharge planning) and both good communication and accurate information when caring for an admitted relative or during the transition back home.19,38,39 Especially in the beginning when family caregivers are new to their role, it is important that care professionals help them navigate this new role.40 Our results showed that trust between the family caregiver and the care professional is an important element throughout the care process. It is important to build a relationship of trust at the beginning of the process; this facilitates the acceptance of support and will ultimately reduce the burden.41 Besides support, involvement was also an important aspect of our findings. It became apparent that family caregivers wanted to be involved; ie wanting to be able to express their opinion and to be involved in decision-making. However, it is important to be cautious because more involvement could also lead to a higher burden. Previous research also stated that once a person becomes more dependent on care, family caregivers spent more time on care-related activities (ie become more involved), which was associated with a higher burden.42–44
Besides knowing what support needs to be provided to meet the needs of family caregivers, it is also important to reflect on how this support should be offered to family caregivers. Our results clearly indicated that family caregivers have difficulty asking for and accepting help, either because they did not want to burden others or they did not want to hand over responsibilities. Previous research found that family members often take on the role of caregiver as a sense of moral commitment based on family obligations and solidarity.45 Willemse et al46 also found that informal caregivers seldom look for professional support. Moreover, previous research states that family caregivers are reluctant to seek external support because they do not want to disclose family-related problems due to a sense of pride,47,48 but are also reluctant to accept help from other family members.49 Additionally, Willemse et al46 found that information on the possibilities was often lacking, and they stressed the necessity of proactively informing caregivers.46 Over the past years, multiple interventions have been described to support family caregivers in their role as a caregiver and to eventually reduce their perceived burden. These interventions use different approaches, such as respite care, psychosocial support (either in group or individual), education/skill-based interventions, assistive technology, or multicomponent interventions.50–55 However, often the family caregivers have to take the initiative themselves, while our findings clearly show that informal caregivers will rarely act proactive in this. Therefore, it is important to, as a care professional, proactively inform the informal caregiver about their options for support and offer a tailor-made, personal approach with enough room to participate in the care process when this is preferred by the informal caregiver.49
The aim of this research was also to inform reablement programs on how to integrate adequate support for family caregivers and how to involve them in reablement services. The previous section has already provided some implications for future practice. First, addressing the need for more guidance and information throughout their relative’s care process is an important element that should be integrated. This is also supported by Hjelle et al,13 who emphasize the importance of family caregivers’ need to receive but also give information. Additionally, making the family caregiver an equal member of the reablement team would make them feel heard and is an important strength of reablement interventions,13,56 but it could also relieve some of the burden by decreasing the feeling of being alone in the process.57 However, informal caregivers need to have a choice in the amount of involvement during the care process. Our study clearly indicated that this wish was not the same for every family caregiver. This finding is in line with previous research showing that family caregivers experience more burden, if they do not have a choice in the amount of involvement.58,59 It is also important that caregivers have someone they can turn to; however, this is often overlooked, so it would be beneficial to appoint a team member as single point of contact for the family caregiver for emotional support.14 To build a family–staff relationship, it is important that care professionals possess the right competencies and skills, eg being empathic, showing interest, etc.60 Last, since reablement focuses on improving well-being, knowing that their relative is supported in activities they value, could add to the caregiver’s trust, which was indicated in previous research to be a benefit of reablement services.57
Some methodological considerations have to be made. First, since we used convenience sampling at two sites, it could be possible that family caregivers who were much overburdened did not participate in our study, although their experiences could be of added value. However, we did manage to include a varied sample in terms of relation type, living situation, or working status, thus providing us with broad insight into the experiences of different family caregivers. Second, we gathered the experiences of family caregivers through (sequential) interviews. However, it could be argued whether this is the most suitable method to get an in-depth perception of participants’ experiences and whether other research methods in which a trusting bond is created between the participant and the reviewer (eg ethnographic research or patient journey method) would be more suitable Last, we did not interview family caregivers who were involved in reablement because it is not common practice yet in the Netherlands. We did, however, try to match the population and setting by choosing geriatric rehabilitation.
Conclusion
To our knowledge this is the first study investigating the perceived support and involvement of family caregivers for reablement programs and shedding light on their needs and wishes for future programs. This study shows that there is a discrepancy between the perceived support and involvement of family caregivers, their expressed needs, and the expectations they have of care professionals. Our findings build upon and reinforce previous research performed on the support and involvement of family caregivers. However, we also demonstrate new insights. Family caregivers say that they lack support and information, whilst also indicating that they do not expect more support or to be supported by care professionals. Additionally, regarding involvement, their experiences were either very positive or very negative. Family caregivers wished that they were consulted more often, but did not have a high need for participation. Trust is an important determinant of how family caregivers experienced the care process and their role as informal caregiver. Whether or not they trusted the care professionals involved in their relative’s care, contributed to their perceived burden and stress. Family caregivers have trouble asking for and accepting help, because they do not want to burden other or they do not want to hand over responsibilities. To respond to family caregivers’ needs, a personalized approach is needed to create room for the family caregiver to be an active participant in their relative’s care process, if preferred, while also providing the right amount of support. Although our findings give a good indication of what the support and involvement of family caregivers should look like, more research is needed to gain additional insight into the experiences of family caregivers who are involved in reablement services. Additionally, this paper makes suggestions on how to integrate adequate support for family caregivers and how to involve them in reablement services. However, these should be pilot tested in practice to make sure they are feasible and lead to an improvement in care.
Abbreviations
ADL, Activities of daily living; QoL, Quality of life; COREQ, Consolidated criteria for reporting qualitative research.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy or consent of research participants.
Ethics Approval and Informed Consent
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Maastricht University, Faculty of Health, Medicine and Life Sciences (approval number FHML-REC/2022/041, approved on the 25 April, 2022). Participants voluntarily signed informed consent after they were fully informed about the purpose and procedures of the study and had the opportunity to ask additional questions or raise any concerns. The informed consent stated that participation in this study is completely voluntary and withdrawal from the study is possible at any moment, with or without providing a reason, by contacting one of the researchers. Additionally, the informed consent included publication of anonymized responses.
Acknowledgments
We would like to thank all the family caregivers who participated in the interviews. Additionally, we would like to thank MeanderGroep Zuid-Limburg and Vitala+ for their participation and help with the recruitment of family caregivers. In particular, we would like to thank Hella Senden (MeanderGroep Zuid-Limburg) and Anjo Franssen (Vitala+) for their help herein.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No 812656 as part of the TRANS-SENIOR project (www.trans-senior.eu).
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Wiles JL, Leibing A, Guberman N, Reeve J, Allen RE. The meaning of “aging in place” to older people. Gerontologist. 2012;52(3):357–366. doi:10.1093/geront/gnr098
2. Smits CH, van den Beld HK, Aartsen MJ, Schroots JJ. Aging in the Netherlands: state of the art and science. Gerontologist. 2014;54(3):335–343. doi:10.1093/geront/gnt096
3. Metzelthin SF, Rostgaard T, Parsons M, Burton E. Development of an internationally accepted definition of reablement: a Delphi study. Ageing Soc. 2022;42(3):703–718. doi:10.1017/S0144686X20000999
4. Doh D, Smith R, Gevers P. Reviewing the reablement approach to caring for older people. Ageing Soc. 2019;2019:1–13. doi:10.1017/s0144686x19000813
5. Aspinal F, Glasby J, Rostgaard T, Tuntland H, Westendorp RG. New horizons: reablement - supporting older people towards Independence. Age Ageing. 2016;45(5):572–576. doi:10.1093/ageing/afw094
6. Metzelthin SF, Zijlstra GA, van Rossum E, et al. ‘Doing with.’ rather than ‘doing for.’ older adults: rationale and content of the ‘Stay Active at Home’ programme. Clin Rehabil. 2017;31(11):1419–1430. doi:10.1177/0269215517698733
7. Buma LE, Vluggen S, Zwakhalen S, Kempen GIJM, Metzelthin SF. Effects on clients’ daily functioning and common features of reablement interventions: a systematic literature review. Eur J Ageing. 2022;19:903–929. doi:10.1007/s10433-022-00693-3
8. Sims-Gould J, Tong CE, Wallis-Mayer L, Ashe MC. Reablement, reactivation, rehabilitation and restorative interventions with older adults in receipt of home care: a systematic review. J Am Med Dir Assoc. 2017;18(8):653–663. doi:10.1016/j.jamda.2016.12.070
9. Rostgaard T, Tuntland H, Parsons J. 1: introduction: the concept, rationale, and implications of reablement. In: Rostgaard T, Parsons J, Tuntland H, editors. Reablement in Long-Term Care for Older People: International Perspectives and Future Directions. Bristol: Policy Press; 2023:3–20.
10. Tessier A, Beaulieu M-D, McGinn CA, Latulippe R. Effectiveness of reablement: a systematic review. Healthc Policy. 2016;11(4):49–59.
11. Whitehead PJ, Worthington EJ, Parry RH, Walker MF, Drummond AE. Interventions to reduce dependency in personal activities of daily living in community dwelling adults who use homecare services: a systematic review. Clin Rehabil. 2015;29(11):1064–1076. doi:10.1177/0269215514564894
12. Resnick B, Galik E, Boltz M. Function focused care approaches: literature review of progress and future possibilities. J Am Med Dir Assoc. 2013;14(5):313–318. doi:10.1016/j.jamda.2012.10.019
13. Hjelle KM, Alvsvåg H, Førland O. The relatives’ voice: how do relatives experience participation in reablement? A qualitative study. J Multidiscip Healthc. 2016;10:1–11. doi:10.2147/JMDH.S122385
14. Wilde A, Glendinning C. ‘If they’re helping me then how can I be independent?’ The perceptions and experience of users of home-care re-ablement services. Health Soc Care Community. 2012;20(6):583–590. doi:10.1111/j.1365-2524.2012.01072.x
15. van Wieringen M, Broese van Groenou MI, Groenewegen P. Impact of home care management on the involvement of informal caregivers by formal caregivers. Home Health Care Serv Q. 2015;34(2):67–84. doi:10.1080/01621424.2015.1029185
16. Mouchaers I, Van Haastregt JCM, Verbeek H, et al. « Reablement » comme outil thérapeutique pour offrir aux personnes âgées une vie de qualité à domicile après une réadaptation gériatrique. Rev Med Brux. 2021;42(4):324–332.
17. Jakobsen FA, Vik K, Ytterhus B. The art of maintaining everyday life: collaboration among older parents, their adult children, and health care professionals in reablement. J Multidiscip Healthc. 2019;12:269–280. doi:10.2147/JMDH.S195833
18. Kraun L, De Vliegher K, Vandamme M, Holtzheimer E, Ellen M, van Achterberg T. Older peoples’ and informal caregivers’ experiences, views, and needs in transitional care decision-making: a systematic review. Int J Nurs Stud. 2022;134:104303. doi:10.1016/j.ijnurstu.2022.104303
19. Bauer M, Fitzgerald L, Haesler E, Manfrin M. Hospital discharge planning for frail older people and their family. Are we delivering best practice? A review of the evidence. J Clin Nurs. 2009;18(18):2539–2546. doi:10.1111/j.1365-2702.2008.02685.x
20. Lutz BJ, Young ME, Creasy KR, et al. Improving stroke caregiver readiness for transition from inpatient rehabilitation to home. Gerontologist. 2017;57(5):880–889. doi:10.1093/geront/gnw135
21. Moon M. The unprepared caregiver. Gerontologist. 2017;57(1):26–31. doi:10.1093/geront/gnw080
22. Bailes CO, Kelley CM, Parker NM. Caregiver burden and perceived health competence when caring for family members diagnosed with Alzheimer’s disease and related dementia. J Am Assoc Nurse Pract. 2016;28(10):534–540. doi:10.1002/2327-6924.12355
23. Makdessi A, Harkness K, Luttik ML, McKelvie RS. The Dutch objective burden inventory: validity and reliability in a Canadian population of caregivers for people with heart failure. Eur J Cardiovasc Nurs. 2011;10(4):234–240. doi:10.1016/j.ejcnurse.2010.08.006
24. Maffoni M, Giardini A, Pierobon A, Ferrazzoli D, Frazzitta G. Stigma experienced by Parkinson’s disease patients: a descriptive review of qualitative studies. Parkinsons Dis. 2017;2017:7203259. doi:10.1155/2017/7203259
25. Leroi I, McDonald K, Pantula H, Harbishettar V. Cognitive impairment in Parkinson disease: impact on quality of life, disability, and caregiver burden. J Geriatr Psychiatry Neurol. 2012;25(4):208–214. doi:10.1177/0891988712464823
26. Grund S, Gordon AL, van Balen R, et al. European consensus on core principles and future priorities for geriatric rehabilitation: consensus statement. Eur Geriatr Med. 2020;11(2):233–238. doi:10.1007/s41999-019-00274-1
27. Mantelzorgconsulent. Available from: https://www.mantelzorg.nl/onderwerpen/ondersteuning/mantelzorgconsulent/.
28. Kafle NP. Hermeneutic phenomenological research method simplified. Bodhi. 2011;5(1):181–200.
29. Starks H, Trinidad SB. Choose your method: a comparison of phenomenology, discourse analysis, and grounded theory. Qual Health Res. 2007;17(10):1372–1380. doi:10.1177/1049732307307031
30. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
31. Koopmans RT, Lavrijsen JC, Hoek JF, Went PB, Schols JM. Dutch elderly care physician: a new generation of nursing home physician specialists. J Am Geriatr Soc. 2010;58(9):1807–1809. doi:10.1111/j.1532-5415.2010.03043.x
32. Actiz. Infographic geriatrische revalidatiezorg; 2019.
33. Robinson RS. Purposive Sampling. In: Michalos AC, editor. Encyclopedia of Quality of Life and Well-Being Research. Dordrecht: Springer Netherlands; 2014:5243–5245.
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
35. Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol. 2022;9(1):3–26. doi:10.1037/qup0000196
36. Weisser FB, Bristowe K, Jackson D. Experiences of burden, needs, rewards and resilience in family caregivers of people living with motor Neurone disease/amyotrophic lateral sclerosis: a secondary thematic analysis of qualitative interviews. Palliat Med. 2015;29(8):737–745. doi:10.1177/0269216315575851
37. Boots LM, Wolfs CA, Verhey FR, Kempen GI, de Vugt ME. Qualitative study on needs and wishes of early-stage dementia caregivers: the paradox between needing and accepting help. Int Psychogeriatr. 2015;27(6):927–936. doi:10.1017/S1041610214002804
38. Hainstock T, Cloutier D, Penning M. From home to ‘home’: mapping the caregiver journey in the transition from home care into residential care. J Aging Stud. 2017;43:32–39. doi:10.1016/j.jaging.2017.09.003
39. Mitchell SE, Laurens V, Weigel GM, et al. Care transitions from patient and caregiver perspectives. Ann Fam Med. 2018;16(3):225–231. doi:10.1370/afm.2222
40. Wolfs CAG, de Vugt ME, Verkaaik M, et al. Rational decision-making about treatment and care in dementia: a contradiction in terms? Patient Educ Couns. 2012;87(1):43–48. doi:10.1016/j.pec.2011.07.023
41. Zegwaard MI, Aartsen MJ, Grypdonck MH, Cuijpers P. Trust: an essential condition in the application of a caregiver support intervention in nursing practice. BMC Psychiatry. 2017;17(1):47. doi:10.1186/s12888-017-1209-2
42. Kim H, Chang M, Rose K, Kim S. Predictors of caregiver burden in caregivers of individuals with dementia. J Adv Nurs. 2012;68(4):846–855. doi:10.1111/j.1365-2648.2011.05787.x
43. Ge L, Mordiffi SZ. Factors associated with higher caregiver burden among family caregivers of elderly cancer patients: a systematic review. Cancer Nurs. 2017;40(6):471–478. doi:10.1097/NCC.0000000000000445
44. Cohen LW, Zimmerman S, Reed D, et al. Dementia in relation to family caregiver involvement and burden in long-term care. J Appl Gerontol. 2014;33(5):522–540. doi:10.1177/0733464813505701
45. Caputo A. The emotional experience of caregiving in dementia: feelings of guilt and ambivalence underlying narratives of family caregivers. Dementia. 2021;20(7):2248–2260. doi:10.1177/1471301221989604
46. Willemse E, Anthierens S, Farfan-Portet MI, et al. Do informal caregivers for elderly in the community use support measures? A qualitative study in five European countries. BMC Health Serv Res. 2016;16(1):270. doi:10.1186/s12913-016-1487-2
47. Bieber A, Nguyen N, Meyer G, Stephan A. Influences on the access to and use of formal community care by people with dementia and their informal caregivers: a scoping review. BMC Health Serv Res. 2019;19(1):88. doi:10.1186/s12913-018-3825-z
48. Phillipson L, Magee C, Jones SC. Why carers of people with dementia do not utilise out-of-home respite services. Health Soc Care Community. 2013;21(4):411–422. doi:10.1111/hsc.12030
49. Teixeira MJC, Abreu W, Costa N, Maddocks M. Understanding family caregivers’ needs to support relatives with advanced progressive disease at home: an ethnographic study in rural Portugal. BMC Palliat Care. 2020;19(1):73. doi:10.1186/s12904-020-00583-4
50. Lopez-Hartmann M, Wens J, Verhoeven V, Remmen R. The effect of caregiver support interventions for informal caregivers of community-dwelling frail elderly: a systematic review. Int J Integr Care. 2012;12:e133. doi:10.5334/ijic.845
51. Madara Marasinghe K. Assistive technologies in reducing caregiver burden among informal caregivers of older adults: a systematic review. Disabil Rehabil Assist Technol. 2016;11(5):353–360. doi:10.3109/17483107.2015.1087061
52. Williams F, Moghaddam N, Ramsden S, De Boos D. Interventions for reducing levels of burden amongst informal carers of persons with dementia in the community. A systematic review and meta-analysis of randomised controlled trials. Aging Ment Health. 2019;23(12):1629–1642. doi:10.1080/13607863.2018.1515886
53. Wiegelmann H, Speller S, Verhaert L-M, Schirra-Weirich L, Wolf-Ostermann K. Psychosocial interventions to support the mental health of informal caregivers of persons living with dementia – a systematic literature review. BMC Geriatr. 2021;21(1):94. doi:10.1186/s12877-021-02020-4
54. Graff MJ, Vernooij-Dassen MJ, Thijssen M, Dekker J, Hoefnagels WH, Olderikkert MG. Effects of community occupational therapy on quality of life, mood, and health status in dementia patients and their caregivers: a randomized controlled trial. J Gerontol a Biol Sci Med Sci. 2007;62(9):1002–1009. doi:10.1093/gerona/62.9.1002
55. Boezeman EJ, Nieuwenhuijsen K, Sluiter JK. An intervention that reduces stress in people who combine work with informal care: randomized controlled trial results. Eur J Public Health. 2018;28(3):485–489. doi:10.1093/eurpub/cky052
56. Mulquiny L, Oakman J. Exploring the experience of reablement: a systematic review and qualitative evidence synthesis of older people’s and carers’ views. Health Soc Care Community. 2022;30(5):e1471–e1483. doi:10.1111/hsc.13837
57. Chiang YH, Hsu HC, Chen CL, et al. Evaluation of reablement home care: effects on care attendants, care recipients, and family caregivers. Int J Environ Res Public Health. 2020;17(23):8784. doi:10.3390/ijerph17238784
58. Al-Janabi H, Carmichael F, Oyebode J. Informal care: choice or constraint? Scand J Caring Sci. 2018;32(1):157–167. doi:10.1111/scs.12441
59. Zarzycki M, Seddon D, Morrison V. Informal caregiver motivations, values, challenges and gains: a photovoice and interpretative phenomenological analysis of interrelationships. J Health Psychol. 2023;28(6):568–582. doi:10.1177/13591053221124647
60. Backhaus R, Hoek LJM, de Vries E, van Haastregt JCM, Hamers JPH, Verbeek H. Interventions to foster family inclusion in nursing homes for people with dementia: a systematic review. BMC Geriatr. 2020;20(1):434. doi:10.1186/s12877-020-01836-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.